
Ki67 and LSD1 Expression in Testicular Germ Cell Tumors Is Not Associated with Patient Outcome: Investigation Using a Digital Pathology Algorithm

 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
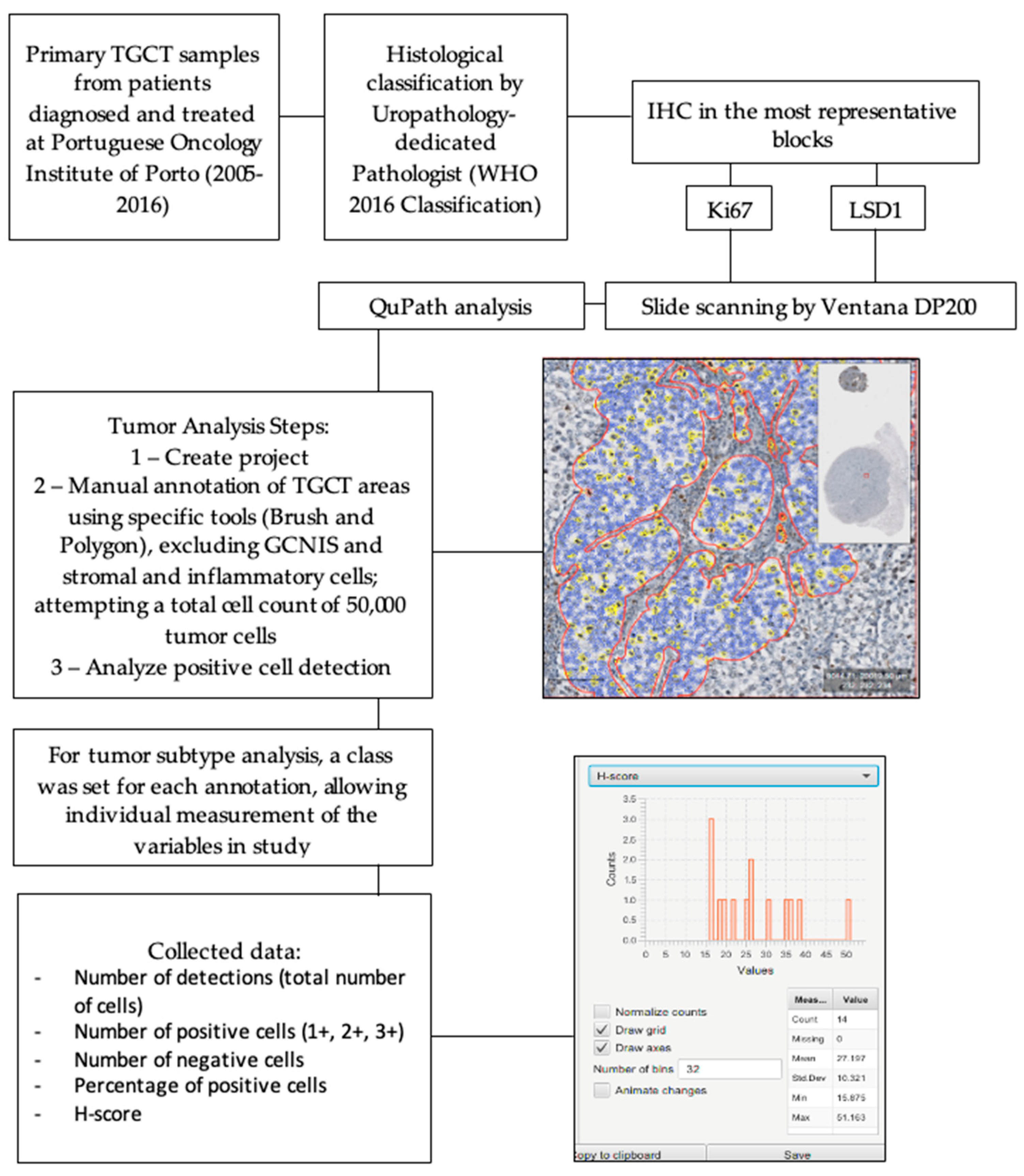
2. Materials and Methods
2.1. Patients and Samples
2.2. Immunohistochemistry
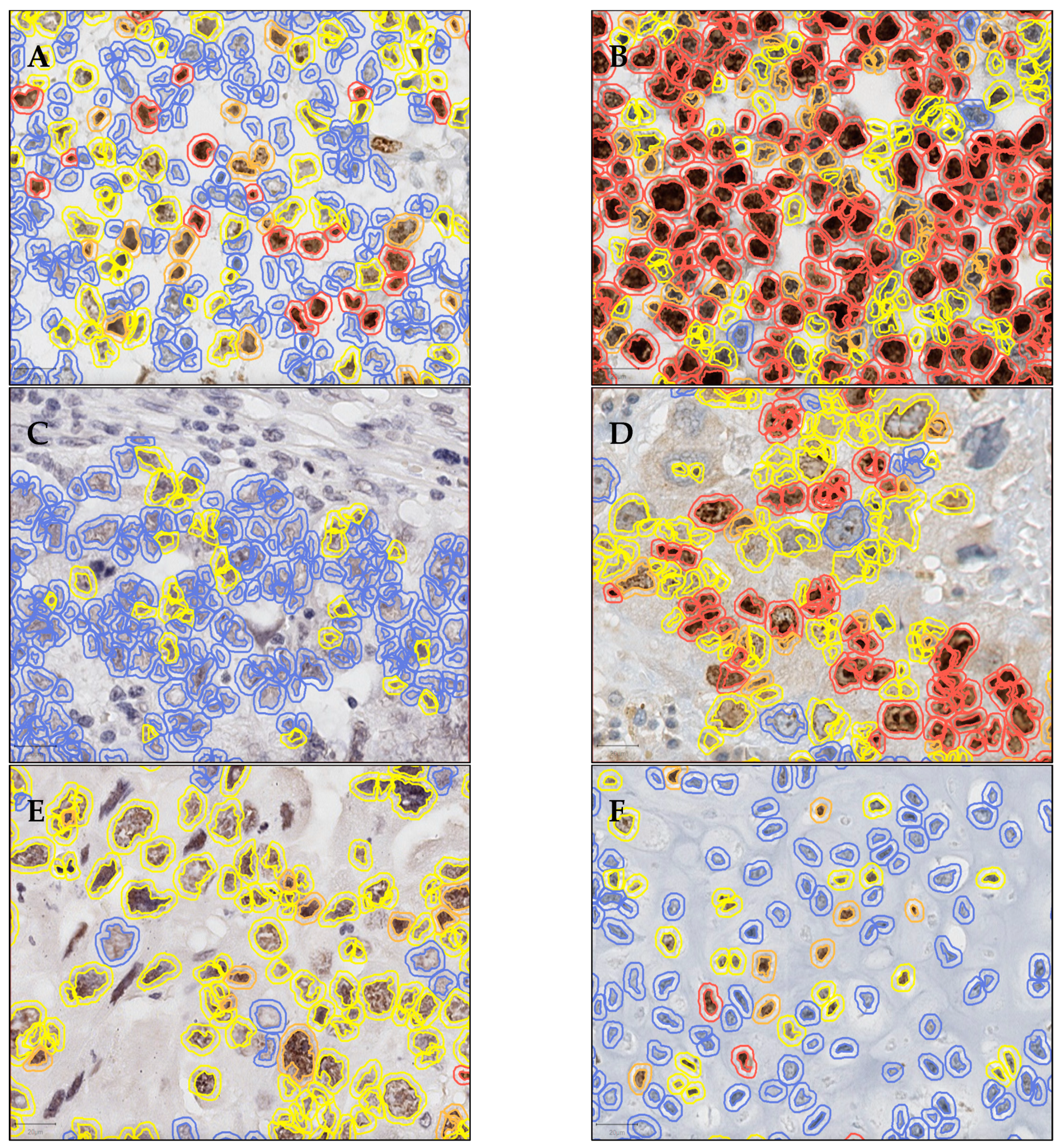
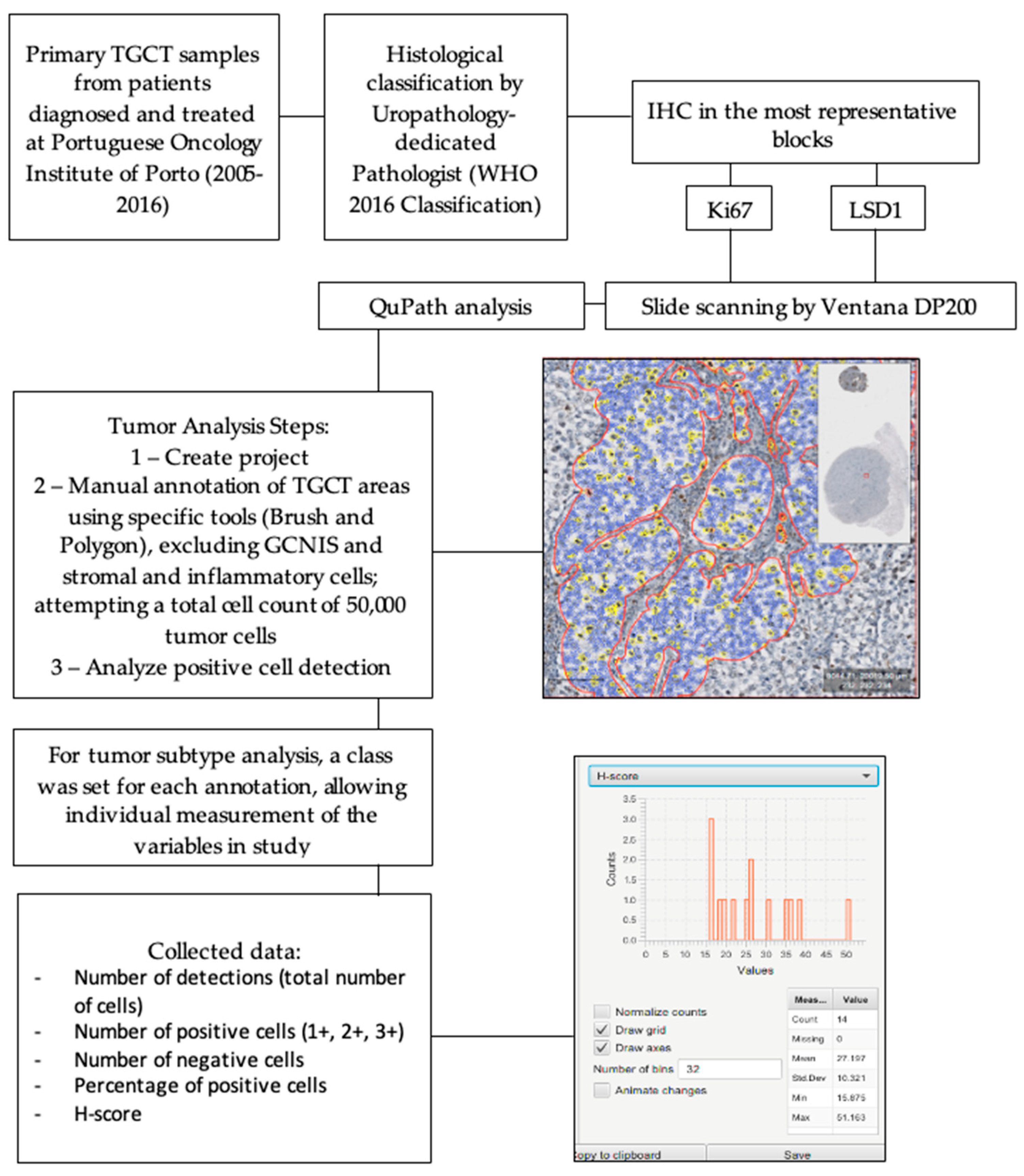
2.3. Digital Pathology Analysis
2.4. In Silico Analysis
2.5. Cell Lines and Treatments
2.6. Western Blot
2.7. Statistical Analysis
3. Results
3.1. Cohort Characterization
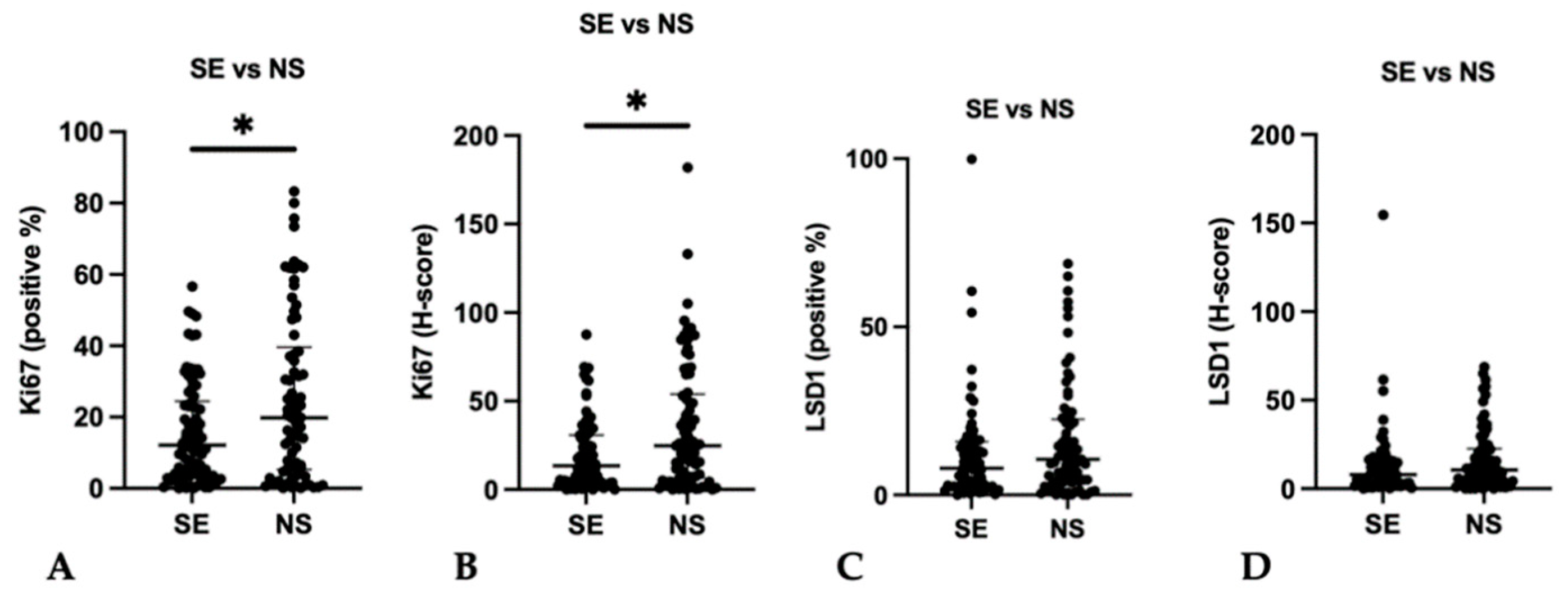
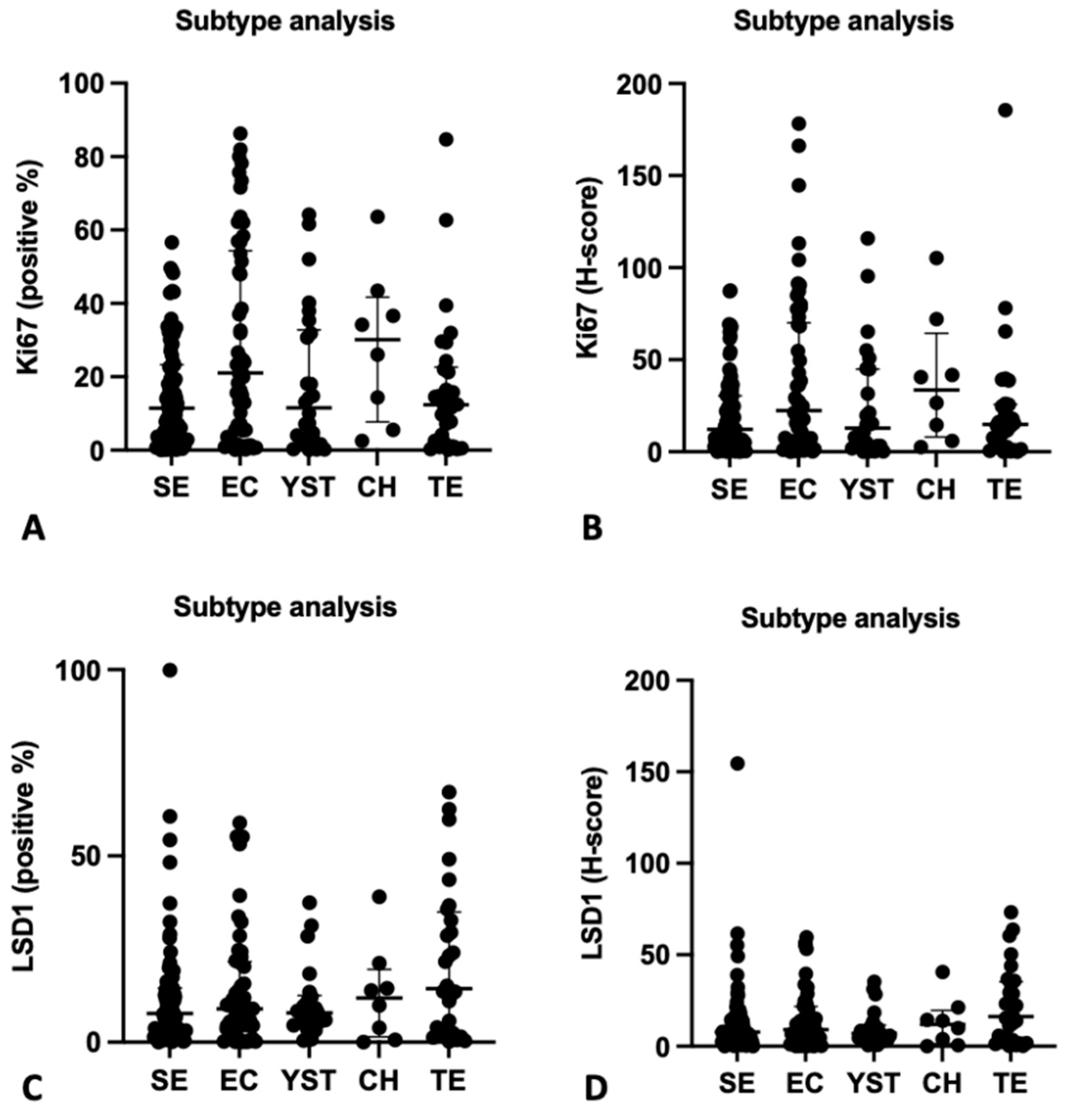
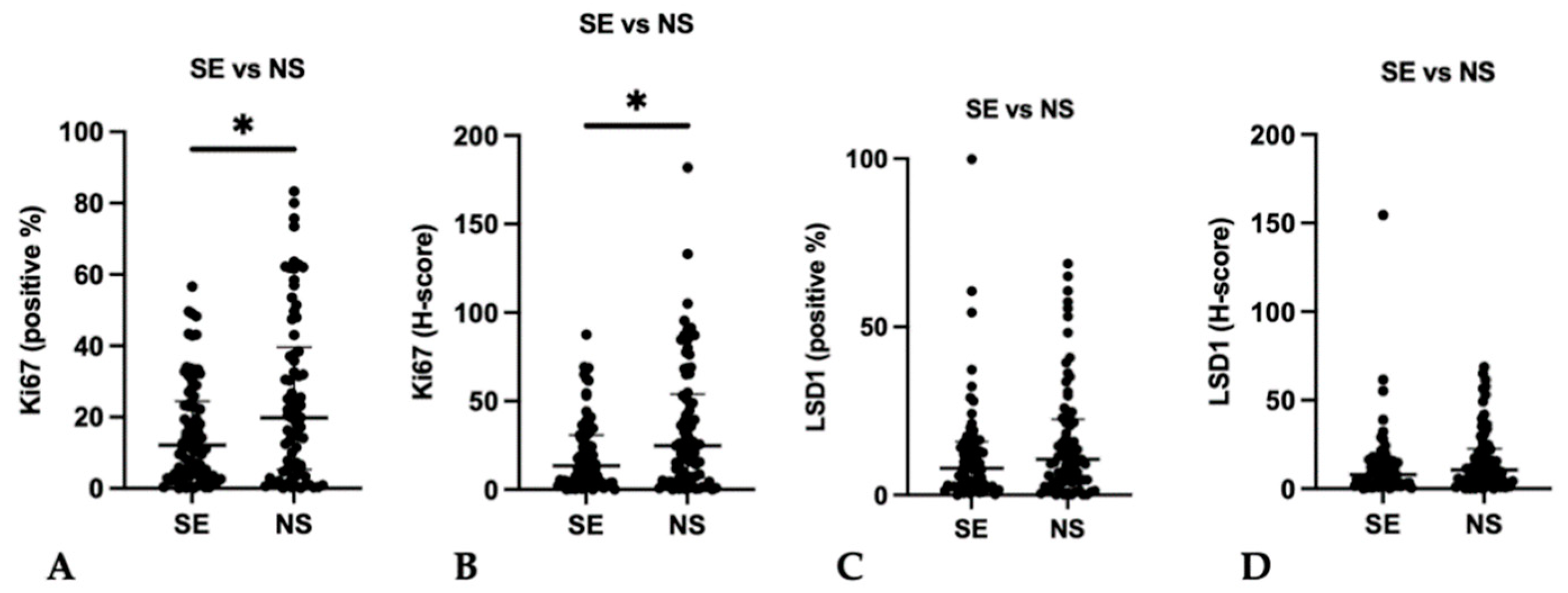
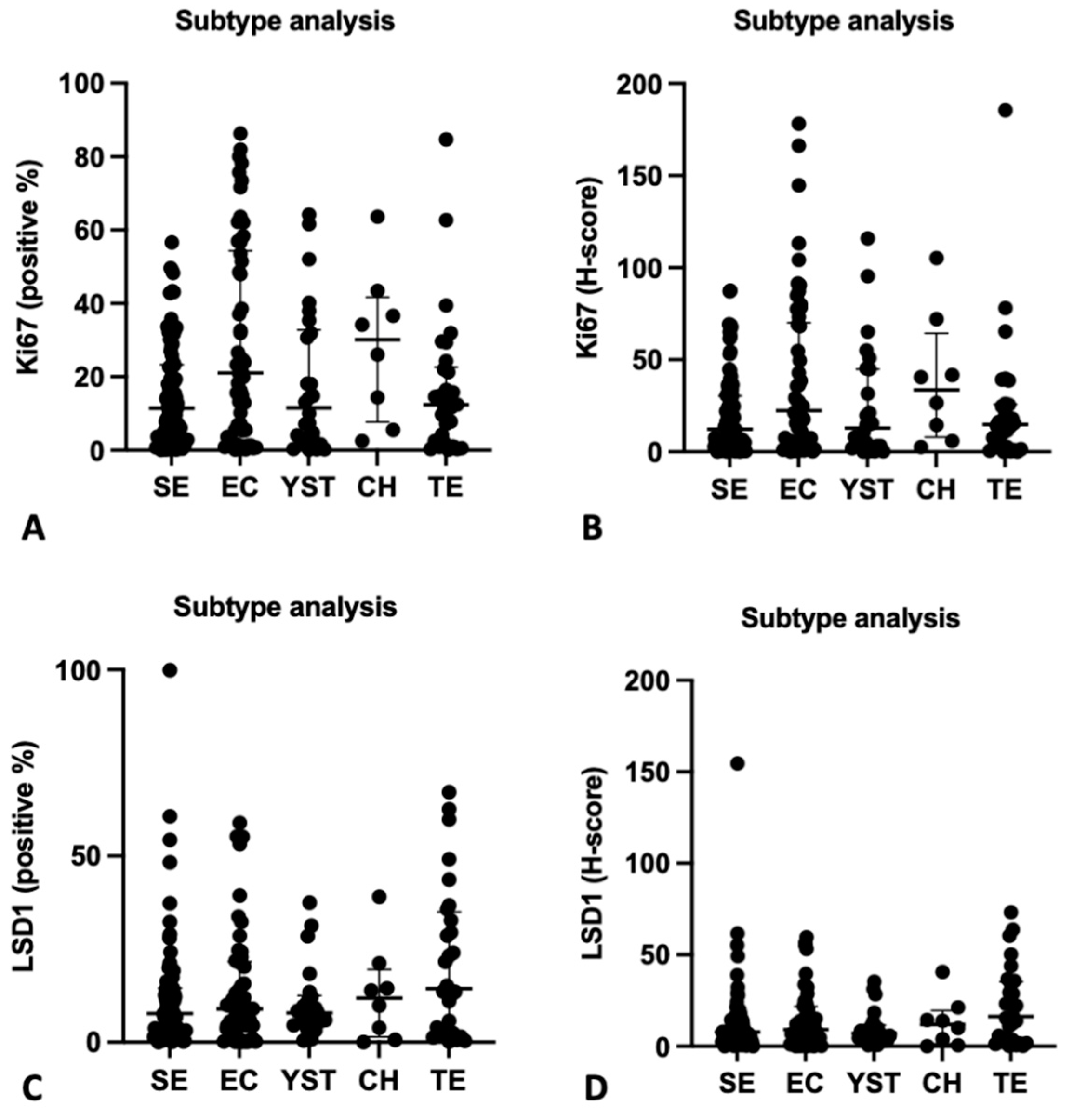
3.2. Immunoexpression of Ki67 and LSD1
3.3. Association with Clinicopathological Features
3.4. In Silico Study—cBioportal Data
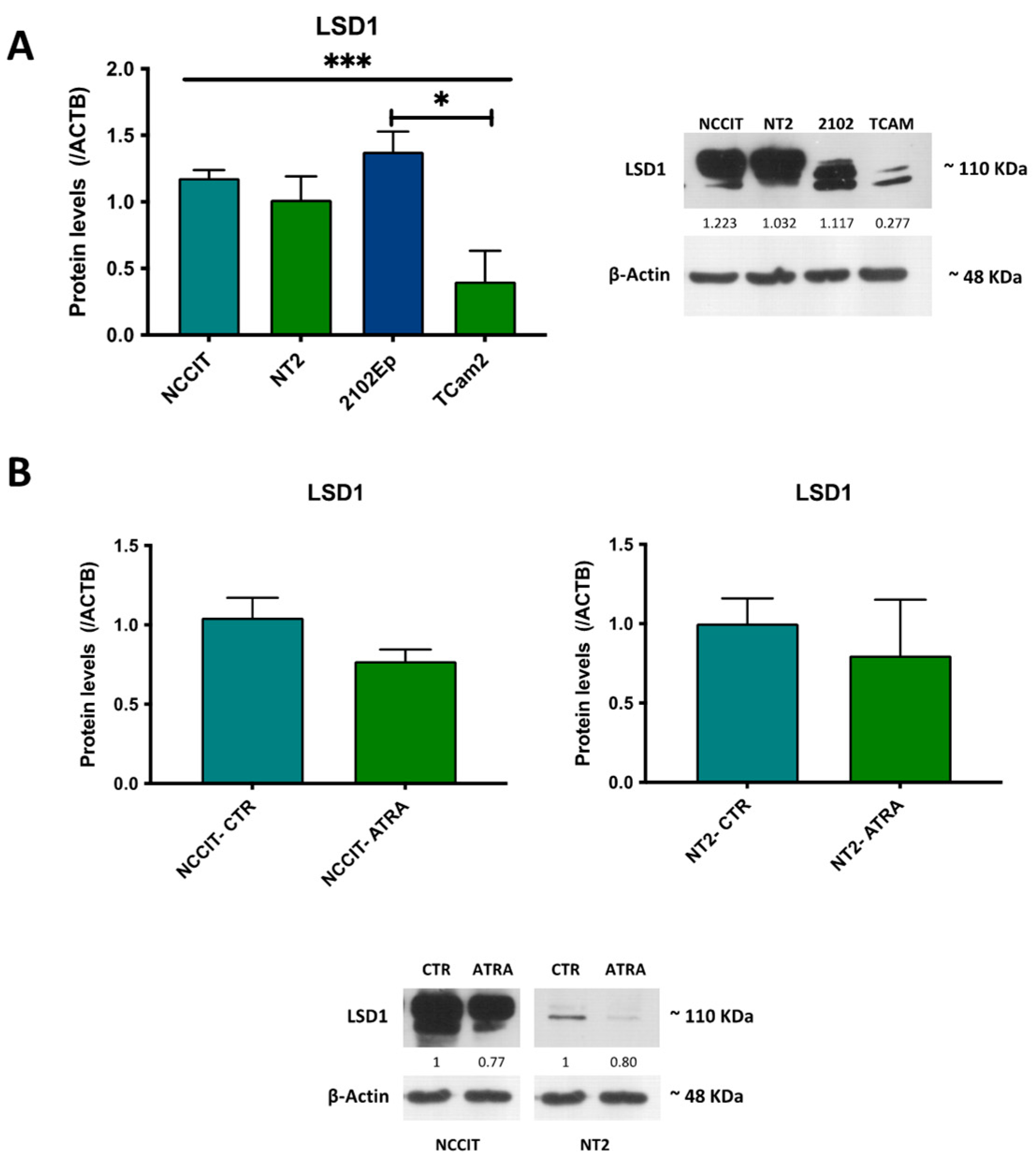
3.5. In Vitro Study—LSD1 Expression in TGCT Cell Lines
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- National Comprehensive Cancer Network. Testicular Cancer NCCN Clinical Pratice Guidelines in Oncology; Version 1.2022; 2021, NCCN Clinical Practice Guidelines in Oncology. Available online: www.nccn.org (accessed on 10 December 2021).
- Lobo, J.; Gillis, A.J.M.; Jeronimo, C.; Henrique, R.; Looijenga, L.H.J. Human Germ Cell Tumors are Developmental Cancers: Impact of Epigenetics on Pathobiology and Clinic. Int. J. Mol. Sci. 2019, 20, 258. [Google Scholar] [CrossRef] [Green Version]
- Lobo, J.; Alzamora, M.A.; Guimaraes, R.; Cantante, M.; Lopes, P.; Braga, I.; Mauricio, J.; Jeronimo, C.; Henrique, R. p53 and MDM2 expression in primary and metastatic testicular germ cell tumors: Association with clinical outcome. Andrology 2020, 8, 1233–1242. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, A.R.; Lobo, J.; Miranda-Goncalves, V.; Henrique, R.; Jeronimo, C. Epigenetic alterations as therapeutic targets in Testicular Germ Cell Tumours: Current and future application of ‘epidrugs’. Epigenetics 2021, 16, 353–372. [Google Scholar] [CrossRef] [PubMed]
- Costa, A.L.; Lobo, J.; Jerónimo, C.; Henrique, R. The epigenetics of testicular germ cell tumors: Looking for novel disease biomarkers. Epigenomics 2017, 9, 155–169. [Google Scholar] [CrossRef] [PubMed]
- Lobo, J.; Rodrigues, A.; Guimaraes, R.; Cantante, M.; Lopes, P.; Mauricio, J.; Oliveira, J.; Jeronimo, C.; Henrique, R. Detailed Characterization of Immune Cell Infiltrate and Expression of Immune Checkpoint Molecules PD-L1/CTLA-4 and MMR Proteins in Testicular Germ Cell Tumors Disclose Novel Disease Biomarkers. Cancers 2019, 11, 1535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sturgeon, C.M.; Duffy, M.J.; Stenman, U.-H.; Lilja, H.; Brunner, N.; Chan, D.W.; Babaian, R.; Bast, R.C.J.; Dowell, B.; Esteva, F.; et al. National Academy of Clinical Biochemistry laboratory medicine practice guidelines for use of tumor markers in testicular, prostate, colorectal, breast, and ovarian cancers. Clin. Chem. 2008, 54, e11–e79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobo, J.; Stoop, H.; Gillis, A.J.M.; Looijenga, L.H.J.; Oosterhuis, W. Interobserver Agreement in Vascular Invasion Scoring and the Added Value of Immunohistochemistry in Stage I Testicular Nonseminoma. Am. J. Surg. Pathol. 2019, 43, 1711–1719. [Google Scholar] [CrossRef]
- Lobo, J.; Gillis, A.J.M.; van den Berg, A.; Looijenga, L.H.J. Prediction of relapse in stage I testicular germ cell tumor patients on surveillance: Investigation of biomarkers. BMC Cancer 2020, 20, 728. [Google Scholar] [CrossRef]
- Burger, H.; Nooter, K.; Boersma, A.W.; Van Wingerden, K.E.; Looijenga, L.H.; Jochemsen, A.G.; Stoter, G. Distinct p53-Independent Apoptotic Cell Death Signalling Pathways In Testicular Germ Cell Tumour Cell Lines. Int. J. Cancer 1999, 81, 620–628. [Google Scholar] [CrossRef]
- Boormans, J.L.; Mayor de Castro, J.; Marconi, L.; Yuan, Y.; Laguna Pes, M.P.; Bokemeyer, C.; Nicolai, N.; Algaba, F.; Oldenburg, J.; Albers, P. Testicular Tumour Size and Rete Testis Invasion as Prognostic Factors for the Risk of Relapse of Clinical Stage I Seminoma Testis Patients Under Surveillance: A Systematic Review by the Testicular Cancer Guidelines Panel. Eur. Urol. 2018, 73, 394–405. [Google Scholar] [CrossRef]
- Leao, R.; Ahmad, A.E.; Hamilton, R.J. Testicular Cancer Biomarkers: A Role for Precision Medicine in Testicular Cancer. Clin. Genitourin. Cancer 2019, 17, e176–e183. [Google Scholar] [CrossRef]
- Lobo, J.; Jeronimo, C.; Henrique, R. Targeting the Immune system and Epigenetic Landscape of Urological Tumors. Int. J. Mol. Sci. 2020, 21, 829. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gilbert, D.C.; Al-Saadi, R.; Thway, K.; Chandler, I.; Berney, D.; Gabe, R.; Stenning, S.P.; Sweet, J.; Huddart, R.; Shipley, J.M. Defining a New Prognostic Index for Stage I Nonseminomatous Germ Cell Tumors Using CXCL12 Expression and Proportion of Embryonal Carcinoma. Clin. Cancer Res. 2016, 22, 1265–1273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belt-Dusebout, A.W.v.d.; de Wit, R.; Gietema, J.A.; Horenblas, S.; Louwman, M.W.; Ribot, J.G.; Hoekstra, H.J.; Ouwens, G.M.; Aleman, B.M.; van Leeuwen, F.E. Treatment-specific risks of second malignancies and cardiovascular disease in 5-year survivors of testicular cancer. J. Clin. Oncol. 2007, 25, 4370–4378. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, R.J.; Nayan, M.; Anson-Cartwright, L.; Atenafu, E.G.; Bedard, P.L.; Hansen, A.; Chung, P.; Warde, P.; Sweet, J.; O’Malley, M.; et al. Treatment of Relapse of Clinical Stage I Nonseminomatous Germ Cell Tumors on Surveillance. J. Clin. Oncol. 2019, 37, 1919–1926. [Google Scholar] [CrossRef]
- Pulzova, L.B.; Roska, J.; Kalman, M.; Kliment, J.; Slavik, P.; Smolkova, B.; Goffa, E.; Jurkovicova, D.; Kulcsar, L.; Leskova, K.; et al. Screening for the Key Proteins Associated with Rete Testis Invasion in Clinical Stage I Seminoma via Label-Free Quantitative Mass Spectrometry. Cancers 2021, 13, 5573. [Google Scholar] [CrossRef]
- Lobo, J.; Rodrigues, A.; Antunes, L.; Graca, I.; Ramalho-Carvalho, J.; Vieira, F.Q.; Martins, A.T.; Oliveira, J.; Jeronimo, C.; Henrique, R. High immunoexpression of Ki67, EZH2, and SMYD3 in diagnostic prostate biopsies independently predicts outcome in patients with prostate cancer. Urol. Oncol. 2018, 36, 161 e7–161 e17. [Google Scholar] [CrossRef]
- Gallegos, I.; Valdevenito, J.P.; Miranda, R.; Fernandez, C. Immunohistochemistry Expression of P53, Ki67, CD30, and CD117 and Presence of Clinical Metastasis at Diagnosis of Testicular Seminoma. Appl. Immunohistochem. Mol. Morphol. 2011, 19, 147–152. [Google Scholar] [CrossRef]
- Albers, P.; Siener, R.; Kliesch, S.; Weissbach, L.; Krege, S.; Sparwasser, C.; Schulze, H.; Heidenreich, A.; de Riese, W.; Loy, V.; et al. Risk factors for relapse in clinical stage I nonseminomatous testicular germ cell tumors: Results of the German Testicular Cancer Study Group Trial. J. Clin. Oncol. 2003, 21, 1505–1512. [Google Scholar] [CrossRef]
- Albers, P.; Bierhoff, E.; Neu, D.; Fimmers, R.; Wernert, N.; Muller, S.C. MIB-1 Immunohistochemistry in Clinical Stage I Nonseminomatous Testicular Germ Cell Tumors Predicts Patients at Low Risk for Metastasis. Am. Cancer Soc. 1996, 79, 1710–1716. [Google Scholar]
- Skowron, M.A.; Oing, C.; Bremmer, F.; Strobel, P.; Murray, M.J.; Coleman, N.; Amatruda, J.F.; Honecker, F.; Bokemeyer, C.; Albers, P.; et al. The developmental origin of cancers defines basic principles of cisplatin resistance. Cancer Lett. 2021, 519, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Lobo, J.; Constancio, V.; Leite-Silva, P.; Guimaraes, R.; Cantante, M.; Braga, I.; Mauricio, J.; Looijenga, L.H.J.; Henrique, R.; Jeronimo, C. Differential methylation EPIC analysis discloses cisplatin-resistance related hypermethylation and tumor-specific heterogeneity within matched primary and metastatic testicular germ cell tumor patient tissue samples. Clin. Epigenetics 2021, 13, 70. [Google Scholar] [CrossRef] [PubMed]
- Muller, M.R.; Skowron, M.A.; Albers, P.; Nettersheim, D. Molecular and epigenetic pathogenesis of germ cell tumors. Asian J. Urol. 2021, 8, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.; Fazal, Z.; Freemantle, S.; Spinella, M. Between a Rock and a Hard Place: An Epigenetic-Centric View of Testicular Germ Cell Tumors. Cancers 2021, 13, 1506. [Google Scholar] [CrossRef]
- Majello, B.; Gorini, F.; Saccà, C.D.; Amente, S. Expanding the Role of the Histone Lysine-Specific Demethylase LSD1 in Cancer. Cancers 2019, 11, 324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayami, S.; Kelly, J.D.; Cho, H.S.; Yoshimatsu, M.; Unoki, M.; Tsunoda, T.; Field, H.I.; Neal, D.E.; Yamaue, H.; Ponder, B.A.; et al. Overexpression of LSD1 contributes to human carcinogenesis through chromatin regulation in various cancers. Int. J. Cancer 2011, 128, 574–586. [Google Scholar] [CrossRef] [PubMed]
- Hoang, N.; Zhang, X.; Zhang, C.; Vo, V.; Leng, F.; Saxena, L.; Yin, F.; Lu, F.; Zheng, G.; Bhowmik, P.; et al. New histone demethylase LSD1 inhibitor selectively targets teratocarcinoma and embryonic carcinoma cells. Bioorg. Med. Chem. 2018, 26, 1523–1537. [Google Scholar] [CrossRef] [PubMed]
- Jostes, S.; Nettersheim, D.; Schorle, H. Epigenetic drugs and their molecular targets in testicular germ cell tumours. Nat. Rev. Urol. 2019, 16, 245–259. [Google Scholar] [CrossRef]
- Lobo, J.; Costa, A.L.; Vilela-Salgueiro, B.; Rodrigues, A.; Guimaraes, R.; Cantante, M.; Lopes, P.; Antunes, L.; Jeronimo, C.; Henrique, R. Testicular germ cell tumors: Revisiting a series in light of the new WHO classification and AJCC staging systems, focusing on challenges for pathologists. Hum. Pathol. 2018, 82, 113–124. [Google Scholar] [CrossRef]
- Cerami, E.; Gao, J.; Dogrusoz, U.; Gross, B.E.; Sumer, S.O.; Aksoy, B.A.; Jacobsen, A.; Byrne, C.J.; Heuer, M.L.; Larsson, E.; et al. The cBio cancer genomics portal: An open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012, 2, 401–404. [Google Scholar] [CrossRef] [Green Version]
- Lobo, J.; Gillis, A.J.M.; van den Berg, A.; Dorssers, L.C.J.; Belge, G.; Dieckmann, K.P.; Roest, H.P.; van der Laan, L.J.W.; Gietema, J.; Hamilton, R.J.; et al. Identification and Validation Model for Informative Liquid Biopsy-Based microRNA Biomarkers: Insights from Germ Cell Tumor In Vitro, In Vivo and Patient-Derived Data. Cells 2019, 8, 1637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobo, J.; Cardoso, A.R.; Miranda-Goncalves, V.; Looijenga, L.H.J.; Lopez, M.; Arimondo, P.B.; Henrique, R.; Jeronimo, C. Targeting Germ Cell Tumors with the Newly Synthesized Flavanone-Derived Compound MLo1302 Efficiently Reduces Tumor Cell Viability and Induces Apoptosis and Cell Cycle Arrest. Pharmaceutics 2021, 13, 73. [Google Scholar] [CrossRef] [PubMed]
- Miranda-Goncalves, V.; Lobo, J.; Guimaraes-Teixeira, C.; Barros-Silva, D.; Guimaraes, R.; Cantante, M.; Braga, I.; Mauricio, J.; Oing, C.; Honecker, F.; et al. The component of the m(6)A writer complex VIRMA is implicated in aggressive tumor phenotype, DNA damage response and cisplatin resistance in germ cell tumors. J. Exp. Clin. Cancer. Res. 2021, 40, 268. [Google Scholar] [CrossRef] [PubMed]
- Humphries, M.P.; Maxwell, P.; Salto-Tellez, M. QuPath: The global impact of an open source digital pathology system. Comput. Struct. Biotechnol. J. 2021, 19, 852–859. [Google Scholar] [CrossRef] [PubMed]
- Cattoretti, G.; Becker, M.H.; Key, G.; Duchrow, M.; Schluter, C.; Gallet, J.; Gerdes, J. Monoclonal antibodies against recombinant parts of the Ki-67 antigen (MIB 1 and MIB 3) detect proliferating cells in microwave-processed formalin-fixed paraffin sections. J. Pathol. 1992, 168, 357–363. [Google Scholar] [CrossRef]
- Albers, P.; Miller, G.A.; Orazi, A.; Ulbright, T.M.; Albers, J.; Donohue, J.P.; Foster, R.S. lmmunohistochemical Assessment of Tumor Proliferationand Volume of Embryonal Carcinoma Identify Patients with Clinical Stage A Nonseminomatous Testicular Germ Cell Tumor at Low Risk for Occult Metastasis. Cancer 1994, 75, 844–850. [Google Scholar] [CrossRef]
- Kloppel, G.; La Rosa, S. Ki67 labeling index: Assessment and prognostic role in gastroenteropancreatic neuroendocrine neoplasms. Virchows Arch. 2018, 472, 341–349. [Google Scholar] [CrossRef]
- Serna, G.; Simonetti, S.; Fasani, R.; Pagliuca, F.; Guardia, X.; Gallego, P.; Jimenez, J.; Peg, V.; Saura, C.; Eppenberger-Castori, S.; et al. Sequential immunohistochemistry and virtual image reconstruction using a single slide for quantitative KI67 measurement in breast cancer. Breast 2020, 53, 102–110. [Google Scholar] [CrossRef]
- Albers, P.; Orazi, A.; Ulbright, T.M.; Miller, G.A.; Haidar, J.H.; Donohue, J.P.; Foster, R.S. Prognostic Significance of Immunohistochemical Proliferation Markers (Ki67/MIB-1 and Proliferation-Associated Nuclear Antigen), p53 Protein Accumulation, and Neovascularization in Clinical Stage A Nonseminomatous Testicular Germ Cell Tumors. Mod. Pathol. 1995, 8, 492–497. [Google Scholar]
- Miller, I.; Min, M.; Yang, C.; Tian, C.; Gookin, S.; Carter, D.; Spencer, S.L. Ki67 is a Graded Rather than a Binary Marker of Proliferation versus Quiescence. Cell Rep. 2018, 24, 1105–1112 e5. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Jiang, G.; Chen, Q.; Zheng, J. Ki67 is a promising molecular target in the diagnosis of cancer (review). Mol. Med. Rep. 2015, 11, 1566–1572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Riese, W.T.; Albers, P.; Walker, E.B.; Ulbright, T.M.; Crabtree, W.N.; Reister, T.; Fosfer, R.S.; Donohue, J.P. Predictive Parameters of Biologic Behavior of Early Stage Nonseminomatous Testicular Germ Cell Tumors. Cancer 1994, 74, 1335–1341. [Google Scholar] [CrossRef]
- Wang, Y.H.; Lai, C.R.; Lien, H.C.; Hsu, C.Y. Good staining quality ensuring the reproducibility of Ki67 assessment. J. Clin. Pathol. 2020, 73, 413–417. [Google Scholar] [CrossRef] [PubMed]
- Backwell, W. Immunohistochemistry and Immunocytochemistry: Essential Methods, 2nd ed.; Wiley: New York, NY, USA, 2017. [Google Scholar]
- Kim, S.W.; Roh, J.; Park, C.S. Immunohistochemistry for Pathologists: Protocols, Pitfalls, and Tips. J. Pathol. Transl. Med. 2016, 50, 411–418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazumdar, M.; Bacik, J.; Tickoo, S.K.; Dobrzynski, D.; Donadio, A.; Bajorin, D.; Motzer, R.; Reuter, V.; Bosl, G.J. Cluster analysis of p53 and Ki67 expression, apoptosis, alpha-fetoprotein, and human chorionic gonadotrophin indicates a favorable prognostic subgroup within the embryonal carcinoma germ cell tumor. J. Clin. Oncol. 2003, 21, 2679–2688. [Google Scholar] [CrossRef]
- Behling, F.; Schittenhelm, J. Tissue microarrays-translational biomarker research in the fast lane. Expert. Rev. Mol. Diagn. 2018, 18, 833–835. [Google Scholar] [CrossRef] [PubMed]
- Lobo, J.; Jeronimo, C.; Henrique, R. Morphological and molecular heterogeneity in testicular germ cell tumors: Implications for dedicated investigations. Virchows Arch. 2021, 479, 865–866. [Google Scholar] [CrossRef]
- Miyai, K.; Yonekura, Y.; Ito, K.; Matsukuma, S.; Tsuda, H. Gene expression microarray analysis of adult testicular germ cell tumor: A comparison between pure-type seminomas and seminoma components in mixed tumors. Virchows Arch. 2021, 479, 1177–1186. [Google Scholar] [CrossRef]
- Amente, S.; Lania, L.; Majello, B. The histone LSD1 demethylase in stemness and cancer transcription programs. Biochim. Biophys. Acta. 2013, 1829, 981–986. [Google Scholar] [CrossRef] [Green Version]
- Yang, G.J.; Lei, P.M.; Wong, S.Y.; Ma, D.L.; Leung, C.H. Pharmacological Inhibition of LSD1 for Cancer Treatment. Molecules 2018, 23, 3194. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Lu, F.; Ren, Q.; Sun, H.; Xu, Z.; Lan, R.; Liu, Y.; Ward, D.; Quan, J.; Ye, T.; et al. Novel histone demethylase LSD1 inhibitors selectively target cancer cells with pluripotent stem cell properties. Cancer Res. 2011, 71, 7238–7249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vega, A.; Baptissart, M.; Caira, F.; Brugnon, F.; Lobaccaro, J.M.; Volle, D.H. Epigenetic: A molecular link between testicular cancer and environmental exposures. Front. Endocrinol. 2012, 3, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Patient Cohort (n = 157) Tumor Samples (n = 221) |
|---|---|
| Age (years) (median, IQR) | 31 (25–36) |
| Laterality (n, %) | |
| Right | 83/153 (54.2) |
| Left | 68/153 (44.5) |
| Bilateral synchronous | 2/153 (1.3) |
| Pre-operative AFP (n, %) | |
| Within normal range | 97/151 (64.2) |
| Elevated | 54/151 (35.8) |
| Pre-operative β-HCG (n, %) | |
| Within normal range | 73/151 (48.3) |
| Elevated | 78/151 (51.7) |
| Pre-operative LDH (n, %) | |
| Within normal range | 71/124 (57.3) |
| Elevated | 53/124 (42.7) |
| Histologic subtypes (n, %) | |
| Pure SE | 82/157 (52.2) |
| Pure EC | 11/157 (7.0) |
| Pure TE | 3/157 (1.9) |
| Mixed Tumor | 61/157 (38.9) |
| Tumor components (n, %) | |
| SE | 96/221 (43.5) |
| EC | 56/221 (25.3) |
| CH | 10/221 (4.5) |
| YST | 27/221 (12.2) |
| TE | 32/221 (14.5) |
| Stage AJCC8 (n, %) | |
| I | 100/156 (64.1) |
| II | 32/156 (20.5) |
| III | 24/156 (15.4) |
| Vascular Invasion (n, %) | |
| Yes | 78/157 (49.7) |
| No | 79/157 (50.3) |
| Tumor largest dimension (cm) (median, range) | 4.7 (0.7–18) |
| Metastatic disease at diagnosis (n, %) | |
| Yes | 56/156 (35.9) |
| No | 100/156 (64.1) |
| IGCCCG prognosis group (with metastatic disease) (n, %) | |
| Good | 42/56 (75) |
| Intermediate | 8/56 (14.3) |
| Poor | 6/56 (10.7) |
| Relapse/Progression (n, %) | |
| Yes | 10/157 (6.4) |
| No | 147/157 (93.6) |
| Additional treatments (n) | |
| RT | 46 |
| CT | 99 |
| Vital status (n, %) | |
| Alive with no disease | 151/157 (96.2) |
| AWD | 3/157 (1.9) |
| DFD | 2/157 (1.3) |
| D-NED | 1/157 (0.6) |
| Stage | I | II | III | p-Value | |
|---|---|---|---|---|---|
| Ki67 | |||||
| Positivity (%) (median (IQR)) | 15.4 (4.7–32.2) | 10.8 (3.4–24.0) | 21.7 (4.3–30.1) | 0.593 | |
| Only SE | 13.9 (3.87–25.4) | 6.6 (3.19–17.6) | 11.1 (5.17–31.2) | 0.791 | |
| Only NS | 22.8 (5.9–58.5) | 14.1 (3.4–32.0) | 22.1 (3.6–30.5) | 0.278 | |
| H-score (median (IQR)) | 17.6 (5.0–42.1) | 11.2 (3.9–26.6) | 24.6 (5.1–35.9) | 0.490 | |
| Only SE | 14.5 (4.2–31.5) | 6.8 (3.5–19.9) | 12.3 (6.4–31.9) | 0.715 | |
| Only NS | 25.5 (6.3–76.2) | 14.2 (4.4–35.8) | 24.8 (4.4–38.6) | 0.274 | |
| LSD1 | |||||
| Positivity (%) (median (IQR)) | 8.2 (2.8–17.2) | 9.4 (2.3–13.7) | 10.6 (3.2–15.6) | 0.894 | |
| Only SE | 7.8 (2.6–15.8) | 9.8 (2.5–15.7) | 13.4 (3.1–16.2) | 0.953 | |
| Only NS | 9.8 (3.7–21.6) | 9.0 (1.6–13.7) | 9.2 (3.2–15.1) | 0.692 | |
| H-score (median (IQR)) | 8.2 (3.1–17.3) | 9.4 (2.1–13.9) | 10.6 (3.2–15.6) | 0.879 | |
| Only SE | 7.9 (2.6–15.8) | 9.8 (2.5–15.7) | 13.4 (3.1–16.2) | 0.960 | |
| Only NS | 9.8 (4.3–22.2) | 9.1 (1.6–14.0) | 9.3 (3.2–15.3) | 0.644 | |
| IGCCCG | Good | Intermediate | Poor | p-value | |
| Ki67 | |||||
| Positivity (%) (median (IQR)) | 10.4 (3.2–26.1) | 20.7 (4.9–41.5) | 23.9 (17.6–28.4) | 0.207 | |
| H-score (median (IQR)) | 11.9 (3.7–27.7) | 23.3 (5.0–75.1) | 29.3 (20.1–35.8) | 0.179 | |
| LSD1 | |||||
| Positivity (%) (median (IQR)) | 10.6 (1.6–15.6) | 5.8 (4.2–40.9) | 6.7 (3.3–13.5) | 0.977 | |
| H-score (median (IQR)) | 10.7 (1.6–15.6) | 5.8 (4.2–41.9) | 6.7 (3.4–13.7) | 0.979 | |
| Vascular Invasion | No Vascular Invasion | p-value | |||
| Ki67 | |||||
| Positivity (%) (median (IQR)) | 17.6 (3.6–33.4) | 13.9 (4.6–29.3) | 0.364 | ||
| H-score (median (IQR)) | 18.6 (4.3–41.7) | 15.4 (4.9–36.3) | 0.470 | ||
| LSD1 | |||||
| Positivity (%) (median (IQR)) | 9.0 (2.4–16.1) | 9.4 (3.3–15.1) | 0.738 | ||
| H-score (median (IQR)) | 9.1 (2.4–16.2) | 9.4 (3.6–16.5) | 0.684 | ||
| SE vs. NS | ||||
|---|---|---|---|---|
| SE | NS | p-Value | ||
| Ki67 mRNA expression (median (IQR)) | 888 (635–1088) | 758 (505–1122) | 0.262 | |
| LSD1 mRNA expression (median (IQR)) | 4012 (3220–4426) | 3903 (2735–5650) | 0.311 | |
| Stage | ||||
| I | II | III | p-value | |
| Ki67 mRNA expression (median (IQR)) | 806 (635–1115) | 592 (424–1054) | 856 (424–1133) | 0.216 |
| LSD1 mRNA expression (median (IQR)) | 3956 (3214–5018) | 4216 (2636–5340) | 4762 (3208–5841) | 0.437 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lourenço, B.C.; Guimarães-Teixeira, C.; Flores, B.C.T.; Miranda-Gonçalves, V.; Guimarães, R.; Cantante, M.; Lopes, P.; Braga, I.; Maurício, J.; Jerónimo, C.; et al. Ki67 and LSD1 Expression in Testicular Germ Cell Tumors Is Not Associated with Patient Outcome: Investigation Using a Digital Pathology Algorithm. Life 2022, 12, 264. https://doi.org/10.3390/life12020264
Lourenço BC, Guimarães-Teixeira C, Flores BCT, Miranda-Gonçalves V, Guimarães R, Cantante M, Lopes P, Braga I, Maurício J, Jerónimo C, et al. Ki67 and LSD1 Expression in Testicular Germ Cell Tumors Is Not Associated with Patient Outcome: Investigation Using a Digital Pathology Algorithm. Life. 2022; 12(2):264. https://doi.org/10.3390/life12020264
Chicago/Turabian StyleLourenço, Beatriz Chaves, Catarina Guimarães-Teixeira, Bianca C. T. Flores, Vera Miranda-Gonçalves, Rita Guimarães, Mariana Cantante, Paula Lopes, Isaac Braga, Joaquina Maurício, Carmen Jerónimo, and et al. 2022. "Ki67 and LSD1 Expression in Testicular Germ Cell Tumors Is Not Associated with Patient Outcome: Investigation Using a Digital Pathology Algorithm" Life 12, no. 2: 264. https://doi.org/10.3390/life12020264
APA StyleLourenço, B. C., Guimarães-Teixeira, C., Flores, B. C. T., Miranda-Gonçalves, V., Guimarães, R., Cantante, M., Lopes, P., Braga, I., Maurício, J., Jerónimo, C., Henrique, R., & Lobo, J. (2022). Ki67 and LSD1 Expression in Testicular Germ Cell Tumors Is Not Associated with Patient Outcome: Investigation Using a Digital Pathology Algorithm. Life, 12(2), 264. https://doi.org/10.3390/life12020264