1. Introduction
Myotonic dystrophy type 1 (DM1) is caused by a CTG (Cytosine-Thymine-Guanine) expansion in the 3′ untranslated region of the dystrophia myotonica-protein kinase (
DMPK) gene [
1]. The CTG expansion is highly unstable, showing size variation both within [
2] and between tissues [
3,
4,
5,
6]. Genetic instability hinders the establishment of genotype/phenotype correlations in patients with DM1, and most studies assessing CTG expansion have focused solely on blood samples [
7,
8,
9,
10]. Here we used small pool polymerase chain reaction (SP-PCR) to study CTG expansion in three different tissues from affected patients. We estimated the progenitor allele, the mode of CTG expansion size and the highest CTG repeat number, as well as the genetic instability of the CTG repeat (i.e., the difference between the progenitor and the mode CTG size) in the different tissues. We also analyzed the potential association between the different CTG measures, on the one hand, and patients’ clinical phenotype, on the other.
2. Materials and Methods
This study was approved by the local ethics committee (University Hospital Germans Trias i Pujol, # PI15-009) and was performed in agreement with the Declaration of Helsinki for Human Research. All participants signed an informed consent. The study included eight patients with DM1 and eight controls with no previous family history of neuromuscular disorders (recruited from the traumatology department in whom surgery was needed. DM1 diagnosis was confirmed or discarded with triplet primed-PCR11 in all the study participants. Clinical information of DM1 patients was obtained from the medical records and updated in the last visit.
We obtained three different samples from patients and controls: blood, muscle biopsy, and skin biopsy. All samples were obtained at the same time. Blood was collected in EDTA tubes and frozen at −20 °C before DNA extraction. The muscle biopsy was obtained from the left biceps muscle in all individuals except for one patient (P8, vastus lateralis muscle). Skin biopsy was obtained with a 0.5 cm skin punch. Muscle biopsies were frozen immediately and stored at −80 °C before DNA extraction. Before freezing skin biopsies at −80 °C for further DNA extraction, they were first seeded and cultured in plates for 6 days to obtain fibroblasts required for other experiments.
Genomic DNA was isolated from peripheral blood [
11]. Genomic DNA was extracted from muscle and skin tissue by homogenization in 100 mM Tris-HCl, pH 7.8, and 5 mM EDTA until these tissues were disaggregated. Thereafter tissues were digested in 20 mg/mL proteinase K and 10% SDS for 16 h at 37 °C, and treated with 5.5 M NaCl, phenol and chloroform isoamyl (1:24) before DNA precipitation with isopropanol. DNA quality and quantity were measured by Qubit Fluorometric (Themo Fisher Scientific; Waltham, MA, USA) and Agilent 4200 TapeStation analysis (Agilent Technologies; Santa Clara, CA, USA).
To measure CTG expansion size, SP-PCR was performed [
12]. Briefly, small amounts of input DNA (300 pg) were used with the flanking primers DM-C and DM-DR as previously described [
12]. We used custom PCR Master Mix (Thermo Fisher Scientific; Waltham, MA, USA) supplemented with 69 mM 2-mercaptoethanol, and Taq polymerase Thermus aquaticus (Sigma-Aldrich; Gillingham, UK) at 1 unit per 10 µL, supplemented with 5% DMSO and the annealing temperature was 63.5 °C. DNA fragments were resolved by electrophoresis on a 1% agarose gel, followed by Southern blot [
13]. The estimated CTG sizes (the progenitor, the mode, and the longest CTG size) in each tissue were determined by comparison against the molecular weight ladder, using GelAnalyzer 19.1 software ((
www.gelanalyzer.com) by Istvan Lazar Jr., PhD and Istvan Lazar Sr., PhD, CSc). We studied four replicates of each sample, allowing the analysis of the allele distribution CTG sizes, since the most representative allele sizes that are present in a given sample are shown in the gel (see
Figure S1 for more information on the different measurements). Genetic instability was calculated by subtracting the progenitor CTG size from the mode CTG size amplified for each sample. This method has been optimized by Prof. Monckton’s group [
12].
We used repeated-measures, one-factor (i.e., ‘tissue’) analysis of variance (ANOVA) to compare CTG variables (progenitor, mode, longest repeat length, and somatic instability) across the different tissue samples within each subject. When a main tissue effect was found, post hoc pairwise comparisons (skin vs. blood, skin vs. muscle, and blood vs. muscle) were done with the Bonferroni test. We also determined the relationship between the aforementioned CTG variables and patients’ clinical characteristics with Pearson’s correlations (or Spearman correlations for those data that were not normally distributed, as determined with the Shapiro–Wilk test). The level of significance was set at 0.05 (two-tailed).
3. Results
We studied eight patients (six women). The patients’ cohort included five unrelated individuals and three sisters from the same family (P3, P4, and P8). Symptom onset occurred during adulthood in seven patients (with symptoms starting around their fifties in two of them (P2, aged 48 years; P7, 50 years)) whereas in one patient the symptoms started earlier in life (P1, 15 years) (
Table 1). One patient (P7) carried previously reported CCG interruptions [
14]. All the patients had clinical myotonia, but only two showed a mild impairment in biceps muscle strength (as reflected by a score of 4 in the 0 to 5 Medical Research Council (MRC) scale). Performance in the 6-min walking distance test averaged 377 m (range 251–519). When using the muscular impairment rating scale (MIRS), 25% of patients showed minimal signs of muscular impairment, 50% had distal weakness, and 25% had mild-moderate proximal weakness. Most patients (87.5%) were independent in daily life activities (score of 0–2 on the modified Rankin (mRS) (0 to 6) scale), and only one (P5) had a moderately severe disability (4).
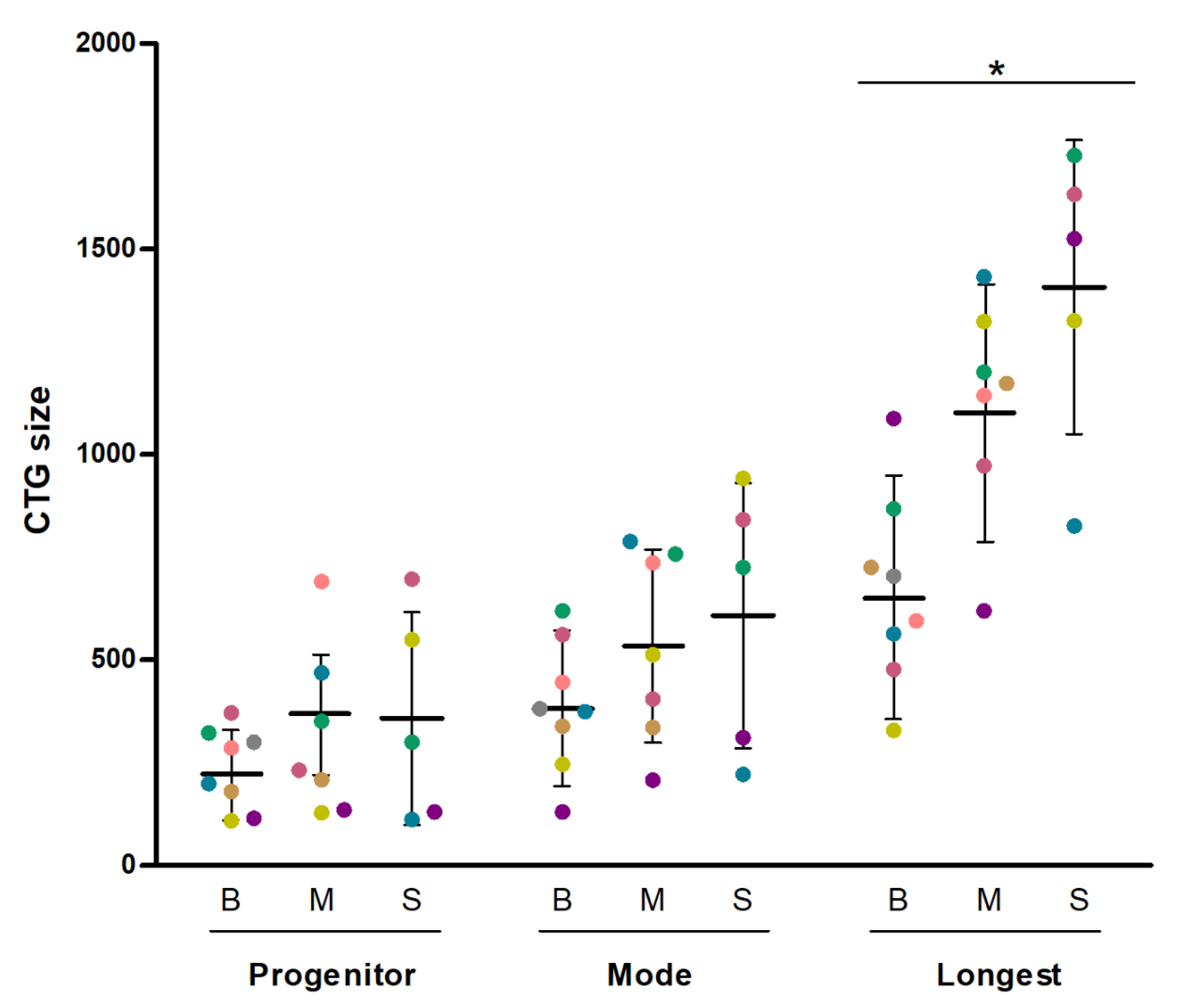
The estimated progenitor, most abundant (mode) and longest CTG expansion size were measured in blood (
n = 8), muscle (
n = 7) and skin samples (
n = 5) (
Figure 1). An example of CTG expansion determination is shown in
Figure S1. DNA from one muscle biopsy and from three skin biopsies yielded no amplification and therefore precluded CTG sizing. We found no differences across tissues for progenitor CTG (
p = 0.449 for tissue effect with the repeated-measures one-factor ANOVA), mode size (
p = 0.247), and genetic instability (
p = 0.691). By contrast, a significant (
p = 0.041) tissue effect was found for the longest CTG with significant differences (
p < 0.05) found for all post hoc pairwise comparisons (thus, mean of the longest CTG size in blood (665 CTGs) < muscle (1110 CTGs) < skin (1408 CTGs). In blood samples, we found the following significant correlations (all
p < 0.05): blood progenitor CTG size vs. mode allele, r = 0.900 (95% confidence interval 0.536–0.982); mode allele vs. longest allele, r = 0.805 (0.231–0.963); and longest allele vs. progenitor allele, r = 0.861 (0.398–0.975). These results suggested that the progenitor, the mode and the longest expansion size were uniformly distributed, with the CTG tract evenly expanded in blood. For muscle and skin samples, a significant (
p < 0.05) correlation was only found between the progenitor and mode size (muscle: r = 0.769 (0.037–0.964); skin: r = 0.895 (0.061–0.993)). No correlation was found between tissues. Finally, as P7 carried variant repeats, we compared the results of this patient with those of patients carrying pure repeats to determine whether P7 showed a more stable CTG repeat behavior in any of the tissues, which was not the case (
Figure S2).
We further studied the relationship between genetic and clinical data and found a significant (
p < 0.05) correlation between the progenitor allele found in muscle and both age of disease onset (r = −0.850 (−0.977–0.268)) and the MRC corresponding to the studied muscles (r = −0.932 (−0.992–0.496)) (
Figure 2). The CTG mode length in muscle was also correlated with the MRC score for the muscle in question (r = −0.898 (−0.989 to −0.319),
p < 0.05). By contrast, no significant correlation was found between CTG expansion in blood or skin and the clinical manifestation of the disease.
4. Discussion
Our preliminary results suggest that CTG expansions might be in general larger in muscle and skin than in blood. Previous studies have reported that (i) patients’ muscle fibers carry larger expansions than peripheral blood leukocytes [
3,
4,
5], and (ii) patients’ fibroblasts carry larger expansions than peripheral blood lymphocytes [
6]. However, no previous study has assessed CTG repeats in blood, muscle and skin cells from the same patients. Furthermore, we studied in depth the CTG expansion size by applying SP-PCR methodology and took into account the genetic instability of CTG expansion (instead of focusing on one single CTG size per tissue using a less accurate southern blot-based analysis). This strategy allowed us to determine that the progenitor and the mode size did not differ significantly across tissues, as opposed to the highest expansion. This finding suggests that the CTG tract is expanding in a different manner in each tissue.
The three tissues presented genetic instability. The complex phenomenon of genetic instability can be produced by numerous mechanisms, including not only DNA repair mechanisms but also DNA replication, transcription, and epigenetic changes. In muscle and skin, a non-dividing cell status coupled with DNA repair mechanisms might play an important role in producing genetic instability. In the case of blood cells, the CTG expansion instability could also be affected by the division status of these cells.
No differences in the CTG stability were found between P7 (who carried variant repeats) and the rest of the patients (who had pure expansion repeats in blood, skin, and muscle). Some authors have shown a stabilizing effect of the variant repeats [
15,
16], which was not confirmed in P7. Although the case of P7 might be an exceptional one, no conclusions can be really drawn as our study is the first to analyze genetic instability in different tissues of a patient with variant repeats.
When analyzing each tissue independently, we found that all measures (progenitor, mode, and highest CTG) were correlated to each other in blood samples, suggesting that the progenitor CTG size leads the genetic instability of CTG expansion in blood. Conversely, in muscle and skin the progenitor was correlated with the mode but not with the highest CTG, suggesting that the genetic instability of the CTG tract is more random in these tissues, probably due to the longer length of CTG repeats.
We found that the progenitor allele in muscle tissue was the only CTG variable associated with age of disease onset. This finding is not surprising when considering that the muscle is one of the most affected tissues in patients with DM1. In this regard, we studied samples mostly from biceps muscle, whereas disease manifestation might start earlier in the tibialis anterior muscle [
17,
18]. However, some authors have hypothesized that CTG in muscle tissue could show a stronger correlation with disease severity than CTG determined in blood cells [
4,
5], for which we were actually able to provide preliminary (‘proof-of-concept’) evidence. Furthermore, our data also suggest that the CTG size in muscle is associated with patients’ muscle impairment (as determined with the MRC scale). These results might reflect a close relationship between CTG expansion in muscle and the degree of functional affectation in this tissue. Although it has been shown that the progenitor size determined in peripheral blood leukocytes of patients with DM1 is also a good indicator of age of disease onset [
19], we failed to find a correlation between blood measures and age of symptom onset, maybe owing to the small sample size of our study. Previous studies in larger cohorts of patients with DM1 have in fact reported a close relationship between CTG size in blood and cardiac complications [
20] or survival [
21].
In conclusion, we found preliminary evidence for the presence of genetic instability in all the patients’ tissues that we studied, yet with muscle and skin cells carrying larger expansions than peripheral blood leukocytes. Although more research is needed in larger cohorts, our preliminary data suggest the estimated progenitor CTG size as determined in muscle tissue is associated with age of disease onset and muscle functional impairment.
Supplementary Materials
The following are available online at
https://www.mdpi.com/2073-4425/11/11/1321/s1, Figure S1: Representative SP-PCR gel with the different CTG size measurements. Figure S2: CTG size allele distribution in blood of the patient carrying interruptions vs one patient carrying pure repeats.
Author Contributions
A.B.-L., E.K. and S.A.C. carried out the experiments. J.N.-M., I.L.-P., M.A., G.L. and A.A. contributed to sample preparation. A.B.-L., A.R.-F., A.M.-P., G.P.-M., C.P.A. and J.C.-C. performed sample collection. G.N.-G. and A.M.-P. conceived the experiments and supervised the project. A.B.-L. performed the data analysis, interpretation of the results and wrote the manuscript. A.L. helped with the statistical analysis. G.N.-G. and A.L. supported and helped in writing the manuscript. D.G.M., S.A.C., provided critical feedback and helped shape the research. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the following projects and institutions: PI15/01756, PI15/00558, PI18/00713, CD14/00032, CPII19/00021 and CM16/00016 (funded by ISCIII and co-financed by Fondos FEDER), AFM Telethon (Trampoline grant number #21108)), FI_B 01090 (Agaur), ID 100010434 and by SGR 1520 (GRC) Generalitat de Catalunya. LCF/BQ/IN18/11660019 (“La Caixa” Foundation co-funded by Marie Skłodowska-Curie grant agreement n◦713673).
Acknowledgments
We gratefully acknowledge the participants in this research, the patients’ associations and the core facilities of the IGTP.
Conflicts of Interest
G.N.G. declares grants from Instituto de Salud Carlos III (Grant Numbers: PI15/01756; P18/00713), Madrid, Spain and AFM Telethon (Trampoline grant number #21108), France. A.L. declares grants from the Spanish government granting agency Instituto de Salud Carlos III, Madrid, Spain. J.N.M. is funded by AFM Telethon Trampoline Grant #21108. A.B.L. is funded by an FI Agaur fellowship FI_B 01090. E.K. is funded by the “La Caixa” Foundation (ID 100010434), fellowship code LCF/BQ/IN18/11660019, co-funded by the European Union’s Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement n°713673. I.L.P. is funded by CP14/00032. G.N.G. is supported by a Miguel Servet research contract (ISCIII CD14/00032, CPII19/00021, and FEDER). G.L. was supported by a Rio Hortega contract (ISCIII CM16/00016 and FEDER). G.P.-M. reports personal honoraria from Shire-Takeda, Amicus, Kyowa-Kirin, and Sanofi-Genzyme, outside the submitted work. The remaining co-authors declare no competing interests.
References
- Brook, J.D.; McCurrach, M.E.; Harley, H.G.; Buckler, A.J.; Church, D.; Aburatani, H.; Hunter, K.; Stanton, V.P.; Thirion, J.-P.; Hudson, T.; et al. Molecular basis of myotonic dystrophy: Expansion of a trinucleotide (CTG) repeat at the 3′ end of a transcript encoding a protein kinase family member. Cell 1992, 68, 799–808. [Google Scholar] [CrossRef]
- La Spada, A.R. Trinucleotide Repeat Instability: Genetic Features and Molecular Mechanisms. Brain Pathol. 1997, 7, 943–963. [Google Scholar] [CrossRef] [PubMed]
- Ashizawa, T.; Dubel, J.R.; Harati, Y. Somatic instability of ctg repeat in myotonic dystrophy. Neurology 1993, 43, 2674–2678. [Google Scholar] [CrossRef] [PubMed]
- Thornton, C.A.; Johnson, K.; Moxley, R.T. Myotonic dystrophy patients have larger CTG expansions in skeletal muscle than in leukocytes. Ann. Neurol. 1994, 35, 104–107. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8285579 (accessed on 25 March 2020). [CrossRef] [PubMed]
- Anvret, M.; Ahlberg, G.; Grandell, U.; Hedberg, B.; Johnson, K.; Edström, L. Larger expansions of the CTG repeat in muscle compared to lymphocytes from patients with myotonic dystrophy. Hum. Mol. Genet. 1993, 2, 1397–1400. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8242063 (accessed on 25 March 2020). [CrossRef] [PubMed]
- Peterlin, B.; Logar, N.; Zidar, J. CTG repeat analysis in lymphocytes, muscles and fibroblasts in patients with myotonic dystrophy. Pflug. Arch. 1996, 431 (Suppl. 2), R199–R200. Available online: http://www.ncbi.nlm.nih.gov/pubmed/8739333 (accessed on 25 March 2020). [CrossRef] [PubMed]
- Kim, H.J.; Na, J.-H.; Lee, Y.-M. Genotype-phenotype correlations in pediatric patients with myotonic dystrophy type 1. Korean J. Pediatr. 2019, 62, 55–61. Available online: http://www.ncbi.nlm.nih.gov/pubmed/30304901 (accessed on 26 March 2020). [CrossRef] [Green Version]
- Hamshere, M.G.; Harley, H.; Harper, P.; Brook, J.D.; Brookfield, J.F.Y. Myotonic dystrophy: The correlation of (CTG) repeat length in leucocytes with age at onset is significant only for patients with small expansions. J. Med. Genet. 1999, 36, 59–61. [Google Scholar] [PubMed]
- Merlevede, K.; Vermander, D.; Theys, P.; Legius, E.; Ector, H.; Robberecht, W. Cardiac involvement and CTG expansion in myotonic dystrophy. J. Neurol. 2002, 249, 693–698. [Google Scholar] [CrossRef]
- Gharehbaghi-Schnell, E.B.; Finsterer, J.; Korschineck, I.; Mamoli, B.; Binder, B.R. Genotype-phenotype correlation in myotonic dystrophy. Clin. Genet. 1998, 53, 20–26. [Google Scholar] [CrossRef]
- Miller, S.A.; Dykes, D.D.; Polesky, H.F. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988, 16, 1215. [Google Scholar] [CrossRef] [Green Version]
- Cumming, S.A.; Jimenez-Moreno, C.; Okkersen, K.; Wenninger, S.; Daidj, F.; Hogarth, F.; Littleford, R.; Gorman, G.; Bassez, G.; Schoser, B.; et al. Genetic determinants of disease severity in the myotonic dystrophy type 1 OPTIMISTIC cohort. Neurology 2019, 93, e995–e1009. Available online: http://www.ncbi.nlm.nih.gov/pubmed/31395669 (accessed on 27 March 2020). [CrossRef] [Green Version]
- Gomes-Pereira, M.; Bidichandani, S.I.; Monckton, D.G. Analysis of unstable triplet repeats using small-pool polymerase chain reaction. Methods Mol Biol. 2004, 277, 61–76. [Google Scholar]
- Ballester-Lopez, A.; Koehorst, E.; Almendrote, M.; Martínez-Piñeiro, A.; Lucente, G.; Linares-Pardo, I.; Núñez-Manchón, J.; Guanyabens, N.; Cano, A.; Lucia, A.; et al. A DM1 family with interruptions associated with atypical symptoms and late onset but not with a milder phenotype. Hum. Mutat. 2020, 41, 420–431. Available online: http://dx.doi.org/10.1002/humu.23932 (accessed on 25 March 2020). [CrossRef] [PubMed]
- Pešović, J.; Perić, S.; Brkušanin, M.; Brajušković, G.; Ević-Stojanović, V.R.; Ević, D.D.-P. Repeat interruptions modify age at onset in myotonic dystrophy type 1 by stabilizing DMPK expansions in somatic cells. Front. Genet. 2018, 9, 1–14. Available online: https://pubmed.ncbi.nlm.nih.gov/30546383/ (accessed on 22 October 2020). [CrossRef]
- Cumming, S.A.; The Scottish Myotonic Dystrophy Consortium; Hamilton, M.J.; Robb, Y.; Gregory, H.; McWilliam, C.; Cooper, A.; Adam, B.; McGhie, J.; Hamilton, G.; et al. De novo repeat interruptions are associated with reduced somatic instability and mild or absent clinical features in myotonic dystrophy type 1. Eur. J. Hum. Genet. 2018, 26, 1635–1647. Available online: http://www.nature.com/articles/s41431-018-0156-9 (accessed on 21 August 2018). [CrossRef] [PubMed]
- Coté, C.; Hiba, B.; Hebert, L.J.; Vial, C.; Remec, J.F.; Janier, M.; Puymirat, J. MRI of tibialis anterior skeletal muscle in myotonic dystrophy type 1. Can. J. Neurol. Sci. 2011, 38, 112–118. Available online: https://pubmed.ncbi.nlm.nih.gov/21156439/ (accessed on 22 October 2020). [CrossRef] [Green Version]
- Iachettini, S.; Valaperta, R.; Marchesi, A.; Perfetti, A.; Cuomo, G.; Fossati, B.; Vaienti, L.; Costa, E.; Meola, G.; Cardani, R. Tibialis anterior muscle needle biopsy and sensitive biomolecular methods: A useful tool in myotonic dystrophy type 1. Eur. J. Histochem. 2015, 59, 243–249. Available online: https://pubmed.ncbi.nlm.nih.gov/26708183/ (accessed on 23 October 2020). [CrossRef] [PubMed] [Green Version]
- Morales, F.; Couto, J.M.; Higham, C.F.; Hogg, G.; Cuenca, P.; Braida, C.; Wilson, R.H.; Adam, B.; Del Valle, G.; Brian, R.; et al. Somatic instability of the expanded CTG triplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait and modifier of disease severity. Hum. Mol. Genet. 2012, 21, 3558–3567. Available online: http://www.ncbi.nlm.nih.gov/pubmed/22595968 (accessed on 26 March 2020). [CrossRef] [Green Version]
- Chong-Nguyen, C.; Wahbi, K.; Algalarrondo, V.; Bécane, H.; Radvanyi-Hoffman, H.; Arnaud, P.; Furling, D.; Bassez, G.; Lazarus, A.; Laforet, P.; et al. Association between Mutation Size and Cardiac Involvement in Myotonic Dystrophy Type 1: An Analysis of the DM1-Heart Registry. Circ. Cardiovasc. Genet. 2017, 10, e001526. Available online: http://www.ncbi.nlm.nih.gov/pubmed/28611030 (accessed on 26 March 2020). [CrossRef] [PubMed] [Green Version]
- Groh, W.J.; Groh, M.R.; Shen, C.; Monckton, D.G.; Bodkin, C.L.; Pascuzzi, R.M. Survival and CTG repeat expansion in adults with myotonic dystrophy type 1. Muscle Nerve 2011, 43, 648–651. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21484823 (accessed on 26 March 2020). [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).

 ,
, 



{kind=link}
{kind=link}