
Transforaminal Lumbar Interbody Fusion (TLIF) versus Oblique Lumbar Interbody Fusion (OLIF) in Interbody Fusion Technique for Degenerative Spondylolisthesis: A Systematic Review and Meta-Analysis



Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analyses
3. Results
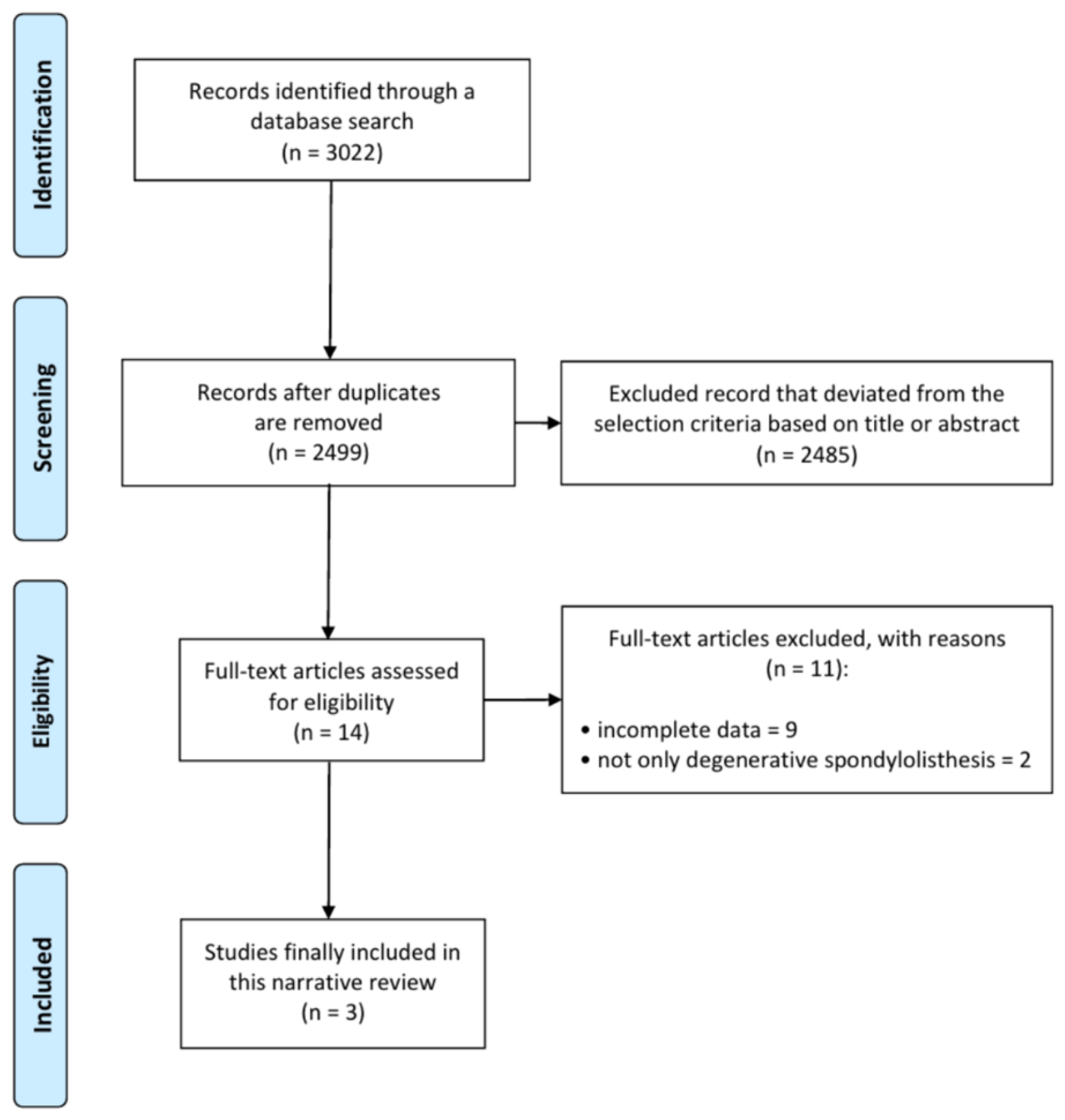
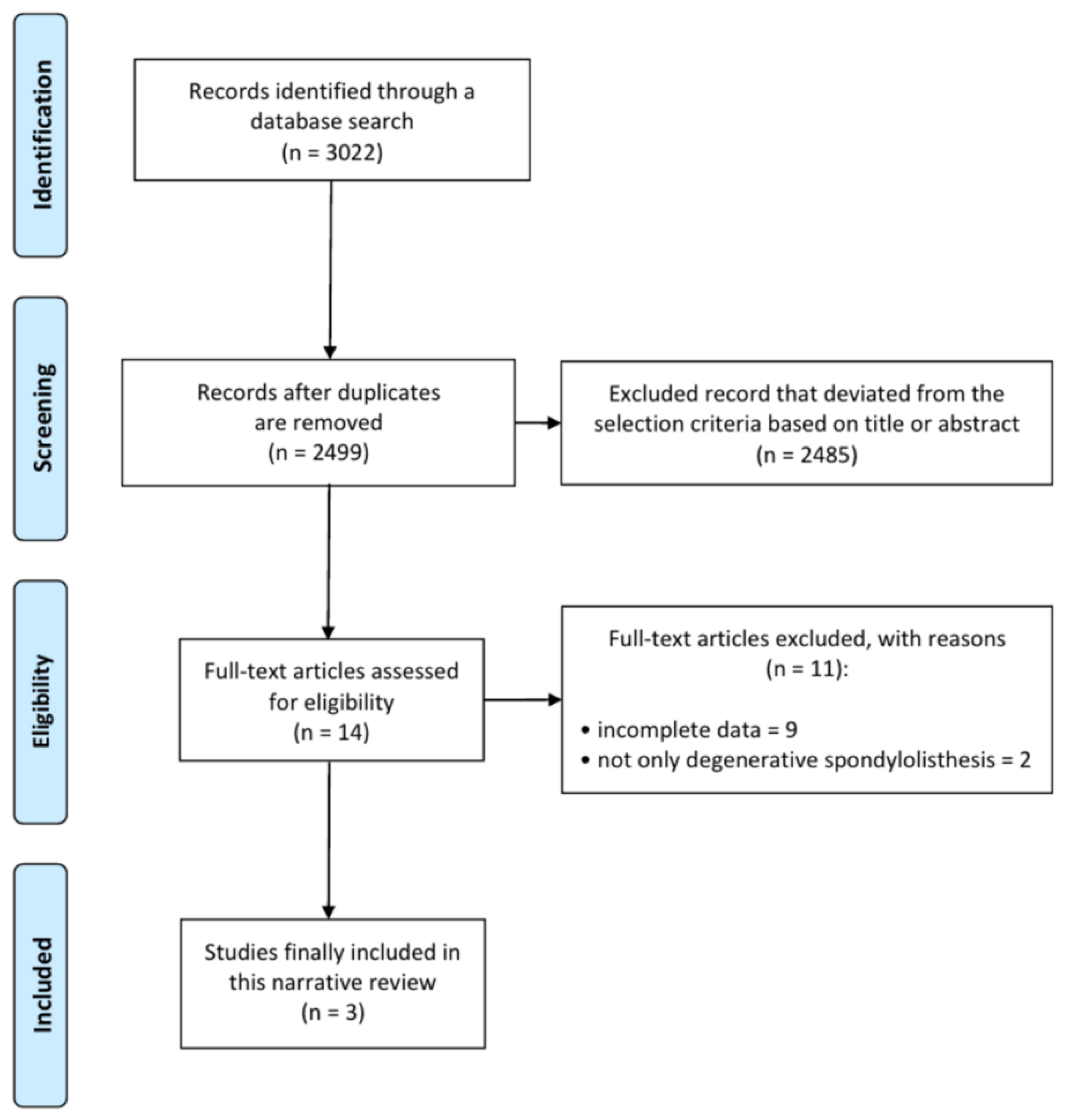
3.1. Study Selection
3.2. Study Characteristics
3.3. Risk of Bias
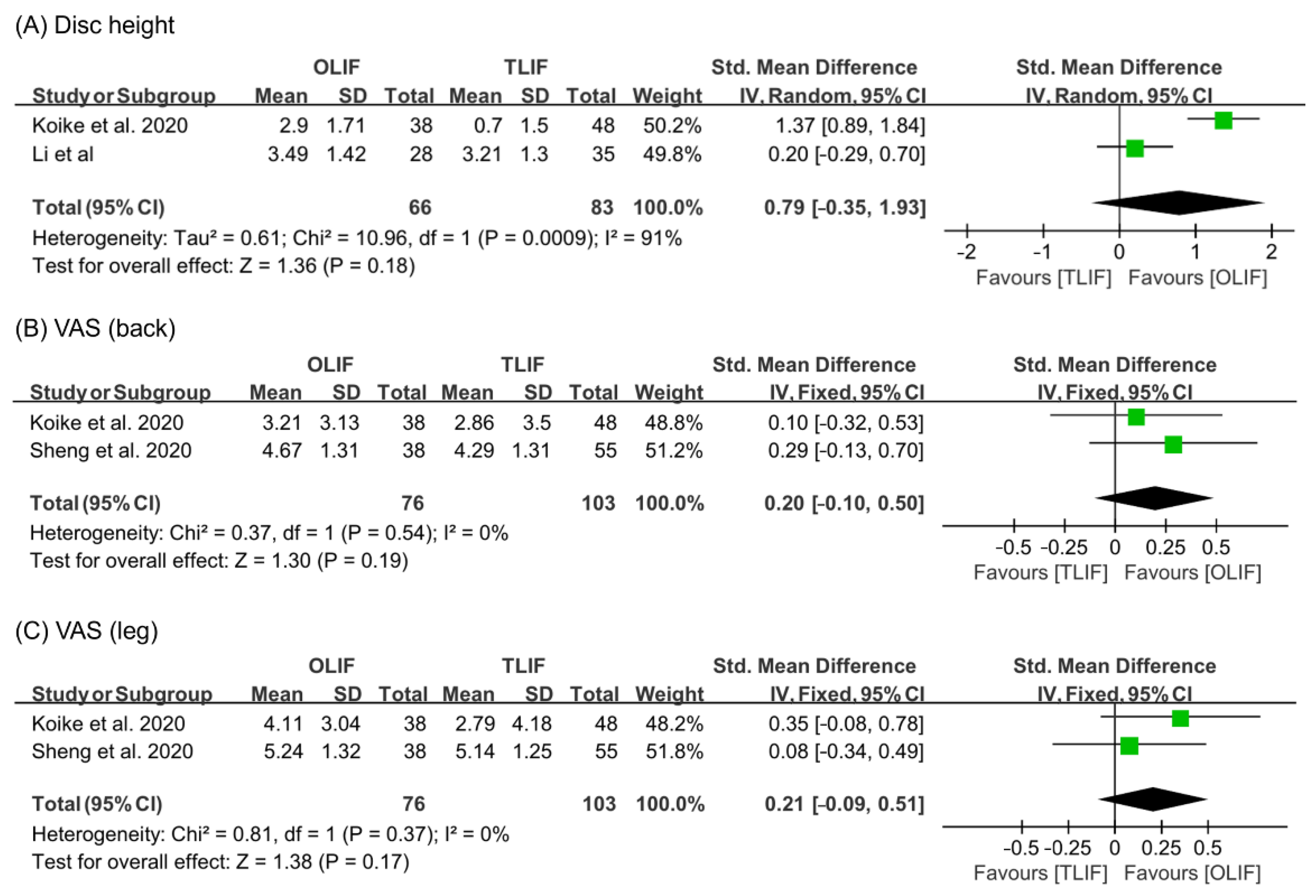
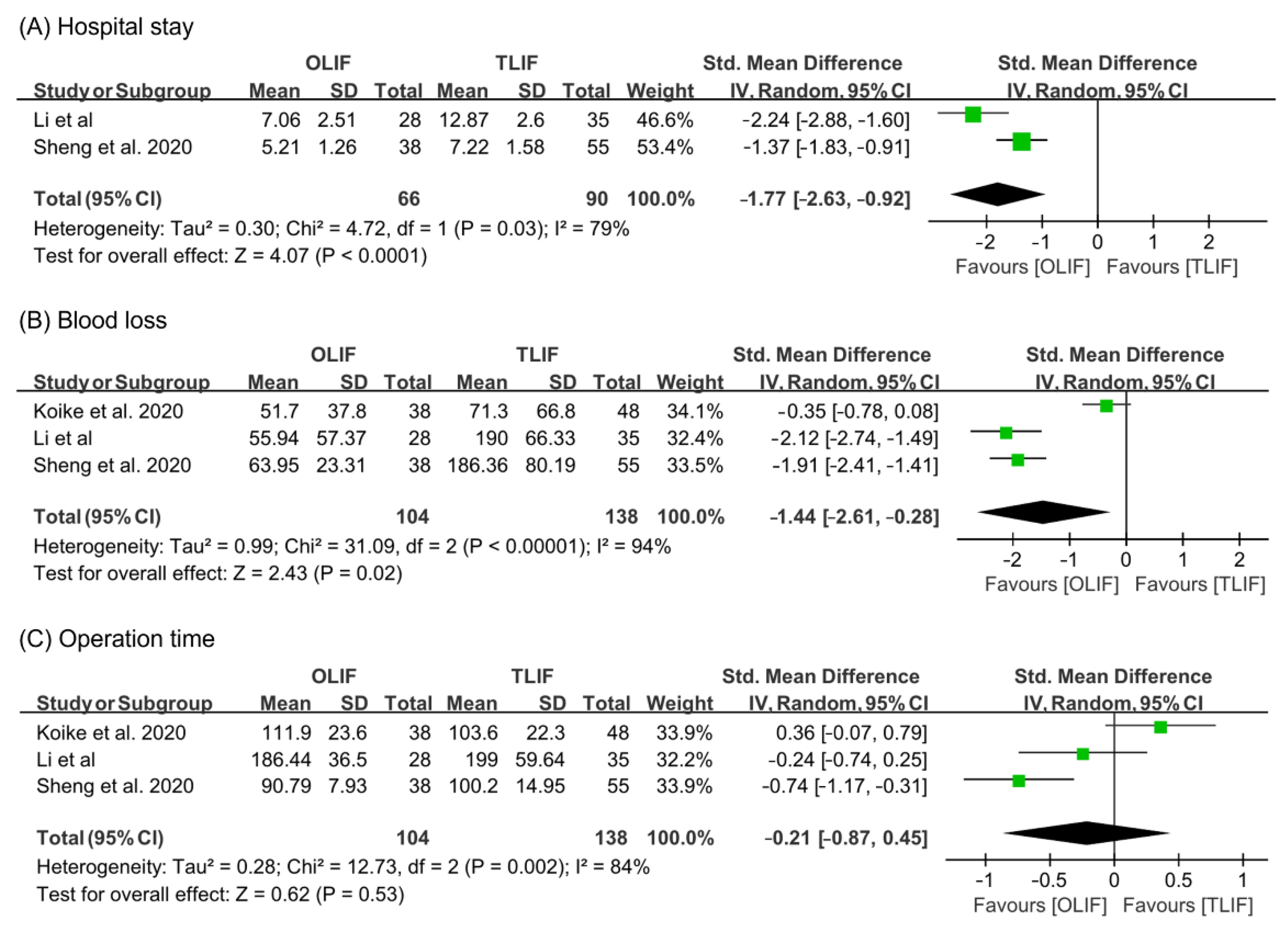
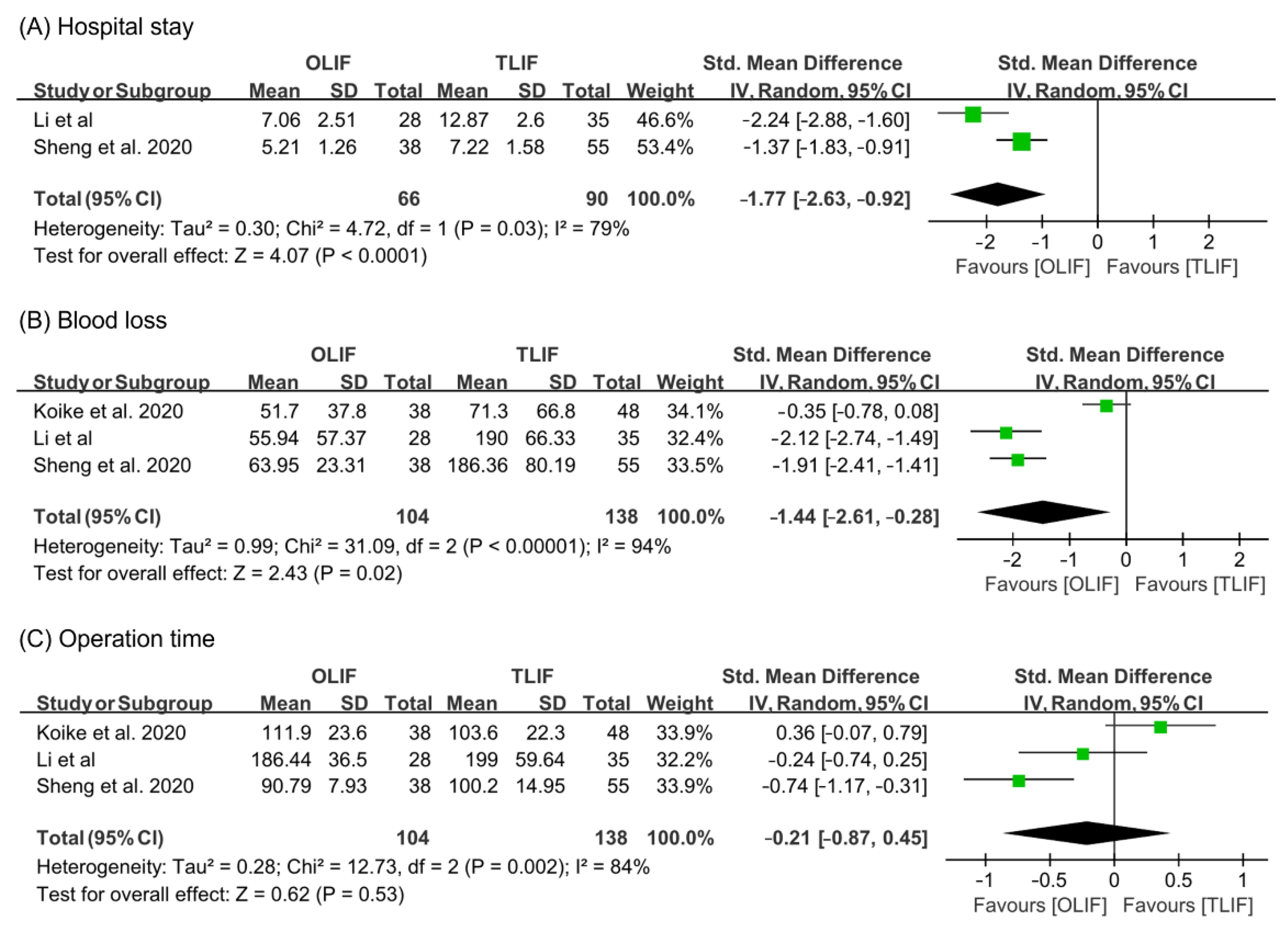
3.4. Meta-Analysis Results
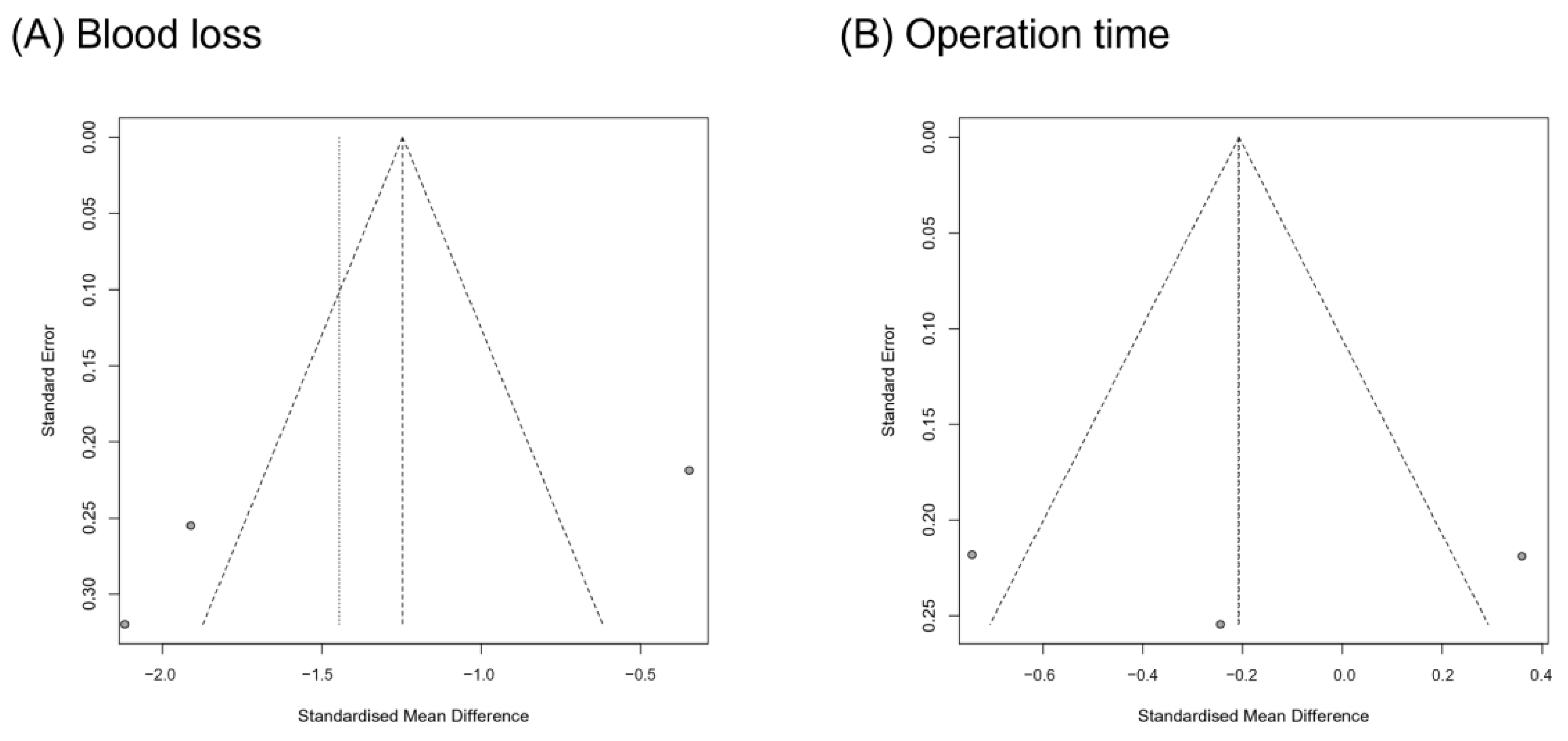
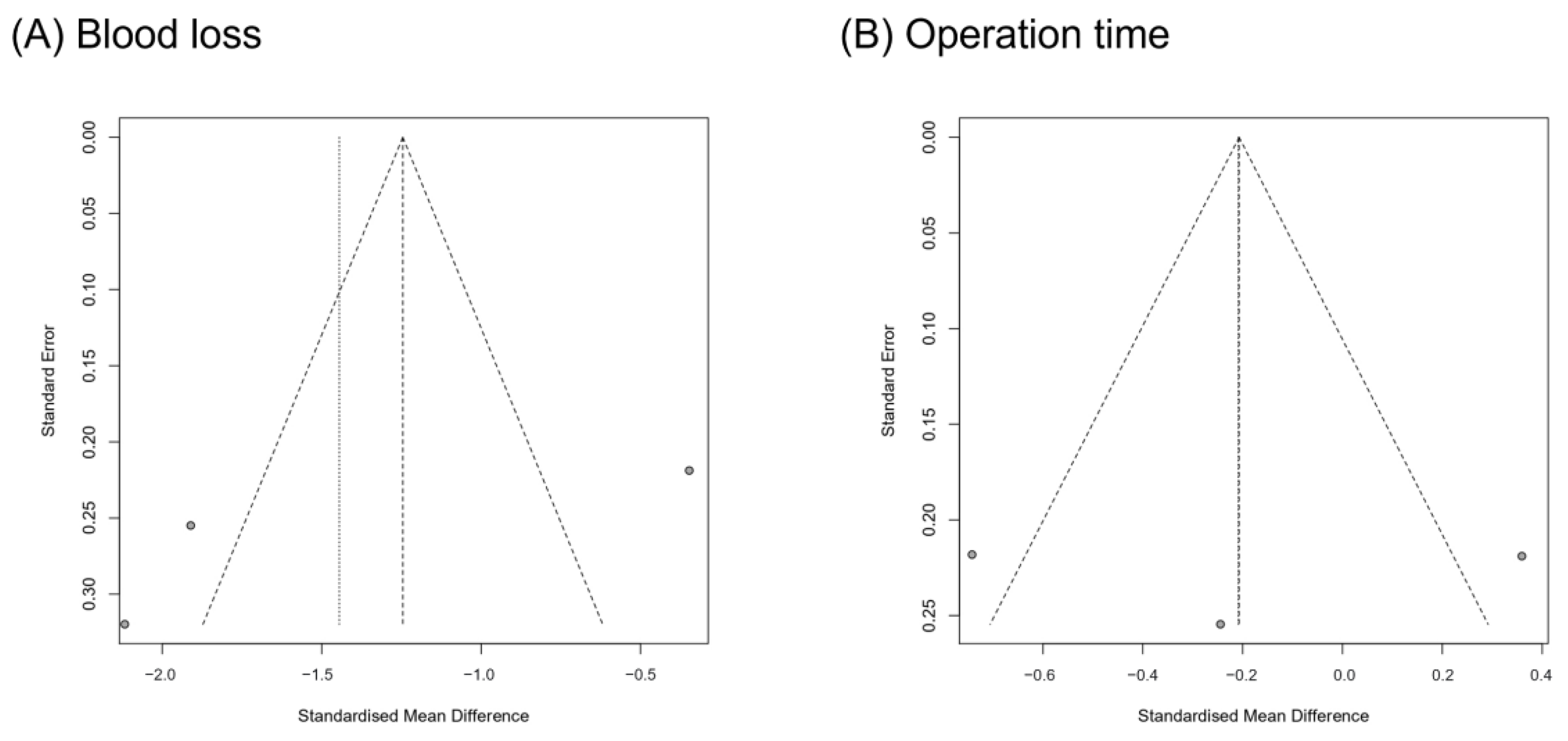
3.5. Publication Bias
4. Discussion
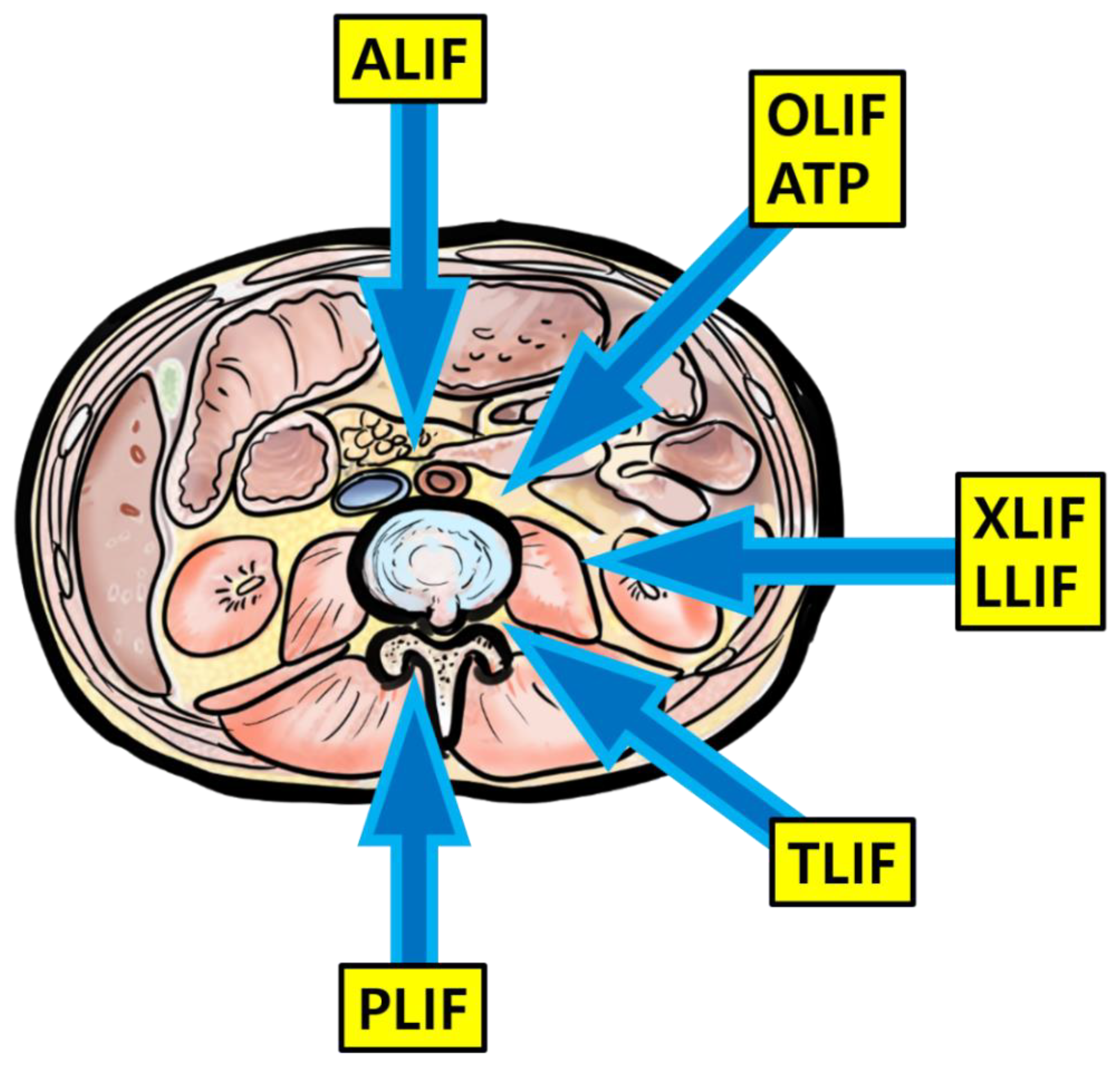
4.1. Summary of Lumbar Interbody Fusion Techniques
4.2. Study Summary and Highlights
4.3. Study Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, G.W.; Son, J.-H.; Ahn, M.-W.; Kim, H.-J.; Yeom, J.S. The comparison of pedicle screw and cortical screw in posterior lumbar interbody fusion: A prospective randomized noninferiority trial. Spine J. 2015, 15, 1519–1526. [Google Scholar] [CrossRef]
- Allain, J.; Dufour, T. Anterior lumbar fusion techniques: ALIF, OLIF, DLIF, LLIF, IXLIF. Orthop. Traumatol. Surg. Res. 2020, 106, S149–S157. [Google Scholar] [CrossRef]
- Lee, N.; Kim, K.N.; Yi, S.; Ha, Y.; Shin, D.A.; Yoon, D.H.; Kim, K.S. Comparison of Outcomes of Anterior, Posterior, and Transforaminal Lumbar Interbody Fusion Surgery at a Single Lumbar Level with Degenerative Spinal Disease. World Neurosurg. 2017, 101, 216–226. [Google Scholar] [CrossRef]
- Li, R.; Li, X.; Zhou, H.; Jiang, W. Development and Application of Oblique Lumbar Interbody Fusion. Orthop. Surg. 2020, 12, 355–365. [Google Scholar] [CrossRef] [Green Version]
- Xu, D.S.; Walker, C.T.; Godzik, J.; Turner, J.D.; Smith, W.; Uribe, J.S. Minimally invasive anterior, lateral, and oblique lumbar interbody fusion: A literature review. Ann. Transl. Med. 2018, 6, 104. [Google Scholar] [CrossRef]
- Upadhyayula, P.S.; Curtis, E.I.; Yue, J.K.; Sidhu, N.; Ciacci, J.D. Anterior Versus Transforaminal Lumbar Interbody Fusion: Perioperative Risk Factors and 30-Day Outcomes. Int. J. Spine Surg. 2018, 12, 533–542. [Google Scholar] [CrossRef] [PubMed]
- Koike, Y.; Kotani, Y.; Terao, H.; Iwasaki, N. Comparison of Outcomes of Oblique Lateral Interbody Fusion with Percutaneous Posterior Fixation in Lateral Position and Minimally Invasive Transforaminal Lumbar Interbody Fusion for Degenerative Spondylolisthesis. Asian Spine J. 2021, 15, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Ko, M.J.; Park, S.W.; Kim, Y.B. Correction of Spondylolisthesis by Lateral Lumbar Interbody Fusion Compared with Transforaminal Lumbar Interbody Fusion at L4–5. J. Korean Neurosurg. Soc. 2019, 62, 422–431. [Google Scholar] [CrossRef] [Green Version]
- Álvaro, D.; Lewandrowski, K.-U. Endoscopic Transforaminal Lumbar Interbody Fusion with a Single Oblique PEEK Cage and Posterior Supplemental Fixation. Int. J. Spine Surg. 2020, 14, S45–S55. [Google Scholar] [CrossRef]
- Kolcun, J.P.G.; Brusko, G.D.; Wang, M.Y. Endoscopic transforaminal lumbar interbody fusion without general anesthesia: Technical innovations and outcomes. Ann. Transl. Med. 2019, 7, S167. [Google Scholar] [CrossRef]
- Hah, R.; Kang, H.P. Lateral and Oblique Lumbar Interbody Fusion—Current Concepts and a Review of Recent Literature. Curr. Rev. Musculoskelet. Med. 2019, 12, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Meng, B.; Bunch, J.; Burton, D.; Wang, J. Lumbar interbody fusion: Recent advances in surgical techniques and bone healing strategies. Eur. Spine J. 2021, 30, 22–33. [Google Scholar] [CrossRef]
- Mobbs, R.J.; Phan, K.; Malham, G.; Seex, K.; Rao, P.J. Lumbar interbody fusion: Techniques, indications and comparison of interbody fusion options including PLIF, TLIF, MI-TLIF, OLIF/ATP, LLIF and ALIF. J. Spine Surg. 2015, 1, 2–18. [Google Scholar] [CrossRef]
- Spiker, W.R.; Goz, V.; Brodke, D.S. Lumbar Interbody Fusions for Degenerative Spondylolisthesis: Review of Techniques, Indications, and Outcomes. Glob. Spine J. 2019, 9, 77–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karikari, I.O.; Isaacs, R.E. Minimally Invasive Transforaminal Lumbar Interbody Fusion. Spine 2010, 35, S294–S301. [Google Scholar] [CrossRef]
- Wong, A.P.; Smith, Z.A.; Stadler, J.A.; Hu, X.Y.; Yan, J.Z.; Li, X.F.; Lee, J.H.; Khoo, L.T. Minimally Invasive Transforaminal Lumbar Interbody Fusion (MI-TLIF). Neurosurg. Clin. N. Am. 2014, 25, 279–304. [Google Scholar] [CrossRef]
- Badlani, N.; Yu, E.; Kreitz, T.; Khan, S.; Kurd, M.F. Minimally Invasive Transforaminal Lumbar Interbody Fusion (TLIF). Clin. Spine Surg. 2020, 33, 62–64. [Google Scholar] [CrossRef]
- Miller, L.E.; Bhattacharyya, S.; Pracyk, J. Minimally Invasive Versus Open Transforaminal Lumbar Interbody Fusion for Single-Level Degenerative Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. World Neurosurg. 2020, 133, 358–365. [Google Scholar] [CrossRef]
- Hammad, A.; Wirries, A.; Ardeshiri, A.; Nikiforov, O.; Geiger, F. Open versus minimally invasive TLIF: Literature review and meta-analysis. J. Orthop. Surg. Res. 2019, 14, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, B.M.; Hilibrand, A.S.; Savas, P.E.; Pellegrino, A.; Vaccaro, A.R.; Siegler, S.; Albert, T.J. Transforaminal Lumbar Interbody Fusion. Spine 2004, 29, E65–E70. [Google Scholar] [CrossRef] [PubMed]
- De Kunder, S.L.; van Kuijk, S.M.J.; Rijkers, K.; Caelers, I.J.M.H.; van Hemert, W.L.W.; de Bie, R.A. Transforaminal lumbar interbody fusion (TLIF) versus posterior lumbar interbody fusion (PLIF) in lumbar spondylolisthesis: A systematic review and meta-analysis. Spine J. 2017, 17, 1712–1721. [Google Scholar] [CrossRef]
- Rickert, M.; Fleege, C.; Tarhan, T.; Schreiner, S.; Makowski, M.R.; Rauschmann, M. Transforaminal lumbar interbody fusion using polyetheretherketone oblique cages with and without a titanium coating: A randomized clinical pilot study. Bone Joint J. 2017, 99-B, 1366–1372. [Google Scholar] [CrossRef]
- Sleem, A.; Marzouk, A. Transforaminal Lumbar Interbody Fusion with Local Bone Graft Alone for Single-Level Isthmic Spondylolisthesis. Int. J. Spine Surg. 2018, 12, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, W.S.; Mummaneni, P.V. Transforaminal Lumbar Interbody Fusion: Technique, Complications, and Early Results. Neurosurgery 2001, 48, 569–575. [Google Scholar] [CrossRef]
- Nakashima, H.; Kanemura, T.; Satake, K.; Ishikawa, Y.; Ouchida, J.; Segi, N.; Yamaguchi, H.; Imagama, S. Comparative Radiographic Outcomes of Lateral and Posterior Lumbar Interbody Fusion in the Treatment of Degenerative Lumbar Kyphosis. Asian Spine J. 2019, 13, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Yang, Z.; Chang, J.; Sun, L.; Chen, C.-M.; Feng, H. Comparing Oblique Lumbar Interbody Fusion with Lateral Screw Fixation and Transforaminal Full-Endoscopic Lumbar Discectomy (OLIF-TELD) and Posterior Lumbar Interbody Fusion (PLIF) for the Treatment of Adjacent Segment Disease. BioMed Res. Int. 2020, 2020, 4610128. [Google Scholar] [CrossRef]
- Lu, T.; Lu, Y. Comparison of Biomechanical Performance among Posterolateral Fusion and Transforaminal, Extreme, and Oblique Lumbar Interbody Fusion: A Finite Element Analysis. World Neurosurg. 2019, 129, e890–e899. [Google Scholar] [CrossRef]
- Park, S.W.; Ko, M.J.; Kim, Y.B.; Le Huec, J.C. Correction of marked sagittal deformity with circumferential minimally invasive surgery using oblique lateral interbody fusion in adult spinal deformity. J. Orthop. Surg. Res. 2020, 15, 13. [Google Scholar] [CrossRef] [PubMed]
- Verma, R.; Virk, S.; Qureshi, S. Interbody Fusions in the Lumbar Spine: A Review. HSS J. 2020, 16, 162–167. [Google Scholar] [CrossRef]
- Kim, S.G.; Kim, J.T.; Shin, M.H.; Choi, D.Y. Lumbopelvic Sagittal Alignment and Foraminal Height from Single Interbody Cage in L5-S1 Segment: Comparison between straight type versus curvilinear type cage. Eur. Spine J. 2015, 24, 2588–2596. [Google Scholar] [CrossRef] [PubMed]
- Sheng, S.R.; Geng, Y.B.; Zhou, K.L.; Wu, A.M.; Ni, W.F. Minimally invasive surgery for degenerative spondylolisthesis: Transforaminal or oblique lumbar interbody fusion. J. Comp. Eff. Res. 2020, 9, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Li, J.X.J.; Phan, K.; Mobbs, R. Oblique Lumbar Interbody Fusion: Technical Aspects, Operative Outcomes, and Complications. World Neurosurg. 2017, 98, 113–123. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Shao, X.; Li, X.; Liu, Y.; Jiang, W. Comparison of clinical outcomes and spino-pelvic sagittal balance in degenerative lumbar spondylolisthesis: Minimally invasive oblique lumbar interbody fusion (OLIF) versus transforaminal lumbar interbody fusion (TLIF). Medicine 2021, 100, e23783. [Google Scholar] [CrossRef]
- Chen, Y.L.; Zhu, Z.H.; Wang, Y.K.; Fan, S.W.; Fang, X.Q.; Wan, S.L.; Zhang, J.F.; Zhao, X.; Zhao, F.D. Effects of oblique lateral interbody fusion and transforaminal lumbar interbody fusion for lordosis correction in degenerative lumbar diseases. Zhonghua Yi Xue Za Zhi 2018, 98, 1990–1995. [Google Scholar] [PubMed]
- Li, A.; Li, X.; Zhong, Y. Is minimally invasive superior than open transforaminal lumbar interbody fusion for single-level degenerative lumbar diseases: A meta-analysis. J. Orthop. Surg. Res. 2018, 13, 241. [Google Scholar] [CrossRef]
- Lin, G.-X.; Akbary, K.; Kotheeranurak, V.; Quillo-Olvera, J.; Jo, H.-J.; Yang, X.-W.; Mahatthanatrakul, A.; Kim, J.-S. Clinical and Radiologic Outcomes of Direct Versus Indirect Decompression with Lumbar Interbody Fusion: A Matched-Pair Comparison Analysis. World Neurosurg. 2018, 119, e898–e909. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Kotani, Y.; Ikeura, A.; Tokunaga, H.; Saito, T. Single-level controlled comparison of OLIF51 and percutaneous screw in lateral position versus MIS-TLIF for lumbosacral degenerative disorders: Clinical and radiologic study. J. Orthop. Sci. 2020. [Google Scholar] [CrossRef]
- Wang, B.; Hua, W.; Ke, W.; Lu, S.; Li, X.; Zeng, X.; Yang, C. Biomechanical Evaluation of Transforaminal Lumbar Interbody Fusion and Oblique Lumbar Interbody Fusion on the Adjacent Segment: A Finite Element Analysis. World Neurosurg. 2019, 126, e819–e824. [Google Scholar] [CrossRef] [PubMed]
- Pawar, A.Y.; Hughes, A.P.; Sama, A.A.; Girardi, F.P.; Lebl, D.R.; Cammisa, F.P. A Comparative Study of Lateral Lumbar Interbody Fusion and Posterior Lumbar Interbody Fusion in Degenerative Lumbar Spondylolisthesis. Asian Spine J. 2015, 9, 668–674. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.J.; Lee, J.W.; Kim, S.M.; Park, K.Y.; Chang, S.H.; Song, D.G. Precautions for combined anterior and posterior long-level fusion for adult spinal deformity: Preoperative surgical complications related to the anterior procedure (Oblique lumbar interbody fusion). Asian Spine J. 2019, 13, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Mun, H.Y.; Ko, M.J.; Kim, Y.B.; Park, S.W. Usefulness of Oblique Lateral Interbody Fusion at L5–S1 Level Compared to Transforaminal Lumbar Interbody Fusion. J. Korean Neurosurg. Soc. 2020, 63, 723–729. [Google Scholar] [CrossRef]
- Lee, G.W.; Shin, J.-H. Comparative Study of Two Surgical Techniques for Proximal Adjacent Segment Pathology after Posterior Lumbar Interbody Fusion with Pedicle Screws: Fusion Extension using Conventional Pedicle Screw vs Cortical Bone Trajectory-Pedicle Screw (Cortical Screw). World Neurosurg. 2018, 117, e154–e161. [Google Scholar] [CrossRef] [PubMed]
- Phan, K.; Maharaj, M.; Assem, Y.; Mobbs, R.J. Review of early clinical results and complications associated with oblique lumbar interbody fusion (OLIF). J. Clin. Neurosci. 2016, 31, 23–29. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Study | Design | Subjects (n, Age, M:F) | Follow-Up (Months) | Outcome Assessment | Complications |
|---|---|---|---|---|---|---|
| 1 | Koike et al. (2020) [7] | Retrospective | OLIF: 38, 72.1 ± 11.4 y, 20:18 TLIF: 48, 70.1 ± 11.5 y, 18:30 | OLIF: 18.1 ± 8.5 TLIF: 22.5 ± 12.8 | Estimated blood loss; operation time; postoperative C-reactive protein level; lower back pain, lumbar function, walking ability, social life, mental health (Japanese Orthopedic Association Back Pain Evaluation Questionnaire); lower back pain, leg pain, leg numbness (VAS); disc height, slipping length (radiographs); degree of stenosis (MRI) | OLIF: 1 superficial injection TLIF: 1 superficial injection |
| 2 | Li et al. (2021) [33] | Retrospective | OLIF: 28, 57.5 ± 10.4 y, 7:21 TLIF: 35, 59.3 ± 9.86 y, 8:27 | OLIF: >12 TLIF: >12 | Length of postoperative hospital stay; estimated blood loss; operation time; length of bed rest (pain (VAS, ODI); disc height, foraminal height, lumbar lordotic angle, pelvic tilt, pelvic incidence, sacral slope (radiographs); complications) * | OLIF: 1 ileus, 1 numbness TLIF: 3 cerebrospinal fluid leakage and root injury |
| 3 | Sheng et al. (2020) [31] | Retrospective | OLIF: 38, 65.3 ± 8.9 y, 9:29 TLIF: 55, 60.6 ± 12.4 y, 25:30 | OLIF: >6 TLIF: >6 | Length of postoperative hospital stay; estimated blood loss; operation time; activity levels (questionnaires); pain (VAS, ODI); satisfaction; motor and sensory function (modified American Spinal Injury Association scale); restoration, alignment and indirect decompression (radiographs and MRI); complications | OLIF: 1 hip flexion weakness, 1 sensory deficit (neural) TLIF: 2 hip flexion weakness, 1 distal motor weakness, 2 sensory deficit (neural) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, M.C.; Kim, G.-U.; Choo, Y.J.; Lee, G.W. Transforaminal Lumbar Interbody Fusion (TLIF) versus Oblique Lumbar Interbody Fusion (OLIF) in Interbody Fusion Technique for Degenerative Spondylolisthesis: A Systematic Review and Meta-Analysis. Life 2021, 11, 696. https://doi.org/10.3390/life11070696
Chang MC, Kim G-U, Choo YJ, Lee GW. Transforaminal Lumbar Interbody Fusion (TLIF) versus Oblique Lumbar Interbody Fusion (OLIF) in Interbody Fusion Technique for Degenerative Spondylolisthesis: A Systematic Review and Meta-Analysis. Life. 2021; 11(7):696. https://doi.org/10.3390/life11070696
Chicago/Turabian StyleChang, Min Cheol, Gang-Un Kim, Yoo Jin Choo, and Gun Woo Lee. 2021. "Transforaminal Lumbar Interbody Fusion (TLIF) versus Oblique Lumbar Interbody Fusion (OLIF) in Interbody Fusion Technique for Degenerative Spondylolisthesis: A Systematic Review and Meta-Analysis" Life 11, no. 7: 696. https://doi.org/10.3390/life11070696
APA StyleChang, M. C., Kim, G.-U., Choo, Y. J., & Lee, G. W. (2021). Transforaminal Lumbar Interbody Fusion (TLIF) versus Oblique Lumbar Interbody Fusion (OLIF) in Interbody Fusion Technique for Degenerative Spondylolisthesis: A Systematic Review and Meta-Analysis. Life, 11(7), 696. https://doi.org/10.3390/life11070696