
Sleep Quality and Duration in Children That Consume Caffeine: Impact of Dose and Genetic Variation in ADORA2A and CYP1A

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measures
2.2.1. Caffeine Intake
2.2.2. Sleep Quality and Duration
2.3. Genotyping, Imputation, and Quality Control Procedures
2.4. Candidate Gene and Variant Selection
2.5. Statistical Analysis
3. Results
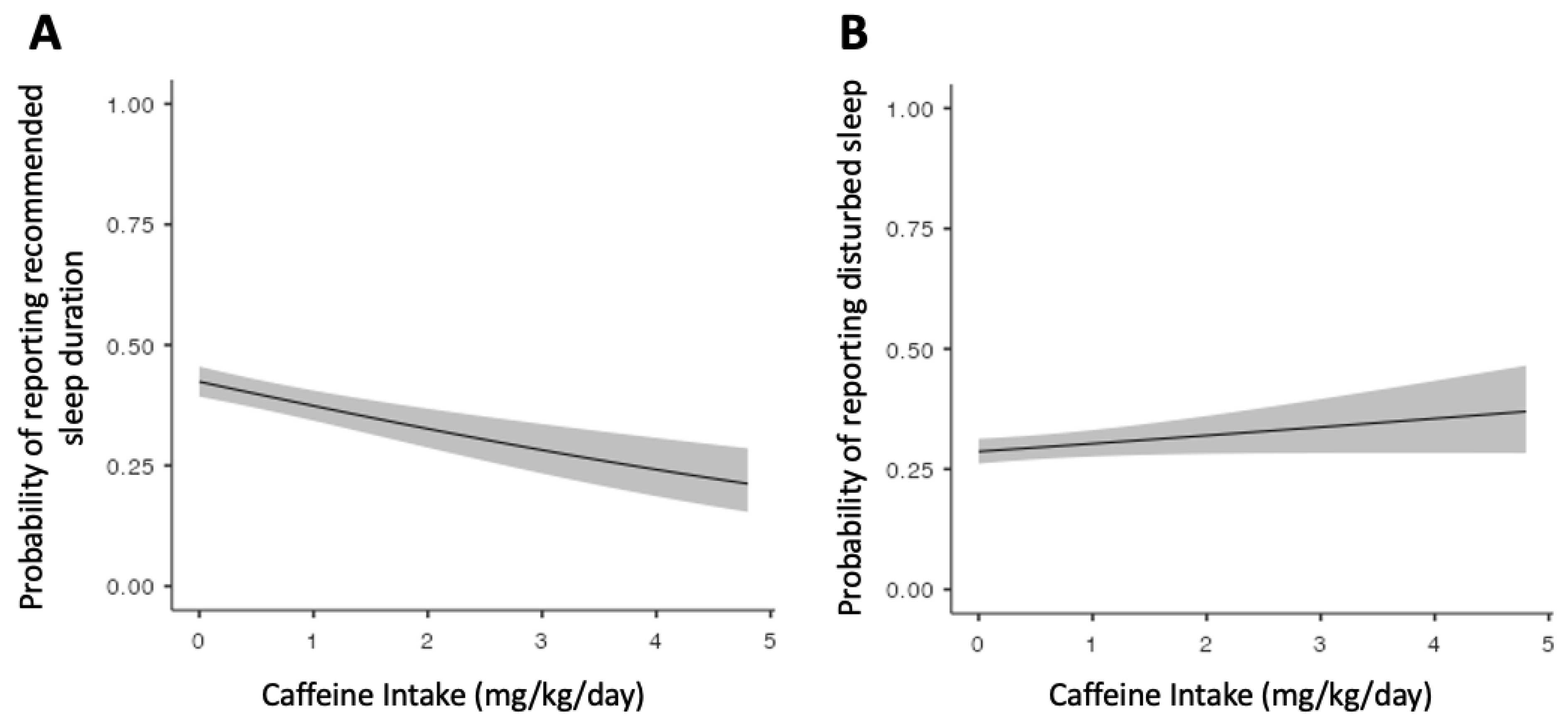
3.1. Effect of Caffeine on Sleep Quality and Duration
3.2. Effect of CYP1A and ADORA2A Genotypes on Caffeine Intake
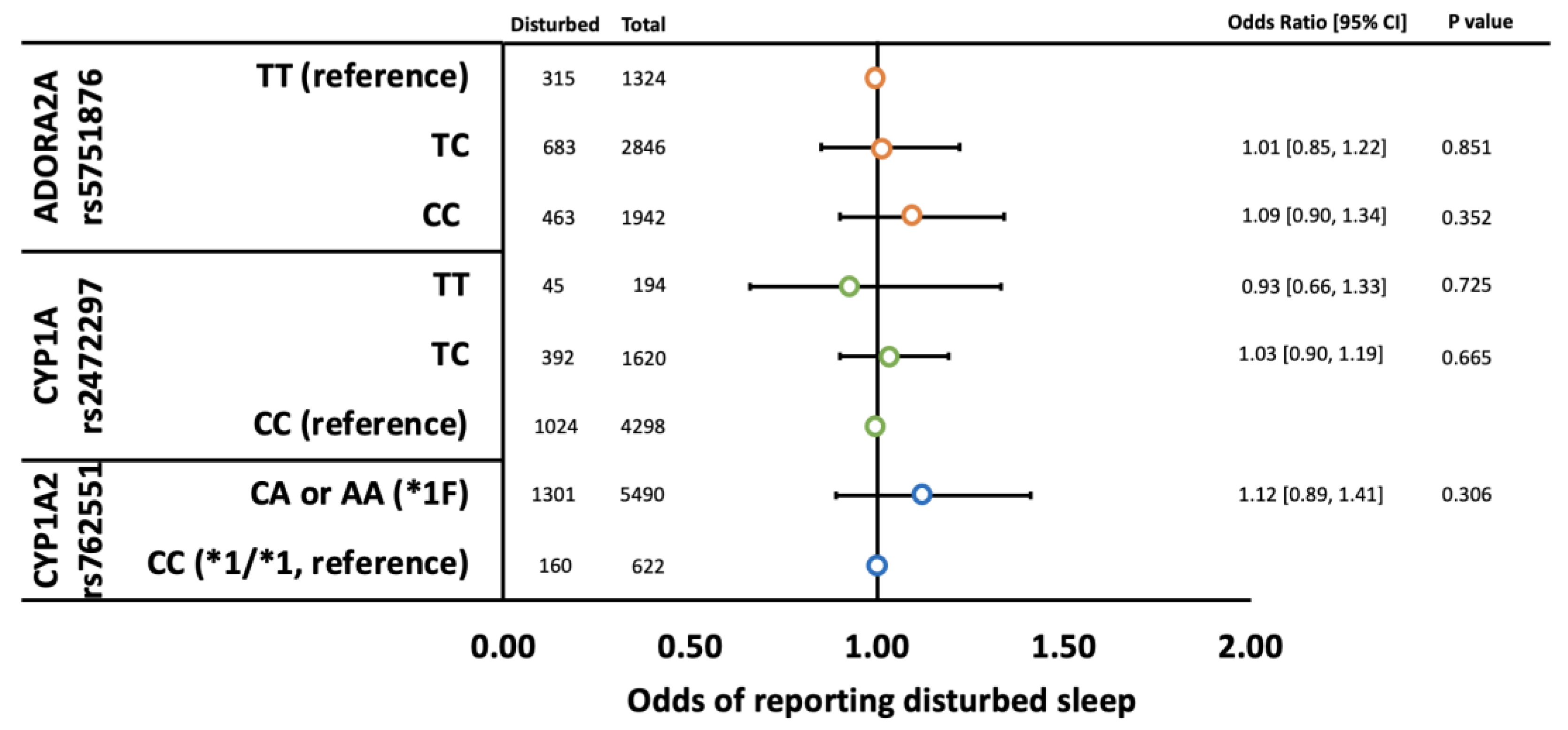
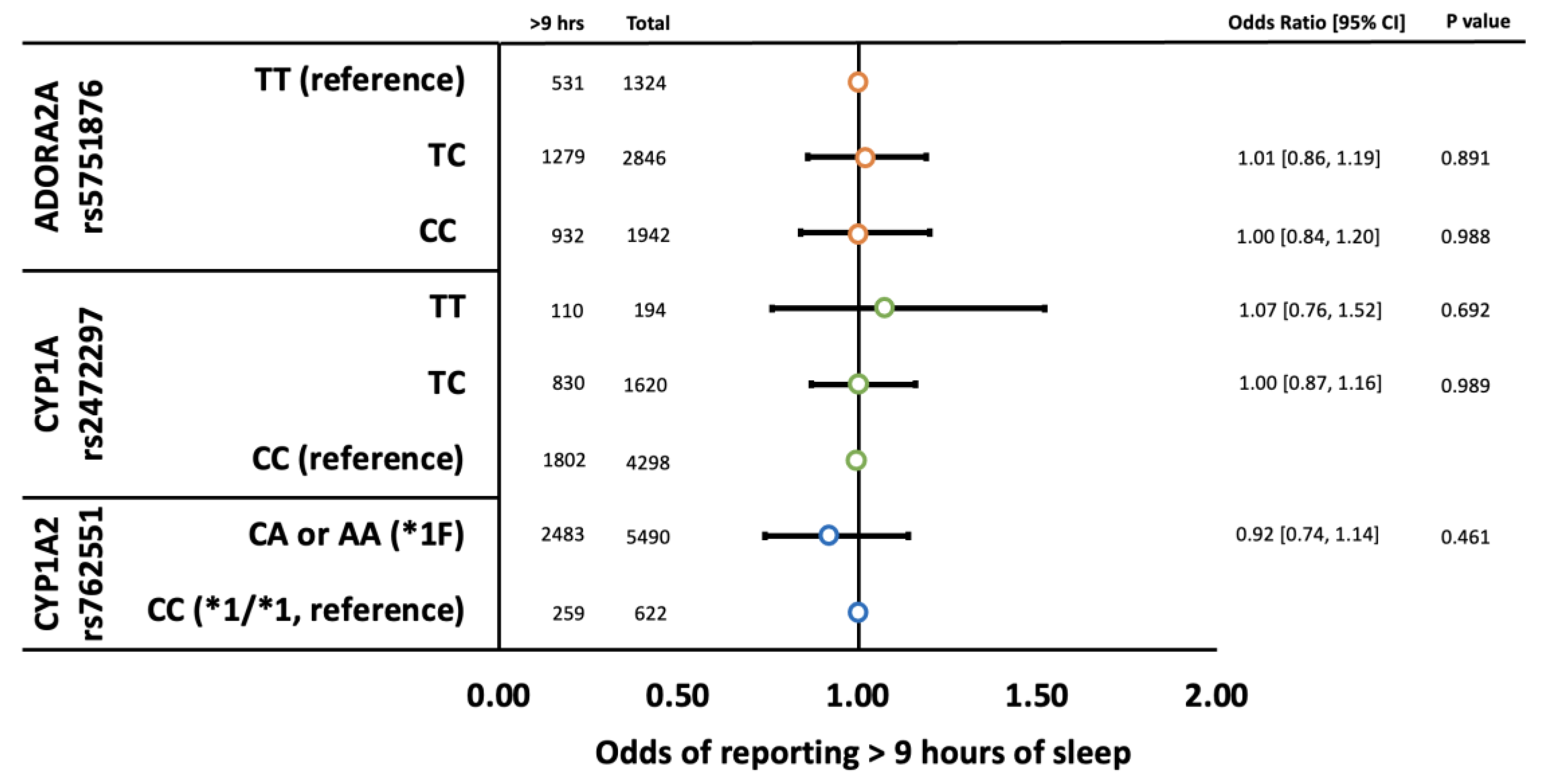
3.3. Effect of CYP1A and ADORA2A Genotypes on Sleep Quality and Duration
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Temple, J.L. Review: Trends, Safety, and Recommendations for Caffeine Use in Children and Adolescents. J. Am. Acad. Child Adolesc. Psychiatry 2018, 58, 36–45. [Google Scholar] [CrossRef] [PubMed]
- Lodato, F.; Araújo, J.; Barros, H.; Lopes, C.; Agodi, A.; Barchitta, M.; Ramos, E. Caffeine intake reduces sleep duration in adolescents. Nutr. Res. 2013, 33, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Owens, J.A.; Mindell, J.; Baylor, A. Effect of energy drink and caffeinated beverage consumption on sleep, mood, and performance in children and adolescents. Nutr. Rev. 2014, 72, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Temple, J.L. Caffeine use in children: What we know, what we have left to learn, and why we should worry. Neurosci. Biobehav. Rev. 2009, 33, 793–806. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Child and Adolescent Psychiatry. Caffeine and Children. No. 131. 2020. Available online: https://www.aacap.org/AACAP/Families_and_Youth/Facts_for_Families/FFF-Guide/Caffeine_and_Children-131.aspx#:~:text=At%20this%20time%2C%20pediatricians%20advise,those%2012%2D18%20years%20old (accessed on 1 September 2022).
- Health Canada. Caffeine in Foods. 2022. Available online: https://www.canada.ca/en/health-canada/services/food-nutrition/food-safety/food-additives/caffeine-foods.html (accessed on 1 September 2022).
- European Food Safety Authority (EFSA). Outcome of a Public Consultation on the Draft Scientific Opinion of the EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA) on the Safety of Caffeine; EFSA: Parma, Italy, 2015; Volume 12, pp. 1–101. [Google Scholar]
- Nehlig, A. Interindividual Differences in Caffeine Metabolism and Factors Driving Caffeine Consumption. Pharmacol. Rev. 2018, 70, 384–411. [Google Scholar] [CrossRef] [PubMed]
- Thorn, C.F.; Aklillu, E.; McDonagh, E.M.; Klein, T.E.; Altman, R.B. PharmGKB summary: Caffeine pathway. Pharmacogenet. Genom. 2012, 22, 389–395. [Google Scholar] [CrossRef]
- Byrne, E.M.; Johnson, J.; McRae, A.F.; Nyholt, D.R.; Medland, S.E.; Gehrman, P.R.; Heath, A.C.; Madden, P.A.; Montgomery, G.W.; Chenevix-Trench, G.; et al. A Genome-Wide Association Study of Caffeine-Related Sleep Disturbance: Confirmation of a Role for a Common Variant in the Adenosine Receptor. Sleep 2012, 35, 967–975. [Google Scholar] [CrossRef]
- Cornelis, M.C.; Kacprowski, T.; Menni, C.; Gustafsson, S.; Pivin, E.; Adamski, J.; Artati, A.; Eap, C.B.; Ehret, G.; Friedrich, N.; et al. Genome-wide association study of caffeine metabolites provides new insights to caffeine metabolism and dietary caffeine-consumption behavior. Hum. Mol. Genet. 2016, 25, 5472–5482. [Google Scholar] [CrossRef]
- Nunes, R.A.; Mazzotti, D.R.; Hirotsu, C.; Andersen, M.L.; Tufik, S.; Bittencourt, L. The association between caffeine consumption and objective sleep variables is dependent on ADORA2A c.1083T>C genotypes. Sleep Med. 2017, 30, 210–215. [Google Scholar] [CrossRef]
- Rétey, J.V.; Adam, M.; Khatami, R.; Luhmann, U.F.O.; Jung, H.H.; Berger, W.; Landolt, H.-P. A genetic variation in the adenosine A2A receptor gene (ADORA2A) contributes to individual sensitivity to caffeine effects on sleep. Clin. Pharmacol. Ther. 2007, 81, 692–698. [Google Scholar] [CrossRef]
- Bodenmann, S.; Hohoff, C.; Freitag, C.; Deckert, J.; Rétey, J.V.; Bachmann, V.; Landolt, H.-P. Polymorphisms of ADORA2A modulate psychomotor vigilance and the effects of caffeine on neurobehavioural performance and sleep EEG after sleep deprivation. Br. J. Pharmacol. 2012, 165, 1904–1913. [Google Scholar] [CrossRef]
- Baur, D.M.; Lange, D.; Elmenhorst, E.-M.; Elmenhorst, D.; Bauer, A.; Aeschbach, D.; Landolt, H.-P. Coffee effectively attenuates impaired attention in ADORA2A C/C-allele carriers during chronic sleep restriction. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 109, 110232. [Google Scholar] [CrossRef]
- Erblang, M.; Drogou, C.; Gomez-Merino, D.; Metlaine, A.; Boland, A.; Deleuze, J.F.; Thomas, C.; Sauvet, F.; Chennaoui, M. The Impact of Genetic Variations in ADORA2A in the Association between Caffeine Consumption and Sleep. Genes 2019, 10, 1021. [Google Scholar] [CrossRef]
- Shin, S.-Y.; The Multiple Tissue Human Expression Resource (MuTHER) Consortium; Fauman, E.B.; Petersen, A.-K.; Krumsiek, J.; Santos, R.; Huang, J.; Arnold, M.; Erte, I.; Forgetta, V.; et al. An atlas of genetic influences on human blood metabolites. Nat. Genet. 2014, 46, 543–550. [Google Scholar] [CrossRef]
- Sulem, P.; Gudbjartsson, D.; Geller, F.; Prokopenko, I.; Feenstra, B.; Aben, K.K.; Franke, B.; Heijer, M.D.; Kovacs, P.; Stumvoll, M.; et al. Sequence variants at CYP1A1–CYP1A2 and AHR associate with coffee consumption. Hum. Mol. Genet. 2011, 20, 2071–2077. [Google Scholar] [CrossRef]
- The Coffee and Caffeine Genetics Consortium; Cornelis, M.C.; Byrne, E.M.; Esko, T.; Nalls, M.A.; Ganna, A.; Paynter, N.; Monda, K.L.; Amin, N.; Fischer, K.; et al. Genome-wide meta-analysis identifies six novel loci associated with habitual coffee consumption. Mol. Psychiatry 2014, 20, 647–656. [Google Scholar] [CrossRef]
- Koonrungsesomboon, N.; Khatsri, R.; Wongchompoo, P.; Teekachunhatean, S. The impact of genetic polymorphisms on CYP1A2 activity in humans: A systematic review and meta-analysis. Pharm. J. 2017, 18, 760–768. [Google Scholar] [CrossRef]
- Karcher, N.R.; Barch, D.M. The ABCD study: Understanding the development of risk for mental and physical health outcomes. Neuropsychopharmacology 2020, 46, 131–142. [Google Scholar] [CrossRef]
- Achenbach, T. The Child Behavior Checklist and related instruments. In The Use of Psychological Testing for Treatment Planning and Outcomes Assessment; Maruish, M.E., Ed.; Lawrence Erlbaum Associates Publishers: Hillsdale, NJ, USA, 1999; pp. 429–466. [Google Scholar]
- Wajszilber, D.; Santisteban, J.A.; Gruber, R. Sleep disorders in patients with ADHD: Impact and management challenges. Nat. Sci. Sleep 2018, 10, 453–480. [Google Scholar] [CrossRef]
- Marmorstein, N.R. Energy Drink and Coffee Consumption and Psychopathology Symptoms Among Early Adolescents: Cross-Sectional and Longitudinal Associations. J. Caffeine Res. 2016, 6, 64–72. [Google Scholar] [CrossRef]
- Vanderlee, L.; Reid, J.L.; White, C.M.; Acton, R.B.; Kirkpatrick, S.I.; Pao, C.-I.; Rybak, M.E.; Hammond, D. Evaluation of a 24-Hour Caffeine Intake Assessment Compared with Urinary Biomarkers of Caffeine Intake among Young Adults in Canada. J. Acad. Nutr. Diet. 2018, 118, 2245–2253.e1. [Google Scholar] [CrossRef]
- Bruni, O.; Ottaviano, S.; Guidetti, V.; Romoli, M.; Innocenzi, M.; Cortesi, F.; Giannotti, F. The Sleep Disturbance Scale for Children (SDSC). Construction and validation of an instrument to evaluate sleep disturbances in childhood and adolescence. J. Sleep Res. 1996, 5, 251–261. [Google Scholar] [CrossRef]
- Paruthi, S.; Brooks, L.J.; D’Ambrosio, C.; Hall, W.A.; Kotagal, S.; Lloyd, R.M.; Malow, B.A.; Maski, K.; Nichols, C.; Quan, S.F. Recommended Amount of Sleep for Pediatric Populations: A Consensus Statement of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2016, 12, 785–786. [Google Scholar] [CrossRef]
- Baurley, J.W.; Edlund, C.K.; Pardamean, C.I.; Conti, D.V.; Bergen, A.W. Smokescreen: A targeted genotyping array for addiction research. BMC Genom. 2016, 17, 145. [Google Scholar] [CrossRef]
- Uban, K.A.; Horton, M.K.; Jacobus, J.; Heyser, C.; Thompson, W.K.; Tapert, S.F.; Madden, P.A.; Sowell, E.R. Biospecimens and the ABCD study: Rationale, methods of collection, measurement and early data. Dev. Cogn. Neurosci. 2018, 32, 97–106. [Google Scholar] [CrossRef]
- Price, A.L.; Patterson, N.J.; Plenge, R.M.; Weinblatt, M.E.; Shadick, N.A.; Reich, D. Principal components analysis corrects for stratification in genome-wide association studies. Nat. Genet. 2006, 38, 904–909. [Google Scholar] [CrossRef]
- Jamovi. The Jamovi Project. 2019. Available online: https://www.jamovi.org (accessed on 11 May 2021).
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- World Health Organization. Weight-for-Age (5–10 Years). Available online: https://www.who.int/tools/growth-reference-data-for-5to19-years/indicators/weight-for-age-5to10-years (accessed on 1 September 2022).
- Flockhart, D. Drug Interactions: Cytochrome P450 Drug Interaction Table 2007. Available online: https://drug-interactions.medicine.iu.edu (accessed on 11 May 2021).
- Fairley, S.; Lowy-Gallego, E.; Perry, E.; Flicek, P. The International Genome Sample Resource (IGSR) collection of open human genomic variation resources. Nucleic Acids Res. 2019, 48, D941–D947. [Google Scholar] [CrossRef]
- Frary, C.D.; Johnson, R.K.; Wang, M.Q. Food sources and intakes of caffeine in the diets of persons in the United States. J. Am. Diet. Assoc. 2005, 105, 110–113. [Google Scholar] [CrossRef]
- Chaudhary, N.S.; Grandner, M.; Jackson, N.J.; Chakravorty, S. Caffeine consumption, insomnia, and sleep duration: Results from a nationally representative sample. Nutrition 2016, 32, 1193–1199. [Google Scholar] [CrossRef]
- Zhang, H.; Lee, Z.X.; Qiu, A. Caffeine intake and cognitive functions in children. Psychopharmacology 2020, 237, 3109–3116. [Google Scholar] [CrossRef]
- Upreti, V.V.; Wahlstrom, J.L. Meta-analysis of hepatic cytochrome P450 ontogeny to underwrite the prediction of pediatric pharmacokinetics using physiologically based pharmacokinetic modeling. J. Clin. Pharmacol. 2015, 56, 266–283. [Google Scholar] [CrossRef]
- Salem, F.; Johnson, T.N.; Abduljalil, K.; Tucker, G.T.; Rostami-Hodjegan, A. A Re-evaluation and Validation of Ontogeny Functions for Cytochrome P450 1A2 and 3A4 Based on In Vivo Data. Clin. Pharmacokinet. 2014, 53, 625–636. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | |
|---|---|
| Gender, % (N) girl | 45.8 (2801) |
| Ancestry, % (N) | |
| European | 62.7 (3835) |
| African | 14.9 (914) |
| East Asian | 0.9 (60) |
| American | 0.8 (52) |
| Admixed | 13.2 (810) |
| Not available | 7.2 (441) |
| Ethnicity (self-reported), % N | |
| White | 48.2 (2948) |
| Black | 14.7 (897) |
| Asian | 1.4 (83) |
| Hispanic | 19.1 (1168) |
| Other | 9.4 (574) |
| Not available | 7.2 (442) |
| Weight, mean (sd) kg | 38.3 (11.1) |
| Concomitant psychotropic use, % (N) | |
| SSRI 1 | 0.8 (47) |
| Antipsychotic 2 | 0.3 (17) |
| Stimulant 3 | 4.9 (298) |
| Caffeine use, mean (sd) mg/kg/day | 0.58 (0.008) |
| Sleep Duration, % (N) | |
| 9–11 h | 44.9 (2742) |
| 8–9 h | 38.4 (2349) |
| 7–8 h | 13.4 (816) |
| 5–7 h | 3.2 (193) |
| <5 h | 0.2 (12) |
| SDSC total score, mean (sd) | 35.8 (0.09) |
| SDSC sleep quality, % (N) disturbed | 23.9 (1461) |
| Caffeine Threshold (mg/kg/day) | Detection of Children Reporting < 9 h of Sleep Per Night | ||
|---|---|---|---|
| Sensitivity | Specificity | Youden J-Index * | |
| 0.01 | 0.99 | 0.01 | 0.00 |
| 0.05 | 0.79 | 0.30 | 0.09 |
| 0.10 | 0.66 | 0.45 | 0.11 |
| 0.25 | 0.41 | 0.68 | 0.09 |
| 0.50 | 0.26 | 0.82 | 0.08 |
| 1.00 | 0.14 | 0.91 | 0.05 |
| 1.50 | 0.08 | 0.95 | 0.02 |
| 2.00 | 0.05 | 0.97 | 0.01 |
| 2.50 a | 0.03 | 0.98 | 0.01 |
| 3.00 b | 0.02 | 0.99 | 0.01 |
| 1000 Genomes Project | ||||||||
|---|---|---|---|---|---|---|---|---|
| SNP | Genotype | Current Study (n = 6112) | ALL (n = 2504) | AFR (n = 661) | AMR (n = 347) | EAS (n = 504) | EUR (n = 503) | SAS (n = 489) |
| rs2472297 | C/C | 70.3 | 88.0 | 97.1 | 83.0 | 100.0 | 62.0 | 93.5 |
| (CYP1A) | C/T | 26.5 | 10.9 | 2.9 | 16.1 | 0.0 | 33.0 | 6.5 |
| T/T | 3.2 | 1.1 | 0.0 | 0.9 | 0.0 | 5.0 | 0.0 | |
| rs762551 | C/C | 10.2 | 15.2 | 19.8 | 7.5 | 10.9 | 11.5 | 22.7 |
| (CYP1A2) | C/A or A/A | 89.8 | 84.8 | 80.2 | 92.5 | 89.1 | 88.5 | 77.3 |
| rs5751876 | C/C | 31.8 | 20.7 | 9.4 | 28.0 | 22.8 | 37.4 | 11.7 |
| (ADORA2A) | C/T | 46.6 | 47.0 | 44.9 | 52.4 | 48.8 | 47.1 | 44.0 |
| T/T | 21.7 | 32.3 | 45.7 | 19.6 | 28.4 | 15.5 | 44.4 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jessel, C.D.; Narang, A.; Zuberi, R.; Bousman, C.A. Sleep Quality and Duration in Children That Consume Caffeine: Impact of Dose and Genetic Variation in ADORA2A and CYP1A. Genes 2023, 14, 289. https://doi.org/10.3390/genes14020289
Jessel CD, Narang A, Zuberi R, Bousman CA. Sleep Quality and Duration in Children That Consume Caffeine: Impact of Dose and Genetic Variation in ADORA2A and CYP1A. Genes. 2023; 14(2):289. https://doi.org/10.3390/genes14020289
Chicago/Turabian StyleJessel, Chaten D., Ankita Narang, Rayyan Zuberi, and Chad A. Bousman. 2023. "Sleep Quality and Duration in Children That Consume Caffeine: Impact of Dose and Genetic Variation in ADORA2A and CYP1A" Genes 14, no. 2: 289. https://doi.org/10.3390/genes14020289
APA StyleJessel, C. D., Narang, A., Zuberi, R., & Bousman, C. A. (2023). Sleep Quality and Duration in Children That Consume Caffeine: Impact of Dose and Genetic Variation in ADORA2A and CYP1A. Genes, 14(2), 289. https://doi.org/10.3390/genes14020289