
Health and Economic Benefits of Accelerating the PM10 Interim Targets in Brazil’s New Air Quality Resolution: A Case Study in Southern Brazil

 ,
,  , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
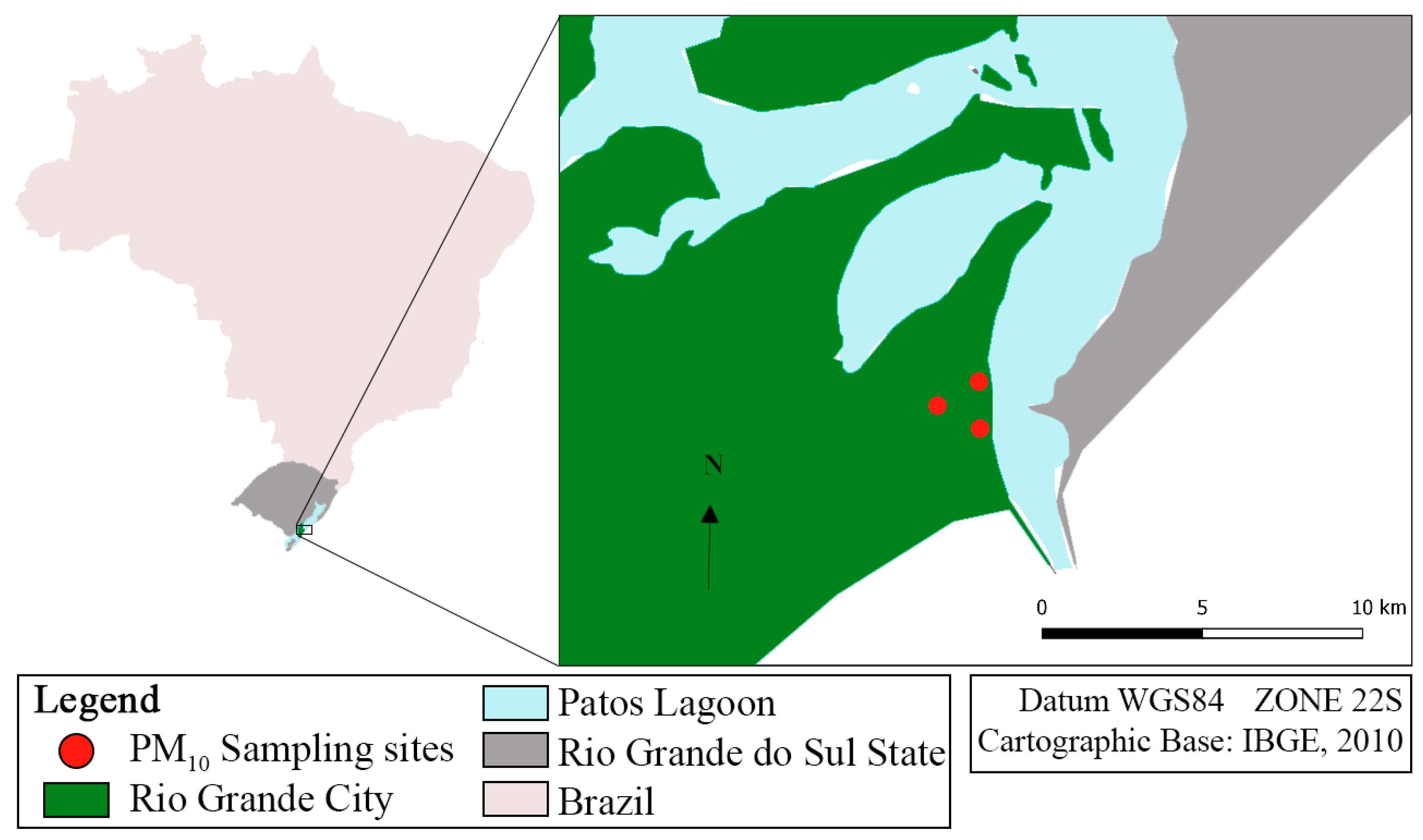
2.1. The Study Area
2.2. The Sampling Procedure and Monitoring Period
2.3. Health Data Acquisition
2.4. The Health Impact Assessment
2.5. The Economic Cost Assessment
2.6. Mortality Attributable to Air Pollution
3. Results and Discussion

{kind=link}
| Respiratory Hospitalizations | Cardiac Hospitalization | |||||
|---|---|---|---|---|---|---|
| Scenario | Original Year | Years Advanced | Avoided | Savings (BRL) | Avoided | Savings (BRL) |
| 30 µg/m3 | 2033 | 8 | 395 | 583,301.82 | 238 | 542,390.90 |
| 20 µg/m3 | 2044 | 19 | 1398 | 2,068,177.66 | 844 | 1,925,761.64 |
| 15 µg/m3 | 2055 | 30 | 2568 | 3,797,969.28 | 1551 | 3,540,607.29 |
| Scenario | Original Year | Years Advanced | Annual Non-External Deaths Avoided | Total Non-External Deaths Avoided |
|---|---|---|---|---|
| 30 µg/m3 | 2033 | 8 | 22 | 173 |
| 20 µg/m3 | 2044 | 19 | 32 | 614 |
| 15 µg/m3 | 2055 | 30 | 38 | 1128 |
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PM10 | Coarse particulate matter with an aerodynamic diameter of less than 10 μm |
| CONAMA | National Environment Council |
| WHO | World Health Organization |
References
- Brauer, M.; A Roth, G.; Aravkin, A.Y.; Zheng, P.; Abate, K.H.; Abate, Y.H.; Abbafati, C.; Abbasgholizadeh, R.; Abbasi, M.A.; Abbasian, M.; et al. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2162–2203. [Google Scholar] [CrossRef]
- Health Effects Institute. State of Global Air 2024. Special Report; Health Effects Institute: Boston, MA, USA, 2024; Available online: https://www.stateofglobalair.org/resources/report/state-global-air-report-2024 (accessed on 26 December 2024).
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and Health Impacts of Air Pollution: A Review. Front. Public Health 2020, 8, 14. [Google Scholar] [CrossRef]
- Feng, W.; Li, H.; Wang, S.; Van Halm-Lutterodt, N.; An, J.; Liu, Y.; Liu, M.; Wang, X.; Guo, X. Short-term PM10 and emergency department admissions for selective cardiovascular and respiratory diseases in Beijing, China. Sci. Total Environ. 2019, 657, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Bălă, G.-P.; Râjnoveanu, R.-M.; Tudorache, E.; Motișan, R.; Oancea, C. Air pollution exposure—The (in)visible risk factor for respiratory diseases. Environ. Sci. Pollut. Res. 2021, 28, 19615–19628. [Google Scholar] [CrossRef]
- Tahery, N.; Geravandi, S.; Goudarzi, G.; Shahriyari, H.A.; Jalali, S.; Mohammadi, M.J. Estimation of PM10 pollutant and its effect on total mortality (TM), hospitalizations due to cardiovascular diseases (HACD), and respiratory disease (HARD) outcome. Environ. Sci. Pollut. Res. 2021, 28, 22123–22130. [Google Scholar] [CrossRef]
- Liu, S.; Wang, L.; Zhou, L.; Li, W.; Pu, X.; Jiang, J.; Chen, Y.; Zhang, L.; Qiu, H. Differential effects of fine and coarse particulate matter on hospitalizations for ischemic heart disease: A population-based time-series analysis in Southwestern China. Atmos. Environ. 2020, 224, 117366. [Google Scholar] [CrossRef]
- Chen, R.; Yin, P.; Meng, X.; Wang, L.; Liu, C.; Niu, Y.; Liu, Y.; Liu, J.; Qi, J.; You, J.; et al. Associations between coarse particulate matter air pollution and cause-specific mortality: A nationwide analysis in 272 Chinese cities. Environ. Health Perspect. 2019, 127, 17008. [Google Scholar] [CrossRef] [PubMed]
- Tran, H.M.; Tsai, F.-J.; Lee, Y.-L.; Chang, J.-H.; Chang, L.-T.; Chang, T.-Y.; Chung, K.F.; Kuo, H.-P.; Lee, K.-Y.; Chuang, K.-J.; et al. The impact of air pollution on respiratory diseases in an era of climate change: A review of the current evidence. Sci. Total. Environ. 2023, 898, 166340. [Google Scholar] [CrossRef] [PubMed]
- Jin, T.; Di, Q.; Réquia, W.J.; Yazdi, M.D.; Castro, E.; Ma, T.; Wang, Y.; Zhang, H.; Shi, L.; Schwartz, J. Associations between long-term air pollution exposure and the incidence of cardiovascular diseases among American older adults. Environ. Int. 2022, 170, 107594. [Google Scholar] [CrossRef]
- Renzi, M.; Badaloni, C.; Trentalange, A.; Porta, D.; Davoli, M.; Michelozzi, P. Association between air pollution, socioeconomic inequalities and cause specific mortality in a large administrative cohort in a contaminated site of central Italy. Atmos. Environ. 2025, 347, 121082. [Google Scholar] [CrossRef]
- Jbaily, A.; Zhou, X.; Liu, J.; Lee, T.-H.; Kamareddine, L.; Verguet, S.; Dominici, F. Air pollution exposure disparities across US population and income groups. Nature 2022, 601, 228–233. [Google Scholar] [CrossRef]
- Rentschler, J.; Leonova, N. Global air pollution exposure and poverty. Nat. Commun. 2023, 14, 4432. [Google Scholar] [CrossRef]
- Fairburn, J.; Schüle, S.A.; Dreger, S.; Hilz, L.K.; Bolte, G. Social inequalities in exposure to ambient air pollution: A systematic review in the WHO european region. Int. J. Environ. Res. Public Health 2019, 16, 3127. [Google Scholar] [CrossRef] [PubMed]
- Maung, T.Z.; Bishop, J.E.; Holt, E.; Turner, A.M.; Pfrang, C. Indoor air pollution and the health of vulnerable groups: A systematic review focused on particulate matter (PM), volatile organic compounds (VOCs) and their effects on children and people with pre-existing lung disease. Int. J. Environ. Res. Public Health 2022, 19, 8752. [Google Scholar] [CrossRef]
- Wu, K.; Ho, H.C.; Su, H.; Huang, C.; Zheng, H.; Zhang, W.; Tao, J.; Hossain, M.Z.; Zhang, Y.; Hu, K.; et al. A systematic review and meta-analysis of intraday effects of ambient air pollution and temperature on cardiorespiratory morbidities: First few hours of exposure matters to life. EBioMedicine 2022, 86, 104327. [Google Scholar] [CrossRef] [PubMed]
- Urbanowicz, T.; Skotak, K.; Olasińska-Wiśniewska, A.; Filipiak, K.J.; Bratkowski, J.; Wyrwa, M.; Sikora, J.; Tyburski, P.; Krasińska, B.; Krasiński, Z.; et al. Long-Term Exposure to PM10 Air Pollution Exaggerates Progression of Coronary Artery Disease. Atmosphere 2024, 15, 216. [Google Scholar] [CrossRef]
- Wang, S.; Song, R.; Xu, Z.; Chen, M.; Di Tanna, G.L.; Downey, L.; Jan, S.; Si, L. The costs, health and economic impact of air pollution control strategies: A systematic review. Glob. Health Res. Policy 2024, 9, 30. [Google Scholar] [CrossRef] [PubMed]
- Ye, T.; Guo, S.; Xie, Y.; Chen, Z.; Abramson, M.J.; Heyworth, J.; Hales, S.; Woodward, A.; Bell, M.; Guo, Y.; et al. Health and related economic benefits associated with reduction in air pollution during COVID-19 outbreak in 367 cities in China. Ecotoxicol. Environ. Saf. 2021, 222, 112481. [Google Scholar] [CrossRef]
- Castro, A.; Künzli, N.; Götschi, T. Health benefits of a reduction of PM10 and NO2 exposure after implementing a clean air plan in the Agglomeration Lausanne-Morges. Int. J. Hyg. Environ. Health 2017, 220, 829–839. [Google Scholar] [CrossRef] [PubMed]
- Mebrahtu, T.F.; Santorelli, G.; Yang, T.C.; Wright, J.; Tate, J.; McEachan, R.R. The effects of exposure to NO2, PM2.5 and PM10 on health service attendances with respiratory illnesses: A time-series analysis. Environ. Pollut. 2023, 333, 122123. [Google Scholar] [CrossRef] [PubMed]
- Khoshnevis Yazdi, S.; Khanalizadeh, B. Air pollution, economic growth and health care expenditure. Econ. Res.-Ekon. Istraž. 2017, 30, 1181–1190. [Google Scholar] [CrossRef]
- National Environment Council (CONAMA), Ministry of Environment and Climate Change, Brazil. CONAMA Resolution no 3, of June 28, 1990. Provides for Air Quality Standards, as Stipulated in PRONAR. 1990. Available online: https://conama.mma.gov.br/?option=com_sisconama&task=arquivo.download&id=100 (accessed on 26 December 2024).
- Tavella, R.A.; de Moura, F.R.; Miraglia, S.G.E.K.; da Silva Júnior, F.M.R. A New Dawn for Air Quality in Brazil. Lancet Planet. Health 2024, 8, e717–e718. [Google Scholar] [CrossRef]
- National Environment Council (CONAMA), Ministry of Environment and Climate Change, Brazil. CONAMA Resolution N. 491, of November 19, 2018. Provides for Air Quality Standards. 2018. Available online: https://conama.mma.gov.br/?option=com_sisconama&task=arquivo.download&id=766 (accessed on 26 December 2024).
- World Health Organization (WHO). WHO Global Air Quality Guidelines: Particulate matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide. World Health Organization. 2021. Available online: https://www.who.int/publications/i/item/9789240034228 (accessed on 26 December 2024).
- National Environment Council (CONAMA), Ministry of Environment and Climate Change, Brazil. CONAMA Resolution No 506, of July 5, 2024. Establishes National Air Quality Standards and Provides Guidelines for Their Application. 2024. Available online: https://conama.mma.gov.br/?option=com_sisconama&task=arquivo.download&id=827 (accessed on 26 December 2024).
- Tavella, R.A.; Penteado, J.O.; de Lima Brum, R.; da Silva Bonifácio, A.d.S.; Martin, M.C.S.; Saes-Silva, E.; Brum, A.N.; Buffarini, R.; Filho, W.L.F.C.; Adamatti, D.F.; et al. An exploratory study on the association between air pollution and health problems (ICD-10) with an emphasis on respiratory diseases. Atmos. Pollut. Res. 2024, 16, 102377. [Google Scholar] [CrossRef]
- Dominski, F.H.; Lorenzetti Branco, J.H.; Buonanno, G.; Stabile, L.; Gameiro da Silva, M.; Andrade, A. Effects of air pollution on health: A mapping review of systematic reviews and meta-analyses. Environ. Res. 2021, 201, 111487. [Google Scholar] [CrossRef]
- Almetwally, A.A.; Bin-Jumah, M.; Allam, A.A. Ambient air pollution and its influence on human health and welfare: An overview. Environ. Sci. Pollut. Res. 2020, 27, 24815–24830. [Google Scholar] [CrossRef]
- Saleh, S.; Shepherd, W.; Jewell, C.; Lam, N.L.; Balmes, J.; Bates, M.N.; Lai, P.S.; Ochieng, C.A.; Chinouya, M.; Mortimer, K. Air pollution interventions and respiratory health: A systematic review. Int. J. Tuberc. Lung Dis. 2020, 24, 150–164. [Google Scholar] [CrossRef] [PubMed]
- Lu, F.; Xu, D.; Cheng, Y.; Dong, S.; Guo, C.; Jiang, X.; Zheng, X. Systematic review and meta-analysis of the adverse health effects of ambient PM2.5 and PM10 pollution in the Chinese population. Environ. Res. 2015, 136, 196–204. [Google Scholar] [CrossRef]
- Keswani, A.; Akselrod, H.; Anenberg, S.C. Health and clinical impacts of air pollution and linkages with climate change. NEJM Évid. 2022, 1, EVIDra2200068. [Google Scholar] [CrossRef]
- Fuller, R.; Landrigan, P.J.; Balakrishnan, K.; Bathan, G.; Bose-O’Reilly, S.; Brauer, M.; Caravanos, J.; Chiles, T.; Cohen, A.; Corra, L.; et al. Pollution and health: A progress update. Lancet Planet. Health 2022, 6, e535–e547. [Google Scholar] [CrossRef]
- Sun, Z.; Zhu, D. Exposure to outdoor air pollution and its human health outcomes: A scoping review. PLoS ONE 2019, 14, e0216550. [Google Scholar] [CrossRef]
- World Health Organization. Review of Evidence on Health Aspects of Air Pollution: REVIHAAP Project: Technical Report (No. WHO/EURO: 2013-4101-43860-61757). World Health Organization. Regional Office for Europe. 2021. Available online: https://iris.who.int/handle/10665/341712 (accessed on 26 January 2025).
- Lee, K.K.; Bing, R.; Kiang, J.; Bashir, S.; Spath, N.; Stelzle, D.; Mortimer, K.; Bularga, A.; Doudesis, D.; Joshi, S.S.; et al. Adverse health effects associated with household air pollution: A systematic review, meta-analysis, and burden estimation study. Lancet Glob. Health 2020, 8, e1427–e1434. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-T. Review of epidemiological studies on air pollution and health effects in children. Clin. Exp. Pediatr. 2020, 64, 3. [Google Scholar] [CrossRef] [PubMed]
- Karimi, S.M.; Maziyaki, A.; Moghadam, S.A.; Jafarkhani, M.; Zarei, H.; Moradi-Lakeh, M.; Pouran, H. Continuous exposure to ambient air pollution and chronic diseases: Prevalence, burden, and economic costs. Rev. Environ. Health 2020, 35, 379–399. [Google Scholar] [CrossRef]
- Duan, R.; Hao, K.; Yang, T. Air pollution and chronic obstructive pulmonary disease. Chronic Dis. Transl. Med. 2020, 6, 260–269. [Google Scholar] [PubMed]
- Wu, M.-Y.; Lo, W.-C.; Chao, C.-T.; Wu, M.-S.; Chiang, C.-K. Association between air pollutants and development of chronic kidney disease: A systematic review and meta-analysis. Sci. Total. Environ. 2020, 706, 135522. [Google Scholar] [CrossRef] [PubMed]
- Arias-Pérez, R.D.; Taborda, N.A.; Gómez, D.M.; Narvaez, J.F.; Porras, J.; Hernandez, J.C. Inflammatory effects of particulate matter air pollution. Environ. Sci. Pollut. Res. 2020, 27, 42390–42404. [Google Scholar] [CrossRef]
- Chen, C.-H.; Wu, C.-D.; Chiang, H.-C.; Chu, D.; Lee, K.-Y.; Lin, W.-Y.; Yeh, J.-I.; Tsai, K.-W.; Guo, Y.-L.L. The effects of fine and coarse particulate matter on lung function among the elderly. Sci. Rep. 2019, 9, 14790. [Google Scholar] [CrossRef]
- Mahapatra, B.; Walia, M.; Avis, W.R.; Saggurti, N. Effect of exposure to PM10 on child health: Evidence based on a large-scale survey from 184 cities in India. BMJ Glob. Health 2020, 5, e002597. [Google Scholar] [CrossRef]
- Tobias, A.; Karanasiou, A.; Amato, F.; Querol, X. Health effects of desert dust and sand storms: A systematic review and meta-analysis. Environ. Epidemiol. 2019, 3, 396. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística (IBGE), Brazil. Produto Interno Bruto dos Municípios. 2021. Available online: https://www.ibge.gov.br/estatisticas/economicas/contas-nacionais/9088-produto-interno-bruto-dos-municipios.html (accessed on 26 December 2024).
- Tavella, R.A.; Brum, R.d.L.; Ramires, P.F.; Santos, J.E.K.; Carvalho, R.B.; Marmett, B.; Vargas, V.M.F.; Baisch, P.R.M.; Júnior, F.M.R. Health impacts of PM2.5-bound metals and PAHs in a medium-sized Brazilian city. Environ. Monit. Assess. 2022, 194, 622. [Google Scholar] [CrossRef] [PubMed]
- Tavella, R.A.; da Rosa Moraes, N.G.; Aick, C.D.M.; Ramires, P.F.; Pereira, N.; Soares, A.G.; da Silva Júnior, F.M.R. Weekend effect of air pollutants in small and medium-sized cities: The role of policies stringency to COVID-19 containment. Atmos. Pollut. Res. 2023, 14, 101662. [Google Scholar] [CrossRef]
- Tavella, R.A.; da Silva Júnior, F.M.R. Exploring the Interruption-Recovery Pattern of Air Pollutants During the COVID-19 Pandemic in Southern Brazil: An Analysis of the New Normal. MAPAN 2023, 39, 211–220. [Google Scholar] [CrossRef]
- de Lima Brum, R.; Penteado, J.O.; Ramires, P.F.; Tavella, R.A.; Honscha, L.C.; da Silva Freitas, L.; de Moura, F.R.; Bonifácio, A.; da Silva, V.M.; da Silva, L.d.; et al. Southern Air Project—Scientific efforts to monitor and measure the impacts of air pollution in southern Brazil. Soc. Impacts 2024, 4, 100074. [Google Scholar] [CrossRef]
- de Sá, S.S.; Tavella, R.A.; Santos, J.E.K.; Aick, C.D.M.; de Oliveira Silveira, G.; Machado, P.D.W.; Martin, M.C.S.; Ramires, P.F.; Mirlean, N.; Baisch, P.R.M.; et al. The Hidden Dangers in the Rain: Human Health Risk Assessment of Fluoride and Nitrate in Rainwater from a Medium-Sized Industrial City. Water Conserv. Sci. Eng. 2024, 9, 51. [Google Scholar] [CrossRef]
- da Silva Bonifácio, A.; de Lima Brum, R.; Tavella, R.A.; They, N.H.; Nadaleti, W.C.; Coronas, M.V.; Saes-Silva, E.; Brum, A.N.; Buffarini, R.; Filho, W.L.F.C.; et al. Health impact assessment of air pollutants in simulated temperature scenarios in the largest coal mining region of Brazil. Case Stud. Chem. Environ. Eng. 2024, 10, 100923. [Google Scholar] [CrossRef]
- Brum, A.N.; de Lima Brum, R.; da Silva Bonifácio, A.; Tavella, R.A.; Penteado, J.O.; Siebel, A.M.; Júnior, F.M.R.d.S.; Zhang, L. Two decades of air pollution: Health impacts in the metropolitan area of Porto Alegre, Brazil. Int. J. Environ. Sci. Technol. 2025, 1–14. [Google Scholar] [CrossRef]
- Instituto Brasileiro de Geografia e Estatística (IBGE), Brazil. Cidades e Estados do País—Rio Grande, Rio Grande do Sul. 2022. Available online: https://cidades.ibge.gov.br/brasil/rs/rio-grande/panorama (accessed on 26 December 2024).
- Agência Nacional de Transportes Aquaviários (ANTAQ), Brazil. Estatístico Aquaviário. 2024. Available online: https://www.gov.br/antaq/pt-br/central-de-conteudos/publicacoes-da-antaq/estatisticos-aquaviarios (accessed on 26 December 2024).
- Beck, H.E.; Zimmermann, N.E.; McVicar, T.R.; Vergopolan, N.; Berg, A.; Wood, E.F. Present and future Köppen-Geiger climate classification maps at 1-km resolution. Sci. Data 2018, 5, 180214. [Google Scholar] [CrossRef]
- NBR 13412 DE 06/1995; Material Particulado em Suspensão na Atmosfera—Determinação da Concentração de Partículas Inaláveis pelo Método do Amostrador de Grande Volume Acoplado a um Separador Inercial de Partículas—Método de Ensaio. Brazilian Association of Technical Standards (ABNT): Rio de Janeiro, Brazil, 1995.
- Departamento de Informação e Informática do Sistema Único de Saúde (DATASUS). Informações de Saúde—Tabnet. 2024. Available online: https://datasus.saude.gov.br/informacoes-de-saude-tabnet/ (accessed on 26 December 2024).
- Pascal, M.; Corso, M.; Chanel, O.; Declercq, C.; Badaloni, C.; Cesaroni, G.; Henschel, S.; Meister, K.; Haluza, D.; Martin-Olmedo, P.; et al. Assessing the public health impacts of urban air pollution in 25 European cities: Results of the Aphekom project. Sci. Total Environ. 2013, 449, 390–400. [Google Scholar] [CrossRef] [PubMed]
- Abe, K.C.; Miraglia, S.G.E.K. Health Impact Assessment of Air Pollution in São Paulo, Brazil. Int. J. Environ. Res. Public Health 2016, 13, 694. [Google Scholar] [CrossRef]
- Rocha, C.A.; Lima, J.L.; Mendonça, K.V.; Marques, E.V.; Zanella, M.E.; Ribeiro, J.P.; Bertoncini, B.V.; Branco, V.T.C.; Cavalcante, R.M. Health impact assessment of air pollution in the metropolitan region of Fortaleza, Ceará, Brazil. Atmos. Environ. 2020, 241, 117751. [Google Scholar] [CrossRef]
- Martins, E.H.; de Souza Eicardi, M.; Nogarotto, D.C.; Pozza, S.A. Health and Economic Benefits of Lowering Particulate Matter (PM) Levels: Scenarios for a Southern Brazilian Metropolis. Aerosol Sci. Eng. 2024, 9, 1–12. [Google Scholar] [CrossRef]
- Abe, K.C.; Miraglia, S.G.E.K. Universidade de São Paulo avaliação de impacto à saúde do programa de controle de poluição do ar por veículos automotores no município de São Paulo, Brasil. Rev. Bras. Ciências Ambient. 2018, 47, 61–73. [Google Scholar] [CrossRef]
- Ostro, B.; World Health Organization. Outdoor Air Pollution: Assessing the Environmental Burden of Disease at National and Local Levels. World Health Organization. 2004. Available online: https://www.who.int/publications/i/item/9241591463 (accessed on 26 December 2024).
- Vormittag, E.d.M.P.A.d.A.; Cirqueira, S.S.R.; Neto, H.W.; Saldiva, P.H.N. Análise do monitoramento da qualidade do ar no Brasil. Estud. Avançados 2021, 35, 7–30. [Google Scholar] [CrossRef]
- IEMA. Instituto de Energia e Meio Ambiente. Dimensionamento da Rede Básica de Monitoramento da Qualidade do Ar no Brasil. 2024. Available online: https://energiaeambiente.org.br/produto/dimensionamento-da-rede-basica-de-monitoramento-da-qualidade-do-ar-no-brasil-cenarios-iniciais (accessed on 25 January 2025).
- da Silva Júnior, F.M.R.; Honscha, L.; Brum, R.; Ramires, P.; Tavella, R.; Fernandes, C.; Penteado, J.; Bonifácio, A.; Volcão, L.; Santos, M.; et al. Air quality in cities of the extreme south of Brazil. Ecotoxicol. Environ. Contam. 2020, 15, 61–67. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alves Laucas e Myrrha, L.H.; Loukili, Y.F.C.; Silveira, G.d.O.; Tavella, R.A.; Bonifácio, A.d.S.; Brum, R.d.L.; Pereira, N.; da Silva Júnior, F.M.R. Health and Economic Benefits of Accelerating the PM10 Interim Targets in Brazil’s New Air Quality Resolution: A Case Study in Southern Brazil. Atmosphere 2025, 16, 270. https://doi.org/10.3390/atmos16030270
Alves Laucas e Myrrha LH, Loukili YFC, Silveira GdO, Tavella RA, Bonifácio AdS, Brum RdL, Pereira N, da Silva Júnior FMR. Health and Economic Benefits of Accelerating the PM10 Interim Targets in Brazil’s New Air Quality Resolution: A Case Study in Southern Brazil. Atmosphere. 2025; 16(3):270. https://doi.org/10.3390/atmos16030270
Chicago/Turabian StyleAlves Laucas e Myrrha, Luiz Henrique, Yasmin Fawzia Cardoso Loukili, Gustavo de Oliveira Silveira, Ronan Adler Tavella, Alicia da Silva Bonifácio, Rodrigo de Lima Brum, Natália Pereira, and Flavio Manoel Rodrigues da Silva Júnior. 2025. "Health and Economic Benefits of Accelerating the PM10 Interim Targets in Brazil’s New Air Quality Resolution: A Case Study in Southern Brazil" Atmosphere 16, no. 3: 270. https://doi.org/10.3390/atmos16030270
APA StyleAlves Laucas e Myrrha, L. H., Loukili, Y. F. C., Silveira, G. d. O., Tavella, R. A., Bonifácio, A. d. S., Brum, R. d. L., Pereira, N., & da Silva Júnior, F. M. R. (2025). Health and Economic Benefits of Accelerating the PM10 Interim Targets in Brazil’s New Air Quality Resolution: A Case Study in Southern Brazil. Atmosphere, 16(3), 270. https://doi.org/10.3390/atmos16030270