
Utilizing Light Cure Units: A Concise Narrative Review


Abstract
1. Introduction
2. Resin Composite; Importance and Composition
2.1. Composition of Resin Composites
2.2. Polymerization of Resin Composites
3. Dental Light Curing
3.1. Light Curing Devices
3.1.1. Quartz–Tungsten Halogen
3.1.2. Plasma-Arc Curing
3.1.3. Light-Emitting Diodes
3.2. Relevant Terms
3.3. Electromagnetic Spectrum
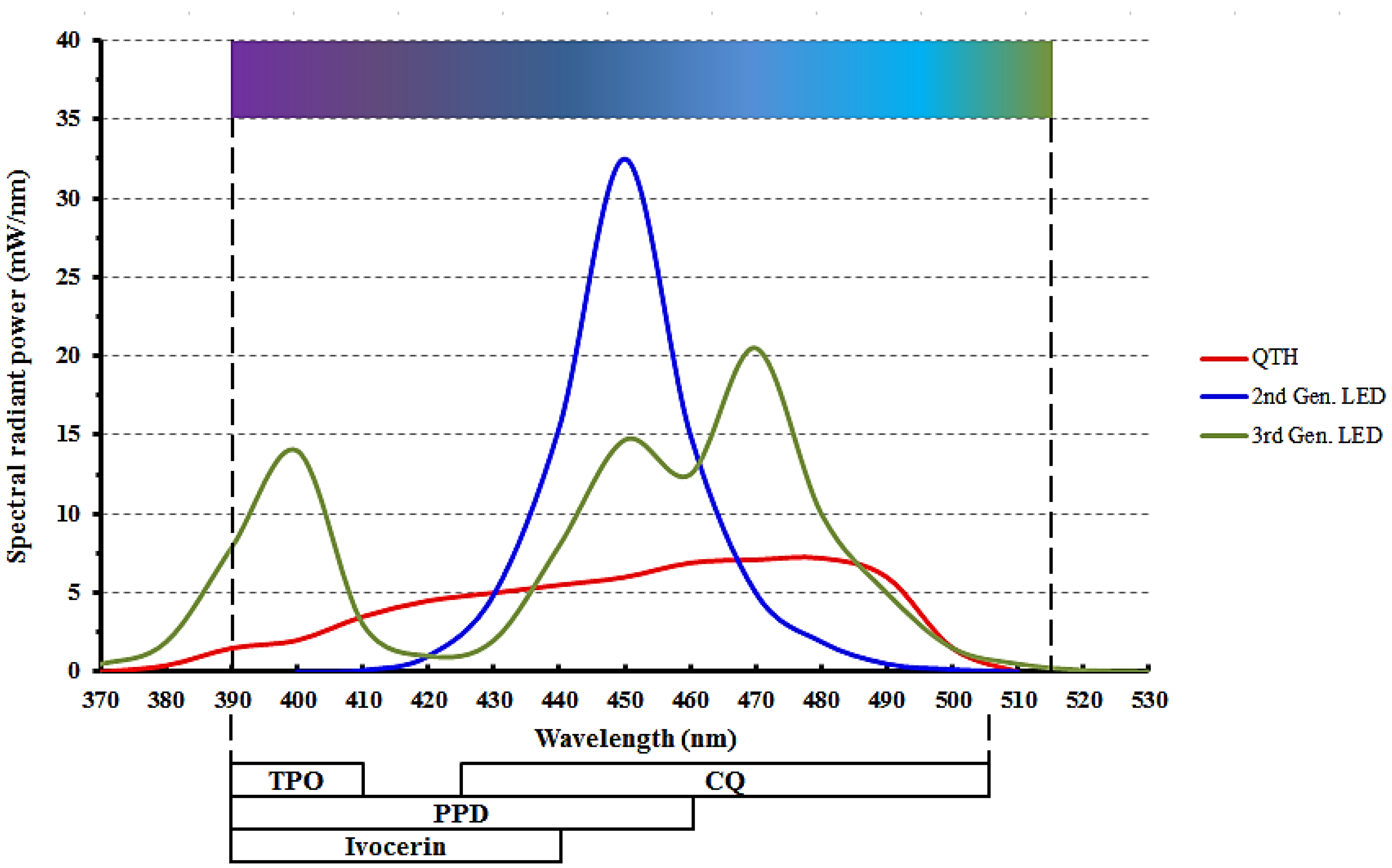
3.4. Photo-Initiators
4. Factors Affecting Light Cure Irradiance
4.1. Radiant Exitance and Irradiance Value
4.2. Active Tip Diameter
4.3. Visible Light Curing and Ophthalmological Hazards
4.4. Light Beam Uniformity
4.5. Effect of Light Cure Tip to Resin Distance
4.6. Effect of Infection Control Barrier
5. Sequelae for Improper Light Curing
6. Best Light Curing Practices
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Chan, K.H.S.; Mai, Y.; Kim, H.; Tong, K.C.T.; Ng, D.; Hsiao, J.C.M. Review: Resin Composite Filling. Materials 2010, 3, 1228–1243. [Google Scholar] [CrossRef]
- Demarco, F.F.; Correa, M.B.; Cenci, M.S.; Moraes, R.R.; Opdam, N.J. Longevity of posterior composite restorations: Not only a matter of materials. Dent. Mater. 2012, 28, 87–101. [Google Scholar] [CrossRef] [PubMed]
- Van Ende, A.; De Munck, J.; Lise, D.P.; van Meerbeek, B. Bulk-Fill Composites: A Review of the Current Literature. J. Adhes Dent. 2017, 19, 95–109. [Google Scholar] [CrossRef] [PubMed]
- Jadhav, S.; Hegde, V.; Aher, G.; Fajandar, N. Influence of light curing units on failure of directcomposite restorations. J. Conserv. Dent. 2011, 14, 225–227. [Google Scholar] [CrossRef] [PubMed]
- Rueggeberg, F.A.; Giannini, M.; Arrais, C.A.G.; Price, R.B.T. Light curing in dentistry and clinical implications: A literature review. Braz. Oral Res. 2017, 31, e61. [Google Scholar] [CrossRef] [PubMed]
- Maktabi, H.; Ibrahim, M.; Alkhubaizi, Q.; Weir, M.; Xu, H.; Strassler, H.; Fugolin, A.P.P.; Pfeifer, C.S.; Melo, M.A.S. Underperforming light curing procedures trigger detrimental irradiance-dependent biofilm response on incrementally placed dental composites. J. Dent. 2019, 88, 103110. [Google Scholar] [CrossRef] [PubMed]
- David, J.R.; Gomes, O.M.; Gomes, J.C.; Loguercio, A.D.; Reis, A. Effect of exposure time on curing efficiency of polymerizing units equipped with light-emitting diodes. J. Oral Sci. 2007, 49, 19–24. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ferracane, J.L. Resin composite—State of the art. Dent. Mater. 2011, 27, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Al Shaafi, M.; Maawadh, A.; Al Qahtani, M. Evaluation of light intensity output of QTH and LED curing devices in various governmental health institutions. Oper. Dent. 2011, 36, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Maghaireh, G.A.; Alzraikat, H.; Taha, N.A. Assessing the irradiance delivered from light-curing units in private dental offices in Jordan. J. Am. Dent. Assoc. 2013, 144, 922–927. [Google Scholar] [CrossRef]
- Santos, G.C.; Santos, M.J.M.C.; El-Mowafy, O.; El-Badrawy, W. Intensity of quartz-tungsten-halogen light polymerization units used in dental offices in Brazil. Int. J. Prosthodont. 2005, 18, 434–435. [Google Scholar]
- Hao, X.Q.; Luo, M.; Wu, J.; Zhu, S. A survey of power density of light-curing units used in private dental offices in Changchun City, China. Laser. Med. Sci. 2015, 30, 493–497. [Google Scholar] [CrossRef] [PubMed]
- Federlin, M.; Price, R. Improving light-curing instruction in dental school. J. Dent. Educ. 2013, 77, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Price, R.B.; Strassler, H.E.; Price, H.L.; Seth, S.; Lee, C.J. The effectiveness of using a patient simulator to teach light-curing skills. J. Am. Dent. Assoc. 2014, 145, 32–43. [Google Scholar] [CrossRef] [PubMed]
- Shortall, A.C.; Price, R.B.; MacKenzie, L.; Burke, F.J.T. Guidelines for the selection, use, and maintenance of LED light-curing units—Part II. Br. Dent. J. 2016, 221, 551–554. [Google Scholar] [CrossRef] [PubMed]
- Lynch, C.D.; Wilson, N.H. Managing the phase-down of amalgam: Part II. Implications for practising arrangements and lessons from Norway. Br. Dent. J. 2013, 215, 159–162. [Google Scholar] [CrossRef]
- Meyer, D.M.; Kaste, L.M.; Lituri, K.M.; Tomar, S.; Fox, C.H.; Petersen, P.E. Policy Development Fosters Collaborative Practice: The Example of the Minamata Convention on Mercury. Dent. Clin. N. Am. 2016, 60, 921–942. [Google Scholar] [CrossRef]
- Randolph, L.D.; Palin, W.M.; Leprince, J.G. Composition of Dental Resin-Based Composites for Direct Restorations. In Dental Composite Materials for Direct Restorations; Miletic, V., Ed.; Springer International Publishing: Cham, Switzerland, 2018; pp. 11–24. [Google Scholar]
- Aminoroaya, A.; Neisiany, R.E.; Khorasani, S.N.; Panahi, P.; Das, O.; Madry, H.; Cucchiarini, M.; Ramakrishna, S. A review of dental composites: Challenges, chemistry aspects, filler influences, and future insights. Compos. Part. B Eng. 2021, 216, 108852. [Google Scholar] [CrossRef]
- D′Ovidio, T.J.; Roberts, R.M.; Gautam, D.; Marks, Z.D.; Saraswathy, M.; Stansbury, J.W.; Nair, D.P. Photopolymerization kinetics of methyl methacrylate with reactive and inert nanogels. J. Mech. Behav. Biomed. Mater. 2018, 85, 218–224. [Google Scholar] [CrossRef] [PubMed]
- Hadis, M.; Leprince, J.G.; Shortall, A.C.; Devaux, J.; Leloup, G.; Palin, W.M. High irradiance curing and anomalies of exposure reciprocity law in resin-based materials. J. Dent. 2011, 39, 549–557. [Google Scholar] [CrossRef]
- Randolph, L.D.; Palin, W.M.; Leloup, G.; Leprince, J.G. Filler characteristics of modern dental resin composites and their influence on physico-mechanical properties. Dent. Mater. 2016, 32, 1586–1599. [Google Scholar] [CrossRef] [PubMed]
- Curtis, A.R.; Palin, W.M.; Fleming, G.J.; Shortall, A.C.; Marquis, P.M. The mechanical properties of nanofilled resin-based composites: Characterizing discrete filler particles and agglomerates using a micromanipulation technique. Dent. Mater. 2009, 25, 180–187. [Google Scholar] [CrossRef]
- Zimmerli, B.; Strub, M.; Jeger, F.; Stadler, O.; Lussi, A. Composite materials: Composition, properties and clinical applications. A literature review. Schweiz. Mon. Für Zahnmed. 2010, 120, 972–986. [Google Scholar]
- Ilie, N.; Hickel, R. Resin composite restorative materials. Aust. Dent. J. 2011, 56 (Suppl. 1), 59–66. [Google Scholar] [CrossRef]
- Neumann, M.G.; Miranda, W.G., Jr.; Schmitt, C.C.; Rueggeberg, F.A.; Correa, I.C. Molar extinction coefficients and the photon absorption efficiency of dental photoinitiators and light curing units. J. Dent. 2005, 33, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Anusavice, K. Phillips’ Science of Dental Materials, 11th ed.; Saunders: St. Louis, MA, USA, 2003. [Google Scholar]
- Ilie, N.; Keßler, A.; Durner, J. Influence of various irradiation processes on the mechanical properties and polymerisation kinetics of bulk-fill resin based composites. J. Dent. 2013, 41, 695–702. [Google Scholar] [CrossRef]
- Leprince, J.G.; Palin, W.M.; Hadis, M.A.; Devaux, J.; Leloup, G. Progress in dimethacrylate-based dental composite technology and curing efficiency. Dent. Mater. 2013, 29, 139–156. [Google Scholar] [CrossRef]
- Opdam, N.J.; van de Sande, F.H.; Bronkhorst, E.; Cenci, M.S.; Bottenberg, P.; Pallesen, U.; Gaengler, P.; Lindberg, A.; Huysmans, M.C.; van Dijken, J.W. Longevity of posterior composite restorations: A systematic review and meta-analysis. J. Dent. Res. 2014, 93, 943–949. [Google Scholar] [CrossRef]
- Alshali, R.Z.; Silikas, N.; Satterthwaite, J.D. Degree of conversion of bulk-fill compared to conventional resin-composites at two time intervals. Dent. Mater. 2013, 29, e213–e217. [Google Scholar] [CrossRef] [PubMed]
- Ilie, N.; Hickel, R. Investigations on mechanical behaviour of dental composites. Clin. Oral Investig. 2009, 13, 427–438. [Google Scholar] [CrossRef] [PubMed]
- Tarle, Z.; Knezevic, A.; Demoli, N.; Meniga, A.; Sutaloa, J.; Unterbrink, G.; Ristic, M.; Pichler, G. Comparison of composite curing parameters: Effects of light source and curing mode on conversion, temperature rise and polymerization shrinkage. Oper. Dent. 2006, 31, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Friedman, J. Dental light-curing lamp unit with interchangeable autofocus light guides. U.S. Patent 4,948,215, 14 August 1990. [Google Scholar]
- Rueggeberg, F.A. State-of-the-art: Dental photocuring—A review. Dent. Mater. 2011, 27, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Price, R.B.; Rueggeberg, F.A. Light Curing of Restorative Materials. In Sturdevant′s Art and Science of Operative Dentistry, 7th ed.; Ritter, A.V., Boushell, L.W., Walter, R., Eds.; Elsevier: Amsterdam, The Netherlands, 2018. [Google Scholar]
- Price, R.B.T. Light Curing in Dentistry. Dent. Clin. N. Am. 2017, 61, 751–778. [Google Scholar] [CrossRef]
- Knezević, A.; Tarle, Z.; Meniga, A.; Sutalo, J.; Pichler, G.; Ristić, M. Degree of conversion and temperature rise during polymerization of composite resin samples with blue diodes. J. Oral Rehabil. 2001, 28, 586–591. [Google Scholar] [CrossRef]
- Price, R.B.; Felix, C.A.; Andreou, P. Third-generation vs a second-generation LED curing light: Effect on Knoop microhardness. Compend. Contin. Educ. Dent. 2006, 27, 490–496, quiz 497, 518. [Google Scholar] [PubMed]
- Jandt, K.D.; Mills, R.W. A brief history of LED photopolymerization. Dent. Mater. 2013, 29, 605–617. [Google Scholar] [CrossRef] [PubMed]
- Shortall, A.C.; Price, R.B.; MacKenzie, L.; Burke, F.J. Guidelines for the selection, use, and maintenance of LED light-curing units—Part 1. Br. Dent. J. 2016, 221, 453–460. [Google Scholar] [CrossRef]
- Price, R.B.; Ferracane, J.L.; Hickel, R.; Sullivan, B. The light-curing unit: An essential piece of dental equipment. Int. Dent. J. 2020, 70, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Dunn, W.J.; Bush, A.C. A comparison of polymerization by light-emitting diode and halogen-based light-curing units. J. Am. Dent. Assoc. 2002, 133, 335–341. [Google Scholar] [CrossRef]
- Price, R.B.; Ferracane, J.L.; Shortall, A.C. Light-Curing Units: A Review of What We Need to Know. J. Dent. Res. 2015, 94, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Watts, D.C.; Kaiser, C.; O′Neill, C.; Price, R.B. Reporting of light irradiation conditions in 300 laboratory studies of resin-composites. Dent. Mater. 2019, 35, 414–421. [Google Scholar] [CrossRef] [PubMed]
- Price, R.B. Is your study reproducible? What “light” are you delivering to your specimens? J. Adhes. Dent. 2018, 20, 375. [Google Scholar] [CrossRef] [PubMed]
- Platt, J.A.; Price, R.B. Light curing explored in Halifax. Oper. Dent. 2014, 39, 561–563. [Google Scholar] [CrossRef] [PubMed]
- Santini, A.; Gallegos, I.T.; Felix, C.M. Photoinitiators in dentistry: A review. Prim. Dent. J. 2013, 2, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Leprince, J.G.; Hadis, M.; Shortall, A.C.; Ferracane, J.L.; Devaux, J.; Leloup, G.; Palin, W.M. Photoinitiator type and applicability of exposure reciprocity law in filled and unfilled photoactive resins. Dent. Mater. 2011, 27, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Miletic, V.; Santini, A. Micro-Raman spectroscopic analysis of the degree of conversion of composite resins containing different initiators cured by polywave or monowave LED units. J. Dent. 2012, 40, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Kowalska, A.; Sokolowski, J.; Bociong, K. The Photoinitiators Used in Resin Based Dental Composite—A Review and Future Perspectives. Polymers 2021, 13, 470. [Google Scholar] [CrossRef] [PubMed]
- Alvim, H.H.; Alecio, A.C.; Vasconcellos, W.A.; Furlan, M.; de Oliveira, J.E.; Saad, J.R.C. Analysis of camphorquinone in composite resins as a function of shade. Dent. Mater. 2007, 23, 1245–1249. [Google Scholar] [CrossRef]
- Silami, F.D.; Mundim, F.M.; Garcia, L.d.F.R.; Sinhoreti, M.A.; Pires-de-Souza, F.d.C.P. Color stability of experimental composites containing different photoinitiators. J. Dent. 2013, 41 (Suppl. 3), e62–e66. [Google Scholar] [CrossRef]
- Li, X.; Pongprueksa, P.; van Meerbeek, B.; de Munck, J. Curing profile of bulk-fill resin-based composites. J. Dent. 2015, 43, 664–672. [Google Scholar] [CrossRef]
- Shimokawa, C.; Turbino, M.L.; Giannini, M.; Braga, R.R.; Price, R.B. Effect of Curing Light and Exposure Time on the Polymerization of Bulk-Fill Resin-Based Composites in Molar Teeth. Oper. Dent. 2020, 45, E141–E155. [Google Scholar] [CrossRef] [PubMed]
- ACGIH. TLVs and BEIs based on the documentation for threshold limit values for chemical substances and physical agents and biological exposure indices. In Proceedings of the American Conference of Governmental Industrial Hygienists (ACGIH), Cincinnati, OH, USA, 2015; Available online: http://dl.mozh.org/up/acgih-2015.pdf (accessed on 13 May 2021).
- Zhao, Z.C.; Zhou, Y.; Tan, G.; Li, J. Research progress about the effect and prevention of blue light on eyes. Int. J. Ophthalmol. 2018, 11, 1999–2003. [Google Scholar] [CrossRef] [PubMed]
- Niwano, Y.; Kanno, T.; Iwasawa, A.; Ayaki, M.; Tsubota, K. Blue light injures corneal epithelial cells in the mitotic phase in vitro. Br. J. Ophthalmol. 2014, 98, 990–992. [Google Scholar] [CrossRef] [PubMed]
- McCusker, N.; Bailey, C.; Robinson, S.; Patel, N.; Sandy, J.R.; Ireland, A.J. Dental light curing and its effects on color perception. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 355–363. [Google Scholar] [CrossRef] [PubMed]
- Kopperud, S.E.; Rukke, H.V.; Kopperud, H.M.; Bruzell, E.M. Light curing procedures—Performance, knowledge level and safety awareness among dentists. J. Dent. 2017, 58, 67–73. [Google Scholar] [CrossRef]
- Labrie, D.; Moe, J.; Price, R.B.; Young, M.E.; Felix, C.M. Evaluation of ocular hazards from 4 types of curing lights. J. Can. Dent. Assoc. 2011, 77, b116. [Google Scholar]
- Seth, S.; Lee, C.J.; Ayer, C.D. Effect of instruction on dental students′ ability to light-cure a simulated restoration. J. Can. Dent. Assoc. 2012, 78, c123. [Google Scholar]
- Price, R.B.; McLeod, M.E.; Felix, C.M. Quantifying light energy delivered to a Class I restoration. J. Can. Dent. Assoc. 2010, 76, a23. [Google Scholar]
- AlShaafi, M.M.; Harlow, J.E.; Price, H.L.; Rueggeberg, F.A.; Labrie, D.; AlQahtani, M.Q.; Price, R.B. Emission Characteristics and Effect of Battery Drain in "Budget" Curing Lights. Oper. Dent. 2016, 41, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Michaud, P.L.; Price, R.B.; Labrie, D.; Rueggeberg, F.A.; Sullivan, B. Localised irradiance distribution found in dental light curing units. J. Dent. 2014, 42, 129–139. [Google Scholar] [CrossRef]
- Price, R.B.; Labrie, D.; Rueggeberg, F.A.; Felix, C.M. Irradiance differences in the violet (405 nm) and blue (460 nm) spectral ranges among dental light-curing units. J. Esthet. Restor. Dent. 2010, 22, 363–377. [Google Scholar] [CrossRef] [PubMed]
- Price, R.B.; Labrie, D.; Rueggeberg, F.A.; Sullivan, B.; Kostylev, I.; Fahey, J. Correlation between the beam profile from a curing light and the microhardness of four resins. Dent. Mater. 2014, 30, 1345–1357. [Google Scholar] [CrossRef]
- Haenel, T.; Hausnerová, B.; Steinhaus, J.; Price, R.B.T.; Sullivan, B.; Moeginger, B. Effect of the irradiance distribution from light curing units on the local micro-hardness of the surface of dental resins. Dent. Mater. 2015, 31, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Leprince, J.; Devaux, J.; Mullier, T.; Vreven, J.; Leloup, G. Pulpal-temperature rise and polymerization efficiency of LED curing lights. Oper. Dent. 2010, 35, 220–230. [Google Scholar] [CrossRef] [PubMed]
- Shortall, A.; El-Mahy, W.; Stewardson, D.; Addison, O.; Palin, W. Initial fracture resistance and curing temperature rise of ten contemporary resin-based composites with increasing radiant exposure. J. Dent. 2013, 41, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Mouhat, M.; Mercer, J.; Stangvaltaite, L.; Ortengren, U. Light-curing units used in dentistry: Factors associated with heat development-potential risk for patients. Clin. Oral Investig. 2017, 21, 1687–1696. [Google Scholar] [CrossRef]
- Ajaj, R.A.; Nassar, H.M.; Hasanain, F.A. Infection Control Barrier and Curing Time as Factors Affecting the Irradiance of Light-Cure Units. J. Int. Soc. Prev. Community Dent. 2018, 8, 523–528. [Google Scholar] [CrossRef]
- McAndrew, R.; Lynch, C.D.; Pavli, M.; Bannon, A.; Milward, P. The effect of disposable infection control barriers and physical damage on the power output of light curing units and light curing tips. Br. Dent. J. 2011, 210, E12. [Google Scholar] [CrossRef]
- Soares, C.J.; Braga, S.S.L.; Ribeiro, M.T.H.; Price, R.B. Effect of infection control barriers on the light output from a multi-peak light curing unit. J. Dent. 2020, 103, 103503. [Google Scholar] [CrossRef] [PubMed]
- Strassler, H.E.; Price, R.B. Understanding light curing, Part I. Delivering predictable and successful restorations. Dent. Today 2014, 33, 114–116. [Google Scholar] [PubMed]
- Price, R.B. Light energy matters. J. Can. Dent. Assoc. 2010, 76, a63. [Google Scholar] [PubMed]
- Balhaddad, A.A.; Garcia, I.; Collares, F.; Felix, C.M.; Ganesh, N.; Alkabashi, Q.; Massei, W.; Strassler, H.; Melo, M.A. Assessment of the radiant emittance of damaged/contaminated dental light-curing tips by spectrophotometric methods. Restor. Dent. Endod. 2020, 45, e55. [Google Scholar] [CrossRef] [PubMed]
- Santerre, J.P.; Shajii, L.; Leung, B.W. Relation of dental composite formulations to their degradation and the release of hydrolyzed polymeric-resin-derived products. Crit. Rev. Oral Biol. Med. 2001, 12, 136–151. [Google Scholar] [CrossRef] [PubMed]
- Van Landuyt, K.L.; Nawrot, T.; Geebelen, B.; De Munck, J.; Snauwaert, J.; Yoshihara, K.; Scheers, H.; Godderis, L.; Hoet, P.; van Meerbeek, B. How much do resin-based dental materials release? A meta-analytical approach. Dent. Mater. 2011, 27, 723–747. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, K.V.; Sathorn, C.; Wong, R.H.; Burrow, M.F. Clinical performance of laminate and non-laminate resin composite restorations: A systematic review. Aust. Dent. J. 2015, 60, 520–527. [Google Scholar] [CrossRef] [PubMed]
- Schultz, S.; Rosentritt, M.; Behr, M.; Handel, G. Mechanical properties and three-body wear of dental restoratives and their comparative flowable materials. Quintessence Int. 2010, 41, e1–e10. [Google Scholar] [PubMed]
- El-Damanhoury, H.M.; Platt, J.A. Polymerization Shrinkage Stress Kinetics and Related Properties of Bulk-fill Resin Composites. Oper. Dent. 2014, 39, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Menees, T.S.; Lin, C.P.; Kojic, D.D.; Burgess, J.O.; Lawson, N.C. Depth of cure of bulk fill composites with monowave and polywave curing lights. Am. J. Dent. 2015, 28, 357–361. [Google Scholar]
- Kim, E.H.; Jung, K.H.; Son, S.A.; Hur, B.; Kwon, Y.H.; Park, J.K. Effect of resin thickness on the microhardness and optical properties of bulk-fill resin composites. Restor. Dent. Endod. 2015, 40, 128–135. [Google Scholar] [CrossRef]
- Sauro, S.; Osorio, R.; Watson, T.F.; Toledano, M. Influence of phosphoproteins′ biomimetic analogs on remineralization of mineral-depleted resin-dentin interfaces created with ion-releasing resin-based systems. Dent. Mater. 2015, 31, 759–777. [Google Scholar] [CrossRef]
- Ritter, A.V.; Swift, E.J., Jr. Current restorative concepts of pulp protection. Endod. Top. 2003, 5, 41–48. [Google Scholar] [CrossRef]
- Price, R.B. Light curing guidelines for practitioners: A consensus statement from the 2014 symposium on light curing in dentistry, Dalhousie University, Halifax, Canada. J. Can. Dent. Assoc. 2014, 80, e61. [Google Scholar] [PubMed]
- Suliman, A.A.; Elmasmari, H.A.; Abdo, A.A. Effect of Contamination, Damage and Barriers on the Light Output of Light-Curing Units. Open Dent. J. 2019, 13, 196–202. [Google Scholar] [CrossRef]
- Assaf, C.; Fahd, J.-C.; Sabbagh, J. Assessing Dental Light-curing Units’ Output Using Radiometers: A Narrative Review. J. Int Soc. Prev Community Dent. 2020, 10, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Price, R.B.; Labrie, D.; Kazmi, S.; Fahey, J.; Felix, C.M. Intra- and inter-brand accuracy of four dental radiometers. Clin. Oral Investig. 2012, 16, 707–717. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Term | Unit Commonly Used in Dentistry | Symbol | Notes/Significance of Term |
|---|---|---|---|
| Radiant energy | Joule | J | This describes the energy from the curing light source |
| Radiant exposure (fluence) | Joule per cubic centimeter | J/cm3 | It describes the energy emitted or received |
| Radiant exitance (or radiant emittance) | Milliwatt per square centimeter | mW/cm2 | Radiant power/flux emitted from a defined area. To be used instead of power density or irradiance when describing the output from a curing light and is influenced by tip diameter |
| Irradiance (incident radiation) | Milliwatt per square centimeter | mW/cm2 | Radiant power on the surface |
| Spectral radiant power | Milliwatt per nanometer | mW/nm | Radiant power emitted per wavelength of light. Longer wavelengths have less energy than shorter wavelengths. Higher power usually needs shorter exposure time, while lower power requires longer exposure time |
| Spectral irradiance | Milliwatt per square centimeter per nanometer | mW/cm2/nm | Irradiance received by the resin at each nm. The further away the LCU tip, the less irradiance received |
| Light Cure Device | Manufacturer Details | Wavelengths (nm) | Curing Tip Diameter (mm) | Modes | Irradiance (mW/cm2) | Built-In Radiometer |
|---|---|---|---|---|---|---|
| Elipar DeepCure-S | 3M ESPE, St. Paul, Minnesota, USA | 430–480 monowave | 10 | Standard | 1470 | No |
| Bluephase PowerCure | Ivoclar Vivadent, Schaan, Liechtenstein | 385–515 multiwave | 9 | PreCure Turbo High power 3 s | 950 1200 2000 3000 | Yes |
| VALO Cordless | Ultradent Products, South Jordon, Utah, USA | 385–515 multiwave | Not disclosed | Normal High power Xtra power | 1000 1400 3200 | No |
| Demi Ultra | KaVo Kerr, Orange, California, USA | 450–470 monowave | 8 | Standard | 1100–1330 | Yes |
| SmartLite Pro | Dentsply Sirona, Konstanz, Germany | Cure tip: 450–480 PolyCure tip: 405–480 monowave | 10 | Standard | 1200 | Yes |
| Material | Main Monomer | Main Fillers | Photo-Initiator | Manufacturer |
|---|---|---|---|---|
| Filtek Bulk-Fill | AUDMA | Silane-treated ceramics | CQ | 3M ESPE, Dental Products, Saint Paul, MN, USA |
| Tetric Evo-Ceram Bulk Fill | Bis-EMA | Barium aluminium silicate glass | CQ, Ivocerin® | Ivoclar Vivadent, Zurich, Switzerland |
| Tetric N-Ceram Bulk Fill | Bis-GMA | Barium aluminium silicate glass | CQ, Ivocerin® | Ivoclar Vivadent, Zurich, Switzerland |
| SonicFill | 3-trimethoxysilylpropyl methacrylate | Barium glass | CQ | Kerr Dental, Orange, CA, USA |
| Beautiful Bulk Restorative | Bis-GMA | S-PRG fluoroboroaluminosilicate glass | Not disclosed | Shofu Inc., Kyoto, Japan |
| X-tra fil | MMA | Inorganic fillers | Not disclosed | Voco, Cuxhaven, Germany |
| SureFil SDR * | UDMA | Barium glass | CQ | Dentsply Caulk, Milford, DE, USA |
| Filtek Bulk Flow * | Bis-GMA | Silane treated ceramic, ytterbium fluoride filler | CQ | 3M ESPE, Dental Products, Saint Paul, MN, USA |
| Tetric Evo-Flow Bulk Fill * | Dimethacrylates | Barium glass | CQ, Ivocerin® | Ivoclar Vivadent, Zurich, Switzerland |
| Venus Bulk-Fill * | UDMA | Barium glass | Not disclosed | Heraeus Kulzer, South Bend, IN, USA |
| Beautifil Bulk Flowable * | Bis-GMA | S-PRG fluoroboroaluminosilicate glass | Not disclosed | Shofu Inc., Kyoto, Japan |
| EverX Posterior * | Bis-GMA | Barium borosilicate glass | CQ | GC Dental Products, Tokyo, Japan |
| X-tra base * | Bis-EMA | Inorganic fillers | Not disclosed | Voco, Cuxhaven, Germany |
| MI Fil * | UDMA | Silica nanofillers | Not disclosed | GC Dental Products, Tokyo, Japan |
| Recommended Practice | Reference(s) |
|---|---|
| Choose the LCU which matches the photo-initiators in the RC material. LEDs are the most commonly used LCUs; therefore, the use of multi-wave LEDs is preferred because it activates all currently used photo-initiators. | Price, 2010 [76] Price, 2014 [87] Rueggeberg et al., 2017 [5] Price, 2017 [37] |
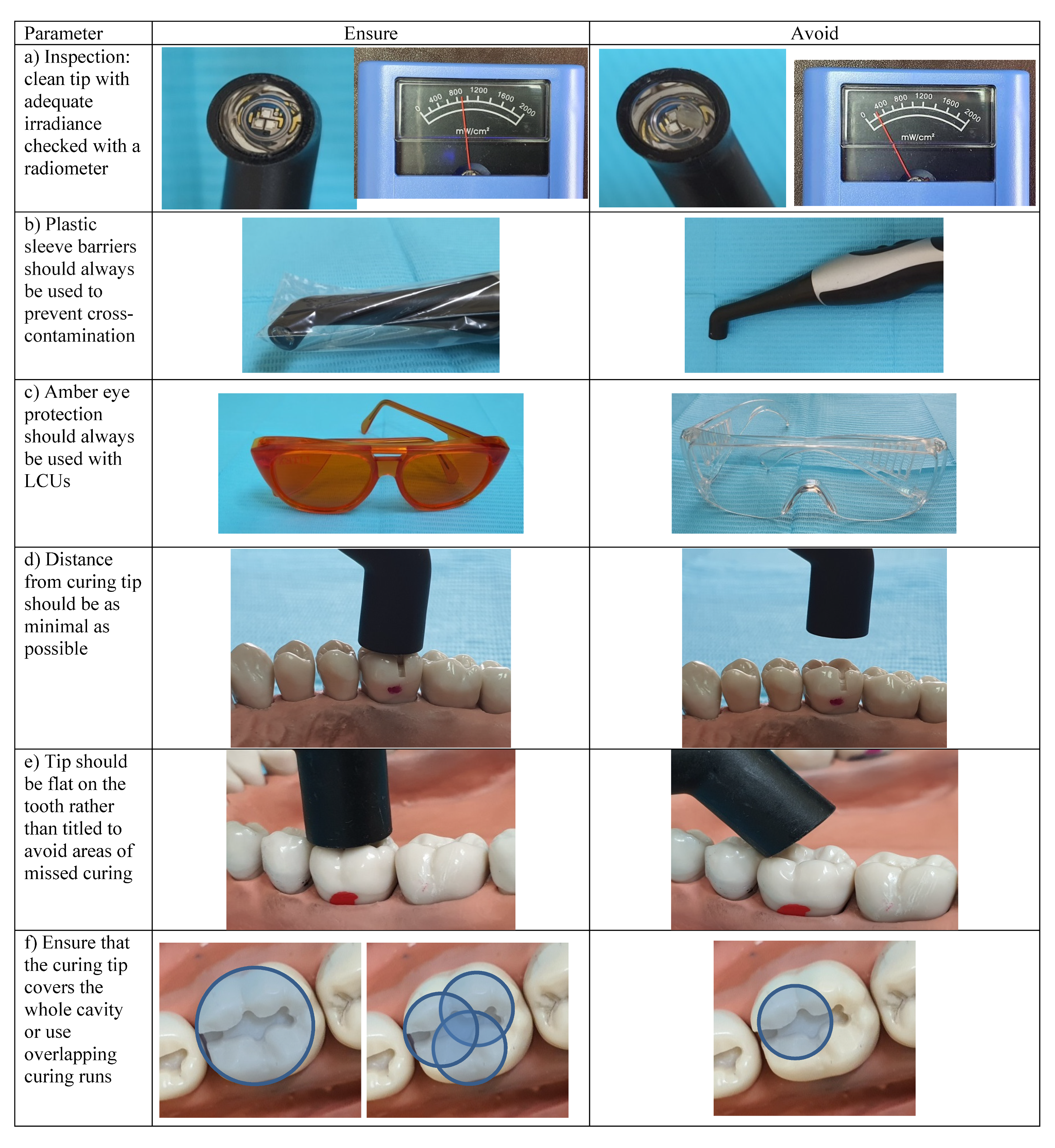
| Prior to each LCU use, check the tip for cleanliness. Any debris on the tip affects the light curing process and should be removed prior to curing the restoration. | Ajaj et al., 2018 [72] Suliman et al., 2019 [88] |
| Ensure that the infection control barrier is used and placed correctly, with no seam covering the active tip diameter. | Rueggeberg et al., 2017 [5] Price, 2017 [37] Ajaj et al., 2018 [72] |
| The use of light-blocking glasses is strongly advocated because they nearly eliminate the blue light hazard. | Rueggeberg et al., 2017 [5] Shortall et al., 2016 [15] Price, 2017 [37] |
| During the use of the LCU inside the patient’s mouth, position the LCU as close as possible to the restoration surface and place it as flat as possible to gain optimal curing. Compromised access and darker shades of composite should be compensated for by increasing the curing time. | Shortall et al., 2016 [15] Price, 2017 [37]. |
| Ensure that the active curing tip covers the entire restoration. If it is smaller than the restoration, several overlapping runs will be needed to attain adequate polymerization of the RC. | Shortall et al., 2016 [15] Price, 2017 [37] Price et al., 2020 [42]. |
| The use of a dental radiometer to monitor the LCU in practice is a quick and easy way to ensure that the LCU is still emitting the required irradiance Regular monitoring also allows the practitioner to know when the irradiance has dropped and LCU unit needs maintenance or replacement. | Rueggeberg et al., 2017 [5] Assaf et al., 2020 [89] Price et al., 2012 [90]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hasanain, F.A.; Nassar, H.M. Utilizing Light Cure Units: A Concise Narrative Review. Polymers 2021, 13, 1596. https://doi.org/10.3390/polym13101596
Hasanain FA, Nassar HM. Utilizing Light Cure Units: A Concise Narrative Review. Polymers. 2021; 13(10):1596. https://doi.org/10.3390/polym13101596
Chicago/Turabian StyleHasanain, Fatin A., and Hani M. Nassar. 2021. "Utilizing Light Cure Units: A Concise Narrative Review" Polymers 13, no. 10: 1596. https://doi.org/10.3390/polym13101596
APA StyleHasanain, F. A., & Nassar, H. M. (2021). Utilizing Light Cure Units: A Concise Narrative Review. Polymers, 13(10), 1596. https://doi.org/10.3390/polym13101596