
Challenges of Providing Safe Drinking Water in African Rural Communities: A Case Study on the Oio Region, Guinea-Bissau


Abstract
1. Introduction
2. Materials and Methods
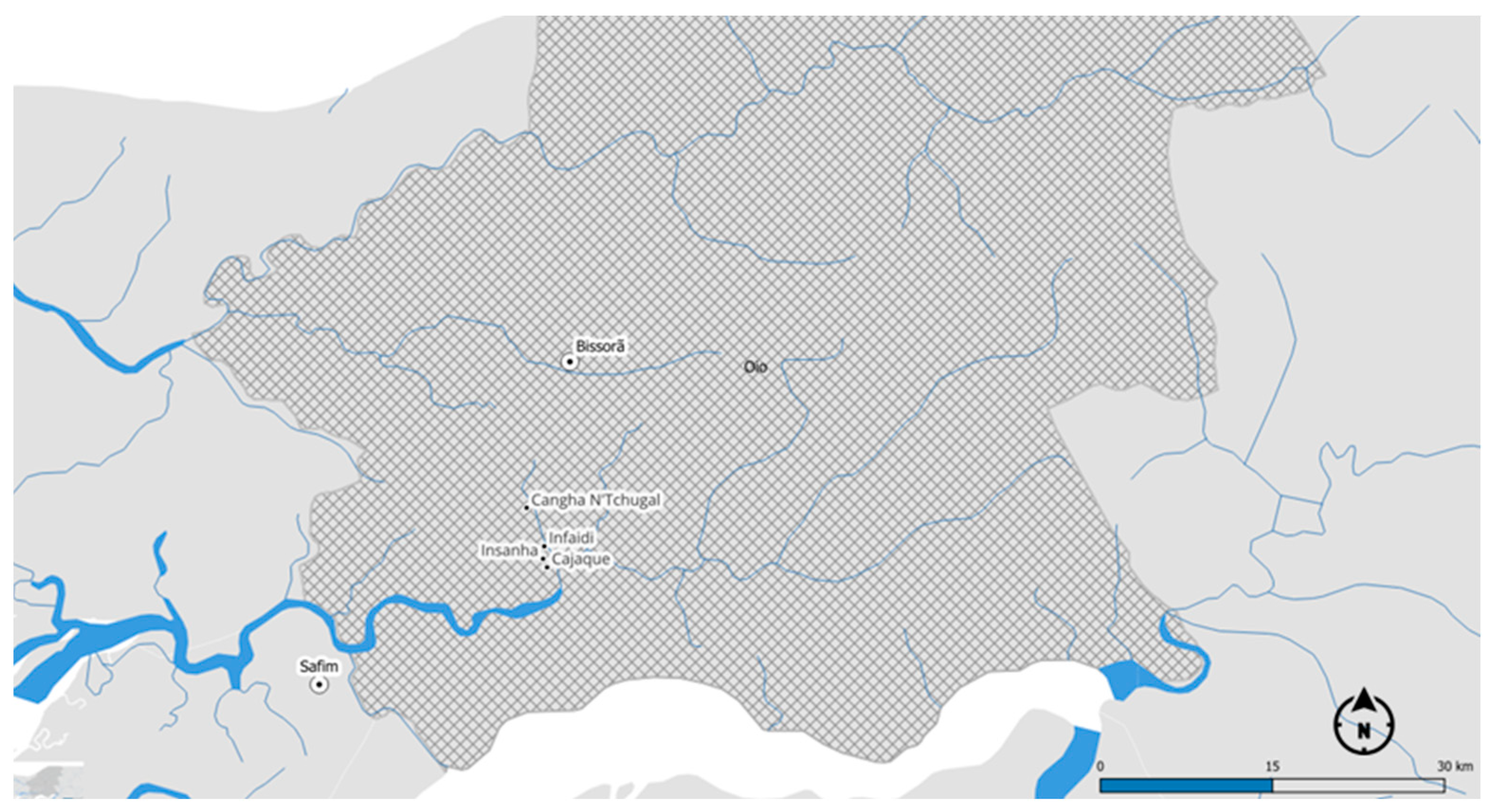
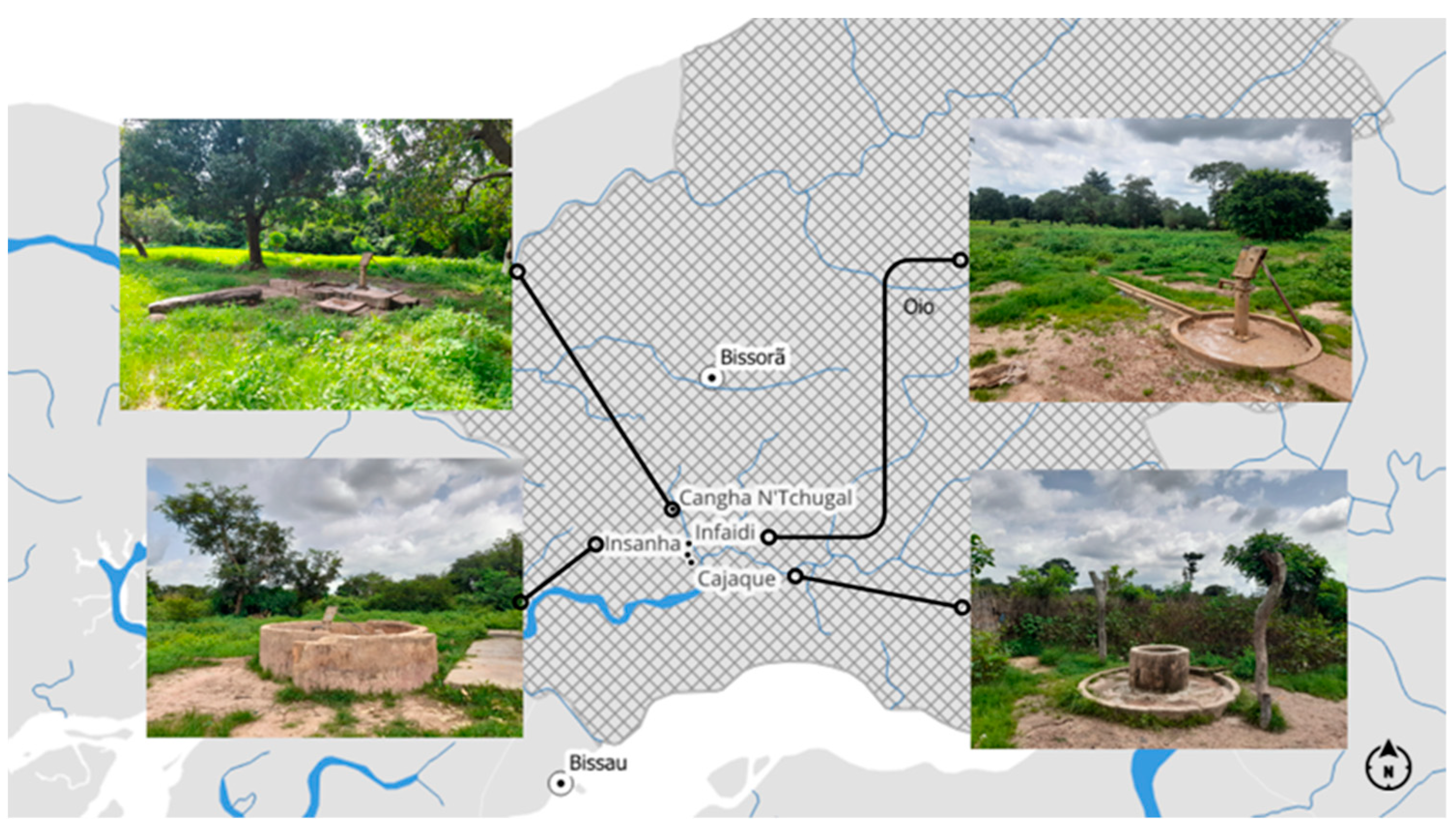
2.1. Study Area and Sampling Sites
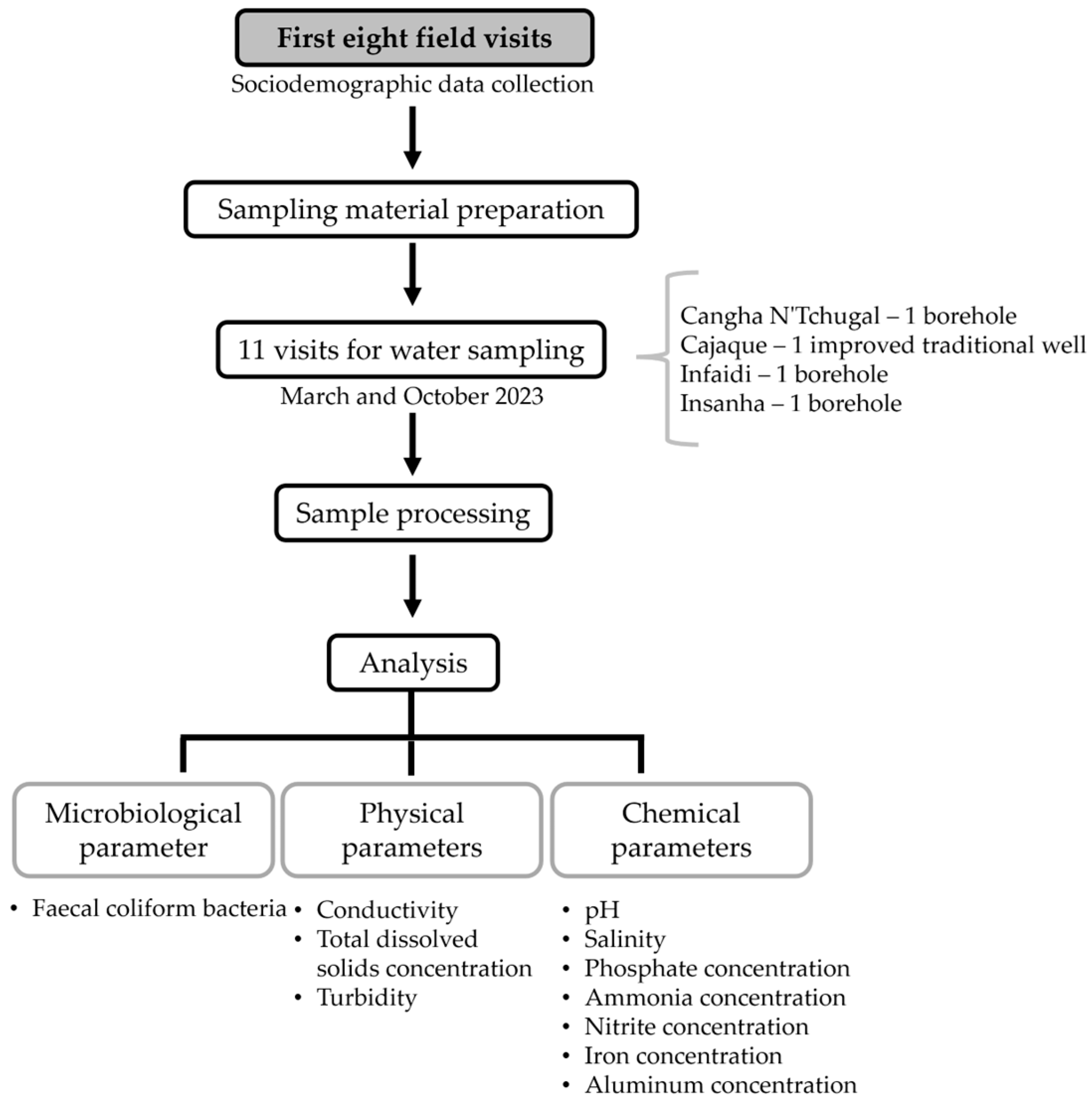
2.2. Sample Collection
2.3. Microbiological Procedures
2.4. Physicochemical Procedures
2.5. Analytical Procedures
3. Results
3.1. Sociodemographic Characterisation of the Study Population
3.2. Assessment of Water Availability and Existing Infrastructure
3.3. Assessment of Microbiological and Physicochemical Quality
3.3.1. Monitoring of Microbiological Parameters—Faecal Coliform Bacteria
3.3.2. Monitoring of Physical Parameters
3.3.3. Monitoring of Chemical Parameters
3.4. Evaluation of Seasonal Variation in Water Quality Parameters and Compliance with Recommended Standards
3.5. Determination of the Safe Water Indicator
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vieira, J.M.P. Água e Saúde Pública, 1st ed.; Sílabo Publishing: Lisbon, Portugal, 2018. [Google Scholar]
- Ogoamaka, E.M. Review of the Effects of Water Characteristics and Quality on Human Health. Int. J. Curr. Res. 2022, 5, 673–685. [Google Scholar] [CrossRef]
- UN-Water. Summary Progress Update 2021—SDG 6—Water and Sanitation for All. Geneva, Switzerland. 2021. Available online: https://www.unwater.org/publications/summary-progress-update-2021-sdg-6-water-and-sanitation-all (accessed on 11 April 2024).
- UN, United Nations. The United Nations World Water Development Report 2023: Partnerships and Cooperation for Water. UNESCO, Paris. 2023. Available online: https://www.unwater.org/publications/un-world-water-development-report-2023 (accessed on 3 April 2024).
- The Global Goals, Goal 6: Ensure Access to Water and Sanitation for All. Available online: https://www.globalgoals.org/goals/6-clean-water-and-sanitation/ (accessed on 16 April 2024).
- Naddeo, V. One Planet, One Health, One Future: The Environmental Perspective. Water Environ. Res. 2021, 93, 1472–1475. [Google Scholar] [CrossRef] [PubMed]
- Planetary Health Alliance Planetary Health. Available online: https://www.planetaryhealthalliance.org/planetary-health (accessed on 16 April 2024).
- UNICEF, United Nations Children’s Fund; WHO, World Health Organization. Progress on Household Drinking Water, Sanitation and Hygiene 2000–2022: Special Focus on Gender. New York, USA. 2023. Available online: https://washdata.org/reports/jmp-2023-wash-households (accessed on 10 February 2024).
- WHO, World Health Organization. Guidelines for Drinking-Water Quality: Fourth Edition Incorporating the First and Second Addenda. Geneva, Switzerland. 2023. Available online: https://www.who.int/publications/i/item/9789241549950 (accessed on 6 November 2023).
- Shah, A.; Arjunan, A.; Baroutaji, A.; Zakharova, J. A Review of Physicochemical and Biological Contaminants in Drinking Water and Their Impacts on Human Health. Water Sci. 2023, 16, 333–344. [Google Scholar] [CrossRef]
- Matthew, M.; Tainter, C.R. Escherichia Coli Infection; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Gray, N.F. Water Technology: An Introduction for Environmental Scientists and Engineers, 3rd ed.; IWA Publishing: London, UK, 2010. [Google Scholar]
- Saccò, M.; Mammola, S.; Altermatt, F.; Alther, R.; Bolpagni, R.; Brancelj, A.; Brankovits, D.; Fišer, C.; Gerovasileiou, V.; Griebler, C.; et al. Groundwater Is a Hidden Global Keystone Ecosystem. Glob. Chang. Biol. 2024, 30, e17066. [Google Scholar] [CrossRef]
- TESE—Associação para o Desenvolvimento (NGDO, Avenida do Brasil, 155 A, 1700–067 Lisbon, Portugal). Benchmark—Gestão e Concessão de Sistemas de Fornecimento de Água e Energia na Guiné-Bissau. Unpublished work. 2021. [Google Scholar]
- World Bank Guiné-Bissau—Aspectos Gerais. Bissau, Guinea-Bissau. 2023. Available online: https://www.worldbank.org/pt/country/guineabissau/overview (accessed on 25 November 2023).
- WHO, World Health Organization—Guinea-Bissau. Bissau, Guinea-Bissau. 2024. Available online: https://www.afro.who.int/pt/countries/guinea-bissau (accessed on 13 April 2024).
- UNDP, United Nations Development Programme. Human Development Report 2021/2022. New York, USA. 2022. Available online: https://hdr.undp.org/system/files/documents/global-report-document/hdr2021-22reportenglish_0.pdf (accessed on 3 November 2023).
- INE, National Institute of Statistics of Guinea-Bissau, Recenseamento Geral da População e Habitação de 2009. Bissau, Guinea-Bissau. Available online: https://www.stat-guinebissau.com/ (accessed on 9 January 2024).
- Ministry of Economy and Finance, General Directorate of Planning; INE, National Institute of Statistics of Guinea-Bissau. Inquérito aos Indicadores Múltiplos (MICS6) 2018–2019, Relatório Final; Bissau, Guinea-Bissau. 2020. Available online: https://www.unicef.org/guineabissau/pt/relatorios/inqu%C3%A9rito-aos-indicadores-m%C3%BAltiplos-2018-2019 (accessed on 24 April 2024).
- Aregu, M.B.; Kanno, G.G.; Ashuro, Z.; Alembo, A.; Alemayehu, A. Safe Water Supply Challenges for Hand Hygiene in the Prevention of COVID-19 in Southern Nations, Nationalities, and People’s Region (SNNPR), Ethiopia. Heliyon 2021, 7, e08430. [Google Scholar] [CrossRef] [PubMed]
- DelAgua Water Testing Ltd., DelAgua Portable Water Testing Kit User Manual. Marlborough, Wiltshire, UK. 2020. Available online: https://www.delagua.org/wp-content/uploads/2021/04/DelAgua-Manual-Revised-2020-V1.pdf (accessed on 12 December 2022).
- Hanna Instruments, HI 98129–HI 98130 Medidores de pH, EC/TDS & Temperature. Woonsocket, USA. 2019. Available online: https://www.hanna.pt/fichs/ficheiros/HI98129_HI98130.pdf (accessed on 12 December 2022).
- Thermo Fisher Scientific, TN-100 Waterproof Turbidimeter. Massachusetts, USA. 2015. Available online: https://www.thermofisher.com/order/catalog/product/ECTN100NOSTDS?SID=srch-srp-ECTN100NOSTDS (accessed on 15 December 2022).
- Lovibonad, Fotómetro MD600/MaxiDirect. Dortmund, Germany. 2017. Available online: https://lovibond.eu/downloads/instructions/md600,md610/ins_md600_gb_lovi.pdf (accessed on 12 December 2022).
- EU, European Union. Directive (EU) 2020/2184 of the European Parliament and of the Council of 16 December 2020 on the Quality of Water Intended for Human Consumption. Brussels, Belgium. 2020. Available online: https://eur-lex.europa.eu/legal-content/PT/TXT/PDF/?uri=CELEX:32020L2184 (accessed on 14 December 2023).
- ERSAR, Regulatory Entity for Water and Waste Services. RASARP 2023—Volume 2—Controlo da Qualidade da Água para Consumo Humano. Lisbon, Portugal. 2023. Available online: https://www.ersar.pt/pt/site-comunicacao/site-notas-a-imprensa/Paginas/rasarp-volume2-edicao2023.aspx (accessed on 24 April 2024).
- TESE—Associação para o Desenvolvimento (NGDO, Avenida do Brasil, 155 A, 1700–067 Lisbon, Portugal). Estudo Socioeconómico para Implementação de Serviços de Água e Energia. Unpublished work. 2021. [Google Scholar]
- Machado, A.; Bordalo, A.A. Diversity and Dynamics of the Vibrio Community in Well Water Used for Drinking in Guinea-Bissau (West Africa). Environ. Monit. Assess. 2014, 186, 5697–5709. [Google Scholar] [CrossRef]
- Machado, A.; Amorim, E.; Bordalo, A.A. Spatial and Seasonal Drinking Water Quality Assessment in a Sub-Saharan Country (Guinea-Bissau). Water 2022, 14, 1987. [Google Scholar] [CrossRef]
- Machado, A.; Bordalo, A.A. Analysis of the Bacterial Community Composition in Acidic Well Water Used for Drinking in Guinea-Bissau, West Africa. J. Environ. Sci. 2014, 26, 1605–1614. [Google Scholar] [CrossRef] [PubMed]
- Abu-Ashour, J.; Joy, D.M.; Lee, H.; Whiteley, H.R.; Zelin, S. Transport of microorganisms through soil. Water Air Soil Poll. 1994, 75, 141–158. [Google Scholar] [CrossRef]
- Boletim Oficial da República da Guiné-Bissau. Código das águas; Bissau, Guinea-Bissau. 1992. Available online: https://faolex.fao.org/docs/pdf/gbs39315.pdf (accessed on 26 April 2024).
- Ashuro, Z.; Aregu, M.B.; Kanno, G.G.; Negassa, B.; Soboksa, N.E.; Alembo, A.; Ararsa, E.; Badecha, F.; Tassew, S. Bacteriological Quality of Drinking Water and Associated Factors at the Internally Displaced People Sites, Gedeo Zone, Southern Ethiopia: A Cross-Sectional Study. Environ. Health Insights 2021, 15, 11786302211026469. [Google Scholar] [CrossRef] [PubMed]
- Mølbak, K.; Aaby, P.; Ingholt, L.; Højlyng, N.; Gottschau, A.; Andersen, H.; Brink, L.; Gansted, U.; Permin, A.; Vollmer, A.; et al. Persistent and acute diarrhea as the leading causes of child mortality in urban Guinea Bissau. Trans. R. Soc. Trop. Med. Hyg. 1992, 86, 216–220. [Google Scholar] [CrossRef]
- Bancessi, A.; Catarino, L.; Silva, M.J.; Ferreira, A.; Duarte, E.; Nazareth, T. Quality Assessment of Three Types of Drinking Water Sources in Guinea-Bissau. Int. J. Environ. Res. Public Health 2020, 17, 7254. [Google Scholar] [CrossRef] [PubMed]
- Bordalo, A.A.; Savva-Bordalo, J. The Quest for Safe Drinking Water: An Example from Guinea-Bissau (West Africa). Water Res. 2007, 41, 2978–2986. [Google Scholar] [CrossRef]
- Biai, I. Efeitos das Alterações Climáticas na Zona Costeira Noroeste da Guiné-Bissau. Master’s Thesis, Instituto Superior Técnico da Universidade de Lisboa, Lisbon, Portugal, 2009. [Google Scholar]
- IOM, Institute of Medicine. Global Issues in Water, Sanitation, and Health; The National Academies Press: Washington, DC, USA, 2009. [Google Scholar]
- Secretary of State for Environment and Sustainable Development. Second National Communication on Climate Changes in Guinea-Bissau. Bissau, Guinea-Bissau. 2011. Available online: https://unfccc.int/sites/default/files/resource/Complete_NC2.pdf (accessed on 20 November 2023).
- Kulinkina, A.V.; Plummer, J.D.; Chui, K.K.H.; Kosinski, K.C.; Adomako-Adjei, T.; Egorov, A.I.; Naumova, E.N. Physicochemical Parameters Affecting the Perception of Borehole Water Quality in Ghana. Int. J. Hyg. Environ. Health 2017, 220, 990–997. [Google Scholar] [CrossRef] [PubMed]
- Lamrani Alaoui, H.; Oufdou, K.; Mezrioui, N. Environmental Pollutions Impacts on the Bacteriological and Physicochemical Quality of Suburban and Rural Groundwater Supplies in Marrakesh Area (Morocco). Environ. Monit. Assess. 2008, 145, 195–207. [Google Scholar] [CrossRef]
- LNEG, Laboratório Nacional de Energia e Geologia, Carta Geológica da República da Guiné-Bissau. Lisbon, Portugal. 2015. Available online: https://geoportal.lneg.pt/pt/dados_abertos/cartografia_geologica/cartografiageologicainternacional/cartaguinebissau/ (accessed on 11 March 2024).
- Madilonga, R.T.; Edokpayi, J.N.; Volenzo, E.T.; Durowoju, O.S.; Odiyo, J.O. Water Quality Assessment and Evaluation of Human Health Risk in Mutangwi River, Limpopo Province, South Africa. Int. J. Environ. Res. Public Health 2021, 18, 6765. [Google Scholar] [CrossRef] [PubMed]
- Gebresilasie, K.G.; Berhe, G.G.; Tesfay, A.H.; Gebre, S.E. Assessment of Some Physicochemical Parameters and Heavy Metals in Hand-Dug Well Water Samples of Kafta Humera Woreda, Tigray, Ethiopia. Int. J. Anal. Chem. 2021, 2021, 8867507. [Google Scholar] [CrossRef]
- WHO, World Health Organization, Improved Sanitation Facilities and Drinking Water Sources. Available online: https://www.who.int/data/nutrition/nlis/info/improved-sanitation-facilities-and-drinking-water-sources (accessed on 12 April 2024).
- Papa, F.; Crétaux, J.F.; Grippa, M.; Robert, E.; Trigg, M.; Tshimanga, R.M.; Kitambo, B.; Paris, A.; Carr, A.; Fleischmann, A.S.; et al. Water Resources in Africa under Global Change: Monitoring Surface Waters from Space. Surv. Geophys. 2023, 44, 43–93. [Google Scholar] [CrossRef]
- Tambi, A.; Brighu, U.; Gupta, A.B. Methods for detection and enumeration of coliforms in drinking water: A review. Water Supply 2023, 23, 4047–4058. [Google Scholar] [CrossRef]
- Wang, H.; Wang, T.; Zhang, B.; Li, F.; Toure, B.; Omosa, I.B.; Chiramba, T.; Abdel-Monem, M.; Pradhan, M. Water and Wastewater Treatment in Africa—Current Practices and Challenges. CLEAN Soil Air Water 2014, 42, 1029–1035. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date | Locations | ||||
|---|---|---|---|---|---|
| Cangha Tchugal * | Cajaque * | Infaidi * | Insanha * | ||
| Dry season (December to May) | 01/March | SC | SC | SC | SC |
| 15/March | SC | SC | SC | SC | |
| 29/March | SC | SC | SC | SC | |
| 10/May | SC | SC | SC | SC | |
| Wet season (June to November) | 05/July | - | SC | - | SC |
| 09/August | SC | SC | - | SC | |
| 23/August | SC | SC | - | SC | |
| 01/September | SC | SC | SC | SC | |
| 06/September | - | - | SC | - | |
| 13/September | SC | - | SC | - | |
| 04/October | - | - | SC | - | |
| Locality | Parameter | Characterisation |
|---|---|---|
| Cangha N’Tchugal | Resident population | 457 inhabitants 65 households |
| Number of houses | 60 houses | |
| Accessibility | Dirty access roads, bad condition | |
| Commercial and religious infrastructures | 7 grocery stores 1 evangelical church | |
| Civil society | 2 community structures (youth and women’s groups) involved in agriculture/horticulture area | |
| School infrastructures | 1 school (first to seventh grade) | |
| Hygiene and sanitary practices | No toilets Open defecation is a common practice | |
| Cajaque | Resident population | 260 inhabitants 37 households |
| Number of houses | 50 houses | |
| Accessibility | Dirty access roads, bad condition | |
| Commercial and religious infrastructures | 1 grocery store | |
| Civil society | Women Farmers Group and NGO intervention in the agriculture sector, mainly in rice production | |
| School infrastructures | No schools | |
| Hygiene and sanitary practices | 3 traditional household toilets Open defecation is a common practice | |
| Infaidi | Resident population | 318 inhabitants 45 households |
| Number of houses | 53 houses | |
| Accessibility | Dirty access roads, bad condition | |
| Commercial and religious infrastructures | Without infrastructures | |
| Civil society | 2 community structures (youth and women’s groups) involved in agriculture/horticulture area | |
| School infrastructures | 1 school—Flora Gomes (teaching up to the ninth grade) | |
| Hygiene and sanitary practices | 13 traditional household toilets Open defecation is a common practice | |
| Insanha | Resident population | 126 inhabitants 18 households |
| Number of houses | 17 houses | |
| Accessibility | Dirty access roads, bad condition | |
| Commercial and religious infrastructures | Without infrastructures | |
| Civil society | 2 community structures (youth and women’s groups) involved in agriculture/horticulture area | |
| School infrastructures | No school | |
| Hygiene and sanitary practices | 1 traditional household toilet Open defecation is a common practice |
| Parameter | Locality | Season | Median Period of Study | Recommended Parametric Value (EU/WHO) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Dry | Wet | ||||||||
| Minimum | Maximum | Median | Minimum | Maximum | Median | ||||
| Faecal Coliforms (CFU/100 mL) | Cangha N’Tchugal | 0 | 0 | 0 | 2.0 | 9.0 | 3.0 | 0 | 0 |
| Cajaque | 26.0 | 40.0 | 29.0 | 38.0 | 50.0 | 50.0 | 39.0 | ||
| Infaidi | 1.0 | 22.0 | 5.0 | 10.0 | 50.0 | 35.5 | 16.0 | ||
| Insanha | 1.0 | 6.0 | 0.5 | 7.0 | 30.0 | 11.5 | 6.5 | ||
| Parameter | Locality | Season | Median Period of Study | Recommended Parametric Value (EU/WHO) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Dry | Wet | |||||||||
| Minimum | Maximum | Median | Minimum | Maximum | Median | |||||
| Physical parameters | Conductivity (μS/cm) | Cangha N’Tchugal (n = 8) | 31.0 | 73.0 | 56.0 | 35.0 | 60.0 | 36.0 | 38.5 | 2500.0 |
| Cajaque (n = 8) | 70.0 | 196.0 | 136.0 | 97.0 | 205.0 | 152.0 | 152.0 | |||
| Infaidi (n = 8) | 300.0 | 380.0 | 370.5 | 292.0 | 388.0 | 352.0 | 368.5 | |||
| Insanha (n = 8) | 314.0 | 418.0 | 346.5 | 94.0 | 456.0 | 252.5 | 346.5 | |||
| Total Dissolved Solids (ppm) | Cangha N’Tchugal (n = 8) | 15.0 | 43.0 | 32.5 | 17.0 | 31.0 | 23.5 | 27.5 | 1000.0 | |
| Cajaque (n = 8) | 44.0 | 96.0 | 81.5 | 63.0 | 102.0 | 78.5 | 78.5 | |||
| Infaidi (n = 8) | 150.0 | 185.0 | 181.0 | 169.0 | 208.0 | 182.5 | 181.5 | |||
| Insanha (n = 8) | 161.0 | 209.0 | 183.0 | 33.0 | 218.0 | 118.0 | 178.5 | |||
| Turbidity (NTU) | Cangha N’Tchugal (n = 8) | 0.1 | 0.3 | 0.2 | 0.1 | 0.2 | 0.1 | 0.1 | 5.0 | |
| Cajaque (n = 8) | 1.1 | 2.0 | 1.7 | 0.8 | 9.0 | 3.3 | 1.7 | |||
| Infaidi (n = 8) | 5.5 | 15.8 | 7.5 | 44.8 | 66.3 | 58.2 | 30.3 | |||
| Insanha (n = 8) | 1.1 | 2.3 | 2.1 | 0.5 | 4.0 | 2.3 | 2.1 | |||
| Chemical parameters | pH | Cangha N’Tchugal (n = 8) | 4.7 | 5.0 | 4.9 | 4.9 | 5.1 | 5.0 | 5.0 | ≥6.5 and ≤9.5 |
| Cajaque (n = 8) | 5.1 | 5.6 | 5.4 | 4.9 | 5.7 | 5.4 | 5.4 | |||
| Infaidi (n = 8) | 6.4 | 6.6 | 6.6 | 6.5 | 6.7 | 6.6 | 6.6 | |||
| Insanha (n = 8) | 6.6 | 6.7 | 6.7 | 5.0 | 6.9 | 6.0 | 6.7 | |||
| Salinity (g/L) | Cangha N’Tchugal (n = 8) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.2 | |
| Cajaque (n = 8) | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | 0.1 | |||
| Infaidi (n = 8) | 0.2 | 0.2 | 0.2 | 0.1 | 0.2 | 0.2 | 0.2 | |||
| Insanha (n = 8) | 0.2 | 0.2 | 0.2 | 0 | 0.2 | 0.1 | 0.2 | |||
| Phosphates (mg/L) | Cangha N’Tchugal (n = 4) | 0 | 0 | 0 | 0.09 | 0.2 | 0.1 | 0.05 | 0.2 | |
| Cajaque (n = 4) | 0.1 | 0.1 | 0.1 | 0.3 | 0.4 | 0.3 | 0.2 | |||
| Infaidi (n = 6) | 0.8 | 1 | 0.9 | 0.5 | 0.8 | 0.6 | 0.8 | |||
| Insanha (n = 4) | 0.3 | 0.4 | 0.4 | 0.3 | 0.3 | 0.3 | 0.3 | |||
| Ammonia (mg/L) | Cangha N’Tchugal (n = 4) | 0.05 | 0.06 | 0.06 | 0.06 | 0.09 | 0.08 | 0.06 | 0.5 | |
| Cajaque (n = 4) | 0.04 | 0.06 | 0.1 | 0.05 | 1.0 | 0.5 | 0.1 | |||
| Infaidi (n = 6) | 0.3 | 0.3 | 0.3 | 0.2 | 0.4 | 0.3 | 0.3 | |||
| Insanha (n = 4) | 0.2 | 0.2 | 0.2 | 0.03 | 0.1 | 0.1 | 0.1 | |||
| Nitrites (mg/L) | Cangha N’Tchugal (n = 4) | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0.5 | |
| Cajaque (n = 4) | 0 | 0 | 0 | 0 | 0.01 | 0.01 | 0 | |||
| Infaidi (n = 6) | 0 | 0 | 0 | 0 | 0.5 | - | 0 | |||
| Insanha (n = 4) | 0 | 0 | 0 | 0 | 0.01 | 0 | 0 | |||
| Iron (mg/L) | Cangha N’Tchugal (n = 5) | 0.2 | 0.3 | 0.3 | 0 | 0.2 | 0.1 | 0.1 | 0.02 | |
| Cajaque (n = 6) | 0.4 | 0.6 | 0.5 | 0.1 | 0.2 | 0.1 | 0.1 | |||
| Infaidi (n = 7) | 3.0 | 3.0 | 3.0 | 3.5 | 4.9 | 3.7 | 3.5 | |||
| Insanha (n = 5) | 0.05 | 0.09 | 0.07 | 0.02 | 0.07 | 0.07 | 0.07 | |||
| Aluminium (mg/L) | Cangha N’Tchugal (n = 4) | 0.05 | 0.06 | 0.06 | 0.03 | 0.03 | 0.03 | 0.04 | 0.2 | |
| Cajaque (n = 4) | 0.05 | 0.06 | 0.1 | 0.02 | 0.07 | 0.05 | 0.1 | |||
| Infaidi (n = 6) | 0.01 | 0.01 | 0.01 | 0.02 | 0.03 | 0.02 | 0.02 | |||
| Insanha (n = 4) | 0 | 0 | 0 | 0 | 0.01 | 0.01 | 0 | |||
| Parameter | Percentage of Analyses Meeting the Recommended Parametric Values | Average Value per Parameter over the Study Period | |||
|---|---|---|---|---|---|
| Cangha N’Tchugal | Cajaque | Infaidi | Insanha | ||
| Faecal coliforms (CFU/100 mL) | 63.0% | 0% | 0% | 25.0% | 22.0% |
| Conductivity (μS/cm) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| pH | 0% | 0% | 75.0% | 75.0% | 38.0% |
| Total dissolved solids (ppm) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Turbidity (NTU) | 100.0% | 88.0% | 0% | 100.0% | 72.0% |
| pH | 0% | 0% | 75.0% | 75.0% | 38.0% |
| Salinity (g/L) | 100.0% | 100.0% | 13.0% | 25.0% | 59.0% |
| Phosphates (mg/L) | 100.0% | 50.0% | 0% | 0% | 38.0% |
| Ammonia (mg/L) | 100.0% | 75.0% | 100.0% | 100.0% | 94.0% |
| Nitrites (mg/L) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Iron (mg/L) | 67.0% | 67.0% | 0% | 100.0% | 58.0% |
| Aluminium (mg/L) | 100.0% | 100.0% | 100.0% | 100.0% | 100.0% |
| Average value per locality over the study period | 85.0% | 71.0% | 53.0% | 75.0% | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silveira, P.; Rebelo, M.T.; Salvador, D. Challenges of Providing Safe Drinking Water in African Rural Communities: A Case Study on the Oio Region, Guinea-Bissau. Water 2024, 16, 3621. https://doi.org/10.3390/w16243621
Silveira P, Rebelo MT, Salvador D. Challenges of Providing Safe Drinking Water in African Rural Communities: A Case Study on the Oio Region, Guinea-Bissau. Water. 2024; 16(24):3621. https://doi.org/10.3390/w16243621
Chicago/Turabian StyleSilveira, Pedro, Maria Teresa Rebelo, and Daniel Salvador. 2024. "Challenges of Providing Safe Drinking Water in African Rural Communities: A Case Study on the Oio Region, Guinea-Bissau" Water 16, no. 24: 3621. https://doi.org/10.3390/w16243621
APA StyleSilveira, P., Rebelo, M. T., & Salvador, D. (2024). Challenges of Providing Safe Drinking Water in African Rural Communities: A Case Study on the Oio Region, Guinea-Bissau. Water, 16(24), 3621. https://doi.org/10.3390/w16243621