
Correlation of Hemodynamic and Respiratory Parameters in Invasive Cardiopulmonary Exercise Testing (iCPET)


Abstract
1. Introduction
2. Patients and Methods
2.1. Patients
2.2. Right Heart Catheterization
2.3. Cardiopulmonary Exercise Test and Blood Gas Analysis
2.4. Statistics
3. Results
3.1. Patient Characteristics
3.2. Oxygen Uptake and Hemodynamic Parameters
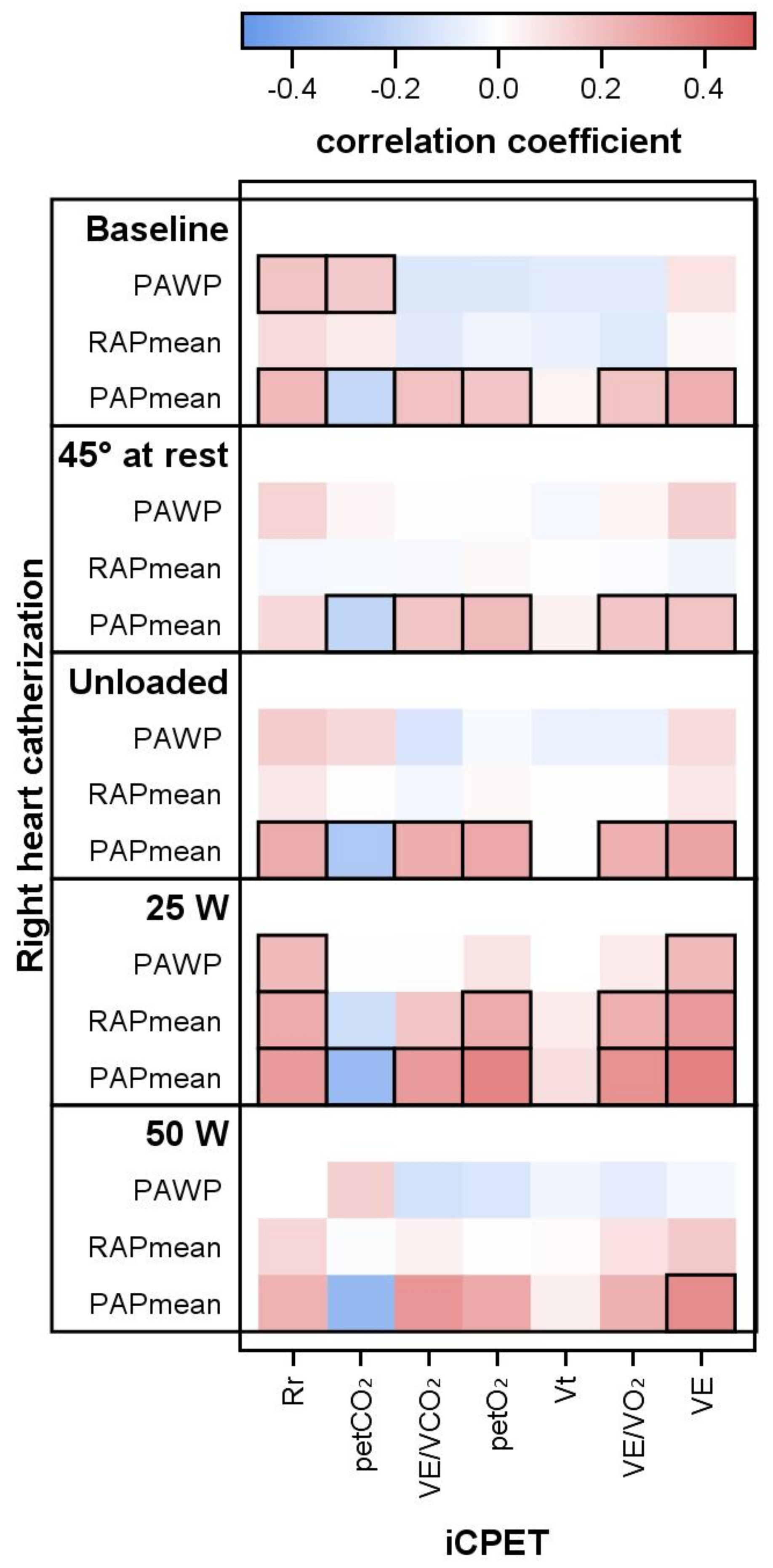
3.3. Respiratory Parameters and PAPmean, PAWP and PVR
4. Discussion
4.1. iCPET and Correlations
4.2. Physiological Considerations
5. Strengths of the Study
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AaDO | arterial-alveolar pressure difference for oxygen |
| CI | cardiac index |
| CHF | chronic heart failure |
| CO | cardiac output |
| CPET | cardiopulmonary exercise testing |
| iCPET | invasive cardiopulmonary exercise testing |
| HFpEF | heart failure with preserved ejection fraction |
| HFrEF | heart failure with reduced ejection fraction |
| pCO | arterial partial pressure of carbon dioxide |
| pO | arterial partial pressure of oxygen |
| pCO | end-tidal partial pressure of carbon dioxide |
| pO | end-tidal partial pressure of oxygen |
| PAH | pulmonary arterial hypertension |
| PAPmean | mean pulmonary artery pressure |
| PAWP | pulmonary arterial wedge pressure |
| peakVO | maximum oxygen uptake per minute at exercise |
| PH | pulmonary hypertension |
| PVR | pulmonary vascular resistance |
| RER | respiratory exchange ratio |
| RHC | right heart catheterisation |
| Rr | respiratory rate |
| RV | right ventricular systolic pressure |
| SD | standard deviation |
| TD | thermodilution |
| V | physiological dead space |
| VE | ventilation per minute |
| V | tidal volume |
| VE/VCO | ventilation to carbon dioxide output ratio |
| VE/VO | ventilation to oxygen uptake ratio |
| VE/VCO-slope | slope of the relation of ventilation and carbon dioxide output, ventilatory efficiency |
| VO | oxygen uptake per minute |
| WU | Wood unit |
References
- Kovacs, G.; Herve, P.; Barbera, J.A.; Chaouat, A.; Chemla, D.; Condliffe, R.; Garcia, G.; Grünig, E.; Howard, L.; Humbert, M.; et al. An official European Respiratory Society statement: Pulmonary haemodynamics during exercise. Eur. Respir. J. 2017, 50, 1700578. [Google Scholar] [CrossRef] [PubMed]
- Oudiz, R.J. The Role of Exercise Testing in the Management of Pulmonary Arterial Hypertension. Semin. Respir. Crit. Care Med. 2005, 26, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Ewert, R.; Obst, A.; Mühle, A.; Halank, M.; Winkler, J.; Trümper, B.; Hoheisel, G.; Hoheisel, A.; Wiersbitzky, M.; Heine, A.; et al. Value of Cardiopulmonary Exercise Testing in the Prognosis Assessment of Chronic Obstructive Pulmonary Disease Patients: A Retrospective, Multicentre Cohort Study. Respiration 2021, 101, 353–366. [Google Scholar] [CrossRef] [PubMed]
- Corrà, U.; Agostoni, P.G.; Anker, S.D.; Coats, A.J.; Leiro, M.G.C.; de Boer, R.A.; Harjola, V.P.; Hill, L.; Lainscak, M.; Lund, L.H.; et al. Role of cardiopulmonary exercise testing in clinical stratification in heart failure. A position paper from the Committee on Exercise Physiology and Training of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2017, 20, 3–15. [Google Scholar] [CrossRef] [PubMed]
- Agostoni, P.; Dumitrescu, D. How to perform and report a cardiopulmonary exercise test in patients with chronic heart failure. Int. J. Cardiol. 2019, 288, 107–113. [Google Scholar] [CrossRef]
- Metra, M.; Faggiano, P.; D’Aloia, A.; Nodari, S.; Gualeni, A.; Raccagni, D.; Cas, L.D. Use of cardiopulmonary exercise testing with hemodynamic monitoring in the prognostic assessment of ambulatory patients with chronic heart failure. J. Am. Coll. Cardiol. 1999, 33, 943–950. [Google Scholar] [CrossRef]
- Nayor, M.; Xanthakis, V.; Tanguay, M.; Blodgett, J.B.; Shah, R.V.; Schoenike, M.; Sbarbaro, J.; Farrell, R.; Malhotra, R.; Houstis, N.E.; et al. Clinical and Hemodynamic Associations and Prognostic Implications of Ventilatory Efficiency in Patients With Preserved Left Ventricular Systolic Function. Circ. Heart Fail. 2020, 13, e006729. [Google Scholar] [CrossRef]
- Ho, J.E.; Zern, E.K.; Lau, E.S.; Wooster, L.; Bailey, C.S.; Cunningham, T.; Eisman, A.S.; Hardin, K.M.; Farrell, R.; Sbarbaro, J.A.; et al. Exercise Pulmonary Hypertension Predicts Clinical Outcomes in Patients With Dyspnea on Effort. J. Am. Coll. Cardiol. 2020, 75, 17–26. [Google Scholar] [CrossRef]
- Huang, W.; Resch, S.; Oliveira, R.K.; Cockrill, B.A.; Systrom, D.M.; Waxman, A.B. Invasive cardiopulmonary exercise testing in the evaluation of unexplained dyspnea: Insights from a multidisciplinary dyspnea center. Eur. J. Prev. Cardiol. 2017, 24, 1190–1199. [Google Scholar] [CrossRef]
- Vignati, C.; Cattadori, G. Measuring Cardiac Output during Cardiopulmonary Exercise Testing. Ann. Am. Thorac. Soc. 2017, 14, S48–S52. [Google Scholar] [CrossRef]
- Berry, N.C.; Manyoo, A.; Oldham, W.M.; Stephens, T.E.; Goldstein, R.H.; Waxman, A.B.; Tracy, J.A.; Leary, P.J.; Leopold, J.A.; Kinlay, S.; et al. Protocol for Exercise Hemodynamic Assessment: Performing an Invasive Cardiopulmonary Exercise Test in Clinical Practice. Pulm. Circ. 2015, 5, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Metra, M.; Cas, L.D.; Panina, G.; Visioli, O. Exercise hyperventilation chronic congestive heart failure, and its relation to functional capacity and hemodynamics. Am. J. Cardiol. 1992, 70, 622–628. [Google Scholar] [CrossRef]
- Raeside, D.; Smith, A.; Brown, A.; Patel, K.; Madhok, R.; Cleland, J.; Peacock, A. Pulmonary artery pressure measurement during exercise testing in patients with suspected pulmonary hypertension. Eur. Respir. J. 2000, 16, 282. [Google Scholar] [CrossRef] [PubMed]
- Galiè, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Noordegraaf, A.V.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [CrossRef] [PubMed]
- Rosenkranz, S.; Behr, J.; Ewert, R.; Ghofrani, H.; Grünig, E.; Halank, M.; Hoeper, M.; Leuchte, H.; Olschewski, H.; Schmeisser, A.; et al. Rechtsherzkatheter-Untersuchung bei pulmonaler Hypertonie. DMW—Dtsch. Med. Wochenschr. 2011, 136, 2601–2625. [Google Scholar] [CrossRef] [PubMed]
- Ewert, R.; Heine, A.; Müller-Heinrich, A.; Bollmann, T.; Obst, A.; Desole, S.; Knaak, C.; Stubbe, B.; Opitz, C.F.; Habedank, D. Exercise and fluid challenge during right heart catheterisation for evaluation of dyspnoea. Pulm. Circ. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- LaFarge, C.G.; Miettinen, O.S. The estimation of oxygen consumption. Cardiovasc. Res. 1970, 4, 23–30. [Google Scholar] [CrossRef]
- Simonneau, G.; Montani, D.; Celermajer, D.S.; Denton, C.P.; Gatzoulis, M.A.; Krowka, M.; Williams, P.G.; Souza, R. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur. Respir. J. 2019, 53, 1801913. [Google Scholar] [CrossRef]
- Koch, B.; Schäper, C.; Ewert, R.; Völzke, H.; Obst, A.; Friedrich, N.; Felix, S.B.; Vogelmeier, C.F.; Schnabel, E.; Karrasch, S.; et al. Lung function reference values in different German populations. Respir. Med. 2011, 105, 352–362. [Google Scholar] [CrossRef][Green Version]
- Gläser, S.; Ittermann, T.; Schäper, C.; Obst, A.; Dörr, M.; Spielhagen, T.; Felix, S.; Völzke, H.; Bollmann, T.; Opitz, C.; et al. Referenzwerte für die Spiroergometrie–Ergebnisse der Study of Health in Pomerania (SHIP). Pneumologie 2012, 67, 58–63. [Google Scholar] [CrossRef]
- Maron, B.A.; Cockrill, B.A.; Waxman, A.B.; Systrom, D.M. The Invasive Cardiopulmonary Exercise Test. Circulation 2013, 127, 1157–1164. [Google Scholar] [CrossRef] [PubMed]
- Schrijen, F.; Ravez, P.; Candina-Villar, R. Respiratory and circulatory adaptation to isometric and dynamic exercise in chronic lung disease. Clin. Physiol. 1984, 4, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, D.; Nagel, C.; Kovacs, G.; Bollmann, T.; Halank, M.; Winkler, J.; Hellmich, M.; Grünig, E.; Olschewski, H.; Ewert, R.; et al. Cardiopulmonary exercise testing for detecting pulmonary arterial hypertension in systemic sclerosis. Heart 2017, 103, 774–782. [Google Scholar] [CrossRef] [PubMed]
- Arena, R.; Owens, D.S.; Arevalo, J.; Smith, K.; Mohiddin, S.A.; Mcareavey, D.; Ulisney, K.L.; Tripodi, D.; Fananapazir, L.; Plehn, J.F. Ventilatory Efficiency and Resting Hemodynamics in Hypertrophic Cardiomyopathy. Med. Sci. Sport. Exerc. 2008, 40, 799–805. [Google Scholar] [CrossRef]
- Taylor, B.J.; Smetana, M.R.; Frantz, R.P.; Johnson, B.D. Submaximal Exercise Pulmonary Gas Exchange in Left Heart Disease Patients With Different Forms of Pulmonary Hypertension. J. Card. Fail. 2015, 21, 647–655. [Google Scholar] [CrossRef]
- Singh, I.; Oliveira, R.K.; Heerdt, P.; Brown, M.B.; Faria-Urbina, M.; Waxman, A.B.; Systrom, D.M. Dynamic right ventricular function response to incremental exercise in pulmonary hypertension. Pulm. Circ. 2020, 10, 1–8. [Google Scholar] [CrossRef]
- Tolle, J.J.; Waxman, A.B.; Horn, T.L.V.; Pappagianopoulos, P.P.; Systrom, D.M. Exercise-Induced Pulmonary Arterial Hypertension. Circulation 2008, 118, 2183–2189. [Google Scholar] [CrossRef]
- Yasunobu, Y.; Oudiz, R.J.; Sun, X.G.; Hansen, J.E.; Wasserman, K. End-tidal PCO2 Abnormality and Exercise Limitation in Patients With Primary Pulmonary Hypertension. Chest 2005, 127, 1637–1646. [Google Scholar] [CrossRef]
- Matsumoto, A.; Itoh, H.; Eto, Y.; Kobayashi, T.; Kato, M.; Omata, M.; Watanabe, H.; Kato, K.; Momomura, S.-i. End-tidal CO2 pressure decreases during exercise in cardiac patients: Association with severity of heart failure and cardiac output reserve. J. Am. Coll. Cardiol. 2000, 36, 242–249. [Google Scholar] [CrossRef]
- Boerrigter, B.G.; Bogaard, H.J.; Trip, P.; Groepenhoff, H.; Rietema, H.; Holverda, S.; Boonstra, A.; Postmus, P.E.; Westerhof, N.; Vonk-Noordegraaf, A. Ventilatory and Cardiocirculatory Exercise Profiles in COPD. Chest 2012, 142, 1166–1174. [Google Scholar] [CrossRef]
- Kozitza, C.J.; Dharmavaram, N.; Tao, R.; Tabima, D.M.; Chesler, N.C.; Raza, F. Pulmonary vascular distensibility with passive leg raise is comparable to exercise and predictive of clinical outcomes in pulmonary hypertension. Pulm. Circ. 2022, 12. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Patients | Percent | Median (25th; 75th) |
|---|---|---|---|
| n = 146 | |||
| female | 72 | 49.3 | |
| age | (range 22–85) | 69 (59; 76) | |
| height (cm) | 170 (162; 176) | ||
| weight (kg) | 80 (68; 98) | ||
| BMI (kg/m²) | 27.2 (24.1; 32.4) | ||
| Diagnoses leading to iCPET | |||
| HFpEF | 44 | 30.1 | |
| CTD including systemic sclerosis | 25 | 17.1 | |
| PAH (suspected echocardiography) | 25 | 17.1 | |
| pulmonary embolism | 20 | 13.7 | |
| interstitial lung disease | 6 | 4.1 | |
| COPD | 5 | 3.4 | |
| HFrEF | 5 | 3.4 | |
| congenital heart disease | 5 | 3.4 | |
| dyspnea of unknown orign | 4 | 2.7 | |
| other with n ≤ 2 | 7 | 4.8 | |
| Comorbidities | |||
| (double categorization possible) | |||
| arterial hypertension | 97 | 66.4 | |
| atrial fibrillation | 45 | 30.8 | |
| diabetes mellitus | 42 | 28.8 | |
| venous thrombembolism | 41 | 28.1 | |
| coronary heart disease | 37 | 25.3 | |
| history of cancer | 26 | 17.8 | |
| chronic renal failure | 24 | 16.4 | |
| peripheral arterial obstruction | 3 | 2.1 | |
| Echocardiography | 135 | 92.5 | |
| LVEF 35–40% | 2 | 1.5 | |
| LVEF ≥ 50% | 133 | 98.5 | |
| TAPSE (mm) | 116 | ||
| TR ≥ 1° | 81 | 60.0 | |
| RV estimated (mmHg) | 92 | ||
| diastolic dysfunktion | 55 | 40.7 | |
| Right heart catheterization at rest | |||
| RAPmean (mmHg) | 144 | 8.0 (6.0; 11.0) | |
| PAPmean (mmHg) | 146 | 28.0 (20.0; 40.0) | |
| PAPmean ≥ 25 mmHg | 83 | 56.8 | |
| PAWP (mmHg) | 144 | 14.0 (10.0; 19.0) | |
| PAWP < 15 mmHg | |||
| PVR (WU) TD | 144 | 2.34 (1.32; 3.90) | |
| CO (l/min) TD | 145 | 5.00 (4.28; 6.01) | |
| CI (l/min/m²) TD | 145 | 2.61 (2.28; 3.02) | |
| PVR (WU) iFM | 143 | 2.68 (1.47; 4.74) | |
| CO (l/min) iFM | 145 | 4.30 (3.64; 5.05) | |
| CI (l/min/m²) iFM | 144 | 2.25 (1.98; 2.57) | |
| PVR (WU) dFM | 140 | 2.24 (1.20; 3.52) | |
| CO (l/min) dFM | 141 | 5.55 (4.34; 6.73) | |
| CI (l/min/m²) dFM | 141 | 2.88 (2.45; 3.49) | |
| Pulmonary function | |||
| TLC (% predicted) | 132 | 93.4 (81.9; 104.4) | |
| reduced < 80% | 31 | 23.5 | |
| FVC (% predicted) | 137 | 92.3 (5.5; 104.5) | |
| reduced < 80% | 40 | 29.2 | |
| FEV1 (% predicted) | 137 | 86.1 (69.4; 97.9) | |
| FEV1/FVC (%) | 137 | 75.8 (69.9; 80.2) | |
| RV (% predicted) | 132 | 107.6 (87.1; 121.0) | |
| RV/TLC (% predicted) | 131 | 44.8 (38.3; 50.9) | |
| DLCO (% predicted) | 122 | 59.8 (44.1; 72.2) | |
| Reduced < 60% | 62 | 50.8 | |
| KCO (% predicted) | 100 | 74.2 (56.4; 90.5) | |
| reduced < 60% | 28 | 28.0 | |
| Cardiopulmonary exercise testing | |||
| maximum power (Watt) | 142 | 84.0 (52.0; 100.0) | |
| maximum power (% predicted) | 142 | 57.3 (43.7; 69.1) | |
| peakVO (ml/min/kg) | 139 | 13.5 (11.3; 17.6) | |
| peakVO (% predicted) | 142 | 63.6 (51.7; 75.4) | |
| peakVO/HR (ml) | 142 | 10.0 (8.0; 12.8) | |
| VE/VCO-slope | 142 | 40.0 (32.0; 49.0) | |
| increased > 34 | 98 | 69.0 | |
| VE/VCO @rest | 138 | 41.0 (5.7; 47.7) | |
| VE/VCO @AT | 134 | 38.2 (32.6; 44.5) | |
| pCO @rest (mmHg) | 142 | 27.1 (23.3; 30.5) | |
| pCO @AT | 136 | 29.0 (25.1; 33.5) | |
| peak AaDO (mmHg) | 141 | 40.5 (31.0; 56.2) | |
| increased > 35 mmHg | 93 | 66.0 | |
| pCO (mmHg) | 141 | 7.2 (4.4; 10.2) | |
| VE/MVV (%) | 137 | 63.1 (49.8; 73.7) | |
| increased > 80% | 13 | 9.5 | |
| pO @rest (mmHg) | 142 | 70.8 (58.5; 77.4) | |
| pO @peak (mmHg) | 141 | 68.1 (54.4; 81.5) | |
| pCO @rest (mmHg) | 142 | 35.0 (31.9; 37.8) | |
| pCO @peak (mmHg) | 141 | 34.7 (31.2; 38.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Habedank, D.; Obst, A.; Heine, A.; Stubbe, B.; Ewert, R. Correlation of Hemodynamic and Respiratory Parameters in Invasive Cardiopulmonary Exercise Testing (iCPET). Life 2022, 12, 655. https://doi.org/10.3390/life12050655
Habedank D, Obst A, Heine A, Stubbe B, Ewert R. Correlation of Hemodynamic and Respiratory Parameters in Invasive Cardiopulmonary Exercise Testing (iCPET). Life. 2022; 12(5):655. https://doi.org/10.3390/life12050655
Chicago/Turabian StyleHabedank, Dirk, Anne Obst, Alexander Heine, Beate Stubbe, and Ralf Ewert. 2022. "Correlation of Hemodynamic and Respiratory Parameters in Invasive Cardiopulmonary Exercise Testing (iCPET)" Life 12, no. 5: 655. https://doi.org/10.3390/life12050655
APA StyleHabedank, D., Obst, A., Heine, A., Stubbe, B., & Ewert, R. (2022). Correlation of Hemodynamic and Respiratory Parameters in Invasive Cardiopulmonary Exercise Testing (iCPET). Life, 12(5), 655. https://doi.org/10.3390/life12050655