Antibodies against Platelet Factor 4 and Their Associated Pathologies: From HIT/HITT to Spontaneous HIT-Like Syndrome, to COVID-19, to VITT/TTS




Abstract
1. Introduction
2. Heparin-Induced Thrombocytopenia (HIT)
3. Spontaneous HIT-Like Syndromes
4. Anti-PF4 Antibodies in COVID-19 Patients
5. Anti-PF4 Antibodies in VITT/TTS
6. Discussion
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prechel, M.M.; Walenga, J.M. Emphasis on the Role of PF4 in the Incidence, Pathophysiology and Treatment of Heparin Induced Thrombocytopenia. Thromb. J. 2013, 11, 7. [Google Scholar] [CrossRef]
- Baluwala, I.; Favaloro, E.J.; Pasalic, L. Therapeutic monitoring of unfractionated heparin—Trials and tribulations. Expert Rev. Hematol. 2017, 10, 595–605. [Google Scholar] [CrossRef]
- Joseph, J.; Rabbolini, D.; Enjeti, A.K.; Favaloro, E.; Kopp, M.C.; McRae, S.; Pasalic, L.; Chee Wee, T.; Ward, C.M.; Chong, B.H. Diagnosis and management of heparin-induced thrombocytopenia: A consensus statement from the Thrombosis and Haemostasis Society of Australia and New Zealand HIT Writing Group. Med. J. Aust. 2019, 210, 509–516. [Google Scholar] [CrossRef]
- Favaloro, E.J.; McCaughan, G.; Pasalic, L. Clinical and laboratory diagnosis of heparin induced thrombocytopenia: An update. Pathology 2017, 49, 346–355. [Google Scholar] [CrossRef]
- Favaloro, E.J. Laboratory tests for identification or exclusion of heparin induced thrombocytopenia—HIT or miss? Am. J. Hematol. 2018, 93, 308–314. [Google Scholar] [CrossRef]
- Pishko, A.M.; Cuker, A. Diagnosing heparin-induced thrombocytopenia: The need for accuracy and speed. Int. J. Lab. Hematol. 2021, 43 (Suppl. 1), 96–102. [Google Scholar] [CrossRef]
- Younis, M.; Ya’qoub, L.; Ali, Z.; Grover, P.; Ya’acoub, R.; Hamarshi, M.S. Comparison of a clinical-laboratory algorithm, 4t and heparin-induced thrombocytopenia expert probability scores in the diagnosis of heparin-induced thrombocytopenia in the critical care setting. Am. J. Blood Res. 2019, 9, 25–33. [Google Scholar]
- Pishko, A.M.; Fardin, S.; Lefler, D.S.; Paydary, K.; Vega, R.; Arepally, G.M.; Crowther, M.; Rice, L.; Cines, D.B.; Cuker, A. Prospective comparison of the HEP score and 4Ts score for the diagnosis of heparin-induced thrombocytopenia. Blood Adv. 2018, 2, 3155–3162. [Google Scholar] [CrossRef]
- Favaloro, E.J.; McCaughan, G.; Mohammed, S.; Lau, K.K.E.; Gemmell, R.; Cavanaugh, L.; Donikian, D.; Kondo, M.; Brighton, T.; Pasalic, L. HIT or miss? A comprehensive contemporary investigation of laboratory tests for heparin induced thrombocytopenia. Pathology 2018, 50, 426–436. [Google Scholar] [CrossRef]
- Favaloro, E.J.; Mohammed, S.; Donikian, D.; Kondo, M.; Duncan, E.; Yacoub, O.; Zebeljan, D.; Ng, S.; Malan, E.; Yuen, A.; et al. A multicentre assessment of contemporary laboratory assays for heparin induced thrombocytopenia. Pathology 2021, 53, 247–256. [Google Scholar] [CrossRef]
- Marashi-Sabouni, Z.; Vayne, C.; Ibrahim-Kosta, M.; Guidon, C.; Loundou, A.; Guery, E.A.; Morange, P.E.; Camoin-Jau, L. Clinical validation of immunoassay HemosIL® AcuStar HIT-IgG (PF4-H) in the diagnosis of Heparin-induced thrombocytopenia. J. Thromb. Thrombolysis 2021, 52, 601–609. [Google Scholar] [CrossRef]
- Jousselme, E.; Guéry, E.A.; Nougier, C.; Sobas, F.; Rollin, J.; Gruel, Y.; Vayne, C.; Pouplard, C. Prospective evaluation of two specific IgG immunoassays (HemosIL AcuStar HIT-IgG and HAT45G) for the diagnosis of heparin-induced thrombocytopenia: A Bayesian approach. Int. J. Lab. Hematol. 2021, 43, 468–476. [Google Scholar] [CrossRef]
- Brodard, J.; Benites, V.; Stalder Zeerleder, D.; Nagler, M. Accuracy of the functional, flow cytometer-based Emo-Test HIT Confirm® for the diagnosis of heparin-induced thrombocytopenia. Thromb. Res. 2021, 203, 22–26. [Google Scholar] [CrossRef]
- Tardy-Poncet, B.; Montmartin, A.; Piot, M.; Alhenc-Gelas, M.; Nguyen, P.; Elalamy, I.; Greinacher, A.; Maistre, E.; Lasne, D.; Horellou, M.H.; et al. Functional Flow Cytometric Assay for Reliable and Convenient Heparin-Induced Thrombocytopenia Diagnosis in Daily Practice. Biomedicines 2021, 9, 332. [Google Scholar] [CrossRef]
- Cipok, M.; Tomer, A.; Elalamy, I.; Kirgner, I.; Dror, N.; Kay, S.; Deutsch, V.R. Pathogenic heparin-induced thrombocytopenia and thrombosis (HIT) antibodies determined by rapid functional flow cytometry. Eur. J. Haematol. 2019, 103, 225–233. [Google Scholar] [CrossRef]
- Warkentin, T.E.; Greinacher, A. Spontaneous HIT syndrome: Knee replacement, infection, and parallels with vaccine-induced immune thrombotic thrombocytopenia. Thromb. Res. 2021, 204, 40–51. [Google Scholar] [CrossRef]
- Okata, T.; Miyata, S.; Miyashita, F.; Maeda, T.; Toyoda, K. Spontaneous heparin-induced thrombocytopenia syndrome without any proximate heparin exposure, infection, or inflammatory condition: Atypical clinical features with heparin-dependent platelet activating antibodies. Platelets 2015, 26, 602–607. [Google Scholar] [CrossRef]
- Warkentin, T.E.; Basciano, P.A.; Knopman, J.; Bernstein, R.A. Spontaneous heparin-induced thrombocytopenia syndrome: 2 new cases and a proposal for defining this disorder. Blood 2014, 12, 3651–3654. [Google Scholar] [CrossRef]
- Lippi, G.; Sanchis-Gomar, F.; Favaloro, E.J.; Lavie, C.J.; Henry, B.M. Coronavirus Disease 2019-Associated Coagulopathy. Mayo Clin. Proc. 2021, 96, 203–217. [Google Scholar] [CrossRef]
- Favaloro, E.J.; Henry, B.M.; Lippi, G. The complicated relationships of heparin-induced thrombocytopenia and platelet factor 4 antibodies with COVID-19. Int. J. Lab. Hematol. 2021, 43, 547–558. [Google Scholar] [CrossRef]
- Appelbaum, J.; Arnold, D.M.; Kelton, J.G.; Gernsheimer, T.B.; Jevtic, S.D.; Ivetic, N.; Smith, J.W.; Nazy, I. SARS-CoV-2 spike-dependent platelet activation in COVID-19 vaccine-induced thrombocytopenia. Blood Adv. 2021. [Google Scholar] [CrossRef]
- Pascreau, T.; Ballester, M.C.; Van Dreden, P.; Zia-Chahabi, S.; Zuber, B.; Choucair, J.; Bironien, R.; Farfour, E.; Vasse, M. The high frequency of anti-PF4/heparin antibodies in patients with COVID-19 is neither related to heparin treatment or to an increased incidence of thrombosis. Clin. Chem. Lab. Med. 2021, 59, e405–e408. [Google Scholar] [CrossRef]
- Favaloro, E.J.; Pasalic, L. COVID-19 vaccine induced (immune) thrombotic thrombocytopenia (VITT)/thrombosis with thrombocytopenia syndrome (TTS): An update. Aust. J. Med. Sci. 2021, 42, 86–93. [Google Scholar]
- World Health Organisation. COVID-19 Vaccines. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/covid-19-vaccines (accessed on 23 December 2021).
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef]
- Schultz, N.H.; Sørvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.H.; Skattør, T.H.; Tjønnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef]
- Scully, M.; Singh, D.; Lown, R.; Poles, A.; Solomon, T.; Levi, M.; Goldblatt, D.; Kotoucek, P.; Thomas, W.; Lester, W. Pathologic Antibodies to Platelet Factor 4 after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2202–2211. [Google Scholar] [CrossRef]
- Favaloro, E.J.; Pasalic, L.; Lippi, G. Review and evolution of guidelines for diagnosis of COVID-19 vaccine induced thrombotic thrombocytopenia (VITT). Clin. Chem. Lab. Med. 2021, 60, 7–17. [Google Scholar] [CrossRef]
- Hafeez, M.U.; Ikram, M.; Shafiq, Z.; Sarfraz, A.; Sarfraz, Z.; Jaiswal, V.; Sarfraz, M.; Chérrez-Ojeda, I. COVID-19 Vaccine-Associated Thrombosis with Thrombocytopenia Syndrome (TTS): A Systematic Review and Post Hoc Analysis. Clin. Appl. Thromb. Hemost. 2021, 27. [Google Scholar] [CrossRef]
- Favaloro, E.J. Laboratory testing for suspected COVID-19 vaccine-induced (immune) thrombotic thrombocytopenia. Int. J. Lab. Hematol. 2021, 43, 559–570. [Google Scholar] [CrossRef]
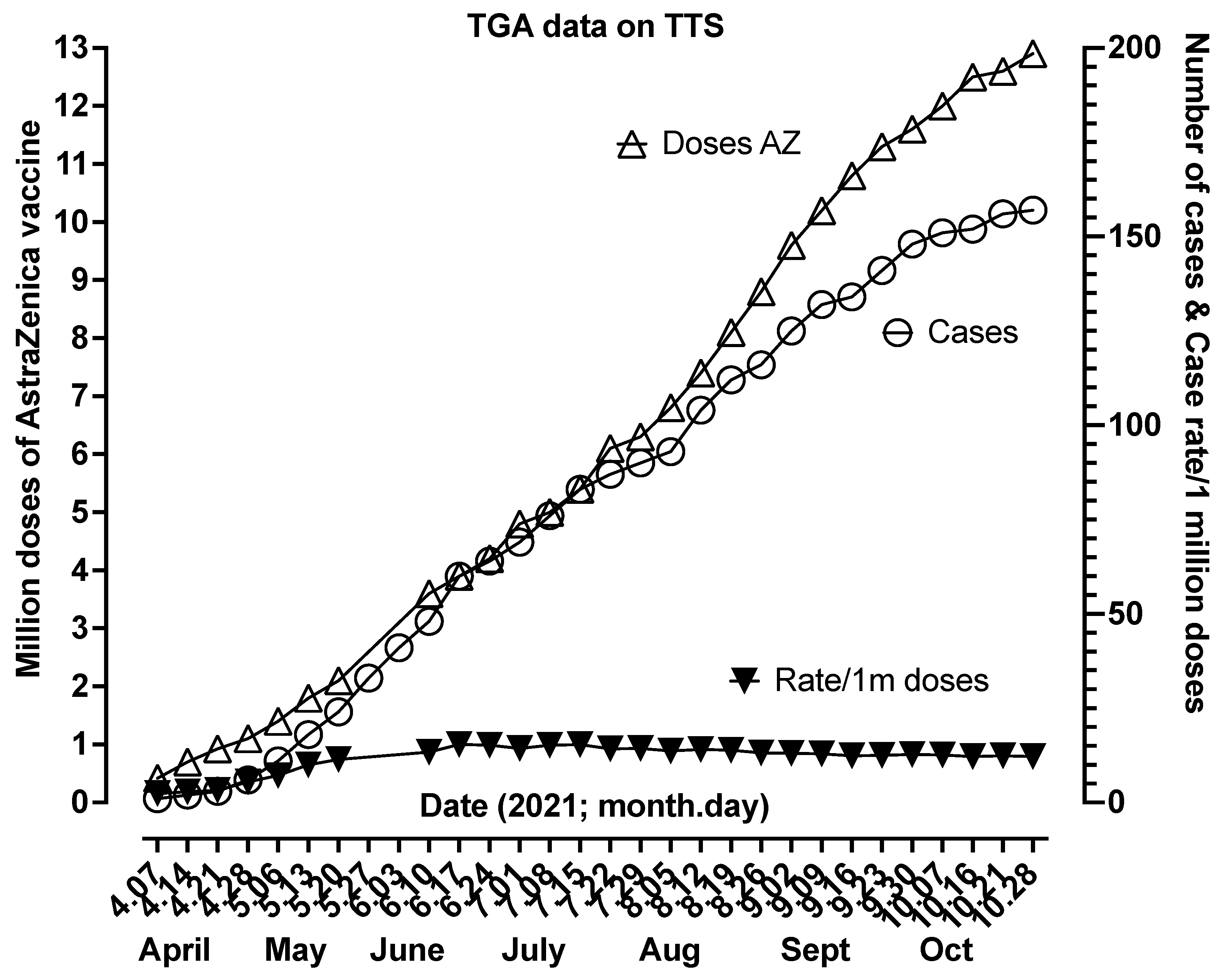
- Therapeutic Goods Administration (TGA). COVID-19 Vaccine Weekly Safety Reports. Available online: https://www.tga.gov.au/covid-19-vaccine-safety-monitoring-and-reporting (accessed on 15 November 2021).
- Goldman, M.; Hermans, C. Thrombotic thrombocytopenia associated with COVID-19 infection or vaccination: Possible paths to platelet factor 4 autoimmunity. PLoS Med. 2021, 18, e1003648. [Google Scholar] [CrossRef]
- Greinacher, A.; Selleng, K.; Palankar, R.; Wesche, J.; Handtke, S.; Wolff, M.; Aurich, K.; Lalk, M.; Methling, K.; Volker, U.; et al. Insights in ChAdOx1 nCov-19 Vaccine-induced Immune Thrombotic Thrombocytopenia (VITT). Blood 2021, 138, 2256–2268. [Google Scholar] [CrossRef]
- Vayne, C.; Rollin, J.; Gruel, Y.; Pouplard, C.; Galinat, H.; Huet, O.; Mémier, V.; Geeraerts, T.; Marlu, R.; Pernod, G.; et al. PF4 Immunoassays in Vaccine-Induced Thrombotic Thrombocytopenia. N. Engl. J. Med. 2021, 385, 376–378. [Google Scholar] [CrossRef]
- Singh, B.; Kanack, A.; Bayas, A.; George, G.; Abou-Ismail, M.Y.; Kohlhagen, M.; Christ, M.; Naumann, M.; Moser, K.; Smock, K.; et al. Anti-PF4 VITT antibodies are oligoclonal and variably inhibited by heparin. medRxiv 2021. [Google Scholar] [CrossRef]
- Chen, V.M.; Curnow, J.L.; Tran, H.A.; Choi, P.Y. Australian and New Zealand approach to diagnosis and management of vaccine-induced immune thrombosis and thrombocytopenia. Med. J. Aust. 2021, 215, 245–249. [Google Scholar] [CrossRef]
- Platton, S.; Bartlett, A.; MacCallum, P.; Makris, M.; McDonald, V.; Singh, D.; Scully, M.; Pavord, S. Evaluation of laboratory assays for anti-platelet factor 4 antibodies after ChAdOx1 nCOV-19 vaccination. J. Thromb. Haemost. 2021, 19, 2007–2013. [Google Scholar] [CrossRef]
- Huynh, A.; Kelton, J.G.; Arnold, D.M.; Daka, M.; Nazy, I. Antibody epitopes in vaccine-induced immune thrombotic thrombocytopaenia. Nature 2021, 596, 565–569. [Google Scholar] [CrossRef]
- Zhang, R.; Duffy, B.F.; Lange, V.; Eby, C.S.; Liu, C. Association between the HLA-DRB1*03:01-DQB1*02:01 haplotype and PF4/heparin antibodies. Blood Adv. 2019, 3, 3136–3142. [Google Scholar] [CrossRef]
- Prechel, M.; Hudec, S.; Lowden, E.; Escalante, V.; Emanuele, N.; Emanuele, M.; Walenga, J.M. Profiling Heparin-Induced Thrombocytopenia (HIT) Antibodies in Hospitalized Patients with and without Diabetes. Clin. Appl. Thromb. Hemost. 2018, 24 (Suppl. 9), 294S–300S. [Google Scholar] [CrossRef]
- Liu, C.C.; Chou, L.P.; Chen, T.S.; Chen, C.A.; Tsai, Y.F. Significant association of anti-platelet factor 4/heparin antibody with cardiovascular disease in hemodialysis patients: A longitudinal 7-year study. Int. Urol. Nephrol. 2018, 50, 2289–2297. [Google Scholar] [CrossRef]
- Maharaj, S.; Chang, S. Anti-PF4/heparin antibodies are increased in hospitalized patients with bacterial sepsis. Thromb. Res. 2018, 171, 111–113. [Google Scholar] [CrossRef]
- Sain, M.; Burilovic, V.; Tomicic, M.; Jelicic, I. High Anti-PF4/Heparin Antibodies Titer and Thromboses Due to Infection 9 Months After Cessation of Heparin in Hemodialyzed Patient with Heparin-Induced Thrombocytopenia. Ther. Apher. Dial. 2018, 22, 558–559. [Google Scholar] [CrossRef]
- Migita, K.; Asano, T.; Sato, S.; Motokawa, S. Induction of anti-PF4/heparin antibodies after arthroplasty for rheumatic diseases. Fukushima J. Med. Sci. 2018, 64, 1–8. [Google Scholar] [CrossRef]
- Meyer, S.C.; Steinmann, E.; Lehmann, T.; Muesser, P.; Passweg, J.R.; Skoda, R.C.; Tsakiris, D.A. Anti-Platelet Factor 4/Heparin Antibody Formation Occurs Endogenously and at Unexpected High Frequency in Polycythemia Vera. Biomed. Res. Int. 2017, 2017, 9876819. [Google Scholar] [CrossRef]
- Selleng, S.; Selleng, K. Heparin-induced thrombocytopenia in cardiac surgery and critically ill patients. Thromb. Haemost. 2016, 116, 843–851. [Google Scholar] [CrossRef]
- Welsby, I.J.; Krakow, E.F.; Heit, J.A.; Williams, E.C.; Arepally, G.M.; Bar-Yosef, S.; Kong, D.F.; Martinelli, S.; Dhakal, I.; Liu, W.W.; et al. The association of anti-platelet factor 4/heparin antibodies with early and delayed thromboembolism after cardiac surgery. J. Thromb. Haemost. 2017, 15, 57–65. [Google Scholar] [CrossRef]
- Selleng, S.; Selleng, K.; Friesecke, S.; Gründling, M.; Kuhn, S.O.; Raschke, R.; Heidecke, O.J.; Hinz, C.; Hron, G.; Warkentin, T.E.; et al. Prevalence and clinical implications of anti-PF4/heparin antibodies in intensive care patients: A prospective observational study. J. Thromb. Thrombolysis 2015, 39, 60–67. [Google Scholar] [CrossRef]
- Bakchoul, T.; Assfalg, V.; Zöllner, H.; Evert, M.; Novotny, A.; Matevossian, E.; Friess, H.; Hartmann, D.; Hron, G.; Althaus, K.; et al. Anti-platelet factor 4/heparin antibodies in patients with impaired graft function after liver transplantation. J. Thromb. Haemost. 2014, 12, 871–878. [Google Scholar] [CrossRef]
- Matsuo, T.; Motohashi, S.; Wanaka, K.; Walenga, J.M. Production of Anti-platelet Factor 4/Heparin Complex Antibodies After Cardiovascular Surgery. Clin. Appl. Thromb. Hemost. 2015, 21, 177–180. [Google Scholar] [CrossRef]
- Zhao, D.; Sun, X.; Yao, L.; Lin, H.; Li, J.; Zhao, J.; Zhang, Z.; Lun, L.; Zhang, J.; Li, M.; et al. The clinical significance and risk factors of anti-platelet factor 4/heparin antibody on maintenance hemodialysis patients: A two-year prospective follow-up. PLoS ONE 2013, 8, e62239. [Google Scholar] [CrossRef]
- Warkentin, T.E.; Sheppard, J.I.; Sun, J.C.; Jung, H.; Eikelboom, J.W. Anti-PF4/heparin antibodies and venous graft occlusion in postcoronary artery bypass surgery patients randomized to postoperative unfractionated heparin or fondaparinux thromboprophylaxis. J. Thromb. Haemost. 2013, 11, 253–260. [Google Scholar] [CrossRef]
- Satoh, T.; Tanaka, Y.; Okazaki, Y.; Kaburaki, J.; Ikeda, Y.; Kuwana, M. Heparin-dependent and -independent anti-platelet factor 4 autoantibodies in patients with systemic lupus erythematosus. Rheumatology 2012, 51, 1721–1728. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Anti-PF4 Antibody Syndrome | Immunological Assays | Functional Assays |
|---|---|---|
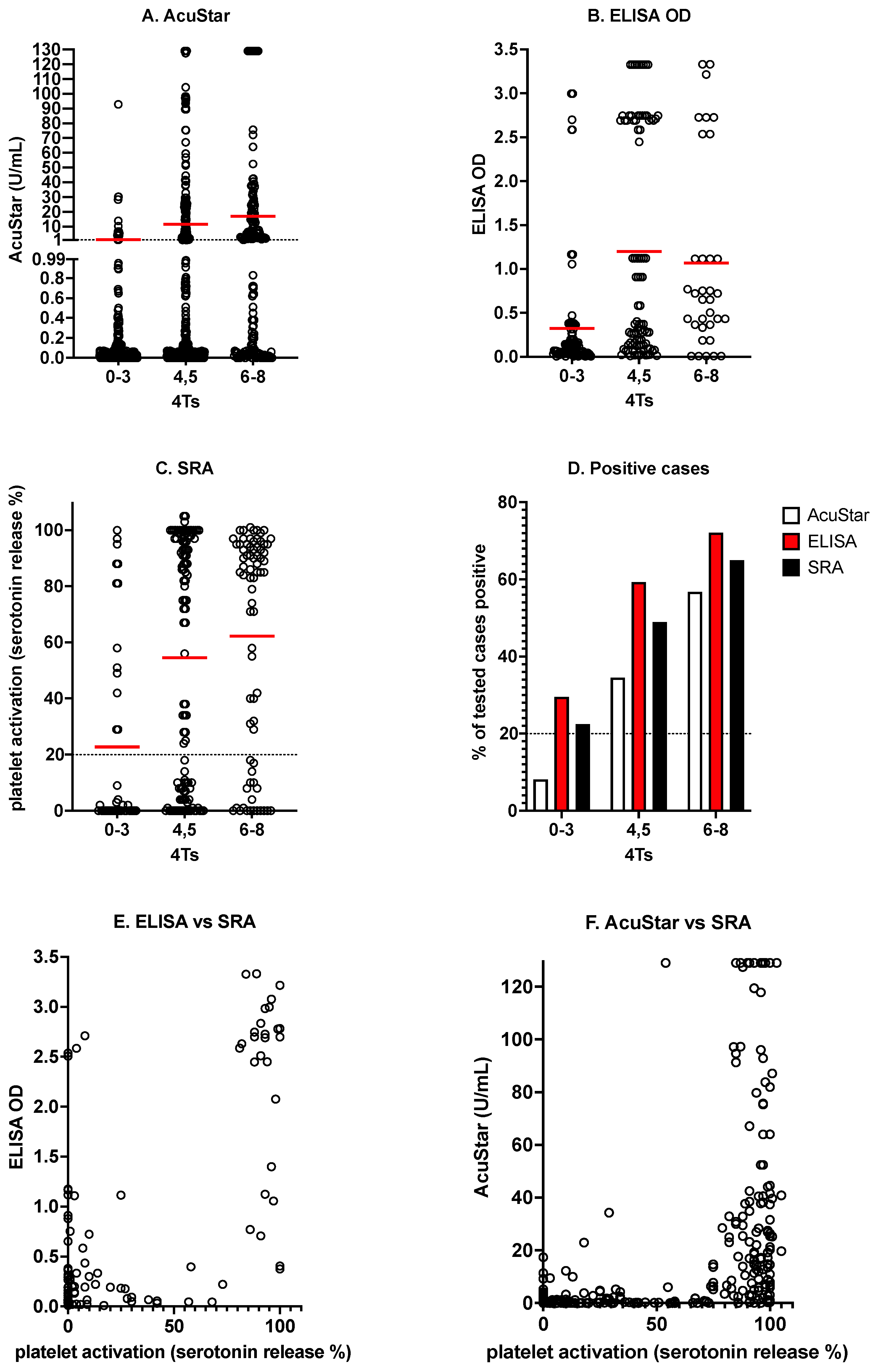
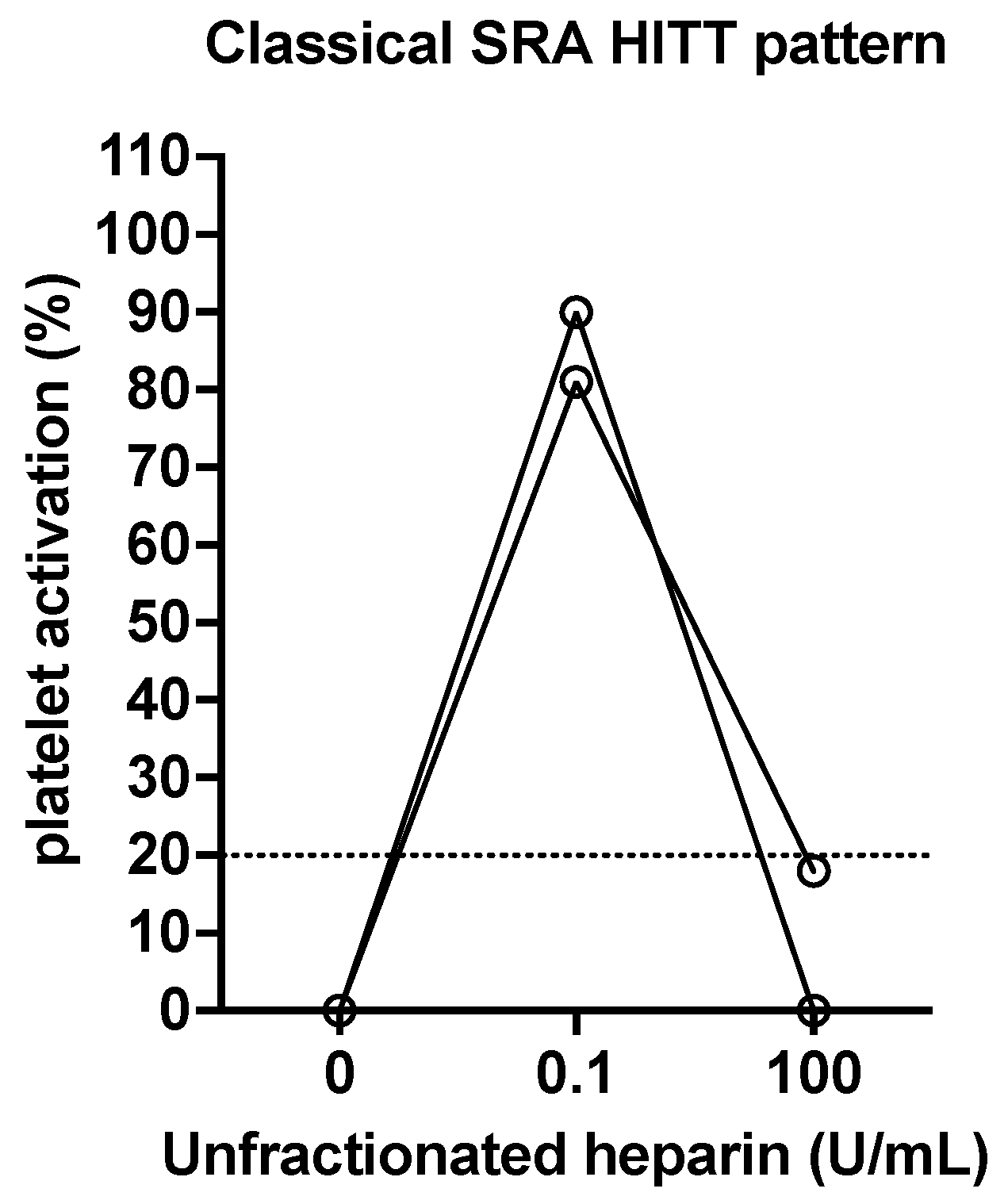
| Heparin-induced thrombocytopenia (HIT) (with thrombosis; HITT) | All anti-PF4 antibody assays expected to be positive | Expected to be positive in those with HITT (particularly in the presence of therapeutic heparin (e.g., 0.1 or 0.5 U/mL)), but not in those without pathological HIT. Negative in the presence of supratherapeutic heparin (e.g., 10 or 100 U/mL) |
| Spontaneous HIT-like syndrome | ELISA-based anti-PF4 antibody assays expected to be positive; insufficient information on other anti-PF4 antibody assays | Expected to be positive in the absence of therapeutic heparin. Negative in the presence of supratherapeutic heparin. |
| COVID-19 | ELISA-based anti-PF4 antibody assays expected to be positive; other anti-PF4 antibody assays also in general will be positive | Expected to be positive, but different findings may be evident in the presence or absence of therapeutic heparin, depending on the ‘trigger’ for antibody development. All cases should be negative in the presence of supratherapeutic heparin. |
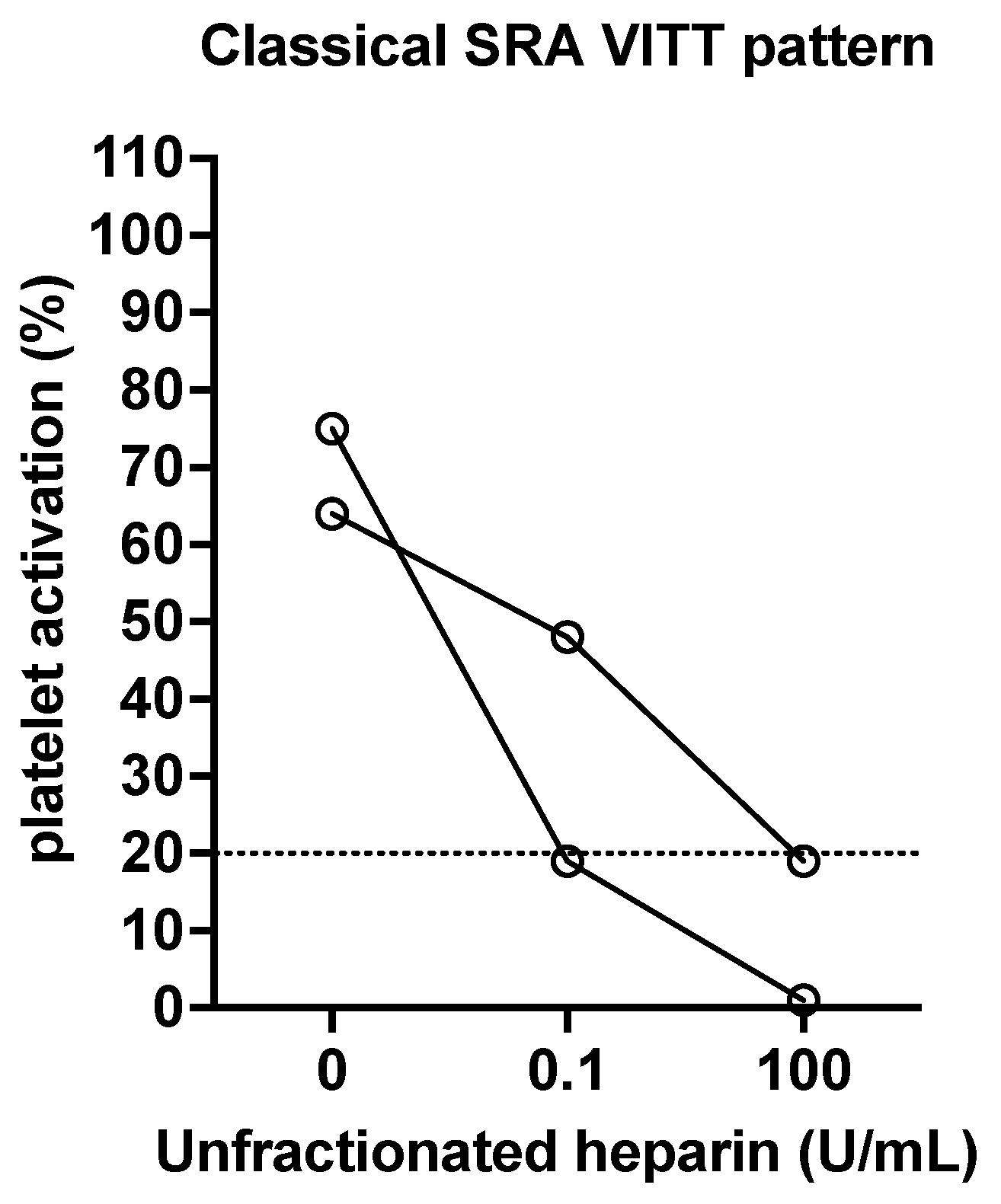
| VITT/TTS | ELISA-based anti-PF4 antibody assays expected to be positive; other anti-PF4 antibody assays, including rapid assays, expected to be generally negative | Expected to be positive in the absence of heparin. Most will show some inhibition in the presence of therapeutic heparin. All cases should be negative in the presence of supratherapeutic heparin. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Favaloro, E.J.; Pasalic, L.; Lippi, G. Antibodies against Platelet Factor 4 and Their Associated Pathologies: From HIT/HITT to Spontaneous HIT-Like Syndrome, to COVID-19, to VITT/TTS. Antibodies 2022, 11, 7. https://doi.org/10.3390/antib11010007
Favaloro EJ, Pasalic L, Lippi G. Antibodies against Platelet Factor 4 and Their Associated Pathologies: From HIT/HITT to Spontaneous HIT-Like Syndrome, to COVID-19, to VITT/TTS. Antibodies. 2022; 11(1):7. https://doi.org/10.3390/antib11010007
Chicago/Turabian StyleFavaloro, Emmanuel J., Leonardo Pasalic, and Giuseppe Lippi. 2022. "Antibodies against Platelet Factor 4 and Their Associated Pathologies: From HIT/HITT to Spontaneous HIT-Like Syndrome, to COVID-19, to VITT/TTS" Antibodies 11, no. 1: 7. https://doi.org/10.3390/antib11010007
APA StyleFavaloro, E. J., Pasalic, L., & Lippi, G. (2022). Antibodies against Platelet Factor 4 and Their Associated Pathologies: From HIT/HITT to Spontaneous HIT-Like Syndrome, to COVID-19, to VITT/TTS. Antibodies, 11(1), 7. https://doi.org/10.3390/antib11010007