The Pregnancy Outcome of Mosaic Embryo Transfer: A Prospective Multicenter Study and Meta-Analysis

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Approval
2.2. Study Design
2.3. Embryo Culture and Biopsy
2.4. PGT-A
2.5. Genetic Counselling
2.6. Outcome Analysis
2.7. Placenta Biopsy
2.8. Meta-Analysis
2.9. Statistical Analyses
3. Results
3.1. Outcome Predictors of Mosaic Embryo Transfers
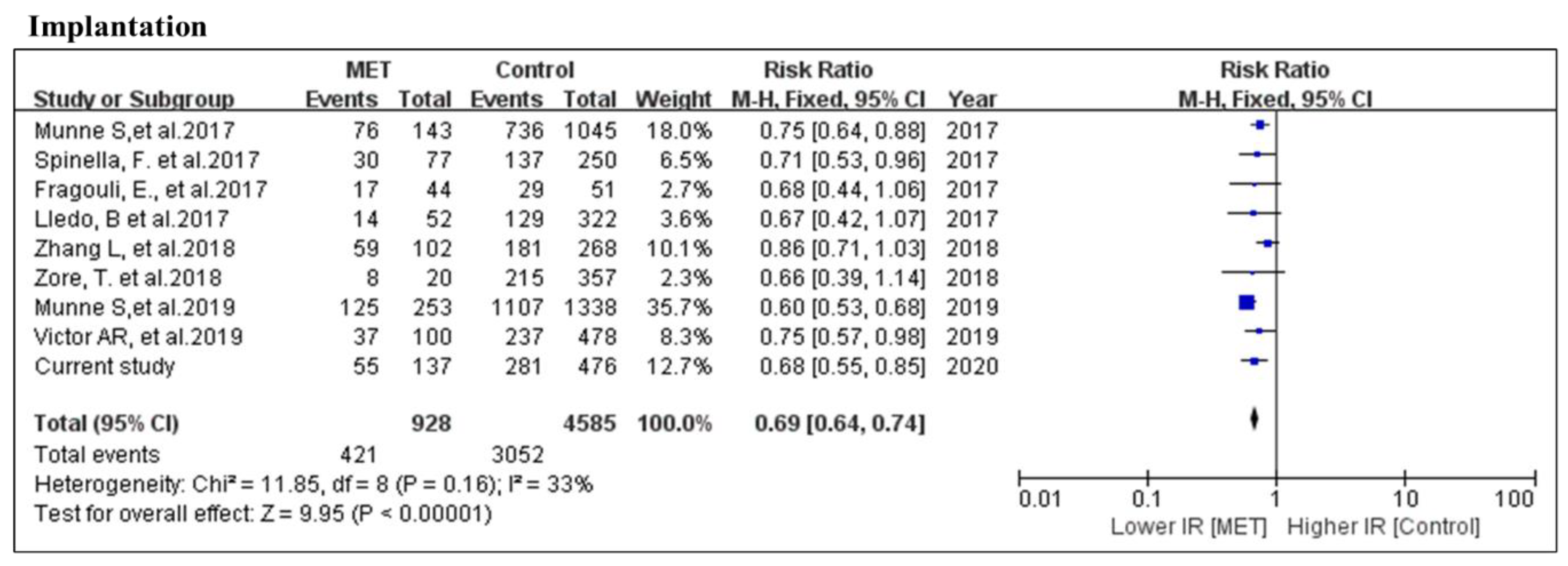
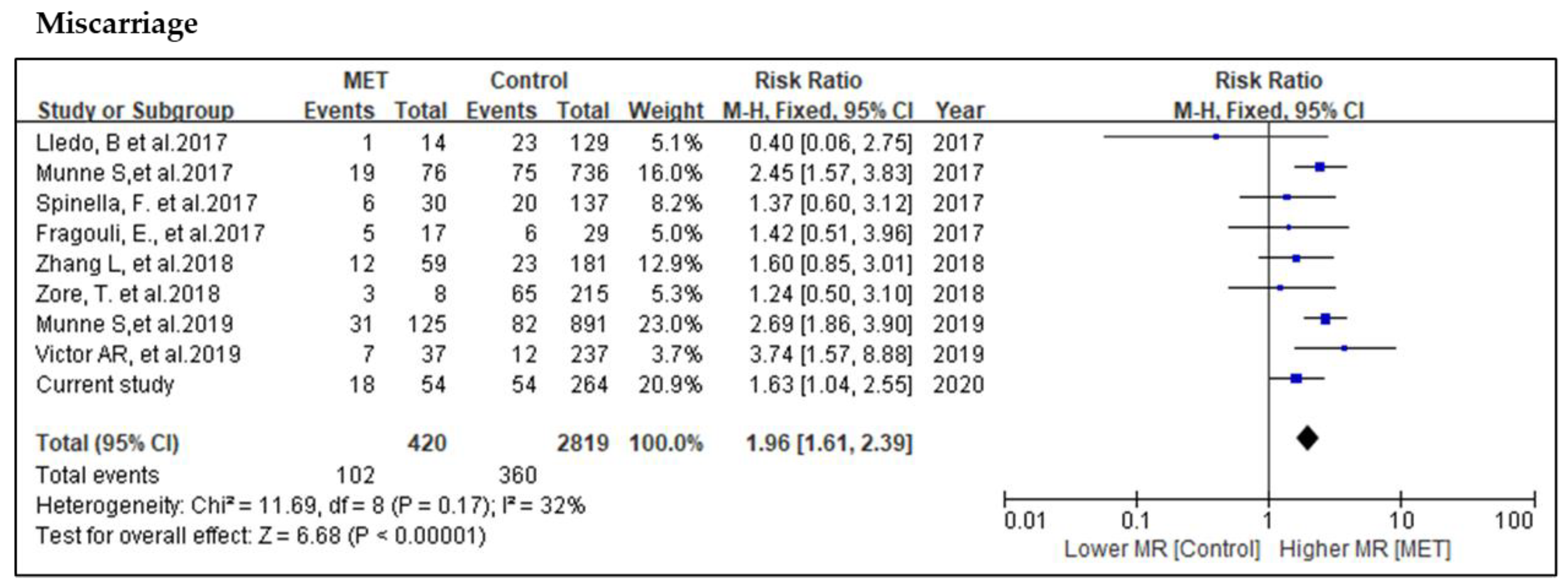
3.2. Systematic Review and Meta-Analysis
3.3. Perinatal Follow-up of MET Pregnancies
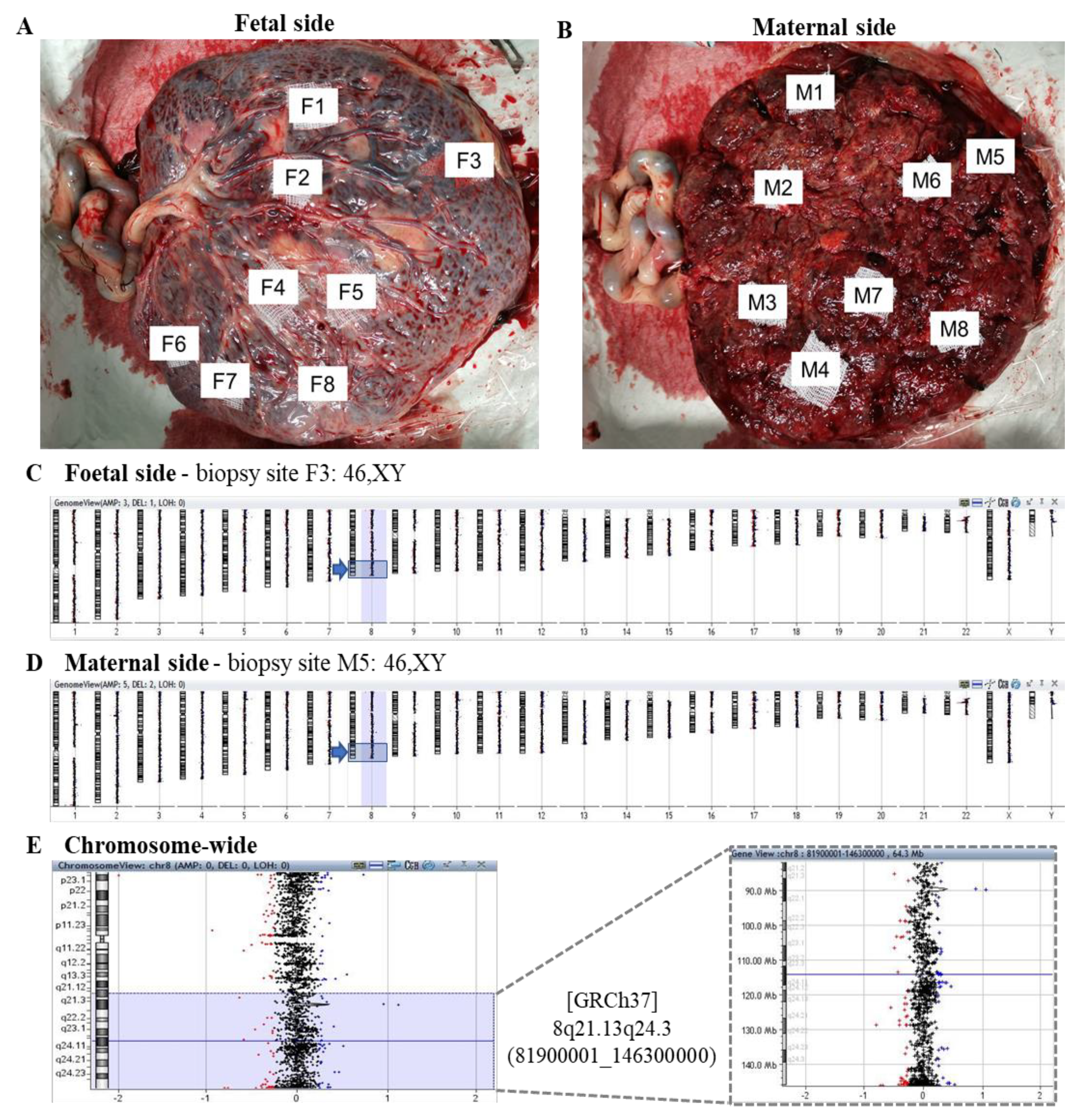
3.4. Postnatal Confirmation by Placental Multiple Biopsy
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

References
- Maxwell, S.M.; Colls, P.; Hodes-Wertz, B.; McCulloh, D.H.; McCaffrey, C.; Wells, D.; Munné, S.; Grifo, J.A. Why do euploid embryos miscarry? A case-control study comparing the rate of aneuploidy within presumed euploid embryos that resulted in miscarriage or live birth using next-generation sequencing. Fertil. Steril. 2016, 106, 1414–1419. [Google Scholar] [CrossRef]
- Munné, S.; Blazek, J.; Large, M.; Martinez-Ortiz, P.A.; Nisson, H.; Liu, E.; Tarozzi, N.; Borini, A.; Becker, A.; Zhang, J.; et al. Detailed investigation into the cytogenetic constitution and pregnancy outcome of replacing mosaic blastocysts detected with the use of high-resolution next-generation sequencing. Fertil. Steril. 2017, 108, 62–71. [Google Scholar] [CrossRef]
- Fragouli, E.; Alfarawati, S.; Spath, K.; Babariya, D.; Tarozzi, N.; Borini, A.; Wells, D. Analysis of implantation and ongoing pregnancy rates following the transfer of mosaic diploid-aneuploid blastocysts. Hum. Genet. 2017, 136, 805–819. [Google Scholar] [CrossRef]
- Grati, F.R.; Ferreira, J.; Benn, P.; Izzi, C.; Verdi, F.; Vercellotti, E.; Dalpiaz, C.; D’Ajello, P.; Filippi, E.; Volpe, N.; et al. Outcomes in pregnancies with a confined placental mosaicism and implications for prenatal screening using cell-free DNA. Obstet. Gynecol. Surv. 2019, 75, 397–398. [Google Scholar] [CrossRef]
- Ruttanajit, T.; Chanchamroen, S.; Cram, D.S.; Sawakwongpra, K.; Suksalak, W.; Leng, X.; Fan, J.; Wang, L.; Yao, Y.; Quangkananurug, W. Detection and quantitation of chromosomal mosaicism in human blastocysts using copy number variation sequencing. Prenat. Diagn. 2016, 36, 154–162. [Google Scholar] [CrossRef]
- Capalbo, A.; Wright, G.; Elliott, T.; Ubaldi, F.M.; Rienzi, L.; Nagy, Z.P. FISH reanalysis of inner cell mass and trophectoderm samples of previously array-CGH screened blastocysts shows high accuracy of diagnosis and no major diagnostic impact of mosaicism at the blastocyst stage. Hum. Reprod. 2013, 28, 2298–2307. [Google Scholar] [CrossRef]
- Munné, S.; Kaplan, B.; Frattarelli, J.L.; Child, T.; Nakhuda, G.; Shamma, F.N.; Silverberg, K.; Kalista, T.; Handyside, A.H.; Katz-Jaffe, M.; et al. Preimplantation genetic testing for aneuploidy versus morphology as selection criteria for single frozen-thawed embryo transfer in good-prognosis patients: A multicenter randomized clinical trial. Fertil. Steril. 2019, 112. [Google Scholar] [CrossRef]
- Bolton, H.; Graham, S.J.L.; Van der Aa, N.; Kumar, P.; Theunis, K.; Gallardo, E.F.; Voet, T.; Zernicka-Goetz, M. Mouse model of chromosome mosaicism reveals lineage-specific depletion of aneuploid cells and normal developmental potential. Nat. Commun. 2016, 7, 11165. [Google Scholar] [CrossRef]
- Barbash-Hazan, S.; Frumkin, T.; Malcov, M.; Yaron, Y.; Cohen, T.; Azem, F.; Amit, A.; Ben-Yosef, D. Preimplantation aneuploid embryos undergo self-correction in correlation with their developmental potential. Fertil. Steril. 2009, 92, 890–896. [Google Scholar] [CrossRef]
- Capalbo, A.; Bono, S.; Spizzichino, L.; Biricik, A.; Baldi, M.; Colamaria, S.; Ubaldi, F.M.; Rienzi, L.; Fiorentino, F. Sequential comprehensive chromosome analysis on polar bodies, blastomeres and trophoblast: Insights into female meiotic errors and chromosomal segregation in the preimplantation window of embryo development. Hum. Reprod. 2013, 28, 509–518. [Google Scholar] [CrossRef]
- Spinella, F.; Fiorentino, F.; Biricik, A.; Bono, S.; Ruberti, A.; Cotroneo, E.; Baldi, M.; Cursio, E.; Minasi, M.G.; Greco, E. Extent of chromosomal mosaicism influences the clinical outcome of in vitro fertilization treatments. Fertil. Steril. 2017, 108, e272. [Google Scholar] [CrossRef][Green Version]
- Victor, A.R.; Tyndall, J.C.; Brake, A.J.; Lepkowsky, L.T.; Murphy, A.E.; Griffin, D.K.; McCoy, R.C.; Barnes, F.L.; Zouves, C.G.; Viotti, M. One hundred mosaic embryos transferred prospectively in a single clinic: Exploring when and why they result in healthy pregnancies. Fertil. Steril. 2019, 111, 280–293. [Google Scholar] [CrossRef]
- Munné, S.; Spinella, F.; Grifo, J.; Zhang, J.; Beltran, M.P.; Fragouli, E.; Fiorentino, F. Clinical outcomes after the transfer of blastocysts characterized as mosaic by high resolution Next Generation Sequencing—Further insights. Eur. J. Med Genet. 2019, 103741. [Google Scholar] [CrossRef]
- Lledó, B.; Morales, R.; Ortiz, J.A.; Blanca, H.; Ten, J.; Llácer, J.; Bernabeu, R. Implantation potential of mosaic embryos. Syst. Biol. Reprod. Med. 2017, 63, 1–3. [Google Scholar] [CrossRef]
- Zore, T.; Kroener, L.L.; Wang, C.; Liu, L.; Buyalos, R.; Hubert, G.; Shamonki, M. Transfer of embryos with segmental mosaicism is associated with a significant reduction in live-birth rate. Fertil. Steril. 2019, 111, 69–76. [Google Scholar] [CrossRef]
- Cram, D.S.; Leigh, D.; Handyside, A.; Rechitsky, L.; Xu, K.; Harton, G.; Grifo, J.; Rubio, C.; Fragouli, E.; Kahraman, S.; et al. PGDIS Position Statement on the Transfer of Mosaic Embryos 2019. Reprod. Biomed. Online 2019, 39, e1. [Google Scholar] [CrossRef]
- Schoolcraft, W.B.; Gardner, D.K.; Lane, M.; Schlenker, T.; Hamilton, F.; Meldrum, D.R. Blastocyst culture and transfer: Analysis of results and parameters affecting outcome in two in vitro fertilization programs. Fertil. Steril. 1999, 72, 604–609. [Google Scholar] [CrossRef]
- Heitmann, R.J.; Hill, M.J.; Richter, K.S.; DeCherney, A.H.; Widra, E.A. The simplified SART embryo scoring system is highly correlated to implantation and live birth in single blastocyst transfers. J. Assist. Reprod. Genet. 2013, 30, 563–567. [Google Scholar] [CrossRef]
- Zheng, H.; Jin, H.; Liu, L.; Liu, J.; Wang, W.-H. Application of next-generation sequencing for 24-chromosome aneuploidy screening of human preimplantation embryos. Mol. Cytogenet. 2015, 8, 38. [Google Scholar] [CrossRef]
- Goodrich, D.; Tao, X.; Bohrer, C.; Lonczak, A.; Xing, T.; Zimmerman, R.; Zhan, Y.; Scott, R.T.; Treff, N.R. A randomized and blinded comparison of qPCR and NGS-based detection of aneuploidy in a cell line mixture model of blastocyst biopsy mosaicism. J. Assist. Reprod. Genet. 2016, 33, 1473–1480. [Google Scholar] [CrossRef]
- Yeung, Q.S.Y.; Zhang, Y.X.; Chung, J.P.W.; Lui, W.T.; Kwok, Y.K.Y.; Gui, B.; Kong, G.W.S.; Cao, Y.; Li, T.C.; Choy, K.W. A prospective study of non-invasive preimplantation genetic testing for aneuploidies (NiPGT-A) using next-generation sequencing (NGS) on spent culture media (SCM). J. Assist. Reprod. Genet. 2019, 1609–1621. [Google Scholar] [CrossRef]
- Gui, B.; Zhang, Y.; Liang, B.; Kwok, Y.K.Y.; Lui, W.T.; Yeung, Q.S.Y.; Kong, L.; Xuan, L.; Chung, J.P.W.; Choy, K.W. Semiconductor sequencing for preimplantation genetic testing for aneuploidy. J. Vis. Exp. 2019, 2019, 1–9. [Google Scholar] [CrossRef]
- Grati, F.R.; Gallazzi, G.; Branca, L.; Maggi, F.; Simoni, G.; Yaron, Y. An evidence-based scoring system for prioritizing mosaic aneuploid embryos following preimplantation genetic screening. Reprod. Biomed. Online 2018, 36, 442–449. [Google Scholar] [CrossRef]
- Chan, Y.-M.; Li, T.-C.; Poon, L.C.Y. Impact of preimplantation genetic testing for aneuploidy on obstetrical practice. Curr. Opin. Obstet. Gynecol. 2019, 31, 127–131. [Google Scholar] [CrossRef]
- Farquharson, R.G.; Jauniaux, E.; Exalto, N. Updated and revised nomenclature for description of early pregnancy events. Hum. Reprod. 2005, 20, 3008–3011. [Google Scholar] [CrossRef]
- Zegers-Hochschild, F.; Adamson, G.D.; Dyer, S.; Racowsky, C.; de Mouzon, J.; Sokol, R.; Rienzi, L.; Sunde, A.; Schmidt, L.; Cooke, I.D.; et al. The International Glossary on Infertility and Fertility Care, 2017. Fertil. Steril. 2017, 108, 393–406. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- The Cochrane Collaboration Review Manager (RevMan). Available online: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman (accessed on 9 June 2020).
- Zhang, L.; Wei, D.; Zhu, Y.; Gao, Y.; Yan, J.; Chen, Z.J. Rates of live birth after mosaic embryo transfer compared with euploid embryo transfer. J. Assist. Reprod. Genet. 2019, 36, 165–172. [Google Scholar] [CrossRef]
- Greco, E.; Minasi, M.G.; Fiorentino, F. Healthy Babies after Intrauterine Transfer of Mosaic Aneuploid Blastocysts. N. Engl. J. Med. 2015, 373, 2089–2090. [Google Scholar] [CrossRef]
- Capalbo, A.; Ubaldi, F.M.; Rienzi, L.; Scott, R.; Treff, N. Detecting mosaicism in trophectoderm biopsies: Current challenges and future possibilities. Hum. Reprod. 2016, 1–7. [Google Scholar] [CrossRef]
- Victor, A.R.; Griffin, D.K.; Brake, A.J.; Tyndall, J.C.; Murphy, A.E.; Lepkowsky, L.T.; Lal, A.; Zouves, C.G.; Barnes, F.L.; McCoy, R.C.; et al. Assessment of aneuploidy concordance between clinical trophectoderm biopsy and blastocyst. Hum. Reprod. 2018, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Grati, F.R.; Malvestiti, F.; Ferreira, J.C.P.B.; Bajaj, K.; Gaetani, E.; Agrati, C.; Grimi, B.; Dulcetti, F.; Ruggeri, A.M.; De Toffol, S.; et al. Fetoplacental mosaicism: Potential implications for false-positive and false-negative noninvasive prenatal screening results. Genet. Med. Off. J. Am. Coll. Med. Genet. 2014, 16, 620–624. [Google Scholar] [CrossRef]
- Grati, F.R.; Malvestiti, F.; Branca, L.; Agrati, C.; Maggi, F.; Simoni, G. Chromosomal mosaicism in the fetoplacental unit. Best Pract. Res. Clin. Obstet. Gynaecol. 2017, 42, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Garrisi, G.; Walmsley, R.H.; Bauckman, K.; Mendola, R.J.; Colls, P.; Munne, S. Discordance among serial biopsies of mosaic embryos. Fertil. Steril. 2016, 106, e151. [Google Scholar] [CrossRef]
- Dong, Z.; Yan, J.; Xu, F.; Yuan, J.; Jiang, H.; Wang, H.; Chen, H.; Zhang, L.; Ye, L.; Xu, J.; et al. Genome Sequencing Explores Complexity of Chromosomal Abnormalities in Recurrent Miscarriage. Am. J. Hum. Genet. 2019, 105, 1102–1111. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.; Wang, H.; Chen, H.; Jiang, H.; Yuan, J.; Yang, Z.; Wang, W.-J.; Xu, F.; Guo, X.; Cao, Y.; et al. Identification of balanced chromosomal rearrangements previously unknown among participants in the 1000 Genomes Project: Implications for interpretation of structural variation in genomes and the future of clinical cytogenetics. Genet. Med. Off. J. Am. Coll. Med. Genet. 2017, 7, 697–707. [Google Scholar] [CrossRef]
- Kahraman, S.; Cetinkaya, M.; Yuksel, B.; Yesil, M.; Cetinkaya, C.P. The birth of a baby with mosaicism resulting from a known mosaic embryo transfer: A case report. Hum. Reprod. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MET | Euploid Control | Non-PGT Control | |
|---|---|---|---|
| Age | 31.8 ± 6.4 | 34.5 ± 5.8 | 36.9 ± 3.3 |
| Embryos | 137 | 476 | 835 |
| ETs | 133 | 447 | 777 |
| Single ET | 129 (97%) | 418 (94%) | 719 |
| Double ET | 4 (3%) | 29 (6%) | 58 |
| Clinical Indications | |||
| AMA | 56 (41%) | 276 (58%) | / |
| RM * | 4 (3%) | 32 (7%) | / |
| RIF * | 4 (3%) | 17 (4%) | / |
| Translocation Carriers * | 0 | 6 (1%) | / |
| Male factors * | 0 | 3 (1%) | / |
| PGT-M * | 2 (2%) | 29 (6%) | / |
| Previous Abnormal Pregnancy * | 6 (5%) | 18 (4%) | / |
| Aneuploidy Screening * | 54 (43%) | 79 (17%) | / |
| Morphology | |||
| Good | 41 (30%) | 141 (44%) | / |
| Fair | 89 (65%) | 160 (50%) | / |
| Poor | 7 (5%) | 19 (6%) | / |
| Birth Weight (g) | 3180 ± 505 | 3047 ± 560 | / |
| Clinical Pregnancy | Ongoing Pregnancy/Live Birth | Miscarriage | |
|---|---|---|---|
| MET | 40.6% a | 27.1% a | 33.3% |
| Euploid Control | 59.1% | 47.0% | 20.5% |
| Non-PGTControl | 48.4% b | 35.1% b | 27.4% b |
| Clinical Pregnancy | Ongoing Pregnancy/Live Birth | Miscarriage | |||||||
|---|---|---|---|---|---|---|---|---|---|
| No. of Embryos | p * | p ** | No. of Embryos | p * | p ** | No. of Embryos | p * | p ** | |
| Euploid | 281 | 223 | 58 | ||||||
| Mosaic level | |||||||||
| <40% | 30 | 0.10 | <0.001 | 21 | 0.38 | <0.001 | 9 | 0.64 | 0.24 |
| ≥40% | 25 | 0.17 | 16 | 0.04 | 9 | 0.08 | |||
| <50% | 47 | 0.27 | <0.001 | 30 | 0.07 | <0.001 | 17 | 0.19 | 0.02 |
| ≥50% | 8 | 0.66 | 7 | 0.99 | 1 | 1 *** | |||
| Classification by Size of Mosaic Variant * | Clinical Pregnancy | Ongoing Pregnancy/Live Birth | Miscarriage | |||
|---|---|---|---|---|---|---|
| MET | p-Value | MET | p-Value | MET | p-Value | |
| Numerical | 20 | 0.79 | 10 | 0.23 | 10 | 0.04 |
| Segmental | 35 | 27 | 8 | |||
| Morphological Grading | Clinical Pregnancy | Ongoing Pregnancy/Live Birth | Miscarriage | ||||||
|---|---|---|---|---|---|---|---|---|---|
| MET | Control | p-Value | MET | Control | p-Value | MET | Control | p-Value | |
| Good | 17 (41.5%) | 87 (61.7%) | 0.021 | 16 (39.0%) | 70 (49.6%) | 0.23 | 1 (5.9%) | 17 (19.5%) | 0.173 |
| Fair | 35 (39.3%) | 97 (60.6%) | <0.05 | 18 (20.2%) | 74 (46.3%) | <0.005 | 17 (48.6%) | 23 (23.7%) | 0.006 |
| Poor | 3 (42.9%) | 11 (57.9%) | 0.67 | 3 (42.9%) | 8 (42.1%) | 1.00 | 0 (0%) | 3 (27.3%) | 1.00 |
| Within group difference (p-value) | 0.96 | 0.94 | 0.05 | 0.75 | < 0.05 | 0.72 | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.X.; Chen, J.J.; Nabu, S.; Yeung, Q.S.Y.; Li, Y.; Tan, J.H.; Suksalak, W.; Chanchamroen, S.; Quangkananurug, W.; Wong, P.S.; et al. The Pregnancy Outcome of Mosaic Embryo Transfer: A Prospective Multicenter Study and Meta-Analysis. Genes 2020, 11, 973. https://doi.org/10.3390/genes11090973
Zhang YX, Chen JJ, Nabu S, Yeung QSY, Li Y, Tan JH, Suksalak W, Chanchamroen S, Quangkananurug W, Wong PS, et al. The Pregnancy Outcome of Mosaic Embryo Transfer: A Prospective Multicenter Study and Meta-Analysis. Genes. 2020; 11(9):973. https://doi.org/10.3390/genes11090973
Chicago/Turabian StyleZhang, Ying Xin, Jang Jih Chen, Sunanta Nabu, Queenie Sum Yee Yeung, Ying Li, Jia Hui Tan, Wanwisa Suksalak, Sujin Chanchamroen, Wiwat Quangkananurug, Pak Seng Wong, and et al. 2020. "The Pregnancy Outcome of Mosaic Embryo Transfer: A Prospective Multicenter Study and Meta-Analysis" Genes 11, no. 9: 973. https://doi.org/10.3390/genes11090973
APA StyleZhang, Y. X., Chen, J. J., Nabu, S., Yeung, Q. S. Y., Li, Y., Tan, J. H., Suksalak, W., Chanchamroen, S., Quangkananurug, W., Wong, P. S., Chung, J. P. W., & Choy, K. W. (2020). The Pregnancy Outcome of Mosaic Embryo Transfer: A Prospective Multicenter Study and Meta-Analysis. Genes, 11(9), 973. https://doi.org/10.3390/genes11090973