
Current State of Genomics in Nursing: A Scoping Review of Healthcare Provider Oriented (Clinical and Educational) Outcomes (2012–2022)

 , , , and
, , , and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Identifying the Research Question
2.2. Identifying the Relevant Literature
2.3. Selecting the Literature
2.4. Charting the Data
2.5. Collating, Summarizing, and Reporting Results
2.6. Synthesis of Results
2.7. Patient and Public Involvement
3. Results
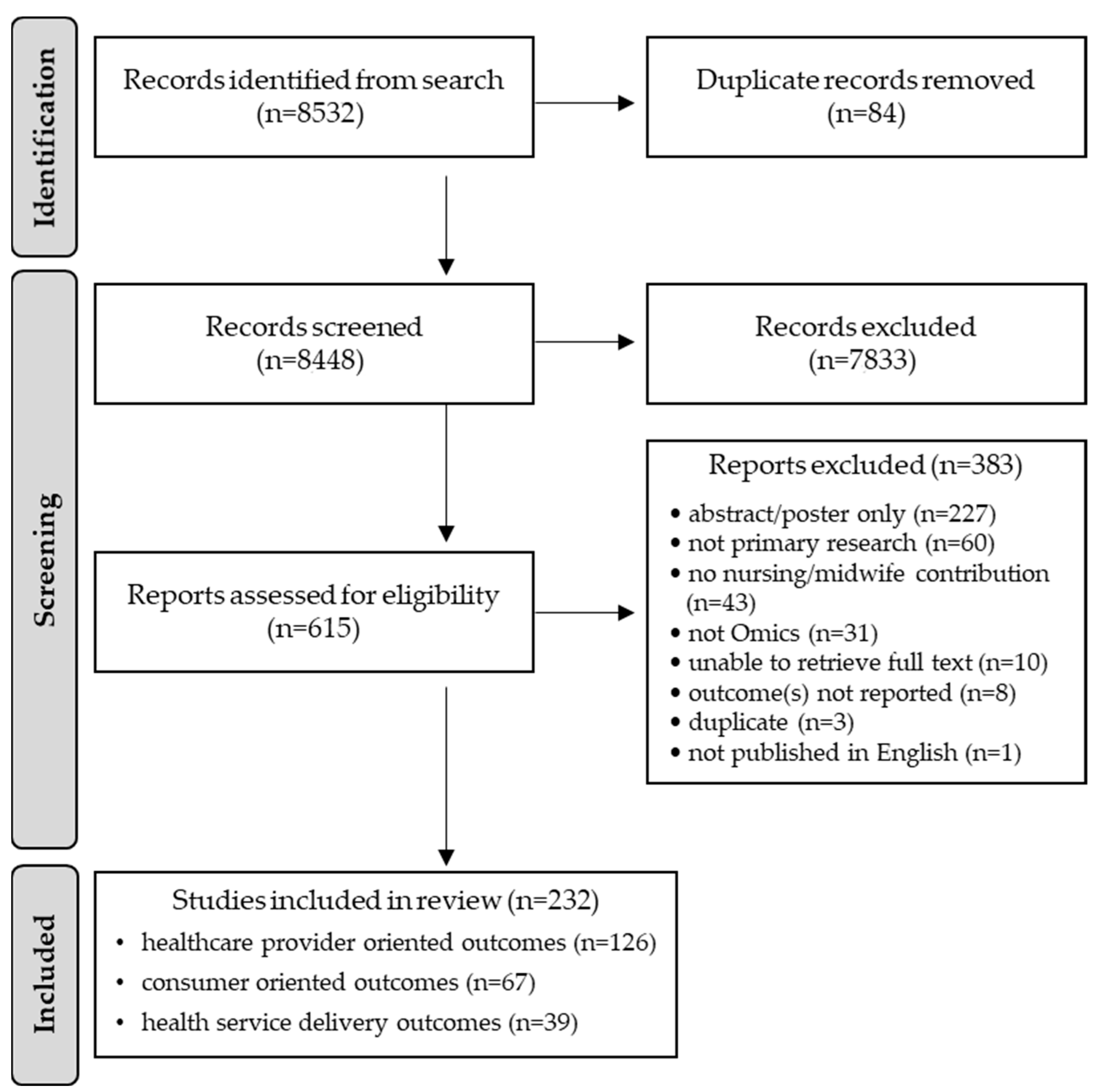
3.1. Selection of Sources of Evidence
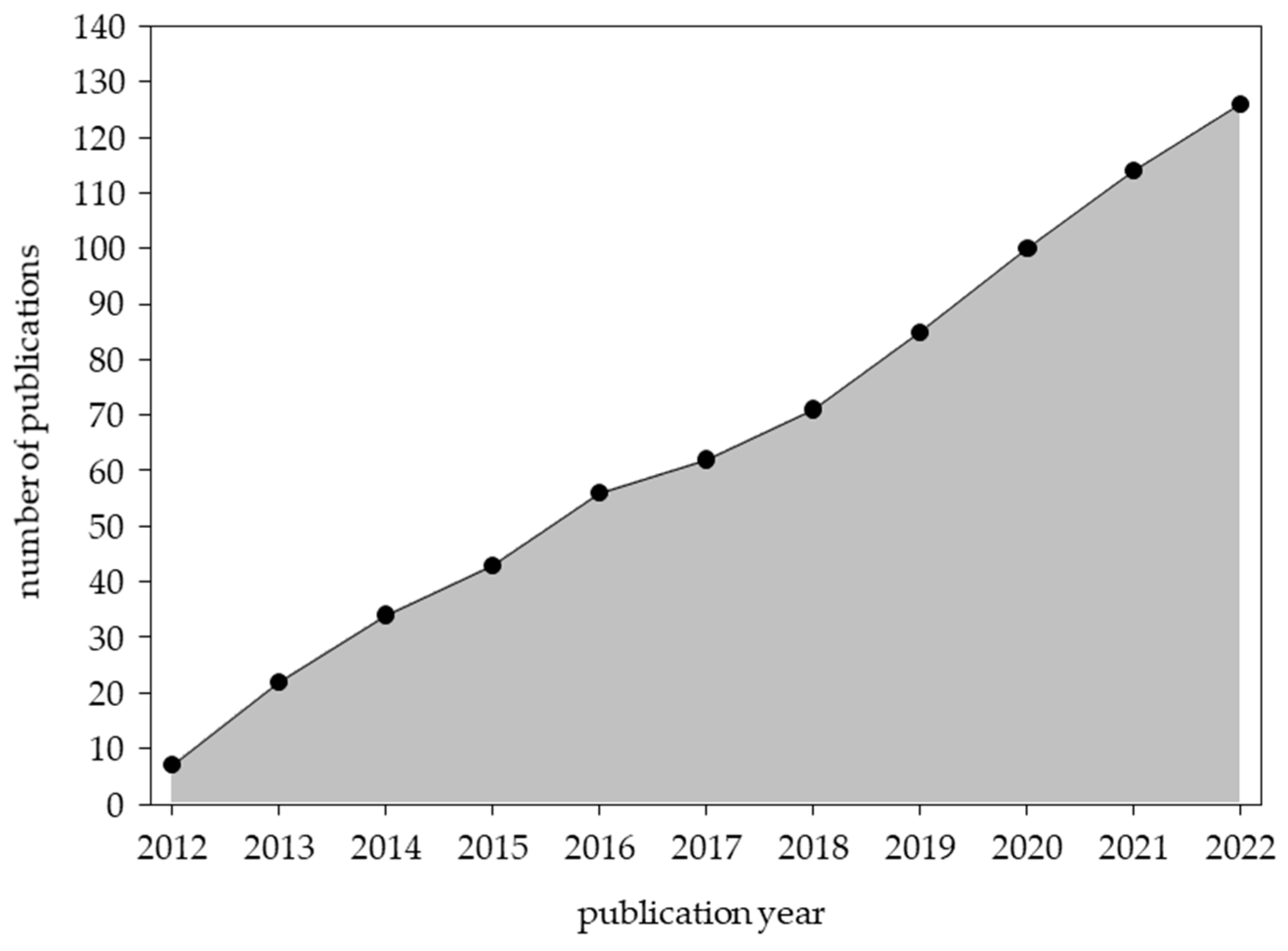
3.2. Characteristics of Sources of Evidence
3.3. Characteristics of Studies Reporting “Healthcare Provider Oriented Outcomes”
3.4. Settings of Articles Reporting “Healthcare Provider Oriented Outcomes”
3.5. Target Groups of Articles Reporting “Healthcare Provider Oriented Outcomes”
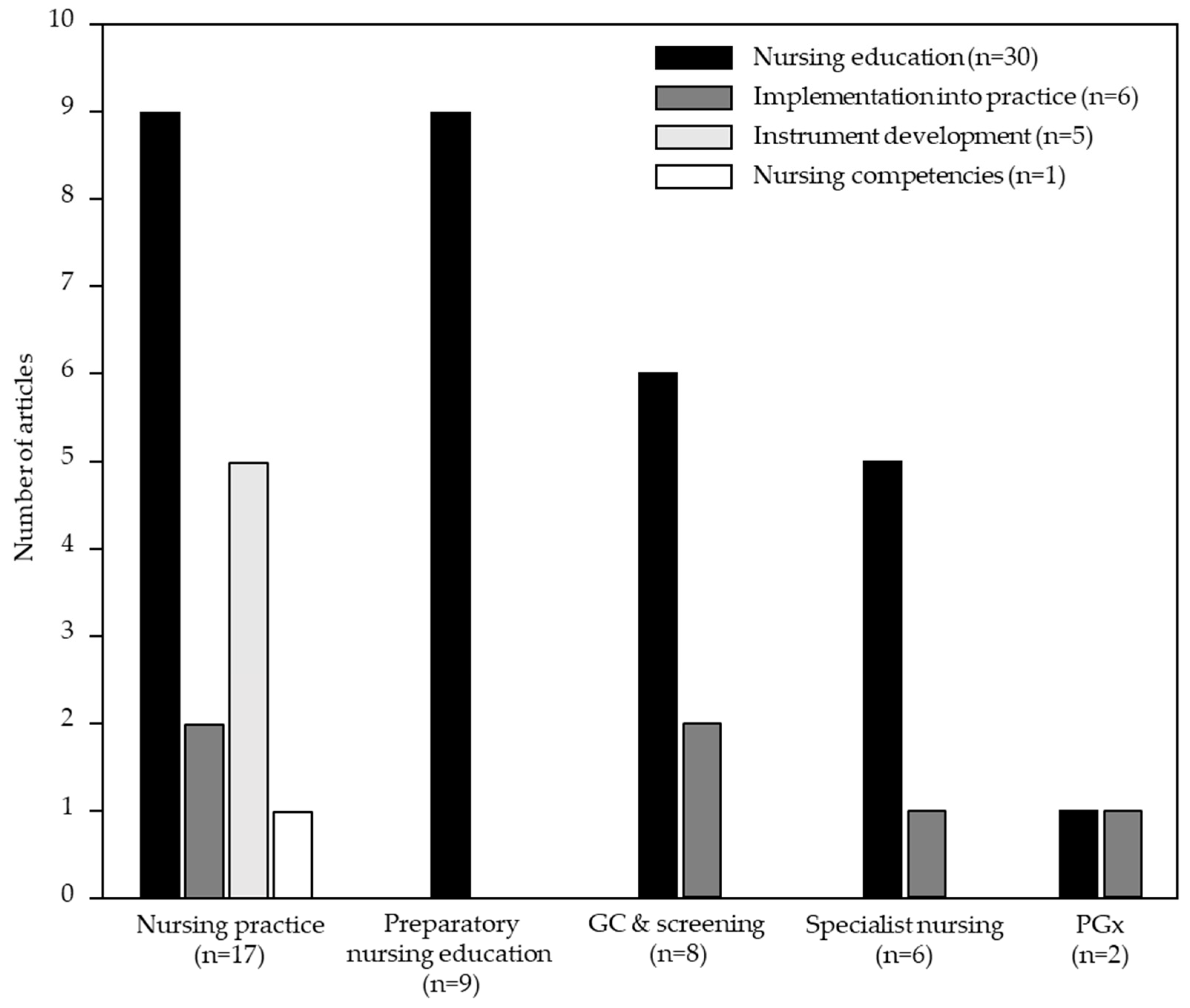
3.6. Current State of Genomics in Nursing across Key Areas of Focus
3.6.1. Nursing Practice Outcomes
3.6.2. Genetic Counseling and Screening Outcomes
3.6.3. Specialist Nursing Outcomes
3.6.4. Preparatory Nursing Education Outcomes
3.6.5. Pharmacogenomics Nursing Outcomes
3.7. Interventional Studies on Nursing in Genomics
4. Discussion
- Global efforts: Expanding integration of genomics into nursing practice beyond high income countries.
- Development pipeline: Dual efforts to instill genomic competencies in practicing nurses and embed competencies into nursing education/training.
- Competent workforce: Basing workforce development on established nursing competencies in genomics.
- Implementation into practice: Shift focus from the “knowledge and understanding” sub-domain to the “consultation process” sub-domain.
- Measurement: Utilize validated instruments to measure application of knowledge and assess interventions.
- Reporting: Use reporting standards to facilitate transparency and comparability.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- PubMed (National Library of Medicine)
- CINAHL Plus (Ebscohost)
- #1
- Title: (nurse OR nurses OR nursing OR midwife OR midwives OR midwifery)
- #2
- Abstract: (nurse OR nurses OR nursing OR midwife OR midwives OR midwifery)
- #3
- Exact Subject Heading: (MH “Nurses”) OR (MH “Midwifery”) OR (MH “Midwives”) OR (MH “Nursing as a Profession”) OR (MH “Research, Nursing”) OR (MH “Research, Midwifery”) OR (MH “Nursing Science”) OR (MH “Education, Nursing”)
- #4
- #1 OR #2 OR #3 = 648,367
- #5
- Title: (gene OR genes OR genomic OR genomics OR omics OR omic OR genetic OR genetics OR transcriptome* OR transcriptomic* OR proteome* OR proteomic* OR epigenetic* OR epigenom* OR nutrigenetic* OR nutrigenom* OR “nutritional genetic*” OR “nutritional genomic*” OR metabolomic* OR metabolome* OR pharmacogenetic* OR pharmacogenomic* OR microbiome* OR microbiomic* OR “precision healthcare” OR “precision health care” OR “precision medicine” OR “precision science” OR “personalized medicine” OR “personalized healthcare” OR “personalized health care” OR “personalised medicine” OR “personalised healthcare” OR “personalised health care” OR “individualized medicine” OR “individualised medicine” OR “family history” OR “family histories” OR “family medical history” OR “family medical histories” OR “symptom science” OR symptomic* OR symptomomic*)
- #6
- Abstract: (gene OR genes OR genomic OR genomics OR omics OR omic OR genetic OR genetics OR transcriptome* OR transcriptomic* OR proteome* OR proteomic* OR epigenetic* OR epigenom* OR nutrigenetic* OR nutrigenom* OR “nutritional genetic*” OR “nutritional genomic*” OR metabolomic* OR metabolome* OR pharmacogenetic* OR pharmacogenomic* OR microbiome* OR microbiomic* OR “precision healthcare” OR “precision health care” OR “precision medicine” OR “precision science” OR “personalized medicine” OR “personalized healthcare” OR “personalized health care” OR “personalised medicine” OR “personalised healthcare” OR “personalised health care” OR “individualized medicine” OR “individualised medicine” OR “family history” OR “family histories” OR “family medical history” OR “family medical histories” OR “symptom science” OR symptomic* OR symptomomic*)
- #7
- Exact Subject Heading: (MH “Genetics”) OR (MH “Genes”) OR (MH “Genetics, Medical”) OR (MH “Nutrigenomics”) OR (MH “Nutrigenetics”) OR (MH “Genomics”) OR (MH “Pharmacogenetics”) OR (MH “Genetics Nursing”) OR (MH “Proteomics”) OR (MH “Metabolomics”) OR (MH “Proteogenomics”) OR (MH “Epigenomics”) OR (MH “Individualized Medicine”) OR (MH “Family History”)
- Embase (Elsevier)
- Web of Science: Core Collection (Clarivate Analytics)
Appendix B
- Domain: Healthcare Provider Oriented Outcomes
- Sub-domain: Knowledge and Understanding
- attitudes, behavior of health professionals
- level of knowledge or skills
- Sub-domain: Consultation process
- practice style (e.g., patient-centeredness)
- provision of interventions
- Domain: Health Service Delivery Oriented Outcomes
- Sub-domain: Service Delivery Level
- adverse events
- health economic outcomes (e.g., costs, service utilization)
- service utilization (e.g., admission, length of stay, readmission)
- Sub-domain: Related to Research
- involvement in research
- recruitment and retention to trials
- feedback from participation in trials
- Sub-domain: Societal or Governmental
- health care monitoring (e.g., audit, accreditation, quality of care)
- health care planning (e.g., priority setting, policy, legislation)
- Domain: Consumer Oriented Outcomes
- Sub-domain: Knowledge and Understanding
- information access and use
- knowledge acquisition (i.e., level of knowledge or increased knowledge)
- retention of information, ability to recall information
- patient satisfaction with the information provided (see Satisfaction)
- psychological stress due to receiving information (see Psychological health)
- Sub-domain: Communication
- communication aides
- communication enhancement
- communication skills or techniques
- Sub-domain: Patient Involvement in Care Process
- decision-making
- patient-held information
- Sub-domain: Evaluation of Care
- consumer–professional interactions experience
- perceptions and ratings of care or interventions
- satisfaction
- Sub-domain: Support
- practical support
- psychosocial support
- Sub-domain: Skills Acquisition
- activities of daily living skills
- communication skills or techniques
- self-care skills
- social skills
- symptom control skills
- Sub-domain: Health Status and Wellbeing
- physical health (patient or carer)
- psychological health (patient or carer)
- psychosocial outcomes
- Sub-domain: Health Behavior
- attitudes
- compliance/adherence
- health-enhancing lifestyle or behavior outcomes
- risk-taking behavior
- use of interventions or services
- Sub-domain: Treatment Outcomes
- adverse outcomes
- clinical assessments (e.g., wound healing, symptom resolution)
- pain assessment or control
- physiological measures (e.g., blood pressure, blood glucose level)
References
- Calzone, K.A.; Jenkins, J.; Nicol, N.; Skirton, H.; Feero, W.G.; Green, E.D. Relevance of genomics to healthcare and nursing practice. J. Nurs. Sch. 2013, 45, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Triebold, M.; Skov, K.; Erickson, L.; Olimb, S.; Puumala, S.; Wallace, I.; Stein, Q. Geographical analysis of the distribution of certified genetic counselors in the United States. J. Genet. Couns. 2021, 30, 448–456. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, J.; Grady, P.A.; Collins, F.S. Nurses and the genomic revolution. J. Nurs. Sch. 2005, 37, 98–101. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. State of the World’s Nursing 2020: Investing in Education, Jobs and Leadership. Available online: https://www.who.int/publications/i/item/9789240003279 (accessed on 15 September 2023).
- Calzone, K.A.; Jenkins, J.; Bakos, A.D.; Cashion, A.K.; Donaldson, N.; Feero, W.G.; Feetham, S.; Grady, P.A.; Hinshaw, A.S.; Knebel, A.R.; et al. A blueprint for genomic nursing science. J. Nurs. Sch. 2013, 45, 96–104. [Google Scholar] [CrossRef]
- Conley, Y.P.; Heitkemper, M.; McCarthy, D.; Anderson, C.M.; Corwin, E.J.; Daack-Hirsch, S.; Dorsey, S.G.; Gregory, K.E.; Groer, M.W.; Henly, S.J.; et al. Educating future nursing scientists: Recommendations for integrating omics content in PhD programs. Nurs. Outlook 2015, 63, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Kirk, M.; Calzone, K.; Arimori, N.; Tonkin, E. Genetics-genomics competencies and nursing regulation. J. Nurs. Sch. 2011, 43, 107–116. [Google Scholar] [CrossRef]
- Lea, D.H. Position statement: Integrating genetics competencies into baccalaureate and advanced nursing education. Nurs. Outlook 2002, 50, 167–168. [Google Scholar] [CrossRef]
- Calzone, K.A.; Jenkins, J.; Culp, S.; Badzek, L. Hospital nursing leadership-led interventions increased genomic awareness and educational intent in Magnet settings. Nurs. Outlook 2018, 66, 244–253. [Google Scholar] [CrossRef]
- Williams, J.K.; Cashion, A.K.; Shekar, S.; Ginsburg, G.S. Genomics, clinical research, and learning health care systems: Strategies to improve patient care. Nurs. Outlook 2016, 64, 225–228. [Google Scholar] [CrossRef]
- Williams, J.K.; Feero, W.G.; Leonard, D.G.; Coleman, B. Implementation science, genomic precision medicine, and improved health: A new path forward? Nurs. Outlook 2017, 65, 36–40. [Google Scholar] [CrossRef]
- Williams, J.K.; Katapodi, M.C.; Starkweather, A.; Badzek, L.; Cashion, A.K.; Coleman, B.; Fu, M.R.; Lyon, D.; Weaver, M.T.; Hickey, K.T. Advanced nursing practice and research contributions to precision medicine. Nurs. Outlook 2016, 64, 117–123. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.K.; Feero, W.G.; Veenstra, D.L.; Starkweather, A.; Cashion, A.K. Considerations in initiating genomic screening programs in health care systems. Nurs. Outlook 2018, 66, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Acorn, M. Chief Nurse Blog: Nursing Matters April 2022. In International Council of Nurses. 2022. Available online: https://www.icn.ch/news/chief-nurse-blog-nursing-matters-april-2022 (accessed on 15 September 2023).
- Morris, Z.S.; Wooding, S.; Grant, J. The answer is 17 years, what is the question: Understanding time lags in translational research. J. R. Soc. Med. 2011, 104, 510–520. [Google Scholar] [CrossRef] [PubMed]
- Hill, S.; Lowe, D.B.; McKenzie, J.E. Identifying outcomes of importance to communication and participation. In The Knowledge Patient: Communication and Participation in Health; Wiley Blackwell: Oxford, UK, 2011. [Google Scholar]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K.; et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef] [PubMed]
- Covidence Systematic Review Software. 2023. Available online: www.covidence.org (accessed on 15 September 2023).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Saunders, C.H.; Sierpe, A.; von Plessen, C.; Kennedy, A.M.; Leviton, L.C.; Bernstein, S.L.; Goldwag, J.; King, J.R.; Marx, C.M.; Pogue, J.A.; et al. Practical thematic analysis: A guide for multidisciplinary health services research teams engaging in qualitative analysis. BMJ 2023, 381, e074256. [Google Scholar] [CrossRef]
- Maradiegue, A.H.; Edwards, Q.T.; Seibert, D. 5-years later—Have faculty integrated medical genetics into nurse practitioner curriculum? Int. J. Nurs. Educ. Sch. 2013, 10, 245–254. [Google Scholar] [CrossRef]
- Butts, B.; Alford, T.; Brewster, G.; Carlson, N.; Coleman, E.; Davis, E.; Ferranti, E.; Kimble, L.P.; Narapareddy, L.; Wells, J.; et al. Adaptation of Metabolomics and Microbiomic Research Protocols During the COVID-19 Pandemic. Nurs. Res. 2022, 71, 128–137. [Google Scholar] [CrossRef]
- Mahon, S.M. Allocation of work activities in a comprehensive cancer genetics program. Clin. J. Oncol. Nurs. 2013, 17, 397–404. [Google Scholar] [CrossRef]
- Koleck, T.A.; Bender, C.M.; Sereika, S.M.; Ahrendt, G.; Jankowitz, R.C.; McGuire, K.P.; Ryan, C.M.; Conley, Y.P. Apolipoprotein E genotype and cognitive function in postmenopausal women with early-stage breast cancer. Oncol. Nurs. Forum 2014, 41, E313–E325. [Google Scholar] [CrossRef]
- Ward, L.D.; French, B.F.; Barbosa-Leiker, C.; Iverson, A.E. Application of Exploratory Factor Analysis and Item Response Theory to Validate the Genomic Nursing Concept Inventory. J. Nurs. Educ. 2016, 55, 9–17. [Google Scholar] [CrossRef]
- Jenkins, J.F.; Calzone, K.A. Are nursing faculty ready to integrate genomic content into curricula? Nurse Educ. 2012, 37, 25–29. [Google Scholar] [CrossRef]
- Johengen, E.K.; Ward, K.M.; Coe, A.B.; Pasternak, A.L. Assessing the knowledge, perceptions, and practices of primary care clinicians toward pharmacogenetics. J. Am. Coll. Clin. Pharm. 2020, 4, 27–32. [Google Scholar] [CrossRef]
- Kronk, R.; Colbert, A.; Lengetti, E. Assessment of a Competency-Based Undergraduate Course on Genetics and Genomics. Nurse Educ. 2018, 43, 201–205. [Google Scholar] [CrossRef]
- Wesmiller, S.W.; Bender, C.M.; Sereika, S.M.; Ahrendt, G.; Bonaventura, M.; Bovbjerg, D.H.; Conley, Y. Association between serotonin transport polymorphisms and postdischarge nausea and vomiting in women following breast cancer surgery. Oncol. Nurs. Forum 2014, 41, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Dodson, C. Attitudes of oncology nurses concerning pharmacogenomics. Per. Med. 2015, 12, 559–562. [Google Scholar] [CrossRef] [PubMed]
- Arguello, L.E.; Mauldin, K.; Goyal, D. Atypical Eating Disinhibition Genotype. J. Nurse Pract. 2018, 14, 491–495. [Google Scholar] [CrossRef]
- Hanish, A.E.; Cohen, M.Z.; Starr, L.J. Autism spectrum disorder and genetic testing: Parental perceptions and decision-making. J. Spec. Pediatr. Nurs. 2018, 23, e12211. [Google Scholar] [CrossRef] [PubMed]
- Rutledge, C.; Gould, C.; Lee, P.C.; Sowden, W.; Lustik, M.; Egan, K. Behavioral Health Screening in Military Cystic Fibrosis Centers: A Survey. Mil. Med. 2022, usac161. [Google Scholar] [CrossRef] [PubMed]
- Vandiver, K.M.; Erdei, E.; Mayer, A.G.; Ricciardi, C.; O’Leary, M.; Burke, K.; Zelikoff, J.T. Building Environmental Health and Genomics Literacy among Healthcare Providers Serving Vulnerable Communities: An Innovative Educational Framework. Int. J. Environ. Res. Public Health 2022, 19, 929. [Google Scholar] [CrossRef] [PubMed]
- Read, C.Y.; Ricciardi, C.E.; Gruhl, A.; Williams, L.; Vandiver, K.M. Building Genetic Competence Through Partnerships and Interactive Models. J. Nurs Educ. 2016, 55, 300–303. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.G.; Royer, J.; Mann, J.; McDermott, S.; Valdez, R. Capture-recapture methodology to study rare conditions using surveillance data for fragile X syndrome and muscular dystrophy. Orphanet J. Rare Dis. 2017, 12, 76. [Google Scholar] [CrossRef] [PubMed]
- Dettwyler, S.A.; Zielinski, R.E.; Yashar, B.M. Certified Nurse-Midwives’ Experiences With Provision of Prenatal Genetic Screening: A Case for Interprofessional Collaboration. J. Perinat. Neonatal Nurs. 2019, 33, E3–E14. [Google Scholar] [CrossRef] [PubMed]
- Driessnack, M.; Gallo, A.M. Children ‘draw-and-tell’ their knowledge of genetics. Pediatr. Nurs. 2013, 39, 173–180. [Google Scholar]
- Palomaki, G.E.; Kloza, E.M.; O’Brien, B.M.; Eklund, E.E.; Lambert-Messerlian, G.M. The clinical utility of DNA-based screening for fetal aneuploidy by primary obstetrical care providers in the general pregnancy population. Genet. Med. 2017, 19, 778–786. [Google Scholar] [CrossRef]
- Anderson, J.L.; Kruisselbrink, T.M.; Lisi, E.C.; Hughes, T.M.; Steyermark, J.M.; Winkler, E.M.; Berg, C.M.; Vierkant, R.A.; Gupta, R.; Ali, A.H.; et al. Clinically Actionable Findings Derived From Predictive Genomic Testing Offered in a Medical Practice Setting. Mayo Clin. Proc. 2021, 96, 1407–1417. [Google Scholar] [CrossRef]
- Unertl, K.M.; Jaffa, H.; Field, J.R.; Price, L.; Peterson, J.F. Clinician Perspectives on Using Pharmacogenomics in Clinical Practice. Per. Med. 2015, 12, 339–347. [Google Scholar] [CrossRef]
- Brandt, D.S.; Shinkunas, L.; Hillis, S.L.; Daack-Hirsch, S.E.; Driessnack, M.; Downing, N.R.; Liu, M.F.; Shah, L.L.; Williams, J.K.; Simon, C.M. A closer look at the recommended criteria for disclosing genetic results: Perspectives of medical genetic specialists, genomic researchers, and institutional review board chairs. J. Genet. Couns. 2013, 22, 544–553. [Google Scholar] [CrossRef]
- Cohen, S.A.; Nixon, D.M. A collaborative approach to cancer risk assessment services using genetic counselor extenders in a multi-system community hospital. Breast Cancer Res. Treat. 2016, 159, 527–534. [Google Scholar] [CrossRef]
- Mowbray, C.; Turner, J.; Gai, J.; Jacobs, S. Comfort with Pharmacogenetic Testing Amongst Pediatric Oncology Providers and Their Patients. J. Pediatr. Hematol. Oncol. Nurs. 2022, 39, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Newcomb, P.; Hudlow, R.; Heilskov, J.; Martinez, C.D.; Le, H. Conversations with children about DNA and genes using an original children’s book. J. Pediatr. Health Care 2014, 28, 497–506. [Google Scholar] [CrossRef] [PubMed]
- Knisely, M.R.; Carpenter, J.S.; Draucker, C.B.; Skaar, T.; Broome, M.E.; Holmes, A.M.; Von Ah, D. CYP2D6 drug-gene and drug-drug-gene interactions among patients prescribed pharmacogenetically actionable opioids. Appl. Nurs. Res. 2017, 38, 107–110. [Google Scholar] [CrossRef]
- Rad, E.J.; Mirza, A.A.; Chhatwani, L.; Purington, N.; Mohabir, P.K. Cystic fibrosis telemedicine in the era of COVID-19. JAMIA Open 2022, 5, ooac005. [Google Scholar] [CrossRef] [PubMed]
- Hickey, K.T.; Sciacca, R.R.; McCarthy, M.S. Descriptive survey of Summer Genetics Institute nurse graduates in the USA. Nurs. Health Sci. 2013, 15, 3–8. [Google Scholar] [CrossRef]
- Ward, L.D.; Haberman, M.; Barbosa-Leiker, C. Development and psychometric evaluation of the genomic nursing concept inventory. J. Nurs. Educ. 2014, 53, 511–518. [Google Scholar] [CrossRef]
- Jabaley, T.; Underhill-Blazey, M.L.; Berry, D.L. Development and Testing of a Decision Aid for Unaffected Women with a BRCA1 or BRCA2 Mutation. J. Cancer Educ. 2020, 35, 339–344. [Google Scholar] [CrossRef]
- Katapodi, M.C.; Jung, M.; Schafenacker, A.M.; Milliron, K.J.; Mendelsohn-Victor, K.E.; Merajver, S.D.; Northouse, L.L. Development of a Web-based Family Intervention for BRCA Carriers and Their Biological Relatives: Acceptability, Feasibility, and Usability Study. JMIR Cancer 2018, 4, e7. [Google Scholar] [CrossRef]
- Kuhl, A.; van Calcar, S.; Baker, M.; Seroogy, C.M.; Rice, G.; Scott Schwoerer, J. Development of carrier testing for common inborn errors of metabolism in the Wisconsin Plain population. Genet. Med. 2017, 19, 352–356. [Google Scholar] [CrossRef]
- Torbert, N.; Neumann, M.; Birge, N.; Perkins, D.; Ehrhardt, E.; Weaver, M.S. Discipline-Specific Perspectives on Caring for Babies with Trisomy 13 or 18 in the Neonatal Intensive Care Unit. Am. J. Perinatol. 2020, 39, 1074–1082. [Google Scholar] [CrossRef]
- Braid, S.M.; Okrah, K.; Shetty, A.; Corrada Bravo, H. DNA Methylation Patterns in Cord Blood of Neonates Across Gestational Age. Nurs. Res. 2017, 66, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Jenerette, C.M.; Brewer, C.A.; Silva, S.; Tanabe, P. Does Attendance at a Sickle Cell Educational Conference Improve Clinician Knowledge and Attitude Toward Patients with Sickle Cell Disease? Pain Manag. Nurs. 2016, 17, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Underwood, S.M.; Kelber, S. Enhancing the Collection, Discussion and Use of Family Health History by Consumers, Nurses and Other Health Care Providers: Because Family Health History Matters. Nurs. Clin. N. Am. 2015, 50, 509–529. [Google Scholar] [CrossRef]
- Regan, M.; Engler, M.B.; Coleman, B.; Daack-Hirsch, S.; Calzone, K.A. Establishing the Genomic Knowledge Matrix for Nursing Science. J. Nurs. Sch. 2019, 51, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Tully, L.A.; Calzone, K.A.; Cashion, A.K. Establishing the Omics Nursing Science & Education Network. J. Nurs. Sch. 2020, 52, 192–200. [Google Scholar] [CrossRef]
- Catherino, A.B.; Halupa, C.; Sharara, F.I.; Bromer, J.G.; Hayward, B.; Catherino, W.H. Evaluation of an embryology and genetic testing patient counseling education intervention for reproductive endocrinology nurses. Fertil. Steril. 2019, 112, 275–282.e271. [Google Scholar] [CrossRef]
- Chen, B.; Shahangian, S.; Taylor, T.H., Jr.; Yesupriya, A.; Greene, C.; Curry, V.J.; Zehnbauer, B. Evaluation of Diverse Health Professionals’ Learning Experience in a Continuing Education Activity for Quality Practices in Molecular Genetic Testing. Clin. Lab. Sci. 2016, 29, 200–211. [Google Scholar] [CrossRef]
- Alexander, K.; Cooper, B.; Paul, S.M.; West, C.; Yates, P.; Kober, K.M.; Aouizerat, B.E.; Miaskowski, C. Evidence of associations between cytokine gene polymorphisms and quality of life in patients with cancer and their family caregivers. Oncol. Nurs. Forum 2014, 41, E267–E281. [Google Scholar] [CrossRef]
- Rogers, M.A.; Lizer, S.; Doughty, A.; Hayden, B.; Klein, C.J. Expanding RN Scope of Knowledge--Genetics/Genomics: The New Frontier. J. Nurses Prof. Dev. 2017, 33, 56–63. [Google Scholar] [CrossRef]
- Coleman, B.; Powell-Young, Y.M.; Martinez, B.; Wooters, J. Exploration of African-American Nurses’ Perceptions Toward Seeking and Utilizing Genetic Information. J. Natl. Black Nurses Assoc. 2018, 29, 9–16. [Google Scholar]
- Bashore, L.M.; Daniels, G.; Borchers, L.; Howington, L.L.; Cheek, D.J. Facilitating faculty competency to integrate genomics into nursing curriculum within a private US University. Nurs. Res. Rev. 2018, 8, 9–14. [Google Scholar] [CrossRef]
- Read, C.Y.; Ward, L.D. Faculty Performance on the Genomic Nursing Concept Inventory. J. Nurs. Sch. 2016, 48, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Ford, C.D.; Rooks, R.N.; Montgomery, M. Family health history and future nursing practice: Implications for undergraduate nursing students. Nurse Educ. Pract. 2016, 21, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Voss, J.G.; Dobra, A.; Morse, C.; Kovacs, J.A.; Danner, R.L.; Munson, P.J.; Logan, C.; Rangel, Z.; Adelsberger, J.W.; McLaughlin, M.; et al. Fatigue-Related Gene Networks Identified in CD14+ Cells Isolated From HIV-Infected Patients-Part I: Research Findings. Biol. Res. Nurs. 2013, 15, 137–151. [Google Scholar] [CrossRef]
- Saligan, L.N.; Rivera, R.R. Filipino-American Nurses’ Knowledge, Perceptions, Beliefs and Practice of Genetics and Genomics. Philipp. J. Nurs. 2014, 84, 48–58. [Google Scholar]
- Dodson, C.H.; Baker, E. Focus group testing of a mobile app for pharmacogenetic-guided dosing. J. Am. Assoc. Nurse Pract. 2021, 33, 205–210. [Google Scholar] [CrossRef]
- Schutte, D.L.; Mukhopadhyay, N.; Holwerda, T.; Sluka, K.; Rakel, B.; Govil, M. Genetic Predictors of Knee Pain in Persons With Mild to Moderate Osteoarthritis. Res. Gerontol. Nurs. 2020, 13, 191–202. [Google Scholar] [CrossRef]
- Williams, L.; Dansereau, C.; Trainor, B. A Genetics Learning Program for Nurses Caring for Children Treated With Ex Vivo Autologous Gene Therapy. J. Contin. Educ. Nurs. 2019, 50, 218–227. [Google Scholar] [CrossRef]
- Downing, N.R.; Williams, J.K.; Daack-Hirsch, S.; Driessnack, M.; Simon, C.M. Genetics specialists’ perspectives on disclosure of genomic incidental findings in the clinical setting. Patient Educ. Couns. 2013, 90, 133–138. [Google Scholar] [CrossRef]
- Jenkins, J.; Calzone, K.A. Genomics nursing Faculty Champion initiative. Nurse Educ. 2014, 39, 8–13. [Google Scholar] [CrossRef]
- Yoes, M.-V.; Thomas, L. Hereditary Cancer Genetic Risk Assessment, Testing, and Counseling: A Nurse Practitioner–Led Program in a Community Setting. J. Nurse Pract. 2020, 16, 660–665. [Google Scholar] [CrossRef]
- Appel, S.J.; Cleiment, R.J. Identifying Women at Risk for Hereditary Breast and Ovarian Cancer Syndrome Utilizing Breast Care Nurse Navigation at Mammography and Imaging Centers. J. Natl. Black Nurses Assoc. 2015, 26, 17–26. [Google Scholar] [PubMed]
- McAllister, K.A.; Schmitt, M.L. Impact of a nurse navigator on genomic testing and timely treatment decision making in patients with breast cancer. Clin. J. Oncol. Nurs. 2015, 19, 510–512. [Google Scholar] [CrossRef]
- Clark, R. Implementation of a Risk Assessment Process in a Primary Clinic to Identify Women at High Risk for Developing Breast Cancer Based on Family History; University of Louisiana at Lafayette: Lafayette, LA, USA, 2016; p. 1. [Google Scholar]
- Marvell, L. Implementing the basic principles of biomarker use in oncology nursing: Enhancing knowledge and practice through an elearning module. Can. Oncol. Nurs. J. 2017, 27, 401–402. [Google Scholar] [PubMed]
- Cohen, S.A.; McIlvried, D.E. Improving access with a collaborative approach to cancer genetic counseling services: A pilot study. Community Oncol. 2013, 10, 227–234. [Google Scholar] [CrossRef]
- Whitt, K.J.; Macri, C.; O’Brien, T.J.; Wright, S. Improving nurse practitioners’ competence with genetics: Effectiveness of an online course. J. Am. Assoc. Nurse Pract. 2016, 28, 151–159. [Google Scholar] [CrossRef]
- Temkin, S.M.; Smeltzer, M.P.; Dawkins, M.D.; Boehmer, L.M.; Senter, L.; Black, D.R.; Blank, S.V.; Yemelyanova, A.; Magliocco, A.M.; Finkel, M.A.; et al. Improving the quality of care for patients with advanced epithelial ovarian cancer: Program components, implementation barriers, and recommendations. Cancer 2022, 128, 654–664. [Google Scholar] [CrossRef]
- Graff, S.L.; Holder, J.M.; Sears, L.E.; Kurbegov, D. Increase in Genetic Counseling and Testing Referrals After Breast Cancer Pathway Implementation. JCO Oncol. Pract. 2020, 16, e1481–e1488. [Google Scholar] [CrossRef]
- LaRonde, M.P.; Connor, J.A.; Cerrato, B.; Chiloyan, A.; Lisanti, A.J. Individualized Family-Centered Developmental Care for Infants With Congenital Heart Disease in the Intensive Care Unit. Am. J. Crit. Care 2022, 31, e10–e19. [Google Scholar] [CrossRef]
- Newcomb, P.; True, B.; Wells, J.N.; Walsh, J.; Pehl, S. Informing New Mothers about Newborn Screening Bloodspot Repositories during Postpartum Hospitalization. MCN Am. J Matern. Child Nurs. 2019, 44, 332–337. [Google Scholar] [CrossRef]
- O’Keefe, L.C.; Koelle, P.; McGee, Z.; Dewberry, L.S.; Wright, C.; Stallings, J.E.; Gates, E.; Chittur, K. Innovations in Worksite Diagnosis of Urinary Tract Infections and the Occupational Health Nurse. Workplace Health Saf. 2019, 67, 268–274. [Google Scholar] [CrossRef]
- Calzone, K.A.; Jenkins, J.; Culp, S.; Caskey, S.; Badzek, L. Introducing a New Competency Into Nursing Practice. J. Nurs. Regul. 2014, 5, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Quinn, G.P.; Knapp, C.; Sehovic, I.; Ung, D.; Bowman, M.; Gonzalez, L.; Vadaparampil, S.T. Knowledge and Educational Needs about Pre-Implantation Genetic Diagnosis (PGD) among Oncology Nurses. J. Clin. Med. 2014, 3, 632–645. [Google Scholar] [CrossRef] [PubMed]
- Newcomb, P.; True, B.; Walsh, J.; Dyson, M.; Lockwood, S.; Douglas, B. Maternal attitudes and knowledge about newborn screening. MCN Am. J. Matern. Child Nurs. 2013, 38, 289–294. [Google Scholar] [CrossRef]
- Jones, T.; Freeman, K.; Ackerman, M.; Trivedi, M.S.; Silverman, T.; Shapiro, P.; Kukafka, R.; Crew, K.D. Mental Illness and BRCA1/2 Genetic Testing Intention Among Multiethnic Women Undergoing Screening Mammography. Oncol. Nurs. Forum 2020, 47, E13–E24. [Google Scholar] [CrossRef] [PubMed]
- Withycombe, J.S.; Eldridge, R.; Jin, Y.; Gu, H.; Castellino, S.M.; Sears, D.D. Metabolites Associated with Fatigue and Physical Activity in Childhood Cancer. Biol. Res. Nurs. 2022, 24, 350–361. [Google Scholar] [CrossRef]
- Jenkins, J.; Calzone, K.A.; Caskey, S.; Culp, S.; Weiner, M.; Badzek, L. Methods of genomic competency integration in practice. J. Nurs. Sch. 2015, 47, 200–210. [Google Scholar] [CrossRef]
- Coleman, B.; Calzone, K.A.; Jenkins, J.; Paniagua, C.; Rivera, R.; Hong, O.S.; Spruill, I.; Bonham, V. Multi-ethnic minority nurses’ knowledge and practice of genetics and genomics. J. Nurs. Sch. 2014, 46, 235–244. [Google Scholar] [CrossRef]
- Spruill, I.J.; Coleman, B.L.; Powell-Young, Y.M.; Williams, T.H.; Magwood, G. Non-Biological (Fictive Kin and Othermothers): Embracing the Need for a Culturally Appropriate Pedigree Nomenclature in African-American Families. J. Natl. Black Nurses Assoc. 2014, 25, 23–30. [Google Scholar]
- Dodson, C. Oncology Nurses’ Knowledge of Pharmacogenomics Before and After Implementation of an Education Module. Oncol. Nurs. Forum 2018, 45, 575–580. [Google Scholar] [CrossRef]
- Henker, R.; Khalil, H.; Sereika, S.; Feng, D.; Alexander, S.; Conley, Y.; Gruen, G.; Tarkin, I.; Siska, P. OPRM1 and COMT Gene Gene Interaction is Associated with Postoperative Pain and Opioid Consumption after Orthopedic Trauma Surgery—28th Annual Scientific Sessions Abstracts. Nurs. Res. 2016, 65, E50–E51. [Google Scholar] [CrossRef]
- Resnick, B.; Klinedinst, N.J.; Yerges-Armstrong, L.; Magaziner, J.; Orwig, D.; Hochberg, M.C.; Gruber-Baldini, A.L.; Hicks, G.E.; Dorsey, S.G. Pain, Genes, and Function in the Post-Hip Fracture Period. Pain Manag. Nurs. 2016, 17, 181–196. [Google Scholar] [CrossRef]
- Flowers, E.; Martin, M.; Abid, H.; Binford, S.; Mackin, L. Pairing pedagogical and genomic advances to prepare advanced practice nurses for the era of precision health. BMC Med. Educ. 2019, 19, 112. [Google Scholar] [CrossRef]
- Williams, T.; Dale, R. A Partnership Approach to Genetic and Genomic Graduate Nursing Curriculum: Report of a New Course’s Impact on Student Confidence. J. Nurs. Educ. 2016, 55, 574–578. [Google Scholar] [CrossRef]
- Farrell, R.M.; Nutter, B.; Agatisa, P.K. Patient-centered prenatal counseling: Aligning obstetric healthcare professionals with needs of pregnant women. Women Health 2015, 55, 280–296. [Google Scholar] [CrossRef]
- Hersperger, C.L.; Boucher, J.; Theroux, R. Paving the Way: A Grounded Theory of Discovery and Decision Making for Individuals With the CDH1 Marker. Oncol. Nurs. Forum 2020, 47, 446–456. [Google Scholar] [CrossRef] [PubMed]
- Manzor Mitrzyk, B.; Plegue, M.A.; Kadri, R.; Danak, S.U.; Hubbard, J.D.; Kaip, E.A.; Roberson, D.N.; Ellingrod, V.L.; Farris, K.B.; Ruffin, M.T.; et al. Pharmacogenomic testing for mental health (Part I): Documenting early adopter perceptions of use for eight scenarios. Pers. Med. 2021, 18, 223–232. [Google Scholar] [CrossRef] [PubMed]
- White, M.M.; Walker, D.K.; Howington, L.L.; Cheek, D.J. Pharmacogenomics and Psychiatric Nursing. Issues Ment. Health Nurs. 2019, 40, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Pierce, J.D.; Shen, Q.H.; Peltzer, J.; Thimmesch, A.; Hiebert, J.B. A pilot study exploring the effects of ubiquinol on brain genomics after traumatic brain injury. Nurs. Outlook 2017, 65, S44–S52. [Google Scholar] [CrossRef] [PubMed]
- Edelman, E.A.; Tanner, P.C.; Taber, K.A.; McConnell, S.C.; Nicholson, L.J.; Ingram, T.M.; Steinmark, L.; Reed, E.K. Provider engagement in precision oncology education: An exploratory analysis of online continuing medical education data. Per. Med. 2019, 16, 199–209. [Google Scholar] [CrossRef]
- Mathis, H.C. Reducing the Intimidation Factor of Teaching Genetics and Genomics in Nursing. J. Nurs. Educ. 2022, 61, 261–263. [Google Scholar] [CrossRef] [PubMed]
- Thompson, C.A.; Tiedt, J.; Beqiri, M.; Smith, D.W. A Retrospective Evaluation of a Nurse Practitioner-Led Cancer Genetics Program. J. Nurse Pract. 2022, 18, 276–284. [Google Scholar] [CrossRef]
- Baker, S.K. Rural Arizona Nurse Practitioners’ Knowledge of Hereditary Breast and Ovarian Cancer Risk Assessment. Ph.D. Thesis, The University of Arizona, Tucson, AZ, USA, 2016; p. 1. [Google Scholar]
- Pal, T.; Cragun, D.; Lewis, C.; Doty, A.; Rodriguez, M.; Radford, C.; Thompson, Z.; Kim, J.; Vadaparampil, S.T. A statewide survey of practitioners to assess knowledge and clinical practices regarding hereditary breast and ovarian cancer. Genet. Test. Mol. Biomark. 2013, 17, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Sloand, E.; Bourguet, A.N.; Engle-Pratt, W.; Bodurtha, J. Striving for Precision: Enhancing Genetic Competency in Primary Care Nurse Practitioner Students. J. Nurs. Educ. 2018, 57, 690–693. [Google Scholar] [CrossRef] [PubMed]
- Calzone, K.A.; Jenkins, J.; Yates, J.; Cusack, G.; Wallen, G.R.; Liewehr, D.J.; Steinberg, S.M.; McBride, C. Survey of nursing integration of genomics into nursing practice. J. Nurs. Sch. 2012, 44, 428–436. [Google Scholar] [CrossRef] [PubMed]
- Kashani, M.; Eliasson, A.; Vernalis, M.; Bailey, K.; Terhaar, M. A systematic approach incorporating family history improves identification of cardiovascular disease risk. J. Cardiovasc. Nurs. 2015, 30, 292–297. [Google Scholar] [CrossRef]
- Calzone, K.A.; Culp, S.; Jenkins, J.; Caskey, S.; Edwards, P.B.; Fuchs, M.A.; Reints, A.; Stange, B.; Questad, J.; Badzek, L. Test-Retest Reliability of the Genetics and Genomics in Nursing Practice Survey Instrument. J. Nurs. Meas. 2016, 24, 54–68. [Google Scholar] [CrossRef]
- Williams, P.H.; Nemeth, L.S.; Sanner, J.E.; Frazier, L.Q. Thematic analysis of cardiac care patients’ explanations for declining contribution to a genomic research-based biobank. Am. J. Crit. Care 2013, 22, 320–327. [Google Scholar] [CrossRef][Green Version]
- Paljevic, E.D. A Transformative Impact of Theory in Clinical Practice: A Study in a Cardiogenetics Clinic. Res. Theory Nurs. Pract. 2020, 34, 129–143. [Google Scholar] [CrossRef]
- Cherry, C.; Ropka, M.; Lyle, J.; Napolitano, L.; Daly, M.B. Understanding the needs of women considering risk-reducing salpingo-oophorectomy. Cancer Nurs. 2013, 36, E33–E38. [Google Scholar] [CrossRef]
- Smania, M. Use of a Point-of-Care Tool to Improve Nurse Practitioner BRCA Knowledge. Clin. J. Oncol. Nurs. 2016, 20, 327–331. [Google Scholar] [CrossRef] [PubMed]
- McCurry, M.K.; Rudd-Arieta, M.; Viveiros, J. Using Consensus Testing to Enhance Genomic Understanding and Teamwork in Doctoral Advanced Practice Nursing Students. Nurs. Educ. Perspect. 2020, 41, 168–170. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.M.; Hellinger, A.; Dionne, R.; Brown, L.; Galvin, R.; Griggs, S.; Mittler, K.; Harney, K.; Manzi, S.; VanderPluym, C.; et al. Utility of a dedicated pediatric cardiac anticoagulation program: The Boston Children’s Hospital experience. Pediatr. Cardiol. 2015, 36, 842–850. [Google Scholar] [CrossRef] [PubMed]
- Plavskin, A.; Samuels, W.E.; Calzone, K.A. Validity evaluation of the genetics and genomics in nursing practice survey. Nurs. Open 2019, 6, 1404–1413. [Google Scholar] [CrossRef] [PubMed]
- Powell-Young, Y.M.; Spruill, I.J. Views of Black nurses toward genetic research and testing. J. Nurs. Sch. 2013, 45, 151–159. [Google Scholar] [CrossRef]
- Hash, M.G.; Walker, P.; Laferriere, H.; Melton, L.A.; Heller, L.; Phillips, J. Virtual and asynchronous teaching of computer-assisted diagnosis of genetic diseases seen in clinics. Mol. Genet. Metab. 2021, 132, S295–S296. [Google Scholar] [CrossRef]
- McCabe, M.; Ward, L.D.; Ricciardi, C. Web-Based Assessment of Genomic Knowledge Among Practicing Nurses: A Validation Study. J. Contin. Educ. Nurs. 2016, 47, 189–196. [Google Scholar] [CrossRef]
- Kessler, T.A. Increasing mammography and cervical cancer knowledge and screening behaviors with an educational program. Oncol. Nurs. Forum 2012, 39, 61–68. [Google Scholar] [CrossRef]
- Crane, M.J.; Quinn Griffin, M.T.; Andrews, C.M.; Fitzpatrick, J.J. The level of importance and level of confidence that midwives in the United States attach to using genetics in practice. J. Midwifery Women’s Health 2012, 57, 114–119. [Google Scholar] [CrossRef]
- Underhill, M.L.; Lally, R.M.; Kiviniemi, M.T.; Murekeyisoni, C.; Dickerson, S.S. Living My Family’s Story Identifying the Lived Experience in Healthy Women at Risk for Hereditary Breast Cancer. Cancer Nurs. 2012, 35, 493–504. [Google Scholar] [CrossRef]
- Calzone, K.A.; Jenkins, J.; Culp, S.; Bonham, V.L., Jr.; Badzek, L. National nursing workforce survey of nursing attitudes, knowledge and practice in genomics. Per. Med. 2013, 10. [Google Scholar] [CrossRef] [PubMed]
- Pestka, E.L.; Meiers, S.J.; Shah, L.L.; Junglen, L.M.; Delgado, A. Nurses’ perceived benefits, barriers, and educational recommendations for using family pedigrees in clinical practice. J. Contin. Educ. Nurs. 2012, 43, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, R.; Kopin, S. Theory development from studies with young women with breast cancer who are BRCA mutation negative. ANS Adv. Nurs. Sci. 2013, 36, E41–E53. [Google Scholar] [CrossRef] [PubMed]
- Labore, N. Transition to Self-Management: The Lived Experience of 21–25 Year Olds with Sickle Cell Disease. Ph.D. Thesis, University of Massachusetts Lowell, Lowell, MA, USA, 2012; p. 277. [Google Scholar]
- Martin, L.; Hutton, E.K.; Gitsels-van der Wal, J.T.; Spelten, E.R.; Kuiper, F.; Pereboom, M.T.; van Dulmen, S. Antenatal counselling for congenital anomaly tests: An exploratory video-observational study about client-midwife communication. Midwifery 2015, 31, 37–46. [Google Scholar] [CrossRef]
- Gitsels-van der Wal, J.T.; Martin, L.; Manniën, J.; Verhoeven, P.; Hutton, E.K.; Reinders, H.S. Antenatal counselling for congenital anomaly tests: Pregnant Muslim Moroccan women’s preferences. Midwifery 2015, 31, e50–e57. [Google Scholar] [CrossRef]
- Dixon, V.; Burton, N. Are midwifery clients in Ontario making informed choices about prenatal screening? Women Birth 2014, 27, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Dewell, S.; Benzies, K.; Ginn, C.; Seneviratne, C. Assessing knowledge of genomic concepts among Canadian nursing students and faculty. Int. J. Nurs. Educ. Sch. 2020, 17, 20200058. [Google Scholar] [CrossRef]
- Visser, A.; Bos, W.; Prins, J.B.; Hoogerbrugge, N.; van Laarhoven, H.W.M. Breast Self-examination Education for BRCA Mutation Carriers by Clinical Nurse Specialists. Clin. Nurse Spec. 2015, 29, E1–E7. [Google Scholar] [CrossRef]
- Reisinho, M.d.C.; Gomes, B.P.; Carvalho, F.; Borges, E. Caring for Adolescents with Cystic Fibrosis, in Portugal: The Nurse’s Role. Compr. Child Adolesc. Nurs. 2022, 45, 182–190. [Google Scholar] [CrossRef]
- Scott, N.; O’Sullivan, J.; Asgeirsson, K.; Macmillan, D.; Wilson, E. Changing practice: Moving to a specialist nurse-led service for BRCA gene testing. Br. J. Nurs. 2020, 29, S6–S13. [Google Scholar] [CrossRef]
- Martin, L.; Gitsels-van der Wal, J.T.; Pereboom, M.T.; Spelten, E.R.; Hutton, E.K.; van Dulmen, S. Clients’ psychosocial communication and midwives’ verbal and nonverbal communication during prenatal counseling for anomaly screening. Patient Educ. Couns. 2016, 99, 85–91. [Google Scholar] [CrossRef]
- Ingrand, I.; Defossez, G.; Richer, J.P.; Tougeron, D.; Palierne, N.; Letard, J.C.; Beauchant, M.; Ingrand, P. Colonoscopy uptake for high-risk individuals with a family history of colorectal neoplasia: A multicenter, randomized trial of tailored counseling versus standard information. Medicine 2016, 95, e4303. [Google Scholar] [CrossRef]
- van der Giessen, J.; Fransen, M.P.; Spreeuwenberg, P.; Velthuizen, M.; van Dulmen, S.; Ausems, M. Communication about breast cancer genetic counseling with patients with limited health literacy or a migrant background: Evaluation of a training program for healthcare professionals. J. Community Genet. 2021, 12, 91–99. [Google Scholar] [CrossRef]
- Gleeson, M.; Meiser, B.; Barlow-Stewart, K.; Trainer, A.H.; Tucker, K.; Watts, K.J.; Friedlander, M.; Kasparian, N. Communication and information needs of women diagnosed with ovarian cancer regarding treatment-focused genetic testing. Oncol. Nurs. Forum 2013, 40, 275–283. [Google Scholar] [CrossRef]
- Murakami, K.; Kutsunugi, S.; Tsujino, K.; Stone, T.E.; Ito, M.; Iida, K. Developing competencies in genetics nursing: Education intervention for perinatal and pediatric nurses. Nurs. Health Sci. 2020, 22, 263–272. [Google Scholar] [CrossRef]
- Burke, S.; Barker, C.; Marshall, D. Developing education tailored to clinical roles: Genetics education for haemophilia nurses. Nurse Educ. Today 2012, 32, 52–56. [Google Scholar] [CrossRef] [PubMed]
- Obayashi, C.; Asahara, K.; Umeda, M. Difficulties in providing genetic consultations by public health nurses in Japan. Public Health Nurs. 2022, 39, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- van der Giessen, J.A.M.; van Dulmen, S.; Velthuizen, M.E.; van den Muijsenbergh, M.; van Engelen, K.; Collée, M.; van Dalen, T.; Aalfs, C.M.; Hooning, M.J.; Spreeuwenberg, P.M.M.; et al. Effect of a health literacy training program for surgical oncologists and specialized nurses on disparities in referral to breast cancer genetic testing. Breast 2021, 58, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Lu, Y.; Liu, Z.; Diao, M.; Yang, L. Establishment and External Validation of a Hypoxia-Derived Gene Signature for Robustly Predicting Prognosis and Therapeutic Responses in Glioblastoma Multiforme. BioMed Res. Int. 2022, 2022, 7858477. [Google Scholar] [CrossRef] [PubMed]
- Kirk, M.; Simpson, A.; Llewellyn, M.; Tonkin, E.; Cohen, D.; Longley, M. Evaluating the role of Cardiac Genetics Nurses in inherited cardiac conditions services using a Maturity Matrix. Eur. J. Cardiovasc. Nurs. 2014, 13, 418–428. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, E.; Coughlan, M.; Corrigan, H.; McKee, G. Evaluation of a nurse-led haemophilia counselling service. Br. J. Nurs. 2012, 21, 864—866, 868. [Google Scholar] [CrossRef] [PubMed]
- Atienza-Carrasco, J.; Linares-Abad, M.; Padilla-Ruiz, M.; Morales-Gil, I.M. Experiences and outcomes following diagnosis of congenital foetal anomaly and medical termination of pregnancy: A phenomenological study. J. Clin. Nurs. 2020, 29, 1220–1237. [Google Scholar] [CrossRef] [PubMed]
- Gitsels-van der Wal, J.T.; Verhoeven, P.S.; Mannien, J.; Martin, L.; Reinders, H.S.; Spelten, E.; Hutton, E.K. Factors affecting the uptake of prenatal screening tests for congenital anomalies; a multicentre prospective cohort study. BMC Pregnancy Childbirth 2014, 14, 264. [Google Scholar] [CrossRef] [PubMed]
- Cooley, C.; Bishop, M. Family history taking at the booking clinic—Results from a pilot audit in the West Midlands. Br. J. Midwifery 2014, 22, 30–34. [Google Scholar] [CrossRef]
- McCarthy, M.C.; De Abreu Lourenco, R.; McMillan, L.J.; Meshcheriakova, E.; Cao, A.; Gillam, L. Finding Out What Matters in Decision-Making Related to Genomics and Personalized Medicine in Pediatric Oncology: Developing Attributes to Include in a Discrete Choice Experiment. Patient 2020, 13, 347–361. [Google Scholar] [CrossRef]
- Godino, L.; Turchetti, D.; Skirton, H. Genetic counseling: A survey to explore knowledge and attitudes of Italian nurses and midwives. Nurs. Health Sci. 2013, 15, 15–21. [Google Scholar] [CrossRef]
- Kawasaki, H.; Kawasaki, M.; Iki, T.; Matsuyama, R. Genetics education program to help public health nurses improve their knowledge and enhance communities’ genetic literacy: A pilot study. BMC Nurs. 2021, 20, 31. [Google Scholar] [CrossRef]
- Wright, H.; Zhao, L.; Birks, M.; Mills, J. Genomic Literacy of Registered Nurses and Midwives in Australia: A Cross-Sectional Survey. J. Nurs. Sch. 2019, 51, 40–49. [Google Scholar] [CrossRef]
- Byrjalsen, A.; Stoltze, U.K.; Castor, A.; Wahlberg, A. Germline whole genome sequencing in pediatric oncology in Denmark-Practitioner perspectives. Mol. Genet. Genom. Med. 2020, 8, e1276. [Google Scholar] [CrossRef]
- Meiser, B.; Gleeson, M.; Watts, K.; Peate, M.; Zilliacus, E.; Barlow-Stewart, K.; Saunders, C.; Mitchell, G.; Kirk, J. Getting to the point: What women newly diagnosed with breast cancer want to know about treatment-focused genetic testing. Oncol. Nurs. Forum 2012, 39, E101–E111. [Google Scholar] [CrossRef]
- Balelah, S.H.; Alawaji, O.M.; Alhejaili, N.S. Health Care Provider Attitude During the Management of Sickle Cell Disease Patients, a Multicenter Study in Saudi Arabia. Indo Am. J. Pharm. Sci. 2019, 6, 460–467. [Google Scholar] [CrossRef]
- Bracci, R.; Gasperini, B.; Capalbo, M.; Campanelli, T.; Caimmi, E.; Mattioli, R.; Espinosa, E.; Prospero, E. How to improve the identification of patients with cancer eligible for genetic counselling? Eur. J. Cancer Care 2020, 29, e13276. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekaran, D.; Sobocan, M.; Blyuss, O.; Miller, R.E.; Evans, O.; Crusz, S.M.; Mills-Baldock, T.; Sun, L.; Hammond, R.F.L.; Gaba, F.; et al. Implementation of Multigene Germline and Parallel Somatic Genetic Testing in Epithelial Ovarian Cancer: SIGNPOST Study. Cancers 2021, 13, 4344. [Google Scholar] [CrossRef] [PubMed]
- Morel, K.; Colclough, K.; Vaughan, N.; Shepherd, M. Improving awareness of monogenic diabetes through a specialist genetic diabetes nurse. J. Diabetes Nurs. 2013, 17, 250–254. [Google Scholar]
- Ingoe, L.; Potter, A.; Musson, S.; Neely, D.; Pilkington, G.; Allen, A.J.; Reay, D.; Luvai, A.; McAnulty, C.; Camm, N.; et al. Improving the identification of patients with a genetic diagnosis of familial hypercholesterolaemia in primary care: A strategy to achieve the NHS long term plan. Atherosclerosis 2021, 325, 38–45. [Google Scholar] [CrossRef]
- Laws, T.; Pelentsov, L.; Steen, M.; Esterman, A. Informing the midwife on rare genetic disorders and their effects on mothers breastfeeding—A mixed methods study. Evid. Based Midwifery 2016, 14, 11–15. [Google Scholar]
- Waddell-Smith, K.E.; Donoghue, T.; Oates, S.; Graham, A.; Crawford, J.; Stiles, M.K.; Aitken, A.; Skinner, J.R. Inpatient detection of cardiac-inherited disease: The impact of improving family history taking. Open Heart 2016, 3, e000329. [Google Scholar] [CrossRef]
- Dagan, E.; Amit, Y.; Sokolov, L.; Litvak, P.; Barnoy, S. Integrating Genomic Professional Skills Into Nursing Practice: Results From a Large Cohort of Israeli Nurses. J. Nurs. Sch. 2021, 53, 753–761. [Google Scholar] [CrossRef]
- Percival, N.; George, A.; Gyertson, J.; Hamill, M.; Fernandes, A.; Davies, E.; Rahman, N.; Banerjee, S. The integration of BRCA testing into oncology clinics. Br. J. Nurs. 2016, 25, 690–694. [Google Scholar] [CrossRef]
- Mor, S.; Lev-Rn, Z.; Tal, S. Is family history of coronary artery disease important in the emergency department triage? Int. Emerg. Nurs. 2020, 50, 100855. [Google Scholar] [CrossRef]
- Hébert, J.; Bergeron, A.S.; Veillette, A.M.; Bouchard, K.; Nabi, H.; Dorval, M. Issues associated with a hereditary risk of cancer: Knowledge, attitudes and practices of nurses in oncology settings. Can. Oncol. Nurs. J. 2022, 32, 272–285. [Google Scholar] [CrossRef] [PubMed]
- Gonthier, C.; Pelletier, S.; Gagnon, P.; Marin, A.; Chiquette, J.; Gagnon, B.; Roy, L.; Cléophat, J.E.; Joly, Y.; Dorval, M. Issues related to family history of cancer at the end of life: A palliative care providers’ survey. Fam. Cancer 2018, 17, 303–307. [Google Scholar] [CrossRef]
- Shin, G.; Jun, M.; Kim, H.K.; Wreen, M.; Kubsch, S.M. Key competencies for Korean nurses in prenatal genetic nursing: Experiential genetic nursing knowledge, and ethics and law. J. Educ. Eval. Health Prof. 2020, 17, 36. [Google Scholar] [CrossRef] [PubMed]
- Itzhaki, M. Knowledge and feelings about colorectal cancer among the Jewish adult population in Israel: A mixed methods study. Appl. Nurs. Res. 2018, 43, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Godino, L.; Turchetti, D.; Skirton, H. Knowledge of genetics and the role of the nurse in genetic health care: A survey of Italian nurses. J. Adv. Nurs. 2013, 69, 1125–1135. [Google Scholar] [CrossRef] [PubMed]
- Rahma, A.T.; Elsheik, M.; Ali, B.R.; Elbarazi, I.; Patrinos, G.P.; Ahmed, L.A.; Al Maskari, F. Knowledge, Attitudes, and Perceived Barriers toward Genetic Testing and Pharmacogenomics among Healthcare Workers in the United Arab Emirates: A Cross-Sectional Study. J. Pers. Med. 2020, 10, 216. [Google Scholar] [CrossRef]
- Nisselle, A.; Bishop, M.; Charles, T.; Morrissy, S.; King, E.; Metcalfe, S.; Gaff, C. Lessons learnt from implementing change in newborn bloodspot screening processes over more than a decade: Midwives, genetics and education. Midwifery 2019, 79, 102542. [Google Scholar] [CrossRef]
- Dearing, A.; Taverner, N. Mainstreaming genetics in palliative care: Barriers and suggestions for clinical genetic services. J. Community Genet. 2018, 9, 243–256. [Google Scholar] [CrossRef]
- Martin, L.; Hutton, E.K.; Spelten, E.R.; Gitsels-van der Wal, J.T.; van Dulmen, S. Midwives’ views on appropriate antenatal counselling for congenital anomaly tests: Do they match clients’ preferences? Midwifery 2014, 30, 600–609. [Google Scholar] [CrossRef]
- Wolters, W.P.G.; Dreijerink, K.M.A.; Giles, R.H.; van der Horst-Schrivers, A.N.A.; van Nesselrooij, B.; Zandee, W.T.; Timmers, H.; Seute, T.; de Herder, W.W.; Verrijn Stuart, A.A.; et al. Multidisciplinary integrated care pathway for von Hippel-Lindau disease. Cancer 2022, 128, 2871–2879. [Google Scholar] [CrossRef]
- Martin, L.; Gitsels-van der Wal, J.T.; Bax, C.J.; Pieters, M.J.; Reijerink-Verheij, J.; Galjaard, R.J.; Henneman, L.; Dutch, N.C. Nationwide implementation of the non-invasive prenatal test: Evaluation of a blended learning program for counselors. PLoS ONE 2022, 17, e0267865. [Google Scholar] [CrossRef] [PubMed]
- Carroll, J.C.; Hayeems, R.Z.; Miller, F.A.; Barg, C.J.; Bombard, Y.; Chakraborty, P.; Potter, B.K.; Bytautas, J.P.; Tam, K.; Taylor, L.; et al. Newborn screening for cystic fibrosis: Role of primary care providers in caring for infants with positive screening results. Can. Fam. Physician 2021, 67, e144–e152. [Google Scholar] [CrossRef] [PubMed]
- Berger-Höger, B.; Vitinius, F.; Fischer, H.; Beifus, K.; Köberlein-Neu, J.; Isselhard, A.; Töpper, M.; Wiedemann, R.; Rhiem, K.; Schmutzler, R.; et al. Nurse-led decision coaching by specialized nurses for healthy BRCA1/2 gene mutation carriers—Adaptation and pilot testing of a curriculum for nurses: A qualitative study. BMC Nurs. 2022, 21, 42. [Google Scholar] [CrossRef] [PubMed]
- Symonds, E.L.; Simpson, K.; Coats, M.; Chaplin, A.; Saxty, K.; Sandford, J.; Young, A.; Cock, C.; Fraser, R.; Bampton, P.A. A nurse-led model at public academic hospitals maintains high adherence to colorectal cancer surveillance guidelines. Med. J. Aust. 2018, 208, 492–496. [Google Scholar] [CrossRef]
- Kirk, M.; Morgan, R.; Tonkin, E.; McDonald, K.; Skirton, H. An objective approach to evaluating an internet-delivered genetics education resource developed for nurses: Using Google Analytics™ to monitor global visitor engagement. J. Res. Nurs. 2012, 17, 557–579. [Google Scholar] [CrossRef]
- van der Steen, S.L.; Houtman, D.; Bakkeren, I.M.; Galjaard, R.H.; Polak, M.G.; Busschbach, J.J.; Tibben, A.; Riedijk, S.R. Offering a choice between NIPT and invasive PND in prenatal genetic counseling: The impact of clinician characteristics on patients’ test uptake. Eur. J. Hum. Genet. 2019, 27, 235–243. [Google Scholar] [CrossRef]
- Goda, H.; Kawasaki, H.; Masuoka, Y.; Kohama, N.; Rahman, M.M. Opportunities and challenges of integrating genetics education about human diversity into public health nurses’ responsibilities in Japan. BMC Nurs. 2019, 18, 65. [Google Scholar] [CrossRef]
- Li, K.C.; Birch, P.H.; Garrett, B.M.; MacPhee, M.; Adam, S.; Friedman, J.M. Parents’ Perspectives on Supporting Their Decision Making in Genome-Wide Sequencing. J. Nurs. Sch. 2016, 48, 265–275. [Google Scholar] [CrossRef]
- Hsiao, C.Y.; Lee, S.H.; Chen, S.J.; Lin, S.C. Perceived knowledge and clinical comfort with genetics among Taiwanese nurses enrolled in a RN-to-BSN program. Nurse Educ. Today 2013, 33, 802–807. [Google Scholar] [CrossRef]
- Lee, T.Y.; Sung, L.W.; Hsu, S.S.; Liaw, J.J. A pilot study on genetic knowledge of maternity and pediatric nurses. J. Med. Sci. 2012, 32, 109–119. [Google Scholar]
- Reisinho, M.D.C.; Gomes, B. Portuguese adolescents with cystic fibrosis and their parents: An intervention proposal for nursing clinical practice. J. Pediatr. Nurs. 2022, 64, e130–e135. [Google Scholar] [CrossRef] [PubMed]
- Bokkers, K.; Zweemer, R.P.; Koudijs, M.J.; Stehouwer, S.; Velthuizen, M.E.; Bleiker, E.M.A.; Ausems, M. Positive experiences of healthcare professionals with a mainstreaming approach of germline genetic testing for women with ovarian cancer. Fam. Cancer 2022, 21, 295–304. [Google Scholar] [CrossRef] [PubMed]
- Cousens, N.E.; Gaff, C.L.; Delatycki, M.B.; Metcalfe, S.A. Prenatal β-thalassemia carrier screening in Australia: Healthcare professionals’ perspectives of clinical practice. Prenat. Diagn. 2014, 34, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Martin, L.; Van Dulmen, S.; Spelten, E.; De Jonge, A.; De Cock, P.; Hutton, E. Prenatal counseling for congenital anomaly tests: Parental preferences and perceptions of midwife performance. Prenat. Diagn. 2013, 33, 341–353. [Google Scholar] [CrossRef]
- Gitsels-van Der Wal, J.T.; Mannien, J.; Gitsels, L.A.; Reinders, H.S.; Verhoeven, P.S.; Ghaly, M.M.; Klomp, T.; Hutton, E.K. Prenatal screening for congenital anomalies: Exploring midwives’ perceptions of counseling clients with religious backgrounds. BMC Pregnancy Childbirth 2014, 14, 237. [Google Scholar] [CrossRef]
- St-Martin, G.; Bedard, A.; Nelmes, J.; Bedard, J.E. Preparing Nurses for Genetic Medicine: Integration of a Brief Education Session in an Undergraduate Nursing Curriculum. J. Nurs. Educ. 2017, 56, 170–173. [Google Scholar] [CrossRef]
- Hayeems, R.Z.; Miller, F.A.; Barg, C.J.; Bombard, Y.; Chakraborty, P.; Potter, B.K.; Patton, S.; Bytautas, J.P.; Tam, K.; Taylor, L.; et al. Primary care providers’ role in newborn screening result notification for cystic fibrosis. Can. Fam. Physician 2021, 67, 439–448. [Google Scholar] [CrossRef]
- Hayeems, R.Z.; Miller, F.A.; Carroll, J.C.; Little, J.; Allanson, J.; Bytautas, J.P.; Chakraborty, P.; Wilson, B.J. Primary care role in expanded newborn screening After the heel prick test. Can. Fam. Physician 2013, 59, 861–868. [Google Scholar]
- Mears, J.; Abubakar, I.; Crisp, D.; Maguire, H.; Innes, J.A.; Lilley, M.; Lord, J.; Cohen, T.; Borgdorff, M.W.; Vynnycky, E.; et al. Prospective evaluation of a complex public health intervention: Lessons from an initial and follow-up cross-sectional survey of the tuberculosis strain typing service in England. BMC Public Health 2014, 14, 1023. [Google Scholar] [CrossRef]
- Woodall, C.A.; Thornton, H.V.; Anderson, E.C.; Ingle, S.M.; Muir, P.; Vipond, B.; Longhurst, D.; Leeming, J.P.; Beck, C.R.; Hay, A.D. Prospective Study of the Performance of Parent-Collected Nasal and Saliva Swab Samples, Compared with Nurse-Collected Swab Samples, for the Molecular Detection of Respiratory Microorganisms. Microbiol. Spectr. 2021, 9, e0016421. [Google Scholar] [CrossRef]
- Qiu, J.; Guan, J.; Yang, X.; Wu, J.; Liu, G.; Di, G.; Chen, C.; Hou, Y.; Han, Q.; Shen, Z.; et al. Quality of Life and Psychological State in Chinese Breast Cancer Patients Who Received BRCA1/2 Genetic Testing. PLoS ONE 2016, 11, e0158531. [Google Scholar] [CrossRef] [PubMed]
- Gitsels-van der Wal, J.T.; Mannien, J.; Ghaly, M.M.; Verhoeven, P.S.; Hutton, E.K.; Reinders, H.S. The role of religion in decision-making on antenatal screening of congenital anomalies: A qualitative study amongst Muslim Turkish origin immigrants. Midwifery 2014, 30, 297–302. [Google Scholar] [CrossRef]
- Dunk, R.; Madge, S. SARS-CoV-2 driving rapid change in adult cystic fibrosis services: The role of the clinical nurse specialist. BMJ Open Qual. 2021, 10, e001427. [Google Scholar] [CrossRef] [PubMed]
- Saleh, M.; Kerr, R.; Dunlop, K. Scoping the Scene: What Do Nurses, Midwives, and Allied Health Professionals Need and Want to Know About Genomics? Front. Genet. 2019, 10, 1066. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, B.; George, E.; Horton, S.; Bellaby, J.; Min, S.S.; Gama, R. A service evaluation: Impact of nurse-led regional familial hypercholesterolaemia service on a hospital adult lipid clinic. Br. J. Nurs. 2020, 29, 1206–1208. [Google Scholar] [CrossRef]
- Kirk, M.; Tonkin, E.; Skirton, H.; McDonald, K.; Cope, B.; Morgan, R. Storytellers as partners in developing a genetics education resource for health professionals. Nurse Educ. Today 2013, 33, 518–524. [Google Scholar] [CrossRef]
- Oulton, K.; Gibson, F.; Williams, A.; Geoghegan, S.; Aldiss, S.; Wray, J. Supporting families of children with an undiagnosed genetic condition: Using co-design to ensure the right person is in the right post doing the right job. Child Care Health Dev. 2021, 47, 300–310. [Google Scholar] [CrossRef]
- van der Giessen, J.A.M.; Ausems, M.; van den Muijsenbergh, M.; van Dulmen, S.; Fransen, M.P. Systematic development of a training program for healthcare professionals to improve communication about breast cancer genetic counseling with low health literate patients. Fam. Cancer 2020, 19, 281–290. [Google Scholar] [CrossRef]
- Fallowfield, L.; Solis-Trapala, I.; Starkings, R.; May, S.; Matthews, L.; Eccles, D.; Evans, D.G.; Turnbull, C.; Crawford, G.; Jenkins, V. Talking about Risk, UncertaintieS of Testing IN Genetics (TRUSTING): Development and evaluation of an educational programme for healthcare professionals about BRCA1 & BRCA2 testing. Br. J. Cancer 2022, 127, 1116–1122. [Google Scholar]
- Shepherd, M.; Colclough, K.; Ellard, S.; Hattersley, A.T. Ten years of the national genetic diabetes nurse network: A model for the translation of genetic information into clinical care. Clin. Med. 2014, 14, 117–121. [Google Scholar] [CrossRef]
- Platten, U.; Rantala, J.; Lindblom, A.; Brandberg, Y.; Lindgren, G.; Arver, B. The use of telephone in genetic counseling versus in-person counseling: A randomized study on counselees’ outcome. Fam. Cancer 2012, 11, 371–379. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Andrews, V.; Tonkin, E.; Lancastle, D.; Kirk, M. Using the Diffusion of Innovations theory to understand the uptake of genetics in nursing practice: Identifying the characteristics of genetic nurse adopters. J. Adv. Nurs. 2014, 70, 878–893. [Google Scholar] [CrossRef] [PubMed]
- Williams, G.M.; Neville, P.; Gillespie, K.M.; Leary, S.D.; Hamilton-Shield, J.P.; Searle, A.J. What factors influence recruitment to a birth cohort of infants with Down’s syndrome? Arch. Dis. Child 2018, 103, 763–766. [Google Scholar] [CrossRef]
- Hickey, M.; Rio, I.; Trainer, A.; Marino, J.L.; Wrede, C.D.; Peate, M. What information do healthcare professionals need to inform premenopausal women about risk-reducing salpingo-oophorectomy? Menopause 2020, 27, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Young, A.L.; Butow, P.N.; Tucker, K.M.; Wakefield, C.E.; Healey, E.; Williams, R. When to break the news and whose responsibility is it? A cross-sectional qualitative study of health professionals’ views regarding disclosure of BRCA genetic cancer risk. BMJ Open 2020, 10, e033127. [Google Scholar] [CrossRef]
- Dodd, S.; Clarke, M.; Becker, L.; Mavergames, C.; Fish, R.; Williamson, P.R. A taxonomy has been developed for outcomes in medical research to help improve knowledge discovery. J. Clin. Epidemiol. 2018, 96, 84–92. [Google Scholar] [CrossRef]
- Haidar, H.; Vanstone, M.; Laberge, A.M.; Bibeau, G.; Ghulmiyyah, L.; Ravitsky, V. Implementation challenges for an ethical introduction of noninvasive prenatal testing: A qualitative study of healthcare professionals’ views from Lebanon and Quebec. BMC Med. Ethics 2020, 21, 15. [Google Scholar] [CrossRef]
- Quinonez, S.C.; O’Connor, B.C.; Jacobs, M.F.; Mekonnen Tekleab, A.; Marye, A.; Bekele, D.; Yashar, B.M.; Hanson, E.; Yeshidinber, A.; Wedaje, G. The introduction of genetic counseling in Ethiopia: Results of a training workshop and lessons learned. PLoS ONE 2021, 16, e0255278. [Google Scholar] [CrossRef]
- Asafa, K.; Ndikom, C.; Adelanwa, A. Midwives’ Knowledge and Readiness to Practice Antenatal Screening and Genetic Testing in selected Hospitals in Lagos, Nigeria. J. Midwifery Reprod. Health 2021, 9, 3007–3016. [Google Scholar] [CrossRef]
- Kudzi, W.; Addy, B.S.; Dzudzor, B. Knowledge of Pharmacogenetics among Healthcare Professionals and Faculty Members of Health Training Institutions in Ghana. Ghana Med. J. 2015, 49, 50–56. [Google Scholar] [CrossRef]
- Jackson, L.; O’Connor, A.; Paneque, M.; Curtisova, V.; Lunt, P.W.; Pourova, R.K.; Macek, M.; Stefansdottir, V.; Turchetti, D.; Campos, M.; et al. The Gen-Equip Project: Evaluation and impact of genetics e-learning resources for primary care in six European languages. Genet. Med. 2019, 21, 718–726. [Google Scholar] [CrossRef]
- Nembaware, V.; Mulder, N. The African Genomic Medicine Training Initiative (AGMT): Showcasing a Community and Framework Driven Genomic Medicine Training for Nurses in Africa. Front. Genet. 2019, 10, 1209. [Google Scholar] [CrossRef]
- Hickey, K.T.; Taylor, J.Y.; Barr, T.L.; Hauser, N.R.; Jia, H.; Riga, T.C.; Katapodi, M. Nursing genetics and genomics: The International Society of Nurses in Genetics (ISONG) survey. Nurse Educ. Today 2018, 63, 12–17. [Google Scholar] [CrossRef]
- Seven, M.; Pasalak, S.I.; Guvenc, G.; Kok, G. Knowledge Level and Educational Needs of Turkish Oncology Nurses Regarding the Genetics of Hereditary Breast and Ovarian Cancer. J. Contin. Educ. Nurs. 2017, 48, 570–576. [Google Scholar] [CrossRef]
- Seven, M.; Akyüz, A.; Elbüken, B.; Skirton, H.; Öztürk, H. Nurses’ knowledge and educational needs regarding genetics. Nurse Educ. Today 2015, 35, 444–449. [Google Scholar] [CrossRef]
- Lopes-Júnior, L.C.; Carvalho Júnior, P.M.; de Faria Ferraz, V.E.; Nascimento, L.C.; Van Riper, M.; Flória-Santos, M. Genetic education, knowledge and experiences between nurses and physicians in primary care in Brazil: A cross-sectional study. Nurs. Health Sci. 2017, 19, 66–74. [Google Scholar] [CrossRef]
- Seven, M.; Eroglu, K.; Akyüz, A.; Ingvoldstad, C. Educational needs of nurses to provide genetic services in prenatal care: A cross-sectional study from Turkey. Nurs. Health Sci. 2017, 19, 294–300. [Google Scholar] [CrossRef] [PubMed]
- Cofie, R.; Sarfo, J.O.; Doe, P. Teaching and Learning of Genetics Using Concept Maps: An Experimental Study Among Midwifery Students in Ghana. Eur. J. Contemp. Educ. 2021, 10, 29–34. [Google Scholar] [CrossRef]
- Burcher, S.; Meiser, B.; Mitchell, G.; Saunders, C.; Rahman, B.; Tucker, K.; Barlow-Stewart, K.; Watts, K.; Gleeson, M.; Kirk, J. Oncology health professionals’ attitudes toward treatment-focused genetic testing for women newly diagnosed with breast cancer. Per. Med. 2013, 10, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Prolla, C.M.; da Silva, P.S.; Netto, C.B.; Goldim, J.R.; Ashton-Prolla, P. Knowledge about breast cancer and hereditary breast cancer among nurses in a public hospital. Rev. Lat. Am. Enferm. 2015, 23, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Nunes, M.R.; Canabarro, S.T.; Vanz, A.P.; Rosa, R.F.M.; Zen, P.R.G. Nursing diagnoses in Turner syndrome. Mundo Saude 2021, 45, 66–74. [Google Scholar] [CrossRef]
- Yacoub, M.I.; Zaiton, H.I.; Abdelghani, F.A.; Elshatarat, R.A. Effectiveness of an Educational Program on Nurses’ Knowledge and Practice in the Management of Acute Painful Crises in Sickle Cell Disease. J. Contin. Educ. Nurs. 2019, 50, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Melo, D.G.; de Paula, P.K.; de Araujo Rodrigues, S.; da Silva de Avó, L.R.; Germano, C.M.; Demarzo, M.M. Genetics in primary health care and the National Policy on Comprehensive Care for People with Rare Diseases in Brazil: Opportunities and challenges for professional education. J. Community Genet. 2015, 6, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Ngim, C.F.; Lai, N.M.; Ibrahim, H. Counseling for prenatal diagnosis and termination of pregnancy due to thalassemia major: A survey of health care workers’ practices in Malaysia. Prenat. Diagn. 2013, 33, 1226–1232. [Google Scholar] [CrossRef]
- Chudleigh, J.; Ren, C.L.; Barben, J.; Southern, K. International approaches for delivery of positive newborn bloodspot screening results for cystic fibrosis. J. Cyst. Fibros. 2018, 17, S18. [Google Scholar] [CrossRef]
- Aboagye, S.; Torto, M.; Asah-Opoku, K.; Nuamah, M.A.; Oppong, S.A.; Samba, A. Sickle Cell Education: A Survey of Antenatal Healthcare Givers. Am. J. Trop. Med. Hyg. 2019, 101, 684–688. [Google Scholar] [CrossRef]
- Plavskin, A.; Samuels, W.E.; Calzone, K.A. Construct Validity Analysis of the Genetics and Genomics in Nursing Practice Survey: Overcoming Challenges in Variable Response Instruments. J. Nurs. Meas. 2023, 31, 259–272. [Google Scholar] [CrossRef]
- Tonkin, E.; Calzone, K.A.; Badzek, L.; Benjamin, C.; Middleton, A.; Patch, C.; Kirk, M. A Maturity Matrix for Nurse Leaders to Facilitate and Benchmark Progress in Genomic Healthcare Policy, Infrastructure, Education, and Delivery. J. Nurs. Sch. 2020, 52, 583–592. [Google Scholar] [CrossRef]
- Read, C.Y.; Ward, L.D. Misconceptions About Genomics Among Nursing Faculty and Students. Nurse Educ. 2018, 43, 196–200. [Google Scholar] [CrossRef]
- Dwyer, A.A.; Calzone, K.A.; Dewell, S.; Badzek, L.; Patch, C. Correspondence on “Ensuring best practice in genomics education and evaluation: Reporting item standards for education and its evaluation in genomics (RISE2 Genomics)” by Nisselle et al. Genet. Med. 2022, 24, 962–963. [Google Scholar] [CrossRef]
- Nisselle, A.; Janinski, M.; Martyn, M.; McClaren, B.; Kaunein, N.; Barlow-Stewart, K.; Belcher, A.; Bernat, J.A.; Best, S.; Bishop, M.; et al. Ensuring best practice in genomics education and evaluation: Reporting item standards for education and its evaluation in genomics (RISE2 Genomics). Genet. Med. 2021, 23, 1356–1365. [Google Scholar] [CrossRef] [PubMed]
- Kirk, M.; Tonkin, E.; Skirton, H. An iterative consensus-building approach to revising a genetics/genomics competency framework for nurse education in the UK. J. Adv. Nurs. 2014, 70, 405–420. [Google Scholar] [CrossRef] [PubMed]
- Skirton, H.; Lewis, C.; Kent, A.; Coviello, D.A. Genetic education and the challenge of genomic medicine: Development of core competences to support preparation of health professionals in Europe. Eur. J. Hum. Genet. 2010, 18, 972–977. [Google Scholar] [CrossRef] [PubMed]
- National Academies of Sciences, Engineering, and Medicine. Understanding Disparities in Access to Genomic Medicine: Proceedings of a Workshop; National Academies Press: Washington, DC, USA, 2018. [Google Scholar]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thomas, J.; Keels, J.; Calzone, K.A.; Badzek, L.; Dewell, S.; Patch, C.; Tonkin, E.T.; Dwyer, A.A. Current State of Genomics in Nursing: A Scoping Review of Healthcare Provider Oriented (Clinical and Educational) Outcomes (2012–2022). Genes 2023, 14, 2013. https://doi.org/10.3390/genes14112013
Thomas J, Keels J, Calzone KA, Badzek L, Dewell S, Patch C, Tonkin ET, Dwyer AA. Current State of Genomics in Nursing: A Scoping Review of Healthcare Provider Oriented (Clinical and Educational) Outcomes (2012–2022). Genes. 2023; 14(11):2013. https://doi.org/10.3390/genes14112013
Chicago/Turabian StyleThomas, Joanne, Jordan Keels, Kathleen A. Calzone, Laurie Badzek, Sarah Dewell, Christine Patch, Emma T. Tonkin, and Andrew A. Dwyer. 2023. "Current State of Genomics in Nursing: A Scoping Review of Healthcare Provider Oriented (Clinical and Educational) Outcomes (2012–2022)" Genes 14, no. 11: 2013. https://doi.org/10.3390/genes14112013
APA StyleThomas, J., Keels, J., Calzone, K. A., Badzek, L., Dewell, S., Patch, C., Tonkin, E. T., & Dwyer, A. A. (2023). Current State of Genomics in Nursing: A Scoping Review of Healthcare Provider Oriented (Clinical and Educational) Outcomes (2012–2022). Genes, 14(11), 2013. https://doi.org/10.3390/genes14112013