
On Analyzing Capnogram as a Novel Method for Screening COVID-19: A Review on Assessment Methods for COVID-19


Abstract
1. Introduction
2. Biological Properties of SARS-CoV-2
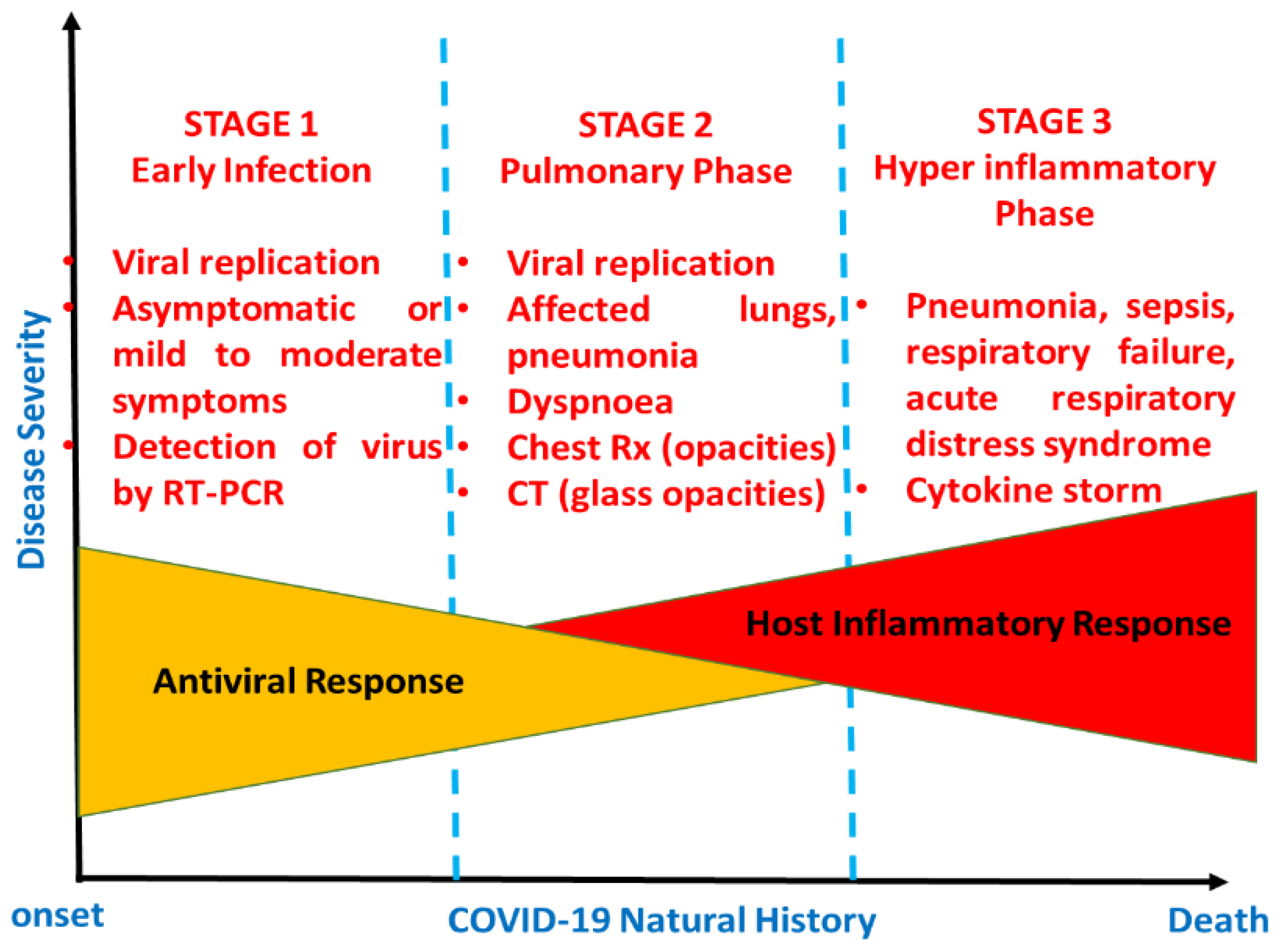
3. Clinical Manifestations of COVID-19
4. Diagnosis of COVID-19
- Collection of samples (this involves the collection of samples at the right time and using the right technique);
- Transportation of samples (this involves maintaining a cold chain and assessing the duration of transport);
- Testing samples (this involves using the most suitable method for analysis).
5. Existing Diagnostic Tools
5.1. Real-Time RT-PCR Test-Molecular Test
5.2. Rapid Antigen Detection (RAD) Test
5.3. Antibodies (Serology) Test
5.4. Chest Computed Tomography (CT)
6. Current Screening Tools for COVID-19
6.1. Thermometers
6.2. Thermal Imaging Systems
7. Expired Carbon Dioxide Measurement: A New Screening Tool for COVID-19
7.1. CO2 Removal from Human Body
7.2. Interpretation of Capnogram
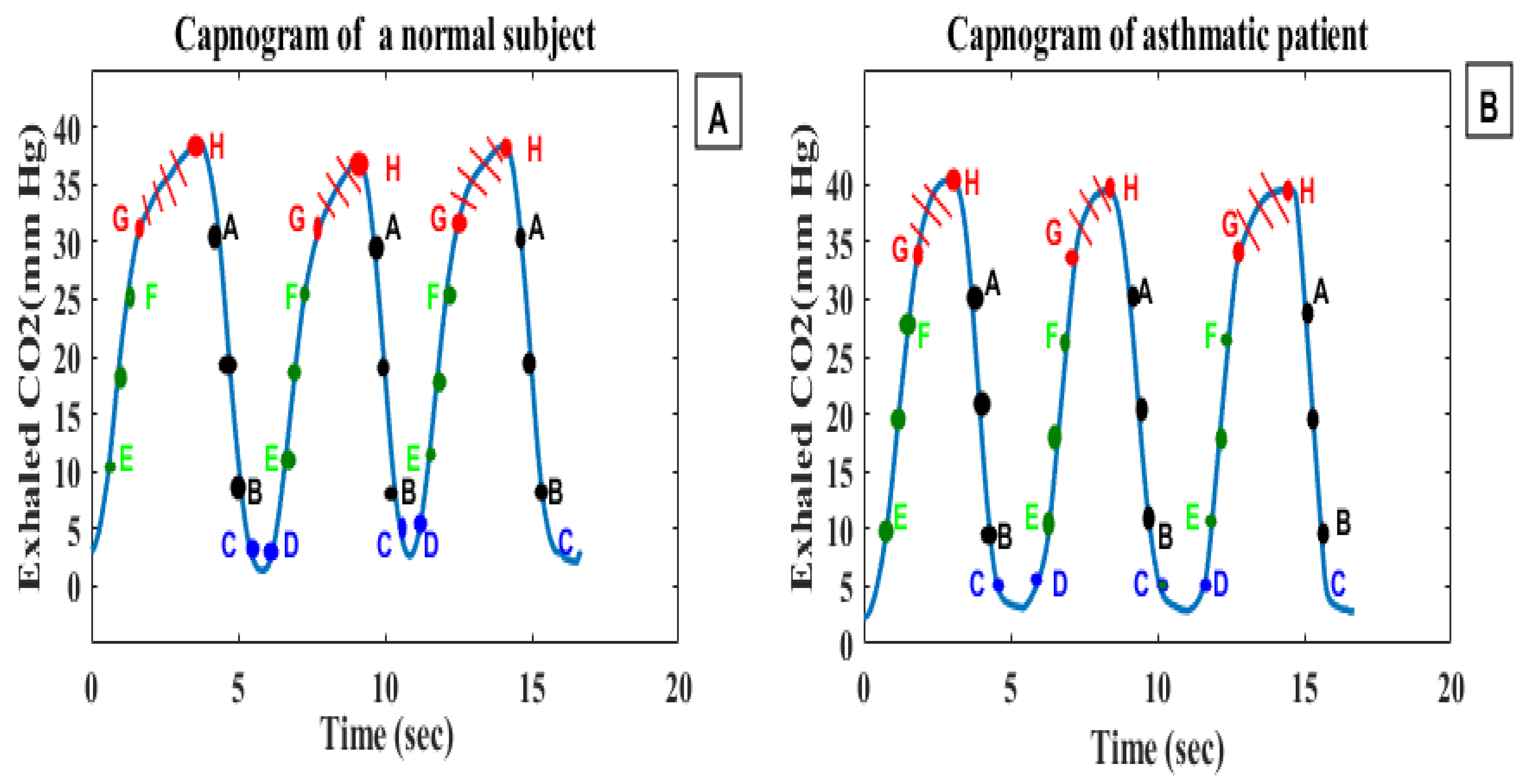
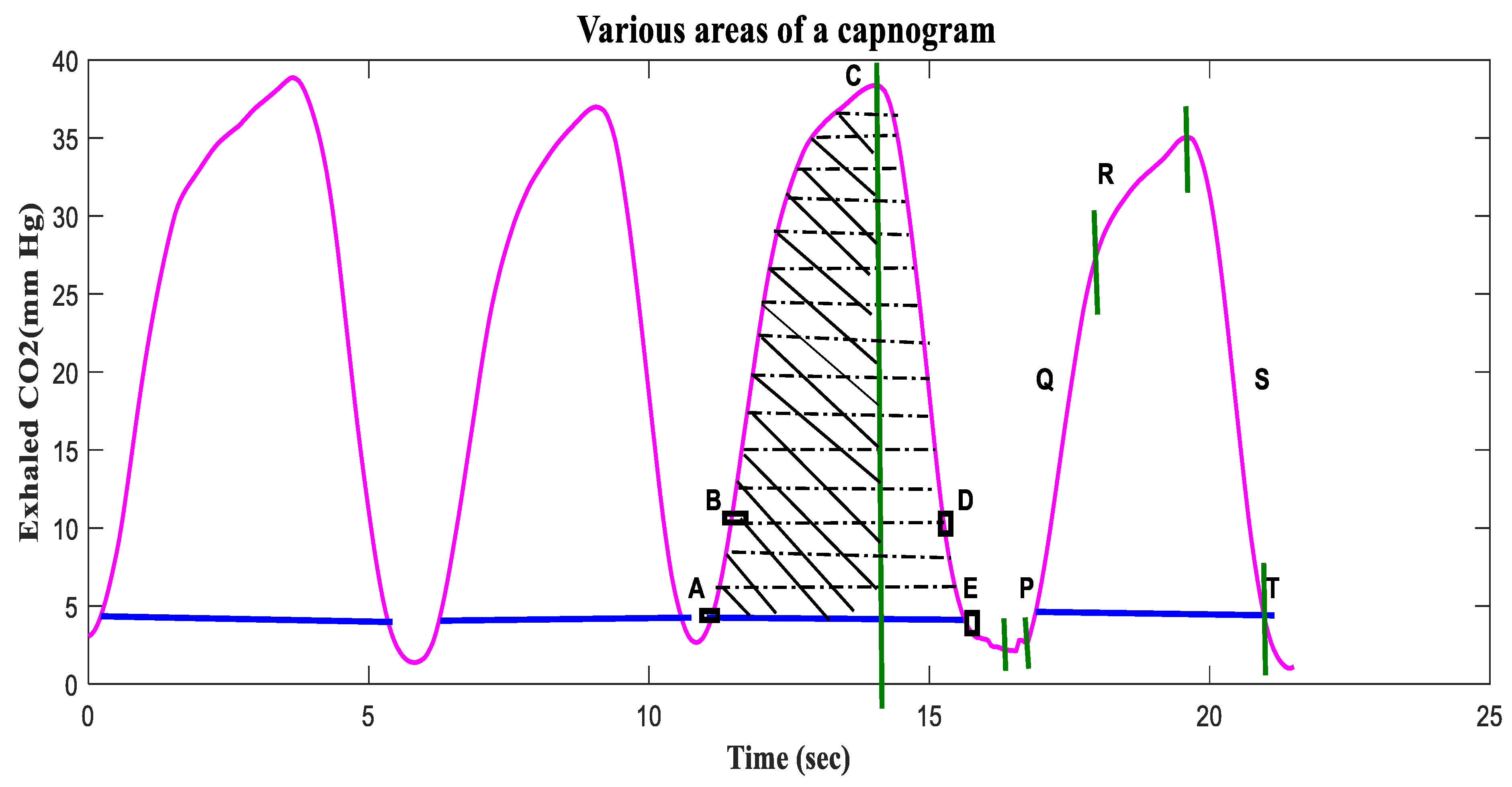
7.3. Analysis of Capnogram Waveform
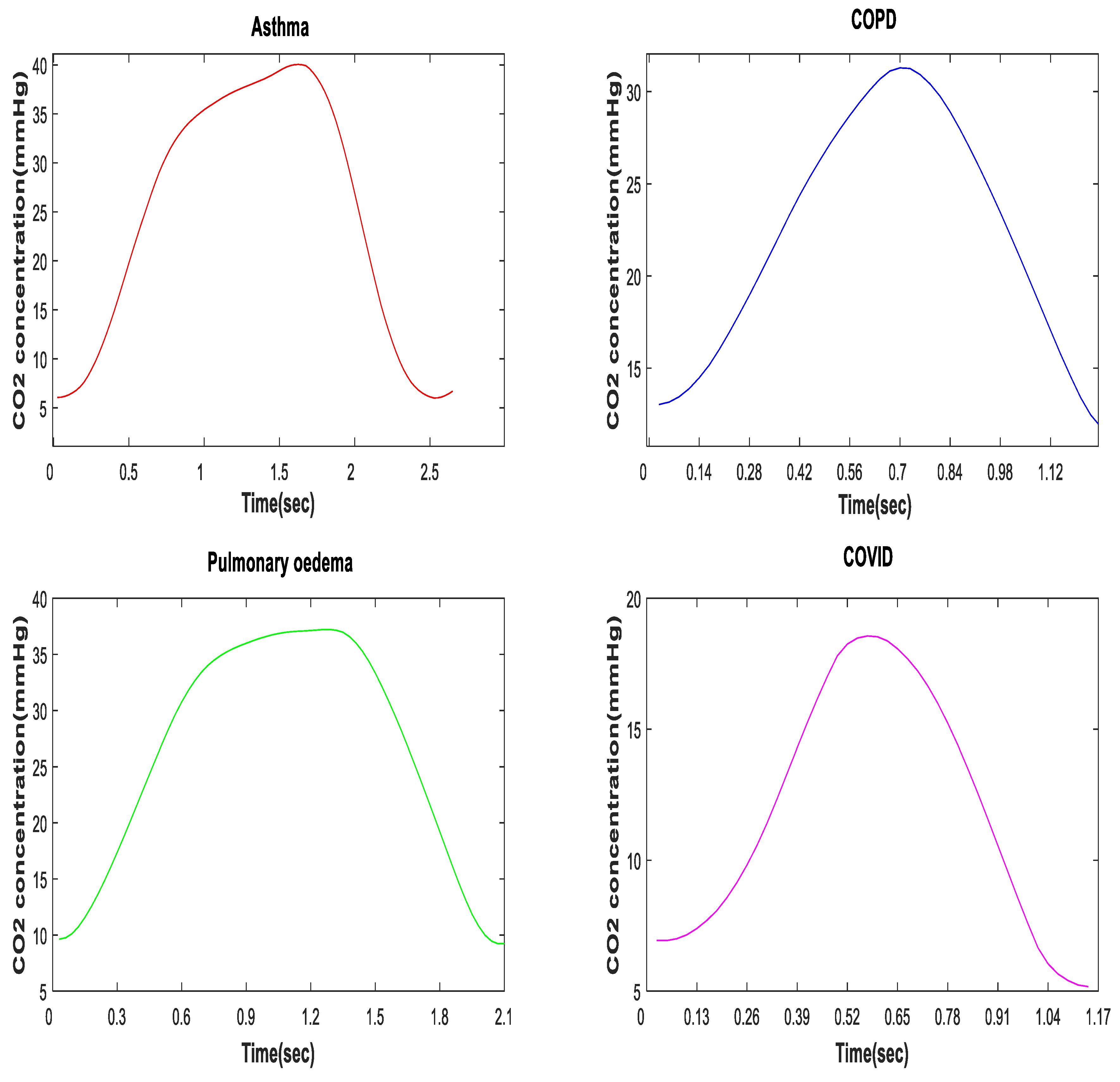
7.4. Relationship of CO2 and SARS-CoV-2 Infection
7.5. On the Capnogram as Feature for COVID-19 Detection
7.5.1. Study Setting
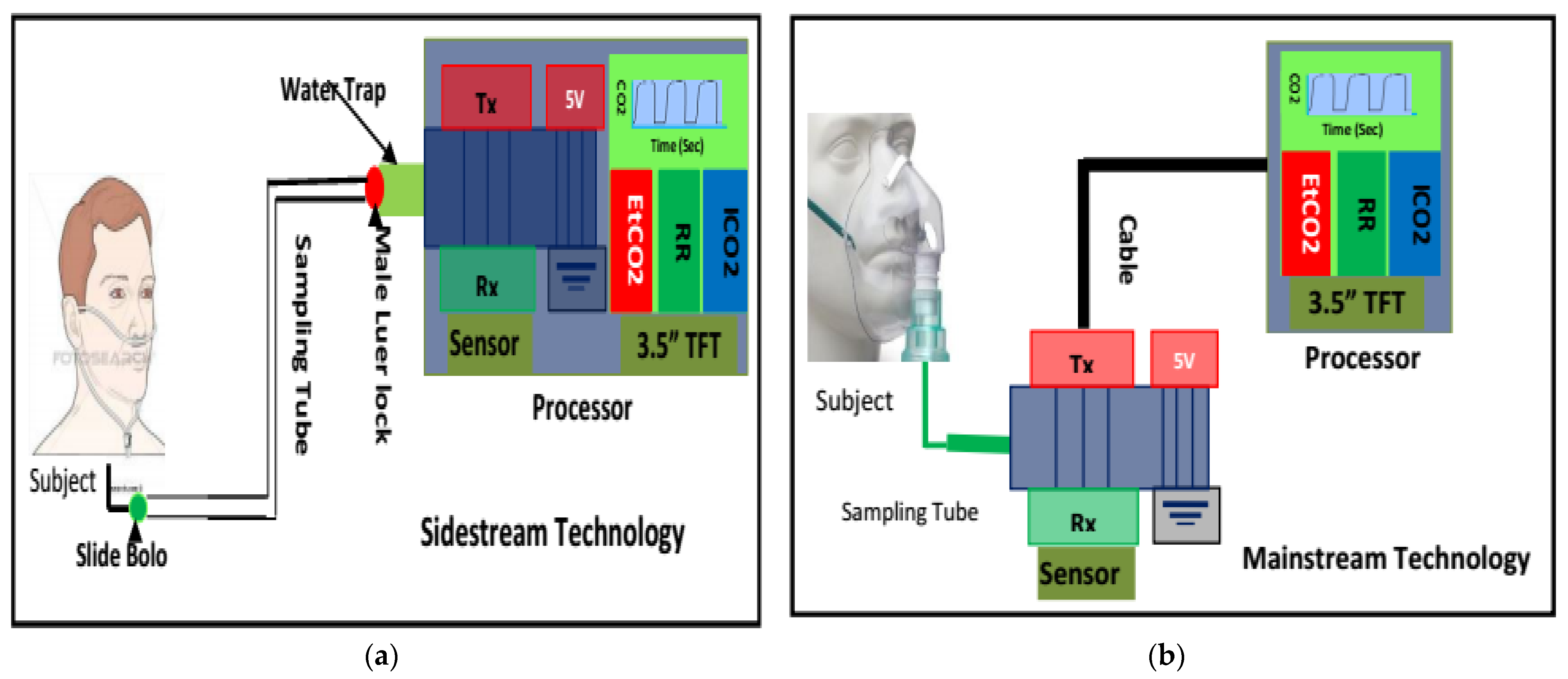
7.5.2. CO2 Data Acquisition
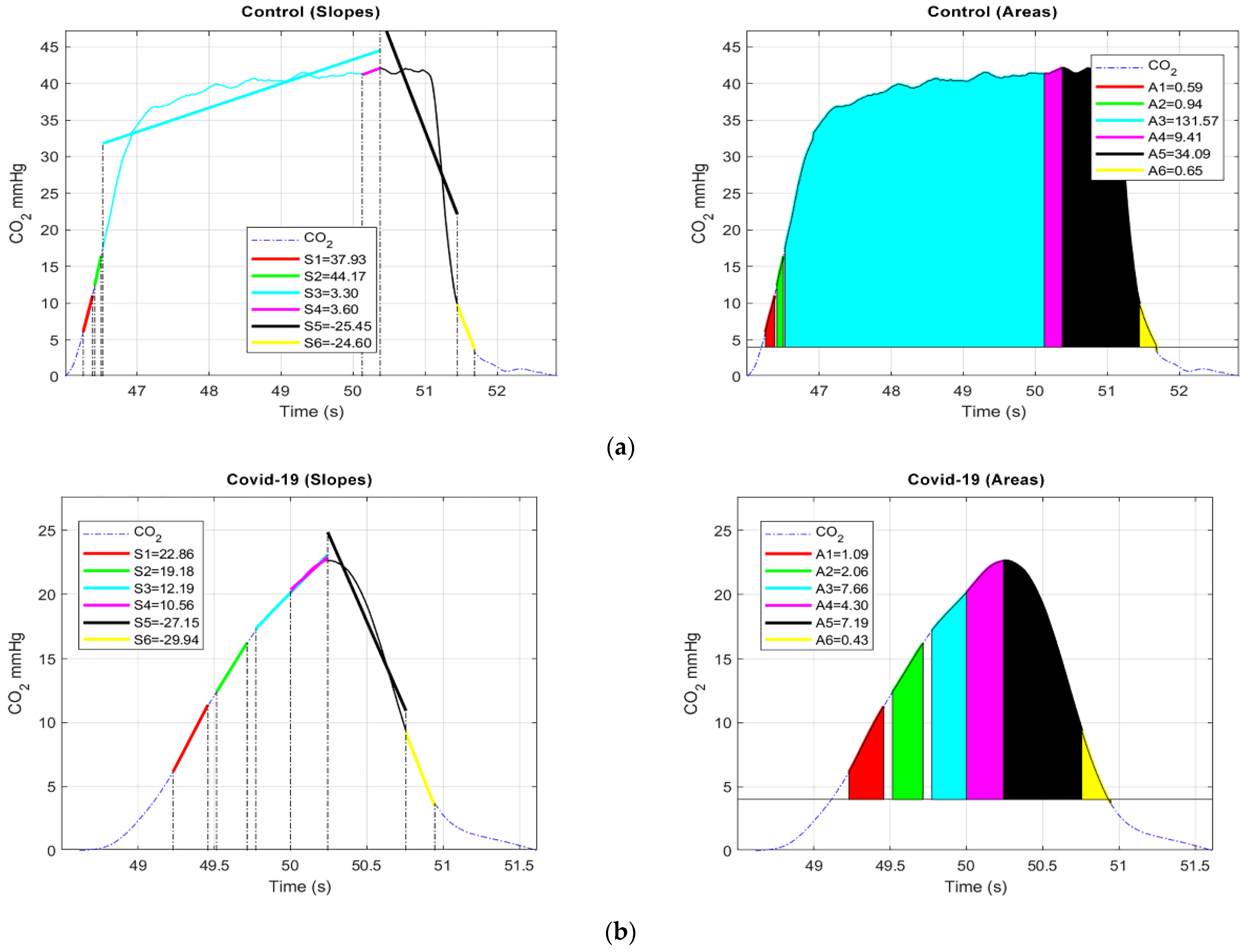
7.5.3. Signal Analysis
- (a)
- 1st sub-cycle: 6 mmHg (start) to 11 mmHg;
- (b)
- 2nd sub-cycle: 12 mmHg to 16 mmHg;
- (c)
- 3rd sub-cycle: 17 mmHg to EtCO2;
- (d)
- 4th sub-cycle: 0.25 s from EtCO2 to EtCO2;
- (e)
- 5th sub-cycle: EtCO2 to 10 mmHg;
- (f)
- 6th sub-cycle: 10 mmHg to 4 mmHg (baseline).
7.5.4. Results
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zu, Z.Y.; Jiang, M.D.; Xu, P.P.; Chen, W.; Ni, Q.Q.; Lu, G.M.; Zhang, L.J. Coronavirus disease 2019 (COVID-19): A perspective from China. Radiology 2020, 296, E15–E25. [Google Scholar] [CrossRef]
- Saif, L.; Wang, Q.; Vlasova, A.; Jung, K.; Xiao, S. Coronaviruses. In Diseases of Swine; John Wiley and Sons, Inc.: Hoboken, NJ, USA, 2019; pp. 488–529. [Google Scholar]
- Fehr, A.R.; Perlman, S. Coronaviruses: An overview of their replication and pathogenesis. Coronaviruses 2015, 1282, 1–23. [Google Scholar]
- Qian, Z.; Alaa, A.M.; van der Schaar, M.; Ercole, A. Between-centre differences for COVID-19 ICU mortality from early data in England. Intensive Care Med. 2020, 46, 1779–1780. [Google Scholar] [CrossRef]
- World Health Organization. Statement on the Second Meeting of the International Health Regulations (2005) Emergency Committee Regarding the Outbreak of Novel Coronavirus (2019-nCoV). Available online: https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov) (accessed on 28 April 2020).
- World Health Organization. Global Leaders Unite to Ensure Everyone Everywhere Can Access New Vaccines, Tests and Treatments for COVID-19. Available online: https://www.who.int/news-room/detail/24-04-2020-global-leaders-unite-to-ensure-everyone-everywhere-can-access-new-vaccines-tests-and-treatments-for-covid-19 (accessed on 28 April 2020).
- WHO. WHO Coronavirus Disease (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 4 February 2021).
- TheStar. COVID-19 Current Situation in Malaysia –Updated Daily. Available online: https://www.thestar.com.my/news/nation/2020/03/23/covid-19-current-situation-in-malaysia-updated-daily (accessed on 4 February 2021).
- Pan, L.; Mu, M.; Yang, P.; Sun, Y.; Wang, R.; Yan, J.; Li, P.; Hu, B.; Wang, J.; Hu, C. Clinical characteristics of COVID-19 patients with digestive symptoms in Hubei, China: A descriptive, cross-sectional, multicenter study. Am. J. Gastroenterol. Epub. 2020, 115, 766–773. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-19) Advice for the Public. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 29 April 2020).
- Liu, C.-C.; Chang, R.-E.; Chang, W.-C. Limitations of forehead infrared body temperature detection for fever screening for severe acute respiratory syndrome. Infect. Control Hosp. Epidemiol. 2004, 25, 1109–1111. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Zhong, Z.; Xie, X.; Yu, Q.; Liu, J. Relation between chest CT findings and clinical conditions of coronavirus disease (COVID-19) pneumonia: A multicenter study. Am. J. Roentgenol. 2020, 214, 1072–1077. [Google Scholar] [CrossRef]
- Infantino, M.; Damiani, A.; Gobbi, F.L.; Grossi, V.; Lari, B.; Macchia, D.; Casprini, P.; Veneziani, F.; Villalta, D.; Bizzaro, N. Serological assays for SARS-CoV-2 infectious disease: Benefits, limitations and perspectives. Isr. Med. Assoc. J. 2020, 22, 203–210. [Google Scholar]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K. Chest CT findings in coronavirus disease-19 (COVID-19): Relationship to duration of infection. Radiology 2020, 295, 3–20043. [Google Scholar] [CrossRef] [PubMed]
- Elengoe, A. COVID-19 outbreak in Malaysia. Osong Public Health Res. Perspect. 2020, 11, 93–100. [Google Scholar] [CrossRef]
- Astuti, I. Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2): An overview of viral structure and host response Diabetes Metab. Syndr. 2020, 14, 407–412. [Google Scholar] [CrossRef]
- Gorbalenya, A.E.; Baker, S.C.; Baric, R.S.; De Groot, R.J.; Drosten, C.; Gulyaeva, A.A.; Haagmans, B.L.; Lauber, C.; Leontovich, A.M.; Neuman, B.W.; et al. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. Available online: https://go.nature.com/3cW9qJR (accessed on 10 October 2021).
- Guo, Y.-R.; Cao, Q.-D.; Hong, Z.-S.; Tan, Y.-Y.; Chen, S.-D.; Jin, H.-J.; Tan, K.-S.; Wang, D.-Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak–an update on the status. Mil. Med Res. 2020, 7, 11. [Google Scholar] [CrossRef]
- Alanagreh, L.A.; Alzoughool, F.; Atoum, M. The human coronavirus disease COVID-19: Its origin, characteristics, and insights into potential drugs and its mechanisms. Pathogens 2020, 9, 331. [Google Scholar] [CrossRef] [PubMed]
- Sabino-Silva, R.; Jardim, A.C.G.; Siqueira, W.L. Coronavirus COVID-19 impacts to dentistry and potential salivary diagnosis. Clin. Oral. Investig. 2020, 24, 1619–1621. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.-H.; Cai, L.; Cheng, Z.-S.; Cheng, H.; Deng, T.; Fan, Y.-P.; Fang, C.; Huang, D.; Huang, L.-Q.; Huang, Q. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med Res. 2020, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Tian, S.; Hu, N.; Lou, J.; Chen, K.; Kang, X.; Xiang, Z.; Chen, H.; Wang, D.; Liu, N.; Liu, D. Characteristics of COVID-19 infection in Beijing. J. Infect. 2020, 80, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Wan, S.; Xiang, Y.; Fang, W.; Zheng, Y.; Li, B.; Hu, Y.; Lang, C.; Huang, D.; Sun, Q.; Xiong, Y. Clinical features and treatment of COVID-19 patients in northeast Chongqing. J. Med. Virol. 2020, 92, 797–806. [Google Scholar] [CrossRef]
- Chen, J.; Qi, T.; Liu, L.; Ling, Y.; Qian, Z.; Li, T.; Li, F.; Xu, Q.; Zhang, Y.; Xu, S. Clinical progression of patients with COVID-19 in Shanghai, China. J. Infect. 2020, 80, e1–e6. [Google Scholar] [CrossRef]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological findings and complications of COVID-19. Am. J. Hematol. Epub. 2020, 95, 834–847. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus–infected pneumonia in Wuhan, China. Jama 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Xie, C.; Jiang, L.; Huang, G.; Pu, H.; Gong, B.; Lin, H.; Ma, S.; Chen, X.; Long, B.; Si, G. Comparison of different samples for 2019 novel coronavirus detection by nucleic acid amplification tests. Int. J. Infect. Dis. 2020, 93, 264–267. [Google Scholar] [CrossRef] [PubMed]
- Dos Santos, W.G. Natural history of COVID-19 and current knowledge on treatment therapeutic options Biomed. Pharmacother. 2020, 129, 110493. [Google Scholar]
- Hafeez, A.; Ahmad, S.; Siddqui, S.A.; Ahmad, M.; Mishra, S. A review of COVID-19 (Coronavirus Disease-2019) diagnosis, treatments and prevention. EJMO 2020, 4, 116–125. [Google Scholar]
- Wu, Y.-C.; Chen, C.-S.; Chan, Y.-J. The outbreak of COVID-19: An overview. J. Chin. Med Assoc. 2020, 83, 217. [Google Scholar] [CrossRef] [PubMed]
- Rao, M.; Rashid, F.A.; Sabri, F.S.; Jamil, N.N.; Zain, R.; Hashim, R.; Amran, F.; Kok, H.T.; Samad, M.A.A.; Ahmad, N. Comparing Nasopharyngeal Swab and Early Morning Saliva for the Identification of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020, 72, e352–e356. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in different types of clinical specimens. Jama 2020, 323, 1843–1844. [Google Scholar] [CrossRef]
- Tahamtan, A.; Ardebili, A. Real-time RT-PCR in COVID-19 detection: Issues affecting the results. Expert Rev. Mol. Diagn. 2020, 20, 453–454. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Yang, Y.; Yang, M.; Shen, C.; Wang, F.; Yuan, J.; Li, J.; Zhang, M.; Wang, Z.; Xing, L.; Wei, J. Laboratory diagnosis and monitoring the viral shedding of 2019-nCoV infections. MedRxiv 2020, 1, 100061. [Google Scholar]
- Cheng, Z.; Lu, Y.; Cao, Q.; Qin, L.; Pan, Z.; Yan, F.; Yang, W. Clinical features and chest CT manifestations of coronavirus disease 2019 (COVID-19) in a single-center study in Shanghai, China. Am. J. Roentgenol. 2020, 215, 121–126. [Google Scholar] [CrossRef]
- Corman, V.M.; Landt, O.; Kaiser, M.; Molenkamp, R.; Meijer, A.; Chu, D.K.; Bleicker, T.; Brünink, S.; Schneider, J.; Schmidt, M.L. Detection of 2019 novel coronavirus (2019-nCoV) by real-time RT-PCR. Eurosurveillance 2020, 25, 2000045. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. CDC 2019-Novel Coronavirus (2019-nCoV) Real-Time RT-PCR Diagnostic Panel. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/rt-pcr-panel-primer-probes.html (accessed on 4 August 2021.).
- Chang, M.C.; Hur, J.; Park, D. Interpreting the COVID-19 test results: A guide for physiatrists. Am. J. Phys. Med. Rehabil. PubMed. 2020, 99, 583–585. [Google Scholar] [CrossRef] [PubMed]
- Afzal, A. Molecular diagnostic technologies for COVID-19: Limitations and challenges. J. Adv. Res. Epub. 2020, 26, 149–159. [Google Scholar] [CrossRef]
- FDA. Coronavirus (COVID-19) Update: FDA Authorizes First Antigen Test to Help in the Rapid Detection of the Virus That Causes COVID-19 in Patients. Available online: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-authorizes-first-antigen-test-help-rapid-detection-virus-causes (accessed on 22 June 2020).
- Mak, G.C.; Cheng, P.K.; Lau, S.S.; Wong, K.K.; Lau, C.; Lam, E.T.; Chan, R.C.; Tsang, D.N. Evaluation of rapid antigen test for detection of SARS-CoV-2 virus. J. Clin. Virol. 2020, 129, 104500. [Google Scholar] [CrossRef]
- News Medical. Developing a COVID-19 Antigen Test. News Medical. Available online: https://www.news-medical.net/news/20200515/Developing-a-COVID-19-Antigen-Test.aspx (accessed on 15 May 2021).
- Mahapatra, S.; Chandra, P. Clinically practiced and commercially viable nanobio engineered analytical methods for COVID-19 diagnosis. Biosens. Bioelectron. 2020, 165, 112361. [Google Scholar] [CrossRef]
- Mertens, P.; De Vos, N.; Martiny, D.; Jassoy, C.; Mirazimi, A.; Cuypers, L.; Van den Wijngaert, S.; Monteil, V.; Melin, P.; Stoffels, K. Development and potential usefulness of the COVID-19 Ag Respi-Strip diagnostic assay in a pandemic context. Front. Med. 2020, 7, 225. [Google Scholar] [CrossRef]
- Scohy, A.; Anantharajah, A.; Bodéus, M.; Kabamba-Mukadi, B.; Verroken, A.; Rodriguez-Villalobos, H. Low performance of rapid antigen detection test as frontline testing for COVID-19 diagnosis. J. Clin. Virol. 2020, 129, 104455. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Yi, Y.; Luo, X.; Xiong, N.; Liu, Y.; Li, S.; Sun, R.; Wang, Y.; Hu, B.; Chen, W. Development and clinical application of a rapid IgM-IgG combined antibody test for SARS-CoV-2 infection diagnosis. J. Med Virol. 2020, 92, 1518–1524. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.-W.; Tsang, O.T.-Y.; Leung, W.-S.; Tam, A.R.; Wu, T.-C.; Lung, D.C.; Yip, C.C.-Y.; Cai, J.-P.; Chan, J.M.-C.; Chik, T.S.-H. Temporal profiles of viral load in posterior oropharyngeal saliva samples and serum antibody responses during infection by SARS-CoV-2: An observational cohort study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef]
- Zhao, J.; Yuan, Q.; Wang, H.; Liu, W.; Liao, X.; Su, Y.; Wang, X.; Yuan, J.; Li, T.; Li, J. Antibody responses to SARS-CoV-2 in patients of novel coronavirus disease 2019. Clin. Infect. Dis. 2020, 71, 2027–2034. [Google Scholar] [CrossRef]
- Guo, L.; Ren, L.; Yang, S.; Xiao, M.; Chang, D.; Yang, F.; Dela Cruz, C.S.; Wang, Y.; Wu, C.; Xiao, Y. Profiling early humoral response to diagnose novel coronavirus disease (COVID-19). Clin. Infect. Dis. 2020, 71, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Schildgen, V.; Demuth, S.; Lüsebrink, J.; Schildgen, O. Limits and Opportunities of SARS-CoV-2 Antigen Rapid Tests: An Experienced-Based Perspective. Pathogens 2021, 10, 38. [Google Scholar] [CrossRef]
- Ye, Z.; Zhang, Y.; Wang, Y.; Huang, Z.; Song, B. Chest CT manifestations of new coronavirus disease 2019 (COVID-19): A pictorial review. Eur. Radiol. 2020, 30, 4381–4389. [Google Scholar] [CrossRef]
- Li, K.; Wu, J.; Wu, F.; Guo, D.; Chen, L.; Fang, Z.; Li, C. The clinical and chest CT features associated with severe and critical COVID-19 pneumonia. Investig. Radiol. PubMed. 2020, 55, 327–331. [Google Scholar] [CrossRef]
- Wu, J.; Wu, X.; Zeng, W.; Guo, D.; Fang, Z.; Chen, L.; Huang, H.; Li, C. Chest CT findings in patients with coronavirus disease 2019 and its relationship with clinical features. Investig. Radiol. 2020, 55, 257–261. [Google Scholar] [CrossRef]
- Chung, M.; Bernheim, A.; Mei, X.; Zhang, N.; Huang, M.; Zeng, X.; Cui, J.; Xu, W.; Yang, Y.; Fayad, Z.A. CT imaging features of 2019 novel coronavirus (2019-nCoV). Radiology 2020, 295, 202–207. [Google Scholar] [CrossRef]
- He, J.-L.; Luo, L.; Luo, Z.-D.; Lyu, J.-X.; Ng, M.-Y.; Shen, X.-P.; Wen, Z. Diagnostic performance between CT and initial real-time RT-PCR for clinically suspected 2019 coronavirus disease (COVID-19) patients outside Wuhan, China. Respir. Med. 2020, 168, 105980. [Google Scholar] [CrossRef]
- Wilder-Smith, A.; Chiew, C.J.; Lee, V.J. Can we contain the COVID-19 outbreak with the same measures as for SARS? Lancet Infect. Dis. 2020, 20, e102–e107. [Google Scholar] [CrossRef]
- Petrosillo, N.; Viceconte, G.; Ergonul, O.; Ippolito, G.; Petersen, E. COVID-19, SARS and MERS: Are they closely related? Clin. Microbiol. Infect. 2020, 26, 729–734. [Google Scholar] [CrossRef]
- Tay, M.; Low, Y.; Zhao, X.; Cook, A.; Lee, V. Comparison of infrared thermal detection systems for mass fever screening in a tropical healthcare setting. Public Health 2015, 129, 1471–1478. [Google Scholar] [CrossRef] [PubMed]
- Aw, J. The non-contact handheld cutaneous infra-red thermometer for fever screening during the COVID-19 global emergency. J. Hosp. Infect. 2020, 104, 451. [Google Scholar] [CrossRef] [PubMed]
- Gold, L.; Balal, E.; Horak, T.; Cheu, R.L.; Mehmetoglu, T.; Gurbuz, O. Health screening strategies for international air travelers during an epidemic or pandemic. J. Air Transp. Manag. 2019, 75, 27–38. [Google Scholar] [CrossRef] [PubMed]
- Food and Drug Administration. Thermal Imaging Systems (Infrared Thermographic Systems/Thermal Imaging Cameras). Available online: https://www.fda.gov/medical-devices/general-hospital-devices-and-supplies/thermal-imaging-systems-infrared-thermographic-systems-thermal-imaging-cameras (accessed on 26 June 2020).
- Techcrunch. Chinese Startup Rokid Pitches COVID-19 Detection Glasses in US. Available online: https://techcrunch.com/2020/04/16/chinese-startup-rokid-pitches-covid-19-detection-glasses-in-u-s/?guccounter=1&guce_referrer=aHR0cHM6Ly9jc2UuZ29vZ2xlLmNvbS9jc2U_cT10aGVybWFsK2ltYWdpbmcrc3lzdGVtcyZzYT1TZWFyY2gmaWU9VVRGLTgmY3g9cGFydG5lciUyRHB1YiUyRDY2MzgyNDc3Nzk0MzM2OTAlM0EzODczMzg0OTkx&guce_referrer_sig=AQAAAJQqc0ni3gq0PLU4OJISavwkMKZKQa3I0iwAzOnOHhyQ0bz-2RFTHnDufbqoJxr969_V4eQ6Tk5tGhhS86qNuJnc9-x3EHjigfzBSSYmFr4J0DOr0rJO_A_it3QgessBCFizYvptC4FL5k2jNu7n3ZV9jbsxdl4rvp0AwUFE9gij (accessed on 16 April 2020).
- Lab manager. Thermal Sensor Screens for Skin Temperatures to Monitor COVID-19. Available online: https://www.labmanager.com/product-news/thermal-sensor-screens-for-skin-temperatures-22355 (accessed on 16 April 2020).
- Guyton, C.A.; Hall, E.J. Medical Physiology, 11th ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2006. [Google Scholar]
- Colman, Y.; Krauss, B. Micro-stream Capnography Technology: A new approach to an old problem. J. Clin. Monit. Comput. 2003, 19, 403–409. [Google Scholar]
- Pekdemir, M.; Cinar, O.; Yilmaz, S.; Yaka, E.; Yuksel, M. Disparity between mainstream and sidestream end-tidal carbon dioxide values and arterial carbon dioxide levels. Respir. Care 2013, 58, 1152–1156. [Google Scholar] [CrossRef]
- Elam, J.; Brown, E.S. Carbon Dioxide Homeostasis during Anesthesia Ventilation and Carbon Dioxide Elimination. Anesthesiol. J. 2001, 18, 115–127. [Google Scholar] [CrossRef]
- Conway, A.; Collins, P.; Chang, K.; Mafeld, S.; Sutherland, J.; Fingleton, J. Sequence analysis of capnography waveform abnormalities during nurse-administered procedural sedation and analgesia in the cardiac catheterization laboratory. Sci. Rep. 2019, 9, 10214. [Google Scholar] [CrossRef]
- Williams, E.; Dassios, T.; Greenough, A. Assessment of sidestream end-tidal capnography in ventilated infants on the neonatal unit. Pediatric Pulmonol. 2020, 55, 1468–1473. [Google Scholar] [CrossRef]
- Takimoto, Y.; Iwasaki, E.; Masaoka, T.; Fukuhara, S.; Kawasaki, S.; Seino, T.; Katayama, T.; Minami, K.; Tamagawa, H.; Machida, Y.; et al. Novel mainstream capnometer system is safe and feasible even under CO2 insufflation during ERCP-related procedure: A pilot study. BMJ Open Gastroenterol. 2019, 6, 1–5. [Google Scholar] [CrossRef]
- Zelikova, T.J. The future of carbon dioxide removal must be transdisciplinary. Interface Focus. The Royal Society Publishing. 2020, 10, 2042–8901. [Google Scholar] [CrossRef]
- Verscheure, S.; Massion, P.B.; Verschuren, F.; Damas, P.; Magder, S. Volumetric capnography: Lessons from the past and current clinical applications. Crit. Care 2016, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Abid, A.; Mieloszyk, R.J.; Verghese, G.C.; Krauss, B.S.; Heldt, T. Model-based estimation of respiratory parameters from capnography, with application to diagnosing obstructive lung disease. IEEE Trans. Biomed. Eng. 2017, 64, 2957–2967. [Google Scholar] [PubMed]
- Rhoades, C.; Thomas, F. Capnography: Beyond the numbers. Air Med. J. 2002, 21, 43–48. [Google Scholar] [CrossRef]
- Long, B.; Koyfman, A.; Vivirito, M.A. Capnography in the Emergency Department: A Review of Uses, Waveforms, and Limitations. J. Emerg. Med. 2017, 53, 829–842. [Google Scholar] [CrossRef]
- Manifold, C.A.; Davids, N.; Villers, L.C.; Wampler, D.A. Capnography for the nonintubated patient in the emergency setting. J. Emerg. Med. 2013, 45, 626–632. [Google Scholar] [CrossRef]
- Smalhout, B.; Kalenda, Z. An Atlas of Capnography, 2nd ed.; Kerckebosche Zeist Press: Kerckebosche Zeist, The Netherlands, 1981; Available online: https://www.worldcat.org/title/atlas-of-capnography-1-1981-222-s-graph-darst/oclc/632907943?referer=di&ht=edition (accessed on 10 October 2021).
- Jaffe, M.B.; Orr, J. Continuous monitoring of respiratory flow and Co2. IEEE Eng. Med. Biol. Mag. 2010, 29, 44–52. [Google Scholar] [CrossRef]
- Howe, T.A.; Jaalam, K.; Ahmad, R.; Sheng, C.K.; Ab Rahman, N.H.N. The use of end-tidal capnography to monitor non-intubated patients presenting with acute exacerbation of asthma in the emergency department. J. Emerg. Med. 2011, 41, 581–589. [Google Scholar] [CrossRef]
- Mieloszyk, R.J.; Verghese, G.C.; Deitch, K.; Cooney, B.; Khalid, A.; Mirre-González, M.A.; Heldt, T.; Krauss, B.S. Automated quantitative analysis of capnogram shape for COPD–normal and COPD–CHF classification. IEEE Trans. Biomed. Eng. 2014, 61, 2882–2890. [Google Scholar] [CrossRef]
- You, B.; Peslin, R.; Duvivier, C.; Vu, V.D.; Grilliat, J. Expiratory capnography in asthma: Evaluation of various shape indices. Eur. Respir. J. 1994, 7, 318–323. [Google Scholar] [CrossRef]
- El-Badawy, I.M.; Singh, O.P.; Omar, Z. Automatic classification of regular and irregular capnogram segments using time-and frequency-domain features: A machine learning-based approach. Technol. Health Care 2020, 29, 59–72. [Google Scholar] [CrossRef] [PubMed]
- Betancourt, J.P.; Tangel, M.L.; Yan, F.; Diaz, M.O.; Otaño, A.E.P.; Dong, F.; Hirota, K. Segmented wavelet decomposition for capnogram feature extraction in asthma classification. J. Adv. Comput. Intell. Intell. Inform. 2014, 18, 480–488. [Google Scholar] [CrossRef]
- Hisamuddin, N.N.; Rashidi, A.; Chew, K.; Kamaruddin, J.; Idzwan, Z.; Teo, A. Correlations between capnographic waveforms and peak flow meter measurement in emergency department management of asthma. Int. J. Emerg. Med. 2009, 2, 83–89. [Google Scholar] [CrossRef] [PubMed]
- Kean, T.T.; Malarvili, M. Analysis of capnography for asthmatic patient. Proceedings of 2009 IEEE International Conference on Signal and Image Processing Applications, Kuala Lumpur, Malaysia, 18–19 November 2009; pp. 464–467. [Google Scholar]
- Doğan, N.Ö.; Şener, A.; Günaydın, G.P.; İçme, F.; Çelik, G.K.; Kavaklı, H.Ş.; Temrel, T.A. The accuracy of mainstream end-tidal carbon dioxide levels to predict the severity of chronic obstructive pulmonary disease exacerbations presented to the ED. Am. J. Emerg. Med. 2014, 32, 408–411. [Google Scholar] [CrossRef] [PubMed]
- Herry, C.L.; Townsend, D.; Green, G.C.; Bravi, A.; Seely, A.J.E. Segmentation and classification of capnograms: Application in respiratory variability analysis. Physiol. Meas. 2014, 35, 2343. [Google Scholar] [CrossRef]
- Singh, O.P.; Palaniappan, R.; Malarvili, M.B. Automatic Quantitative Analysis of Human Respired Carbon Dioxide Waveform for Asthma and Non-Asthma Classification Using Support Vector Machine. IEEE Access 2018, 6, 55245–55256. [Google Scholar] [CrossRef]
- Yaron, M.; Padyk, P.; Hutsinpiller, M.; Cairns, C.B. Utility of the expiratory capnogram in the assessment of bronchospasm. Ann. Emerg. Med. 1996, 28, 403–407. [Google Scholar] [CrossRef]
- Singh, O.P.; Howe, T.A.; Malarvili, M.B. Real-time human respiration carbon dioxide measurement device for cardiorespiratory assessmen. J. Breath Res. 2018, 12, 026003. [Google Scholar] [CrossRef]
- Asher, R.J.; Heldt, T.; Verghese, G.C.; Krauss, B.S. System and Methods for Quantitative Capnogram. Analysis. U.S. Patent Application No. 13/849, 2014, 284.
- Yao, X.; Li, T.; He, Z.; Ping, Y.; Liu, H.; Yu, S.; Mou, H.; Wang, L.; Zhang, H.; Fu, W. A pathological report of three COVID-19 cases by minimally invasive autopsies. Zhonghua Bing Li Xue Za Zhi Chin. J. Pathol. 2020, 49, 411–417. [Google Scholar]
- Jonson, B. Volumetric capnography for noninvasive monitoring of acute respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 2018, 198, 396–398. [Google Scholar] [CrossRef]
- Matthay, M.A.; Zemans, R.L.; Zimmerman, G.A.; Arabi, Y.M.; Beitler, J.R.; Mercat, A.; Herridge, M.; Randolph, A.G.; Calfee, C.S. Acute respiratory distress syndrome. Nat. Rev. Dis. Primers 2019, 5, 18. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Miao, J.H.; Yetiskul, E.; Anokhin, A.; Majmundar, S.H. Physiology, Carbon Dioxide Retention; StatPearls: Treasure Island, FL, USA, 2018. [Google Scholar]
- Hu, D.; Li, J.; Gao, R.; Wang, S.; Li, Q.; Chen, S.; Huang, J.; Huang, Y.; Li, M.; Long, W. Decreased CO2 Levels as Indicators of Possible Mechanical Ventilation-Induced Hyperventilation in COVID-19 Patients: A Retrospective Analysis. Front. Public Health 2021, 8, 912. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, G. What to Know about the CO2 Blood Test. Available online: https://www.medicalnewstoday.com/articles/325259 (accessed on 28 April 2021).
- Castro, D.; Patil, S.M.; Keenaghan, M. Arterial Blood Gas; StatPearls: Treasure Island, FL, USA, 2021. [Google Scholar]
- Rosner, B. Fundamentals of Biostatistics, 5th ed.; Duxbury Thomson Learning: Pacific Grove, CA, USA, 2000. [Google Scholar]
- Shapiro, S.S.; Wilk, M.B. An Analysis of Variance Test for Normality (Complete Samaples); Oxford University Press: Oxford, UK, 1965; Volume 52. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Disease | Feature | Classifier | Performance Measure (Accuracy, Sensitivity, Specificity)/AUC | Limitations |
|---|---|---|---|---|---|
| You, B. et al. [84] | Asthma | S1, S2, S3, SR, A1 A2, SD1, SD2, SD3 | - | p < 0.001 in all indices | Real-time implementation is still challenging due to the random time-based setting criteria |
| Hisamuddin et al. [87] | Asthma | Slope of phase 2, slope of phase 3, α angle | - | Angle α: p < 0.001 slope of phase 3: p < 0.001 slope of phase 2: p = 0.35 | Selection bias of waveform for analysis |
| Kean et al. [88] | Asthma | Area (A1) and (A2), area ratio (AR), S1 and S2 (Slope), SR (slope ratio), α angle, HP1 and HP2 (activity), HP1 and HP2 (mobility), HP1 and HP2 (complexity) | - | p < 0.0001 (SR) p = 0.0001051 (HP2 mobility) | Capnogram features were extracted manually |
| Betancourt et al. [86] | Asthma | Wavelet coefficients | Support vector machine | sensitivity: 55.71%, specificity: 99.38%, | Improper prediction of asthma severity degree 1 |
| Doğan, Nurettin Özgür et al. [89] | COPD | EtCO2 | - | sensitivity: 65.2% specificity: 63.6% | Small sample size The mean bias of the study was 4.68 ± 7.21 |
| Mieloszyk et al. [83] | COPD, CHF, normal subject | Exhalation duration, Pet CO2, time spent at Pet CO2, exhalation slope | Quadratic discriminant analysis | Accuracy: 93.9%, for COPD/normal classification Accuracy: 80.0%, for COPD/CHF classification | Inability of tracking changes in disease severity and response to treatment over time Some patients presented with a mixed picture of CHF and COPD |
| Herry, C. L et al. [90] | Breath classification (normal or abnormal) in intubated patients in ICU | Plateau slope, residuals, TO angle, α angle, β angle, PeakCO2, SR1, min plateau, skew, kurtosis, inspiration slope, expiration slope, width, sharpness, MinCO2 | Decision tree (DT), k-nearest neighbors (KNN), and naive Bayes (NB) | AUC: 90% (DT) AUC: 89%(KNN) AUC: 88%(NB) | The type of abnormalities was not classified |
| Singh, O. P., Palaniappan, R., and Malarvili, M. B. [91] | Asthma | Upward expiration (AR1), downward inspiration (AR2), and the sum of AR1 and AR2 | Support vector machine (SVM) k-nearest neighbor (k-NN) and naive Bayes (NB) | Average accuracy of 94.52%, sensitivity of 97.67%, and specificity of 90% | - |
| El-Badawy, I. M., Singh, O. P., and Omar, Z. [85] | Differentiation of regular and irregular capnograms | Energy, variance, skewness and kurtosis, number of relatively high spectral peaks and the area under the normalized magnitude spectrum | Support vector machine | accuracy: 86.5% specificity: 84% sensitivity: 89% precision: 86.51% | On average, 13.5% of the capnogram segments were misclassified due to the overlap between some regular and irregular capnogram samples |
| S. No. | Segmented Sub-Cycles | Features | p-Value |
|---|---|---|---|
| 1 | 6–11 mmHg | A1 | 0.05 |
| S1 | 0.003 | ||
| 2 | 12–16 mmHg | A2 | 0.01 |
| S2 | 0.002 | ||
| 3 | 17 mmHg–EtCO2 | A3 | 0.001 |
| S3 | 0.08 | ||
| 4 | 0.25 s from EtCO2 to EtCO2 | A4 | 0.07 |
| S4 | 0.05 | ||
| 5 | EtCO2–10 mmHg | A5 | 0.07 |
| S5 | 0.01 | ||
| 6 | 10 mmHg–4 mmHg | A6 | 0.09 |
| S6 | 0.08 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malarvili, M.B.; Alexie, M.; Dahari, N.; Kamarudin, A. On Analyzing Capnogram as a Novel Method for Screening COVID-19: A Review on Assessment Methods for COVID-19. Life 2021, 11, 1101. https://doi.org/10.3390/life11101101
Malarvili MB, Alexie M, Dahari N, Kamarudin A. On Analyzing Capnogram as a Novel Method for Screening COVID-19: A Review on Assessment Methods for COVID-19. Life. 2021; 11(10):1101. https://doi.org/10.3390/life11101101
Chicago/Turabian StyleMalarvili, M. B., Mushikiwabeza Alexie, Nadhira Dahari, and Anhar Kamarudin. 2021. "On Analyzing Capnogram as a Novel Method for Screening COVID-19: A Review on Assessment Methods for COVID-19" Life 11, no. 10: 1101. https://doi.org/10.3390/life11101101
APA StyleMalarvili, M. B., Alexie, M., Dahari, N., & Kamarudin, A. (2021). On Analyzing Capnogram as a Novel Method for Screening COVID-19: A Review on Assessment Methods for COVID-19. Life, 11(10), 1101. https://doi.org/10.3390/life11101101