1. Introduction
The United Nations established the Sustainable Development Goals (SDGs) in 2015, with the goal of ending poverty by the year 2030. Of the 17 goals, SDG 6 seeks to achieve universal, adequate, and equitable access to drinking water, sanitation, and hygiene. The World Health Organization (WHO) and United Nations Children’s Fund’s (UNICEF) Joint Monitoring Program (JMP) tracks the progress made toward achieving SDG 6 and noted that, as of 2023, the world is not on target to meet its water and sanitation goals. Achieving universal coverage by the year 2030 will necessitate a sixfold increase in drinking water access and a fivefold increase in sanitation [
1].
The consequences of insufficient access to improved water and sanitation are well-established, especially in relation to health. Inadequate water, sanitation, and hygiene caused an estimated 1.6 million deaths in 2016, accounting for 2.8% of total deaths; the majority of those deaths were from diarrheal diseases [
2]. Unimproved water and sanitation are also associated with child undernutrition, child mortality, increased maternal mortality, and respiratory infections [
3]. Zambia has some of the lowest levels of access to sanitation in Sub-Saharan Africa, and estimates suggest it loses 1.3% of its Gross Domestic Product every year because of poor sanitation [
4]. Russpatrick et al. [
5] suggest that inadequate sanitation contributes to the high rates of child stunting in rural Zambia. Additionally, unsafe water is the third largest cause of mortality in children under five years old in Zambia [
6].
Water and sanitation interventions can have many important impacts. In terms of health, they can lead to an increase in healthy life years [
7], reduced healthcare costs [
8], and fewer incidences of diarrhea, which reduces childhood malnutrition and pneumonia [
9]. The economic impacts include increased productive time as result of less time spent accessing water and sanitation services [
8] and fewer lost school days [
10]. The social impacts include reduced gender inequality and greater economic empowerment for women [
3] and a reduction in the risk of rape or physical assault [
10].
The maximum health gains come from piped water and sewer connections, but those interventions are the most expensive; disinfection of water supplies at the point of use has the lowest cost but still results in substantial health improvements [
7]. Even considering both the initial and annual running costs, a USD 1 investment in water and sanitation interventions returns between USD 5 to USD 46 [
8]. Mara et al. [
10] estimate that a reduction in water and sanitation-related diseases could save USD 7 billion a year in healthcare costs.
Despite the clear benefits of improved water and sanitation, interventions and improvements are not always successful and face significant spatial barriers. Effective community demand, local financing and cost recovery, and dynamic operation and maintenance are important factors for the sustainability of rural water and sanitation services [
11]. Mulenga et al. [
12] highlight wealth and location as important determinants of improved water and sanitation access. Additional facilitators in regard to the effective implementation of water and sanitation programs include a community’s effective engagement in interventions, increased investment in infrastructure, increased latrine ownership, and the development of social capital [
13].
Munamati et al. [
14] suggest that the failure of sanitation programs can be attributed to a lack of demand that comes from either contentment with the current situation, low income, an unwillingness to pay for services, a lack of political will, or a lack of citizen empowerment to ask for services. There is also a historical lack of demand for improved sanitation, with people either not using latrines or not maintaining them [
15]. Other barriers include environmental conditions, such as high water tables and sandy soils, that can lead to latrine collapse and a lack of tenure, which makes households unwilling to invest in sanitation improvements [
14]. Zuin et al. [
15] highlight a lack of funding for water and sanitation services, with rural areas being especially disadvantaged; they also note that a lack of affordable products and dysfunctional institutional arrangements are barriers to improvements. Additional barriers include climate change, low investment in water and sanitation infrastructure, low knowledge levels in regard to waterborne diseases, and ineffective local community engagement [
11]. Tseole et al. [
13] found that spatial inequalities are the most significant barrier to service provision in rural communities in southern Africa, including Zambia. Inequalities go beyond the urban–rural dichotomy [
16]; in fact, service coverage varies substantially between rural areas, as this study demonstrates.
This paper uses empirical data from four rural study sites to highlight two types of spatial barriers to improved water and sanitation in rural, western Zambia. The first barrier is the location in Zambia’s Western Province, a region with lower incomes and higher poverty rates compared to the capital of Lusaka, the country’s Copperbelt, and other parts of rural Zambia. Beyond the socioeconomic situation in this province, the rural nature of the study sites makes the provision of piped water and sanitation cost prohibitive. The second barrier is the location on a floodplain. During Zambia’s rainy seasons, residents of the study sites temporarily migrate to higher ground, which negatively impacts water and sanitation access, by necessitating changes in the water supply and increasing the rate of open defecation, since many latrines are either inaccessible or unusable. After situating Zambia within global and national water and sanitation policies, this paper uses household survey data to illustrate the implications of these barriers and offer context-specific recommendations to mitigate their impact. In particular, we advocate for the use of appropriate technology to ensure that policies consider the local situation in order to meet the basic needs of residents.
3. Methodology and Study Site
The Republic of Zambia is a landlocked country, situated in southern Africa, occupying a significant portion of the high Central African Plateau. Zambia’s climate is predominantly tropical, characterized by distinct wet and dry seasons, influenced by the seasonal movement of the Intertropical Convergence Zone. Zambia’s hydrography is dominated by the Zambezi River basin. Originating in northwestern Zambia, the Zambezi River is not only the source of the country’s name but also forms a significant portion of its southern border, notably featuring the iconic Victoria Falls (Mosi-oa-Tunya). This extensive river network, along with its numerous tributaries and associated wetlands, is crucial for Zambia’s water resources; it also presents challenges related to seasonal flooding and water management.
Zambia’s human geography is characterized by rapid population growth and a significant youth demographic. In 2024, the population growth rate in Zambia was estimated at 2.8%, placing it in the top 20 countries with the highest growth rates in the world [
22]. This growth contributes to a very young population, with approximately 42% under the age of 15 [
22]. Zambia’s development trajectory has been historically shaped by its substantial copper reserves. Periods of high global commodity prices have fueled economic growth, leading to its reclassification as a lower-middle income country in 2011 [
23]. However, periods of low global commodity prices equally stifle Zambia’s economic growth. Due to this economic downturn, Zambia was reclassified as a low-income country in 2022 [
23].
These structural vulnerabilities, coupled with governance challenges, have contributed to persistently high rates of poverty and profound income inequality. The World Bank reports that Zambia ranks sixth globally for both of these indicators. The disparity is particularly stark between urban and rural populations. Although 60% of the Zambian population lives in rural areas, these residents constitute a disproportionate 80% of the poor and 84% of the extremely poor, according to the 2022 Living Conditions Monitoring Survey by the Zambian Statistics Agency [
24]. These challenges are acutely felt in regions like Western Province, where our study sites are located, and where 80% of the population lives in poverty. These realities fuel widespread dissatisfaction among Zambians. An Afrobarometer survey revealed that 66% of respondents describe their personal living conditions as “fairly bad” or “very bad” [
25]. Specific to this study, access to clean water is a significant factor, as the same survey reported that 39% of respondents experienced insufficient clean water at least several times in the past year and Zambians identified “water supply” as the country’s second most pressing issue [
25].
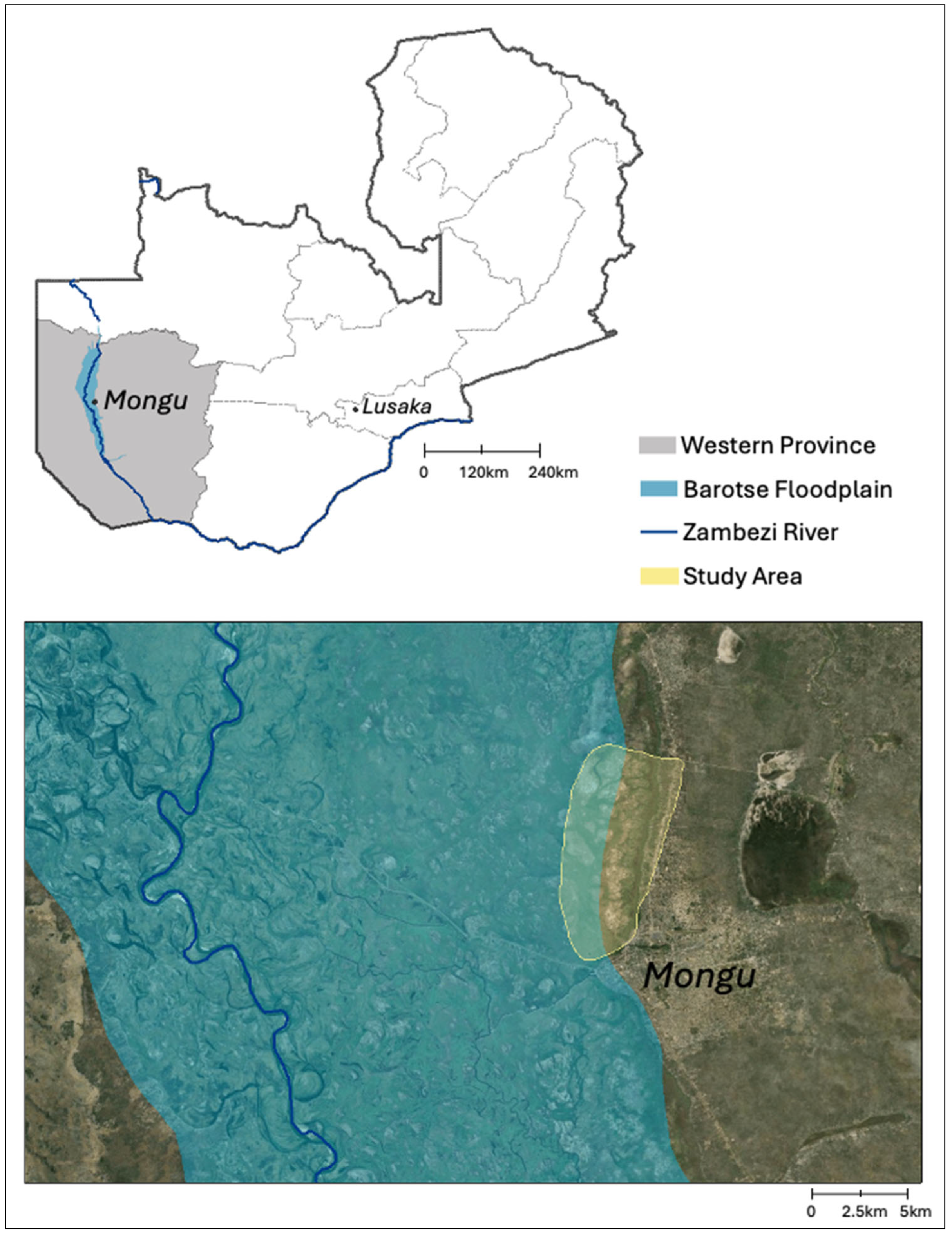
This project collected data on water and sanitation between June and August 2021, using household surveys. This study examines levels of water and sanitation access in four rural wards (Lealui, Mabumbu, Kanyonyo, and Katongo), located in the Barotse Floodplain in Mongu District (
Scheme 1). The primary considerations guiding ward selection included rurality and proximity to the Barotse Floodplain. Our examination of rural wards furthers the understanding of the unique infrastructural, logistical, and socioeconomic barriers to water and sanitation access prevalent in such settings. The inclusion of wards containing villages situated at contrasting elevations enables the analysis and discussion of the challenges and responses to seasonal flooding, including consideration of the impacts of inundation on water sources and sanitation facilities. The specific village names are not identified to protect the privacy of the research subjects. Surveys were conducted verbally in Lozi by a team of five trained research assistants who live in the area. They were trained and supervised by one of the authors.
We surveyed 362 adult heads of households. The respondents were selected within the four wards based on their availability and willingness to participate. The surveys were conducted at various times of the day (morning, afternoon, and evening) to ensure participation from a variety of residents, as the demographics of the sites vary depending on the time of day and their outside obligations, such as farming, marketing, or fetching water. A total of 218 of these respondents identified as female and 144 identified as male. A total of 112 respondents were under the age of 30, 123 were between the ages of 31 and 45, 63 were between the ages of 46 and 60, and 64 were over the age of 61. All of the respondents practiced subsistence agriculture, with common crops being rice, maize, sugar cane, sorghum, sweet potatoes, pumpkins, onions, and tomatoes. Many of the respondents also engaged in the sale of their surplus crops in local markets and in the nearby town of Mongu.
The surveys included demographic questions about the respondent’s age and length of residence and questions focused on water and sanitation access. Specifically, questions were asked about respondents’ sources of drinking water, drinking water access, the type of sanitation, their preferred type of sanitation, how water sources change seasonally, and how floods impact sanitation facilities. IRB approval was obtained through one author’s university and recognized by the other author’s institution. All the survey respondents provided verbal informed consent to participate, and all the risks and benefits of the research were fully explained to the respondents.
The study sites are located north of Mongu, the provincial capital of Western Province, Zambia (see
Scheme 1). Western Province lies approximately 600 km west of Zambia’s capital, Lusaka. Western Province has the lowest rates of access to water supplies and sanitation within the country (see
Table 3 and
Table 4). Additionally, the province has the highest poverty levels in Zambia, with 80% of the population living in poverty and 64% living in extreme poverty [
26].
Rural livelihoods in the area are intricately linked to the seasonal flooding of the Zambezi River. The extent of the Barotse Floodplain is highlighted on
Scheme 1 and it is the second largest wetland in Zambia. The rainy season in Barotse Plain begins in December and ends in May. Peak flooding occurs in April, about 3 months after peak rainfall; approximately 1500 mm of rain falls over the headwaters of the Zambezi annually [
27]. During the peak flooding period, the Barotse Plain is transformed into a large water reservoir, approximately 5–6 m in depth and covering an area of over 10,000 km
2 [
27]. It takes about 4 months for floods to recede from their maximum inundation [
26]. Most of the villages located in the plain have a corresponding high-ground village that people use during peak flooding. People return to the same village on higher ground each year, and it shares the same name as the village in the plain. For example, the village of Naloyela exists on the floodplain and on higher ground and is referred to as
Naloyela ya kwa plain and
Naloyela ya kwa ng’ambamo, respectively. Although some people have permanently relocated to higher ground to avoid the inconvenience of seasonal moves, they still travel to the plain daily to access their crops, cattle, and livelihoods. Climate change has affected the timing of the flood, with flooding happening both earlier and later; these changes make it difficult to prepare, including knowing when to relocate [
28]. The Intergovernmental Panel on Climate Change categorized the Zambezi as the river basin expected to face the worst potential effects of climate change among 11 major African basins [
29].
The floodplain is home to 33,000 people and 10,849 buildings [
28]. Since 1989, the amount of flooded cropland has increased from 9% to 73% and the number of flooded homes has increased from 6% to 47% [
28]. Communities throughout the Barotse Plain have developed sophisticated adaptation strategies to accommodate the shifting water levels, including the construction of homestead mounds (
mazulu), transportation and drainage canals, and adaptive agricultural practices. These adaptations include temporary migration to higher ground during floods, and reflect deep indigenous knowledge of the Zambezi, which is challenged by the pressures and impacts of climate change [
30]. Seasonal migration of people and livestock occurs in relation to the water levels and impacts the construction and reconstruction of sanitation facilities and sources of drinking water. The floods support the long-term cultivation of rice, maize, and vegetables throughout the floodplain, but they also lead to crop damage and food storage challenges if the flooding is severe or unpredictable. Climate change continues to alter the timing, duration, and intensity of floods and droughts, undermining traditional adaptation strategies, increasing food insecurity, and causing higher levels of socioeconomic vulnerability.
4. Results
4.1. Water
The participants were asked about their primary source of drinking water during the dry season. As seen in
Table 5, the majority of respondents (64%) drink unimproved water. Unimproved sources in the study area include unprotected wells and surface water sources.
Figure 1 provides some examples of common unimproved sources utilized throughout the study area.
Basic and limited water both come from improved sources. An improved source is one that has “the potential to deliver safe water by nature of their design and construction” [
1] (p. 96). Basic water involves a collection time of 30 min or less, while limited water collection times are greater than 30 min. Only a small portion (11%) of our respondents have a source of drinking water on their premises. Of those, only 3% had an improved source on their premises, with the others having an unprotected well. All the other respondents with improved water must walk to fetch it, including those with both limited and basic access.
For SDG monitoring, improved water sources are not tested to confirm their quality. When respondents who drink improved water were asked about its quality, the results were mixed. Of the 113 who drink improved water, 18 expressed concerns including its brown color, salty taste, the presence of sand and insects, and generally describing it as very poor and bad. Most of those complaints were in reference to groundwater and discoloration is caused by particulates in the water.
Most of our respondents (64%) drank unimproved water. Unprotected wells are generally hand dug, shallow, and either completely uncovered or partially covered by a removable piece of wood, metal, or a sandbag. Depending on the depth of the well, people use a rope or their hands to lower a container to collect water. Surface water refers to the Zambezi River and its tributaries, which are home to Nile crocodiles; crocodile attacks occur annually in the region. The quality of unimproved water is generally poor, with contamination by fecal matter, particulates, and even chemicals. High rates of open defecation, along with the presence of animals, such as cows, chickens, and dogs, means that unimproved water often contains E. coli and total coliforms. Although boiling and the use of chlorine can improve the quality, water treatment is not widespread because the cost of charcoal and purification tablets is prohibitive. All groundwater sources, whether improved or unimproved, have the potential for contamination from pit latrines. Zambia does not specify a required minimum distance between latrines and water sources. Although people try to separate them, the regular relocation of latrines due to flood damage can make it difficult to maintain proper distancing. These groundwater sources can also become contaminated by surface water during episodes of flooding.
Of the 90% of respondents that indicated they walk to collect their water, 16% spend more than 30 min on their round-trip collections, including walking, queuing, and filling their containers. Although most of those people with extended collection times use improved sources, including taps and boreholes, some spend a significant amount of time fetching unimproved water.
The annual flooding of the Barotse Plain presents unique challenges and considerations for water access. Of 362 participants, 45 indicated that their drinking water source changes between the dry and wet season. Of those, 44% switch to drinking surface water from the Zambezi River and the streams that feed it, while 42% begin drinking rainwater.
4.2. Sanitation
The participants were asked about their primary form of sanitation during the dry season. As seen in
Table 6, only 1% (just one person) uses a form of improved sanitation; all of the others use either unimproved sanitation or lack any form of sanitation and, thus, practice open defecation.
In many areas of Zambia, access to improved sanitation facilities remains limited, making pit latrines a common choice for households in rural areas. Pit latrines can be a form of improved sanitation if they are “designed to hygienically separate excreta from human contact” [
1] (p. 96). A slab composed of durable and easy to clean material is one way for pit latrines to be classified as improved. In our study sites, however, the latrines are unimproved. They are generally simple, hand-dug structures, typically approximately 2 m deep, lacking a slab and constructed using local materials (see
Figure 2).
A critical factor in our study area is the predominantly sandy soil, which makes pit latrines highly susceptible to collapse. To counter this possibility, the pit walls are lined using woven twine, sticks, and reeds. These pit liners are called
singangabela (see
Figure 3). Pit latrines in the region often lack a concrete slab because of the high cost of cement and instead use sandbags around the latrine opening for users to stand on (see
Figure 4). Given that the area is sand covered, residents collect the sand directly from their immediate surroundings and typically pack the sand into used cornmeal (mealie meal) bags. These bags are generally large, durable, woven polypropylene bags that are universally available in each household, as mealie meal is a staple food in Zambia. Although more affordable than a concrete slab, the possibility of the bags harboring bacteria makes these latrines a form of unimproved sanitation. The latrines in the region also incorporate a variety of shelters for privacy and shelter from the elements. Most often, the shelters are constructed using reeds and grass, but other materials, such as excess iron sheets, are used when available. The design generally aims to keep the interior relatively dark to discourage flies, while still allowing some airflow for ventilation.
The floodwaters of the Zambezi River impact sanitation practices, particularly the use and effectiveness of pit latrines. Pit latrines located in the floodplain are highly susceptible to being submerged during the rainy season, which can lead to the overflow of fecal matter and other waste, contaminating surface and groundwater sources. The flooding also makes latrines unusable. A total of 125 respondents said that they switch their form of sanitation during the rainy season. These changes occur because they have relocated to higher ground and because they need to construct a new latrine. Flooded areas do not lessen the practice of open defecation; in fact, eight respondents indicated they switch from latrines to open defecation during the rainy season.
5. Discussion
Although the world has experienced significant gains in water and sanitation access, progress has been uneven. Developed regions have better access than developing regions. Urban areas have better access than rural areas, and that gap is larger in Sub-Saharan Africa than other world regions. Higher income households have better access than lower income households. As the previous sections show, there is also disparity within these categories; our rural study area has much lower levels of water and sanitation access than rural Zambia as a whole. The following sections discuss various aspects of water and sanitation in our study area.
5.1. Water Fetching
The majority of survey respondents walk to fetch water. This finding is consistent with other parts of Sub-Saharan Africa, where more than 2/3 of the population fetches water from outside the home [
31]. Globally the burden of water collection falls to women and girls, and this burden is even more pronounced in rural areas [
32]. This burden can be measured in regard to time, distance, calorie expenditure, and opportunity costs [
33]. There is also a physical burden from carrying heavy vessels and walking on uneven terrain; water fetchers are also at risk of assaults, attacks, and being struck by vehicles [
33].
For those households that walk to fetch water, a round trip (including queuing) of 30 min or less is considered to be basic water access. Yet, a shorter walk does not necessarily mean a shorter overall time burden. Water is generally fetched in 20 L containers. The UN indicates that people require between 50 and 100 L of water per day to meet their personal and domestic needs [
34]. Given that the average household size in our survey is over five people, water fetchers must make multiple trips per day. In fact, one respondent explained that they made four trips per day, with each trip taking 30 min. The majority of respondents spending over 30 min per collection trip were women. The highest collection times of 7 h per day and 4 h per day were both experienced by women. Across Sub-Saharan Africa, women collect the majority of water on trips over 30 min in duration [
31].
5.2. Rainwater
The JMP classifies rainwater as an improved source of drinking water, but the type of collection practiced by our respondents raised some concerns. Most rainwater harvesting in Zambia follows a traditional ad hoc, low technology process [
35]. A study in urban Zambia found the presence of both total and fecal coliforms in rainwater samples, which was attributed to bird droppings, insects, and dust [
35].
Our participants collect rainwater via roof runoff, and the runoff is collected directly into an open container. Since all of the homes in the study area have thatched roofs, there is no concern about heavy metals in the water from corrugated iron roofs; there is, however, the possibility of fungal contamination during the rainy season. This rainwater is used for both drinking and household activities. This type of collection and storage presents the potential for microbial, fecal, or particulate contamination, which could have negative health impacts. There are specific actions that can be taken to improve the quality of harvested rainwater, such as not collecting water from the first rainfall event [
36]. Handia [
35] describes the process of a first flush, wherein collected water is discarded after the first rainfall event and the container is cleaned before collecting water again. Additionally, placing material on top of the container to filter out large contamination particles could help improve the quality of the rainwater collected. There is a lack of data on roof water quality in developing countries; there is a generalized notion that roof runoff is suitable for human consumption, but there is still a risk of contamination due to animal and plant activity [
37]. Still, of those participants that collect rainwater in this study, 79% perceive the quality as pure, clean, or good.
5.3. Unimproved Sanitation and Open Defecation
One target of the SDGs is to eliminate the practice of open defecation by 2030. In 2022, 193 million people practiced open defecation in Sub-Saharan Africa, which accounted for 46% of the world’s population without a form of sanitation [
1]. Open defecation is problematic not only in terms of its health impacts, but also its sociological impacts; women and girls who practice open defecation are more likely than men and boys to experience physical, sexual, or verbal assaults [
1]. Unimproved access to sanitation facilities can decrease personal safety, increase exposure to deadly pathogens, and is ultimately a violation of the human rights to water and sanitation.
Latrines located at a distance from residents’ homes, along with locked shared latrines, lead to open defecation [
38]. Likewise, some people do not like to be seen walking to or using a latrine, so may instead choose open defecation. Additionally, the practice persists because some people cannot afford a toilet [
39]. The construction of pit latrines can feel burdensome, due to the lack of both human and financial resources, which contributes to the prevalence of open defecation [
40,
41]. Bhatt et al. [
42] classified the reasons for open defecation in rural Nepal as either by choice or by compulsion. Those motivated by choice saw open defecation as a way to socialize and to enjoy the outdoors spiritually. Those motivated by compulsion either had no latrine at home or were unable to use their latrine due to cultural norms, such as the notion that women and men should not use the same latrine. Thus, they note that simply building new latrines is not necessarily enough to reduce open defecation.
Community-led total sanitation (CLTS) was developed to improve sanitation in rural areas of developing countries in a more effective and sustainable way. In Zambia, CLTS began in November 2011 as part of the Zambia Sanitation and Hygiene Programme [
4]. This program identified community champions that were trained to facilitate a triggering process that was “designed to persuade communities to realize that residents ‘eat their own feces’ because of poor hygiene and sanitation” [
41] (p. 553). As part of the triggering process, residents walk around their villages to identify areas of open defecation and collect feces. The behavior change around ending open defecation is facilitated by shame, disgust, peer pressure, and competition with other communities [
41]. The goal is to get villages to create sanitation committees to construct latrines and end open defecation. Zambia sought to have all latrines include a “a smooth cleanable floor, a lid to completely cover the hole, a structure that provides privacy and a handwashing station with water and soap or ash” [
5] (p. 437).
Zambia’s CLTS program led to an increase in the number of households with improved sanitation facilities, a decrease in the number of households with no sanitation facilities, and a decrease in households with someone practicing open defecation on a daily basis [
4]. Although many villages met the goal of ending open defecation, not all were able to sustain this progress, especially during the rainy season [
5].
There are several explanations for why people continue to use unimproved sanitation. Although development programs advocate improved sanitation for health reasons, people rarely use improved sanitation for that reason [
9]. Rather, their reasons for adopting improved sanitation include the “desire for privacy and to avoid embarrassment, wanting to be modern, the desire for convenience and to avoid the discomforts or dangers of the bush (e.g., snakes, pests, rain), and wanting social acceptance or status” [
10] (p. 3). The development policy distinction between improved and unimproved sanitation may be too simplistic and may not explain sanitation decisions [
38]. For example, a slab may not necessarily be cleaned regularly. Likewise, a private sanitation facility is not guaranteed to be safe or improved. Rather, the type of construction and the behavior of the users may be more important than the classification [
38].
In the Barotse Floodplain, unimproved sanitation and open defecation persist for multiple reasons. As noted previously, residents migrate seasonally to escape flood waters. Sanitation facilities located in the homes that are left behind are often damaged. Replacing or repairing an unimproved facility is more affordable than an improved one. There is also little appetite to construct an improved latrine at their temporary home, as abandoning it would not be cost effective. The following section further explains these economic considerations.
5.4. Preferred Sanitation
Even though unimproved sanitation is the reality for most of our participants, it is not necessarily preferred. When asked what their ideal form of sanitation would be, nearly all of the respondents (96%) expressed a desire for an improved facility. The respondents described this type of ideal sanitation as either a flushing toilet or a well-constructed latrine with cement or brick walls. Even if this type of facility was preferred, many acknowledged it was not feasible. One individual, who currently uses a pit latrine, specified they wanted a modern toilet, but do not have “enough money to acquire the toilet of my desire.” Another respondent, who uses a pit latrine, indicated they would like a modern toilet with a permanent brick structure, but noted that they build traditional toilets because they have no money. Another person, who currently has a pit latrine, wished for a modern flushing toilet, but indicated it was too expensive to construct and was well beyond what they could afford. Another individual, who currently uses a pit latrine, expressed a similar situation, stating that while they wished for a modern flushing toilet, they could not afford the equipment to construct it. Especially noteworthy was a response from an elderly woman who lacks a sanitation facility and, thus, practices open defecation. She indicated, “I do not need a toilet. What I need is someone to help me with the school fees of my grandchild. For toilets, I do not care.” Another individual who currently practices open defecation indicated that, “I do not need a toilet. We have the bush. What I want is food and money.”
The remaining respondents primarily practice open defecation and indicated that any type of toilet would be preferred but noted that a lack of money and resources prevents them from having one. One person expressed that, “there are all women in house, we cannot build a toilet and do not have money to pay people.” Additionally, eight people described a precarious situation of wanting to have an improved facility but being limited in their ability to act upon such a desire because they are renting the land they live on and, therefore, do not have the tenure security or financial ability to construct one.
5.5. Sanitation and Hygiene Knowledge
The respondents were asked whether they knew of any sanitation or hygiene programs in the area, and 71% indicated that there were such programs. They were aware of programs through healthcare facilities, the radio, at schools, and directly in their villages from healthcare workers. For those that were unaware of these programs, most thought they would be useful. Of those that are aware of such programs, the responses are mixed in regard to their outcomes. Some respondents saw improvements, such as reduced incidences of diarrhea, more handwashing facilities, increased numbers of latrines, and the use of soap during handwashing. However, others commented that there have been no improvements, either because of a lack of resources or ignorance.
The respondents were asked where sanitation and hygiene rank in terms of importance in regard to all of their daily challenges. Many noted that sanitation and hygiene are important for health, stating that they are either the top or one of the top issues. Still, some respondents indicated that other issues are more pressing. For example, one respondent commented that, “my worry is that I do not even have soap to bathe so how can I be able to use soap after the toilet?” Others commented that food is a much more important issue. One noted: “I don’t worry much about having toilets as it is because of having enough food that we need toilets. I need first food and then sanitation.”
Even those that acknowledge that sanitation and hygiene are the most pressing issues, they also acknowledge that it is not possible to address them: “These are the most important, but some things are just not possible. My parents cannot even afford my education and don’t think they can waste money to build a modern toilet.” Another respondent described constructing a toilet as a waste of money when meeting other needs is very expensive.
Thus, the “one-size-fits-all” approach of a permanent, dry land latrine might not be feasible in all areas. Educational materials focused on sustainable sanitation, including low-cost options, are imperative for success [
14]. In the Barotse Floodplain, additional education is needed, but it will be important to tailor it to the specific geography of the area to take into account the impacts of flooding, migration, and the high rates of poverty.
6. Conclusions
Water and sanitation are crucial for public health and are rightly considered a development priority, as evidenced by SDG 6 and numerous national policies and programs within Zambia. However, achieving equitable access remains a significant challenge on the ground. In western Zambia, the spatial barriers to equitable access are about much more than the distance from water or sanitation sources. Although the ideal of piped water and private, waste-treating toilets are often prioritized, those solutions are not always practical or attainable, especially in the context of the economic marginalization, poverty, and extensive seasonal flooding observed in this study area. For many of our respondents, immediate needs, such as food, family support, and education, often take priority over water and sanitation improvements. One respondent explained:
Hygiene and sanitation is very important as for our health is concerned. It protects us from diseases such as cholera, malaria, etc. We also value it. It’s just because of our economic status why we don’t practice it. We spend more time looking for money to buy food than getting the same to buy a singangabela for a toilet or buying toilet material.
The concerns about the practicality or reality of piped water and piped sewage should not lead to the suggestion that the only possible alternatives are fetching surface water and practicing open defecation. Rather, we can consider the role of appropriate technology in solving these water and sanitation problems. Murphy et al. [
43] stress that appropriate technology is always context specific in regard to the local conditions and emphasizes the importance of meeting basic needs in a sustainable way and with a goal of capacity building. They note that local conditions can vary within a community, so the focus should be on meeting basic needs through affordable and flexible technology that uses local resources and knowledge [
43]. In these study communities, appropriate technology will require thinking beyond the SDGs’ requirements of safely managed water and sanitation and instead striving for safe, affordable, and equitable solutions that meet people’s needs.
Mara [
44] describes multiple sanitation technologies that have been successfully applied in rural areas. Although some would be cost prohibitive, Arborloos offer an interesting possibility. These are shallow, short-life pit latrines that include a portable slab and a structure made from local materials. When full, the pit is covered with soil and a fruit tree is planted to provide food and income. A new pit is dug, and the slab and structure are reused. A similar process is practiced in our study area; the pits tend to be deeper, but the sandbags are reused, and either nut or fruit trees are planted. Adapting this practice to include a higher quality and easily cleaned slab would be beneficial. One possibility is to create a slab using 3D printing, if the technology evolves to make use of local materials and solar power [
45]. Another option is the creation of tiles from plastic bags; in Togo, sand is used in combination with plastic bags as part of a low-technology and low-capital process [
46].
Given the existing use of rainwater, finding ways to expand and improve this practice could improve water access. As previously discussed, the current practices are less than ideal, but a major limitation to safe expansion is the high cost of storage tanks. One potential alternative is to use local materials to create a wattle and daub container and then line it with plastic sheeting [
47]. The ideal situation would see fewer people drinking surface water and water from unprotected wells. The alternative of protected wells or boreholes, however, is expensive. Martinez-Santos et al. [
48] propose manual boreholes as a more cost-effective approach in rural areas of the developing world; they note an estimated cost of USD 5000–15000 for a mechanized borehole, USD 2500–
$8000 for a protected well, and USD 100–2500 for a manual borehole. Although likely out of economic reach for those in our study area, the possibilities offered by different technologies are promising.
Although Western Province’s marginalization in Zambia is a complex issue, a dedicated focus on Western Province’s explicit inclusion within Zambia’s national development priorities presents opportunities to mitigate some of the spatial barriers explored in this paper. Since its independence, national development planning in Zambia has been highly centralized, with limited consideration or consultation with local communities. Due to Western Province’s political and geographic isolation, this limited consultation has been determinantal to development in the province, generally, and to the provision of adequate water and sanitation systems, specifically. The unique environment here, characterized by seasonal flooding and migration, requires tailored development approaches that build on local knowledge of the Barotse Floodplain. The existing literature on flooding often either focuses on temporary displacements after extreme events or coping measures [
49]. These responses overlook the cyclical relocation strategies commonly practiced in our study area. Understanding these unique local realities, and the spatial barriers embedded therein, is essential for developing more effective and sustainable interventions. A shift towards more participatory planning and investment, rooted in the lived experiences and expertise of the Barotse people, is essential to addressing the persistent disparities and to make sustainable progress in regard to water and sanitation development in Western Province.









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}