
Association between Long-Term Exposure to Fine Particulate Matter and Asthma Incidence among School-Aged Children

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
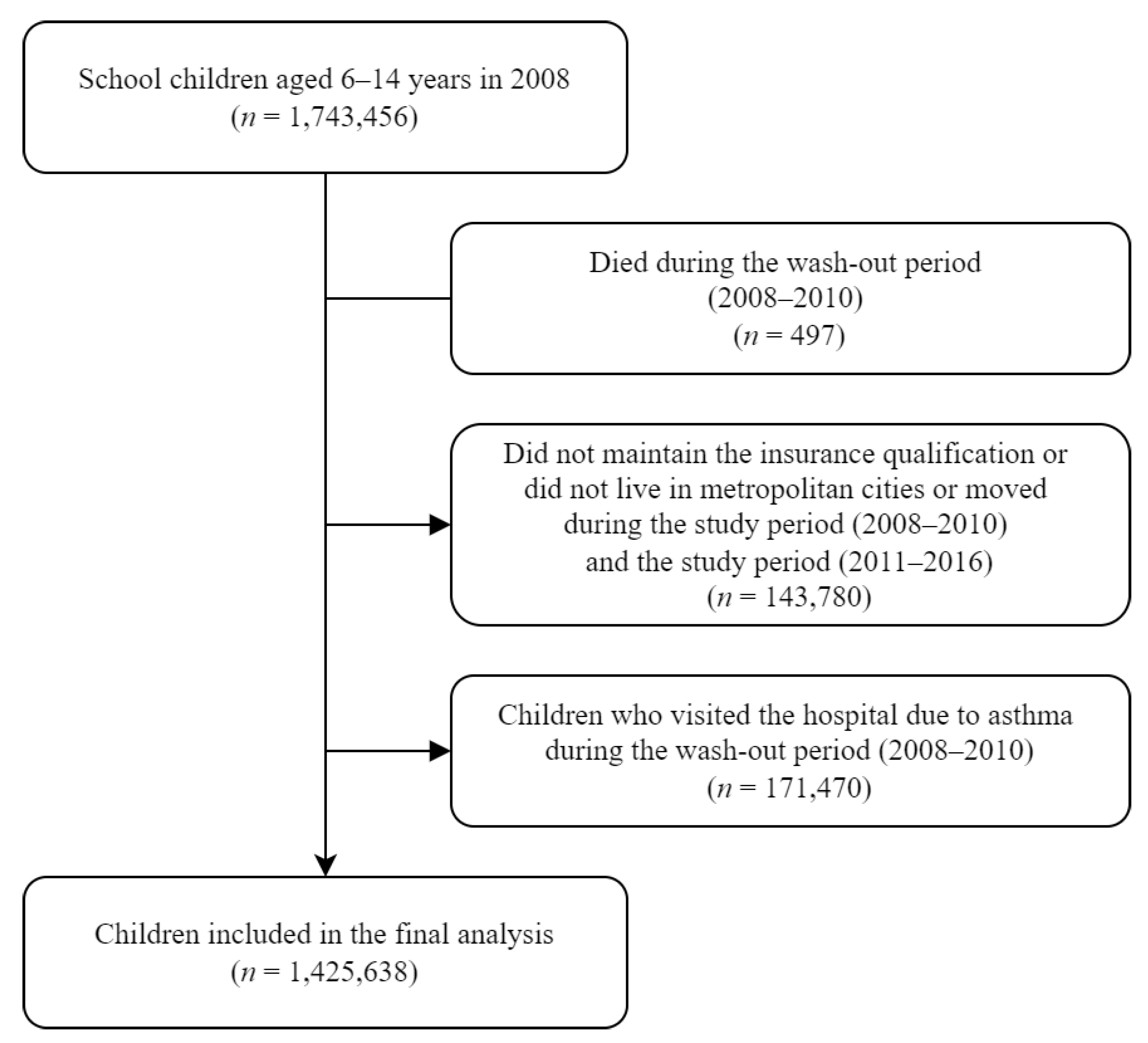
2.1. Study Design
2.2. Outcome Variable: Asthma incidence
2.3. Exposure Parameters: PM2.5 Exposure Level
2.4. Covariates
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Addo-Yobo, E.; Ade, S.; Agodokpessi, G.; Aguirre, V.; Aït-Khaled, N. The Global Asthma Report 2018; The Global Asthma Network: Auckland, New Zealand, 2018. [Google Scholar]
- Toskala, E.; Kennedy, D.W. Asthma risk factors. Int. Forum Fllergy Rhinol. 2015, 5, S11–S16. [Google Scholar] [CrossRef]
- Holst, G.J.; Pedersen, C.B.; Thygesen, M.; Brandt, J.; Geels, C.; Bønløkke, J.H.; Sigsgaard, T. Air pollution and family related determinants of asthma onset and persistent wheezing in children: Nationwide case-control study. BMJ 2020, 370, m2791. [Google Scholar] [CrossRef] [PubMed]
- Khreis, H.; Kelly, C.; Tate, J.; Parslow, R.; Lucas, K.; Nieuwenhuijsen, M. Exposure to traffic-related air pollution and risk of development of childhood asthma: A systematic review and meta-analysis. Environ. Int. 2017, 100, 1–31. [Google Scholar] [CrossRef] [PubMed]
- Burnett, R.; Chen, H.; Szyszkowicz, M.; Fann, N.; Hubbell, B.; Pope, C.A.; Apte, J.S.; Brauer, M.; Cohen, A.; Weichenthal, S. Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter. Proc. Natl. Acad. Sci. USA 2018, 115, 9592–9597. [Google Scholar] [CrossRef]
- Bateson, T.F.; Schwartz, J. Children’s response to air pollutants. J. Toxicol. Environ. Health Part A 2007, 71, 238–243. [Google Scholar] [CrossRef]
- Bowatte, G.; Lodge, C.; Lowe, A.J.; Erbas, B.; Perret, J.; Abramson, M.J.; Matheson, M.; Dharmage, S.C. The influence of childhood traffic-related air pollution exposure on asthma, allergy and sensitization: A systematic review and a meta-analysis of birth cohort studies. Allergy 2015, 70, 245–256. [Google Scholar] [CrossRef] [PubMed]
- Jung, C.-R.; Chen, W.-T.; Tang, Y.-H.; Hwang, B.-F. Fine particulate matter exposure during pregnancy and infancy and incident asthma. J. Allergy Clin. Immunol. 2019, 143, 2254–2262.e5. [Google Scholar] [CrossRef]
- Yang, S.I.; Lee, S.Y.; Kim, H.B.; Kim, H.C.; Leem, J.H.; Yang, H.J.; Kwon, H.; Seo, J.H.; Cho, H.J.; Yoon, J. Prenatal particulate matter affects new asthma via airway hyperresponsiveness in schoolchildren. Allergy 2019, 74, 675–684. [Google Scholar] [CrossRef]
- World Health Organization. WHO AIr Quality Database 2022. Available online: https://www.who.int/publications/m/item/who-air-quality-database-2022 (accessed on 23 July 2022).
- Cheol Seong, S.; Kim, Y.-Y.; Khang, Y.-H.; Heon Park, J.; Kang, H.-J.; Lee, H.; Do, C.-H.; Song, J.-S.; Hyon Bang, J.; Ha, S. Data resource profile: The national health information database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799–800. [Google Scholar] [CrossRef]
- Bateman, E.D.; Hurd, S.S.; Barnes, P.J.; Bousquet, J.; Drazen, J.M.; FitzGerald, M.; Gibson, P.; Ohta, K.; O’byrne, P.; Pedersen, S.E.; et al. Global strategy for asthma management and prevention: GINA executive summary. Eur. Respir. J. 2008, 31, 143–178. [Google Scholar] [CrossRef]
- Ma, Y.-C.; Lin, C.-C.; Yang, S.-Y.; Chen, H.-J.; Li, T.-C.; Lin, J.-G. Time trend analysis of the prevalence and incidence of diagnosed asthma and traditional Chinese medicine use among adults in Taiwan from 2000 to 2011: A population-based study. PLoS ONE 2015, 10, e0140318. [Google Scholar] [CrossRef]
- Lee, D.-W.; Han, C.-W.; Hong, Y.-C.; Oh, J.-M.; Bae, H.-J.; Kim, S.; Lim, Y.-H. Long-term exposure to fine particulate matter and incident asthma among elderly adults. Chemosphere 2021, 272, 129619. [Google Scholar] [CrossRef]
- Skamarock, W.C.; Klemp, J.B. A time-split nonhydrostatic atmospheric model for weather research and forecasting applications. J. Comput. Phys. 2008, 227, 3465–3485. [Google Scholar] [CrossRef]
- Kim, H.C.; Kim, E.; Bae, C.; Cho, J.H.; Kim, B.-U.; Kim, S. Regional contributions to particulate matter concentration in the Seoul metropolitan area, South Korea: Seasonal variation and sensitivity to meteorology and emissions inventory. Atmos. Chem. Phys. 2017, 17, 10315–10332. [Google Scholar] [CrossRef]
- Kim, B.-U.; Bae, C.; Kim, H.C.; Kim, E.; Kim, S. Spatially and chemically resolved source apportionment analysis: Case study of high particulate matter event. Atmos. Environ. 2017, 162, 55–70. [Google Scholar] [CrossRef]
- Han, C.; Oh, J.; Lim, Y.-H.; Kim, S.; Hong, Y.-C. Long-term exposure to fine particulate matter and development of chronic obstructive pulmonary disease in the elderly. Environ. Int. 2020, 143, 105895. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.W.; Ko, Y.S.; Kim, Y.J.; Sung, K.M.; Kim, H.J.; Choi, H.Y.; Sung, C.; Jeong, E. Korea community health survey data profiles. Osong Public Health Res. Perspect. 2015, 6, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Dekker, F.W.; De Mutsert, R.; Van Dijk, P.C.; Zoccali, C.; Jager, K.J. Survival analysis: Time-dependent effects and time-varying risk factors. Kidney Int. 2008, 74, 994–997. [Google Scholar] [CrossRef]
- Gan, W.Q.; FitzGerald, J.M.; Carlsten, C.; Sadatsafavi, M.; Brauer, M. Associations of ambient air pollution with chronic obstructive pulmonary disease hospitalization and mortality. Am. J. Respir. Crit. Care Med. 2013, 187, 721–727. [Google Scholar] [CrossRef]
- Lavigne, É.; Talarico, R.; van Donkelaar, A.; Martin, R.V.; Stieb, D.M.; Crighton, E.; Weichenthal, S.; Smith-Doiron, M.; Burnett, R.T.; Chen, H. Fine particulate matter concentration and composition and the incidence of childhood asthma. Environ. Int. 2021, 152, 106486. [Google Scholar] [CrossRef]
- Keet, C.A.; Keller, J.P.; Peng, R.D. Long-term coarse particulate matter exposure is associated with asthma among children in Medicaid. Am. J. Respir. Crit. Care Med. 2018, 197, 737–746. [Google Scholar] [CrossRef] [PubMed]
- Sol, I.S.; Jang, H.; Noh, J.; Kim, S.Y.; Kim, M.J.; Kim, Y.H.; Kim, C.; Sohn, M.H.; Kim, K.W. Mortality and morbidity in children with asthma: A nationwide study in Korea. Respir. Med. 2021, 177, 106306. [Google Scholar] [CrossRef]
- Engelkes, M.; Janssens, H.M.; de Ridder, M.A.; de Jongste, J.C.; Sturkenboom, M.C.; Verhamme, K.M. Time trends in the incidence, prevalence and age at diagnosis of asthma in children. Pediatric Allergy Immunol. 2015, 26, 367–374. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Salam, M.T.; Alderete, T.L.; Habre, R.; Bastain, T.M.; Berhane, K.; Gilliland, F.D. Effects of childhood asthma on the development of obesity among school-aged children. Am. J. Respir. Crit. Care Med. 2017, 195, 1181–1188. [Google Scholar] [CrossRef]
- Henriksen, L.; Simonsen, J.; Haerskjold, A.; Linder, M.; Kieler, H.; Thomsen, S.F.; Stensballe, L.G. Incidence rates of atopic dermatitis, asthma, and allergic rhinoconjunctivitis in Danish and Swedish children. J. Allergy Clin. Immunol. 2015, 136, 360–366.e2. [Google Scholar] [CrossRef] [PubMed]
- Honkamäki, J.; Hisinger-Mölkänen, H.; Ilmarinen, P.; Piirilä, P.; Tuomisto, L.E.; Andersén, H.; Huhtala, H.; Sovijärvi, A.; Backman, H.; Lundbäck, B. Age-and gender-specific incidence of new asthma diagnosis from childhood to late adulthood. Respir. Med. 2019, 154, 56–62. [Google Scholar] [CrossRef]
- Bae, H.-J. Effects of Reduced Ambient PM 10 Levels on the Health of Children in Lower-income Families. J. Environ. Health Sci. 2010, 36, 182–190. [Google Scholar] [CrossRef]
- O’lenick, C.R.; Winquist, A.; Mulholland, J.A.; Friberg, M.D.; Chang, H.H.; Kramer, M.R.; Darrow, L.A.; Sarnat, S.E. Assessment of neighbourhood-level socioeconomic status as a modifier of air pollution–asthma associations among children in Atlanta. J Epidemiol. Community Health 2017, 71, 129–136. [Google Scholar] [CrossRef]
- Norbäck, D.; Lu, C.; Wang, J.; Zhang, Y.; Li, B.; Zhao, Z.; Huang, C.; Zhang, X.; Qian, H.; Sun, Y. Asthma and rhinitis among Chinese children—Indoor and outdoor air pollution and indicators of socioeconomic status (SES). Environ. Int. 2018, 115, 1–8. [Google Scholar] [CrossRef]
- Leon Hsu, H.-H.; Mathilda Chiu, Y.-H.; Coull, B.A.; Kloog, I.; Schwartz, J.; Lee, A.; Wright, R.O.; Wright, R.J. Prenatal particulate air pollution and asthma onset in urban children. Identifying sensitive windows and sex differences. Am. J. Respir. Crit. Care Med. 2015, 192, 1052–1059. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Variable | Total | Non-Asthmatic | Asthmatic |
|---|---|---|---|
| n (%) a | n (%) b | n (%) b | |
| Total | 1,425,638 (100.0) | 1,373,505 (96.3) | 52,133 (3.7) |
| Sex | |||
| Boy | 746,130 (52.3) | 716,794 (96.1) | 29,336 (3.9) |
| Girl | 679,508 (47.7) | 656,711 (96.6) | 22,797 (3.4) |
| Age | |||
| 6–9 | 603,578 (42.3) | 573,721 (95.1) | 29,857 (4.9) |
| 10–14 | 822,060 (57.7) | 799,784 (97.3) | 22,276 (2.7) |
| Income status | |||
| Q1 (lowest) | 269,275 (18.9) | 261,038 (96.9) | 8237 (3.1) |
| Q2 | 250,953 (17.6) | 242,370 (96.6) | 8223 (3.3) |
| Q3 | 296,398 (20.8) | 284,512 (96.0) | 11,886 (4.0) |
| Q4 (highest) | 609,012 (42.7) | 585,225 (96.1) | 23,787 (3.9) |
| Metropolitan city | |||
| Seoul | 570,263 (40.0) | 547,533 (96.0) | 22,730 (4.0) |
| Busan | 203,661 (14.3) | 197,215 (96.8) | 6446 (3.2) |
| Daegu | 154,420 (10.8) | 147,866 (95.8) | 6554 (4.2) |
| Incheon | 190,641 (13.4) | 183,862 (96.4) | 6779 (3.6) |
| Gwangju | 118,820 (8.3) | 115,296 (97.0) | 3524 (3.0) |
| Daejeon | 105,302 (7.4) | 101,915 (96.8) | 3327 (3.2) |
| Ulsan | 82,531 (5.8) | 19,158 (96.6) | 2773 (3.4) |
| Contextual variables (district level) | |||
| Proportion of high school diploma (%) | 68.0 ± 4.5 | 68.0 ± 4.5 | 68.1 ± 4.6 |
| Proportion of current smokers (%) | 24.5 ± 2.3 | 24.5 ± 2.3 | 24.5 ± 2.3 |
| Monthly average income (1000 KRW) | 1307 ± 86.4 | 1307 ± 86.4 | 1310 ± 87.0 |
| Moving Average Exposure (Months) | n | Cases | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|---|---|
| HR | (95% CI) | p-Value | HR | (95% CI) | p-Value | |||
| 12 | 1,425,638 | 52,133 | 1.065 | (1.023–1.107) | 0.003 | 1.056 | (1.013–1.099) | 0.013 |
| 24 | 1.040 | (0.995–1.086) | 0.087 | 1.031 | (0.984–1.078) | 0.204 | ||
| 36 | 1.078 | (1.030–1.127) | 0.002 | 1.070 | (1.019–1.120) | 0.008 | ||
| 48 | 1.086 | (1.038–1.135) | 0.001 | 1.075 | (1.024–1.126) | 0.005 | ||
| 60 | 1.079 | (1.030–1.128) | 0.002 | 1.068 | (1.017–1.119) | 0.011 | ||
| Variable | n | Cases | Person-Year | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|---|---|---|
| HR | (95% CI) | p-Value | HR | (95% CI) | p-Value | ||||
| Total | 1,425,638 | 52,133 | 7,558,765 | 1.086 | (1.038, 1.135) | 0.001 | 1.075 | (1.024–1.126) | 0.005 |
| Sex | |||||||||
| Boy | 746,130 | 29,336 | 3,948,420 | 1.056 | (0.991–1.120) | 0.096 | 1.059 | (0.991–1.127) | 0.099 |
| Girl | 679,508 | 22,797 | 3,610,345 | 1.135 | (1.061–1.209) | 0.001 | 1.108 | (1.031–1.185) | 0.009 |
| Age | |||||||||
| 6–9 | 603,578 | 29,857 | 3,173,598 | 1.121 | (1.057–1.185) | <0.001 | 1.112 | (1.045–1.178) | 0.002 |
| 10–14 | 822,060 | 22,276 | 4,395,116 | 1.036 | (0.961–1.111) | 0.362 | 1.029 | (0.950–1.108) | 0.474 |
| Income | |||||||||
| Q1 (lowest) | 269,275 | 8237 | 1,431,347 | 0.886 | (0.757–1.014) | 0.065 | 0.841 | (0.708–0.974) | 0.011 |
| Q2 | 250,953 | 8223 | 1,323,283 | 1.082 | (0.957–1.207) | 0.218 | 1.078 | (0.948–1.207) | 0.258 |
| Q3 | 296,398 | 11,886 | 1,557,103 | 0.962 | (0.858–1.066) | 0.462 | 0.940 | (0.831–1.048) | 0.260 |
| Q4 (highest) | 609,012 | 23,787 | 3,247,031 | 1.217 | (1.148–1.286) | <0.001 | 1.234 | (1.161–1.308) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, H.-M.; Ryoo, S.-W.; Hong, Y.-C.; Kim, S.-T.; Lim, Y.-H.; Lee, D.-W. Association between Long-Term Exposure to Fine Particulate Matter and Asthma Incidence among School-Aged Children. Atmosphere 2022, 13, 1430. https://doi.org/10.3390/atmos13091430
Lim H-M, Ryoo S-W, Hong Y-C, Kim S-T, Lim Y-H, Lee D-W. Association between Long-Term Exposure to Fine Particulate Matter and Asthma Incidence among School-Aged Children. Atmosphere. 2022; 13(9):1430. https://doi.org/10.3390/atmos13091430
Chicago/Turabian StyleLim, Hyun-Mook, Seung-Woo Ryoo, Yun-Chul Hong, Soon-Tae Kim, Youn-Hee Lim, and Dong-Wook Lee. 2022. "Association between Long-Term Exposure to Fine Particulate Matter and Asthma Incidence among School-Aged Children" Atmosphere 13, no. 9: 1430. https://doi.org/10.3390/atmos13091430
APA StyleLim, H.-M., Ryoo, S.-W., Hong, Y.-C., Kim, S.-T., Lim, Y.-H., & Lee, D.-W. (2022). Association between Long-Term Exposure to Fine Particulate Matter and Asthma Incidence among School-Aged Children. Atmosphere, 13(9), 1430. https://doi.org/10.3390/atmos13091430