
Automated Pupillometry as an Assessment Tool for Intracranial Hemodynamics in Septic Patients

 , ,
, ,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Transcranial Doppler and CA Assessment
2.4. PLR Assessment
2.5. Study Outcomes
2.6. Statistical Analysis
3. Results
3.1. Study Population and CA
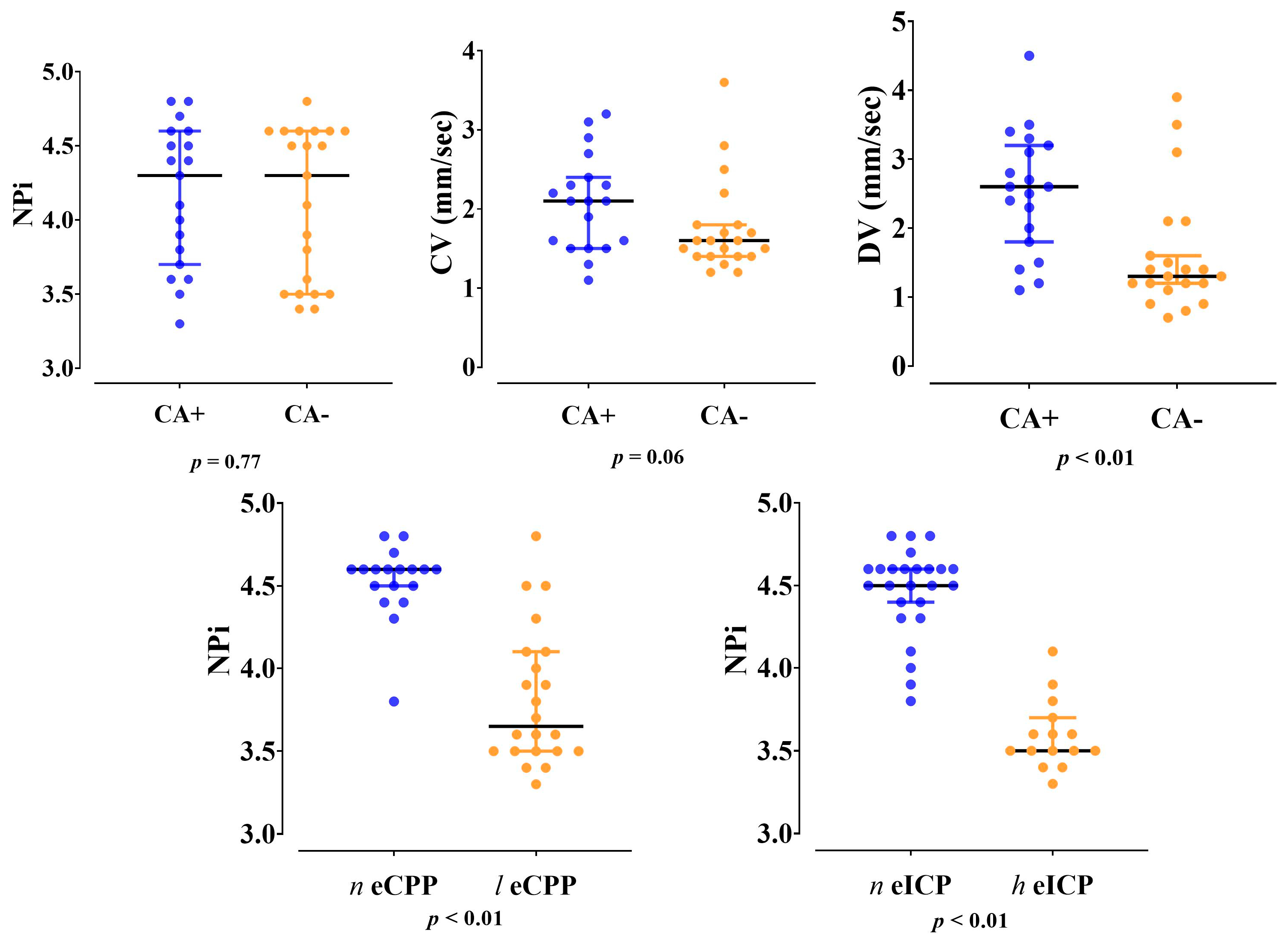
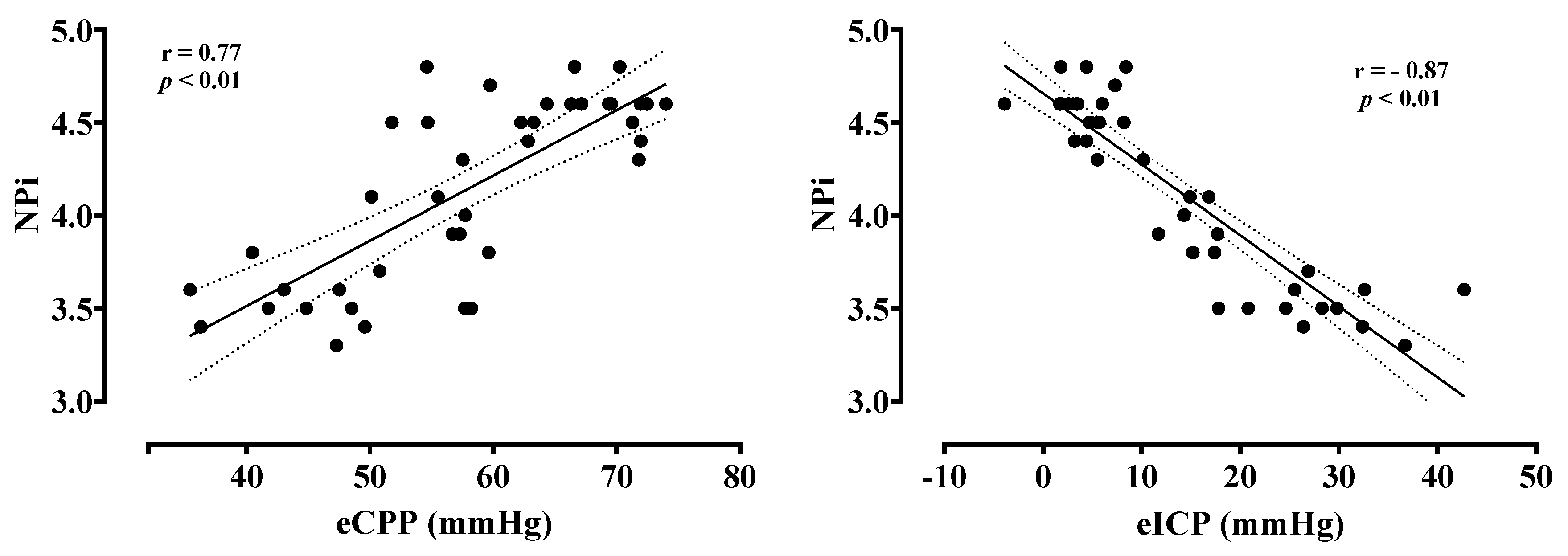
3.2. Automated Pupillometry, eCPP and eICP
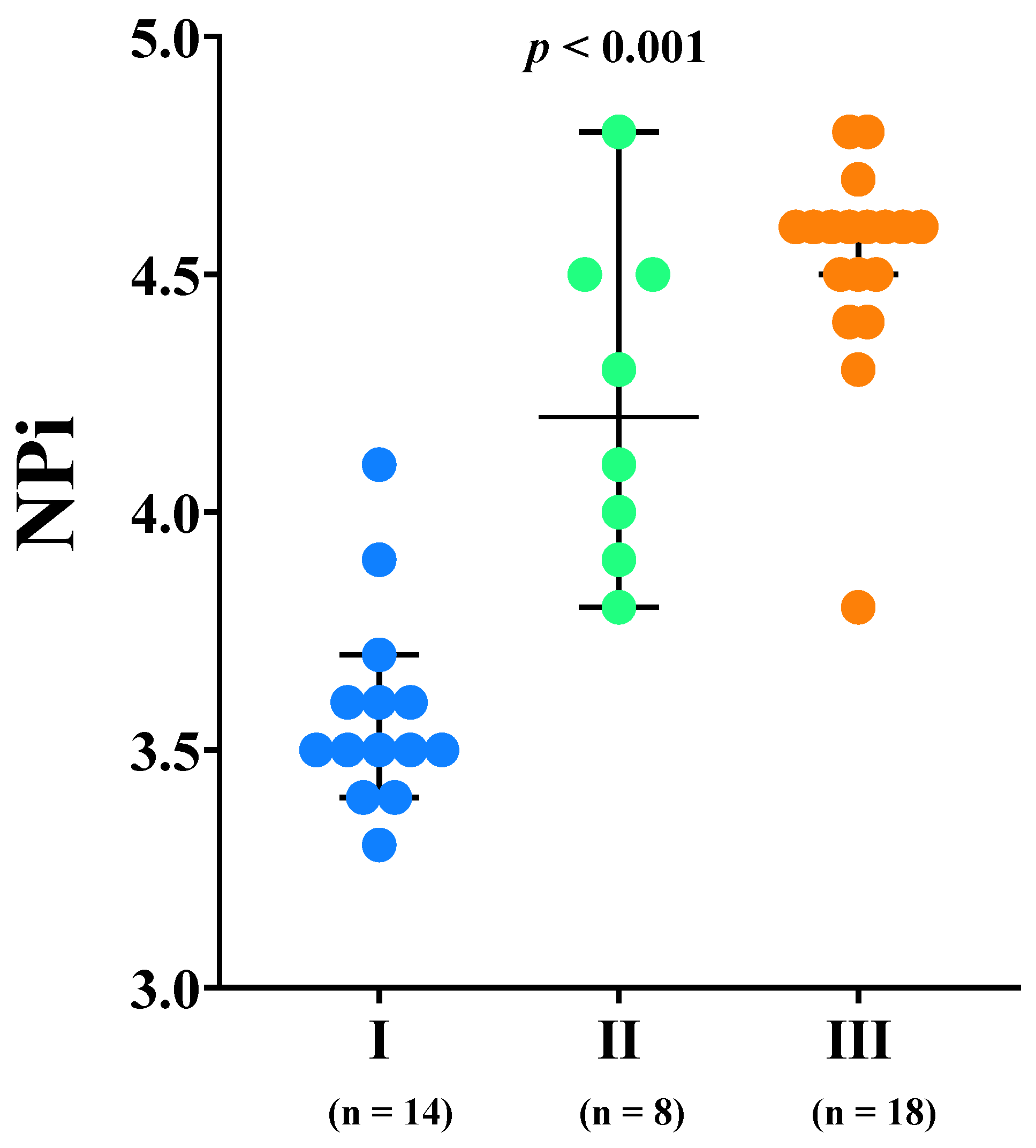
3.3. Primary Outcome
3.4. Secondary Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Crippa, I.A.; Taccone, F.S.; Wittebole, X.; Martin-Loeches, I.; Schroeder, M.E.; François, B.; Kotfis, K.; Ñamendys-Silva, S.A.; Forceville, X.; Solé-Violán, J.; et al. The Prognostic Value of Brain Dysfunction in Critically Ill Patients with and without Sepsis: A. Brain Sci. 2021, 11, 530. [Google Scholar] [CrossRef] [PubMed]
- Robba, C.; Crippa, I.A.; Taccone, F.S. Septic Encephalopathy. Curr. Neurol. Neurosci. Rep. 2018, 18, 82. [Google Scholar] [CrossRef] [PubMed]
- Mazeraud, A.; Righy, C.; Bouchereau, E.; Benghanem, S.; Bozza, F.A.; Sharshar, T. Septic-Associated Encephalopathy: A Comprehensive Review. Neurotherapeutics 2020, 17, 392–403. [Google Scholar] [CrossRef] [PubMed]
- Strandgaard, S.; Sigurdsson, S.T. Last Word on Point:Counterpoint: Sympathetic nervous activity does/does not influence cerebral blood flow. J. Appl. Physiol. 2008, 105, 1375. [Google Scholar] [CrossRef]
- Levine, B.D.; Zhang, R. Comments on Point:Counterpoint: Sympathetic activity does/does not influence cerebral blood flow. Autonomic control of the cerebral circulation is most important for dynamic cerebral autoregulation. J. Appl. Physiol. 2008, 105, 1369–1373. [Google Scholar] [CrossRef]
- Van Lieshout, J.J.; Secher, N.H. Point:Counterpoint: Sympathetic activity does/does not influence cerebral blood flow. Point: Sympathetic activity does influence cerebral blood flow. J. Appl. Physiol. 2008, 105, 1364–1366. [Google Scholar] [CrossRef]
- Ter Laan, M.; van Dijk, J.M.; Elting, J.W.; Staal, M.J.; Absalom, A.R. Sympathetic regulation of cerebral blood flow in humans: A review. Br. J. Anaesth. 2013, 111, 361–367. [Google Scholar] [CrossRef] [Green Version]
- Crippa, I.A.; Subirà, C.; Vincent, J.L.; Fernandez, R.F.; Hernandez, S.C.; Cavicchi, F.Z.; Creteur, J.; Taccone, F.S. Impaired cerebral autoregulation is associated with brain dysfunction in patients with sepsis. Crit. Care 2018, 22, 327. [Google Scholar] [CrossRef] [Green Version]
- Brassard, P.; Labrecque, L.; Smirl, J.D.; Tymko, M.M.; Caldwell, H.G.; Hoiland, R.L.; Lucas, S.J.E.; Denault, A.Y.; Couture, E.J.; Ainslie, P.N. Losing the dogmatic view of cerebral autoregulation. Physiol. Rep. 2021, 9, e14982. [Google Scholar] [CrossRef]
- Kinoshita, K. Traumatic brain injury: Pathophysiology for neurocritical care. J. Intensive Care 2016, 4, 29. [Google Scholar] [CrossRef] [Green Version]
- Goodson, C.M.; Rosenblatt, K.; Rivera-Lara, L.; Nyquist, P.; Hogue, C.W. Cerebral Blood Flow Autoregulation in Sepsis for the Intensivist: Why Its Monitoring May Be the Future of Individualized Care. J. Intensive Care Med. 2018, 33, 63–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenblatt, K.; Walker, K.A.; Goodson, C.; Olson, E.; Maher, D.; Brown, C.H.; Nyquist, P. Cerebral Autoregulation-Guided Optimal Blood Pressure in Sepsis-Associated Encephalopathy: A Case Series. J. Intensive Care Med. 2020, 35, 1453–1464. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Zuckerman, J.H.; Iwasaki, K.; Wilson, T.E.; Crandall, C.G.; Levine, B.D. Autonomic neural control of dynamic cerebral autoregulation in humans. Circulation 2002, 106, 1814–1820. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castro, P.; Serrador, J.; Sorond, F.; Azevedo, E.; Rocha, I. Sympathovagal imbalance in early ischemic stroke is linked to impaired cerebral autoregulation and increased infarct volumes. Auton. Neurosci. 2022, 241, 102986. [Google Scholar] [CrossRef]
- Lavinio, A.; Ene-Iordache, B.; Nodari, I.; Girardini, A.; Cagnazzi, E.; Rasulo, F.; Smielewski, P.; Czosnyka, M.; Latronico, N. Cerebrovascular reactivity and autonomic drive following traumatic brain injury. Acta Neurochir. Suppl. 2008, 102, 3–7. [Google Scholar] [CrossRef]
- Carrara, M.; Ferrario, M.; Bollen Pinto, B.; Herpain, A. The autonomic nervous system in septic shock and its role as a future therapeutic target: A narrative review. Ann. Intensive Care 2021, 11, 80. [Google Scholar] [CrossRef]
- Fernandez, R.; Nardocci, G.; Navarro, C.; Reyes, E.P.; Acuña-Castillo, C.; Cortes, P.P. Neural reflex regulation of systemic inflammation: Potential new targets for sepsis therapy. Front Physiol. 2014, 5, 489. [Google Scholar] [CrossRef]
- Pfister, D.; Siegemund, M.; Dell-Kuster, S.; Smielewski, P.; Rüegg, S.; Strebel, S.P.; Marsch, S.C.; Pargger, H.; Steiner, L.A. Cerebral perfusion in sepsis-associated delirium. Crit. Care 2008, 12, R63. [Google Scholar] [CrossRef] [Green Version]
- Oddo, M.; Taccone, F.S. How to monitor the brain in septic patients? Minerva Anestesiol. 2015, 81, 776–788. [Google Scholar]
- Robba, C.; Cardim, D.; Sekhon, M.; Budohoski, K.; Czosnyka, M. Transcranial Doppler: A stethoscope for the brain-neurocritical care use. J. Neurosci. Res. 2018, 96, 720–730. [Google Scholar] [CrossRef] [Green Version]
- Rasulo, F.A.; Calza, S.; Robba, C.; Taccone, F.S.; Biasucci, D.G.; Badenes, R.; Piva, S.; Savo, D.; Citerio, G.; Dibu, J.R.; et al. Transcranial Doppler as a screening test to exclude intracranial hypertension in brain-injured patients: The IMPRESSIT-2 prospective multicenter international study. Crit. Care 2022, 26, 110. [Google Scholar] [CrossRef] [PubMed]
- Smielewski, P.; Czosnyka, M.; Kirkpatrick, P.; McEroy, H.; Rutkowska, H.; Pickard, J.D. Assessment of cerebral autoregulation using carotid artery compression. Stroke 1996, 27, 2197–2203. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.A.; Chilcott, R.P. Eyeing up the Future of the Pupillary Light Reflex in Neurodiagnostics. Diagnostics 2018, 8, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quispe Cornejo, A.; Fernandes Vilarinho, C.S.; Crippa, I.A.; Peluso, L.; Calabrò, L.; Vincent, J.L.; Creteur, J.; Taccone, F.S. The use of automated pupillometry to assess cerebral autoregulation: A retrospective study. J. Intensive Care 2020, 8, 57. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Purkayastha, S.; Sorond, F. Transcranial Doppler ultrasound: Technique and application. Semin. Neurol. 2012, 32, 411–420. [Google Scholar] [CrossRef] [Green Version]
- Zeiler, F.A.; Donnelly, J.; Calviello, L.; Menon, D.K.; Smielewski, P.; Czosnyka, M. Pressure Autoregulation Measurement Techniques in Adult Traumatic Brain Injury, Part I: A Scoping Review of Intermittent/Semi-Intermittent Methods. J. Neurotrauma 2017, 34, 3207–3223. [Google Scholar] [CrossRef]
- Czosnyka, M.; Matta, B.F.; Smielewski, P.; Kirkpatrick, P.J.; Pickard, J.D. Cerebral perfusion pressure in head-injured patients: A noninvasive assessment using transcranial Doppler ultrasonography. J. Neurosurg. 1998, 88, 802–808. [Google Scholar] [CrossRef]
- Norager, N.H.; Olsen, M.H.; Pedersen, S.H.; Riedel, C.S.; Czosnyka, M.; Juhler, M. Reference values for intracranial pressure and lumbar cerebrospinal fluid pressure: A systematic review. Fluids Barriers CNS 2021, 18, 19. [Google Scholar] [CrossRef]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef] [PubMed]
- Giller, C.A. A bedside test for cerebral autoregulation using transcranial Doppler ultrasound. Acta Neurochir. 1991, 108, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Tibble, R.K.; Girling, K.J.; Mahajan, R.P. A comparison of the transient hyperemic response test and the static autoregulation test to assess graded impairment in cerebral autoregulation during propofol, desflurane, and nitrous oxide anesthesia. Anesth. Analg. 2001, 93, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Cavill, G.; Simpson, E.J.; Mahajan, R.P. Factors affecting assessment of cerebral autoregulation using the transient hyperaemic response test. Br. J. Anaesth. 1998, 81, 317–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Samuels, E.R.; Szabadi, E. Functional neuroanatomy of the noradrenergic locus coeruleus: Its roles in the regulation of arousal and autonomic function part II: Physiological and pharmacological manipulations and pathological alterations of locus coeruleus activity in humans. Curr. Neuropharmacol. 2008, 6, 254–285. [Google Scholar] [CrossRef] [Green Version]
- Pantzaris, N.D.; Platanaki, C.; Tsiotsios, K.; Koniari, I.; Velissaris, D. The Use of Electroencephalography in Patients with Sepsis: A Review of The Literature. J. Transl. Int. Med. 2021, 9, 12–16. [Google Scholar] [CrossRef]
- Couret, D.; Boumaza, D.; Grisotto, C.; Triglia, T.; Pellegrini, L.; Ocquidant, P.; Bruder, N.J.; Velly, L.J. Reliability of standard pupillometry practice in neurocritical care: An observational, double-blinded study. Crit. Care 2016, 20, 99. [Google Scholar] [CrossRef] [Green Version]
- Rollins, M.D.; Feiner, J.R.; Lee, J.M.; Shah, S.; Larson, M. Pupillary effects of high-dose opioid quantified with infrared pupillometry. Anesthesiology 2014, 121, 1037–1044. [Google Scholar] [CrossRef] [Green Version]
- Jahns, F.P.; Miroz, J.P.; Messerer, M.; Daniel, R.T.; Taccone, F.S.; Eckert, P.; Oddo, M. Quantitative pupillometry for the monitoring of intracranial hypertension in patients with severe traumatic brain injury. Crit. Care 2019, 23, 155. [Google Scholar] [CrossRef] [Green Version]
- Osman, M.; Stutzman, S.E.; Atem, F.; Olson, D.; Hicks, A.D.; Ortega-Perez, S.; Aoun, S.G.; Salem, A.; Aiyagari, V. Correlation of Objective Pupillometry to Midline Shift in Acute Stroke Patients. J. Stroke Cerebrovasc. Dis. 2019, 28, 1902–1910. [Google Scholar] [CrossRef]
- Aoun, S.G.; Stutzman, S.E.; Vo, P.N.; El Ahmadieh, T.Y.; Osman, M.; Neeley, O.; Plitt, A.; Caruso, J.P.; Aiyagari, V.; Atem, F.; et al. Detection of delayed cerebral ischemia using objective pupillometry in patients with aneurysmal subarachnoid hemorrhage. J. Neurosurg. 2019, 132, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Papangelou, A.; Zink, E.K.; Chang, W.W.; Frattalone, A.; Gergen, D.; Gottschalk, A.; Geocadin, R.G. Automated Pupillometry and Detection of Clinical Transtentorial Brain Herniation: A Case Series. Mil. Med. 2018, 183, e113–e121. [Google Scholar] [CrossRef] [Green Version]
- Oddo, M.; Sandroni, C.; Citerio, G.; Miroz, J.P.; Horn, J.; Rundgren, M.; Cariou, A.; Payen, J.F.; Storm, C.; Stammet, P.; et al. Quantitative versus standard pupillary light reflex for early prognostication in comatose cardiac arrest patients: An international prospective multicenter double-blinded study. Intensive Care Med. 2018, 44, 2102–2111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.H.; Wu, C.Y.; Liu, C.C.; Hsu, T.C.; Liu, M.A.; Wu, M.C.; Tsai, M.S.; Chang, W.T.; Huang, C.H.; Lee, C.C.; et al. Neuroprognostic Accuracy of Quantitative Versus Standard Pupillary Light Reflex for Adult Postcardiac Arrest Patients: A Systematic Review and Meta-Analysis. Crit. Care Med. 2021, 49, 1790–1799. [Google Scholar] [CrossRef] [PubMed]
- Favre, E.; Bernini, A.; Morelli, P.; Pasquier, J.; Miroz, J.P.; Abed-Maillard, S.; Ben-Hamouda, N.; Oddo, M. Neuromonitoring of delirium with quantitative pupillometry in sedated mechanically ventilated critically ill patients. Crit. Care 2020, 24, 66. [Google Scholar] [CrossRef] [Green Version]
- Peluso, L.; Ferlini, L.; Talamonti, M.; Ndieugnou Djangang, N.; Gouvea Bogossian, E.; Menozzi, M.; Annoni, F.; Macchini, E.; Legros, B.; Severgnini, P.; et al. Automated Pupillometry for Prediction of Electroencephalographic Reactivity in Critically Ill Patients: A Prospective Cohort Study. Front Neurol. 2022, 13, 867603. [Google Scholar] [CrossRef]
- Czempik, P.F.; Pluta, M.P.; Krzych, Ł. Sepsis-Associated Brain Dysfunction: A Review of Current Literature. Int. J. Environ. Res. Public Health 2020, 17, 5852. [Google Scholar] [CrossRef]
- Pfister, D.; Schmidt, B.; Smielewski, P.; Siegemund, M.; Strebel, S.P.; Rüegg, S.; Marsch, S.C.; Pargger, H.; Steiner, L.A. Intracranial pressure in patients with sepsis. Acta Neurochir. Suppl. 2008, 102, 71–75. [Google Scholar] [CrossRef]
- Topcuoglu, M.A. Transcranial Doppler ultrasound in neurovascular diseases: Diagnostic and therapeutic aspects. J. Neurochem. 2012, 123, 39–51. [Google Scholar] [CrossRef] [Green Version]
- Cardim, D.; Robba, C.; Bohdanowicz, M.; Donnelly, J.; Cabella, B.; Liu, X.; Cabeleira, M.; Smielewski, P.; Schmidt, B.; Czosnyka, M. Non-invasive Monitoring of Intracranial Pressure Using Transcranial Doppler Ultrasonography: Is It Possible? Neurocrit. Care 2016, 25, 473–491. [Google Scholar] [CrossRef] [Green Version]
- de Azevedo, D.S.; Salinet, A.S.M.; de Lima Oliveira, M.; Teixeira, M.J.; Bor-Seng-Shu, E.; de Carvalho Nogueira, R. Cerebral hemodynamics in sepsis assessed by transcranial Doppler: A systematic review and meta-analysis. J. Clin. Monit. Comput. 2017, 31, 1123–1132. [Google Scholar] [CrossRef] [PubMed]
- Ritter, A.M.; Muizelaar, J.P.; Barnes, T.; Choi, S.; Fatouros, P.; Ward, J.; Bullock, M.R. Brain stem blood flow, pupillary response, and outcome in patients with severe head injuries. Neurosurgery 1999, 44, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, Y.; Iwasaki, K.; Aoki, K.; Kojima, W.; Kato, J.; Ogawa, S. Dexmedetomidine weakens dynamic cerebral autoregulation as assessed by transfer function analysis and the thigh cuff method. Anesthesiology 2008, 109, 642–650. [Google Scholar] [CrossRef] [Green Version]
- Ogawa, Y.; Iwasaki, K.; Shibata, S.; Kato, J.; Ogawa, S.; Oi, Y. The effect of sevoflurane on dynamic cerebral blood flow autoregulation assessed by spectral and transfer function analysis. Anesth. Analg. 2006, 102, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Harrison, J.M.; Girling, K.J.; Mahajan, R.P. Effects of propofol and nitrous oxide on middle cerebral artery flow velocity and cerebral autoregulation. Anaesthesia 2002, 57, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Harrison, J.M.; Girling, K.J.; Mahajan, R.P. Effects of target-controlled infusion of propofol on the transient hyperaemic response and carbon dioxide reactivity in the middle cerebral artery. Br. J. Anaesth. 1999, 83, 839–844. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, E.T.; McCulloch, J.; O’Kean, M.; Pickard, J.D.; Harper, A.M. Cerebral circulation and norepinephrine: Relevance of the blood-brain barrier. Am. J. Physiol. 1976, 231, 483–488. [Google Scholar] [CrossRef]
- Myburgh, J.A.; Upton, R.N.; Grant, C.; Martinez, A. The cerebrovascular effects of adrenaline, noradrenaline and dopamine infusions under propofol and isoflurane anaesthesia in sheep. Anaesth. Intensive Care 2002, 30, 725–733. [Google Scholar] [CrossRef]
- Froese, L.; Dian, J.; Gomez, A.; Unger, B.; Zeiler, F.A. The cerebrovascular response to norepinephrine: A scoping systematic review of the animal and human literature. Pharmacol. Res. Perspect 2020, 8, e00655. [Google Scholar] [CrossRef]
- Froese, L.; Dian, J.; Batson, C.; Gomez, A.; Alarifi, N.; Unger, B.; Zeiler, F.A. The Impact of Vasopressor and Sedative Agents on Cerebrovascular Reactivity and Compensatory Reserve in Traumatic Brain Injury: An Exploratory Analysis. Neurotrauma Rep. 2020, 1, 157–168. [Google Scholar] [CrossRef]
- Opic, P.; Rüegg, S.; Marsch, S.; Gut, S.S.; Sutter, R. Automated Quantitative Pupillometry in the Critically Ill: A Systematic Review of the Literature. Neurology 2021, 97, e629–e642. [Google Scholar] [CrossRef] [PubMed]
- Opic, P.; Sutter, R. Author Response: Automated Quantitative Pupillometry in the Critically Ill: A Systematic Review of the Literature. Neurology 2021, 97, 1140–1141. [Google Scholar] [CrossRef] [PubMed]
- Taccone, F.S.; Citerio, G. Reader Response: Automated Quantitative Pupillometry in the Critically Ill: A Systematic Review of the Literature. Neurology 2021, 97, 1138–1139. [Google Scholar] [CrossRef]
- Larson, M.D. Reader Response: Automated Quantitative Pupillometry in the Critically Ill: A Systematic Review of the Literature. Neurology 2021, 97, 1140. [Google Scholar] [CrossRef] [PubMed]
- Newell, D.W.; Aaslid, R.; Lam, A.; Mayberg, T.S.; Winn, H.R. Comparison of flow and velocity during dynamic autoregulation testing in humans. Stroke 1994, 25, 793–797. [Google Scholar] [CrossRef] [Green Version]
- Schreiber, S.J.; Gottschalk, S.; Weih, M.; Villringer, A.; Valdueza, J.M. Assessment of blood flow velocity and diameter of the middle cerebral artery during the acetazolamide provocation test by use of transcranial Doppler sonography and MR imaging. AJNR Am. J. Neuroradiol. 2000, 21, 1207–1211. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| All (n = 40) | Intact CA (n = 19) | Impaired CA (n = 21) | p-Value | |
|---|---|---|---|---|
| Age, years | 74 [63–79] | 76 [62–79] | 67 [63–79] | 0.77 |
| Male gender, n (%) | 23 (58) | 10 (53) | 13 (62) | 0.75 |
| APACHE II score | 24 [19–29] | 24 [19–29] | 23 [19–26] | 0.48 |
| Arterial hypertension, n (%) | 7 (18) | 3 (16) | 4 (19) | 1.00 |
| Diabetes, n (%) | 5 (13) | 2 (11) | 3 (14) | 1.00 |
| Coronary artery disease, n (%) | 2 (5) | 1 (5) | 1 (5) | 1.00 |
| COPD, n (%) | 3 (8) | 1 (5) | 2 (10) | 1.00 |
| CKD, n (%) | 1 (3) | 0 (0) | 1 (5) | 1.00 |
| Obesity, n (%) | 13 (33) | 4 (21) | 9 (43) | 0.19 |
| Smoking, n (%) | 4 (10) | 3 (16) | 1 (5) | 0.33 |
Source of infection:
| 14 (35) 16 (40) 4 (10) 6 (15) | 6 (32) 7 (37) 2 (11) 4 (21) | 8 (38) 9 (43) 2 (10) 2 (10) | 0.78 |
| ON THE DAY OF CA ASSESSMENT | ||||
| Heart rate, bpm | 88 [76–103] | 89 [77–112] | 85 [73–98] | 0.22 |
| MAP, mmHg | 71 [66–76] | 71 [67–77] | 72 [66–75] | 0.66 |
| Temperature, °C | 37.2 [36.9–37.6] | 37.1 [36.9–37.4] | 37.2 [37.1–37.7] | 0.29 |
| Mechanical ventilation, n (%) | 36 (90) | 17 (90) | 19 (91) | 1.00 |
| FiO2, % | 55 [50–60] | 55 [50–60] | 55 [48–60] | 0.57 |
| PEEP, cmH2O | 8 [8–10] | 8 [8–10] | 10 [8–10] | 0.36 |
| pH | 7.36 [7.35–7.39] | 7.37 [7.35–7.41] | 7.35 [7.34–7.38] | 0.07 |
| PaO2, mmHg | 91 [69–101] | 95 [74–101] | 91 [64–103] | 0.96 |
| PaCO2, mmHg | 41 [38–44] | 41 [38–43] | 41 [39–45] | 0.35 |
| Lactate, mEq/L | 1.9 [1.5–2.3] | 2.1 [1.8–2.3] | 1.6 [1.1–2.6] | 0.10 |
| Hb, g/dL | 9.1 [8.7–9.9] | 9.2 [8.6–10.0] | 9.1 [8.7–9.6] | 0.75 |
Cardio-active medications
| 38 (95) 8 (10) 7 (18) | 18 (95) 4 (21) 3 (16) | 20 (95) 4 (19) 4 (19) | 0.76 |
| All (n = 40) | Intact CA (n = 19) | Impaired CA (n = 21) | p-Value | |
|---|---|---|---|---|
| FVm, cm/s | 55 [53–62] | 54 [53–61] | 59 [54–65] | 0.60 |
| eCPP, mmHg | 58 [50–67] | 58 [51–67] | 58 [49–70] | 0.83 |
| Low eCPP, n (%) | 22 (55) | 10 (53) | 12 (57) | 1.00 |
| eICP, mmHg | 9 [4–24] | 10 [4–21] | 6 [3–25] | 0.56 |
| High eICP, n (%) | 15 (38) | 7 (37) | 8 (38) | 1.00 |
| NPi | 4.3 [3.6–4.6] | 4.3 [3.7–4.6] | 4.3 [3.5–4.6] | 0.77 |
| Constriction velocity, mm/s | 1.7 [1.5–2.3] | 2.1 [1.5–2.4] | 1.6 [1.4–1.8] | 0.06 |
| Dilation velocity, mm/s | 1.7 [1.2–2.8] | 2.6 [1.8–3.2] | 1.3 [1.2–1.9] | 0.02 |
| Dead at ICU discharge, n (%) | 7 (18) | 5 (26) | 2 (10) | 0.23 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crippa, I.A.; Pelosi, P.; Quispe-Cornejo, A.A.; Messina, A.; Corradi, F.; Taccone, F.S.; Robba, C. Automated Pupillometry as an Assessment Tool for Intracranial Hemodynamics in Septic Patients. Cells 2022, 11, 2206. https://doi.org/10.3390/cells11142206
Crippa IA, Pelosi P, Quispe-Cornejo AA, Messina A, Corradi F, Taccone FS, Robba C. Automated Pupillometry as an Assessment Tool for Intracranial Hemodynamics in Septic Patients. Cells. 2022; 11(14):2206. https://doi.org/10.3390/cells11142206
Chicago/Turabian StyleCrippa, Ilaria Alice, Paolo Pelosi, Armin Alvaro Quispe-Cornejo, Antonio Messina, Francesco Corradi, Fabio Silvio Taccone, and Chiara Robba. 2022. "Automated Pupillometry as an Assessment Tool for Intracranial Hemodynamics in Septic Patients" Cells 11, no. 14: 2206. https://doi.org/10.3390/cells11142206
APA StyleCrippa, I. A., Pelosi, P., Quispe-Cornejo, A. A., Messina, A., Corradi, F., Taccone, F. S., & Robba, C. (2022). Automated Pupillometry as an Assessment Tool for Intracranial Hemodynamics in Septic Patients. Cells, 11(14), 2206. https://doi.org/10.3390/cells11142206