
Soft Tissue and Bone Tumor Diagnostics: Harnessing the Power of Molecular Techniques

 , , and
, , and
Abstract
:1. Introduction
2. Molecular Testing for Diagnosis
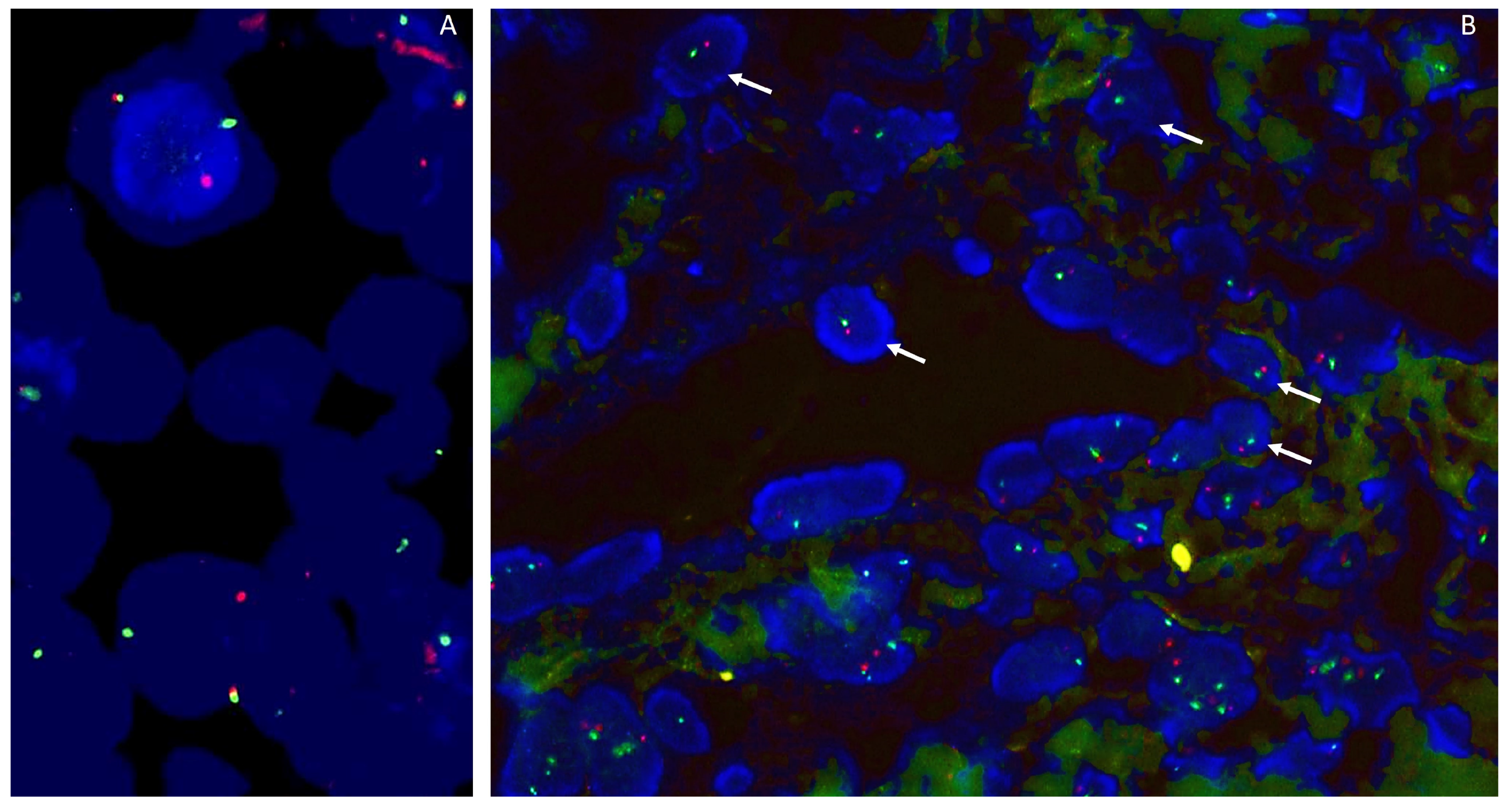
2.1. Fluorescence In Situ Hybridization
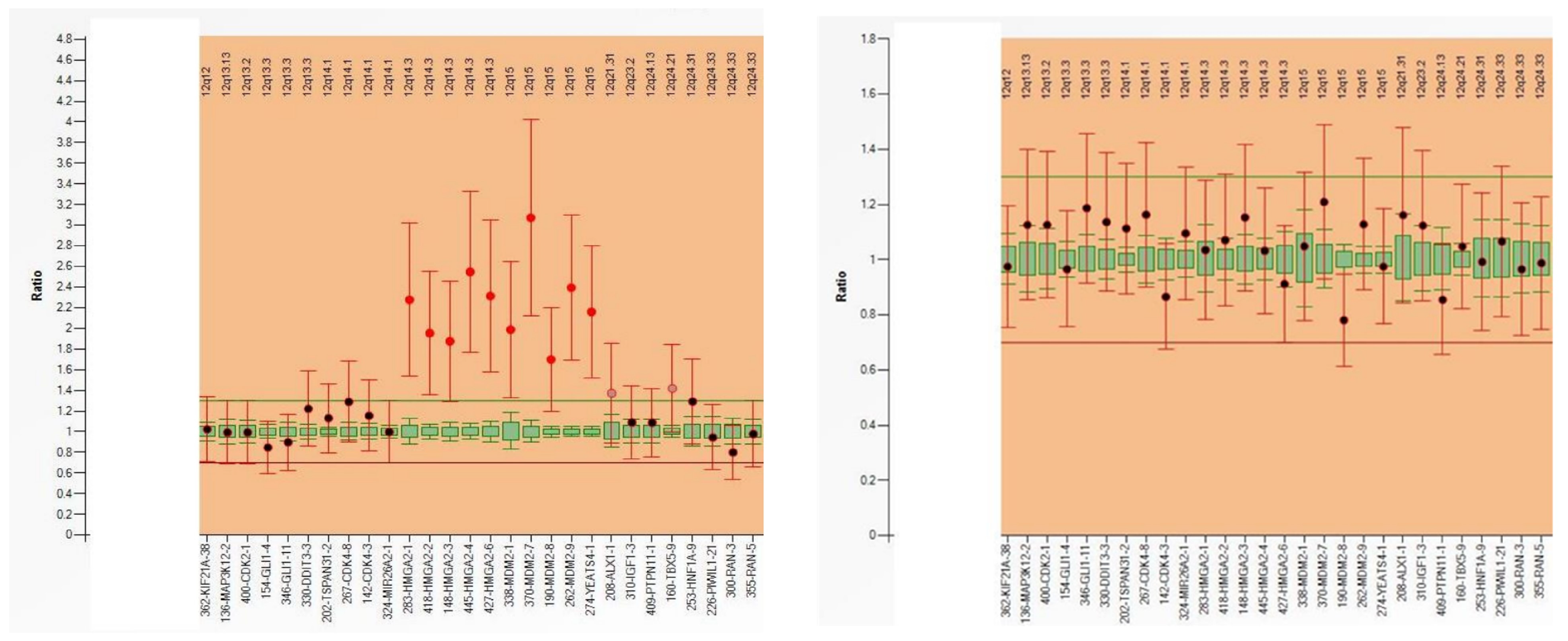
2.2. Reverse Transcriptase Polymerase Chain Reaction (RT-PCR), Digital PCR (dPCR) and Multiplex Ligation-Dependent Probe Amplification (MLPA)
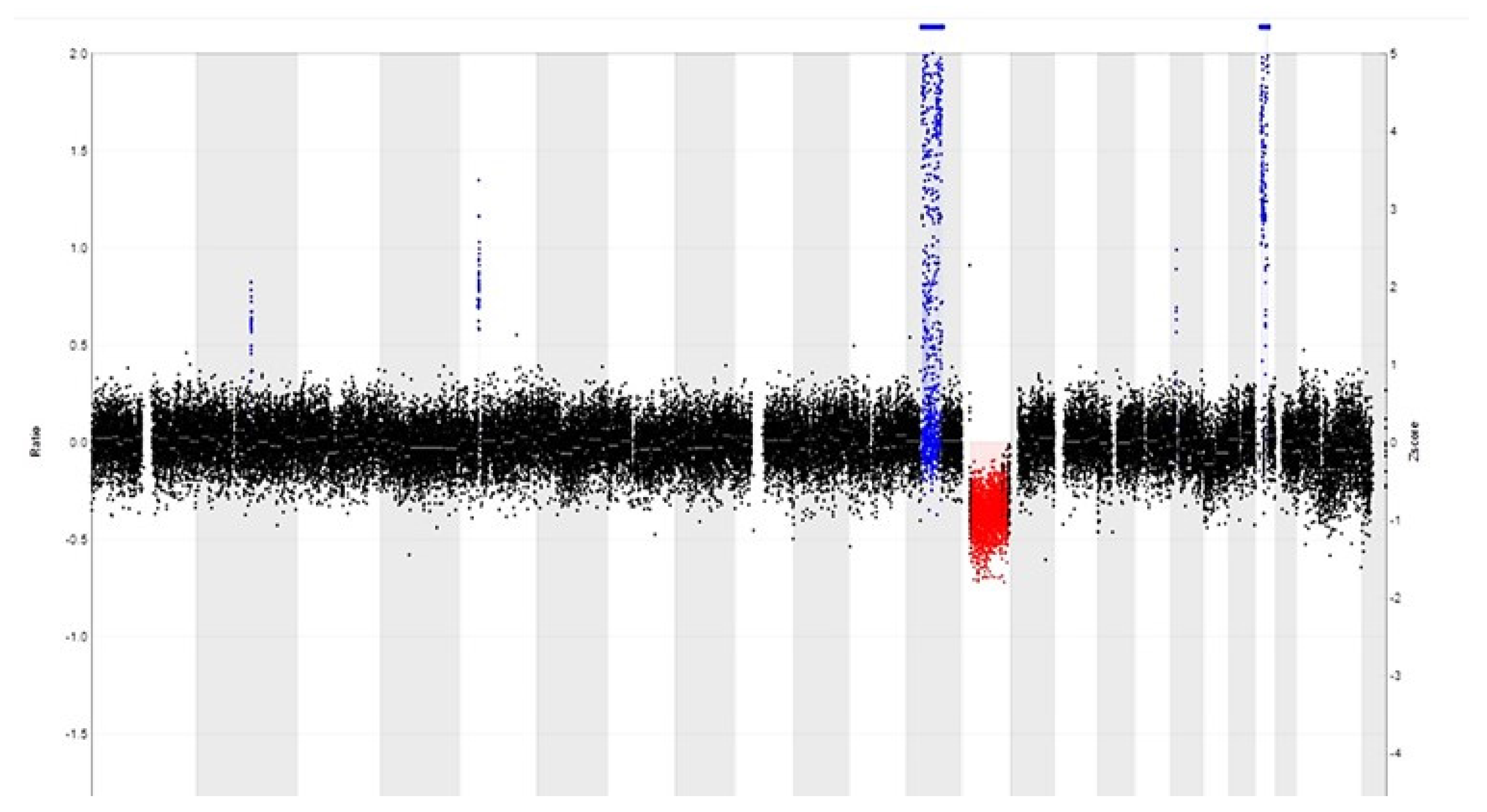
2.3. Copy Number Variation Sequencing (CNV Sequencing)
2.4. DNA- and RNA-Based Next-Generation Sequencing (DNA/RNA-Based NGS)
2.5. DNA Methylation Profiling
2.6. Nanopore Sequencing
2.7. Liquid Biopsy
2.8. New Evolving Techniques
3. Molecular Testing for Therapeutic Decision Making
4. Clinical Applications of Molecular Testing in Soft Tissue and Bone Tumor Pathology
4.1. Case 1
4.2. Case 2
4.3. Case 3
4.4. Case 4
4.5. Case 5
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Antonescu, C.R. The role of genetic testing in soft tissue sarcoma. Histopathology 2006, 48, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Anderson, W.J.; Jo, V.Y. Diagnostic Immunohistochemistry of Soft Tissue and Bone Tumors: An Update on Biomarkers That Correlate with Molecular Alterations. Diagnostics 2021, 11, 690. [Google Scholar] [CrossRef] [PubMed]
- WHO. Classification of Central Nervous Tumors Tumors, 5th ed.; International Agency for Research on Cancer: Lyon, France, 2021. [Google Scholar]
- Bridge, J.A.; Sandberg, A.A. Cytogenetic and molecular genetic techniques as adjunctive approaches in the diagnosis of bone and soft tissue tumors. Skelet. Radiol. 2000, 29, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Creytens, D.; Van Gorp, J.; Speel, E.J.; Ferdinande, L. Characterization of the 12q amplicons in lipomatous soft tissue tumors by multiplex ligation-dependent probe amplification-based copy number analysis. Anticancer. Res. 2015, 35, 1835–1842. [Google Scholar] [PubMed]
- Chebib, I.; Taylor, M.S.; Nardi, V.; Rivera, M.N.; Lennerz, J.K.; Cote, G.M.; Choy, E.; Calderón, S.A.L.; Raskin, K.A.; Schwab, J.H.; et al. Clinical Utility of Anchored Multiplex Solid Fusion Assay for Diagnosis of Bone and Soft Tissue Tumors. Am. J. Surg. Pathol. 2021, 45, 1127–1137. [Google Scholar] [CrossRef] [PubMed]
- Nazir, S. Medical diagnostic value of digital PCR (dPCR): A systematic review. Biomed. Eng. Adv. 2023, 6, 100092. [Google Scholar] [CrossRef]
- Mao, X.; Liu, C.; Tong, H.; Chen, Y.; Liu, K. Principles of digital PCR and its applications in current obstetrical and gynecological diseases. Am. J. Transl. Res. 2019, 11, 7209–7222. [Google Scholar]
- Creytens, D.; van Gorp, J.; Ferdinande, L.; Speel, E.J.; Libbrecht, L. Detection of MDM2/CDK4 amplification in lipomatous soft tissue tumors from formalin-fixed, paraffin-embedded tissue: Comparison of multiplex ligation-dependent probe amplification (MLPA) and fluorescence in situ hybridization (FISH). Appl. Immunohistochem. Mol. Morphol. AIMM 2015, 23, 126–133. [Google Scholar] [CrossRef]
- Hömig-Hölzel, C.; Savola, S. Multiplex Ligation-dependent Probe Amplification (MLPA) in Tumor Diagnostics and Prognostics. Diagn. Mol. Pathol. Am. J. Surg. Pathol. Part B 2012, 21, 189–206. [Google Scholar] [CrossRef]
- Stuppia, L.; Antonucci, I.; Palka, G.; Gatta, V. Use of the MLPA Assay in the Molecular Diagnosis of Gene Copy Number Alterations in Human Genetic Diseases. Int. J. Mol. Sci. 2012, 13, 3245–3276. [Google Scholar] [CrossRef]
- Van der Linden, M.; Raman, L.; Trappen, A.V.; Dheedene, A.; De Smet, M.; Sante, T.; Creytens, D.; Lievens, Y.; Menten, B.; Van Dorpe, J.; et al. Detection of Copy Number Alterations by Shallow Whole-Genome Sequencing of Formalin-Fixed, Paraffin-Embedded Tumor Tissue. Arch. Pathol. Lab. Med. 2019, 144, 974–981. [Google Scholar] [CrossRef] [PubMed]
- Scheinin, I.; Sie, D.; Bengtsson, H.; van de Wiel, M.A.; Olshen, A.B.; van Thuijl, H.F.; van Essen, H.F.; Eijk, P.P.; Rustenburg, F.; Meijer, G.A.; et al. DNA copy number analysis of fresh and formalin-fixed specimens by shallow whole-genome sequencing with identification and exclusion of problematic regions in the genome assembly. Genome Res. 2014, 24, 2022–2032. [Google Scholar] [CrossRef] [PubMed]
- Creytens, D.; Folpe, A.L.; Koelsche, C.; Mentzel, T.; Ferdinande, L.; van Gorp, J.M.; Van der Linden, M.; Raman, L.; Menten, B.; Fritchie, K.; et al. Myxoid pleomorphic liposarcoma-a clinicopathologic, immunohistochemical, molecular genetic and epigenetic study of 12 cases, suggesting a possible relationship with conventional pleomorphic liposarcoma. Mod. Pathol. 2021, 34, 2043–2049. [Google Scholar] [CrossRef] [PubMed]
- Zare, F.; Dow, M.; Monteleone, N.; Hosny, A.; Nabavi, S. An evaluation of copy number variation detection tools for cancer using whole exome sequencing data. BMC Bioinform. 2017, 18, 286. [Google Scholar] [CrossRef] [PubMed]
- Zhu, G.; Benayed, R.; Ho, C.; Mullaney, K.; Sukhadia, P.; Rios, K.; Berry, R.; Rubin, B.P.; Nafa, K.; Wang, L.; et al. Diagnosis of known sarcoma fusions and novel fusion partners by targeted RNA sequencing with identification of a recurrent ACTB-FOSB fusion in pseudomyogenic hemangioendothelioma. Mod. Pathol. 2019, 32, 609–620. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, J.; Heyn, H.; Moran, S.; Serra-Musach, J.; Pujana, M.A.; Bibikova, M.; Esteller, M. Validation of a DNA methylation microarray for 450,000 CpG sites in the human genome. Epigenetics 2011, 6, 692–702. [Google Scholar] [CrossRef]
- Moran, S.; Arribas, C.; Esteller, M. Validation of a DNA methylation microarray for 850,000 CpG sites of the human genome enriched in enhancer sequences. Epigenomics 2016, 8, 389–399. [Google Scholar] [CrossRef]
- Capper, D.; Jones, D.T.W.; Sill, M.; Hovestadt, V.; Schrimpf, D.; Sturm, D.; Koelsche, C.; Sahm, F.; Chavez, L.; Reuss, D.E.; et al. DNA methylation-based classification of central nervous system tumours. Nature 2018, 555, 469–474. [Google Scholar] [CrossRef]
- Koelsche, C.; Schrimpf, D.; Stichel, D.; Sill, M.; Sahm, F.; Reuss, D.E.; Blattner, M.; Worst, B.; Heilig, C.E.; Beck, K.; et al. Sarcoma classification by DNA methylation profiling. Nat. Commun. 2021, 12, 498. [Google Scholar] [CrossRef]
- Liu, M.C.; Oxnard, G.R.; Klein, E.A.; Swanton, C.; Seiden, M.V.; CCGA Consortium. Sensitive and specific multi-cancer detection and localization using methylation signatures in cell-free DNA. Ann. Oncol. 2020, 31, 745–759. [Google Scholar] [CrossRef]
- Iluz, A.; Maoz, M.; Lavi, N.; Charbit, H.; Or, O.; Olshinka, N.; Demma, J.A.; Adileh, M.; Wygoda, M.; Blumenfeld, P.; et al. Rapid Classification of Sarcomas Using Methylation Fingerprint: A Pilot Study. Cancers 2023, 15, 4168. [Google Scholar] [CrossRef] [PubMed]
- Miettinen, M.; Abdullaev, Z.; Turakulov, R.; Quezado, M.; Contreras, A.L.; Curcio, C.A.; Rys, J.; Chlopek, M.; Lasota, J.; Aldape, K.D. Assessment of the Utility of the Sarcoma DNA Methylation Classifier in Surgical Pathology. Am. J. Surg. Pathol. 2023. Online ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Kuschel, L.P.; Hench, J.; Frank, S.; Hench, I.B.; Girard, E.; Blanluet, M.; Masliah-Planchon, J.; Misch, M.; Onken, J.; Czabanka, M.; et al. Robust methylation-based classification of brain tumours using nanopore sequencing. Neuropathol. Appl. Neurobiol. 2023, 49, e12856. [Google Scholar] [CrossRef] [PubMed]
- MPG, C.V.; Kester, L.; Kranendonk, M.; Wesseling, P.; Verburg, N.; de Witt Hamer, P.; Kooi, E.; Dankmeijer, L.; van der Lugt, J.; van Baarsen, K.; et al. Ultra-fast deep-learned CNS tumor classification during surgery. Neuro-Oncology 2023, 25, ii104. [Google Scholar]
- Hadjimichael, A.C.; Pergaris, A.; Kaspiris, A.; Foukas, A.F.; Theocharis, S.E. Liquid Biopsy: A New Translational Diagnostic and Monitoring Tool for Musculoskeletal Tumors. Int. J. Mol. Sci. 2021, 22, 11526. [Google Scholar] [CrossRef] [PubMed]
- van der Laan, P.; van Houdt, W.J.; van den Broek, D.; Steeghs, N.; van der Graaf, W.T.A. Liquid Biopsies in Sarcoma Clinical Practice: Where Do We Stand? Biomedicines 2021, 9, 1315. [Google Scholar] [CrossRef] [PubMed]
- Heinhuis, K.M.; In’t Veld, S.; Dwarshuis, G.; van den Broek, D.; Sol, N.; Best, M.G.; van Coevorden, F.; Haas, R.L.; Beijnen, J.H.; van Houdt, W.J.; et al. RNA-Sequencing of Tumor-Educated Platelets, a Novel Biomarker for Blood-Based Sarcoma Diagnostics. Cancers 2020, 12, 1372. [Google Scholar] [CrossRef]
- Peneder, P.; Stütz, A.M.; Surdez, D.; Krumbholz, M.; Semper, S.; Chicard, M.; Sheffield, N.C.; Pierron, G.; Lapouble, E.; Tötzl, M.; et al. Multimodal analysis of cell-free DNA whole-genome sequencing for pediatric cancers with low mutational burden. Nat. Commun. 2021, 12, 3230. [Google Scholar] [CrossRef]
- Wolff, A.C.; Hammond, M.E.H.; Hicks, D.G.; Dowsett, M.; McShane, L.M.; Allison, K.H.; Allred, D.C.; Bartlett, J.M.S.; Bilous, M.; Fitzgibbons, P.; et al. Recommendations for Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline Update. J. Clin. Oncol. 2013, 31, 3997–4013. [Google Scholar] [CrossRef]
- Hayes, D.F. Considerations for Implementation of Cancer Molecular Diagnostics into Clinical Care. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, 292–296. [Google Scholar] [CrossRef]
- Graham, R.P.; Yasir, S.; Fritchie, K.J.; Reid, M.D.; Greipp, P.T.; Folpe, A.L. Polypoid fibroadipose tumors of the esophagus: ‘Giant fibrovascular polyp’ or liposarcoma? A clinicopathological and molecular cytogenetic study of 13 cases. Mod. Pathol. 2018, 31, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Brooks, P.J.; Chadwick, J.W.; Caminiti, M.; Dickson, B.; Leong, I. Primary aneurysmal bone cyst of the mandibular condyle with USP6-CDH11 fusion. Pathol. Res. Pract. 2019, 215, 607–610. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.M.; Perez-Atayde, A.R.; Inwards, C.Y.; Medeiros, F.; Derr, V.; Hsi, B.-L.; Gebhardt, M.C.; Rosenberg, A.E.; Fletcher, J.A. USP6 and CDH11 Oncogenes Identify the Neoplastic Cell in Primary Aneurysmal Bone Cysts and Are Absent in So-Called Secondary Aneurysmal Bone Cysts. Am. J. Pathol. 2004, 165, 1773–1780. [Google Scholar] [CrossRef] [PubMed]
- Lopes, M. Osteosarcoma of the bone. In WHO Classification of Head and Neck Tumors, 5th ed.; IARC Press: Lyon, France, 2022. [Google Scholar]
- Ibstedt, S.; de Mattos, C.B.R.; Köster, J.; Mertens, F. A cryptic EWSR1::DDIT3 fusion in myxoid liposarcoma: Potential pitfalls with FISH and cytogenetics. Genes Chromosom. Cancer 2023, 62, 167–170. [Google Scholar] [CrossRef] [PubMed]
- Scapa, J.V.; Cloutier, J.M.; Raghavan, S.S.; Peters-Schulze, G.B.; Varma, S.B.; Charville, G.W. DDIT3 Immunohistochemistry Is a Useful Tool for the Diagnosis of Myxoid Liposarcoma. Am. J. Surg. Pathol. 2021, 45, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Amary, M.F.; Bacsi, K.; Maggiani, F.; Damato, S.; Halai, D.; Berisha, F.; Pollock, R.; O’Donnell, P.; Grigoriadis, A.; Diss, T.; et al. IDH1 and IDH2 mutations are frequent events in central chondrosarcoma and central and periosteal chondromas but not in other mesenchymal tumours. J. Pathol. 2011, 224, 334–343. [Google Scholar] [CrossRef]
- Nord, K.H.; Lilljebjörn, H.; Vezzi, F.; Nilsson, J.; Magnusson, L.; Tayebwa, J.; de Jong, D.; Bovée, J.V.M.G.; Hogendoorn, P.C.W.; Szuhai, K. GRM1 is upregulated through gene fusion and promoter swapping in chondromyxoid fibroma. Nat. Genet. 2014, 46, 474–477. [Google Scholar] [CrossRef]
- Hrzenjak, A. JAZF1/SUZ12 gene fusion in endometrial stromal sarcomas. Orphanet J. Rare Dis. 2016, 11, 15. [Google Scholar] [CrossRef]
- Le Page, C.; Almadani, N.; Turashvili, G.; Bataillon, G.; Portelance, L.; Provencher, D.; Anne-Marie, M.-M.; Blake, G.; Lien, H.; Kurosh, R. SATB2 Expression in Uterine Sarcoma: A Multicenter Retrospective Study. Int. J. Gynecol. Pathol. 2021, 40, 487–494. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Technique | Advantages | Disadvantages |
|---|---|---|
| FISH | - Specific visualization of genetic abnormalities at the chromosomal level - High sensitivity for detecting gene rearrangements, deletions and amplification - Applicable to interphase nuclei in fixed tissues. | - Limited to the targeted regions - Subject to observer variability in interpretation |
| RT-PCR, digital-PCR and MLPA | - High sensitivity and specificity - Digital PCR offers absolute quantification - MLPA allows for multiplex analysis | - RT-PCR is limited to targeted regions - RT-PCR may be affected by amplification biases - Digital PCR may have limited throughput - MLPA is semi-quantitative and may miss novel rearrangements |
| CNV sequencing | - Genome-wide detection of CNVs - High resolution for identifying small variations - Improved sensitivity compared to array-based methods | - Higher cost than targeted approaches - Requires extensive computational analysis - Interpretation complexity due to ploidy, heterogeneity and purity - Limited ability to detect balanced chromosomal rearrangements |
| DNA- and RNA-based NGS | - Comprehensive profiling of genetic alterations - Simultaneous analysis of multiple genes - Detection of novel and known mutations | - High cost and complexity - Bioinformatics challenges in data analysis - Limited ability to detect structural variations |
| DNA methylation profiling | - Epigenetic information for gene expression regulation - Identification of methylation patterns associated with specific soft tissue tumors | - Technical challenges and restricted range of methylation classes - Interpretation complexity due to tissue heterogeneity |
| Nanopore sequencing | - Long-read sequencing for improved structural variant detection - Real-time sequencing without the need for extensive library preparation - Single-molecule sequencing | - Higher error rates compared to short-read technologies - Restricted range of methylation classes - Fresh tissue samples |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cordier, F.; Ferdinande, L.; Hoorens, A.; Van de Vijver, K.; Van Dorpe, J.; Creytens, D. Soft Tissue and Bone Tumor Diagnostics: Harnessing the Power of Molecular Techniques. Genes 2023, 14, 2229. https://doi.org/10.3390/genes14122229
Cordier F, Ferdinande L, Hoorens A, Van de Vijver K, Van Dorpe J, Creytens D. Soft Tissue and Bone Tumor Diagnostics: Harnessing the Power of Molecular Techniques. Genes. 2023; 14(12):2229. https://doi.org/10.3390/genes14122229
Chicago/Turabian StyleCordier, Fleur, Liesbeth Ferdinande, Anne Hoorens, Koen Van de Vijver, Jo Van Dorpe, and David Creytens. 2023. "Soft Tissue and Bone Tumor Diagnostics: Harnessing the Power of Molecular Techniques" Genes 14, no. 12: 2229. https://doi.org/10.3390/genes14122229
APA StyleCordier, F., Ferdinande, L., Hoorens, A., Van de Vijver, K., Van Dorpe, J., & Creytens, D. (2023). Soft Tissue and Bone Tumor Diagnostics: Harnessing the Power of Molecular Techniques. Genes, 14(12), 2229. https://doi.org/10.3390/genes14122229