
Endoscopic Delivery of Polymers Reduces Delayed Bleeding after Gastric Endoscopic Submucosal Dissection: A Systematic Review and Meta-Analysis

 , , , ,
, , , , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Selection Process
2.3. Data Extraction
2.4. Quality Assessment
2.5. Inclusion and Exclusion Criteria
2.6. Outcome Assessment
2.7. Statistical Analysis
3. Results
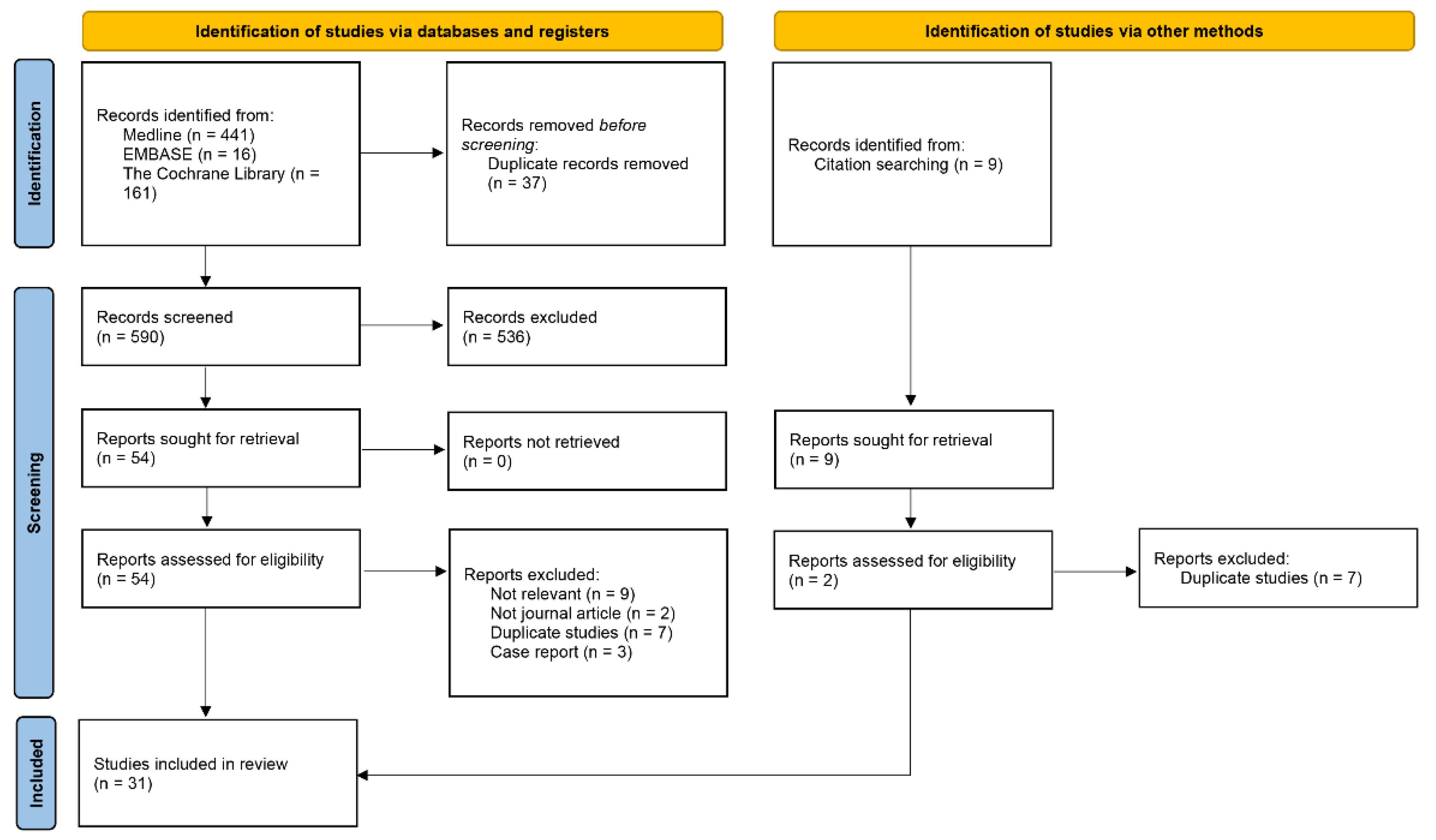
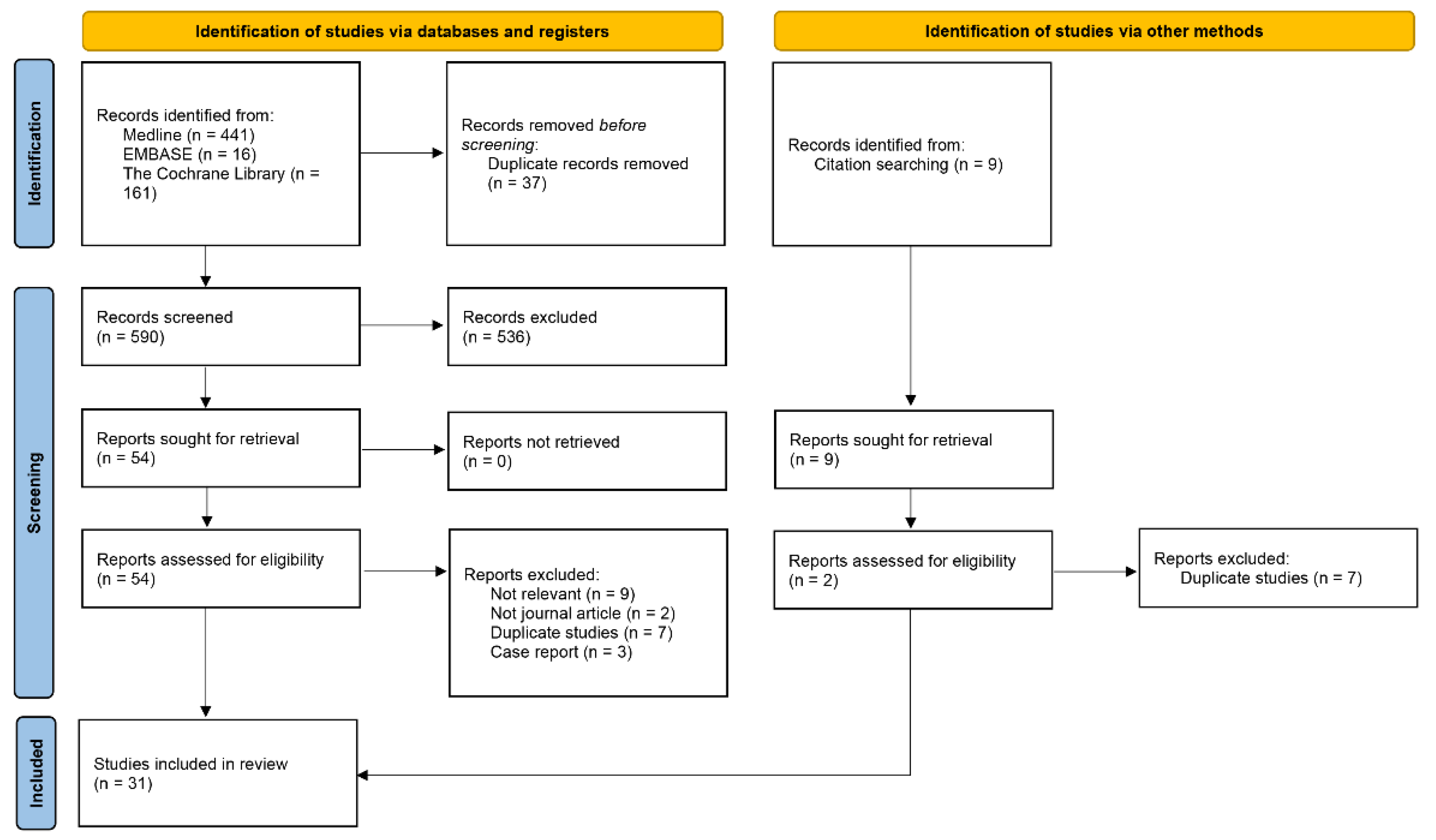
3.1. Identified Studies and Quality
3.2. Non-Comparative Trial Synthesis
3.2.1. Delayed Bleeding Rates
3.2.2. Procedure Time
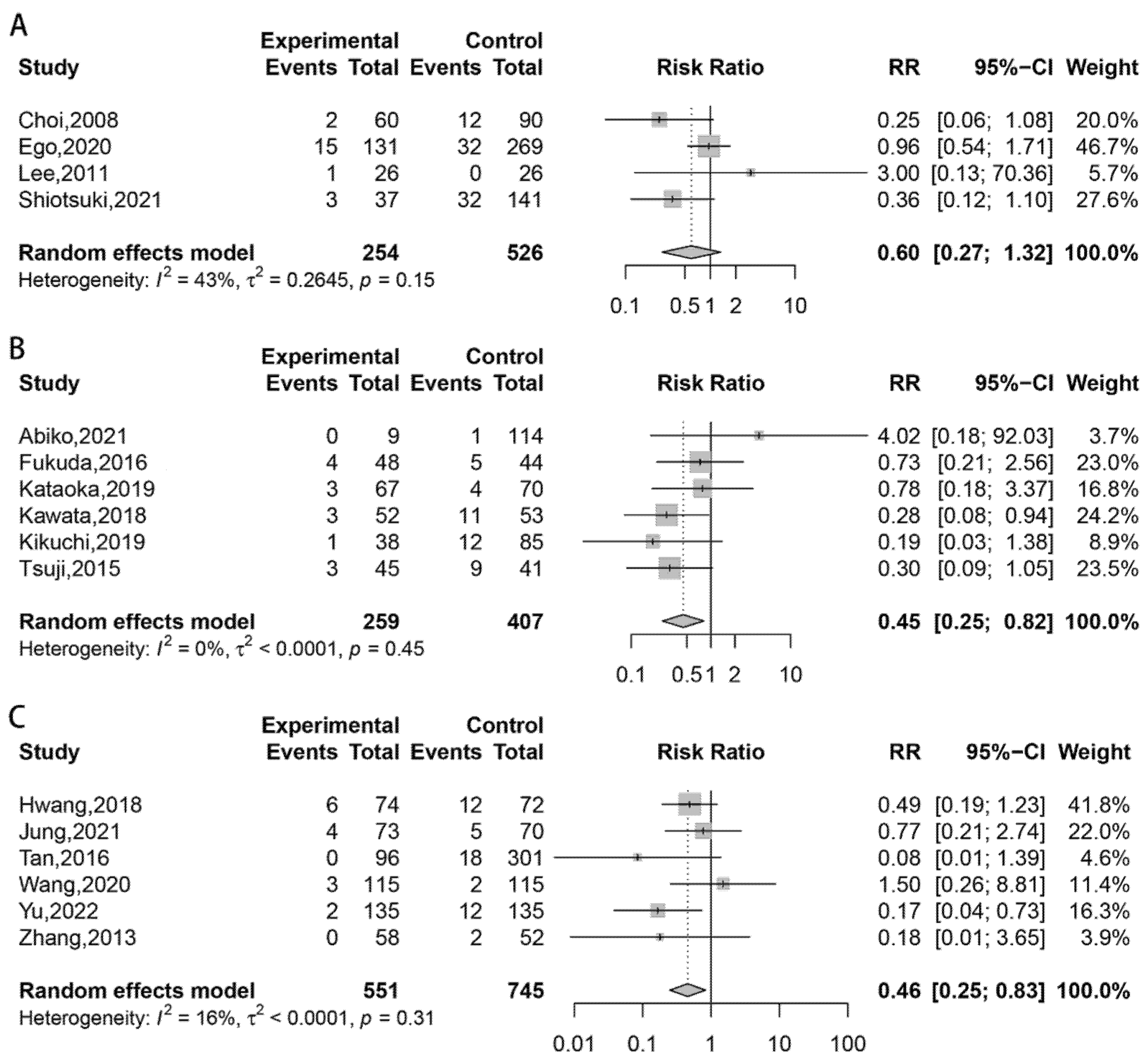
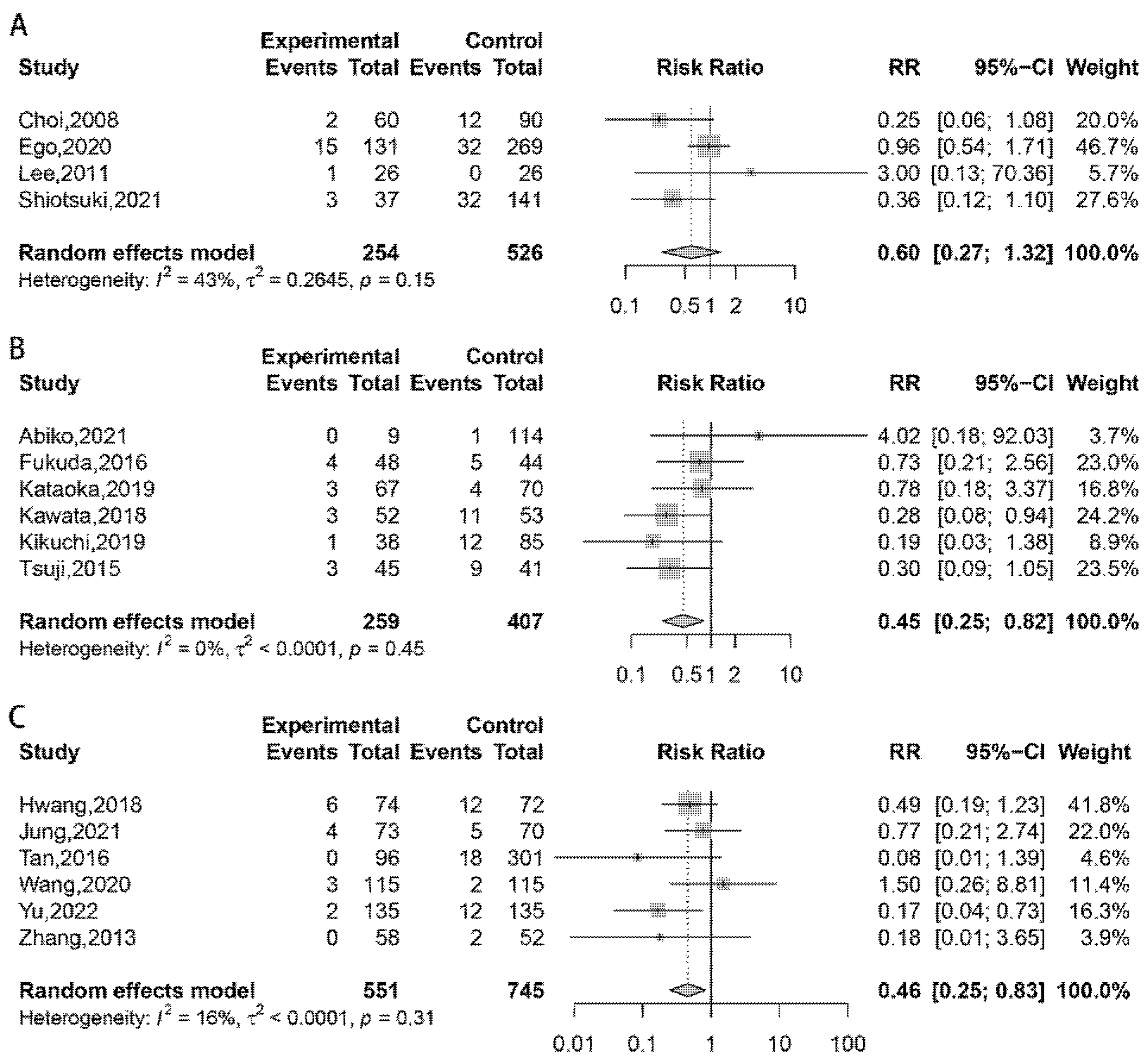
3.3. Pairwise Meta-Analysis Results
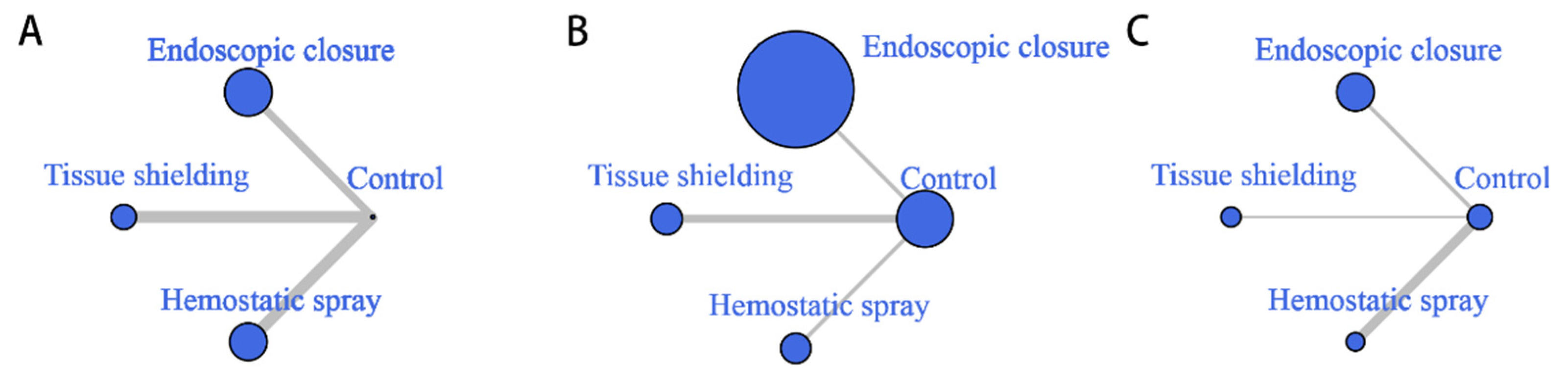
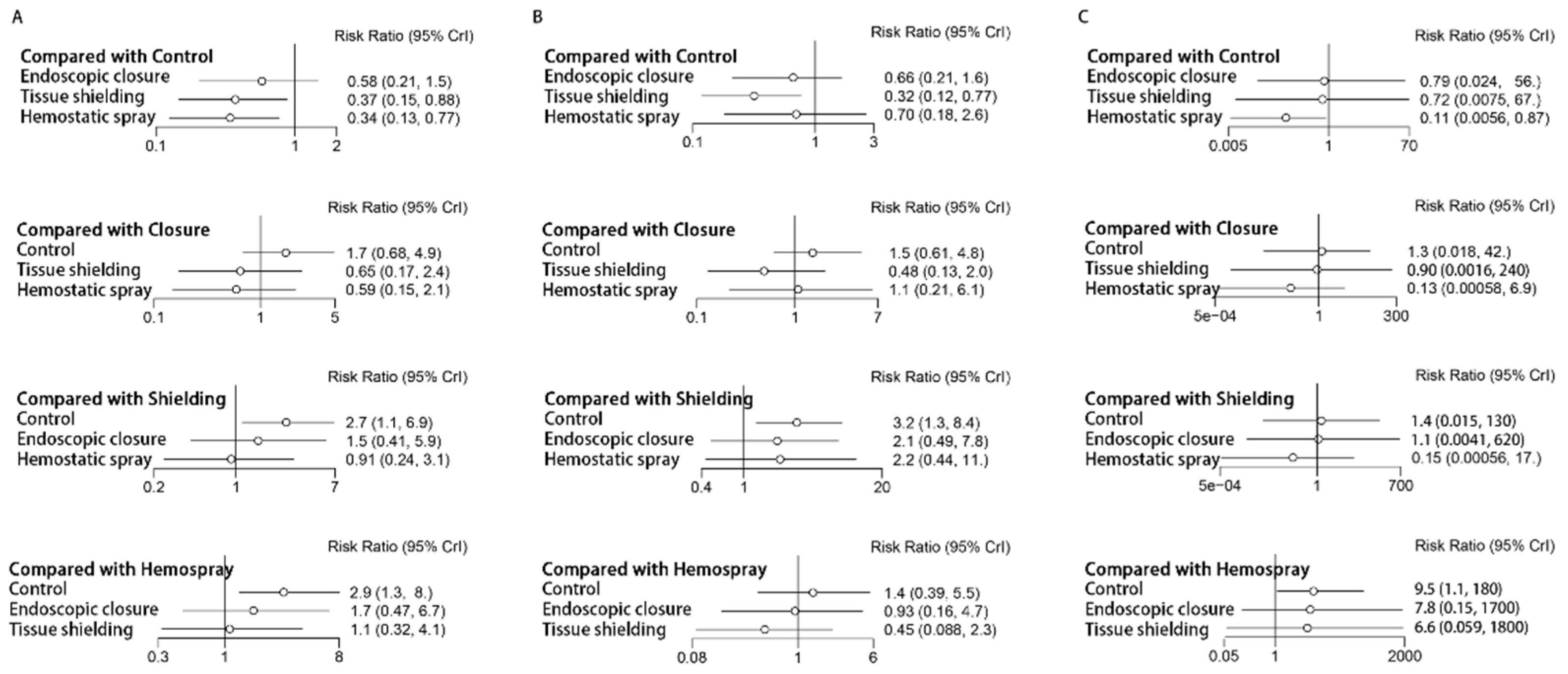
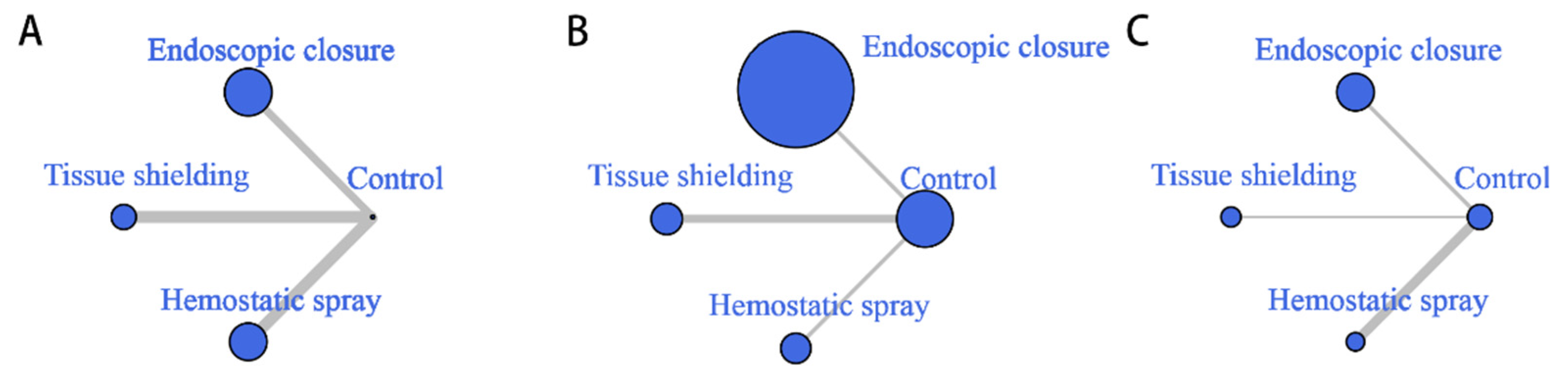
3.4. Network Meta-Analysis Results
3.4.1. Network Quality
3.4.2. Delayed Bleeding Rates
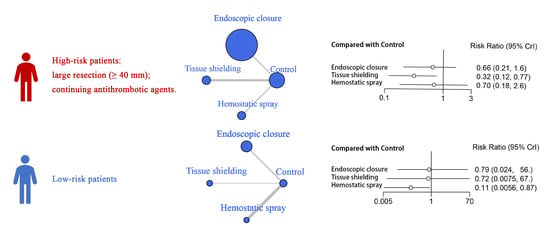
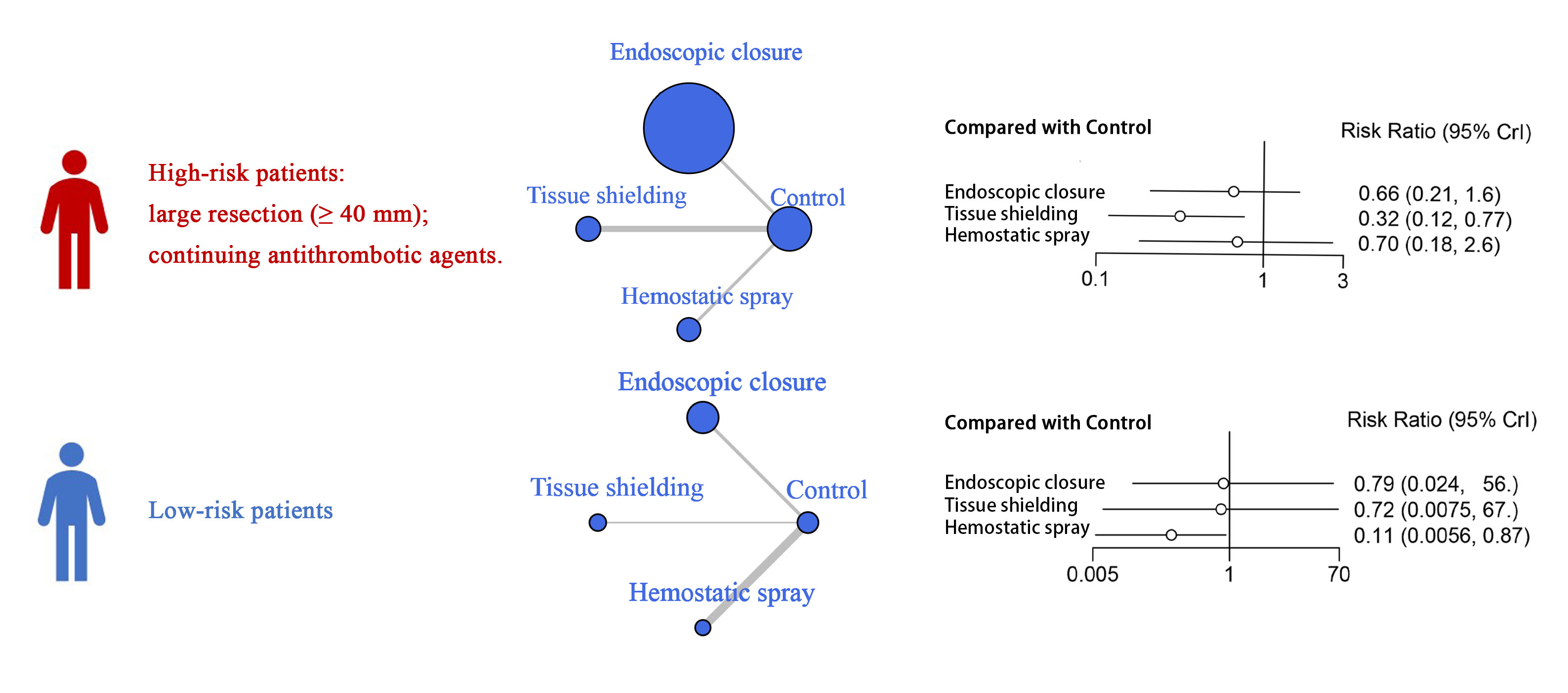
3.4.3. Subgroup Network Analysis
3.4.4. Publication Bias
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Search Strategies
Appendix B

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section and Topic | Item # | Checklist Item | Location Where Item Is Reported |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a systematic review. | Page 1 |
| ABSTRACT | |||
| Abstract | 2 | See the PRISMA 2020 for Abstracts checklist. | Page 2 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of existing knowledge. | Page 2–3 |
| Objectives | 4 | Provide an explicit statement of the objective(s) or question(s) the review addresses. | Page 3 |
| METHODS | |||
| Eligibility criteria | 5 | Specify the inclusion and exclusion criteria for the review and how studies were grouped for the syntheses. | Page 4 |
| Information sources | 6 | Specify all databases, registers, websites, organisations, reference lists and other sources searched or consulted to identify studies. Specify the date when each source was last searched or consulted. | Page 3–4; Appendix A |
| Search strategy | 7 | Present the full search strategies for all databases, registers and websites, including any filters and limits used. | Appendix A |
| Selection process | 8 | Specify the methods used to decide whether a study met the inclusion criteria of the review, including how many reviewers screened each record and each report retrieved, whether they worked independently, and if applicable, details of automation tools used in the process. | Page 4 |
| Data collection process | 9 | Specify the methods used to collect data from reports, including how many reviewers collected data from each report, whether they worked independently, any processes for obtaining or confirming data from study investigators, and if applicable, details of automation tools used in the process. | Page 4 |
| Data items | 10a | List and define all outcomes for which data were sought. Specify whether all results that were compatible with each outcome domain in each study were sought (e.g., for all measures, time points, analyses), and if not, the methods used to decide which results to collect. | Page 4 |
| 10b | List and define all other variables for which data were sought (e.g., participant and intervention characteristics, funding sources). Describe any assumptions made about any missing or unclear information. | Page 4 | |
| Study risk of bias assessment | 11 | Specify the methods used to assess risk of bias in the included studies, including details of the tool(s) used, how many reviewers assessed each study and whether they worked independently, and if applicable, details of automation tools used in the process. | Page 4–5 |
| Effect measures | 12 | Specify for each outcome the effect measure(s) (e.g., risk ratio, mean difference) used in the synthesis or presentation of results. | Page 4–5 |
| Synthesis methods | 13a | Describe the processes used to decide which studies were eligible for each synthesis (e.g., tabulating the study intervention characteristics and comparing against the planned groups for each synthesis (item #5)). | Page 4–5 |
| 13b | Describe any methods required to prepare the data for presentation or synthesis, such as handling of missing summary statistics, or data conversions. | Page 4–5 | |
| 13c | Describe any methods used to tabulate or visually display results of individual studies and syntheses. | Page 4–5 | |
| 13d | Describe any methods used to synthesize results and provide a rationale for the choice(s). If meta-analysis was performed, describe the model(s), method(s) to identify the presence and extent of statistical heterogeneity, and software package(s) used. | Page 4–5 | |
| 13e | Describe any methods used to explore possible causes of heterogeneity among study results (e.g., subgroup analysis, meta-regression). | Page 4–5 | |
| 13f | Describe any sensitivity analyses conducted to assess robustness of the synthesized results. | Not applicable. | |
| Reporting bias assessment | 14 | Describe any methods used to assess risk of bias due to missing results in a synthesis (arising from reporting biases). | Page 4–5 |
| Certainty assessment | 15 | Describe any methods used to assess certainty (or confidence) in the body of evidence for an outcome. | Page 4–5 |
| RESULTS | |||
| Study selection | 16a | Describe the results of the search and selection process, from the number of records identified in the search to the number of studies included in the review, ideally using a flow diagram. | Page 5 |
| 16b | Cite studies that might appear to meet the inclusion criteria, but which were excluded, and explain why they were excluded. | Not applicable. | |
| Study characteristics | 17 | Cite each included study and present its characteristics. | Page 7–11 |
| Risk of bias in studies | 18 | Present assessments of risk of bias for each included study. | Page 5; Supplementary Table S1 |
| Results of individual studies | 19 | For all outcomes, present, for each study: (a) summary statistics for each group (where appropriate) and (b) an effect estimate and its precision (e.g., confidence/credible interval), ideally using structured tables or plots. | Supplementary Figure S2 |
| Results of syntheses | 20a | For each synthesis, briefly summarise the characteristics and risk of bias among contributing studies. | Supplementary Table S1; Supplementary Figure S9 |
| 20b | Present results of all statistical syntheses conducted. If meta-analysis was done, present for each the summary estimate and its precision (e.g., confidence/credible interval) and measures of statistical heterogeneity. If comparing groups, describe the direction of the effect. | Page 12–15 | |
| 20c | Present results of all investigations of possible causes of heterogeneity among study results. | Page 14–15 | |
| 20d | Present results of all sensitivity analyses conducted to assess the robustness of the synthesized results. | Not applicable. | |
| Reporting biases | 21 | Present assessments of risk of bias due to missing results (arising from reporting biases) for each synthesis assessed. | Not applicable. |
| Certainty of evidence | 22 | Present assessments of certainty (or confidence) in the body of evidence for each outcome assessed. | Page 12–15 |
| DISCUSSION | |||
| Discussion | 23a | Provide a general interpretation of the results in the context of other evidence. | Page 15 |
| 23b | Discuss any limitations of the evidence included in the review. | Page 16–17 | |
| 23c | Discuss any limitations of the review processes used. | Page 16–17 | |
| 23d | Discuss implications of the results for practice, policy, and future research. | Page 17 | |
| OTHER INFORMATION | |||
| Registration and protocol | 24a | Provide registration information for the review, including register name and registration number, or state that the review was not registered. | Page 2 |
| 24b | Indicate where the review protocol can be accessed, or state that a protocol was not prepared. | Page 2 | |
| 24c | Describe and explain any amendments to information provided at registration or in the protocol. | Not applicable. | |
| Support | 25 | Describe sources of financial or non-financial support for the review, and the role of the funders or sponsors in the review. | Page 17 |
| Competing interests | 26 | Declare any competing interests of review authors. | Page 17 |
| Availability of data, code and other materials | 27 | Report which of the following are publicly available and where they can be found: template data collection forms; data extracted from included studies; data used for all analyses; analytic code; any other materials used in the review. | Page 17 |
References
- Gotoda, T.; Ho, K.Y.; Soetikno, R.; Kaltenbach, T.; Draganov, P. Gastric ESD: Current status and future directions of devices and training. Gastrointest. Endosc. Clin. N. Am. 2014, 24, 213–233. [Google Scholar] [CrossRef]
- Pimentel-Nunes, P.; Dinis-Ribeiro, M.; Ponchon, T.; Repici, A.; Vieth, M.; De Ceglie, A.; Amato, A.; Berr, F.; Bhandari, P.; Bialek, A.; et al. Endoscopic submucosal dissection: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2015, 47, 829–854. [Google Scholar] [CrossRef] [Green Version]
- Uedo, N.; Takeuchi, Y.; Yamada, T.; Ishihara, R.; Ogiyama, H.; Yamamoto, S.; Kato, M.; Tatsumi, K.; Masuda, E.; Tamai, C.; et al. Effect of a proton pump inhibitor or an H2-receptor antagonist on prevention of bleeding from ulcer after endoscopic submucosal dissection of early gastric cancer: A prospective randomized controlled trial. Am. J. Gastroenterol. 2007, 102, 1610–1616. [Google Scholar] [CrossRef]
- Niimi, K.; Fujishiro, M.; Goto, O.; Kodashima, S.; Minatsuki, C.; Hirayama, I.; Mochizuki, S.; Ono, S.; Yamamichi, N.; Kakushima, N.; et al. Prospective single-arm trial of two-week rabeprazole treatment for ulcer healing after gastric endoscopic submucosal dissection. Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2012, 24, 110–116. [Google Scholar] [CrossRef]
- Takizawa, K.; Oda, I.; Gotoda, T.; Yokoi, C.; Matsuda, T.; Saito, Y.; Saito, D.; Ono, H. Routine coagulation of visible vessels may prevent delayed bleeding after endoscopic submucosal dissection--an analysis of risk factors. Endoscopy 2008, 40, 179–183. [Google Scholar] [CrossRef]
- Park, Y.M.; Cho, E.; Kang, H.Y.; Kim, J.M. The effectiveness and safety of endoscopic submucosal dissection compared with endoscopic mucosal resection for early gastric cancer: A systematic review and metaanalysis. Surg. Endosc. 2011, 25, 2666–2677. [Google Scholar] [CrossRef]
- Nam, H.S.; Choi, C.W.; Kim, S.J.; Kim, H.W.; Kang, D.H.; Park, S.B.; Ryu, D.G. Risk factors for delayed bleeding by onset time after endoscopic submucosal dissection for gastric neoplasm. Sci. Rep. 2019, 9, 2674. [Google Scholar] [CrossRef] [Green Version]
- Okada, K.; Yamamoto, Y.; Kasuga, A.; Omae, M.; Kubota, M.; Hirasawa, T.; Ishiyama, A.; Chino, A.; Tsuchida, T.; Fujisaki, J.; et al. Risk factors for delayed bleeding after endoscopic submucosal dissection for gastric neoplasm. Surg. Endosc. 2011, 25, 98–107. [Google Scholar] [CrossRef]
- Goto, O.; Fujishiro, M.; Oda, I.; Kakushima, N.; Yamamoto, Y.; Tsuji, Y.; Ohata, K.; Fujiwara, T.; Fujiwara, J.; Ishii, N.; et al. A multicenter survey of the management after gastric endoscopic submucosal dissection related to postoperative bleeding. Dig. Dis. Sci. 2012, 57, 435–439. [Google Scholar] [CrossRef]
- Kataoka, Y.; Tsuji, Y.; Hirasawa, K.; Takimoto, K.; Wada, T.; Mochizuki, S.; Ohata, K.; Sakaguchi, Y.; Niimi, K.; Ono, S.; et al. Endoscopic tissue shielding to prevent bleeding after endoscopic submucosal dissection: A prospective multicenter randomized controlled trial. Endoscopy 2019, 51, 619–627. [Google Scholar] [CrossRef]
- Koh, R.; Hirasawa, K.; Yahara, S.; Oka, H.; Sugimori, K.; Morimoto, M.; Numata, K.; Kokawa, A.; Sasaki, T.; Nozawa, A.; et al. Antithrombotic drugs are risk factors for delayed postoperative bleeding after endoscopic submucosal dissection for gastric neoplasms. Gastrointest. Endosc. 2013, 78, 476–483. [Google Scholar] [CrossRef] [PubMed]
- Ono, S.; Fujishiro, M.; Yoshida, N.; Doyama, H.; Kamoshida, T.; Hirai, S.; Kishihara, T.; Yamamoto, Y.; Sakae, H.; Imagawa, A.; et al. Thienopyridine derivatives as risk factors for bleeding following high risk endoscopic treatments: Safe Treatment on Antiplatelets (STRAP) study. Endoscopy 2015, 47, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Yoshio, T.; Nishida, T.; Kawai, N.; Yuguchi, K.; Yamada, T.; Yabuta, T.; Komori, M.; Yamaguchi, S.; Kitamura, S.; Iijima, H.; et al. Gastric ESD under Heparin Replacement at High-Risk Patients of Thromboembolism Is Technically Feasible but Has a High Risk of Delayed Bleeding: Osaka University ESD Study Group. Gastroenterol. Res. Pract. 2013, 2013, 365830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cho, S.J.; Choi, I.J.; Kim, C.G.; Lee, J.Y.; Nam, B.H.; Kwak, M.H.; Kim, H.J.; Ryu, K.W.; Lee, J.H.; Kim, Y.W. Aspirin use and bleeding risk after endoscopic submucosal dissection in patients with gastric neoplasms. Endoscopy 2012, 44, 114–121. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, Y.; Kikuchi, D.; Nagami, Y.; Nonaka, K.; Tsuji, Y.; Fujimoto, A.; Sanomura, Y.; Tanaka, K.; Abe, S.; Zhang, S.; et al. Management of adverse events related to endoscopic resection of upper gastrointestinal neoplasms: Review of the literature and recommendations from experts. Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2019, 31 (Suppl. 1), 4–20. [Google Scholar] [CrossRef]
- Yamamoto, Y.; Yahagi, N.; Yamamoto, H.; Ono, H.; Inoue, H. Innovative therapeutic endoscopy in the upper gastrointestinal tract: Review of Japan Gastroenterological Endoscopic Society Core Sessions. Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2020, 32, 882–887. [Google Scholar] [CrossRef]
- Manoukian, O.S.; Sardashti, N.; Stedman, T.; Gailiunas, K.; Ojha, A.; Penalosa, A.; Mancuso, C.; Hobert, M.; Kumbar, S.G. Biomaterials for Tissue Engineering and Regenerative Medicine. In Encyclopedia of Biomedical Engineering; Narayan, R., Ed.; Elsevier: Oxford, UK, 2019; pp. 462–482. [Google Scholar] [CrossRef]
- Pioche, M.; Camus, M.; Rivory, J.; Leblanc, S.; Lienhart, I.; Barret, M.; Chaussade, S.; Saurin, J.C.; Prat, F.; Ponchon, T. A self-assembling matrix-forming gel can be easily and safely applied to prevent delayed bleeding after endoscopic resections. Endosc. Int. Open 2016, 4, E415–E419. [Google Scholar] [CrossRef] [Green Version]
- Tan, E.S.; Wang, H.; Lua, G.W.; Liu, F.; Shi, X.G.; Li, Z.S. Fibrin Glue Spray as a Simple and Promising Method to Prevent Bleeding after Gastric Endoscopic Submucosal Dissection. Dig. Surg. 2016, 33, 455–461. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.htm (accessed on 29 April 2022).
- Krishnamoorthi, R.; Mohan, B.P.; Jayaraj, M.; Wang, K.K.; Katzka, D.A.; Ross, A.; Adler, D.G.; Iyer, P.G. Risk of progression in Barrett’s esophagus indefinite for dysplasia: A systematic review and meta-analysis. Gastrointest. Endosc. 2020, 91, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological quality and synthesis of case series and case reports. BMJ Evid.-Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [Green Version]
- Shim, S.R.; Kim, S.J.; Lee, J.; Rücker, G. Network meta-analysis: Application and practice using R software. Epidemiol. Health 2019, 41, e2019013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, C.; Sayed, T. Random parameters Bayesian hierarchical modeling of traffic conflict extremes for crash estimation. Accid. Anal. Prev. 2021, 157, 106159. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Akimoto, T.; Goto, O.; Sasaki, M.; Mizutani, M.; Tsutsumi, K.; Kiguchi, Y.; Takatori, Y.; Nakayama, A.; Kato, M.; Fujimoto, A.; et al. Endoscopic hand suturing for mucosal defect closure after gastric endoscopic submucosal dissection may reduce the risk of postoperative bleeding in patients receiving antithrombotic therapy. Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2022, 34, 123–132. [Google Scholar] [CrossRef]
- Choi, K.D.; Jung, H.Y.; Lee, G.H.; Oh, T.H.; Jo, J.Y.; Song, H.J.; Hong, S.S.; Kim, J.H. Application of metal hemoclips for closure of endoscopic mucosal resection-induced ulcers of the stomach to prevent delayed bleeding. Surg. Endosc. 2008, 22, 1882–1886. [Google Scholar] [CrossRef]
- Ego, M.; Abe, S.; Nonaka, S.; Suzuki, H.; Yoshinaga, S.; Oda, I.; Saito, Y. Endoscopic Closure Utilizing Endoloop and Endoclips After Gastric Endoscopic Submucosal Dissection for Patients on Antithrombotic Therapy. Dig. Dis. Sci. 2020, 66, 2336–2344. [Google Scholar] [CrossRef]
- Goto, O.; Sasaki, M.; Akimoto, T.; Ochiai, Y.; Kiguchi, Y.; Mitsunaga, Y.; Fujimoto, A.; Maehata, T.; Nishizawa, T.; Takeuchi, H.; et al. Endoscopic hand-suturing for defect closure after gastric endoscopic submucosal dissection: A pilot study in animals and in humans. Endoscopy 2017, 49, 792–797. [Google Scholar] [CrossRef] [PubMed]
- Goto, O.; Oyama, T.; Ono, H.; Takahashi, A.; Fujishiro, M.; Saito, Y.; Abe, S.; Kaise, M.; Iwakiri, K.; Yahagi, N. Endoscopic hand-suturing is feasible, safe, and may reduce bleeding risk after gastric endoscopic submucosal dissection: A multicenter pilot study (with video). Gastrointest. Endosc. 2020, 91, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Han, S.; Wani, S.; Edmundowicz, S.A.; Soetikno, R.; Hammad, H. Feasibility of endoscopic suturing to prevent adverse events and hospitalization after endoscopic submucosal dissection. Endosc. Int. Open 2020, 8, E1212–E1217. [Google Scholar] [CrossRef] [PubMed]
- Kantsevoy, S.V.; Bitner, M.; Mitrakov, A.A.; Thuluvath, P.J. Endoscopic suturing closure of large mucosal defects after endoscopic submucosal dissection is technically feasible, fast, and eliminates the need for hospitalization (with videos). Gastrointest. Endosc. 2014, 79, 503–507. [Google Scholar] [CrossRef]
- Lee, B.I.; Kim, B.W.; Kim, H.K.; Choi, H.; Ji, J.S.; Hwang, S.M.; Cho, Y.S.; Chae, H.S.; Choi, K.Y. Routine mucosal closure with a detachable snare and clips after endoscopic submucosal dissection for gastric epithelial neoplasms: A randomized controlled trial. Gut Liver 2011, 5, 5–454. [Google Scholar] [CrossRef] [Green Version]
- Maekawa, S.; Nomura, R.; Murase, T.; Ann, Y.; Harada, M. Complete closure of artificial gastric ulcer after endoscopic submucosal dissection by combined use of a single over-the-scope clip and through-the-scope clips (with videos). Surg. Endosc. 2015, 29, 500–504. [Google Scholar] [CrossRef] [Green Version]
- Nishiyama, N.; Kobara, H.; Kobayashi, N.; Chiyo, T.; Tada, N.; Kozuka, K.; Matsui, T.; Yachida, T.; Fujihara, S.; Shi, T.T.; et al. Efficacy of endoscopic ligation with O-ring closure for preventing gastric post- ESD bleeding under antithrombotic therapy: A prospective observational study. Endoscopy 2022, 52, E413–E414. [Google Scholar] [CrossRef]
- Shiotsuki, K.; Takizawa, K.; Notsu, A.; Kakushima, N.; Kawata, N.; Yoshida, M.; Yabuuchi, Y.; Kishida, Y.; Ito, S.; Imai, K.; et al. Endoloop closure following gastric endoscopic submucosal dissection to prevent delayed bleeding in patients receiving antithrombotic therapy. Scand. J. Gastroenterol. 2021, 56, 1117–1125. [Google Scholar] [CrossRef]
- Yoshida, A.; Kurumi, H.; Ikebuchi, Y.; Kawaguchi, K.; Yashima, K.; Kamitani, Y.; Yasui, S.; Nakada, Y.; Kanda, T.; Takata, T.; et al. New Closure Method Using Loop and Open-Close Clips after Endoscopic Submucosal Dissection of Stomach and Colon Lesions. J. Clin. Med. 2021, 10, 3260. [Google Scholar] [CrossRef]
- Abiko, S.; Oda, S.; Meno, A.; Shido, A.; Yoshida, S.; Yoshikawa, A.; Harada, K.; Kawagishi, N.; Sano, I.; Oda, H.; et al. Feasibility of a modified search, coagulation, and clipping method with and without the use of polyglycolic acid sheets and fibrin glue for preventing delayed bleeding after gastric endoscopic submucosal dissection. BMC Gastroenterol. 2021, 21, 63. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, H.; Yamaguchi, N.; Isomoto, H.; Matsushima, K.; Minami, H.; Akazawa, Y.; Ohnita, K.; Takeshima, F.; Shikuwa, S.; Nakao, K. Polyglycolic Acid Felt Sealing Method for Prevention of Bleeding Related to Endoscopic Submucosal Dissection in Patients Taking Antithrombotic Agents. Gastroenterol. Res. Pract. 2016, 2016, 1457357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawata, N.; Ono, H.; Takizawa, K.; Kakushima, N.; Tanaka, M.; Igarashi, K.; Yoshida, M.; Kishida, Y.; Iwai, T.; Ito, S.; et al. Efficacy of polyglycolic acid sheets and fibrin glue for prevention of bleeding after gastric endoscopic submucosal dissection in patients under continued antithrombotic agents. Gastric Cancer Off. J. Int. Gastric Cancer Assoc. Jpn. Gastric Cancer Assoc. 2018, 21, 696–702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kikuchi, D.; Iizuka, T.; Makino, S.; Hayasaka, J.; Odagiri, H.; Ochiai, Y.; Suzuki, Y.; Nomura, K.; Ohkura, Y.; Okamoto, Y.; et al. Utility of autologous fibrin glue and polyglycolic acid sheet for preventing delayed bleeding associated with antithrombotic therapy after gastric ESD. Endosc. Int. Open 2019, 7, E1542–E1548. [Google Scholar] [CrossRef] [Green Version]
- Kobayashi, N.; Kobara, H.; Nishiyama, N.; Fujihara, S.; Kozuka, K.; Tada, N.; Matsui, T.; Chiyo, T.; Takata, T.; Fujita, K.; et al. Wafer paper and ring-mounted polyglycolic acid sheet method for shielding artificial gastric floor. Minim. Invasive Ther. Allied Technol. 2021, 33, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Mori, H.; Guan, Y.; Kobara, H.; Kobayashi, S.; Nishiyama, N.; Kobayashi, N.; Masaki, T. Efficacy of innovative polyglycolic acid sheet device delivery station system: A randomized prospective study. Surg. Endosc. 2018, 32, 3076–3086. [Google Scholar] [CrossRef] [Green Version]
- Tsuji, Y.; Fujishiro, M.; Kodashima, S.; Ono, S.; Niimi, K.; Mochizuki, S.; Asada-Hirayama, I.; Matsuda, R.; Minatsuki, C.; Nakayama, C.; et al. Polyglycolic acid sheets and fibrin glue decrease the risk of bleeding after endoscopic submucosal dissection of gastric neoplasms (with video). Gastrointest. Endosc. 2015, 81, 906–912. [Google Scholar] [CrossRef]
- Haddara, S.; Jacques, J.; Lecleire, S.; Branche, J.; Leblanc, S.; Le Baleur, Y.; Privat, J.; Heyries, L.; Bichard, P.; Granval, P.; et al. A novel hemostatic powder for upper gastrointestinal bleeding: A multicenter study (the “GRAPHE” registry). Endoscopy 2016, 48, 1084–1095. [Google Scholar] [CrossRef]
- Hahn, K.Y.; Park, J.C.; Lee, Y.K.; Shin, S.K.; Lee, S.K.; Lee, Y.C. Efficacy of hemostatic powder in preventing bleeding after gastric endoscopic submucosal dissection in high-risk patients. J. Gastroenterol. Hepatol. 2018, 33, 656–663. [Google Scholar] [CrossRef]
- Hwang, J.J.; Hong, S.J.; Han, J.P.; Ko, B.M.; Lee, T.H.; Lee, J.S. Efficacy of Surgicel® (Fibrillar) for preventing bleeding after endoscopic submucosal dissection for gastric epithelial tumors. J. Dig. Dis. 2018, 19, 657–663. [Google Scholar] [CrossRef]
- Jung, D.H.; Moon, H.S.; Park, C.H.; Park, J.C. Polysaccharide hemostatic powder to prevent bleeding after endoscopic submucosal dissection in high risk patients: A randomized controlled trial. Endoscopy 2021, 53, 994–1002. [Google Scholar] [CrossRef]
- Subramaniam, S.; Kandiah, K.; Thayalasekaran, S.; Longcroft-Wheaton, G.; Bhandari, P. Haemostasis and prevention of bleeding related to ER: The role of a novel self-assembling peptide. United Eur. Gastroenterol. J. 2019, 7, 155–162. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wu, Q.; Yan, Y.; Li, S.J.; Yuan, P.; Cao, C.Q.; Niu, D.F.; Li, Z.Y.; Bu, Z.D.; Ji, J.F. Effectiveness of fibrin sealant as hemostatic technique in accelerating ESD-induced ulcer healing: A retrospective study. Surg. Endosc. 2020, 34, 1191–1199. [Google Scholar] [CrossRef]
- Yu, Y.; Hu, T.; Kuai, X.; Liu, X.; Li, R.; Zhou, C. Propensity score matching analysis to evaluate efficacy of polyethylene oxide adhesive on preventing delayed bleeding after gastric endoscopic submucosal dissection. Sci. Rep. 2022, 12, 4538. [Google Scholar] [CrossRef]
- Zhang, Y.; Chen, Y.; Qu, C.Y.; Zhou, M.; Ni, Q.W.; Xu, L.M. Effects of medical adhesives in prevention of complications after endoscopic submucosal dissection. World J. Gastroenterol. 2013, 19, 2704–2708. [Google Scholar] [CrossRef]
- Uraoka, T.; Ochiai, Y.; Fujimoto, A.; Goto, O.; Kawahara, Y.; Kobayashi, N.; Kanai, T.; Matsuda, S.; Kitagawa, Y.; Yahagi, N. A novel fully synthetic and self-assembled peptide solution for endoscopic submucosal dissection-induced ulcer in the stomach. Gastrointest. Endosc. 2016, 83, 1259–1264. [Google Scholar] [CrossRef]
- van Valkenhoef, G.; Dias, S.; Ades, A.E.; Welton, N.J. Automated generation of node-splitting models for assessment of inconsistency in network meta-analysis. Res. Synth. Methods 2016, 7, 80–93. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Xiong, F.; Xu, Z.L.; Zhang, D.G.; Yao, J.; Wang, L.S. Polyglycolic acid sheets decrease post-endoscopic submucosal dissection bleeding in early gastric cancer: A systematic review and meta-analysis. J. Dig. Dis. 2020, 21, 437–444. [Google Scholar] [CrossRef]
- Kouketsu, A.; Nogami, S.; Fujiwara, M.; Mori, S.; Yamauchi, K.; Hashimoto, W.; Miyashita, H.; Kurihara, J.; Kawai, T.; Higuchi, K.; et al. Clinical evaluations of autologous fibrin glue and polyglycolic acid sheets as oral surgical wound coverings after partial glossectomy. J. Craniomaxillofac. Surg. 2016, 44, 964–968. [Google Scholar] [CrossRef]
- Suzuki, K.; Kawauchi, A.; Nakamura, T.; Itoi, S.; Ito, T.; So, J.; Ukimura, O.; Hagiwara, A.; Yamagishi, H.; Miki, T. Histologic and electrophysiological study of nerve regeneration using a polyglycolic acid-collagen nerve conduit filled with collagen sponge in canine model. Urology 2009, 74, 958–963. [Google Scholar] [CrossRef]
- Takao, T.; Takegawa, Y.; Shinya, N.; Tsudomi, K.; Oka, S.; Ono, H. Tissue shielding with polyglycolic acid sheets and fibrin glue on ulcers induced by endoscopic submucosal dissection in a porcine model. Endosc Int Open 2015, 3, E146–E151. [Google Scholar] [CrossRef] [Green Version]
- Ceonzo, K.; Gaynor, A.; Shaffer, L.; Kojima, K.; Vacanti, C.A.; Stahl, G.L. Polyglycolic acid-induced inflammation: Role of hydrolysis and resulting complement activation. Tissue Eng. 2006, 12, 301–308. [Google Scholar] [CrossRef]
- Murakami, D.; Harada, H.; Amano, Y.; Yamato, M. Do polyglycolic acid sheets really prevent bleeding after endoscopic submucosal dissection? An opinion from physiological viewpoints. Endoscopy 2020, 52, 76. [Google Scholar] [CrossRef]
- Oda, R.; Okuda, K.; Yamada, T.; Yukiue, H.; Fukai, I.; Kawano, O.; Matsui, T.; Tatematsu, T.; Yokota, K.; Nakanishi, R. Comparison of the efficacy of novel two covering methods for spontaneous pneumothorax: A multi-institutional study. BMJ Open Respir. Res. 2022, 9, e001231. [Google Scholar] [CrossRef]
- Mori, H.; Kobara, H.; Nishiyama, N.; Masaki, T. Novel concept of endoscopic device delivery station system for rapid and tight attachment of polyglycolic acid sheet. World J. Gastroenterol. 2018, 24, 211–215. [Google Scholar] [CrossRef]
- Chedgy, F.; Bhattacharyya, R.; Kandiah, K.; Kumar, A.; Bhandari, P. OC-025 Endoclot polysaccharide haemostatic system to reduce delayed bleeding following upper and lower gastrointestinal resection—Preliminary results of the haemostop study. Gut 2015, 64, A13. [Google Scholar] [CrossRef]
- Becker, J.C.; Beckbauer, M.; Domschke, W.; Herbst, H.; Pohle, T. Fibrin glue, healing of gastric mucosal injury, and expression of growth factors: Results from a human in vivo study. Gastrointest. Endosc. 2005, 61, 560–567. [Google Scholar] [CrossRef]
- Kobara, H.; Fujihara, S. Advanced endoscopic gastric defect closure: Preventive effects on post-endoscopic submucosal dissection bleeding. Dig. Endosc. Off. J. Jpn. Gastroenterol. Endosc. Soc. 2022, 34, 483–484. [Google Scholar] [CrossRef]

| Article (Author, Year) | Country | Design | No. of Centers | Sample Size | Patient Characteristics | Additional Procedure Time (Mean ± SD) | Study Group Intervention | Control Group Intervention | Follow-Up Time |
|---|---|---|---|---|---|---|---|---|---|
| Abiko, 2021 [43] | Japan | Retrospective case series | single | 123 | High risk in treatment group and low risk in control group | 55.33 ± 16.62 | Modified search, coagulation, and clipping method (HX-610-135S; Olympus, Tokyo, Japan) + PGA (Neoveil; Gunze Co., Tokyo, Japan) + fibrin glue (Beriplast P combi-set; CSL Behring Pharma, Tokyo, Japan) (PMSCC) | Modified search, coagulation, and clipping (HX-610-135S; Olympus, Tokyo, Japan) method (MSCC) | 7 days |
| Akimoto, 2021 [31] | Japan | Prospective, single-arm study | single | 20 | High risk | 38.36 ± 10.56 | Endoscopic hand suturing (EHS) (VLOCL0604; Covidien, Mansfield, MA, USA) | NA | 4 weeks |
| Choi, 2008 [32] | Korea | Retrospective cohort study | single | 150 | Low risk | 18.00 ± 7.78 | Hemoclips (HX600-090L; Olympus, Tokyo, Japan) | Heat probe coagulation, coagulation forceps, argon plasma coagulation (APC), and/or hemoclips (HX600-090L; Olympus, Tokyo, Japan) | 2 days |
| Ego, 2020 [33] | Japan | Retrospective cohort study | single | 400 | High risk | 23.50 ± 10.80 | Endoloop (MAJ-254; Olympus Medical, Tokyo, Japan) and Endoclips (HX-610-090, Olympus Medical, Tokyo, Japan or ZEOCLIP ZP-CH, Zeon medical, Tokyo, Japan) | Coagulation using hemostatic forceps | 56 days |
| Fukuda, 2016 [44] | Japan | Retrospective cohort study | single | 92 | Low risk | NA | PGA (Neoveil; Gunze Co., Tokyo, Japan) + fibrin glue (Beriplast P combi-set; CSL Behring Pharma, Tokyo, Japan); modified clip-and-pull method | Non-sealing | ≥40 days |
| Goto, 2020 [35] | Japan | Prospective, single-arm study | multiple | 30 | Mixed and grouped | 46.20 ± 17.00 | EHS (VLOCL0604; Covidien, Mansfield, MA, USA) | NA | 3–4 weeks |
| Goto, 2017 [34] | Japan | Prospective case series | single | 18 | NA | NA | EHS (VLOCL0604; Covidien, Mansfield, MA, USA) | NA | 4 weeks |
| Haddara, 2016 [50] | France | Retrospective case series | multiple | 2 | Mixed | NA | TC-325 hemostatic powder (Hemospray; Cook Medical, Winston-Salem, NC, USA) | NA | 30 days |
| Hahn, 2017 [51] | Korea | Prospective, single-arm study | single | 44 | High risk | NA | Polysaccharide hemostatic powder (EndoClot; Endo-Clot Plus, Inc., Santa Clara, CA, USA) | NA | 4 weeks |
| Han, 2020 [36] | USA | Prospective cohort study | single | 18 | Mixed | 13.40 ± 5.90 | Endoscopic overstitch suturing (Apollo Endosurgery Inc., Austin, TX, USA) | NA | 6 months |
| Hwang, 2018 [52] | Korea | RCT | single | 146 | Low risk | NA | Polyanhydroglucuronic acid gauze (Surgicel; Ethicon Inc., Johnson and Johnson, Somerville, NJ, USA) | Hemostatic forceps and hemostatic clips (HX-610-135 or HX-610-090L; Olympus, Tokyo, Japan) | 7 days |
| Jung, 2021 [53] | Korea | RCT | multiple | 143 | High risk | <2 | Polysaccharide hemostatic powder (EndoClot; Endo-Clot Plus, Inc., Santa Clara, CA, USA) | Hemostatic forceps and hemostatic clip | 4 weeks |
| Kantsevoy, 2014 [37] | USA | Retrospective case series | single | 4 | NA | 10.00 ± 5.80 | Endoscopic overstitch suturing (Apollo Endosurgery Inc., Austin, TX, USA) | NA | 3 months |
| Kataoka, 2019 [10] | Japan | RCT | multiple | 137 | High risk | 25.50 ± 15.00 | PGA (Neoveil; Gunze Co., Osaka, Japan) + fibrin glue (Beriplast P Combi-Set; CSL Behring Pharma, Tokyo, Japan); step-by-step method, clip-and-pull method | Coagulation using hemostatic forceps | 28 days |
| Kawata, 2018 [45] | Japan | Retrospective cohort study | single | 105 | High risk | 21.00 ± 10.41 | PGA (Neoveil; Gunze, Kyoto, Japan) + fibrin glue (Beriplast P Combi-Set; CSL Behring Pharma, Tokyo, Japan); original method | Coagulation using hemostatic forceps | ≥20 days |
| Kikuchi, 2019 [46] | Japan | Retrospective cohort study | single | 123 | High risk | NA | PGA (Neoveil; Gunze Co., Kyoto, Japan) + autologous fibrin glue; clip-and-pull method | Coagulation using hemostatic forceps | 8 weeks |
| Kobayashi, 2021 [47] | Japan | Retrospective case series | single | 24 | High risk | 10.50 ± 6.70 | Wafer paper and ring-mounted PGA sheet (WaRP) | NA | ≥17 days |
| Lee, 2011 [38] | Korea | RCT | single | 52 | Low risk | 17.08 ± 6.24 | Detachable snare and clips (Olympus, Tokyo, Japan) | Mucosal defects unclosed | 8 weeks |
| Maekawa, 2015 [39] | Japan | Prospective, single-arm study | single | 12 | NA | 15.18 ± 7.64 | Combined use of a single over-the-scope clip (OTSC [Ovesco Endoscopy, Tübingen, Germany]) and through-the-scope clips (TTSCs, ZEOCLIP [Zeon Medical Inc., Tokyo, Japan] or Rotatable Clip Fixing Device, EZ Clip, long type, HX-610135L [Olympus Medical Systems Corp., Tokyo, Japan]) | NA | 2 months |
| Mori, 2018 [48] | Japan | RCT | single | 39 | Low risk | 27.20 ± 18.10/35.98 ± 12.38 | PGA (Neoveil; Gunze Co., Kyoto, Japan) + fibrin glue (Beriplast P combi-set; CSL Behring Pharma, Tokyo, Japan) + device delivery station system (DDSS) | PGA (Neoveil; Gunze Co., Kyoto, Japan) + fibrin glue (Beriplast P combi-set; CSL Behring Pharma, Tokyo, Japan) | 7 days |
| Nishiyama, 2022 [40] | Japan | Prospective, single-arm study | single | 48 | High risk | 29.90 ± 12.50 | O-ring nylon loop and hemoclip (E-LOC) (HX-610- 090; Olympus, Tokyo, Japan) | NA | 12–13 days |
| Pioche, 2016 [18] | France | Retrospective case series | multiple | 19 | Mixed | 2.10 ± 1.20 | Self-assembling peptide gel (PuraStat; 3-D Matrix Ltd., Tokyo, Japan) | NA | 1 months |
| Subramaniam, 2019 [54] | UK | Prospective, single-arm study | single | 11 | Mixed | NA | self-assembling peptide gel (PuraStat; 3-D Matrix Ltd., France) | Coagulation using knife or snare tip using forced/swift coagulation or coagrasper in soft coagulation mode | 1 months |
| Shiotsuki, 2021 [41] | Japan | Retrospective cohort study | single | 178 | High risk | 20.75 ± 9.17 | Endoloop (HX-20Q-1, MAJ-340, MAJ-254; Olympus, Tokyo, Japan) and Endoclips (HX-110LR, HX-610; Olympus, Tokyo, Japan) | Coagulation using hot biopsy forceps | 2 months |
| Tan, 2016 [19] | Malaysia | Retrospective cohort study | single | 397 | Low risk | 15.25 ± 28.95 | Fibrin glue (YueLingJiao, Hangzhou PuJi Medical Tech, Hangzhou, China) | Coagrasper or hemostatic clips (Olympus, Tokyo, Japan) | 12 months |
| Tsuji, 2015 [49] | Japan | Nonrandomized trial with historical control | single | 86 | High risk | 20.40 ± 9.50 | PGA (Neoveil; Gunze Co., Kyoto, Japan) + fibrin glue (Beriplast P Combi-Set; CSL Behring Pharma, Tokyo, Japan); clip-and-pull method | Coagulation using hemostatic forceps in soft coagulation mode | ≥14 days |
| Uraoka, 2016 [58] | Japan | Prospective, single-arm study | single | 51 | Mixed | <1 | Self-assembling peptide gel (PuraStat; 3-D Matrix Ltd., Tokyo, Japan) | NA | 8 weeks |
| Wang, 2020 [55] | China | Retrospective cohort study | single | 230 | Low risk | NA | Fibrin sealant (BIOSEAl; Guangzhou Bioseal Biotechnology Co., Ltd., Guangzhou, China) | Coagulation using hot biopsy forceps | 1 months |
| Yoshida, 2021 [42] | Japan | Retrospective, single-arm study | single | 10 | Low risk | 6.5 ± 15.27 | Part of the S-O clip (Zeon Medical, Toyama, Japan) +open–close SureClip clips (Microtech, MI, USA) +endoclips (HX-610-090S, HX-610-090, HX-610-090L, HX-610-135L; Olympus, Tokyo, Japan) (LOCCM) | NA | 2 months |
| Yu, 2022 [56] | China | Retrospective cohort study | multiple | 270 | Mixed and grouped | 1.80 ± 0.43 | Polyethylene oxide adhesive (EndoClot; EndoClot Plus Co., Ltd., Suzhou, Jiangsu, China) | Coagulation using hemostatic forceps | 15 days |
| Zhang, 2013 [57] | China | RCT | single | 110 | Low risk | 4.97 ± 24.27 | α-cyanoacrylate medical adhesive (COMPONT; Beijing Compont Medical Devices Co., Ltd., Beijing, China) | Coagulation using APC or hot biopsy forceps | 12 months |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Zhao, X.; Wang, D.; Liu, X.; Chen, J.; Song, J.; Bai, T.; Hou, X. Endoscopic Delivery of Polymers Reduces Delayed Bleeding after Gastric Endoscopic Submucosal Dissection: A Systematic Review and Meta-Analysis. Polymers 2022, 14, 2387. https://doi.org/10.3390/polym14122387
Chen Y, Zhao X, Wang D, Liu X, Chen J, Song J, Bai T, Hou X. Endoscopic Delivery of Polymers Reduces Delayed Bleeding after Gastric Endoscopic Submucosal Dissection: A Systematic Review and Meta-Analysis. Polymers. 2022; 14(12):2387. https://doi.org/10.3390/polym14122387
Chicago/Turabian StyleChen, Youli, Xinyan Zhao, Dongke Wang, Xinghuang Liu, Jie Chen, Jun Song, Tao Bai, and Xiaohua Hou. 2022. "Endoscopic Delivery of Polymers Reduces Delayed Bleeding after Gastric Endoscopic Submucosal Dissection: A Systematic Review and Meta-Analysis" Polymers 14, no. 12: 2387. https://doi.org/10.3390/polym14122387
APA StyleChen, Y., Zhao, X., Wang, D., Liu, X., Chen, J., Song, J., Bai, T., & Hou, X. (2022). Endoscopic Delivery of Polymers Reduces Delayed Bleeding after Gastric Endoscopic Submucosal Dissection: A Systematic Review and Meta-Analysis. Polymers, 14(12), 2387. https://doi.org/10.3390/polym14122387