
Microbiological Evaluation and Sperm DNA Fragmentation in Semen Samples of Patients Undergoing Fertility Investigation


 , ,
, ,  and
and
Abstract
1. Introduction
2. Material and Methods
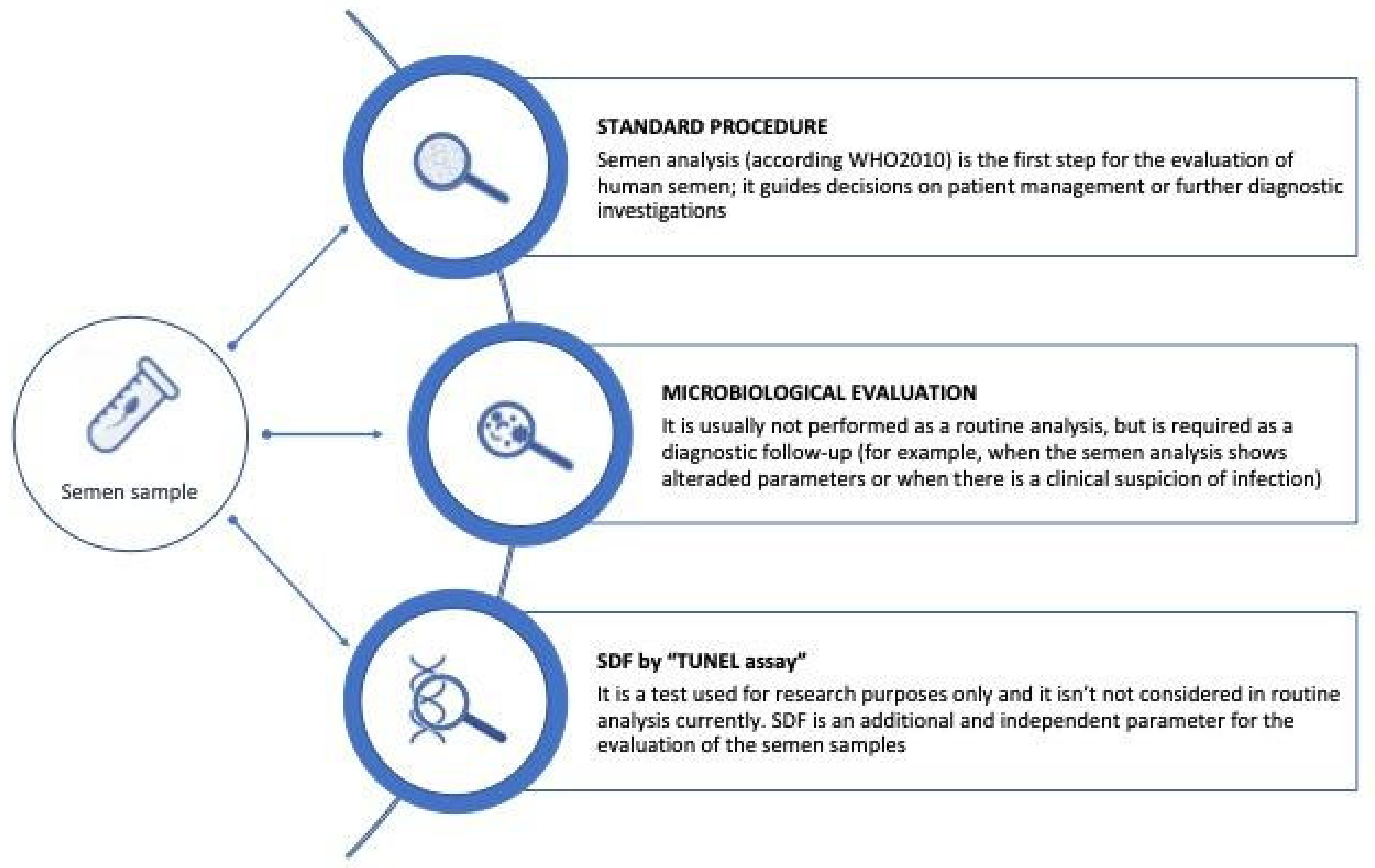
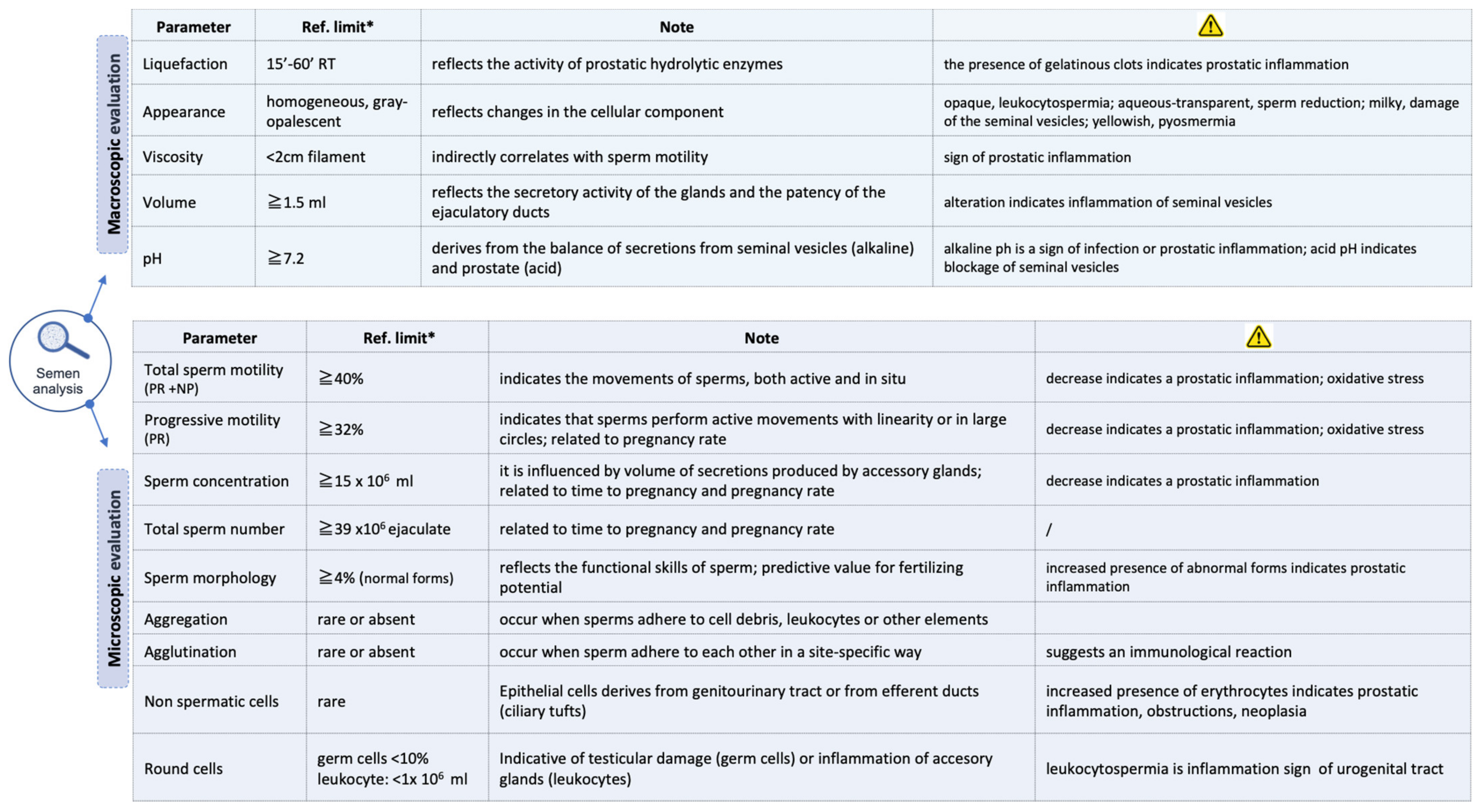
2.1. Semen Samples Collection
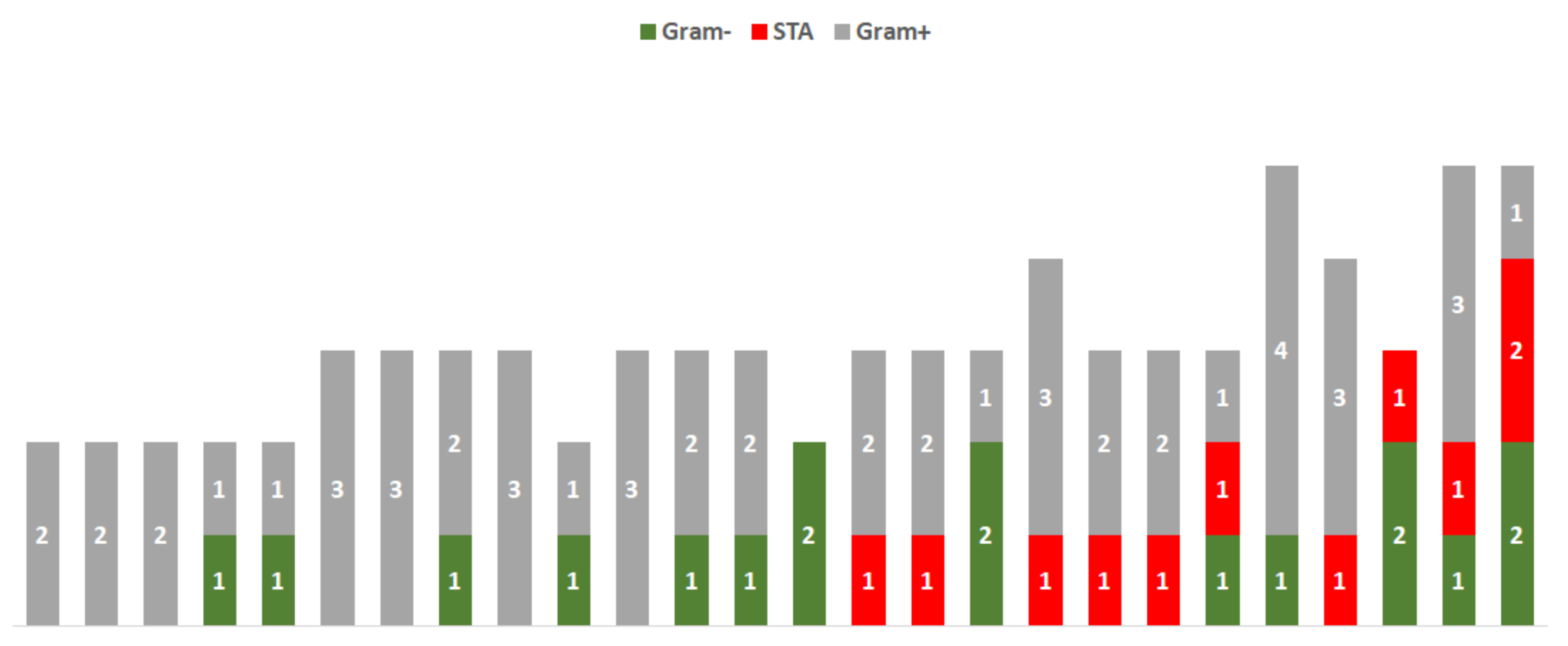
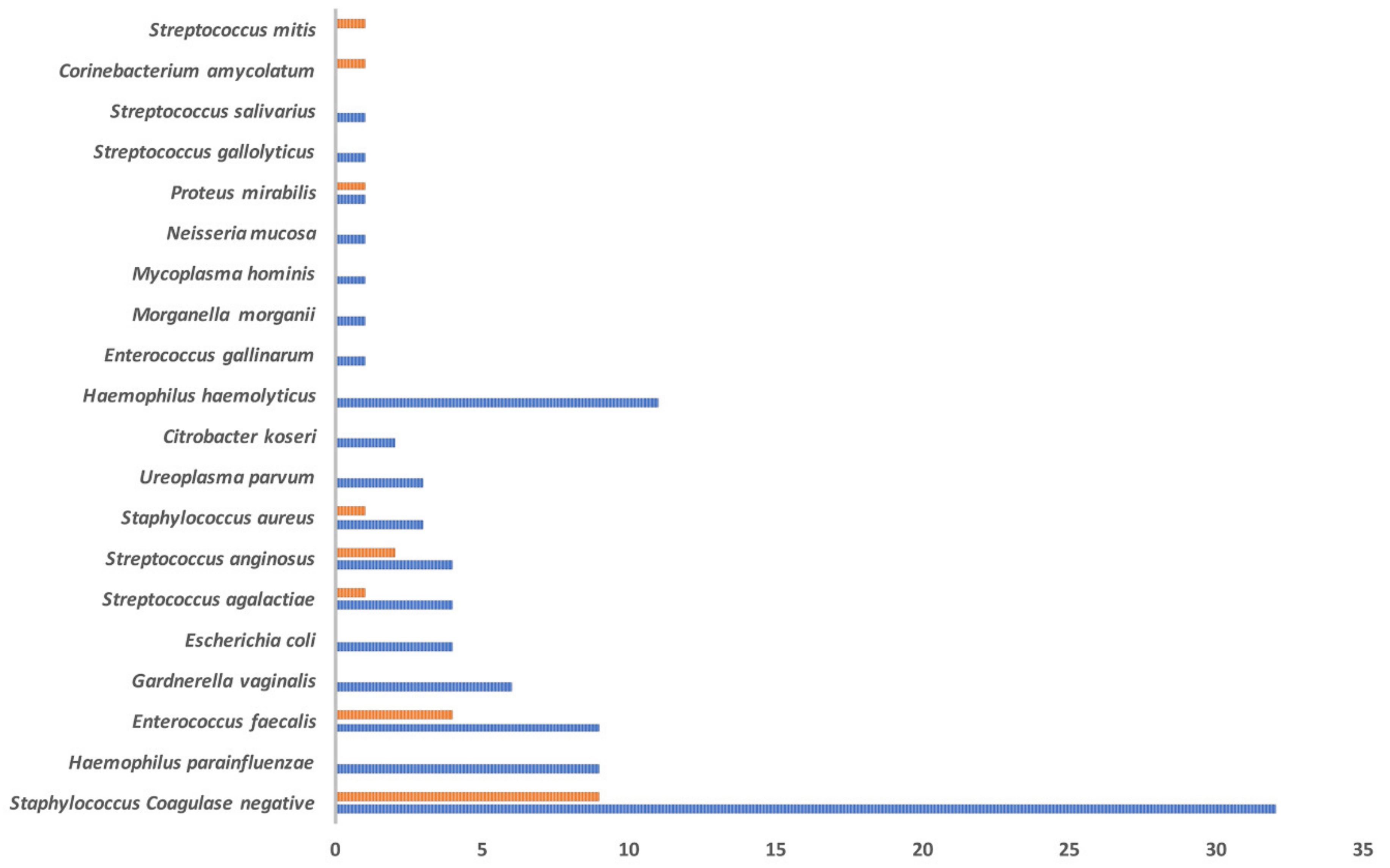
2.2. Microbiological Evaluation
2.3. Sperm DNA Fragmentation Analysis
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| OAT | oligo-astheno-teratozoospermia |
| Ct | cycle threshold |
| FITC | -dUTP fluorescein isothiocyanate-2′-deoxyuridine-5-triphosphate |
| IL | interleukin |
| ICSI | intracytoplasmic sperm injection |
| IVF | in vitro fertilization |
| NP | non-progressive |
| PBS | phosphate-buffered saline |
| PI | propidium iodide |
| PR | rapid progressive |
| ROS | reactive oxygen species |
| %SDF | percentage of sperm DNA fragmentation |
| SDF | sperm DNA fragmentation |
| STA | sexually transmitted agents |
| STI | sexually transmitted infection |
| TNF-α | tumor necrosis factor-α |
References
- Agarwal, A.; Parekh, N.; Panner Selvam, M.K.; Henkel, R.; Shah, R.; Homa, S.T.; Ramasamy, R.; Ko, E.; Tremellen, K.; Esteves, S.; et al. Male Oxidative Stress Infertility (MOSI): Proposed Terminology and Clinical Practice Guidelines for Management of Idiopathic Male Infertility. World J. Men’s Health 2019, 37, 296–312. [Google Scholar] [CrossRef] [PubMed]
- Krausz, C. Male infertility: Pathogenesis and clinical diagnosis. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 271–285. [Google Scholar] [CrossRef]
- Cariati, F.; D’Argenio, V.; Tomaiuolo, R. The evolving role of genetic tests in reproductive medicine. J. Transl. Med. 2019, 17, 267. [Google Scholar] [CrossRef] [PubMed]
- Cariati, F.; D’Uonno, N.; Borrillo, F.; Iervolino, S.; Galdiero, G.; Tomaiuolo, R. Bisphenol a: An emerging threat to male fertility. Reprod. Biol. Endocrinol. 2019, 17, 6. [Google Scholar] [CrossRef]
- Tomaiuolo, R.; Veneruso, I.; Cariati, F.; D’Argenio, V. Microbiota and Human reproduction: The case of male infertility. High Throughput 2020, 9, 10. [Google Scholar] [CrossRef]
- World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen, 5th ed.; WHO Press: Geneva, Switzerland, 2010; Available online: https://apps.who.int/iris/handle/10665/44261 (accessed on 15 January 2021).
- Vicari, E.; Calogero, A.E.; Condorelli, R.A.; Vicari, L.O.; La Vignera, S. Male accessory gland infection frequency in infertile patients with chronic microbial prostatitis and irritable bowel syndrome: Transrectal ultrasound examination helps to understand the links. J. Androl. 2012, 33, 404–411. [Google Scholar] [CrossRef]
- Pellati, D.; Mylonakis, I.; Bertoloni, G.; Fiore, C.; Andrisani, A.; Ambrosini, G.; Armanini, D. Genital tract infections and infertility. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 140, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Solomon, M.; Henkel, R. Semen culture and the assessment of genitourinary tract infections. Indian J. Urol. 2017, 33, 188–193. [Google Scholar]
- Nieschlag, E.; Behre, H. Andrology: Male Reproductive Health and Dysfunction; Springer: Berlin, Germany, 1997. [Google Scholar]
- Bayasgalan, G.; Naranbat, D.; Tsedmaa, B.; Tsogmaa, B.; Sukhee, D.; Amarjargal, O.; Lhagvasuren, T.; Radnaabazar, J.; Rowe, P.J. Clinical patterns and major causes of infertility in Mongolia. J. Obstet. Gynaecol. Res. 2004, 30, 386–393. [Google Scholar] [CrossRef]
- Sellami, H.; Znazen, A.; Sellami, A.; Mnif, H.; Louati, N.; Zarrouk, S.B.; Keskes, L.; Rebai, T.; Gdoura, R.; Hammami, A. Molecular detection of Chlamydia trachomatis and other sexually transmitted bacteria in semen of male partners of infertile couples in Tunisia: The effect on semen parameters and spermatozoa apoptosis markers. PLoS ONE 2014, 9, e98903. [Google Scholar] [CrossRef]
- Moazenchi, M.; Totonchi, M.; Salman Yazdi, R.; Hratian, K.; Mohseni Meybodi, M.A.; Ahmadi Panah, M.; Chehrazi, M.; Mohseni Meybodi, A. The impact of Chlamydia trachomatis infection on sperm parameters and male fertility: A comprehensive study. Int. J. STD AIDS 2018, 29, 466–473. [Google Scholar] [CrossRef]
- Sergerie, M.; Laforest, G.; Bujan, L.; Bissonnette, F.; Bleau, G. Sperm DNA fragmentation: Threshold value in male fertility. Hum. Reprod. 2005, 20, 3446–3451. [Google Scholar] [CrossRef]
- Osman, A.; Alsomait, H.; Seshadri, S.; El-Toukhy, T.; Khalaf, Y. The effect of sperm DNA fragmentation on live birth rate after IVF or ICSI: A systematic review and meta-analysis. Reprod. Biomed. Online 2015, 30, 120–127. [Google Scholar] [CrossRef]
- Simon, L.; Zini, A.; Dyachenko, A. A systematic review and meta-analysis to determine the effect of sperm DNA damage on in vitro fertilization and intracytoplasmic sperm injection outcome. Asian J. Androl. 2017, 19, 80–90. [Google Scholar]
- Evenson, D.P.; Wixon, R. Data analysis of two in vivo fertility studies using Sperm Chromatin Structure Assay-derived DNA fragmentation index vs. pregnancy outcome. Fertil. Steril. 2008, 90, 1229–1231. [Google Scholar] [CrossRef] [PubMed]
- Cicatiello, A.G.; Iula, D.V.; Pagliuca, C.; Pastore, G.; Pagliarulo, C.; Catania, M.R.; Colicchio, R.; Picardi, M.; Raia, V.; Salvatore, P. Identification of Inquilinus limosus in cystic fibrosis: A first report in Italy. N. Microbiol. 2014, 37, 567–571. [Google Scholar]
- La Vignera, S.; Condorelli, R.A.; Vicari, E.; Salmeri, M.; Morgia, G.; Favilla, V.; Cimino, S.; Calogero, A.E. Microbiological investigation in male infertility: A practical overview. J. Med. Microbiol. 2014, 63 Pt 1, 1–14. [Google Scholar] [CrossRef]
- Ochsendorf, F.R. Sexually transmitted infections: Impact on male fertility. Andrologia 2008, 40, 72–75. [Google Scholar] [CrossRef] [PubMed]
- Grande, G.; Milardi, D.; Baroni, S.; Luca, G.; Pontecorvi, A. Identification of seminal markers of male accessory gland inflammation: From molecules to proteome. Am. J. Reprod. Immunol. 2018, 80, e12992. [Google Scholar] [CrossRef] [PubMed]
- Barroso, G.; Morshedi, M.; Oehninger, S. Analysis of DNA fragmentation, plasma membrane translocation of phosphatidyl- serine and oxidative stress in human spermatozoa. Hum. Reprod. 2000, 15, 1338–1344. [Google Scholar] [CrossRef] [PubMed]
- Aitken, R.J.; De Iuliis, G.N. On the possible origins of DNA damage in human spermatozoa. Mol. Hum. Reprod. 2010, 16, 3–13. [Google Scholar] [CrossRef]
- Sakkas, D.; Alvarez, J.G. Sperm DNA fragmentation: Mechanisms of origin, impact on reproductive outcome, and analysis. Fertil. Steril. 2010, 93, 1027–1036. [Google Scholar] [CrossRef] [PubMed]
- La Vignera, S. Male accessory gland infections: Anatomical extension of inflammation and severity of symptoms evaluated by an original questionnaire. Andrologia 2012, 44 (Suppl. 1), 739–746. [Google Scholar] [CrossRef]
- La Vignera, S.; Vicari, E.; Condorelli, R.; D’Agata, R.; Calogero, A.E. Hypertrophic-congestive and fibro-sclerotic ultrasound variants of male accessory gland infection have different sperm output. J. Endocrinol. Investig. 2011, 34, 330–335. [Google Scholar] [CrossRef]
- Lanzafame, F.M.; La Vignera, S.; Vicari, E.; Calogero, A.E. Oxidative stress and medical antioxidant treatment in male infertility. Reprod. Biomed. Online 2009, 19, 638–659. [Google Scholar] [CrossRef] [PubMed]
- Ollero, M.; Gil-Guzman, E.; Lopez, M.C.; Sharma, R.K.; Agarwal, A.; Larson, K.; Evenson, D.; Thomas, A.J., Jr.; Alvarez, J.G. Characterization of subsets of human spermatozoa at different stages of maturation: Implications in the diagnosis and treatment of male infertility. Hum. Reprod. 2001, 16, 1912–1921. [Google Scholar] [CrossRef]
- Erenpreiss, J.; Hlevicka, S.; Zalkalns, J.; Erenpreisa, J. Effect of leukocytospermia on sperm DNA integrity: A negative effect in abnormal semen samples. J. Androl. 2002, 23, 717–723. [Google Scholar] [PubMed]
- Fraczek, M.; Kurpisz, M. Mechanisms of the harmful effects of bacterial semen infection on ejaculated human spermatozoa: Potential inflammatory markers in semen. Folia Histochem. Cytobiol. 2015, 53, 201–217. [Google Scholar] [CrossRef] [PubMed]
- Fujita, Y.; Mihara, T.; Okazaki, T.; Shitanaka, M.; Kushino, R.; Ikeda, C.; Negishi, H.; Liu, Z.; Richards, J.S.; Shimada, M. Toll-like receptors (TLR) 2 and 4 on human sperm recognize bacterial endotoxins and mediate apoptosis. Hum. Reprod. 2011, 26, 2799–2806. [Google Scholar] [CrossRef]
- Schuppe, H.C.; Meinhardt, A.; Allam, J.P.; Bergmann, M.; Weidner, W.; Haidl, G. Chronic orchitis: A neglected cause of male infertility? Andrologia 2008, 40, 84–91. [Google Scholar] [CrossRef]
- Perdichizzi, A.; Nicoletti, F.; La Vignera, S.; Barone, N.; D’Agata, R.; Vicari, E.; Calogero, A.E. Effects of tumour necrosis factor-alpha on human sperm motility and apoptosis. J. Clin. Immunol. 2007, 27, 152–162. [Google Scholar] [CrossRef]
- Farsimadan, M.; Motamedifar, M. Bacterial infection of the male reproductive system causing infertility. J. Reprod. Immunol. 2020, 142, 103183. [Google Scholar] [CrossRef] [PubMed]
- Korrovits, P.; Ausmees, K.; Mändar, R.; Punab, M. Prevalence of asymptomatic inflammatory (National Institutes of Health Category IV) prostatitis in young men according to semen analysis. Urology 2008, 71, 1010–1015. [Google Scholar] [CrossRef] [PubMed]
- La Vignera, S.; Condorelli, R.A.; Vicari, E.; Tumino, D.; Morgia, G.; Favilla, V.; Cimino, S.; Calogero, A.E. Markers of semen inflammation: Supplementary semen analysis? J. Reprod. Immunol. 2013, 100, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Irvine, D.S.; Twigg, J.P.; Gordon, E.L.; Fulton, N.; Milne, P.A.; Aitken, R.J. DNA integrity in human spermatozoa: Relationships with semen quality. J. Androl. 2000, 21, 33–44. [Google Scholar]
- Lopes, S.; Sun, J.G.; Jurisicova, A.; Meriano, J.; Casper, R.F. Sperm deoxyribonucleic acid fragmentation is increased in poor-quality semen samples and correlates with failed fertilization in intra- cytoplasmic sperm injection. Fertil. Steril. 1998, 69, 528–532. [Google Scholar] [CrossRef]
- Muratori, M.; Piomboni, P.; Baldi, E.; Filimberti, E.; Pecchioli, P.; Moretti, E.; Gambera, L.; Baccetti, B.; Biagiotti, R.; Forti, G.; et al. Functional and ultrastructural features of DNA- fragmented human sperm. J. Androl. 2000, 21, 903–912. [Google Scholar] [PubMed]
- Agarwal, A.; Allamaneni, S.S. Sperm DNA damage assessment: A test whose time has come. Fertil. Steril. 2005, 84, 850–853. [Google Scholar] [CrossRef]
- Miller, D.; Vukina, J. Recent advances in clinical diagnosis and treatment of male factor infertility. Postgrad. Med. 2020, 132 (Suppl. 4), 28–34. [Google Scholar] [CrossRef]
- Cissen, M.; Wely, M.V.; Scholten, I.; Mansell, S.; Bruin, J.P.; Mol, B.W.; Braat, D.; Repping, S.; Hamer, G. Measuring Sperm DNA Fragmentation and Clinical Outcomes of Medically Assisted Reproduction: A Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0165125. [Google Scholar] [CrossRef]
- Simon, L.; Castillo, J.; Oliva, R.; Lewis, S.E. Relationships between human sperm protamines, DNA damage and assisted reproduction outcomes. Reprod. Biomed. Online 2011, 23, 724–734. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wang, L.; Cai, J.; Huang, H. Correlation of sperm DNA damage with IVF and ICSI outcomes: A systematic review and meta-analysis. J. Assist. Reprod. Genet. 2006, 23, 367–376. [Google Scholar] [CrossRef]
- Evenson, D.P. Evaluation of sperm chromatin structure and DNA strand breaks is an important part of clinical male fertility assessment. Transl. Androl. Urol. 2017, 6 (Suppl. 4), S495–S500. [Google Scholar] [CrossRef]
- Štšepetova, J.; Baranova, J.; Simm, J.; Parm, Ü.; Rööp, T.; Sokmann, S.; Korrovits, P.; Jaagura, M.; Rosenstein, K.; Salumets, A.; et al. The complex microbiome from native semen to embryo culture environment in human in vitro fertilization procedure. Reprod. Biol. Endocrinol. 2020, 18, 1–13. [Google Scholar] [CrossRef]
- Cariati, F.; Savarese, M.; D’Argenio, V.; Salvatore, F.; Tomaiuolo, R. The SEeMORE strategy: Single-tube electrophoresis analysis-based genotyping to detect monogenic diseases rapidly and effectively from conception until birth. Clin. Chem. Lab. Med. 2017, 56, 40–50. [Google Scholar] [CrossRef] [PubMed]
- D’Argenio, V.; Nunziato, M.; D’Uonno, N. Indicazioni e limiti della diagnosi genetica preimpianto. Bioch. Clinic. 2017, 4, 314–321. [Google Scholar]
- Rusz, A.; Pilatz, A.; Wagenlehner, F.; Linn, T.; Diemer, T.; Schuppe, H.C.; Lohmeyer, J.; Hossain, H.; Weidner, W. Influence of urogenital infections and inflammation on semen quality and male fertility. World J. Urol. 2011, 30, 23–30. [Google Scholar] [CrossRef] [PubMed]
- Simon, L.; Emery, B.; Carrell, D.T. Sperm DNA Fragmentation: Consequences for Reproduction. Adv. Exp. Med. Biol. 2019, 1166, 87–105. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Correlation Coefficient | p-Value |
|---|---|---|
| pH | 0.046 | 0.790 |
| Volume | −0.346 | 0.038 * |
| Conc (×106 mL) | −0.223 | 0.192 |
| Conc/tot | −0.404 | 0.014 * |
| Motility PR + NP (%) | −0.460 | 0.005 ** |
| Motility PR (%) | −0.437 | 0.008 ** |
| Leucocytes (1 × 106/mL) | 0.185 | 0.280 |
| Normal forms (%) | −0.258 | 0.135 |
| %SDF Levels | Person’s Chi Squared | p-Value | OR (95%CI) |
|---|---|---|---|
| ≥30 | 0.020 | 0.029 | 5.95 (1.18–29.96) |
| <30–≥15 | 1.926 | 0.165 | 0.40 (0.11–1.49) |
| ≤15–>5 | 1.300 | 0.254 | 0.50 (0.15–1.66) |
| Test Group | Control Group | |||
|---|---|---|---|---|
| Parameters | SDF Tunel | p-Value | SDF Tunel | p-Value |
| pH | −0.362 | 0.028 * | −0.067 | 0.806 |
| Volume | 0.228 | 0.174 | −0.005 | 0.987 |
| Conc (×106 mL) | 0.031 | 0.857 | −0.277 | 0.298 |
| Conc/tot | 0.114 | 0.501 | 0.083 | 0.761 |
| Motility PR + NP (%) | −0.336 | 0.042 * | 0.272 | 0.309 |
| Motility PR (%) | −0.346 | 0.036 * | 0.322 | 0.224 |
| Leucocytes (1 × 106/mL) | −0.037 | 0.827 | −0.214 | 0.426 |
| Normal forms (%) | −0.190 | 0.268 | −0.177 | 0.512 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pagliuca, C.; Cariati, F.; Bagnulo, F.; Scaglione, E.; Carotenuto, C.; Farina, F.; D’Argenio, V.; Carraturo, F.; D’Aprile, P.; Vitiello, M.; et al. Microbiological Evaluation and Sperm DNA Fragmentation in Semen Samples of Patients Undergoing Fertility Investigation. Genes 2021, 12, 654. https://doi.org/10.3390/genes12050654
Pagliuca C, Cariati F, Bagnulo F, Scaglione E, Carotenuto C, Farina F, D’Argenio V, Carraturo F, D’Aprile P, Vitiello M, et al. Microbiological Evaluation and Sperm DNA Fragmentation in Semen Samples of Patients Undergoing Fertility Investigation. Genes. 2021; 12(5):654. https://doi.org/10.3390/genes12050654
Chicago/Turabian StylePagliuca, Chiara, Federica Cariati, Francesca Bagnulo, Elena Scaglione, Consolata Carotenuto, Fabrizio Farina, Valeria D’Argenio, Francesca Carraturo, Paola D’Aprile, Mariateresa Vitiello, and et al. 2021. "Microbiological Evaluation and Sperm DNA Fragmentation in Semen Samples of Patients Undergoing Fertility Investigation" Genes 12, no. 5: 654. https://doi.org/10.3390/genes12050654
APA StylePagliuca, C., Cariati, F., Bagnulo, F., Scaglione, E., Carotenuto, C., Farina, F., D’Argenio, V., Carraturo, F., D’Aprile, P., Vitiello, M., Strina, I., Alviggi, C., Colicchio, R., Tomaiuolo, R., & Salvatore, P. (2021). Microbiological Evaluation and Sperm DNA Fragmentation in Semen Samples of Patients Undergoing Fertility Investigation. Genes, 12(5), 654. https://doi.org/10.3390/genes12050654