
Analysis of Symptomology, Infectiveness, and Reinfections between Male and Female COVID-19 Patients: Evidence from Japanese Registry Data


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data
2.2. Analysis
3. Results
3.1. Symptoms
3.2. Reinfection
3.3. Asymptomatic Patients
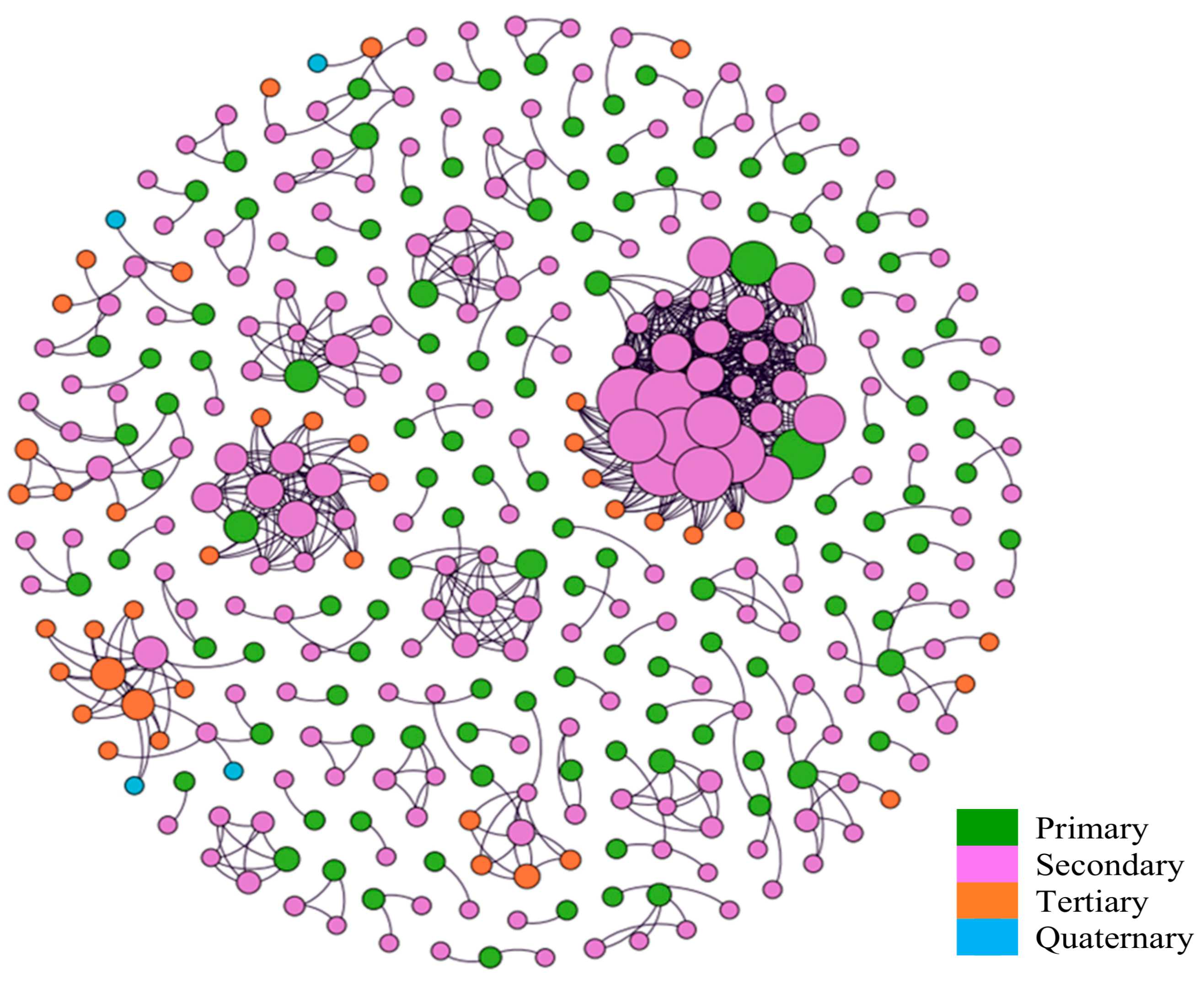
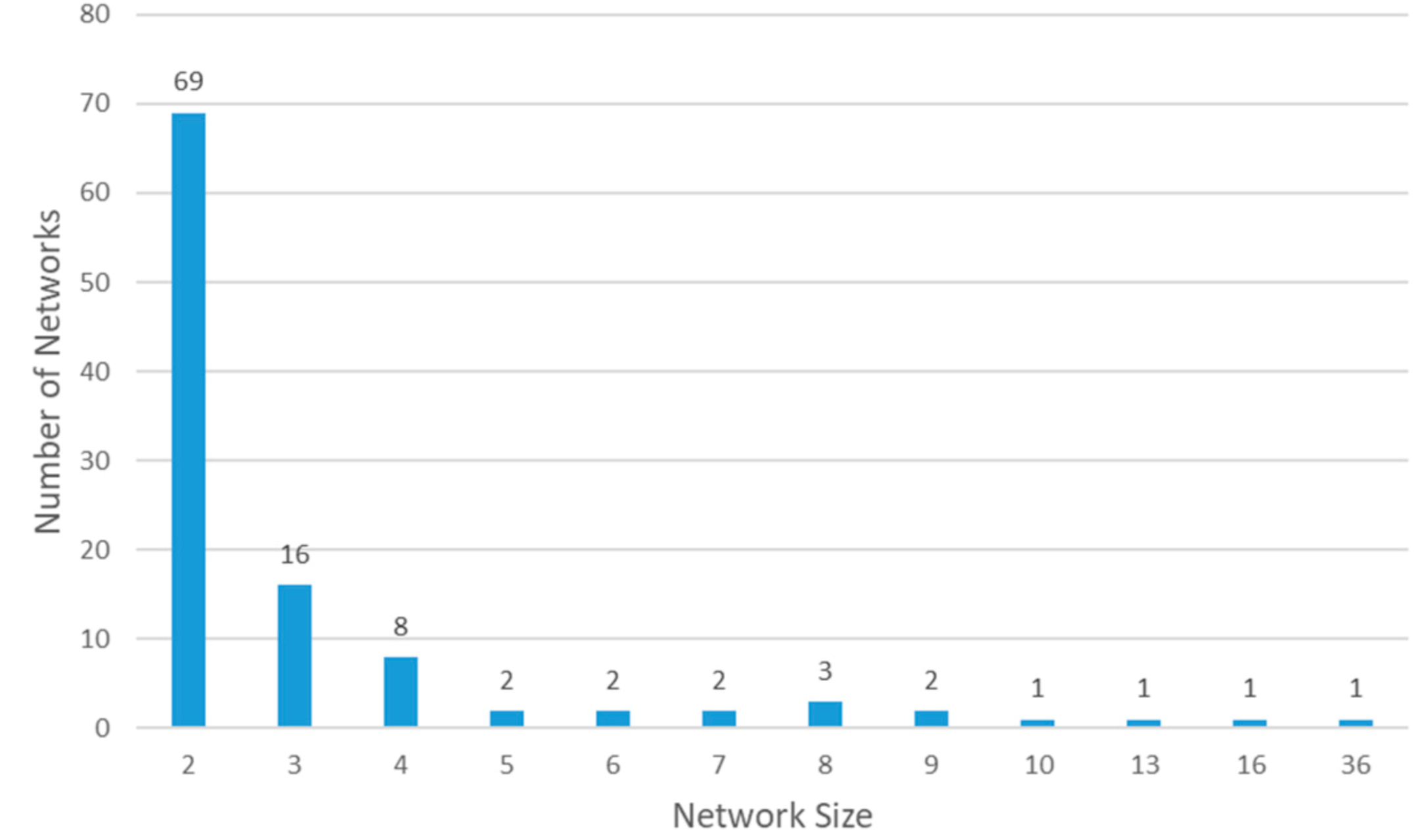
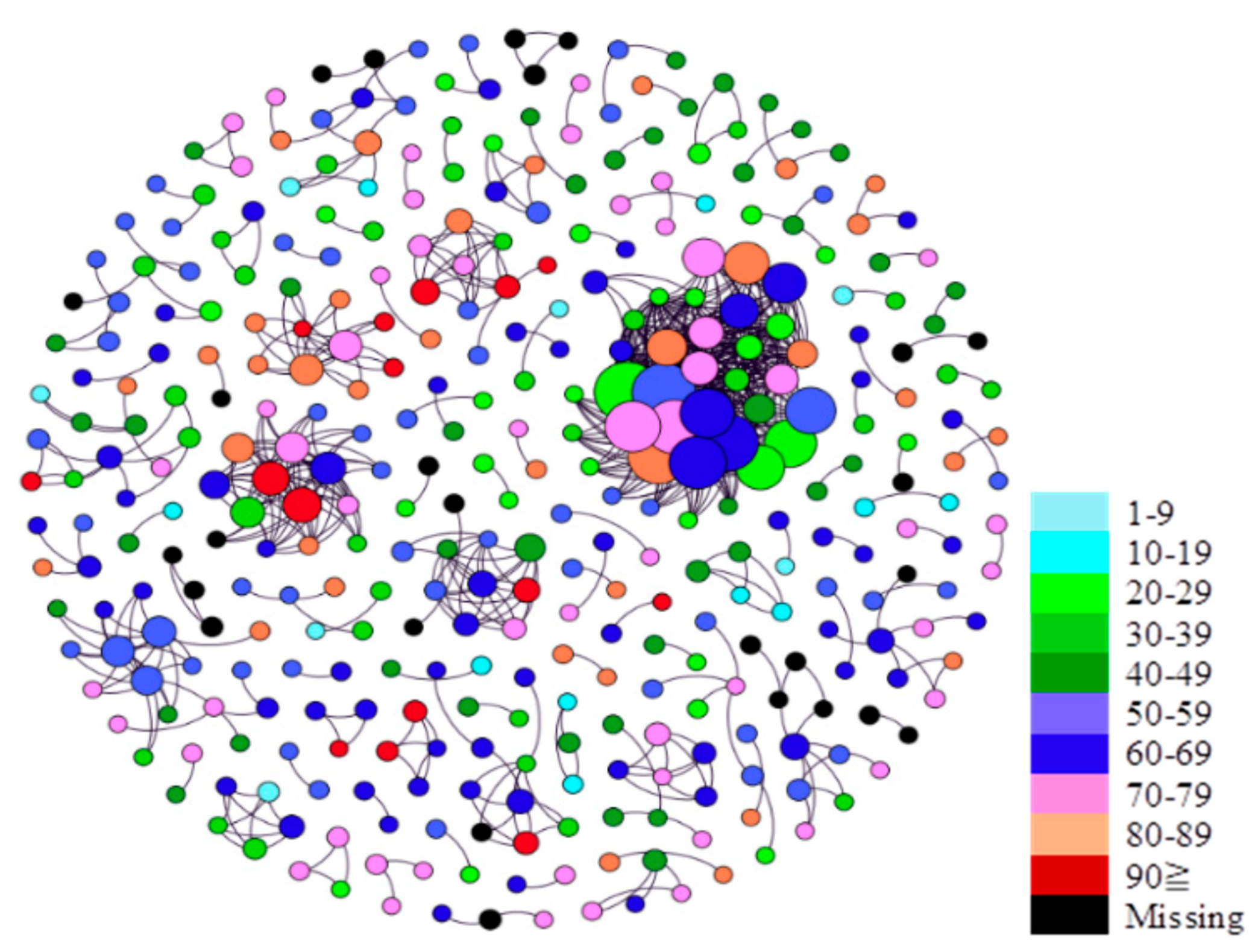
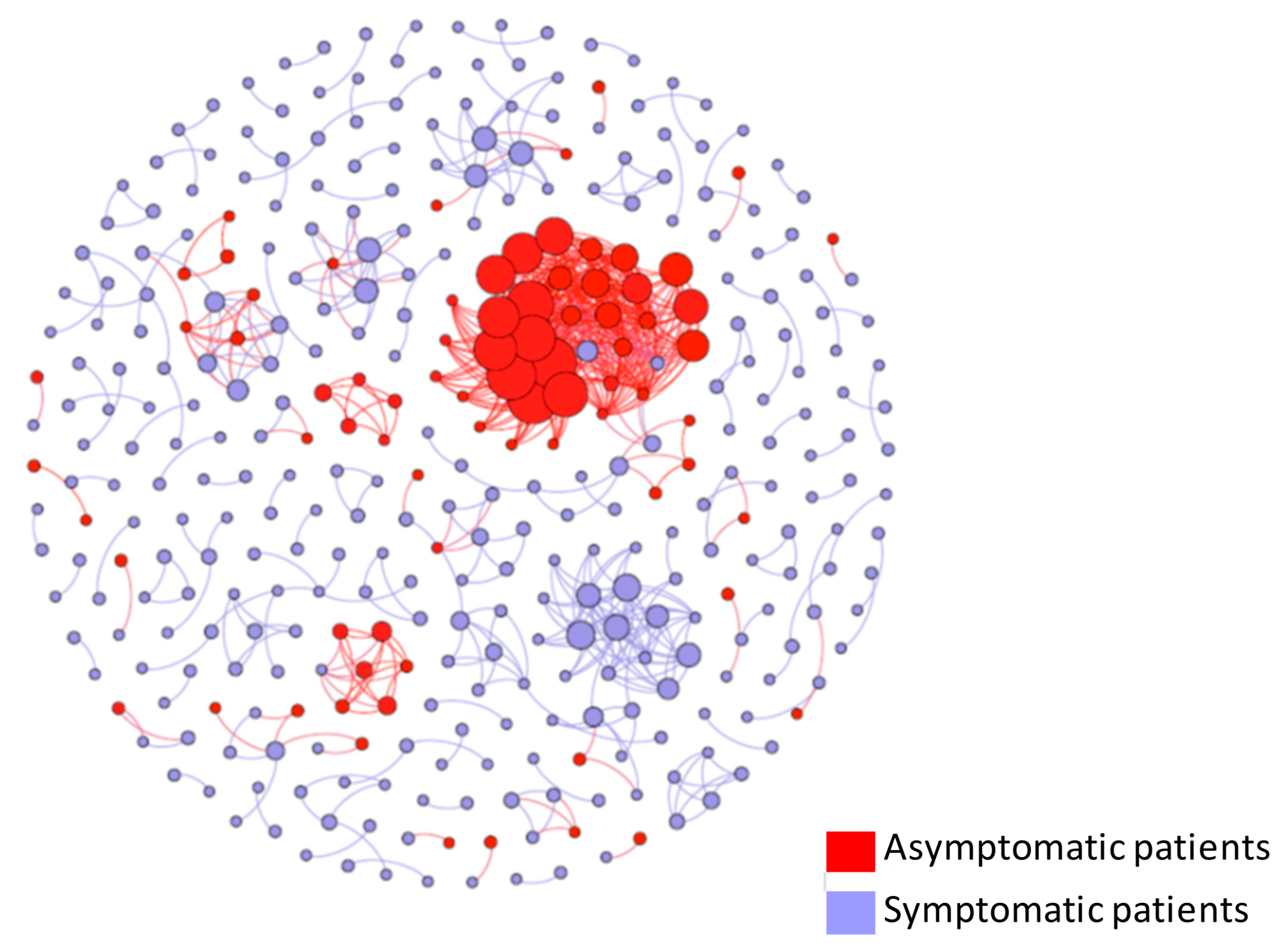
3.4. Viral Transmission
3.5. Severity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefan, N.; Birkenfeld, A.L.; Schulze, M.B.; Ludwig, D. Obesity and impaired metabolic health in patients with COVID-19. Nat. Rev. Endocrinol. 2020, 16, 341–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, Y.; Yao, L.; Wei, T.; Tian, F.; Jin, D.Y.; Chen, L.; Wang, M. Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA 2020, 323, 1406–1407. [Google Scholar] [CrossRef] [Green Version]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-nCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [Green Version]
- Gao, Z.; Xu, Y.; Sun, C.; Wang, X.; Guo, Y.; Qiu, S.; Ma, K. A systematic review of asymptomatic infections with COVID-19. J. Microbiol. Immunol. Infect. 2020, 54, 12–16. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, A.; Yi, B.; Ding, K.; Wang, H.; Wang, J.; Shi, H.; Wang, S.; Xu, G. The epidemiological characteristics of infection in close contacts of COVID-19 in Ningbo city. Chin. J. Epidemiol. 2020, 41, 667–671. [Google Scholar]
- Health and Welfare Department, Health and Safety Bureau Community Health Division. New Corona: Occurrence in Hokkaido. 2020. Available online: http://www.pref.hokkaido.lg.jp/hf/kth/kak/hasseijoukyou.htm (accessed on 8 July 2020).
- Oshitani, H. Cluster-Based Approach to Coronavirus Disease 2019 (COVID-19) Response in Japan, from February to April 2020. Jpn. J. Infect. Dis. 2020, 73, 491–493. [Google Scholar] [CrossRef]
- Leonard, A. This Japanese Island Lifted Its Coronavirus Lockdown Too Soon and Became a Warning to the World. 2020. Available online: https://time.com/5826918/hokkaido-coronavirus-lockdown/ (accessed on 8 July 2020).
- Sapporo. About Emergency Measures. 2020. Available online: http://www.city.sapporo.jp/2019n-cov/kinkyujitai.html (accessed on 8 July 2020).
- Furuse, Y.; Sando, E.; Tsuchiya, N.; Miyahara, R.; Yasuda, I.; Ko, Y.K.; Saito, M.; Morimoto, K.; Imamura, T.; Shobugawa, Y.; et al. Clusters of Coronavirus Disease in Communities, Japan, January–April 2020. Emerg. Infect. Dis. 2020, 26, 2176–2179. [Google Scholar] [CrossRef]
- Imamura, T.; Saito, T.; Oshitani, H. Roles of Public Health Centers and Cluster-Based Approach for COVID-19 Response in Japan. Health Secur. 2021, 19, 229–231. [Google Scholar] [CrossRef]
- National Institute of Infectious Diseases. Guidelines for Conducting an Active Epidemiological Survey on Patients with Coronavirus Infection. 2021. Available online: https://www.niid.go.jp/niid/images/epi/corona/COVID19-02-210108.pdf (accessed on 5 February 2021).
- Japan Epidemiological Association. Guide on Active Epidemiological Investigation for Public Health Nurses in Response to COVID-19 in Japan. 2020. Available online: https://jeaweb.jp/covid/links/guide_0421.pdf (accessed on 5 February 2021).
- World Health Organization. Clinical Management of COVID-19: Interim Guidance, 27 May 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Larsen, J.R.; Martin, M.R.; Martin, J.D.; Kuhn, P.; Hicks, J.B. Modeling the Onset of Symptoms of COVID-19. Front. Public Health 2020, 8, 473. [Google Scholar] [CrossRef]
- Tian, Y.; Rong, L.; Nian, W.; He, Y. Review article: Gastrointestinal features in COVID-19 and the possibility of faecal transmission. Aliment. Pharmacol. Ther. 2020, 51, 843–851. [Google Scholar] [CrossRef]
- Dong, Y.; Mo, X.; Hu, Y.; Qi, X.; Jiang, F.; Jiang, Z.; Ton, S. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics 2020, 58, 712–713. [Google Scholar] [CrossRef]
- Liu, W.; Zhang, Q.; Chen, J.; Xiang, R.; Song, H.; Shu, S.; Chen, L.; Liang, L.; Zhou, J.; You, L.; et al. Detection of COVID-19 in Children in Early January 2020 in Wuhan, China. N. Engl. J. Med. 2020, 382, 1370–1371. [Google Scholar] [CrossRef]
- Xia, W.; Shao, J.; Guo, Y.; Peng, X.; Li, Z.; Hu, D. Clinical and CT features in pediatric patients with COVID-19 infection: Different points from adults. Pediatr. Pulmonol. 2020, 55, 1169–1174. [Google Scholar] [CrossRef] [Green Version]
- Abduljali, J.M.; Abduljali, B.M. Epidemiology, genome and clinical features of the pandemic SARS-CoV-2: A recent view. New Microbes New Infect. 2020, 35, 100672. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Yang, R.; Gui, X.; Xiong, Y. Comparison of Clinical Characteristics of Patients with Asymptomatic vs. Symptomatic Coronavirus Disease 2019 in Wuhan, China. JAMA Netw. Open 2020, 3, e2010182. [Google Scholar] [CrossRef]
- Kronbichler, A.; Kresse, D.; Yoon, S.; Lee, K.H.; Effenberger, M.; Shin, J.I. Asymptomatic patients as a source of COVID-19 infections: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 98, 180–186. [Google Scholar] [CrossRef]
- Wu, C.; Yang, W.; Wu, X.; Zhang, T.; Zhao, Y.; Ren, W.; Xia, J. Clinical Manifestation and Laboratory Characteristics of SARS-CoV-2 Infection in Pregnant Women. Virol. Sin. 2020, 35, 305–310. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef] [PubMed]
- Roche, J.A.; Roche, R. A hypothesized role for dysregulated bradykinin signaling in COVID-19 respiratory complications. FASEB J. 2020, 34, 7265–7269. [Google Scholar] [CrossRef] [PubMed]
- Garvin, M.R.; Alvarez, C.; Miller, J.I.; Prates, E.T.; Walker, A.M.; Amos, B.K.; Mast, A.; Justice, A.; Aronow, B.; Jacobson, D. Author response: A mechanistic model and therapeutic interventions for COVID-19 involving a RAS-mediated bradykinin storm. Elife 2020, 9, e59177. [Google Scholar] [CrossRef] [PubMed]
- Brosnihan, K.; Senanayake, P.; Li, P.; Ferrario, C. Bi-directional actions of estrogen on the renin-angiotensin system. Braz. J. Med. Biol. Res. 1999, 32, 373–381. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, J.C. Sex and the renin-angiotensin system: Inequality between the sexes in response to RAS stimulation and inhibition. Am. J. Physiol. Integr. Comp. Physiol. 2008, 294, R1220–R1226. [Google Scholar] [CrossRef] [Green Version]
- Brosnihan, K.B.; Neves, L.A.; Joyner, J.; Averill, D.B.; Chappell, M.C.; Sarao, R.; Penninger, J.; Ferrario, C.M. Enhanced Renal Immunocytochemical Expression of ANG-(1-7) and ACE2 During Pregnancy. Hypertension 2003, 42, 749–753. [Google Scholar] [CrossRef] [Green Version]
- Sodhi, C.P.; Wohlford-Lenane, C.; Yamaguchi, Y.; Prindle, T.; Fulton, W.B.; Wang, S.; McCray, P.B., Jr.; Chappell, M.; Hackam, D.J.; Jia, H.; et al. Attenuation of pulmonary ACE2 activity impairs inactivation of des-Arg9 bradykinin/BKB1R axis and facilitates LPS-induced neutrophil infiltration. Am. J. Physiol. Lung Cell. Mol. Physiol. 2018, 314, L17–L31. [Google Scholar] [CrossRef]
- Bharadwaj, M.S.; Strawn, W.B.; Groban, L.; Yamaleyeva, L.M.; Chappell, M.C.; Horta, C.; Atkins, K.; Firmes, L.; Gurley, S.B.; Brosnihan, K.B. Angiotensin-Converting Enzyme 2 Deficiency Is Associated with Impaired Gestational Weight Gain and Fetal Growth Restriction. Hypertension 2011, 58, 852–858. [Google Scholar] [CrossRef] [Green Version]
- Luo, L.; Liu, D.; Liao, X.; Wu, X.; Jing, Q.; Zheng, J.; Liu, F.; Yang, S.; Bi, H.; Li, Z.; et al. Contact Settings and Risk for Transmission in 3410 Close Contacts of Patients With COVID-19 in Guangzhou, China. Ann. Intern. Med. 2020, 173, 879–887. [Google Scholar] [CrossRef]
- Ye, G.; Pan, Z.; Pan, Y.; Deng, Q.; Chen, L.; Li, J.; Li, Y.; Wang, X. Clinical characteristics of severe acute respiratory syndrome coronavirus 2 reactivation. J. Infect. 2020, 80, e14–e17. [Google Scholar] [CrossRef]
- Ravioli, S.; Ochsner, H.; Lindner, G. Reactivation of COVID-19 pneumonia: A report of two cases. J. Infect. 2020, 81, e72–e73. [Google Scholar] [CrossRef]
- Loconsole, D.; Passerini, F.; Palmieri, V.O.; Centrone, F.; Sallustio, A.; Pugliese, S.; Grimaldi, L.D.; Portincasa, P.; Chironna, M. Recurrence of COVID-19 after recovery: A case report from Italy. Infection 2020, 48, 965–967. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Male (n = 595) | Female (n = 674) | p-Value |
|---|---|---|---|
| Age 1, mean (SD) | 54 (23) | 53 (22) | 0.24 |
| Asymptomatic cases, n (%) | 80 (13%) | 177 (26%) | <0.001 |
| Symptom, n (%) | |||
| Fever | 430 (88%) | 388 (81%) | 0.01 |
| Cough | 202 (41%) | 193 (40%) | 0.77 |
| Pharyngitis | 72 (15%) | 102 (21%) | 0.01 |
| Rhinitis | 60 (12%) | 97 (20%) | 0.01 |
| Fatigue | 213 (43%) | 195 (41%) | 0.38 |
| Diarrhea | 44 (9%) | 49 (10%) | 0.51 |
| Headache | 82 (15%) | 103 (21%) | 0.05 |
| Pneumonia | 71 (14%) | 54 (11%) | 0.14 |
| Dyspnea | 70 (14%) | 53 (11%) | 0.13 |
| Loss of taste | 73 (15%) | 94 (20%) | 0.05 |
| Loss of smell | 8 (2%) | 9 (2%) | 0.77 |
| Reduced appetite | 12 (2%) | 6 (1%) | 0.17 |
| Body aches | 73 (15%) | 58 (12%) | 0.20 |
| Nausea/Vomiting | 5 (1%) | 22 (5%) | 0.001 |
| Phlegm | 8 (2%) | 13 (3%) | 0.24 |
| Chill | 2 (<1%) | 3 (1%) | 0.64 |
| Reinfection cases, n (%) | 4 (1%) | 4 (1%) | 0.79 |
| No. of symptoms 2, mean (SD) | 2.91 (1.52) | 3.00 (1.62) | 0.34 |
| No. of individuals who infected others, n (%) | 122 (21%) | 88 (13%) | <0.001 |
| Avg. no. of infectees per infector, mean (SD) | 3.48 (5.07) | 3.89 (5.90) | 0.60 |
| Duration: Onset-PCR, mean # days (SD) | 6.90 (6.55) | 6.29 (5.23) | 0.09 |
| Symptoms | 1–9 | 10–19 | 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80–89 | 90–99 | Total | p-Value | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | |
| Fever (n) | 12 | 2 | 5 | 10 | 38 | 43 | 39 | 40 | 59 | 49 | 63 | 56 | 80 | 49 | 75 | 62 | 39 | 39 | 12 | 25 | 422 | 375 | ||
| (%) | 100.00 | 100.00 | 62.50 | 90.91 | 84.44 | 75.44 | 88.64 | 83.33 | 89.39 | 84.48 | 91.30 | 82.35 | 90.91 | 76.56 | 87.21 | 80.52 | 81.25 | 81.25 | 80.00 | 92.59 | 87.73 | 81.52 | 0.25 | 0.54 |
| Cough (n) | 5 | 0 | 2 | 3 | 17 | 30 | 26 | 23 | 36 | 26 | 31 | 24 | 29 | 24 | 37 | 35 | 12 | 14 | 5 | 9 | 200 | 188 | ||
| (%) | 41.67 | 0.00 | 25.00 | 27.27 | 37.78 | 52.63 | 59.09 | 47.92 | 54.55 | 44.83 | 44.93 | 35.29 | 32.95 | 37.50 | 43.02 | 45.45 | 25.00 | 29.17 | 33.33 | 33.33 | 40.87 | 40.87 | 0.02 | 0.21 |
| Pharyngitis (n) | 0 | 0 | 0 | 3 | 4 | 18 | 10 | 11 | 10 | 11 | 17 | 17 | 16 | 19 | 11 | 13 | 3 | 4 | 0 | 2 | 71 | 98 | ||
| (%) | 0 | 0 | 0 | 27.27 | 8.89 | 31.58 | 22.73 | 22.92 | 15.15 | 18.97 | 24.64 | 25.00 | 18.18 | 29.69 | 12.79 | 16.88 | 6.25 | 8.33 | 0 | 7.41 | 14.76 | 21.3 | 0.03 | 0.05 |
| Rhinitis (n) | 4 | 0 | 1 | 6 | 9 | 18 | 5 | 21 | 6 | 8 | 8 | 11 | 10 | 11 | 11 | 9 | 2 | 3 | 1 | 2 | 57 | 89 | ||
| (%) | 33.33 | 0 | 12.50 | 54.55 | 20.00 | 31.58 | 11.36 | 43.75 | 9.09 | 13.79 | 11.59 | 16.18 | 11.36 | 17.19 | 12.79 | 11.69 | 4.17 | 6.25 | 6.67 | 7.41 | 11.85 | 19.35 | 0.22 | <0.001 |
| Fatigue (n) | 0 | 0 | 4 | 2 | 19 | 28 | 25 | 20 | 35 | 27 | 33 | 34 | 35 | 24 | 38 | 28 | 18 | 16 | 3 | 12 | 210 | 191 | ||
| (%) | 0 | 0 | 50.00 | 18.18 | 43.18 | 49.12 | 56.82 | 41.67 | 53.03 | 46.55 | 47.83 | 50.00 | 39.77 | 37.50 | 44.19 | 36.36 | 37.50 | 33.33 | 20.00 | 44.44 | 43.66 | 41.52 | 0.02 | 0.31 |
| Diarrhea (n) | 0 | 0 | 2 | 2 | 4 | 3 | 4 | 8 | 6 | 4 | 9 | 12 | 9 | 9 | 6 | 7 | 3 | 3 | 0 | 1 | 43 | 49 | ||
| (%) | 0.00 | 0.00 | 25 | 18.18 | 8.89 | 5.26 | 9.09 | 16.67 | 9.09 | 6.90 | 13.04 | 17.65 | 10.23 | 14.06 | 6.98 | 9.09 | 5.77 | 6.25 | 0 | 3.70 | 8.94 | 10.65 | 0.51 | 0.21 |
| Headache (n) | 0 | 0 | 2 | 3 | 20 | 20 | 12 | 21 | 16 | 14 | 12 | 17 | 13 | 6 | 6 | 13 | 1 | 2 | 0 | 1 | 82 | 97 | ||
| (%) | 0 | 0 | 25.00 | 27.27 | 44.44 | 35.09 | 27.27 | 43.75 | 24.24 | 24.14 | 17.39 | 25.00 | 14.77 | 9.38 | 6.98 | 16.88 | 2.08 | 4.17 | 0 | 3.70 | 17.05 | 21.09 | <0.001 | <0.001 |
| Pneumonia (n) | 0 | 0 | 0 | 0 | 5 | 4 | 5 | 3 | 9 | 10 | 13 | 13 | 14 | 3 | 17 | 9 | 7 | 5 | 0 | 6 | 70 | 53 | ||
| (%) | 0.00 | 0.00 | 0.00 | 0.00 | 11.11 | 7.02 | 11.36 | 6.25 | 13.64 | 17.24 | 18.84 | 19.12 | 15.91 | 4.69 | 19.77 | 11.69 | 14.58 | 10.42 | 0.00 | 22.22 | 14.55 | 11.52 | 0.37 | 0.07 |
| Dyspnea (n) | 0 | 0 | 1 | 0 | 3 | 10 | 8 | 4 | 10 | 8 | 12 | 9 | 9 | 10 | 13 | 4 | 13 | 5 | 1 | 3 | 70 | 53 | ||
| (%) | 0.00 | 0.00 | 12.50 | 0.00 | 6.67 | 17.54 | 18.18 | 8.33 | 15.15 | 13.79 | 17.39 | 13.24 | 10.23 | 15.63 | 15.12 | 5.19 | 27.08 | 10.42 | 6.67 | 11.11 | 14.55 | 11.11 | 0.15 | 0.45 |
| Loss of Taste (n) | 1 | 0 | 4 | 5 | 18 | 22 | 13 | 18 | 15 | 13 | 10 | 14 | 6 | 8 | 3 | 2 | 2 | 6 | 0 | 2 | 72 | 90 | ||
| (%) | 8.33 | 0.00 | 50.00 | 45.45 | 40.00 | 39.6 | 29.55 | 37.50 | 22.73 | 22.41 | 14.49 | 20.59 | 6.82 | 12.50 | 3.49 | 2.60 | 4.17 | 12.50 | 0 | 7.41 | 14.97 | 19.57 | <0.001 | <0.001 |
| Loss of Smell (n) | 0 | 0 | 0 | 0 | 5 | 3 | 2 | 1 | 1 | 0 | 0 | 0 | 0 | 2 | 0 | 1 | 0 | 0 | 0 | 0 | 8 | 7 | ||
| (%) | 0.00 | 0.00 | 0.00 | 0.00 | 11.11 | 5.26 | 4.55 | 2.08 | 1.52 | 0.00 | 0.00 | 0.00 | 0.00 | 3.13 | 0.00 | 1.30 | 0.00 | 0.00 | 0.00 | 0.00 | 1.66 | 1.47 | <0.001 | 0.36 |
| Reduced Appetite (n) | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 2 | 0 | 0 | 0 | 3 | 1 | 4 | 4 | 1 | 0 | 0 | 0 | 11 | 6 | ||
| (%) | 0.00 | 0.00 | 0.00 | 0.00 | 2.08 | 0.00 | 0.00 | 2.08 | 3.03 | 0.00 | 0.00 | 0.00 | 3.41 | 1.56 | 4.65 | 5.19 | 2.08 | 0.00 | 0.00 | 0.00 | 2.29 | 1.30 | 0.71 | 0.17 |
| Body Aches (n) | 0 | 0 | 2 | 3 | 6 | 9 | 14 | 8 | 15 | 11 | 11 | 14 | 14 | 5 | 8 | 5 | 1 | 0 | 0 | 1 | 71 | 56 | ||
| (%) | 0.00 | 0.00 | 25.00 | 27.27 | 13.33 | 15.79 | 31.82 | 16.67 | 22.72 | 18.97 | 15.94 | 20.59 | 15.91 | 7.69 | 9.30 | 6.02 | 2.08 | 0.00 | 0.00 | 3.70 | 14.76 | 12.17 | <0.001 | 0.01 |
| Nausea/Vomiting (n) | 0 | 0 | 1 | 3 | 0 | 4 | 1 | 1 | 0 | 2 | 0 | 1 | 2 | 5 | 1 | 3 | 0 | 2 | 0 | 1 | 5 | 22 | ||
| (%) | 0.00 | 0.00 | 12.50 | 27.27 | 0.00 | 7.02 | 2.27 | 2.08 | 0.00 | 3.45 | 0.00 | 1.47 | 2.27 | 7.81 | 1.16 | 3.90 | 0.00 | 4.17 | 0.00 | 3.70 | 1.04 | 4.78 | 0.10 | 0.05 |
| Phlegm (n) | 0 | 0 | 0 | 1 | 1 | 2 | 4 | 0 | 0 | 3 | 2 | 2 | 0 | 1 | 0 | 1 | 0 | 2 | 1 | 0 | 8 | 12 | ||
| (%) | 0.00 | 0.00 | 0.00 | 9.09 | 2.22 | 3.51 | 9.09 | 0.00 | 0.00 | 5.17 | 2.90 | 2.94 | 0.00 | 1.56 | 0.00 | 1.30 | 0.00 | 4.17 | 6.67 | 0.00 | 1.66 | 2.61 | 0.01 | 0.65 |
| Chill (n) | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 2 | 3 | ||
| (%) | 0.00 | 0.00 | 0.00 | 0.00 | 2.22 | 0.00 | 2.27 | 0.00 | 0.00 | 1.72 | 0.00 | 0.00 | 0.00 | 1.56 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 3.70 | 0.42 | 0.65 | 0.45 | 0.56 |
| Asymptomatic | 1–9 | 10–19 | 20–29 | 30–39 | 40–49 | 50–59 | 60–69 | 70–79 | 80–89 | 90–99 | Total | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | |
| No (n) | 12 | 2 | 8 | 11 | 46 | 58 | 44 | 48 | 68 | 59 | 71 | 72 | 91 | 65 | 91 | 83 | 52 | 50 | 18 | 27 | 515 | 497 |
| (%) | 100 | 40 | 57 | 85 | 92 | 75 | 90 | 75 | 84 | 82 | 95 | 82 | 89 | 81 | 84 | 81 | 80 | 56 | 78 | 52 | 87 | 74 |
| Yes (n) | 0 | 3 | 6 | 2 | 4 | 19 | 5 | 16 | 13 | 13 | 4 | 16 | 11 | 15 | 17 | 20 | 13 | 39 | 5 | 25 | 80 | 177 |
| (%) | 0 | 60 | 43 | 15 | 8 | 25 | 10 | 25 | 16 | 18 | 5 | 18 | 11 | 19 | 16 | 19 | 20 | 44 | 22 | 48 | 13 | 26 |
| Total (n) | 12 | 5 | 14 | 13 | 50 | 77 | 49 | 64 | 81 | 72 | 75 | 88 | 102 | 80 | 108 | 103 | 65 | 89 | 23 | 52 | 595 | 674 |
| (%) | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| p-value | 0.003 | 0.118 | 0.020 | 0.045 | 0.740 | 0.010 | 0.130 | 0.480 | 0.002 | 0.030 | <0.001 | |||||||||||
| Characteristics | Odds Ratio | p-Value | (95% C.I.) |
|---|---|---|---|
| Age | 1.01 | <0.001 | 1.01 1.02 |
| Female | 2.31 | <0.001 | 1.72 3.11 |
| Characteristics | Odds Ratio | p-Value | (95% C.I.) |
|---|---|---|---|
| Duration: PCR-onset | 1.05 | <0.001 | 1.03 1.08 |
| Male | 1.82 | <0.001 | 1.31 2.55 |
| Asymptomatic | 1.81 | 0.018 | 1.11 2.97 |
| Pneumonia | 0.46 | 0.019 | 0.24 0.88 |
| Characteristics | Odds Ratio | p-Value | (95% C.I.) |
|---|---|---|---|
| Regression 1 | |||
| Diarrhea | 1.82 | 0.05 | 1.01 3.29 |
| Male | 1.59 | 0.02 | 1.09 2.32 |
| Regression 2 | |||
| Nausea/Vomiting | 4.73 | <0.001 | 1.99 11.21 |
| Male | 1.71 | 0.01 | 1.17 2.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, M.-H.; Siddique, A.B.; Andalibi, A.; Koizumi, N. Analysis of Symptomology, Infectiveness, and Reinfections between Male and Female COVID-19 Patients: Evidence from Japanese Registry Data. Atmosphere 2021, 12, 1528. https://doi.org/10.3390/atmos12111528
Li M-H, Siddique AB, Andalibi A, Koizumi N. Analysis of Symptomology, Infectiveness, and Reinfections between Male and Female COVID-19 Patients: Evidence from Japanese Registry Data. Atmosphere. 2021; 12(11):1528. https://doi.org/10.3390/atmos12111528
Chicago/Turabian StyleLi, Meng-Hao, Abu Bakkar Siddique, Ali Andalibi, and Naoru Koizumi. 2021. "Analysis of Symptomology, Infectiveness, and Reinfections between Male and Female COVID-19 Patients: Evidence from Japanese Registry Data" Atmosphere 12, no. 11: 1528. https://doi.org/10.3390/atmos12111528
APA StyleLi, M.-H., Siddique, A. B., Andalibi, A., & Koizumi, N. (2021). Analysis of Symptomology, Infectiveness, and Reinfections between Male and Female COVID-19 Patients: Evidence from Japanese Registry Data. Atmosphere, 12(11), 1528. https://doi.org/10.3390/atmos12111528