
The Significance of Mylohyoid Muscle Release (MMR) in the Vertical and Horizontal Ridge Augmentation Surgeries; Clinical and Human Cadaver Analyses of the Techniques



Abstract
1. Introduction
2. Presentation of the Techniques
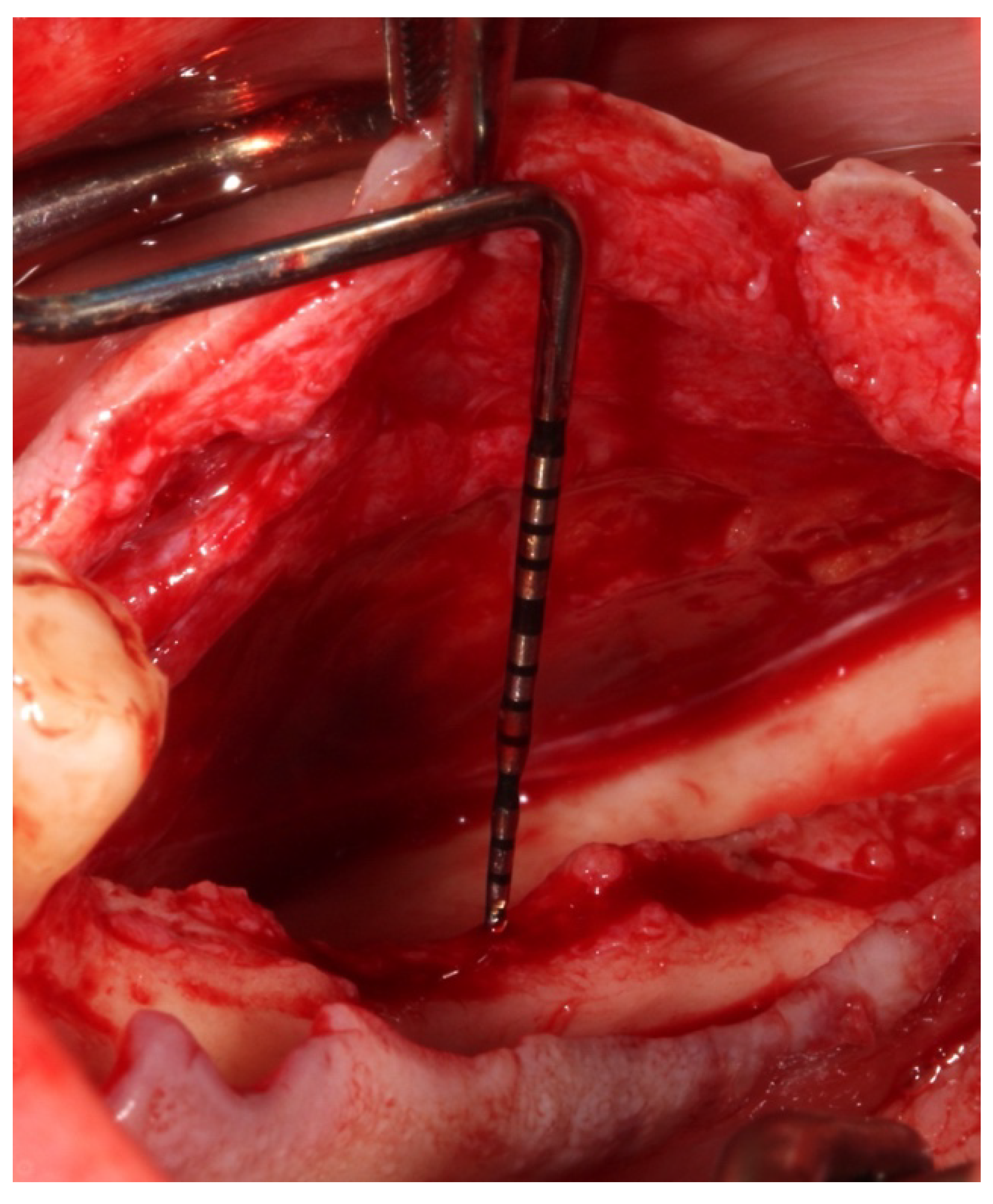
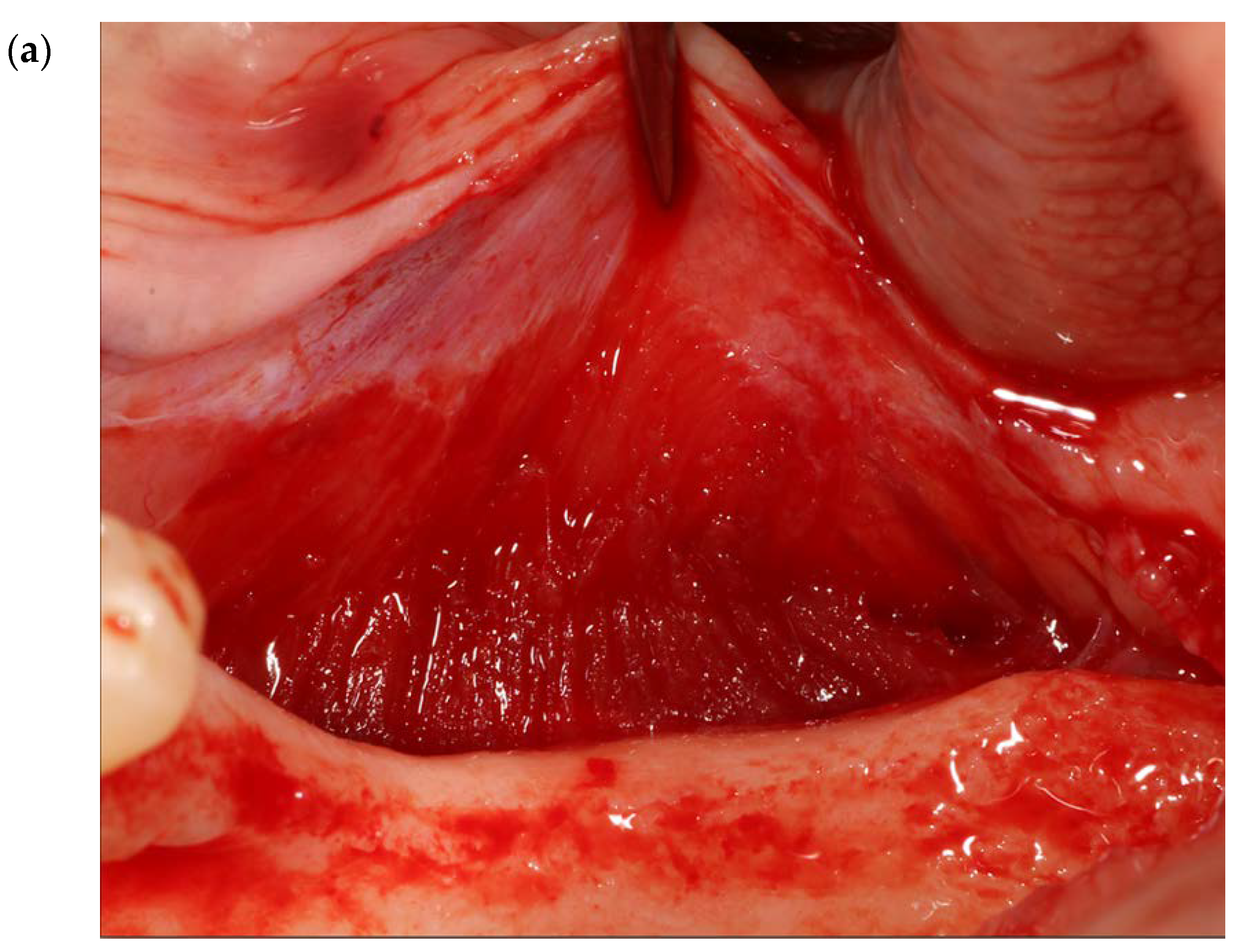
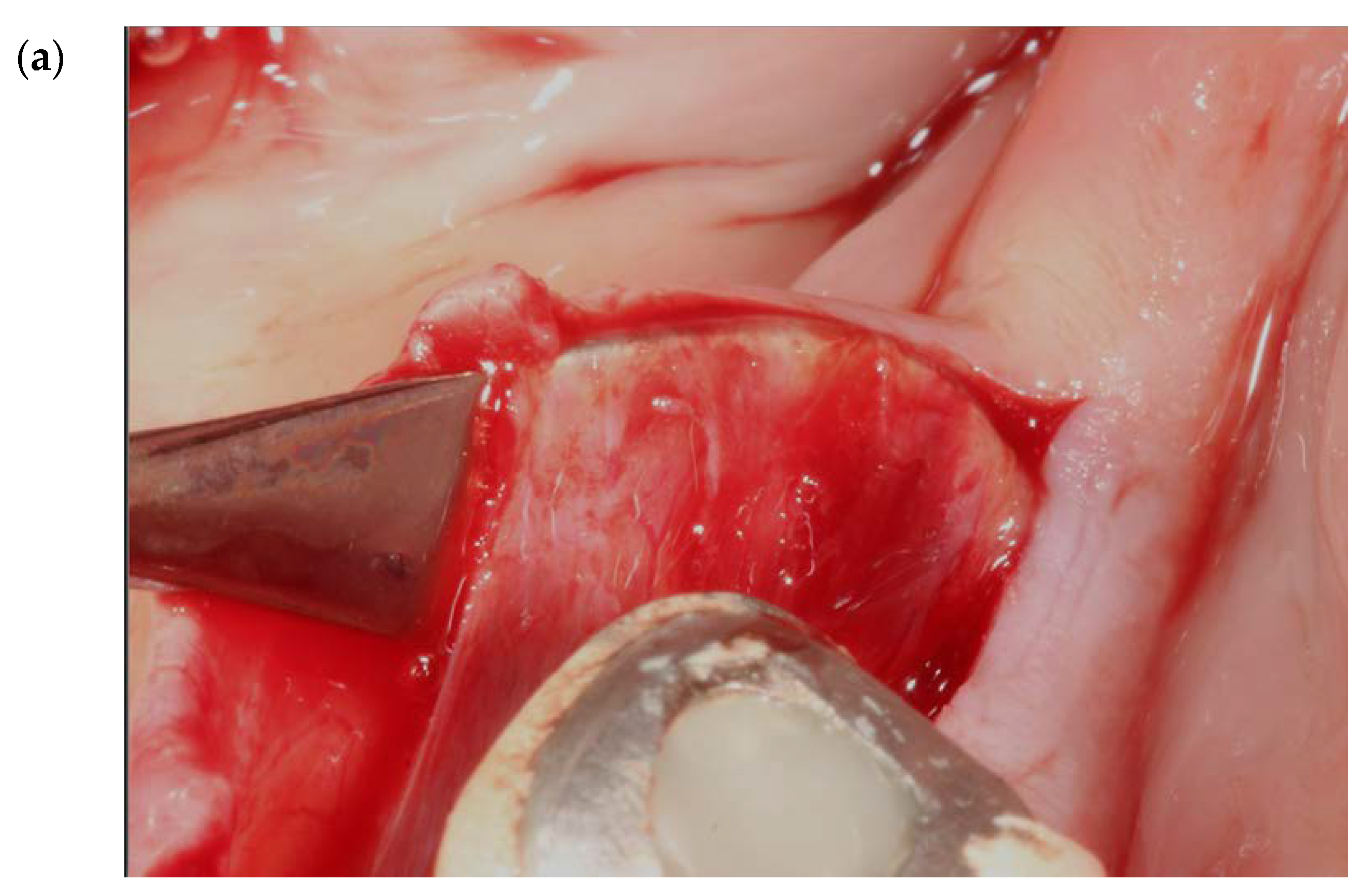
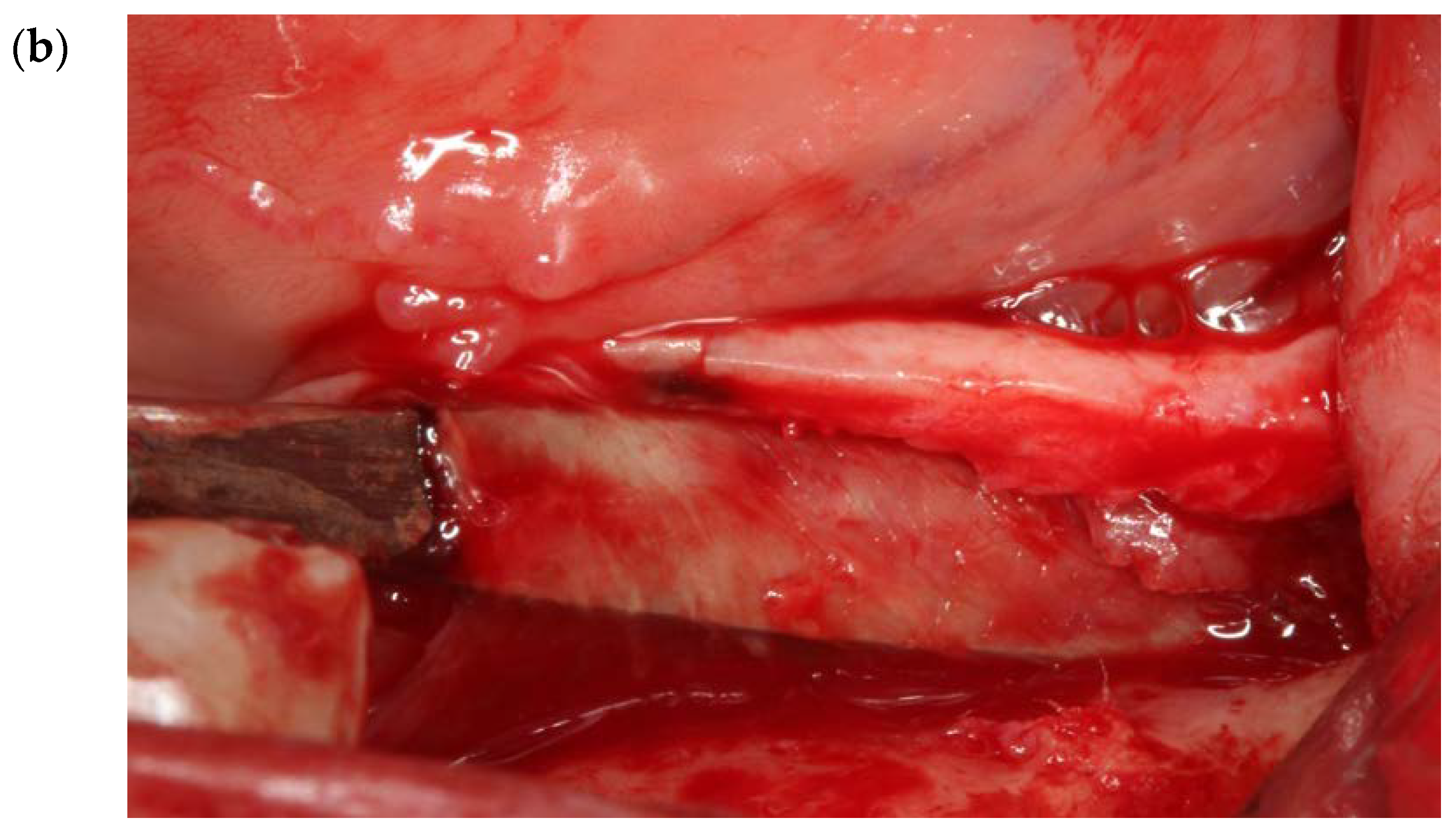
2.1. Finger Sweep Technique (FST) [19,22,27]
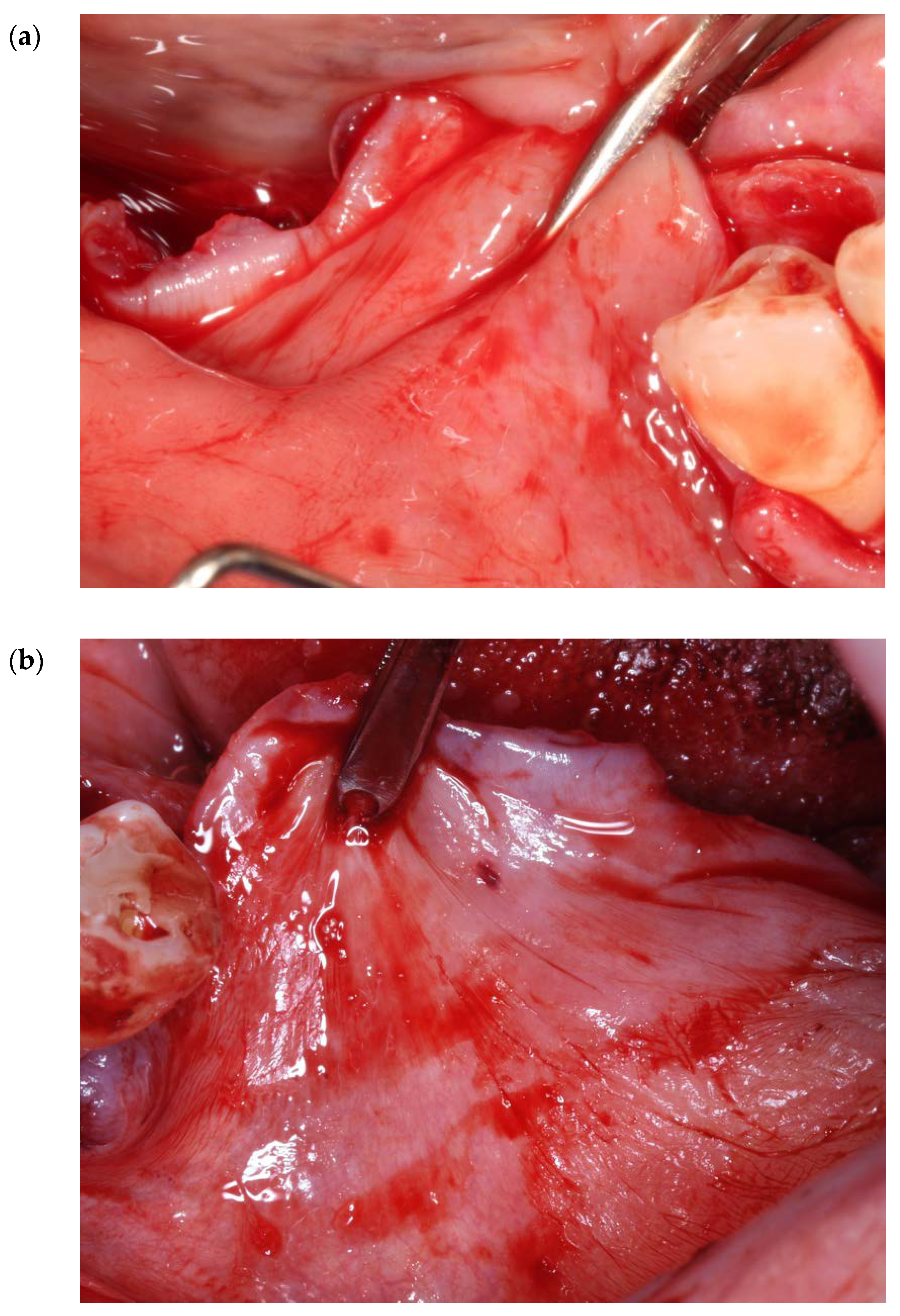
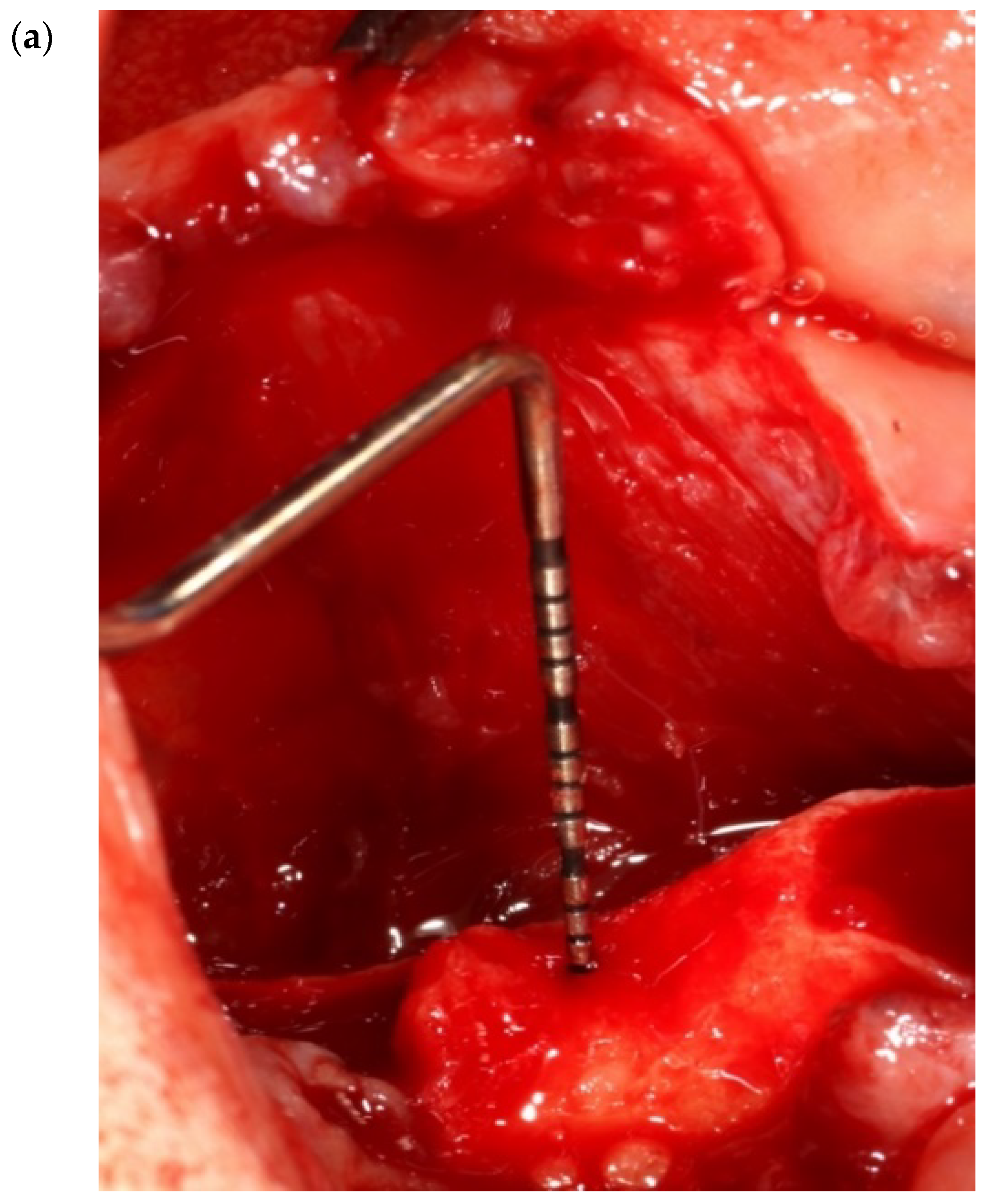
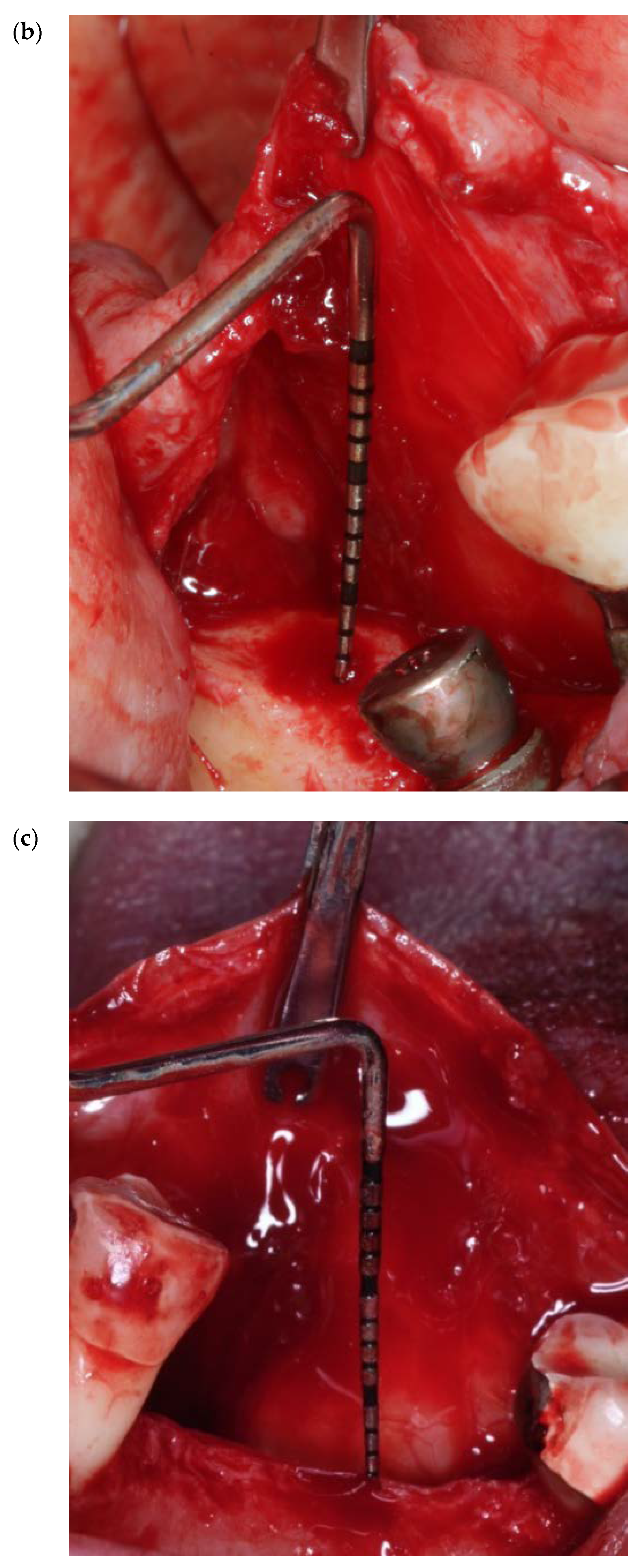
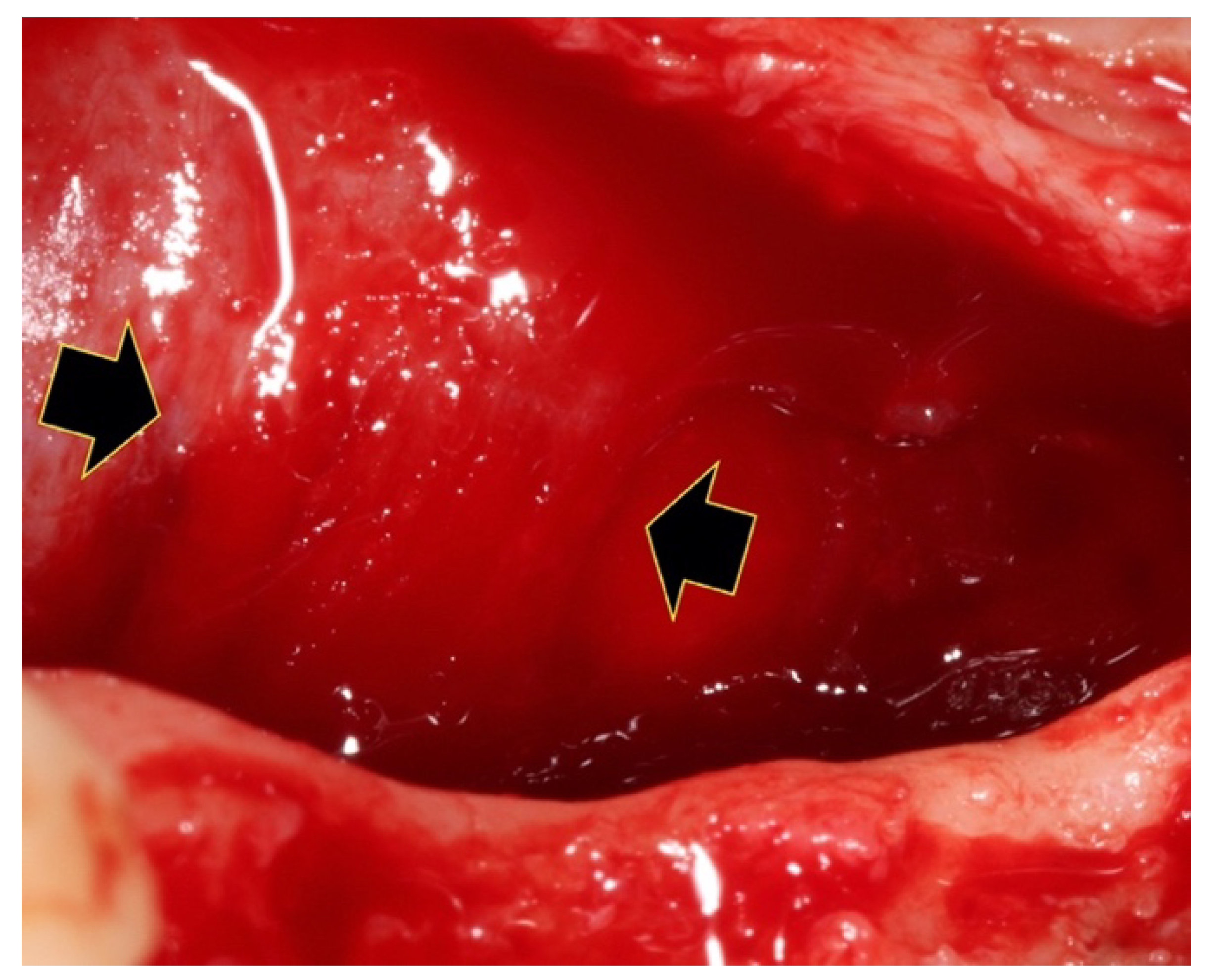
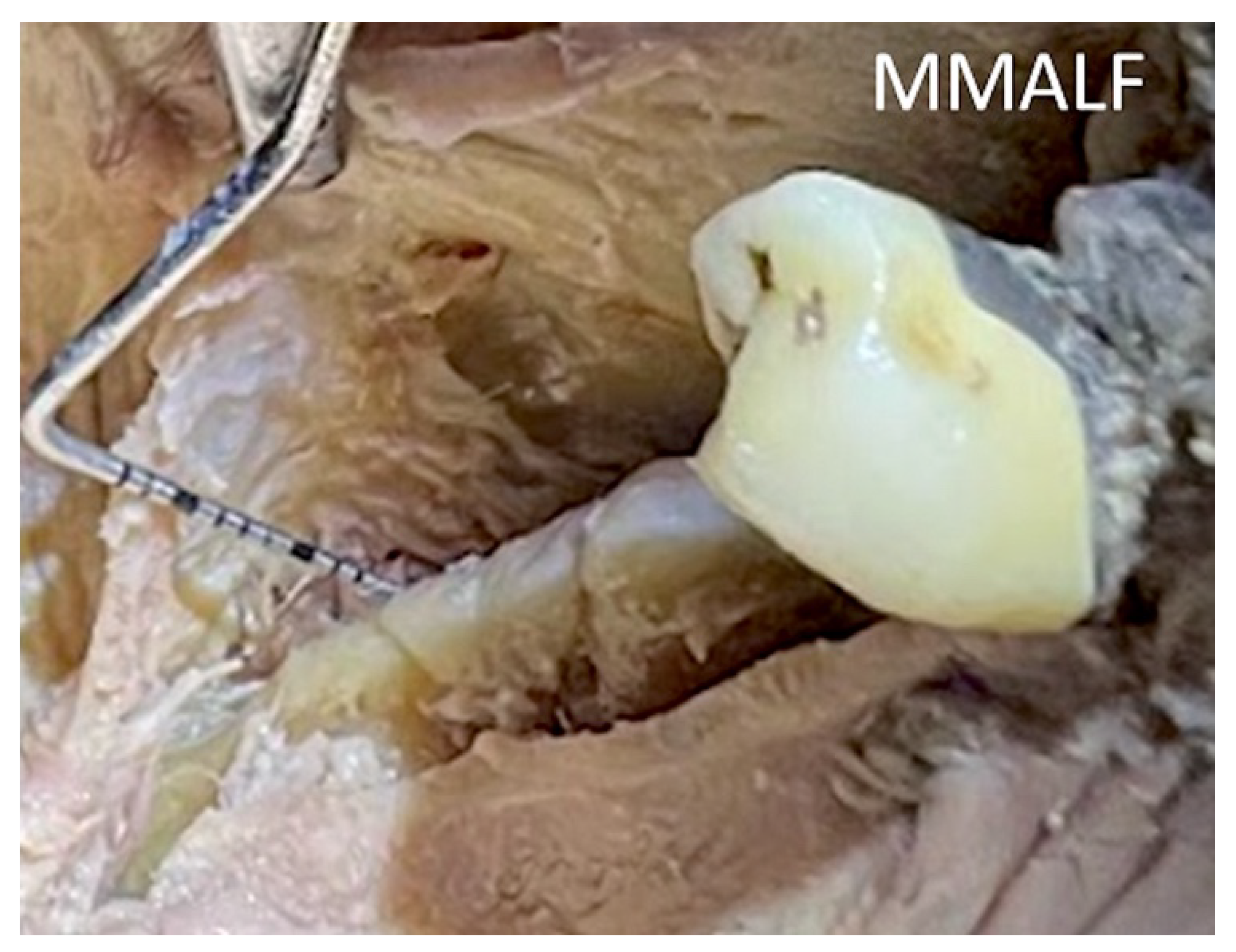
2.2. Release of the Mylohyoid Muscle Attachment on the Lingual Flap (MMALF) [15,28]
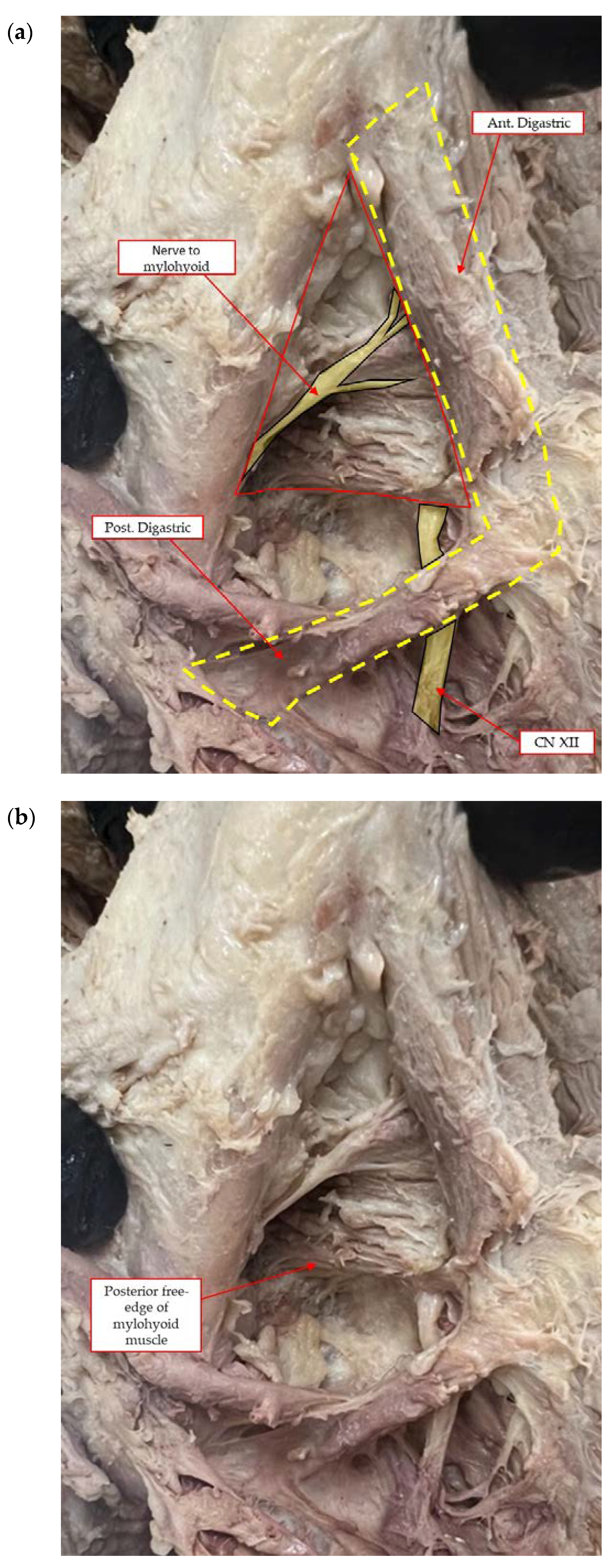
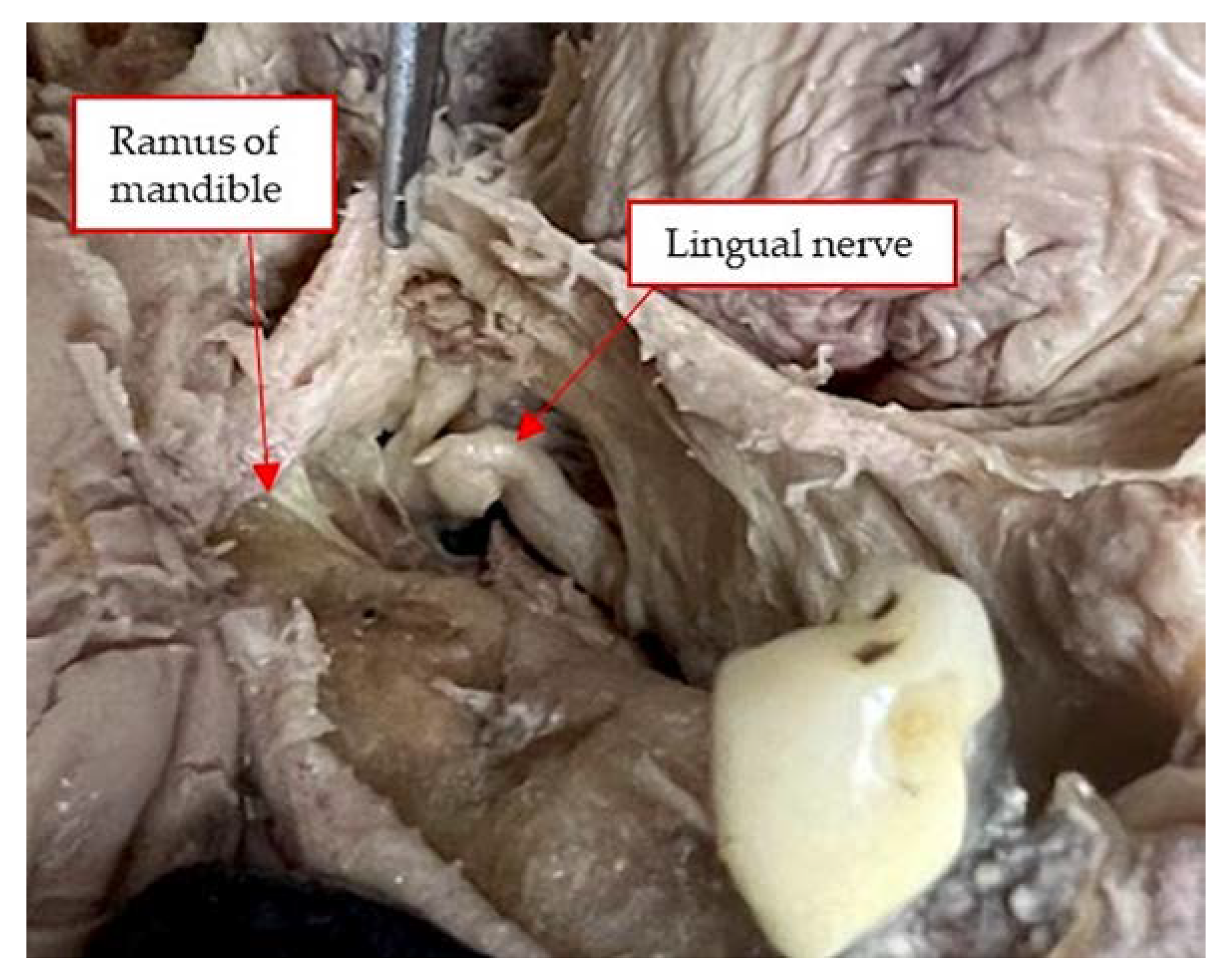
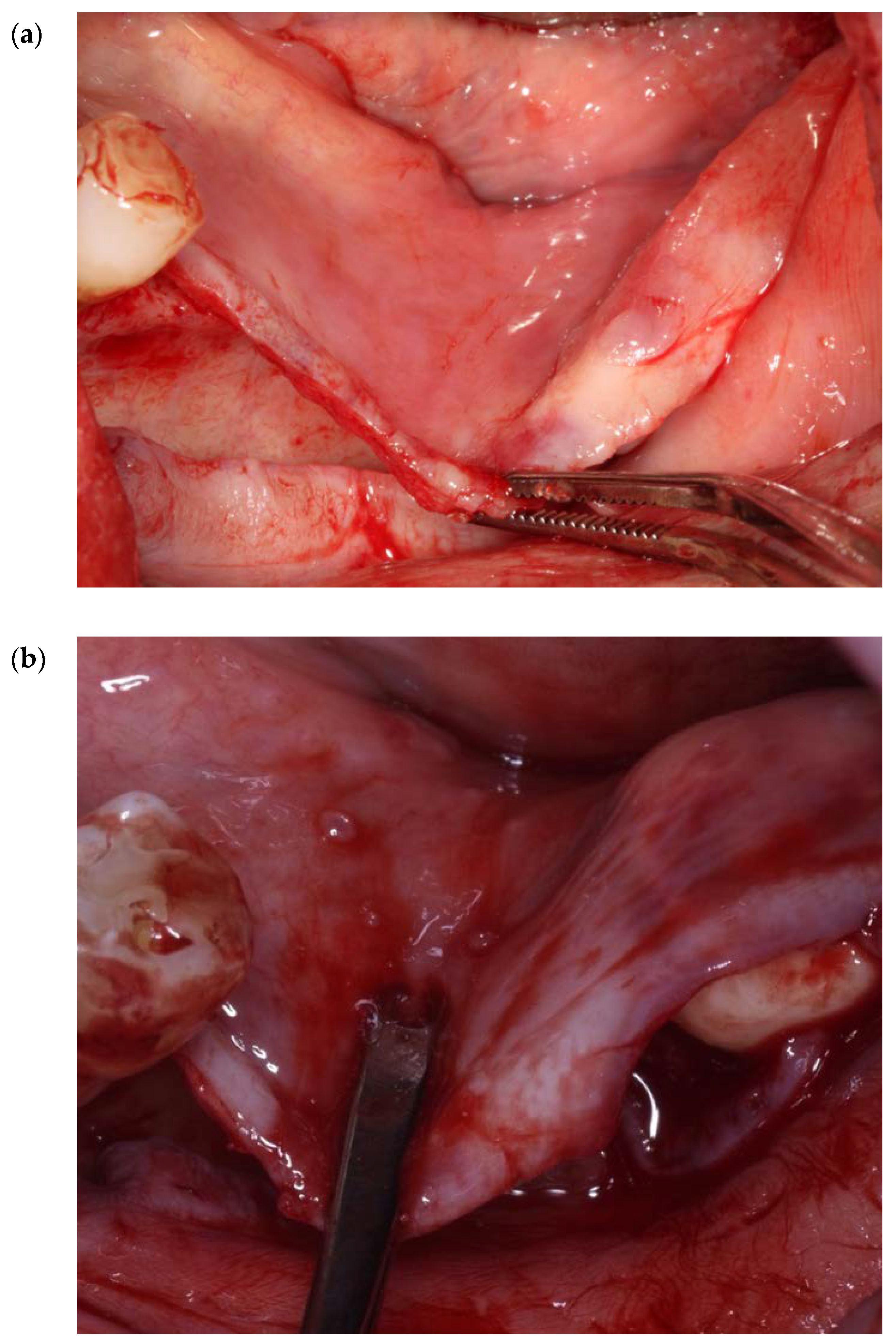
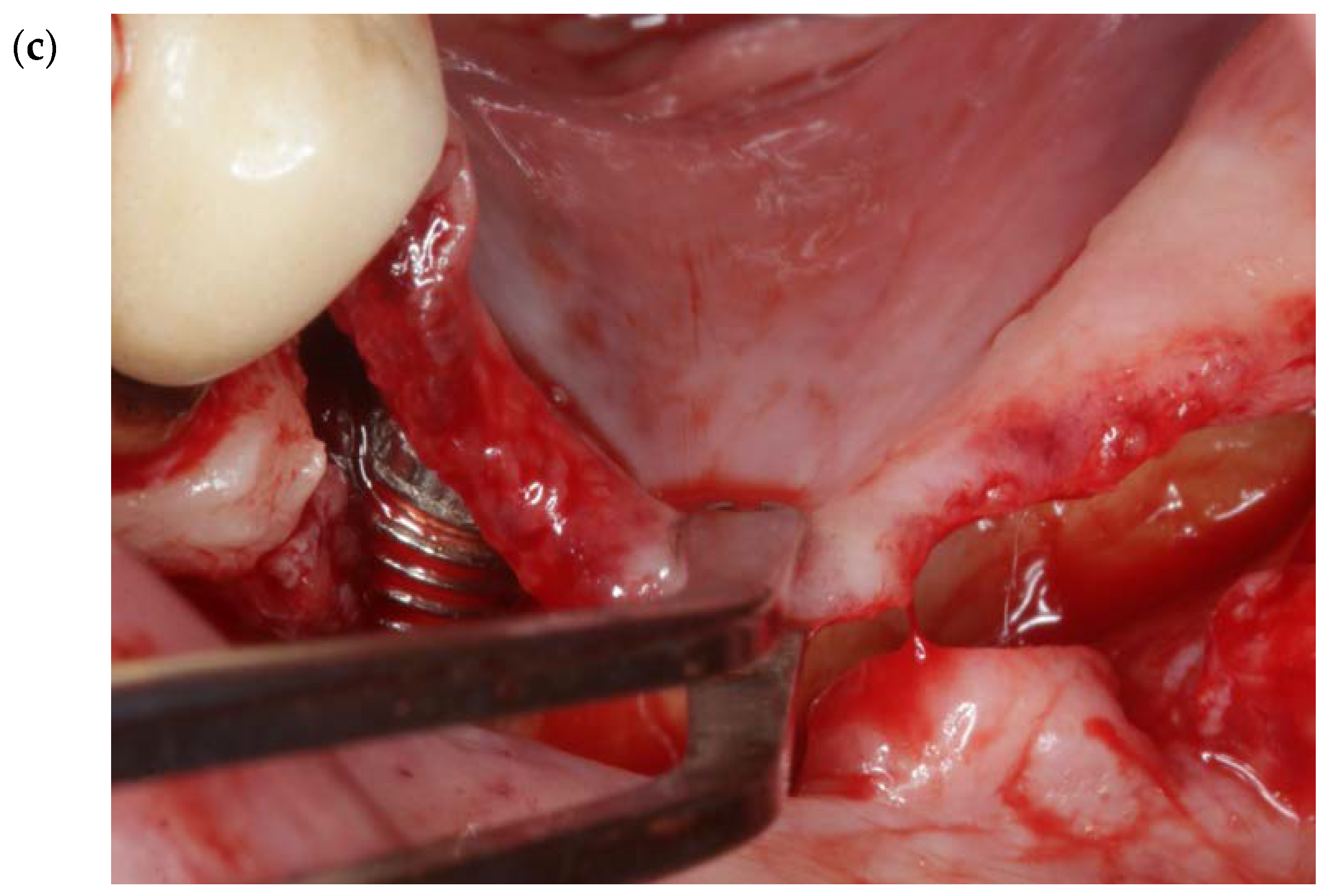
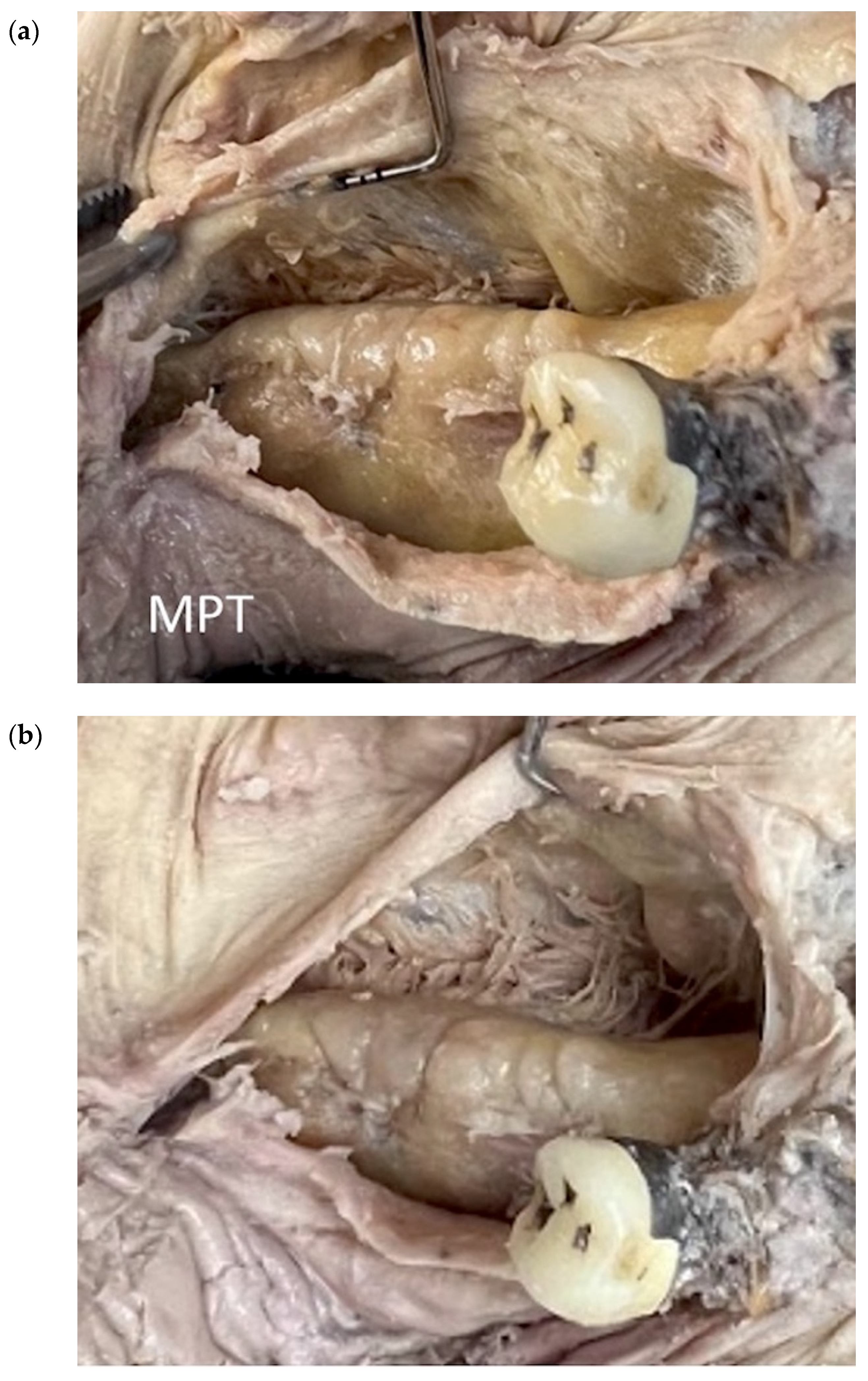
2.3. Mylohyoid Preservation Technique (MPT) in Three Key Anatomical Zones [6,13,14]
3. Cadaver Analyses of the Techniques
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Seibert, J.S. Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. Part I. Technique and wound healing. Compend Contin Educ. Dent 1983, 4, 437–453. [Google Scholar] [PubMed]
- Wang, H.L.; Al-Shammari, K. HVC ridge deficiency classification: A therapeutically oriented classification. Int. J. Periodontics Restor. Dent 2002, 22, 335–343. [Google Scholar]
- Urban, I.; Monje, A.; Lozada, J.; Wang, H.L. Vertical ridge augmentation and soft tissue reconstruction of the anterior atrophic maxillae: A case series. Int. J. Periodontics Restor. Dent 2015, 35, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Schropp, L.; Wenzel, A.; Kostopoulos, L.; Karring, T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int. J. Periodontics Restor. Dent 2003, 23, 313–323. [Google Scholar]
- Dahlin, C.; Linde, A.; Gottlow, J.; Nyman, S. Healing of bone defects by guided tissue regeneration. Plast. Reconstr. Surg. 1988, 81, 672–676. [Google Scholar] [CrossRef]
- Urban, I.; Monje, A.; Lozada, J.; Wang, H.-L. Principles for vertical ridge augmentation in the atrophic posterior mandible: A technical review. Int. J. Periodontics Restor. Dent 2017, 37, 639–645. [Google Scholar] [CrossRef]
- Simion, M.; Jovanovic, S.A.; Trisi, P.; Scarano, A.; Piattelli, A. Vertical ridge augmentation around dental implants using a membrane technique and autogenous bone or allografts in humans. Int. J. Periodontics Restor. Dent 1998, 18, 8–23. [Google Scholar]
- Simion, M.; Jovanovic, S.A.; Tinti, C.; Benfenati, S. Long term evaluation of osseointegrated implants inserted at the time or after vertical ridge augmentation. A retrospective study on 123 implants with 1-5-year follow-up. Clin. Oral Implants Res. 2001, 12, 35–45. [Google Scholar] [CrossRef]
- Soldatos, N.; Nelson-Rabe, L.; Ferguson, B.; Soldatos, K.; Weltman, R. Vertical ridge augmentation (VRA) with the use of cross-linked resorbable membrane, tenting screws, and a combination grafting technique: A report of three cases. Quintessence Int. 2021, 52, 328–339. [Google Scholar]
- Soldatos, N.K.; Stylianou, P.; Koidou, V.P.; Angelov, N.; Yukna, R.; Romanos, G.E. Limitations and options using resorbable versus resorbable membranes for successful guided bone regeneration procedures. Quintessence Int. 2017, 48, 131–147. [Google Scholar]
- Soldatos, N.; Garcia, M.; Umoh, E.; Irizarry, A.; Weltman, R. Vertical ridge augmentation around dental implants with the use of a dense PTFE membrane to correct previously failed augmentations. Clin. Adv. Periodontics 2022, 12, 51–56. [Google Scholar] [CrossRef]
- Jepsen, S.; Schwarz, F.; Cordaro, L.; Derks, J.; Hämmerle, C.H.; Heitz-Mayfield, L.J.; Hernández Alfaro, F.; Meijer, H.J.; Naenni, N.; Ortiz-Vigón, A.; et al. Regeneration of alveolar ridge defects. Consensus report of group 4 of the 15th European Workshop on Periodontology on Bone Regeneration. J. Clin. Periodontol 2019, 46, 277–286. [Google Scholar] [CrossRef]
- Urban, I.; Traxler, H.; Romero-Bustillos, M.; Farkasdi, S.; Bartee, B.; Baksa, G.; Avila-Ortiz, G. Effectiveness of two different lingual flap advancing techniques for vertical bone augmentation in the posterior mandible: A comparative, split-mouth cadaver study. Int. J. Periodontics Restor. Dent 2018, 38, 35–40. [Google Scholar] [CrossRef]
- Urban, I.; Monje, A.; Wang, H.-L.; Gerber, G. Mandibular regional anatomical landmarks, and clinical implications for ridge augmentation. Int. J. Periodontics Restor. Dent 2017, 37, 347–353. [Google Scholar] [CrossRef]
- Ronda, M.; Stacchi, C. Management of coronally advanced lingual flap in regenerative osseous surgery: A case series introducing a novel technique. Int. J. Periodontics Restor. Dent 2011, 31, 505–513. [Google Scholar]
- Machtei, E.E. The effect of membrane exposure on the outcome of regenerative procedures in humans: A meta-analysis. J. Periodontol. 2001, 72, 512–516. [Google Scholar] [CrossRef]
- Retzepi, M.; Donos, N. Guided Bone Regeneration: Biological principle and therapeutic applications. Clin. Oral Imp. Res. 2010, 21, 567–576. [Google Scholar] [CrossRef]
- Wang, H.L.; Boyapati, L. "PASS" principles for predictable bone regeneration. Implant Dent 2006, 15, 8–17. [Google Scholar] [CrossRef]
- Romanos, G.E. Periosteal releasing incision for successful coverage of augmented sites. A technical note. J. Oral Implantol. 2010, 36, 25–30. [Google Scholar] [CrossRef]
- Bunyaratavej, P.; Wang, H.L. Collagen membranes: A review. J. Periodontol. 2001, 72, 215–229. [Google Scholar] [CrossRef]
- Chasioti, E.; Tat Fai, C.; Drew, H. Maintaining space in localized ridge augmentation using guided bone regeneration with tenting screw technology. Quintessence Int. 2013, 44, 763–771. [Google Scholar] [PubMed]
- Pikos, M.A. Atrophic posterior maxilla, and mandible: Alveolar ridge reconstruction with mandibular block autografts. Alpha Omegan 2005, 98, 34–45. [Google Scholar] [PubMed]
- Simion, M.; Fontana, F.; Rasperini, G.; Maiorana, C. Vertical ridge augmentation by expanded-polytetrafluoroethylene membrane and a combination of intraoral autogenous bone graft and deproteinized anorganic bovine bone. Clin. Oral Implant. Res. 2007, 18, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Greenstein, G.; Greenstein, B.; Cavallaro, J.; Tarnow, D. The role of decortication in enhancing the results of guided bone regeneration: A literature review. J. Periodontol. 2009, 80, 175–189. [Google Scholar] [CrossRef] [PubMed]
- Burkhardt, R.; Lang, N.P. Role of flap tension in primary wound closure of mucoperiosteal flaps: A prospective cohort study. Clin. Oral Imp. Res. 2010, 21, 50–54. [Google Scholar] [CrossRef]
- Herring, M.J.; Fehrenbach, S.W. Illustrated Anatomy of the Head and Neck, 4th ed.; Elsevier/Saunders: St. Louis, MO, USA, 2013. [Google Scholar]
- Pikos, M.A. Atrophic posterior mandibular reconstruction utilizing mandibular block autografts: Risk management. Int. J. Oral Maxillofac. Implant. 2003, 18, 765–766. [Google Scholar]
- Ronda, M.; Rebaudi, A.; Torelli, L.; Stacchi, C. Expanded vs. dense polytetrafluoroethylene membranes in vertical ridge augmentation around dental implants: A prospective randomized controlled clinical trial. Clin. Oral Implant. Res. 2014, 25, 859–866. [Google Scholar] [CrossRef]
- Simion, M.; Trisi, P.; Piattelli, A. Vertical ridge augmentation using a membrane technique associated with osseointegrated implants. Int. J. Periodontics Restor. Dent 1994, 14, 496–511. [Google Scholar]
- Urban, I.A.; Lozada, J.L.; Jovanovic, S.A.; Nagursky, H.; Nagy, K. Vertical ridge augmentation with titanium- reinforced dense PTFE membranes and a combination of particulated autogenous bone and anorganic bovine bone-derived mineral: A prospective case series in 19 patients. Int. J. Oral Maxillofac. Implant. 2014, 29, 185–193. [Google Scholar] [CrossRef]
- Niamtu, J., 3rd. Near-fatal airway obstruction after routine implant placement. Oral Surg Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 92, 597–600. [Google Scholar] [CrossRef]
- Tinti, C.; Parma-Benfenati, S.; Polizzi, G. Vertical ridge augmentation: What is the limit? Int. J. Periodontics Restor. Dent 1996, 16, 221–229. [Google Scholar]
- Tinti, C.; Parma-Benfenati, S. Vertical ridge augmentation: Surgical protocol and retrospective evaluation of 48 consecutively inserted implants. Int. J. Periodontics Restor. Dent 1998, 18, 435–443. [Google Scholar]
- Fugazzotto, P. Maintaining primary closure after guided bone regeneration procedures: Introduction of a new flap design and preliminary results. J. Periodontol. 2006, 77, 1452–1457. [Google Scholar] [CrossRef]
- Merli, M.; Lombardini, F.; Esposito, M. Vertical ridge augmentation with autogenous bone grafts 3 years after loading: Resorbable barriers versus titanium-reinforced barriers. A randomized controlled clinical trial. Int. J. Oral Maxillofac. Implant. 2010, 25, 801–807. [Google Scholar]
- Fugazzotto, P. Maintenance of soft tissue closure following guided bone regeneration: Technical considerations and report of 723 Cases. J. Periodontol. 1999, 70, 1085–1097. [Google Scholar] [CrossRef]
- Soldatos, N.; Weltman, R. Vertical ridge augmentation (VRA): Success and predictability. Curr. Oral Health Rep. 2022, 9, 197–204. [Google Scholar] [CrossRef]
- Stanley, R. Mandibular lingual releasing approach to oral and oropharyngeal carcinomas. Laryngoscope 1984, 94, 596–600. [Google Scholar] [CrossRef]
- Li, H.; Li, J.; Yang, B.; Su, M.; Xing, R.; Han, Z. Mandibular lingual release versus mandibular lip-split approach for expanded resection of middle-late tongue cancer: A case-control study. J. Cranio-Maxillo-Facial Surg. 2015, 43, 1054–1058. [Google Scholar] [CrossRef]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Techniques | Methods | Limitations |
|---|---|---|
| FST (Pikos 2005 [22], Romanos 2010 [19]) | Blunt dissection/separation of the superficial from the deep mylohyoid muscle fibers without any sharp dissection with the use of the index finger. | Creation of communication between the surgical site and the submandibular or sublingual space. |
| MMALF (Ronda et al. 2011 [15]) | A blunt instrument is inserted under the mylohyoid muscular insertion at the lingual flap. With a gentle traction in a coronal direction, the connective tissue band is detached. | Overthinning of the lingual flap, which may lead to flap necrosis and exposure of the graft in the early healing period. |
| MPT (Urban et al. 2018 [13]) | 1. Tunneling and lifting of the retromolar pad (zone I). 2. Flap separation with mylohyoid muscle preservation (zone II). 3. Anterior, semi blunt periosteal release (zone III) with the use of a 15c blade in a perpendicular angle. | More complex and technique sensitive approach, especially in zone III; the use of a 15c blade over the mesial aspect of the lingual flap endangers a possible flap perforation. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soldatos, N.; Immonen, J.; Romanos, G.; Weltman, R. The Significance of Mylohyoid Muscle Release (MMR) in the Vertical and Horizontal Ridge Augmentation Surgeries; Clinical and Human Cadaver Analyses of the Techniques. Genes 2023, 14, 595. https://doi.org/10.3390/genes14030595
Soldatos N, Immonen J, Romanos G, Weltman R. The Significance of Mylohyoid Muscle Release (MMR) in the Vertical and Horizontal Ridge Augmentation Surgeries; Clinical and Human Cadaver Analyses of the Techniques. Genes. 2023; 14(3):595. https://doi.org/10.3390/genes14030595
Chicago/Turabian StyleSoldatos, Nikolaos, Jessica Immonen, Georgios Romanos, and Robin Weltman. 2023. "The Significance of Mylohyoid Muscle Release (MMR) in the Vertical and Horizontal Ridge Augmentation Surgeries; Clinical and Human Cadaver Analyses of the Techniques" Genes 14, no. 3: 595. https://doi.org/10.3390/genes14030595
APA StyleSoldatos, N., Immonen, J., Romanos, G., & Weltman, R. (2023). The Significance of Mylohyoid Muscle Release (MMR) in the Vertical and Horizontal Ridge Augmentation Surgeries; Clinical and Human Cadaver Analyses of the Techniques. Genes, 14(3), 595. https://doi.org/10.3390/genes14030595