
Lack of Association between LOXL1 Variants and Pigment Dispersion Syndrome/Pigmentary Glaucoma: A Meta-Analysis



Abstract
1. Introduction
2. Materials and Methods
2.1. Identification of Gene Association Studies Testing
2.2. Data Extraction
2.3. Quanlity Assessment and Control of Risk of Bias
2.4. Genetic Meta-Analysis
2.5. Functional Annotation of Gene Variants
2.6. Power Analysis
3. Results
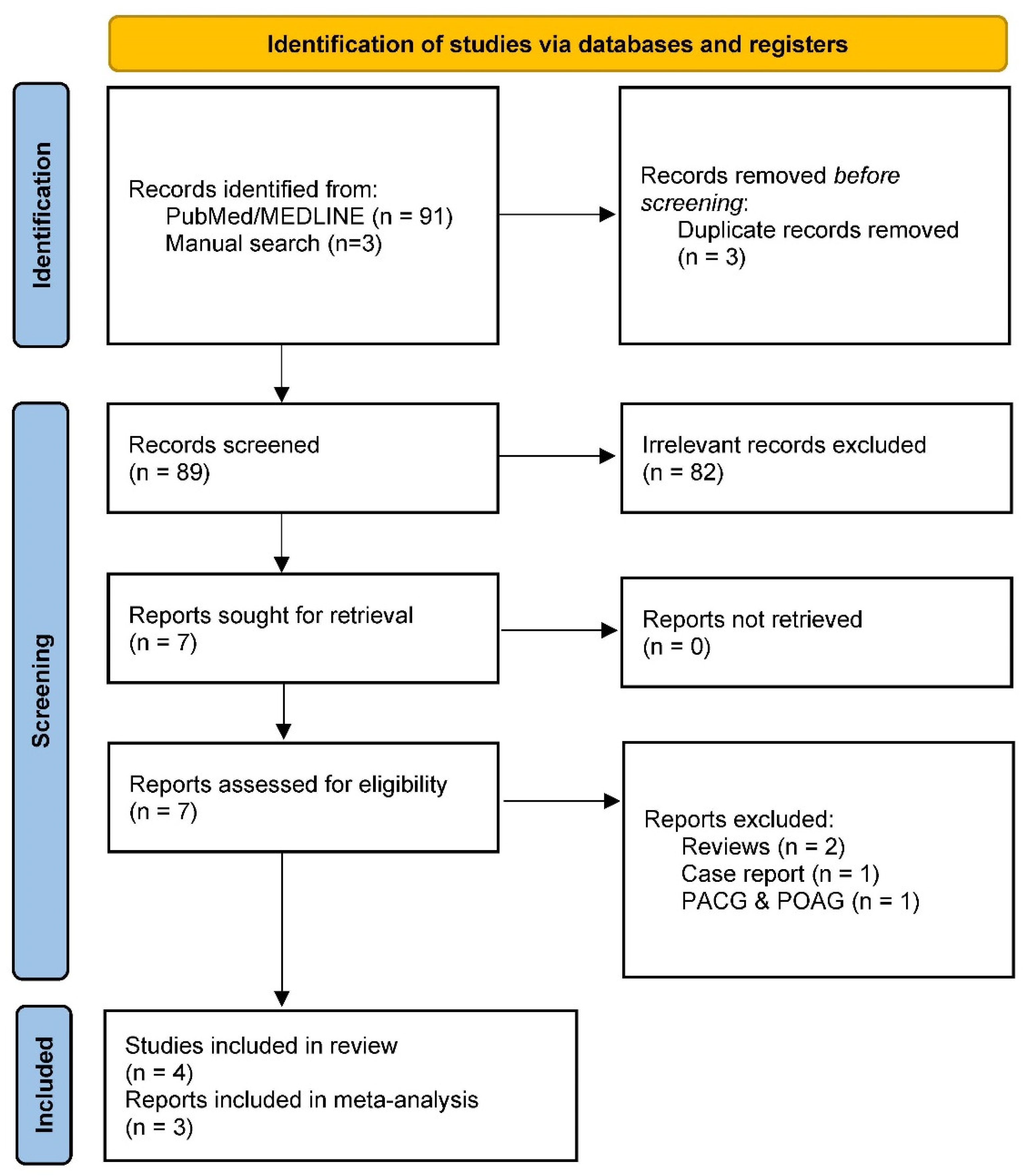
3.1. Studies Testing XFS/XFG-Associated Genes in PDS/PG
3.2. Genetic Association of LOXL1 with PDS/PG
3.3. Risk of Bias Assessments and Sensitivity Analysis
3.4. Functional Relevance of the LOXL1 Coding Variants
3.5. Power Analysis
4. Discussion
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A. Newcastle–Ottawa Quality Assessment Scale for Case Control Studies
- NEWCASTLE—OTTAWA QUALITY ASSESSMENT SCALE
- CASE CONTROL STUDIES
- (accessed via http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp)
- Note: A study can be awarded a maximum of one star for each numbered item within the Selection and Exposure categories. A maximum of two stars can be given for Comparability.
- Selection
- (1)
- Is the case definition adequate?
- (a)
- Yes, with independent validation.
- (b)
- Yes, e.g., record linkage or based on self-reports.
- (c)
- No description.
- (2)
- Representativeness of the cases
- (a)
- Consecutive or obviously representative series of cases.
- (b)
- Potential for selection biases or not stated.
- (3)
- Selection of Controls
- (a)
- Community controls.
- (b)
- Hospital controls.
- (c)
- No description.
- (4)
- Definition of controls
- (a)
- No history of disease (endpoint).
- (b)
- No description of source.
- Comparability
- (1)
- Comparability of cases and controls on the basis of the design or analysis
- (a)
- Study controls for _______________ (select the most important factor: ethnicity).
- (b)
- Study controls for any additional factor (these criteria could be modified to indicate specific control for a second important factor).
- Exposure
- (1)
- Ascertainment of exposure
- (a)
- Secure record (e.g., surgical records).
- (b)
- Structured interview where blind to case/control status.
- (c)
- Interview not blinded to case/control status.
- (d)
- Written self-report or medical record only.
- (e)
- No description.
- (2)
- Same method of ascertainment for cases and controls
- (a)
- Yes.
- (b)
- No.
- (3)
- Non-response rate
- (a)
- Same rate for both groups.
- (b)
- Non respondents described.
- (c)
- Rate different and no designation.
References
- Migliazzo, C.V.; Shaffer, R.N.; Nykin, R.; Magee, S. Long-term analysis of pigmentary dispersion syndrome and pigmentary glaucoma. Ophthalmology 1986, 93, 1528–1536. [Google Scholar] [CrossRef]
- Ritch, R.; Steinberger, D.; Liebmann, J.M. Prevalence of pigment dispersion syndrome in a population undergoing glaucoma screening. Am. J. Ophthalmol. 1993, 115, 707–710. [Google Scholar] [CrossRef]
- Roberts, D.K.; Chaglasian, M.A.; Meetz, R.E. Clinical signs of the pigment dispersion syndrome in blacks. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 1997, 74, 993–1006. [Google Scholar] [CrossRef]
- Qing, G.; Wang, N.; Tang, X.; Zhang, S.; Chen, H. Clinical characteristics of pigment dispersion syndrome in Chinese patients. Eye 2009, 23, 1641–1646. [Google Scholar] [CrossRef]
- Yamamoto, T.; Iwase, A.; Araie, M.; Suzuki, Y.; Abe, H.; Shirato, S.; Kuwayama, Y.; Mishima, H.K.; Shimizu, H.; Tomita, G.; et al. The Tajimi Study report 2: Prevalence of primary angle closure and secondary glaucoma in a Japanese population. Ophthalmology 2005, 112, 1661–1669. [Google Scholar] [CrossRef]
- Farrar, S.M.; Shields, M.B.; Miller, K.N.; Stoup, C.M. Risk factors for the development and severity of glaucoma in the pigment dispersion syndrome. Am. J. Ophthalmol. 1989, 108, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Richter, C.U.; Richardson, T.M.; Grant, W.M. Pigmentary dispersion syndrome and pigmentary glaucoma. A prospective study of the natural history. Arch. Ophthalmol. 1986, 104, 211–215. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, Y.; Ten Hulzen, R.D.; Cameron, J.D.; Hodge, D.O.; Johnson, D.H. What is the risk of developing pigmentary glaucoma from pigment dispersion syndrome? Am. J. Ophthalmol. 2003, 135, 794–799. [Google Scholar] [CrossRef] [PubMed]
- Scheie, H.G.; Cameron, J.D. Pigment dispersion syndrome: A clinical study. Br. J. Ophthalmol. 1981, 65, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.W.; Sakiyalak, D.; Krupin, T. Pigmentary glaucoma. J. Glaucoma 2001, 10, S30–S32. [Google Scholar] [CrossRef] [PubMed]
- Lindberg, J.G. Clinical investigations on depigmentation of the pupillary border and translucency of the iris in cases of senile cataract and in normal eyes in elderly persons. Acta Ophthalmol. Suppl. 1989, 190, 1–96. [Google Scholar]
- Ritch, R. Ocular and systemic manifestations of exfoliation syndrome. J. Glaucoma 2014, 23, S1–S8. [Google Scholar] [CrossRef]
- Idakwo, U.; Olawoye, O.; Ajayi, B.G.; Ritch, R. Exfoliation syndrome in Northern Nigeria. Clin. Ophthalmol. 2018, 12, 271–277. [Google Scholar] [CrossRef]
- Olawoye, O.O.; Ashaye, A.O.; Teng, C.C.; Liebmann, J.M.; Ritch, R.; Ajayi, B.G. Exfoliation syndrome in Nigeria. Middle East Afr. J. Ophthalmol. 2012, 19, 402–405. [Google Scholar] [CrossRef] [PubMed]
- Schlotzer-Schrehardt, U.; Naumann, G.O. Ocular and systemic pseudoexfoliation syndrome. Am. J. Ophthalmol. 2006, 141, 921–937. [Google Scholar] [CrossRef] [PubMed]
- Arnarsson, A.; Damji, K.F.; Sverrisson, T.; Sasaki, H.; Jonasson, F. Pseudoexfoliation in the Reykjavik Eye Study: Prevalence and related ophthalmological variables. Acta Ophthalmol. Scand. 2007, 85, 822–827. [Google Scholar] [CrossRef] [PubMed]
- Topouzis, F.; Wilson, M.R.; Harris, A.; Anastasopoulos, E.; Yu, F.; Mavroudis, L.; Pappas, T.; Koskosas, A.; Coleman, A.L. Prevalence of open-angle glaucoma in Greece: The Thessaloniki Eye Study. Am. J. Ophthalmol. 2007, 144, 511–519. [Google Scholar] [CrossRef]
- Topouzis, F.; Founti, P.; Yu, F.; Wilson, M.R.; Coleman, A.L. Twelve-Year Incidence and Baseline Risk Factors for Pseudoexfoliation: The Thessaloniki Eye Study (An American Ophthalmological Society Thesis). Am. J. Ophthalmol. 2019, 206, 192–214. [Google Scholar] [CrossRef]
- Shazly, T.A.; Farrag, A.N.; Kamel, A.; Al-Hussaini, A.K. Prevalence of pseudoexfoliation syndrome and pseudoexfoliation glaucoma in Upper Egypt. BMC Ophthalmol. 2011, 11, 18. [Google Scholar] [CrossRef]
- Rao, R.Q.; Arain, T.M.; Ahad, M.A. The prevalence of pseudoexfoliation syndrome in Pakistan. Hospital based study. BMC Ophthalmol. 2006, 6, 27. [Google Scholar] [CrossRef]
- Kılıç, R.; Karagöz, N.; Çetin, A.B.; Çakmak, Y.; Sezer, H.; Özay, Y.; Çomçalı, S.; Dursun, A. The prevalence of exfoliation syndrome in Turkey. Acta Ophthalmol. 2016, 94, e105–e108. [Google Scholar] [CrossRef] [PubMed]
- Tenkir, A.; Solomon, B.; Deribew, A. Glaucoma subtypes in Ethiopian clinic patients. J. Glaucoma 2013, 22, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Giorgis, A.T.; Mulugeta, A.; Aga, A.; Deyassa, N. The spectrum of glaucoma presentation at Menelik II Hospital, Addis Ababa. Ethiop. Med. J. 2012, 50, 259–264. [Google Scholar] [PubMed]
- Ren, R.; Ding, J.; Wang, N.; Teng, C.C.; de Moraes, G.V.; Jonas, J.B.; Ritch, R. Clinical Signs and Characteristics of Exfoliation Syndrome and Exfoliative Glaucoma in Northern China. Asia Pac. J. Ophthalmol. 2015, 4, 86–88. [Google Scholar] [CrossRef]
- Zhang, H.; Jia, H.; Duan, X.; Li, L.; Wang, H.; Wu, J.; Hu, J.; Cao, K.; Zhao, A.; Liang, J.; et al. The Chinese Glaucoma Study Consortium for Patients With Glaucoma: Design, Rationale and Baseline Patient Characteristics. J. Glaucoma 2019, 28, 974–978. [Google Scholar] [CrossRef]
- Andersen, J.S.; Pralea, A.M.; DelBono, E.A.; Haines, J.L.; Gorin, M.B.; Schuman, J.S.; Mattox, C.G.; Wiggs, J.L. A gene responsible for the pigment dispersion syndrome maps to chromosome 7q35–q36. Arch. Ophthalmol. 1997, 115, 384–388. [Google Scholar] [CrossRef]
- Wiggs, J.L.; Del Bono, E.A.; Schuman, J.S.; Hutchinson, B.T.; Walton, D.S. Clinical features of five pedigrees genetically linked to the juvenile glaucoma locus on chromosome 1q21–q31. Ophthalmology 1995, 102, 1782–1789. [Google Scholar] [CrossRef]
- Paglinauan, C.; Haines, J.L.; Del Bono, E.A.; Schuman, J.; Stawski, S.; Wiggs, J.L. Exclusion of chromosome 1q21-q31 from linkage to three pedigrees affected by the pigment-dispersion syndrome. Am. J. Hum. Genet. 1995, 56, 1240–1243. [Google Scholar]
- Simcoe, M.J.; Shah, A.; Fan, B.; Choquet, H.; Weisschuh, N.; Waseem, N.H.; Jiang, C.; Melles, R.B.; Ritch, R.; Mahroo, O.A.; et al. Genome-Wide Association Study Identifies Two Common Loci Associated with Pigment Dispersion Syndrome/Pigmentary Glaucoma and Implicates Myopia in its Development. Ophthalmology 2022, 129, 626–636. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Zeng, L.; Wang, Y.; Liu, G.; Huang, L.; Chen, D.; Wang, X.; Fan, N.; He, Y.; Liu, X. Compound Heterozygous Variants of the CPAMD8 Gene Co-Segregating in Two Chinese Pedigrees With Pigment Dispersion Syndrome/Pigmentary Glaucoma. Front. Genet. 2022, 13, 845081. [Google Scholar] [CrossRef] [PubMed]
- van der Heide, C.; Goar, W.; Meyer, K.J.; Alward, W.L.M.; Boese, E.A.; Sears, N.C.; Roos, B.R.; Kwon, Y.H.; DeLuca, A.P.; Siggs, O.M.; et al. Exome-based investigation of the genetic basis of human pigmentary glaucoma. BMC Genom. 2021, 22, 477. [Google Scholar] [CrossRef] [PubMed]
- Lahola-Chomiak, A.A.; Footz, T.; Nguyen-Phuoc, K.; Neil, G.J.; Fan, B.; Allen, K.F.; Greenfield, D.S.; Parrish, R.K.; Linkroum, K.; Pasquale, L.R.; et al. Non-Synonymous variants in premelanosome protein (PMEL) cause ocular pigment dispersion and pigmentary glaucoma. Hum. Mol. Genet. 2019, 28, 1298–1311. [Google Scholar] [CrossRef] [PubMed]
- Hodges, E.D.; Chrystal, P.W.; Footz, T.; Doucette, L.P.; Noel, N.C.L.; Li, Z.; Walter, M.A.; Allison, W.T. Disrupting the Repeat Domain of Premelanosome Protein (PMEL) Produces Dysamyloidosis and Dystrophic Ocular Pigment Reflective of Pigmentary Glaucoma. Int. J. Mol. Sci. 2023, 24, 14424. [Google Scholar] [CrossRef] [PubMed]
- Thorleifsson, G.; Magnusson, K.P.; Sulem, P.; Walters, G.B.; Gudbjartsson, D.F.; Stefansson, H.; Jonsson, T.; Jonasdottir, A.; Jonasdottir, A.; Stefansdottir, G.; et al. Common sequence variants in the LOXL1 gene confer susceptibility to exfoliation glaucoma. Science 2007, 317, 1397–1400. [Google Scholar] [CrossRef] [PubMed]
- Aung, T.; Ozaki, M.; Mizoguchi, T.; Allingham, R.R.; Li, Z.; Haripriya, A.; Nakano, S.; Uebe, S.; Harder, J.M.; Chan, A.S.; et al. A common variant mapping to CACNA1A is associated with susceptibility to exfoliation syndrome. Nat. Genet. 2015, 47, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Aung, T.; Ozaki, M.; Lee, M.C.; Schlötzer-Schrehardt, U.; Thorleifsson, G.; Mizoguchi, T.; Igo, R.P., Jr.; Haripriya, A.; Williams, S.E.; Astakhov, Y.S.; et al. Genetic association study of exfoliation syndrome identifies a protective rare variant at LOXL1 and five new susceptibility loci. Nat. Genet. 2017, 49, 993–1004. [Google Scholar] [CrossRef]
- Rao, K.N.; Ritch, R.; Dorairaj, S.K.; Kaur, I.; Liebmann, J.M.; Thomas, R.; Chakrabarti, S. Exfoliation syndrome and exfoliation glaucoma-associated LOXL1 variations are not involved in pigment dispersion syndrome and pigmentary glaucoma. Mol. Vis. 2008, 14, 1254–1262. [Google Scholar] [PubMed]
- Wolf, C.; Gramer, E.; Müller-Myhsok, B.; Pasutto, F.; Gramer, G.; Wissinger, B.; Weisschuh, N. Lysyl oxidase-like 1 gene polymorphisms in German patients with normal tension glaucoma, pigmentary glaucoma and exfoliation glaucoma. J. Glaucoma 2010, 19, 136–141. [Google Scholar] [CrossRef]
- Giardina, E.; Oddone, F.; Lepre, T.; Centofanti, M.; Peconi, C.; Tanga, L.; Quaranta, L.; Frezzotti, P.; Novelli, G.; Manni, G. Common sequence variants in the LOXL1 gene in pigment dispersion syndrome and pigmentary glaucoma. BMC Ophthalmol. 2014, 14, 52. [Google Scholar] [CrossRef]
- Fan, B.J.; Pasquale, L.; Grosskreutz, C.L.; Rhee, D.; Chen, T.; DeAngelis, M.M.; Kim, I.; del Bono, E.; Miller, J.W.; Li, T.; et al. DNA sequence variants in the LOXL1 gene are associated with pseudoexfoliation glaucoma in a U.S. clinic-based population with broad ethnic diversity. BMC Med. Genet. 2008, 9, 5. [Google Scholar] [CrossRef]
- Kirkwood, B.; Sterne, J. Essentials of Medical Statistics, 2nd ed.; Blackwell Science: Hoboken, NJ, USA, 2003; p. 501. [Google Scholar]
- Kmet, L.M.; Lee, R.C.; Cook, L.S. Standard Quality Assessment Criteria for Evaluating Primary Research Papers from a Variety of Fields; Alberta Heritage Foundation for Medical Research: Edmonton, AB, Canada, 2004; p. 22. [Google Scholar]
- Khan, K.S.; Riet, G.t.; Popay, J.; Nixon, J.; Kleijnen, J. Conducting the review: Phase 5 study quality assessment. In Undertaking Systematic Reviews of Research Effectiveness CDC’s Guidance for Those Carrying Out or Commissioning Reviews; University of York Centre for Reviews and Dissemination: Heslington, UK, 2001; p. 20. [Google Scholar]
- Squires, J.E.; Estabrooks, C.A.; Gustavsson, P.; Wallin, L. Individual determinants of research utilization by nurses: A systematic review update. Implement. Sci. IS 2011, 6, 11. [Google Scholar] [CrossRef]
- McPheeters, M.L.; Kripalani, S.; Peterson, N.B.; Idowu, R.T.; Jerome, R.N.; Potter, S.A.; Andrews, J.C. Closing the quality gap: Revisiting the state of the science (vol. 3: Quality improvement interventions to address health disparities). Evid. Rep./Technol. Assess. 2012, 3, 1–475. [Google Scholar]
- Peters, J.L.; Sutton, A.J.; Jones, D.R.; Abrams, K.R.; Rushton, L. Contour-enhanced meta-analysis funnel plots help distinguish publication bias from other causes of asymmetry. J. Clin. Epidemiol. 2008, 61, 991–996. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions. Available online: www.cochrane-handbook.org (accessed on 20 November 2023).
- Sterne, J.A.; Gavaghan, D.; Egger, M. Publication and related bias in meta-analysis: Power of statistical tests and prevalence in the literature. J. Clin. Epidemiol. 2000, 53, 1119–1129. [Google Scholar] [CrossRef] [PubMed]
- Rong, S.S.; Peng, Y.; Liang, Y.B.; Cao, D.; Jhanji, V. Does cigarette smoking alter the risk of pterygium? A systematic review and meta-analysis. Investig. Ophthalmol. Vis. Sci. 2014, 55, 6235–6243. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.H.; Rong, S.S.; Chong, K.K.; Young, A.L.; Pang, C.P.; Chen, L.J. Genetic Associations of Interleukin-related Genes with Graves’ Ophthalmopathy: A Systematic Review and Meta-analysis. Sci. Rep. 2015, 5, 16672. [Google Scholar] [CrossRef]
- Yu, X.; Rong, S. Genome-Wide Associations and Confirmatory Meta-Analyses in Diabetic Retinopathy. Genes 2023, 14, 653. [Google Scholar] [CrossRef]
- Rong, S.S.; Yu, X. Phenotypic and Genetic Links between Body Fat Measurements and Primary Open-Angle Glaucoma. Int. J. Mol. Sci. 2023, 24, 3925. [Google Scholar] [CrossRef]
- Lu, S.Y.; Rong, S.S.; Wu, Z.; Huang, C.; Matsushita, K.; Ng, T.K.; Leung, C.K.S.; Kawashima, R.; Usui, S.; Tam, P.O.S.; et al. Association of the CAV1-CAV2 locus with normal-tension glaucoma in Chinese and Japanese. Clin. Exp. Ophthalmol. 2020, 48, 658–665. [Google Scholar] [CrossRef] [PubMed]
- Rong, S.S.; Lu, S.Y.; Matsushita, K.; Huang, C.; Leung, C.K.S.; Kawashima, R.; Usui, S.; Tam, P.O.S.; Young, A.L.; Tsujikawa, M.; et al. Association of the SIX6 locus with primary open angle glaucoma in southern Chinese and Japanese. Exp. Eye Res. 2019, 180, 129–136. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Vaser, R.; Adusumalli, S.; Leng, S.N.; Sikic, M.; Ng, P.C. SIFT missense predictions for genomes. Nat. Protoc. 2016, 11, 1–9. [Google Scholar] [CrossRef]
- Adzhubei, I.A.; Schmidt, S.; Peshkin, L.; Ramensky, V.E.; Gerasimova, A.; Bork, P.; Kondrashov, A.S.; Sunyaev, S.R. A method and server for predicting damaging missense mutations. Nat. Methods 2010, 7, 248–249. [Google Scholar] [CrossRef]
- Kircher, M.; Witten, D.M.; Jain, P.; O’Roak, B.J.; Cooper, G.M.; Shendure, J. A general framework for estimating the relative pathogenicity of human genetic variants. Nat. Genet. 2014, 46, 310–315. [Google Scholar] [CrossRef]
- Boyle, A.P.; Hong, E.L.; Hariharan, M.; Cheng, Y.; Schaub, M.A.; Kasowski, M.; Karczewski, K.J.; Park, J.; Hitz, B.C.; Weng, S.; et al. Annotation of functional variation in personal genomes using RegulomeDB. Genome Res. 2012, 22, 1790–1797. [Google Scholar] [CrossRef] [PubMed]
- Consortium, G.T. The Genotype-Tissue Expression (GTEx) project. Nat. Genet. 2013, 45, 580–585. [Google Scholar] [CrossRef]
- Lascaratos, G.; Shah, A.; Garway-Heath, D.F. The genetics of pigment dispersion syndrome and pigmentary glaucoma. Surv. Ophthalmol. 2013, 58, 164–175. [Google Scholar] [CrossRef]
- Chakrabarti, S.; Rao, K.N.; Kaur, I.; Parikh, R.S.; Mandal, A.K.; Chandrasekhar, G.; Thomas, R. The LOXL1 gene variations are not associated with primary open-angle and primary angle-closure glaucomas. Investig. Ophthalmol. Vis. Sci. 2008, 49, 2343–2347. [Google Scholar] [CrossRef]
- Pokrovskaya, O.; O’Brien, C. What’s in a Gene? Pseudoexfoliation Syndrome and Pigment Dispersion Syndrome in the Same Patient. Case Rep. Ophthalmol. 2016, 7, 54–60. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Author | Country | Ethnicity | Phenotypes | Sample Size | Age of Cases/Control | Studied SNPs | Ref. | |
|---|---|---|---|---|---|---|---|---|
| Case | Control | |||||||
| Giardina, E., et al. (2014) | Italy | Caucasians | PDS/PG | 84 | 200 | 48.0 ± 4.9 / 46.7 ± 5.2 | rs1048661, rs3825942, rs2165241, rs2304722, rs8818, rs3522 | [39] |
| Wolf, C., et al. (2010) | German | Caucasians | PG | 88 | 280 | 53.8 ± 13.5 / 66 ± 13 | rs2165241, rs1048661, rs3825942, rs893818, rs1530169, rs750460, rs1284049 | [38] |
| Rao, K.N., et al. (2008) | USA | Caucasians | PDS+PG | 78 | 108 | Not reported | rs1048661, rs3825942, rs2165241 | [37] |
| SNP | Position (GRCh38) | Functional Relevance | Author (Year) | Phenotypes Studied | Sample Size | Effect Allele | Ref. Allele | A1 Frequency | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Case | Control | Cases | Controls | |||||||
| rs1048661 | Chr15:73927205 | Exon 1 Arg141Leu | [39] | PDS/PG | 84 | 200 | T | G | 0.340 | 0.290 |
| [38] | PG | 88 | 280 | T | G | 0.369 | 0.340 | |||
| [37] | PDS + PG | 78 | 108 | T | G | 0.326 | 0.276 | |||
| rs3825942 | Chr15:73927241 | Exon 1 Gly153Asp | [39] | PDS/PG | 84 | 200 | A | G | 0.160 | 0.200 |
| [38] | PG | 88 | 280 | A | G | 0.119 | 0.154 | |||
| [37] | PDS + PG | 78 | 108 | A | G | 0.148 | 0.178 | |||
| rs2165241 | Chr15:73929861 | Intron 1 | [39] | PDS/PG | 84 | 200 | T | C | 0.490 | 0.500 |
| [38] | PG | 88 | 280 | T | C | 0.488 | 0.491 | |||
| [37] | PDS + PG | 78 | 108 | T | C | 0.514 | 0.471 | |||
| Author (Year of Publication) | Newcastle–Ottawa Quality Assessment Scale for Case-Control Studies | Reference | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Selection | Comparability | Exposure | Total Stars | |||||||
| 1 | 2 | 3 | 4 | 1 | 1 | 2 | 3 | |||
| Giardina, E., et al. (2014) | a | a | b | a | age, sex, ethnicity | a | a | a | 8 | [39] |
| Wolf, C., et al. (2010) | a | a | b | a | age, sex, ethnicity | a | a | a | 8 | [38] |
| Rao, K.N., et al. (2008) | a | a | b | a | not reported | a | a | a | 7 | [37] |
| SNP | Position | Gene | Location | SIFT | PolyPhen | CADD | RegulomeDB * | eQTL Tissue (p)—Allele for Higher Expression |
|---|---|---|---|---|---|---|---|---|
| rs1048661 | Chr15:73927205 | LOXL1 | Exon 1 Arg141Leu | Deleterious | Benign | 24.4 | 1f | Cells—Cultured fibroblasts (1.40 × 10−12)—G |
| rs3825942 | Chr15:73927241 | LOXL1 | Exon 1 Gly153Asp | Deleterious | Benign | 22.9 | 1b | Cells—Cultured fibroblasts (8.50 × 10−37)—A |
| rs2165241 | Chr15:73929861 | LOXL1 | Intron 1 | na | na | 9.749 | 1f | Pituitary (1.30 × 10−10)—C |
| PDS/PG | XFS/XFG | |
|---|---|---|
| Comparable manifestations | ||
| Prevalence | More common in Caucasians | More common in Caucasians |
| Cornea | Krukenberg’s spindle | Occasional endothelial pigment |
| Iris | Mid-peripheral iris transillumination defects | Transillumination at pupillary border |
| Iridocorneal angle | Open, posterior iris bowing, TM pigmentation | Open, TM pigmentation |
| Different manifestations | ||
| Age of onset | Young | Elderly |
| Gender preference | Male | Female |
| Inheritance | Autosomal dominant, autosomal recessive, or sporadic | Undefined |
| Anterior chamber | Floating pigment | Quiet |
| Exfoliation material | None | Visible on pupillary border and anterior lens |
| Lens | Normal | Exfoliation material, weak zonules |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rong, S.; Yu, X. Lack of Association between LOXL1 Variants and Pigment Dispersion Syndrome/Pigmentary Glaucoma: A Meta-Analysis. Genes 2024, 15, 161. https://doi.org/10.3390/genes15020161
Rong S, Yu X. Lack of Association between LOXL1 Variants and Pigment Dispersion Syndrome/Pigmentary Glaucoma: A Meta-Analysis. Genes. 2024; 15(2):161. https://doi.org/10.3390/genes15020161
Chicago/Turabian StyleRong, Shisong, and Xinting Yu. 2024. "Lack of Association between LOXL1 Variants and Pigment Dispersion Syndrome/Pigmentary Glaucoma: A Meta-Analysis" Genes 15, no. 2: 161. https://doi.org/10.3390/genes15020161
APA StyleRong, S., & Yu, X. (2024). Lack of Association between LOXL1 Variants and Pigment Dispersion Syndrome/Pigmentary Glaucoma: A Meta-Analysis. Genes, 15(2), 161. https://doi.org/10.3390/genes15020161