
Liquid Biopsy and Potential Liquid Biopsy-Based Biomarkers in Philadelphia-Negative Classical Myeloproliferative Neoplasms: A Systematic Review

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
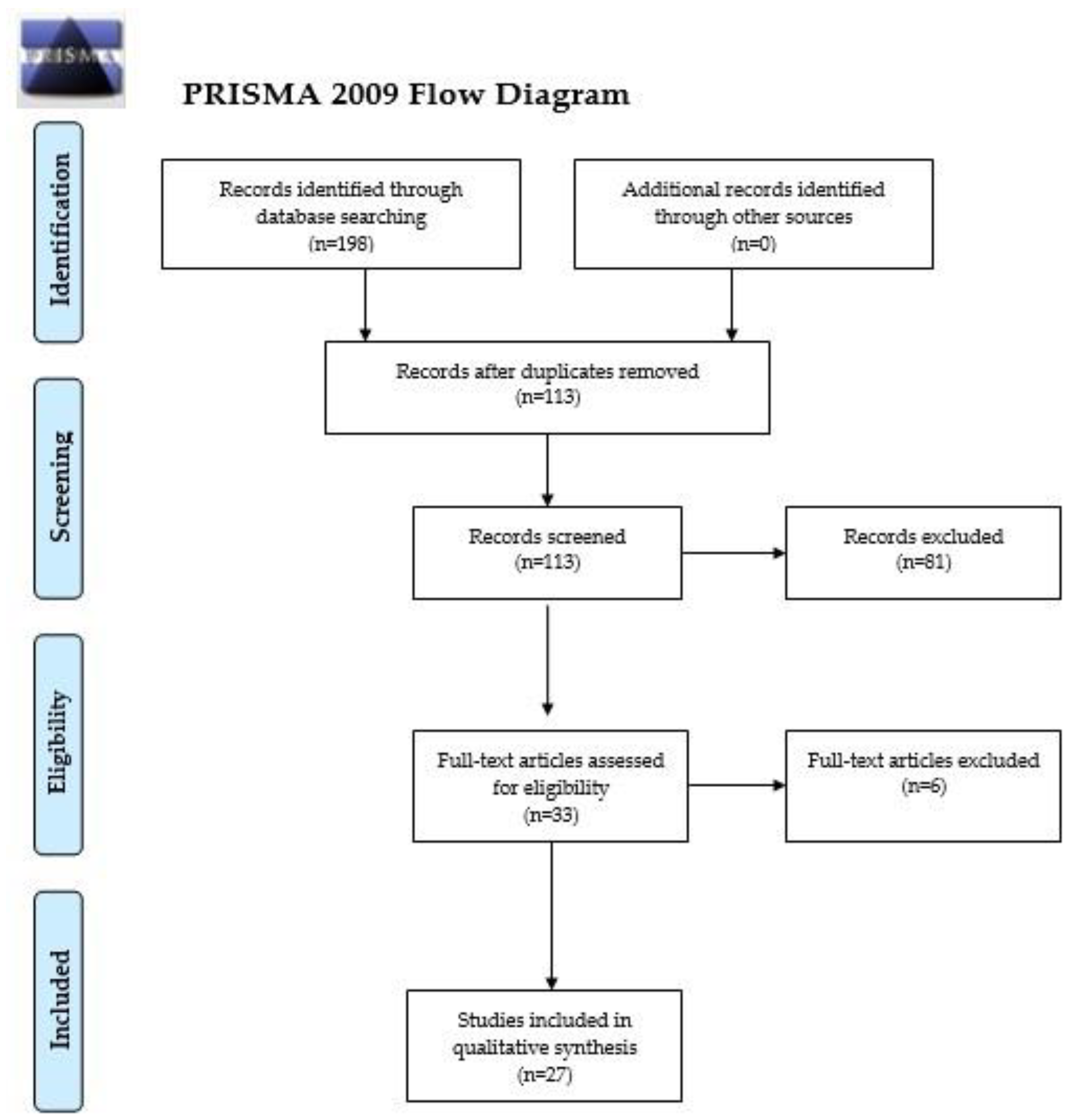
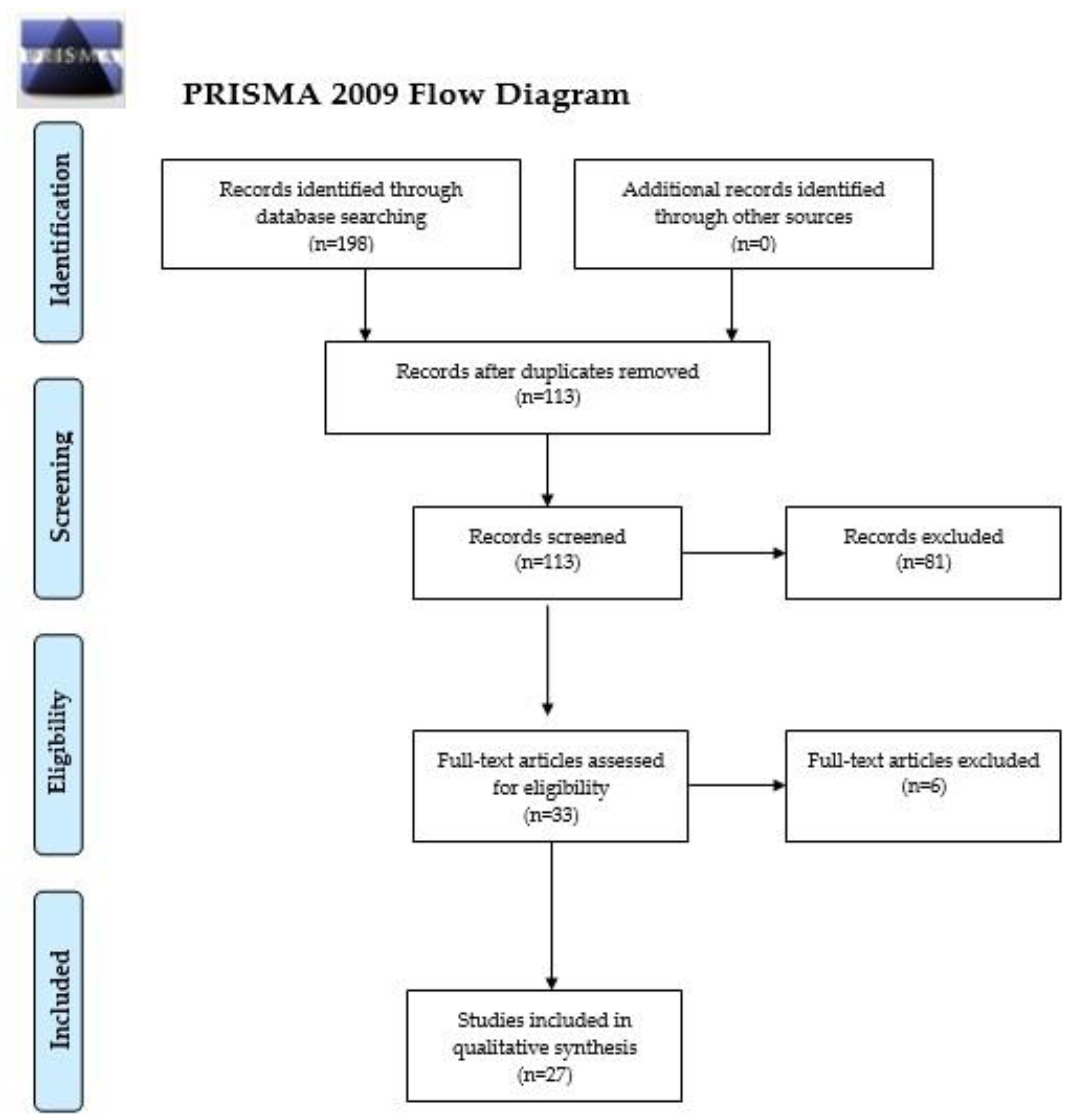
2. Materials and Methods
3. Results
3.1. Cell-Free DNA
3.2. Extracellular Vesicles
3.3. Microparticles
3.4. Circulating Endothelial Cells
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADM | adrenomedullin |
| ANA | anagrelide |
| APs | activated platelets |
| ASA | acetylsalycilic acid |
| CALR | calreticulin |
| CD | cluster of differentiation |
| CEC | circulating endothelial cells |
| cfDNA | cell-free DNA |
| CK | cytokine(s) |
| CML | chronic myeloid leukemia |
| CPA | circulating procoagulant activity of plasma |
| CV risk | cardiovascular risk |
| ED-1 | endothelin-1 |
| ELISA | enzyme-linked immunoassay |
| EM+IGA | electron microscopy and immunogold analysis |
| EMPs | endothelial MPs |
| EMVs | endothelial MVs |
| ET | essential thrombocythemia |
| ETP | endogeneous thrombin potential |
| GMPs | granulocyte-derived MPs |
| Hb | hemoglobin |
| Ht | hematocrit |
| IL-6 | interleukin-6 |
| LDH | lactate dehydrogenase |
| MEVs-CK | monocyte-derived extracellular vesicles |
| MF | myelofibrosis (unspecified whether primary or secondary) |
| miR | microRNA |
| MKMVs | megakaryocyte MVs |
| MMPs | monocyte-derived MPs |
| MMVs | monocyte MVs |
| MP | microparticles |
| MPN | myeloproliferative neoplasms |
| MPNu | MPN unclassifiable |
| MVs | microvesicles |
| PaCS | particulate cytoplasmic structures |
| PCA | procoagulant activity |
| PLTs | platelets |
| PLTMVs | platelet MVs |
| PMF | primary myelofibrosis |
| PMAs | platelet microaggregates |
| PMPs | platelet-derived MPs |
| PMCs | platelet-monocyte conjugates |
| PNCs | platelet-neutrophil conjugates |
| PS | phosphatidylserine |
| PV | polycythemia vera |
| RBCs | red blood cells |
| RMPs | red blood cell MPs |
| RT | reactive thrombocytosis |
| RUX | ruxolitinib |
| SMF | secondary MF |
| SP | secondary polycythemia |
| TFMPs | tissue factor-positive MPs |
| TN | triple-negative |
| VAF | variant allele frequency |
| VEFGR2 | vascular endothelial growth factor receptor 2 |
| VTE | venous thromboembolism |
| vs | versus |
| WB | Western Blot |
| WBCs | white blood cell count (leukocytes) |
| ↑ | increased |
| ↓ | decreased |
| (+) | positive |
| (−) | negative |
References
- Kim, S.Y.; Bae, S.H.; Bang, S.M.; Eom, K.S.; Hong, J.; Jang, S.; Jung, C.W.; Kim, H.J.; Kim, H.Y.; Kim, M.K.; et al. The 2020 revision of the guidelines for the management of myeloproliferative neoplasms. Korean J. Intern. Med. 2021, 36, 45–62. [Google Scholar] [CrossRef]
- Di Battista, V.; Bochicchio, M.T.; Giordano, G.; Napolitano, M.; Lucchesi, A. Genetics and pathogenetic role of inflammasomes in Philadelphia negative chronic myeloproliferative neoplasms: A narrative review. Int. J. Mol. Sci. 2021, 22, 561. [Google Scholar] [CrossRef]
- Moisa, C.; Gaman, M.A.; Pascu, E.G.; Assani, A.D.; Dragusin, O.C.; Epingeac, M.E.; Gaman, A.M. The role of oxidative stress in essential thrombocythemia. Arch. Balk. Med. Union 2018, 53, 70–75. [Google Scholar]
- Spivak, J.L. Myeloproliferative neoplasms. N. Engl. J. Med. 2017, 376, 2168–2181. [Google Scholar] [CrossRef] [Green Version]
- Arachchillage, D.R.J.; Laffan, M. Pathogenesis and management of thrombotic disease in myeloproliferative neoplasms. Semin. Thromb. Hemost. 2019, 45, 604–611. [Google Scholar] [CrossRef]
- Hultcrantz, M.; Wilkes, S.R.; Kristinsson, S.Y.; Andersson, T.M.-L.; Derolf, Å.R.; Eloranta, S.; Samuelsson, J.; Landgren, O.; Dickman, P.W.; Lambert, P.C.; et al. Risk and cause of death in patients diagnosed with myeloproliferative neoplasms in Sweden between 1973 and 2005: A population-based study. J. Clin. Oncol. 2015, 33, 2288–2295. [Google Scholar] [CrossRef] [PubMed]
- Gaman, A.M.; Moisa, C.; Diaconu, C.C.; Gaman, M.A. Crosstalk between Oxidative Stress, Chronic Inflammation and Disease Progression in Essential Thrombocythemia. Rev. Chim. 2019, 70, 3486–3489. [Google Scholar] [CrossRef]
- Spina, V.; Rossi, D. Liquid biopsy in tissue-born lymphomas. Swiss Med. Wkly. 2019, 149, w14709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, Y.; Zhang, Y.; Khoo, B.L. Liquid biopsy technologies for hematological diseases. Med. Res. Rev. 2021, 41, 246–274. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Matoba, R.; Kato, K. Recent advances in liquid biopsy in precision oncology research. Biol. Pharm. Bull. 2019, 42, 337–342. [Google Scholar] [CrossRef] [Green Version]
- Junqueira-Neto, S.; Batista, I.A.; Costa, J.L.; Melo, S.A. Liquid biopsy beyond circulating tumor cells and cell-free DNA. Acta Cytol. 2019, 63, 479–488. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Pluye, P.; Robert, E.; Cargo, M.; Bartlett, G.; O’cathain, A.; Griffiths, F.; Boardman, F.; Gagnon, M.P.; Rousseau, M.C. Proposal: A Mixed Methods Appraisal Tool for Systematic Mixed Studies Reviews; McGill University: Montréal, QC, Canada, 2011; Volume 2. [Google Scholar]
- Garcia-Gisbert, N.; Fernández-Ibarrondo, L.; Fernández-Rodríguez, C.; Gibert, J.; Andrade-Campos, M.; Arenillas, L.; Camacho, L.; Angona, A.; Longarón, R.; Salar, A.; et al. Circulating Cell-Free DNA Improves the Molecular Characterisation of Ph-Negative Myeloproliferative Neoplasms. Br. J. Haematol. 2021, 192, 300–309. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.; Ricci, F.; Sollazzo, D.; Ottaviani, E.; Romano, M.; Auteri, G.; Bartoletti, D.; Reggiani, M.L.B.; Vianelli, N.; Tazzari, P.L.; et al. Circulating megakaryocyte and platelet microvesicles correlate with response to ruxolitinib and distinct disease severity in patients with myelofibrosis. Br. J. Haematol. 2019, 185, 987–991. [Google Scholar] [CrossRef] [PubMed]
- Barone, M.; Catani, L.; Ricci, F.; Romano, M.; Forte, D.; Auteri, G.; Bartoletti, D.; Ottaviani, E.; Tazzari, P.L.; Vianelli, N.; et al. The Role of Circulating Monocytes and JAK Inhibition in the Infectious-Driven Inflammatory Response of Myelofibrosis. Oncoimmunology 2020, 9, 1782575. [Google Scholar] [CrossRef] [PubMed]
- Poisson, J.; Tanguy, M.; Davy, H.; Camara, F.; El Mdawar, M.-B.; Kheloufi, M.; Dagher, T.; Devue, C.; Lasselin, J.; Plessier, A.; et al. Erythrocyte-Derived Microvesicles Induce Arterial Spasms in JAK2V617F Myeloproliferative Neoplasm. J. Clin. Investig. 2020, 130, 2630–2643. [Google Scholar] [CrossRef] [Green Version]
- Pecci, A.; Necchi, V.; Barozzi, S.; Vitali, A.; Boveri, E.; Elena, C.; Bernasconi, P.; Noris, P.; Solcia, E. Particulate Cytoplasmic Structures with High Concentration of Ubiquitin-Proteasome Accumulate in Myeloid Neoplasms. J. Hematol. Oncol. 2015, 8, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caivano, A.; Laurenzana, I.; De Luca, L.; La Rocca, F.; Simeon, V.; Trino, S.; D’Auria, F.; Traficante, A.; Maietti, M.; Izzo, T.; et al. High Serum Levels of Extracellular Vesicles Expressing Malignancy-Related Markers Are Released in Patients with Various Types of Hematological Neoplastic Disorders. Tumour Biol. 2015, 36, 9739–9752. [Google Scholar] [CrossRef]
- Fel, A.; Lewandowska, A.E.; Petrides, P.E.; Wiśniewski, J.R. Comparison of Proteome Composition of Serum Enriched in Extracellular Vesicles Isolated from Polycythemia Vera Patients and Healthy Controls. Proteomes 2019, 7, 20. [Google Scholar] [CrossRef] [Green Version]
- Forte, D.; Barone, M.; Morsiani, C.; Simonetti, G.; Fabbri, F.; Bruno, S.; Bandini, E.; Sollazzo, D.; Collura, S.; Deregibus, M.C.; et al. Distinct Profile of CD34+ Cells and Plasma-Derived Extracellular Vesicles from Triple-Negative Patients with Myelofibrosis Reveals Potential Markers of Aggressive Disease. J. Exp. Clin. Cancer Res. 2021, 40, 49. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Qi, J.; Zhao, S.; Shen, W.; Dai, L.; Han, W.; Huang, M.; Wang, Z.; Ruan, C.; Wu, D.; et al. Clinical Significance of Circulating Microparticles in Ph- Myeloproliferative Neoplasms. Oncol. Lett. 2017, 14, 2531–2536. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villmow, T.; Kemkes-Matthes, B.; Matzdorff, A.C. Markers of Platelet Activation and Platelet-Leukocyte Interaction in Patients with Myeloproliferative Syndromes. Thromb. Res. 2002, 108, 139–145. [Google Scholar] [CrossRef]
- Trappenburg, M.C.; van Schilfgaarde, M.; Marchetti, M.; Spronk, H.M.; ten Cate, H.; Leyte, A.; Terpstra, W.E.; Falanga, A. Elevated Procoagulant Microparticles Expressing Endothelial and Platelet Markers in Essential Thrombocythemia. Haematologica 2009, 94, 911–918. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taniguchi, Y.; Tanaka, H.; Luis, E.J.; Sakai, K.; Kumode, T.; Sano, K.; Serizawa, K.; Rai, S.; Morita, Y.; Hanamoto, H.; et al. Elevated Plasma Levels of Procoagulant Microparticles Are a Novel Risk Factor for Thrombosis in Patients with Myeloproliferative Neoplasms. Int. J. Hematol. 2017, 106, 691–703. [Google Scholar] [CrossRef]
- Tan, X.; Shi, J.; Fu, Y.; Gao, C.; Yang, X.; Li, J.; Wang, W.; Hou, J.; Li, H.; Zhou, J. Role of Erythrocytes and Platelets in the Hypercoagulable Status in Polycythemia Vera through Phosphatidylserine Exposure and Microparticle Generation. Thromb. Haemost. 2013, 109, 1025–1032. [Google Scholar]
- Piccin, A.; Steurer, M.; Feistritzer, C.; Murphy, C.; Eakins, E.; Van Schilfgaarde, M.; Corvetta, D.; Di Pierro, A.M.; Pusceddu, I.; Marcheselli, L.; et al. Observational Retrospective Study of Vascular Modulator Changes during Treatment in Essential Thrombocythemia. Transl. Res. 2017, 184, 21–34. [Google Scholar] [CrossRef]
- Ahadon, M.; Abdul Aziz, S.; Wong, C.L.; Leong, C.F. Plasma-Derived Microparticles in Polycythaemia Vera. Malays. J. Pathol. 2018, 40, 41–48. [Google Scholar]
- Aswad, M.H.; Kissová, J.; Rihova, L.; Zavrelova, J.; Ovesná, P.; Penka, M. High Level of Circulating Microparticles in Patients with BCR/ABL Negative Myeloproliferative Neoplasm—A Pilot Study. Klin. Onkol. 2019, 32, 109–116. [Google Scholar] [CrossRef]
- Charpentier, A.; Lebreton, A.; Rauch, A.; Bauters, A.; Trillot, N.; Nibourel, O.; Tintillier, V.; Wemeau, M.; Demory, J.-L.; Preudhomme, C.; et al. Microparticle Phenotypes Are Associated with Driver Mutations and Distinct Thrombotic Risks in Essential Thrombocythemia. Haematologica 2016, 101, e365–e368. [Google Scholar] [CrossRef] [Green Version]
- Marchetti, M.; Tartari, C.J.; Russo, L.; Panova-Noeva, M.; Leuzzi, A.; Rambaldi, A.; Finazzi, G.; Woodhams, B.; Falanga, A. Phospholipid-Dependent Procoagulant Activity Is Highly Expressed by Circulating Microparticles in Patients with Essential Thrombocythemia. Am. J. Hematol. 2014, 89, 68–73. [Google Scholar] [CrossRef] [Green Version]
- Moles-Moreau, M.-P.; Ternisien, C.; Tanguy-Schmidt, A.; Boyer, F.; Gardembas, M.; Dib, M.; Ponthieux, A.; Guardiola, P.; Ifrah, N.; Hunault-Berger, M. Flow Cytometry-Evaluated Platelet CD36 Expression, Reticulated Platelets and Platelet Microparticles in Essential Thrombocythaemia and Secondary Thrombocytosis. Thromb. Res. 2010, 126, e394–e396. [Google Scholar] [CrossRef] [Green Version]
- Connor, D.E.; Ma, D.D.F.; Joseph, J.E. Flow Cytometry Demonstrates Differences in Platelet Reactivity and Microparticle Formation in Subjects with Thrombocytopenia or Thrombocytosis Due to Primary Haematological Disorders. Thromb. Res. 2013, 132, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Duchemin, J.; Ugo, V.; Ianotto, J.-C.; Lecucq, L.; Mercier, B.; Abgrall, J.-F. Increased Circulating Procoagulant Activity and Thrombin Generation in Patients with Myeloproliferative Neoplasms. Thromb. Res. 2010, 126, 238–242. [Google Scholar] [CrossRef] [PubMed]
- Kissova, J.; Ovesna, P.; Bulikova, A.; Zavřelova, J.; Penka, M. Increasing Procoagulant Activity of Circulating Microparticles in Patients with Philadelphia-Negative Myeloproliferative Neoplasms: A Single-Centre Experience: A Single-Centre Experience. Blood Coagul. Fibrinolysis 2015, 26, 448–453. [Google Scholar] [CrossRef]
- Alonci, A.; Allegra, A.; Bellomo, G.; Penna, G.; D’Angelo, A.; Quartarone, E.; Musolino, C. Evaluation of Circulating Endothelial Cells, VEGF and VEGFR2 Serum Levels in Patients with Chronic Myeloproliferative Diseases. Hematol. Oncol. 2008, 26, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Belotti, A.; Elli, E.; Speranza, T.; Lanzi, E.; Pioltelli, P.; Pogliani, E. Circulating endothelial cells and endothelial activation in essential thrombocythemia: Results from CD146+ immunomagnetic enrichment—Flow cytometry and soluble E-selectin detection. Am. J. Hematol. 2012, 87, 319–320. [Google Scholar] [CrossRef]
- Torres, C.; Fonseca, A.M.; Leander, M.; Matos, R.; Morais, S.; Campos, M.; Lima, M. Circulating Endothelial Cells in Patients with Venous Thromboembolism and Myeloproliferative Neoplasms. PLoS ONE 2013, 8, e81574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treliński, J.; Wierzbowska, A.; Krawczyńska, A.; Sakowicz, A.; Pietrucha, T.; Smolewski, P.; Robak, T.; Chojnowski, K. Plasma Levels of Angiogenic Factors and Circulating Endothelial Cells in Essential Thrombocythemia: Correlation with Cytoreductive Therapy and JAK2-V617F Mutational Status. Leuk. Lymphoma 2010, 51, 1727–1733. [Google Scholar] [CrossRef]
- Treliński, J.; Wierzbowska, A.; Krawczyńska, A.; Sakowicz, A.; Pietrucha, T.; Smolewski, P.; Robak, T.; Chojnowski, K. Circulating Endothelial Cells in Essential Thrombocythemia and Polycythemia Vera: Correlation with JAK2-V617F Mutational Status, Angiogenic Factors and Coagulation Activation Markers. Int. J. Hematol. 2010, 91, 792–798. [Google Scholar] [CrossRef]
- Hultcrantz, M.; Björkholm, M.; Dickman, P.W.; Landgren, O.; Derolf, Å.R.; Kristinsson, S.Y.; Andersson, T.M.L. Risk for Arterial and Venous Thrombosis in Patients with Myeloproliferative Neoplasms: A Population-Based Cohort Study. Ann. Intern. Med. 2018, 168, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Tefferi, A.; Barbui, T. Polycythemia Vera and Essential Thrombocythemia: 2021 Update on Diagnosis, Risk-Stratification and Management. Am. J. Hematol. 2020, 95, 1599–1613. [Google Scholar] [CrossRef] [PubMed]
- Moisa, C.; Gaman, M.A.; Diaconu, C.C.; Gaman, A.M. Oxidative Stress Levels, JAK2V617F Mutational Status and Thrombotic Complications in Patients with Essential Thrombocythemia. Rev. Chim. 2019, 70, 2822–2825. [Google Scholar] [CrossRef]
- Moisă, C.; Găman, M.A.; Diaconu, C.C.; Assani, A.D.; Găman, A.M. The Evaluation of Oxidative Stress in Patients with Essential Thrombocythemia Treated with Risk-Adapted Therapy. Arch. Balk. Med. Union 2018, 53, 529–534. [Google Scholar] [CrossRef]
- Osteikoetxea, X.; Németh, A.; Sódar, B.W.; Vukman, K.V.; Buzás, E.I. Extracellular Vesicles in Cardiovascular Disease: Are They Jedi or Sith? J. Physiol. 2016, 594, 2881–2894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Żmigrodzka, M.; Witkowska-Piłaszewicz, O.; Winnicka, A. Platelets Extracellular Vesicles as Regulators of Cancer Progression-an Updated Perspective. Int. J. Mol. Sci. 2020, 21, 5195. [Google Scholar] [CrossRef] [PubMed]
- French, S.L.; Butov, K.R.; Allaeys, I.; Canas, J.; Morad, G.; Davenport, P.; Laroche, A.; Trubina, N.M.; Italiano, J.E.; Moses, M.A.; et al. Platelet-Derived Extracellular Vesicles Infiltrate and Modify the Bone Marrow during Inflammation. Blood Adv. 2020, 4, 3011–3023. [Google Scholar] [CrossRef]
- Nomura, S. Extracellular Vesicles and Blood Diseases. Int. J. Hematol. 2017, 105, 392–405. [Google Scholar] [CrossRef]
- Reeves, B.N.; Beckman, J.D. Novel Pathophysiological Mechanisms of Thrombosis in Myeloproliferative Neoplasms. Curr. Hematol. Malig. Rep. 2021, 16, 204–313. [Google Scholar] [CrossRef]
- Woo, J.; Baumann, A.; Arguello, V. Recent Advancements of Flow Cytometry: New Applications in Hematology and Oncology. Expert Rev. Mol. Diagn. 2014, 14, 67–81. [Google Scholar] [CrossRef]
- Lazar, S.; Goldfinger, L.E. Platelets and Extracellular Vesicles and Their Cross-Talk with Cancer. Blood 2021, 137, 3192–3200. [Google Scholar] [CrossRef] [PubMed]
- Cacic, D.; Reikvam, H.; Nordgård, O.; Meyer, P.; Hervig, T. Platelet Microparticles Protect Acute Myelogenous Leukemia Cells against Daunorubicin-Induced Apoptosis. Cancers 2021, 13, 1870. [Google Scholar] [CrossRef] [PubMed]
- Galeano-Valle, F.; Ordieres-Ortega, L.; Oblitas, C.M.; Del-Toro-Cervera, J.; Alvarez-Sala-Walther, L.; Demelo-Rodríguez, P. Inflammatory Biomarkers in the Short-Term Prognosis of Venous Thromboembolism: A Narrative Review. Int. J. Mol. Sci. 2021, 22, 2627. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Maitusong, M.; Muyesai, N. Association of Endothelial and Red Blood Cell Microparticles with Acute Myocardial Infarction in Chinese: A Retrospective Study. Ann. Palliat. Med. 2020, 9, 1564–1570. [Google Scholar] [CrossRef]
- Noulsri, E. Effects of Cell-Derived Microparticles on Immune Cells and Potential Implications in Clinical Medicine. Lab. Med. 2021, 52, 122–135. [Google Scholar] [CrossRef]
- Alam, A.U.; Karkhaneh, M.; Sun, H.L.; Wu, C. Survival patterns among venous thromboembolism patients with hematologic malignancies in Alberta, Canada from 2003 to 2015. Thromb. Res. 2021, 199, 59–66. [Google Scholar] [CrossRef]
- Carobbio, A.; Ferrari, A.; Masciulli, A.; Ghirardi, A.; Barosi, G.; Barbui, T. Leukocytosis and thrombosis in essential thrombocythemia and polycythemia vera: A systematic review and meta-analysis. Blood Adv. 2019, 3, 1729–1737. [Google Scholar] [CrossRef]

{kind=link}
| Author and Year | Study Location | Study Design | MPN | Patients No., Time Point | Parameters Assessed | Methods of Evaluation | Main Results |
|---|---|---|---|---|---|---|---|
| Garcia-Gisbert et al. (2020) [15] | Spain | Cross-sectional | PV, ET, PMF | 107 diagnosis follow-up | cfDNA | DNA isolation | ↑ cfDNA ↑ cfDNA, cfDNA/WBCs in PMF vs. PV, ET ↑ cfDNA in MPNs with thrombosis at diagnosis/during follow-up ↑ VAF JAK2, MPL, SRSF2 in cfDNA vs. granulocyte DNA |
| Barone et al. (2019) [16] | Italy | Cross-sectional | ET, PMF, SMF | 81 follow-up | PLTMVs, MKMVs, EMVs, MMVs, | Flow cytometry | ↓ MKMVs in JAK2(+)/CALR(+)/TN MF ↓ MKMVs, ↑ PLTMVs in MF & ET ↑ PLTMVs in ET vs. MF ↑ PLTMVs in JAK2(+)/CALR(+) MF vs. TN MPNs or controls ↓ PLTMVs in TN vs. JAK2(+)/CALR(+) MF ↓ MKMVs, ↑ PLTMVs in JAK2(+)/CALR(+) ET vs. controls & TN-ET ↑ PLTMVs, ↓ MKMVs in high/intermediate 2 vs. low/intermediate-1 risk MF & controls MKMVs in MF: (+) correlation wit PLTs, (−) with IL-6 PLTMVs in MF: (−) correlation with splenomegaly degree, (+) with P-selectin, thrombopoietin ↓ PLTMVs, ↑MKMVs in RUX spleen-responders in MF at baseline MKMVs <19.95% = spleen non-responders RUX ↓PLTMVs, ↑MKMVs in spleen-responders at 6 months ↑EMVs, MMVs in MF RUX ↓ EMVs in spleen-responders |
| Barone et al. (2020) [17] | Italy | Experimental | MF | 30 diagnosis | MEVs-CK | Flow cytometry | RUX ↑ IL-1β, IL-6, TNF-α in LPS-stimulated MF monocytes |
| Poisson et al. (2020) [18] | France | Experimental | JAK2V617F(+) MPNs | 7 follow-up | Plasma MVs | Flow cytometry | MVs from JAK2 V617F-positive MPNs ↑phenylephrine-induced contraction in mice aorta |
| Pecci et al. (2015) [19] | Italy | Cross-sectional | PV, ET, PMF | 5 follow-up | PaCS, proteasome levels | EM+IGA, WB, ELISA | ↑ PaCS in PLTs, granulocytes ↑ proteasome levels in PLTs and granulocytes extracts ↑ proteasome levels in plasma |
| Caivano et al. (2015) [20] | Italy | Cross-sectional | PMF | 5 follow-up | MVs | Flow cytometry | ↑ small-diameter MVs |
| Fel et al. (2019) [21] | Germany | Case-control | PV | 9 follow-up | EVs | Liquid chromatography, tandem mass spectrometry | ↑ CD42d+, CD71+, CD62L+ cells in PV ↑ APs, ↑ inflammatory/immune/angiogenic/procoagulant markers ↑ 13x transferrin receptor protein 1 ↑ 11.2x heparanase ↑ 5–6x plasminogen activator inhibitor 1, histone H4 and H2B, angiogenin ↑ 4–5x matrix metalloproteinase-9, neurogenic locus notch homolog protein 3, lysozyme C, histone H3, L-selectin, lactotransferrin, solute carrier family 2 ↑ 3–4x coagulation factor XI, myeloperoxidase, C-reactive protein, vinculin, platelet multimerin-1 |
| Forte et al. (2011) [22] | Italy | Cross-sectional | PMF | 29 follow-up | EVs | Flow cytometry | ↓ MK-EVs in JAK2 V617F (+) & TN-MF ↓ PLT-EVs in TN-MF, controls vs. JAK2 V617F (+) MF ↑ in vitro survival, ↑ miR-361-5p of TN-MF EVs miR-34a-5p, miR-222-3p, miR-361-5p upregulated in JAK2 V617F (+) & TN-MF miR-127-3p upregulated in JAK2 V617F (+) MF (+) miR-34a-5p, (−) miR-212-3p & JAK2 V617F VAF association |
| Zhang et al. (2017) [23] | China | Cross-sectional | PV, ET, PMF | 92 follow-up | PMPs, EMPs, RMPs, TF+MPs | Flow cytometry | ↑ RMPs, ↑ PMPs, ↑ EMPs, ↑ TF+MPs PMF vs. PV: ↑ RMPs, ↑ PMPs, ↑ EMPs, ↑ TF+MPs ET vs. PV: ↑ EMPs |
| Villmow et al. (2003) [24] | Germany | Cross-sectional | PV, ET, PMF | 37 follow-up | PMPs, PMAs, APs, PNCs, PMCs | Flow cytometry | ↑ APs ↑ PMPs in PV, ET, MF vs. CML, controls ↑ PNCs, ↑PMCs in ET, PV vs. MF, CML, controls |
| Trappenburg et al. (2009) [25] | Italy | Cross-sectional | ET | 21 follow-up | PMPs, EMPs, GMPs, MMPs, TF+MPs | Flow cytometry | ↑ MPs, ↑ CD61(+) PMPs, ↓ CD63(+) PMPs, ↑ vWF, ↑ TF+MPs ↑ EMPs, i.e., CD62E(+), CD144(+) ↑ GMPs, i.e., CD66b(+) and CD66acde(+) ↑ MMPs, i.e., CD14(+) ↑ CD62E(+)/CD41(+) EMPs in ET with ↑ CV risk |
| Taniguchi et al. (2017) [26] | Japan | Cross-sectional | PV, ET, PMF, SMF | 59 follow-up | PMPs, EMPs, TF+MPs | Flow cytometry | cytoreduction ↓ procoagulant, annexin V(+) MPs, ↓ TF+MPs anticoagulation ↓ MPs in MPNs 70% of annexin V(+) MPs = PMPs, i.e., CD41a(+) 30% of annexin V(+) MPs = EMPs, i.e., CD146(+), or CD45(+), i.e., leukocyte-derived history of thrombosis +/− no cytoreduction =↑ TF+MPs >84.7 TF+MPs/µL, documented CV risk = predictors of thrombosis in MPNs |
| Tan et al. (2013) [27] | China | Cross-sectional | PV | 23 follow-up | PMPs, GMPs, EMPs, RMPs, TF+MPs | Flow cytometry | ↑MPs, ↑ PMPs, ↑ RMPs, ↑ GMPs, ↑ EMPs in PV vs. SP or controls ↑ PS(+) PLTs, RBCs in PV vs. SP or controls ↓ clotting time, ↑thrombin and FXase generation in PV HU ↓ MPs, ↑ PMPs, ↑ RMPs, PS(+) PLTs/RBCs in PV |
| Piccin et al. (2017) [28] | Italy | Cross-sectional | JAK2V617F(+) ET | 66 follow-up | PMPs, EMPs, RMPs, TF+MPs | Flow cytometry | ↓ MPs, ↓ PMPs, ↑ NO, ↑ ADM in ET on ASA, HU+ASA ↑ EMPs, ↑ RMPs in untreated ET ↑ EMPs in ET vs. controls ↓ EMPs, ↓ ED-1 in ET on ASA+ANA |
| Ahadon et al. (2018) [29] | Malaysia | Case-control | PV | 15 diagnosis | PMPs, EMPs | Flow cytometry | ↑ PMPs |
| Aswad et al. (2019) [30] | Czech Republic | Cross-sectional | PV, ET, PMF | 179 diagnosis follow-up | PMPs, RMPs | Flow cytometry, functional coagulation assays | ↑ PMPs, RMPs ↑ PMPs in PV, ET vs. PMF ↑ procoagulant activity of MPs association of PMPs procoagulant activity and PMPs levels ↓ PMPs in MPNs with (+) history of thrombosis ↑ PMPs in JAK2 V617F (+) MPNs PMPs correlated with Hb, Ht, RBCs, PLTs, WBCs |
| Charpentier et al. (2016) [31] | France | Cross-sectional | ET | 74 diagnosis | PMPs, RMPs, MMPs, GMPs, EMPs | Flow cytometry | ↑ total MPs, RMPs, PMPs in JAK2 V617F (+) vs. CALR(+)/TN-ET (+) associations of MPs with thrombin generation, phospholipid-dependent procoagulant activity ↑ procoagulant activity in JAK2 V617F (+) vs. CALR(+)/TN-ET ↑ MPs in high vs. intermediate/low thrombotic risk ET >4600 MPs/µL = high-risk of thrombosis in ET |
| Marchetti et al. (2014) [32] | Italy | Cross-sectional | ET | 73 follow-up | MPs | Flow cytometry | ↑ ETP, ↑ peak of thrombin, ↓ lag-time, ↓ time to peak, ↓ clotting times ↑ ETP, ↑ peak of thrombin, ↓ lag-time, ↓time to peak in JAK2 V617F (+) vs. (−) ↓ clotting times in JAK2 V617F (+) vs. (−) JAK2 V617F predicts shortened clotting times (+) association of PCA and lag-time, time to peak (−) association of PCA and peak of thrombin, ETP removal of MPs ↓ EDT, ↑ clotting times in ET, controls ↑ TF, ↑ FVIIa/AT in JAK2 V617F (+) ET |
| Moles-Moreau et al. (2009) [33] | France | Cross-sectional | ET | 37 diagnosis | PMPs | Flow cytometry | ↑ PMPs, PMPs/PLTs, ↑ CD36+ cells ↑ PMPs/PLTs ratio, ↑ CD36+ cells in ET vs. RT ↑ PMPs, PMPs/PLTs ratio in RT vs. controls |
| Connor et al. (2013) [34] | Australia | Cross-sectional | ET | 10 follow-up | PMPs | Flow cytometry | ↑PMPs |
| Duchemin et al. (2010) [35] | France | Cross-sectional | PV, ET | 44 follow-up | MPs | Functional assays | ↑ CPA, ↓ ETP in MPNs pre-/post-filtration of MPs ↑ CPA in JAK2 V617F (+), homozygous genotype ↑ TM-resistance, ↓free protein S (+) association of CPA and neutrophils, RBCs, PLTs (−) association of ETP and JAK2 V617F allele burden ↑ CPA, ↓ ETP in JAK2 V617F homozygous genotype MPNs post-filtration of MPs |
| Kissova et al. (2015) [36] | Czech Republic | Cross-sectional | PV, ET, PMF | 126 follow-up | MPs | Flow cytometry | ↑ MPs ↑ PCA of MPs in PV vs. ET/ PMF ↑ PCA of MPs in JAK2 V617F (+) vs. (−) MPNs (+) association of PCA of MPs with Hb, Ht in PV association of PCA with PLTs ↑ PCA of MPs in MPNs with venous thrombosis history cytoreduction ↓PCA of MPs |
| Alonci et al. (2008) [37] | Italy | Cross-sectional | PV, ET, PMF | 40 follow-up | CECs | Flow cytometry | ↑ CD34+ CECs, ↑ CD34+ CD133- VEGFR2+ CECs ↑ CD34+ CECs in PMF vs. ET, PV ↑ CD34+ CD133+ VEGFR2+ CECs in PMF, PV vs. controls, ET ↑ CD34+ CD133- VEGFR2+ CECs in PMF vs. PV |
| Belotti et al. (2011) [38] | Italy | Cross-sectional | ET | 39 follow-up | CECs | Flow cytometry | ↑ CD146+ CD45-CECs, soluble E-selectin |
| Torres et al. (2013) [39] | Portugal | Cross-sectional | PV, ET | 17 follow-up | CECs | Flow cytometry | ↑ MPNs, VTE vs. controls ↓ progenitor CECs in VTE vs. MPNs, controls ↑ CD62E+ CECs in MPNs vs. controls ↑ CD62E+, CD54+, CD142+ CECs in VTE vs. controls (+) associations of WBCs with total CECs, progenitor CECs, CD62E+CECs (−) associations of PLTs with CD54+CECs |
| Trelinski et al. (2010) [40] | Poland | Cross-sectional | ET | 65 diagnosis follow-up | CECs | Flow cytometry | ↑total, activated, resting, progenitor, CD46+, apoptotic CECs, VEGF, soluble VEFGR 1 ↓ placenta growth factor |
| Trelinski et al. (2010) [41] | Poland | Cross-sectional | PV, ET | 46 follow-up | CECs | Flow cytometry | ↑ total, activated, progenitor, apoptotic CECs ↑ resting CECs in ET versus PV, controls ↑ apoptotic CECs in ET versus PV ↑apoptotic CECs in PV with >8700 vs.<8700 WBCs |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Găman, M.-A.; Cozma, M.-A.; Dobrică, E.-C.; Crețoiu, S.M.; Găman, A.M.; Diaconu, C.C. Liquid Biopsy and Potential Liquid Biopsy-Based Biomarkers in Philadelphia-Negative Classical Myeloproliferative Neoplasms: A Systematic Review. Life 2021, 11, 677. https://doi.org/10.3390/life11070677
Găman M-A, Cozma M-A, Dobrică E-C, Crețoiu SM, Găman AM, Diaconu CC. Liquid Biopsy and Potential Liquid Biopsy-Based Biomarkers in Philadelphia-Negative Classical Myeloproliferative Neoplasms: A Systematic Review. Life. 2021; 11(7):677. https://doi.org/10.3390/life11070677
Chicago/Turabian StyleGăman, Mihnea-Alexandru, Matei-Alexandru Cozma, Elena-Codruța Dobrică, Sanda Maria Crețoiu, Amelia Maria Găman, and Camelia Cristina Diaconu. 2021. "Liquid Biopsy and Potential Liquid Biopsy-Based Biomarkers in Philadelphia-Negative Classical Myeloproliferative Neoplasms: A Systematic Review" Life 11, no. 7: 677. https://doi.org/10.3390/life11070677
APA StyleGăman, M.-A., Cozma, M.-A., Dobrică, E.-C., Crețoiu, S. M., Găman, A. M., & Diaconu, C. C. (2021). Liquid Biopsy and Potential Liquid Biopsy-Based Biomarkers in Philadelphia-Negative Classical Myeloproliferative Neoplasms: A Systematic Review. Life, 11(7), 677. https://doi.org/10.3390/life11070677