
Myelin Oligodendrocyte Glycoprotein-Antibody Associated Disease: An Updated Review of the Clinical Spectrum, Pathogenetic Mechanisms and Therapeutic Management



Abstract
1. Introduction
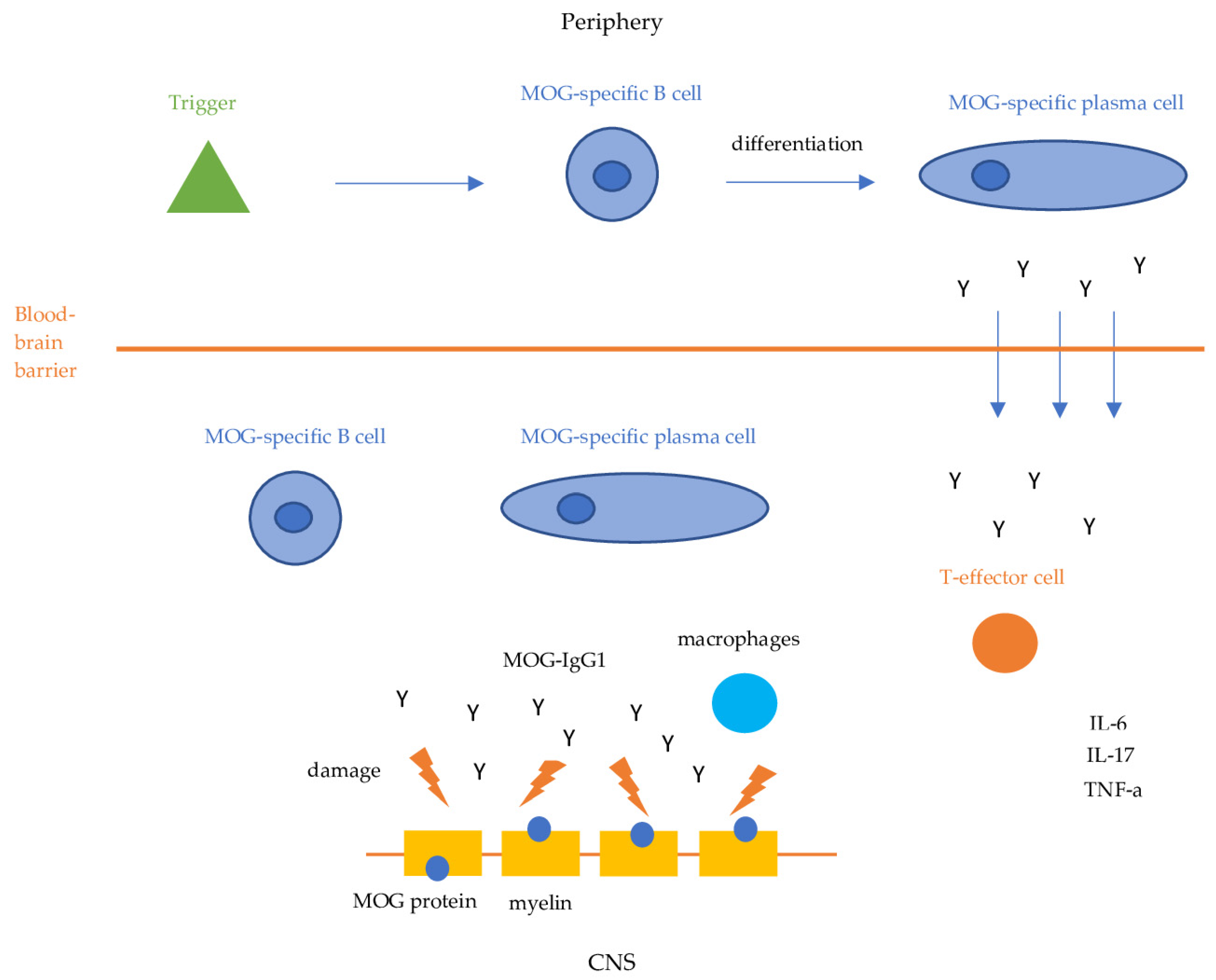
2. Pathogenesis
3. Clinical Spectrum
3.1. Frequency and Demographics
3.2. Clinical Syndromes
3.2.1. Optic Neuritis
3.2.2. Transverse Myelitis
3.2.3. ADEM
3.2.4. Fluid Attenuated Inversion Recovery (FLAIR)-Hyperintense Lesions in Anti-MOG-Associated Encephalitis with Seizures (FLAMES)
3.2.5. MOGAD and N-Methyl-D-Aspartate-Receptor (NMDAR) Encephalitis Overlap
3.2.6. Other Demyelinating Syndromes
4. Imaging Characteristics and Biochemical Biomarkers
4.1. Imaging Studies
4.2. Biomarkers
5. Diagnostic Criteria
6. Disease Course and Prognosis
7. MOGAD and Pregnancy
8. Treatment
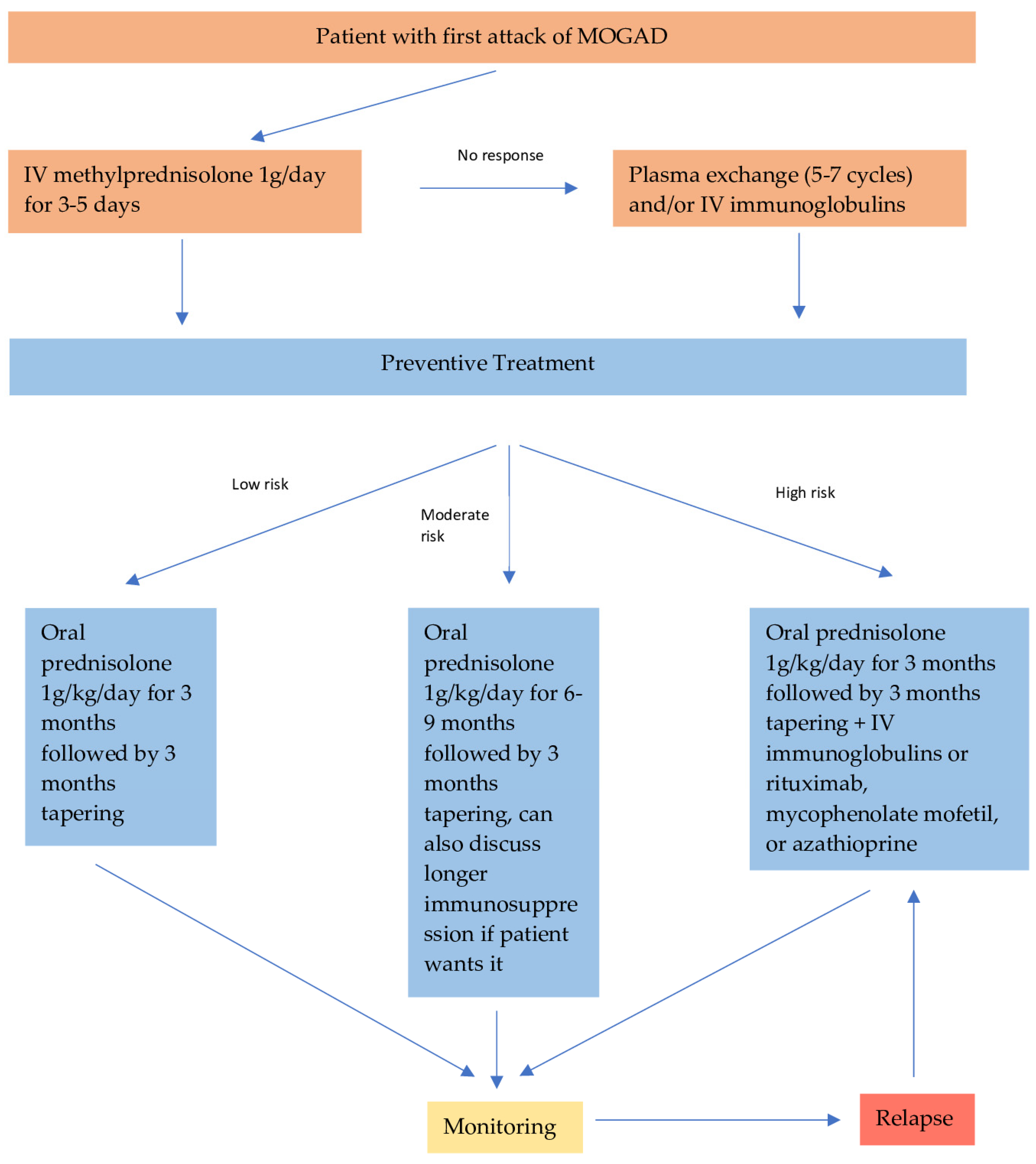
8.1. Acute Treatment
8.2. Preventive Treatment
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schluesener, H.; Sobel, R.A.; Linington, C.; Weiner, H.L. A monoclonal antibody against a myelin oligodendrocyte glycoprotein induces relapses and demyelination in central nervous system autoimmune disease. J. Immunol. 1987, 139, 4016–4021. [Google Scholar] [CrossRef] [PubMed]
- Reindl, M.; Di Pauli, F.; Rostásy, K.; Berger, T. The spectrum of MOG autoantibody-associated demyelinating diseases. Nat. Rev. Neurol. 2013, 9, 455–461. [Google Scholar] [CrossRef]
- Johns, T.G.; Bernard, C.C. The structure and function of myelin oligodendrocyte glycoprotein. J. Neurochem. 1999, 72, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Hemmer, B.; Archelos, J.J.; Hartung, H.P. New concepts in the immunopathogenesis of multiple sclerosis. Nat. Rev. Neurosci. 2002, 3, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Cobo-Calvo, A.; Ruiz, A.; Maillart, E.; Audoin, B.; Zephir, H.; Bourre, B.; Ciron, J.; Collongues, N.; Brassat, D.; Cotton, F.; et al. Clinical spectrum and prognostic value of CNS MOG autoimmunity in adults: The MOGADOR study. Neurology 2018, 90, e1858–e1869. [Google Scholar] [CrossRef]
- Hacohen, Y.; Mankad, K.; Chong, W.K.; Barkhoff, F.; Vincent, A.; Lim, M.; Wassmer, E.; Ciccarelli, O.; Hemingway, C. Diagnostic algorithm for relapsing acquired demyelinating syndromes in children. Neurology 2017, 89, 269–278. [Google Scholar] [CrossRef] [PubMed]
- Flach, A.C.; Litke, T.; Strauss, J.; Haberl, M.; Gomez, C.C.; Reindl, M.; Saiz, A.; Fehling, H.J.; Wienands, H.; Odoardi, F.; et al. Autoantibody-boosted T-cell reactivation in the target organ triggers manifestation of autoimmune CNS disease. Proc. Natl. Acad. Sci. USA 2016, 113, 3323–3328. [Google Scholar] [CrossRef] [PubMed]
- Kinzel, S.; Lehmann-Horn, K.; Torke, S.; Hausler, D.; Winkler, A.; Stadelmann, C.; Payne, N.; Feldmann, L.; Saiz, A.; Reindl, M.; et al. Myelin-reactive antibodies initiate T cell-mediated CNS autoimmune disease by opsonization of endogenous antigen. Acta Neuropathol. 2016, 132, 43–58. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, K.; Sato, D.K.; Nakashima, I.; Ogawa, R.; Akaishi, T.; Takai, Y.; Nishiyama, S.; Takahashi, T.; Misu, T.; Kuroda, H.; et al. CSF cytokine profile in MOG-IgG+ neurological disease is similar to AQP4-IgG+ NMOSD but distinct from MS: A cross-sectional study and potential therapeutic implications. J. Neurol. Neurosurg. Psychiatry 2018, 89, 927–936. [Google Scholar] [CrossRef] [PubMed]
- Mariotto, S.; Gajofatto, A.; Batzu, L.; Delogu, R.; Sechi, R.; Leoni, S.; Pirastru, M.I.; Bonetti, B.; Zanoni, M.; Alberti, D.; et al. Relevance of antibodies to myelin oligodendrocyte glycoprotein in CSF of seronegative cases. Neurology 2019, 93, e1867–e1872. [Google Scholar]
- Spadaro, M.; Winklmeier, S.; Beltrán, E.; Macrini, C.; Hoftberger, R.; Schuh, E.; Thaler, F.S.; Gerdes, L.A.; Laurent, S.; Gerhards , R.; et al. Pathogenicity of human antibodies against myelin oligodendrocyte glycoprotein. Ann. Neurol. 2018, 84, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Takai, Y.; Misu, T.; Kaneko, K.; Chihara, N.; Narikawa, K.; Tsuchida, S.; Nishida, H.; Komori, T.; Seki, M.; Komatsu, T.; et al. Myelin oligodendrocyte glycoprotein antibody-associated disease: An immunopathological study. Brain 2020, 143, 1431–1446. [Google Scholar] [CrossRef] [PubMed]
- Mariotto, S.; Ferrari, S.; Monaco, S.; Benedetti, M.D.; Schanda, K.; Alberti, D.; Farinazzo, A.; Capra, R.; Mancinelli, C.; De Rossi, N.; et al. Clinical spectrum and IgG subclass analysis of anti-myelin oligodendrocyte glycoprotein antibody-associated syndromes: A multicenter study. J. Neurol. 2017, 264, 2420–2430. [Google Scholar] [CrossRef] [PubMed]
- Ramanathan, S.; Mohammad, S.; Tantsis, E.; Nguyen, T.K.; Merheb, V.; Fung, V.S.C.; White, O.B.; Broadley, S.; Lechner-Scott, J.; Vucic, S.; et al. Clinical course, therapeutic responses and outcomes in relapsing MOG antibody-associated demyelination. J. Neurol. Neurosurg. Psychiatry 2018, 89, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Marignier, R.; Hacohen, Y.; Cobo-Calvo, A.; Pröbstel, A.K.; Aktas, O.; Alexopoulos, H.; Amato, M.P.; Asgari, N.; Banwell, B.; Bennett, J.; et al. Myelin-oligodendrocyte glycoprotein antibody-associated disease. Lancet Neurol. 2021, 20, 762–772, Erratum in Lancet Neurol. 2021, 20, e6; Erratum in Lancet Neurol. 2022, 21, e1. [Google Scholar] [CrossRef] [PubMed]
- Hor, J.Y.; Fujihara, K. Epidemiology of myelin oligodendrocyte glycoprotein antibody-associated disease: A review of prevalence and incidence worldwide. Front. Neurol. 2023, 14, 1260358. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sechi, E.; Cacciaguerra, L.; Chen, J.J.; Mariotto, S.; Fadda, G.; Dinoto, A.; Lopez-Chiriboga, A.S.; Pittock, S.J.; Flanagan, E.P. Myelin Oligodendrocyte Glycoprotein Antibody-Associated Disease (MOGAD): A Review of Clinical and MRI Features, Diagnosis, and Management. Front. Neurol. 2022, 13, 885218. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Flanagan, E.P.; Cabre, P.; Weinshenker, B.G.; Sauver, J.S.; Jacobson, D.J.; Majed, M.; Lennon, V.A.; Lucchinetti, C.F.; McKeon, A.; Matiello, M. Epidemiology of aquaporin-4 autoimmunity and neuromyelitis optica spectrum. Ann. Neurol. 2016, 79, 775–783. [Google Scholar] [CrossRef] [PubMed]
- De Mol, C.L.; Wong, Y.Y.M.; Van Pelt, E.D.; Wokke, B.H.A.; Siepman, T.A.M.; Neuteboom, R.F.; Hamann, D.; Hintzen, R.Q. The clinical spectrum and incidence of anti-MOG-associated acquired demyelinating syndromes in children and adults. Mult. Scler. 2020, 26, 806–814. [Google Scholar] [CrossRef]
- Sepúlveda, M.; Aldea, M.; Escudero, D.; Llufriu, S.; Arrambide, G.; Otero-Romero, S.; Sastre-Garriga, J.; Romero-Pinel, L.; Martínez-Yélamos, S.; Sola-Valls, N.; et al. Epidemiology of NMOSD in Catalonia: Influence of the new 2015 criteria in incidence and prevalence estimates. Mult. Scler. 2017, 24, 1843–1851. [Google Scholar] [CrossRef]
- Hennes, E.M.; Baumann, M.; Schanda, K.; Anlar, B.; Bajer-Kornek, B.; Blaschek, A.; Brantner-Inthaler, S.; Diepold, K.; Eisenkölbl, A.; Gotwald, T.; et al. Prognostic relevance of MOG antibodies in children with an acquired demyelinating syndrome. Neurology 2017, 89, 900–908. [Google Scholar] [CrossRef] [PubMed]
- de Mol, C.L.; Wong, Y.Y.M.; van Pelt, E.D.; Ketelslegers, I.A.; Bakker, D.P.; Boon, M.; Braun, K.P.J.; van Dijk, K.G.J.; Eikelenboom, M.J.; Engelen, M.; et al. Incidence and outcome of acquired demyelinating syndromes in Dutch children: Update of a nationwide and prospective study. J. Neurol. 2018, 265, 1310–1319. [Google Scholar] [CrossRef] [PubMed]
- Armangue, T.; Olivé-Cirera, G.; Martínez-Hernandez, E.; Sepulveda, M.; Ruiz-Garcia, R.; Muñoz-Batista, M.; Ariño, H.; González-Álvarez, V.; Felipe-Rucián, A.; Jesús Martínez-González, M.; et al. Associations of paediatric demyelinating and encephalitic syndromes with myelin oligodendrocyte glycoprotein antibodies: A multicentre observational study. Lancet Neurol. 2020, 19, 234–246. [Google Scholar] [CrossRef] [PubMed]
- Boesen, M.S.; Jensen, P.E.H.; Born, A.P.; Magyari, M.; Nilsson, A.C.; Hoei-Hansen, C.; Blinkenberg, M.; Sellebjerg, F. Incidence of pediatric neuromyelitis optica spectrum disorder and myelin oligodendrocyte glycoprotein antibody-associated disease in Denmark 2008–2018: A nationwide, population-based cohort study. Mult. Scler. Relat. Disord. 2019, 33, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Waters, P.; Fadda, G.; Woodhall, M.; O’Mahony, J.; Brown, R.A.; Castro, D.A.; Longoni, G.; Irani, S.R.; Sun, B.; Yeh, E.; et al. Serial anti-myelin oligodendrocyte glycoprotein antibody analyses and outcomes in children with demyelinating syndromes. JAMA Neurol. 2020, 77, 82–93. [Google Scholar] [CrossRef] [PubMed]
- Cobo-Calvo, Á.; d’Indy, H.; Ruiz, A.; Collongues, N.; Kremer, L.; Durand-Dubief, F.; Rollot, F.; Casey, R.; Vukusic, S.; De Seze, J.; et al. Frequency of myelin oligodendrocyte glycoprotein antibody in multiple sclerosis: A multicenter cross-sectional study. Neurol. Neuroimmunol. Neuroinflamm. 2019, 7, e649. [Google Scholar] [CrossRef] [PubMed]
- Kunchok, A.; Chen, J.J.; McKeon, A.; Mills, J.R.; Flanagan, E.P.; Pittock, S.J. Coexistence of myelin oligodendrocyte glycoprotein and aquaporin-4 antibodies in adult and pediatric patients. JAMA Neurol. 2020, 77, 257–259. [Google Scholar] [CrossRef] [PubMed]
- Cobo-Calvo, A.; Ruiz, A.; Rollot, F.; Arrambide, G.; Deschamps, R.; Maillart, E.; Papeix, C.; Audoin, B.; Lépine, A.F.; Maurey, H.; et al. Clinical features and risk of relapse in children and adults with myelin oligodendrocyte glycoprotein antibody-associated disease. Ann. Neurol. 2021, 89, 30–41. [Google Scholar] [CrossRef]
- Baumann, M.; Hennes, E.M.; Schanda, K.; Karenfort, M.; Kornek, B.; Seidl, R.; Diepold, K.; Lauffer, H.; Marquardt, I.; Strautmanis, J.; et al. Children with multiphasic disseminated encephalomyelitis and antibodies to the myelin oligodendrocyte glycoprotein (MOG): Extending the spectrum of MOG antibody positive diseases. Mult. Scler. 2016, 22, 1821–1829. [Google Scholar] [CrossRef]
- Satukijchai, C.; Mariano, R.; Messina, S.; Sa, M.; Woodhall, M.R.; Robertson, N.P.; Ming, L.; Wassmer, E.; Kneen, R.; Huda, S.; et al. Factors associated with relapse and treatment of myelin oligodendrocyte glycoprotein antibody-associated disease in the United Kingdom. JAMA Netw. Open 2022, 5, e2142780. [Google Scholar] [CrossRef]
- Klein da Costa, B.; Banwell, B.L.; Sato, D.K. Treatment of MOG-IgG associated disease in paediatric patients: A systematic review. Mult. Scler. Relat. Disord. 2021, 56, 103216. [Google Scholar] [CrossRef] [PubMed]
- Jurynczyk, M.; Messina, S.; Woodhall, M.R.; Raza, N.; Everett, R.; Roca-Fernandez, A.; Tackley, G.; Hamid, S.; Sheard, A.; Reynolds, G.; et al. Clinical presentation and prognosis in MOG-antibody disease: A UK study. Brain 2017, 140, 3128–3138. [Google Scholar] [CrossRef] [PubMed]
- Yeh, E.A.; Graves, J.S.; Benson, L.A.; Wassmer, E.; Waldman, A. Pediatric optic neuritis. Neurology 2016, 87, S53. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.J.; Flanagan, E.P.; Jitprapaikulsan, J.; López-Chiriboga, A.S.S.; Fryer, J.P.; Leavitt, J.A.; Weinshenker, B.G.; McKeon, A.; Tillema, J.M.; Lennon, V.A.; et al. Myelin oligodendrocyte glycoprotein antibody-positive optic neuritis: Clinical characteristics, radiologic clues, and outcome. Am. J. Ophthalmol. 2018, 195, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.J.; Bhatti, M.T. Clinical phenotype, radiological features, and treatment of myelin oligodendrocyte glycoprotein-immunoglobulin G (MOG-IgG) optic neuritis. Curr. Opin. Neurol. 2020, 33, 47. [Google Scholar] [CrossRef] [PubMed]
- Jitprapaikulsan, J.; Chen, J.J.; Flanagan, E.P.; Tobin, W.O.; Fryer, J.P.; Weinshenker, B.G.; McKeon, A.; Lennon, V.A.; Leavitt, J.A.; Tillema, J.M.; et al. Aquaporin-4 and Myelin Oligodendrocyte Glycoprotein Autoantibody Status Predict Outcome of Recurrent Optic Neuritis. Ophthalmology 2018, 125, 1628. [Google Scholar] [CrossRef]
- Oertel, F.C.; Sotirchos, E.S.; Zimmermann, H.G.; Motamedi, S.; Specovius, S.; Asseyer, E.S.; Chien, C.; Cook, L.; Vasileiou, E.; Filippatou, A.; et al. Longitudinal Retinal Changes in MOGAD. Ann. Neurol. 2022, 92, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Pakeerathan, T.; Havla, J.; Schwake, C.; Salmen, A.; Bigi, S.; Abegg, M.; Brügger, D.; Ferrazzini, T.; Runge, A.K.; Breu, M.; et al. Characteristic retinal atrophy pattern allows differentiation between pediatric MOGAD and MS after a single optic neuritis episode. J. Neurol. 2022, 269, 6366–6376. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fadda, G.; Flanagan, E.P.; Cacciaguerra, L.; Jitprapaikulsan, J.; Solla, P.; Zara, P.; Sechi, E. Myelitis features and outcomes in CNS demyelinating disorders: Comparison between multiple sclerosis, MOGAD, and AQP4-IgG-positive NMOSD. Front. Neurol. 2022, 13, 1011579. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mariano, R.; Messina, S.; Kumar, K.; Kuker, W.; Leite, M.I.; Palace, J. Comparison of Clinical Outcomes of Transverse Myelitis Among Adults With Myelin Oligodendrocyte Glycoprotein Antibody vs. Aquaporin-4 Antibody Disease. JAMA Netw. Open 2019, 2, e1912732. [Google Scholar] [CrossRef]
- Ciron, J.; Cobo-Calvo, A.; Audoin, B.; Bourre, B.; Brassat, D.; Cohen, M.; Collongues, N.; Deschamps, R.; Durand-Dubief, F.; Laplaud, D.; et al. Frequency and characteristics of short versus longitudinally extensive myelitis in adults with MOG antibodies: A retrospective multicentric study. Mult. Scler. 2020, 26, 936. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B.; Tardieu, M.; Amato, M.P.; Banwell, B.; Chitnis, T.; Dale, R.C.; Ghezzi, A.; Hintzen, R.; Kornberg, A.; Pohl, D.; et al. International Pediatric Multiple Sclerosis Study Group criteria for pediatric multiple sclerosis and immune-mediated central nervous system demyelinating disorders: Revisions to the 2007 definitions. Mult. Scler. 2013, 19, 1261. [Google Scholar] [CrossRef]
- Wendel, E.M.; Thonke, H.S.; Bertolini, A.; Baumann, M.; Blaschek, A.; Merkenschlager, A.; Karenfort, M.; Kornek, B.; Lechner, C.; Pohl, D.; et al. Temporal Dynamics of MOG Antibodies in Children With Acquired Demyelinating Syndrome. Neurol. Neuroimmunol. Neuroinflamm. 2022, 9, e200035. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ogawa, R.; Nakashima, I.; Takahashi, T.; Kaneko, K.; Akaishi, T.; Takai, Y.; Sato, D.K.; Nishiyama, S.; Misu, T.; Kuroda, H.; et al. MOG antibody-positive, benign, unilateral, cerebral cortical encephalitis with epilepsy. Neurol. Neuroimmunol. Neuroinflamm. 2017, 4, e322. [Google Scholar] [CrossRef] [PubMed]
- Budhram, A.; Mirian, A.; Le, C.; Hosseini-Moghaddam, S.M.; Sharma, M.; Nicolle, M.W. Unilateral cortical FLAIR-hyperintense lesions in anti-MOG-associated Encephalitis with seizures (FLAMES): Characterization of a distinct clinico-radiographic syndrome. J. Neurol. 2019, 266, 2481–2487. [Google Scholar] [CrossRef] [PubMed]
- Stamenova, S.; Redha, I.; Schmierer, K.; Garcia, M.E. FLAIR-hyperintense lesions in anti-MOG-associated encephalitis with seizures (FLAMES) unmasked by withdrawal of immunosuppression for Crohn’s disease? Mult. Scler. Relat. Disord. 2021, 48, 102729. [Google Scholar] [CrossRef] [PubMed]
- Jain, K.; Cherian, A.; Thomas, B.J.N. FLAMES: A novel burning entity in MOG IgG associated disease. Mult. Scler. Relat. Disord. 2021, 49, 102759. [Google Scholar] [CrossRef]
- Hokama, H.; Sakamoto, Y.; Hayashi, T.; Hatake, S.; Takahashi, M.; Kodera, H.; Kutsuna, A.; Nito, C.; Nakane, S.; Nagayama, H.; et al. A case report of FLAMES with elevated myelin basic protein followed by myelitis. Intern. Med. 2022, 61, 3585–3588. [Google Scholar] [CrossRef] [PubMed]
- Maniscalco, G.T.; Allegorico, L.; Alfieri, G.; Napolitano, M.; Ranieri, A.; Renna, R.; Servillo, G.; Pezzella, M.; Capone, E.; Altomare, L.; et al. Anti-MOG-associated demyelinating disorders: Two sides of the same coin. Neurol. Sci. 2021, 42, 1531–1534. [Google Scholar] [CrossRef]
- Lopez Chiriboga, S.; Flanagan, E.P. Myelitis and other autoimmune myelopathies. Continuum 2021, 27, 62–92. [Google Scholar] [CrossRef]
- Budhram, A.; Kunchok, A.; Flanagan, E. Adding FUEL to the FLAMES: FLAIR-Variable Unilateral Enhancement of the Leptomeninges (FUEL) in MOG-IgG-Associated Disease (862); AANEnterprises: Chester, PA, USA, 2020. [Google Scholar]
- Yao, T.; Zeng, Q.; Xie, Y.; Bi, F.; Zhang, L.; Xiao, B.; Zhou, J. Clinical analysis of adult MOG antibody-associated cortical encephalitis. Mult. Scler. Relat. Disord. 2022, 60, 103727. [Google Scholar] [CrossRef] [PubMed]
- Titulaer, M.J.; Höftberger, R.; Iizuka, T.; Leypoldt, F.; McCracken, L.; Cellucci, T.; Benson, L.A.; Shu, H.; Irioka, T.; Hirano, M.; et al. Overlapping demyelinating syndromes and anti–N-methyl-D-aspartate receptor encephalitis. Ann. Neurol. 2014, 75, 411–428. [Google Scholar] [CrossRef] [PubMed]
- Reindl, M.; Jarius, S.; Rostasy, K.; Berger, T. Myelin oligodendrocyte glycoprotein antibodies: How clinically useful are they? Curr. Opin. Neurol. 2017, 30, 295–301. [Google Scholar] [CrossRef]
- Jarius, S.; Kleiter, I.; Ruprecht, K.; Asgari, N.; Pitarokoili, K.; Borisow, N.; Hümmert, M.W.; Trebst, C.; Pache, F.; Winkelmann, A.; et al. MOG-IgG in NMO and related disorders: A multicenter study of 50 patients. Part 3: Brainstem involvement—Frequency, presentation and outcome. J. Neuroinflamm. 2016, 13, 281. [Google Scholar] [CrossRef] [PubMed]
- Kunchok, A.; Krecke, K.N.; Flanagan, E.P.; Jitprapaikulsan, J.; Lopez-Chiriboga, A.S.; Chen, J.J.; Weinshenker, B.G.; Pittock, S.J. Does area postrema syndrome occur in myelin oligodendrocyte glycoprotein-IgG-associated disorders (MOGAD)? Neurology 2020, 94, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Paviolo, J.P.; Tkachuk, V.A. Isolated area postrema syndrome with anti-MOG antibodies, a rare association. Rev. Neurol. 2020, 71, 125–126. (In Spanish) [Google Scholar] [CrossRef] [PubMed]
- Chan, K.H.; Vorobeychik, G. Area postrema syndrome: A neurological presentation of nausea, vomiting and hiccups. BMJ Case Rep. 2020, 13, e238588. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Akaishi, T.; Konno, M.; Nakashima, I.; Aoki, M. Intractable hiccup in demyelinating disease with anti-myelin oligodendrocyte glycoprotein (MOG) antibody. Intern. Med. 2016, 55, 2905–2906. [Google Scholar] [CrossRef]
- Carnero Contentti, E.; Rojas, J.I.; Criniti, J.; Lopez, P.A.; Daccach Marques, V.; Soto de Castillo, I.; Tkachuk, V.; Marrodan, M.; Correale, J.; Farez, M.F.; et al. Towards imaging criteria that best differentiate MS from NMOSD and MOGAD: Large multi-ethnic population and different clinical scenarios. Mult. Scler. Relat. Disord. 2022, 61, 103778. [Google Scholar] [CrossRef] [PubMed]
- Baumann, M.; Grams, A.; Djurdjevic, T.; Wendel, E.M.; Lechner, C.; Behring, B.; Blaschek, A.; Diepold, K.; Eisenkölbl, A.; Fluss, J.; et al. MRI of the first event in pediatric acquired demyelinating syndromes with antibodies to myelin oligodendrocyte glycoprotein. J. Neurol. 2018, 265, 845–855. [Google Scholar] [CrossRef]
- Juryńczyk, M.; Tackley, G.; Kong, Y.; Geraldes, R.; Matthews, L.; Woodhall, M.; Waters, P.; Kuker, W.; Craner, M.; Weir, A.; et al. Brain lesion distribution criteria distinguish MS from AQP4-antibody NMOSD and MOG-antibody disease. J. Neurol. Neurosurg. Psychiatry 2017, 88, 132–136. [Google Scholar] [CrossRef] [PubMed]
- Jurynczyk, M.; Geraldes, R.; Probert, F.; Woodhall, M.R.; Waters, P.; Tackley, G.; DeLuca, G.; Chandratre, S.; Leite, M.I.; Vincent, A.; et al. Distinct brain imaging characteristics of autoantibody-mediated CNS conditions and multiple sclerosis. Brain 2017, 140, 617–627. [Google Scholar] [CrossRef]
- Dubey, D.; Pittock, S.J.; Krecke, K.N.; Morris, P.P.; Sechi, E.; Zalewski, N.L.; Weinshenker, B.G.; Shosha, E.; Lucchinetti, C.F.; Fryer, J.P.; et al. Clinical, Radiologic, and prognostic features of myelitis associated with myelin oligodendrocyte glycoprotein autoantibody. JAMA Neurol. 2019, 76, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Hacohen, Y.; Rossor, T.; Mankad, K.; Chong, W.; Lux, A.; Wassmer, E.; Lim, M.; Barkhof, F.; Ciccarelli, O.; Hemingway, C. ‘Leukodystrophy-like’ phenotype in children with myelin oligodendrocyte glycoprotein antibody-associated disease. Dev. Med. Child. Neurol. 2018, 60, 417–423. [Google Scholar] [CrossRef] [PubMed]
- Waters, P.J.; Komorowski, L.; Woodhall, M.; Lederer, S.; Majed, M.; Fryer, J.; Mills, J.; Flanagan, E.P.; Irani, S.R.; Kunchok, A.C.; et al. A multicenter comparison of MOG-IgG cell-based assays. Neurology 2019, 92, e1250. [Google Scholar] [CrossRef] [PubMed]
- Yeh, E.A.; Nakashima, I. Live-cell based assays are the gold standard for anti-MOG-Ab testing. Neurology 2019, 92, 501. [Google Scholar] [CrossRef] [PubMed]
- Sechi, E.; Buciuc, M.; Pittock, S.J.; Chen, J.J.; Fryer, J.P.; Jenkins, S.M.; Budhram, A.; Weinshenker, B.G.; Lopez-Chiriboga, A.S.; Tillema, J.M.; et al. Positive Predictive Value of Myelin Oligodendrocyte Glycoprotein Autoantibody Testing. JAMA Neurol. 2021, 78, 741. [Google Scholar] [CrossRef] [PubMed]
- Held, F.; Kalluri, S.R.; Berthele, A.; Klein, A.K.; Reindl, M.; Hemmer, B. Frequency of myelin oligodendrocyte glycoprotein antibodies in a large cohort of neurological patients. Mult. Scler. J. Exp. Transl. Clin. 2021, 7, 20552173211022767. [Google Scholar] [CrossRef]
- Jarius, S.; Ruprecht, K.; Stellmann, J.P.; Huss, A.; Ayzenberg, I.; Willing, A.; Trebst, C.; Pawlitzki, M.; Abdelhak, A.; Grüter, T.; et al. MOG-IgG in primary and secondary chronic progressive multiple sclerosis: A multicenter study of 200 patients and review of the literature. J. Neuroinflamm. 2018, 15, 88. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jarius, S.; Paul, F.; Aktas, O.; Asgari, N.; Dale, R.C.; de Seze, J.; Franciotta, D.; Fujihara, K.; Jacob, A.; Kim, H.J.; et al. MOG encephalomyelitis: International recommendations on diagnosis and antibody testing. J. Neuroinflamm. 2018, 15, 134. [Google Scholar] [CrossRef]
- Banwell, B.; Bennett, J.L.; Marignier, R.; Kim, H.J.; Brilot, F.; Flanagan, E.P.; Ramanathan, S.; Waters, P.; Tenembaum, S.; Graves, J.S.; et al. Diagnosis of myelin oligodendrocyte glycoprotein antibody-associated disease: International MOGAD Panel proposed criteria. Lancet Neurol. 2023, 22, 268–282. [Google Scholar] [CrossRef] [PubMed]
- Hegen, H.; Reindl, M. Recent developments in MOG-IgG associated neurological disorders. Ther. Adv. Neurol. Disord. 2020, 13, 1756286420945135. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, B.; Gomez-Figueroa, E.; Redenbaugh, V.; Francis, A.; Satukijchai, C.; Wu, Y.; Messina, S.; Sa, M.; Woodhall, M.; Paul, F.; et al. Do Early Relapses Predict the Risk of Long-Term Relapsing Disease in an Adult and Paediatric Cohort with MOGAD? Ann. Neurol. 2023, 94, 508–517, Erratum in Ann. Neurol. 2024, 95, 623. [Google Scholar] [CrossRef] [PubMed]
- Leite, M.I.; Panahloo, Z.; Harrison, N.; Palace, J. A systematic literature review to examine the considerations around pregnancy in women of child-bearing age with myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD) or aquaporin 4 neuromyelitis optica spectrum disorder (AQP4+ NMOSD). Mult. Scler. Relat. Disord. 2023, 75, 104760. [Google Scholar] [CrossRef] [PubMed]
- Jarius, S.; Ruprecht, K.; Kleiter, I.; Borisow, N.; Asgari, N.; Pitarokoili, K.; Pache, F.; Stich, O.; Beume, L.A.; Hümmert, M.W.; et al. MOG-IgG in NMO and related disorders: A multicenter study of 50 patients. Part 2: Epidemiology, clinical presentation, radiological and laboratory features, treatment responses, and long-term outcome. J. Neuroinflamm. 2016, 13, 280. [Google Scholar] [CrossRef] [PubMed]
- Hacohen, Y.; Wong, Y.Y.; Lechner, C.; Jurynczyk, M.; Wright, S.; Konuskan, B.; Kalser, J.; Poulat, A.L.; Maurey, H.; Ganelin-Cohen, E.; et al. Disease course and treatment responses in children with relapsing myelin oligodendrocyte glycoprotein antibody-associated disease. JAMA Neurol. 2018, 75, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Lu, X.; Zhang, Y.; Ji, T.; Jin, Y.; Xu, M.; Bao, X.; Zhang, Y.; Xiong, H.; Chang, X.; et al. Follow-up study on Chinese children with relapsing MOG-IgG-associated central nervous system demyelination. Mult. Scler. Relat. Disord. 2019, 28, 4–10. [Google Scholar] [CrossRef]
- Chen, J.J.; Flanagan, E.P.; Bhatti, M.T.; Jitprapaikulsan, J.; Dubey, D.; Lopez Chiriboga, A.S.S.; Fryer, J.P.; Weinshenker, B.G.; McKeon, A.; Tillema, J.M.; et al. Steroid-sparing maintenance immunotherapy for MOG-IgG associated disorder. Neurology 2020, 95, e111–e120. [Google Scholar] [CrossRef] [PubMed]
- Cobo-Calvo, A.; Sepúlveda, M.; Rollot, F.; Armangué, T.; Ruiz, A.; Maillart, E.; Papeix, C.; Audoin, B.; Zephir, H.; Biotti, D.; et al. Evaluation of treatment response in adults with relapsing MOG-Ab-associated disease. J. Neuroinflamm. 2019, 16, 134. [Google Scholar] [CrossRef]
- Cobo-Calvo, A.; Sepúlveda, M.; Rollot, F.; Armangué, T.; Ruiz, A.; Maillart, E.; Papeix, C.; Audoin, B.; Zephir, H.; Biotti, D.; et al. A comparison of the effects of rituximab versus other immunotherapies for MOG-IgG-associated central nervous system demyelination: A meta-analysis. Mult. Scler. Relat. Disord. 2021, 53, 103044. [Google Scholar]
- Elsbernd, P.M.; Hoffman, W.R.; Carter, J.L.; Wingerchuk, D.M. Interleukin-6 inhibition with tocilizumab for relapsing MOG-IgG associated disorder (MOGAD): A case-series and review. Mult. Scler. Relat. Disord. 2021, 48, 102696. [Google Scholar] [CrossRef] [PubMed]
- Bril, V.; Drużdż, A.; Grosskreutz, J.; Habib, A.A.; Mantegazza, R.; Sacconi, S.; Utsugisawa, K.; Vissing, J.; Vu, T.; Boehnlein, M.; et al. Safety and efficacy of rozanolixizumab in patients with generalised myasthenia gravis (MycarinG): A randomised, double-blind, placebo-controlled, adaptive phase 3 study. Lancet Neurol. 2023, 22, 383–394, Erratum in Lancet Neurol. 2023, 22, e11. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Clinical Syndrome | Features | ||
|---|---|---|---|
| Optic Neuritis (ON) | Most common presentation in adults (50%) | Often bilateral Long lesions within the anterior optic pathway | Good recovery, but with excessive optic disc edema and RNFL thinning |
| Transverse Myelitis | Initial presentation in 30% of adults | Motor, sensory, or autonomic symptoms | Significant predictor of disability, but more steroid responsive than NMOSD and MS |
| ADEM | Initial presentation in 50% of children. Very rare in adults (5%) | Presenting symptom is seizures in 40% of the children with ADEM and MOGAD | Increased risk of post-ADEM epilepsy |
| FLAMES | Unilateral cortical hyperintensities in the FLAIR sequence with associated seizures | Focal seizures which can progress to generalized, headache, encephalopathy | Meningeal involvement can be present |
| MOGAD & NMDAR overlapping syndrome | MOG antibodies and NMDAR-antibodies co-existence | Patients present with atypical NMDAR encephalitis or atypical MOGAD | Requires more aggressive treatment than MOGAD alone and cancer screening |
| Multifocal CNS attack | Can involve the optic nerve, spinal cord, brainstem and cerebellum | Vision loss, motor/sensory symptoms, ataxia, diplopia | |
| NMOSD syndrome | ON, LETM | Rarely intractable nausea and vomiting | AQP4 seronegative |
| Specificity | MOG-IgG Testing Using a Cell-Based Assay with Full-Length MOG Yields Highly Specific Results. |
| Preferred specimen type | Testing in serum is optimal; however, CSF testing might be considered in highly suspected seronegative cases. |
| Timing of testing | Testing is best to be done during attacks and prior to immunotherapy. |
| Patient selection | Testing should be done only in patients with clinical or imaging features consistent with MOGAD. |
| Routine Screening | Routine screening of all multiple sclerosis (MS) patients for MOG-IgG is not advisable, as it can heighten the risk of false positives. |
| False positives | False positives are known to occur, especially at low titers and when the antibody test is requested in low-probability situations. |
| MOGAD | AQP4 + NMOSD | MS | |
|---|---|---|---|
| Demographics | |||
| Age at onset | Fourth decade of life | Fourth or fifth decade of life | End of third decade of life |
| Sex | Slightly more predominant in women (1.5:1) | Female: Male = 9:1 | Female: Male = 3:1 |
| Race | No specific differences among different ethnic groups | Afro-Caribbean or Afro-American | White ethnic groups of European descent, although increasing prevalence in all ethnic/racial groups |
| Clinical Features | |||
| Course | 65% monophasic, 35% relapsing (relapses mostly manifest as optic neuritis) | Relapsing | Mostly relapsing, but can be progressive from the beginning |
| Clinical presentation | Optic neuritis, transverse myelitis, ADEM or other type of encephalitis, FLAMES, brainstem demyelination | Optic neuritis with poor recovery, severe transverse myelitis, area postrema syndrome, brainstem, diencephalic or cerebral syndrome | Spinal cord, brainstem or cerebellar syndrome. Optic neuritis or cognitive dysfunction |
| Outcome | Mostly favorable outcomes with low risk of future disability. In up to 60–70% of patients with disability, disability comes from the first attack | High risk of disability. Poor prognosis and high relapse rate | High risk of disability accumulation because of relapse associated worsening and progression independent of relapses |
| MRI | |||
| Optic Nerve | Bilateral optic nerve involvement, anterior optic pathway. More than 50% of the optic nerve is enhancing. Optic disc edema | Bilateral optic nerve involvement, posterior optic pathway including optic chiasm. More than 50% of the optic nerve is enhancing | Unilateral optic nerve involvement. Short lesions |
| Brain | Heterogenous imaging features. ADEM-like, poorly demarcated, fluffy white matter, deep grey matter lesions, cortical lesions, infratentorial lesions particularly within the cerebellar peduncles and pons. Can be entirely normal | Can be entirely normal. Also, can have deep white matter lesions, or large hemispheric lesions or lesions adjacent to the third or fourth ventricle where AQP4 is mostly expressed | Ovoid lesions perpendicular to the corpus callosum, lesions adjacent to the lateral ventricles, deep white matter lesions or brainstem lesions |
| Spinal cord | LETM or shorter lesions. Confined to the grey matter (H-shaped). Common involvement of the conus medullaris. Infrequent enhancement | LETM (>3 vertebral segments). Centrally located but not H-shaped. Frequently contrast enhancing | Short lesions peripherally located involving the dorsal or lateral columns. Frequent enhancement |
| CSF | |||
| White blood cells | Pleocytosis (100–1000 white blood cells/mm—mostly lymphocytes) in 50% of the patients | Pleocytosis (100–1000 cells—mostly lymphocytes) in 50% of the patients | Pleocytosis not so common < 50% of the patients |
| Biochemistry | Oligoclonal bands < 10% | Oligoclonal bands < 10% | Oligoclonal bands very common > 85–90% |
| Elevated protein | Elevated protein | Protein can be elevated or within normal range |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gklinos, P.; Dobson, R. Myelin Oligodendrocyte Glycoprotein-Antibody Associated Disease: An Updated Review of the Clinical Spectrum, Pathogenetic Mechanisms and Therapeutic Management. Antibodies 2024, 13, 43. https://doi.org/10.3390/antib13020043
Gklinos P, Dobson R. Myelin Oligodendrocyte Glycoprotein-Antibody Associated Disease: An Updated Review of the Clinical Spectrum, Pathogenetic Mechanisms and Therapeutic Management. Antibodies. 2024; 13(2):43. https://doi.org/10.3390/antib13020043
Chicago/Turabian StyleGklinos, Panagiotis, and Ruth Dobson. 2024. "Myelin Oligodendrocyte Glycoprotein-Antibody Associated Disease: An Updated Review of the Clinical Spectrum, Pathogenetic Mechanisms and Therapeutic Management" Antibodies 13, no. 2: 43. https://doi.org/10.3390/antib13020043
APA StyleGklinos, P., & Dobson, R. (2024). Myelin Oligodendrocyte Glycoprotein-Antibody Associated Disease: An Updated Review of the Clinical Spectrum, Pathogenetic Mechanisms and Therapeutic Management. Antibodies, 13(2), 43. https://doi.org/10.3390/antib13020043