
Simulating the Impact of Crossover Kidney Transplantation on the Nord Italia Transplant Program


Abstract
:1. Introduction
1.1. Medical Background
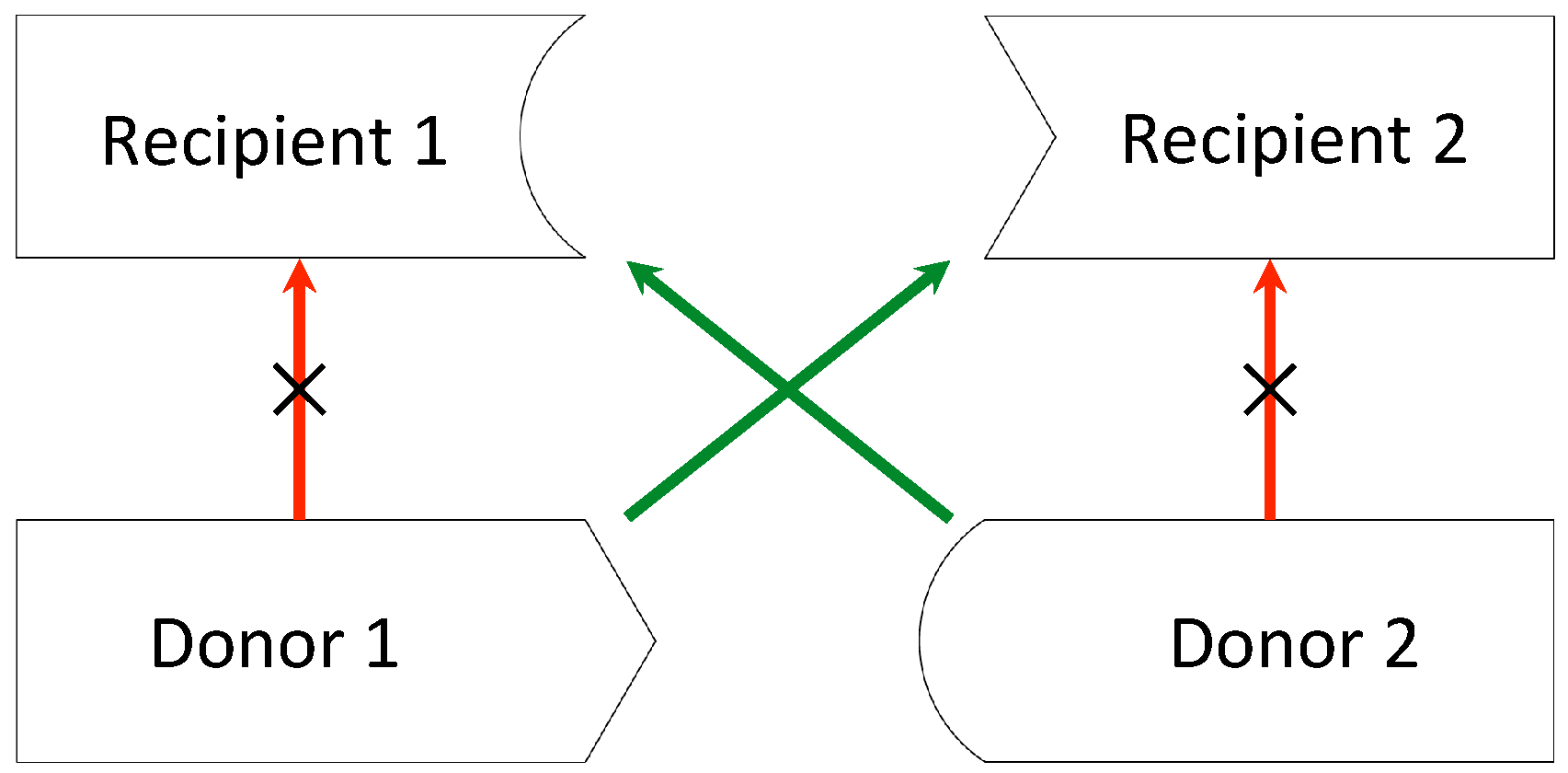
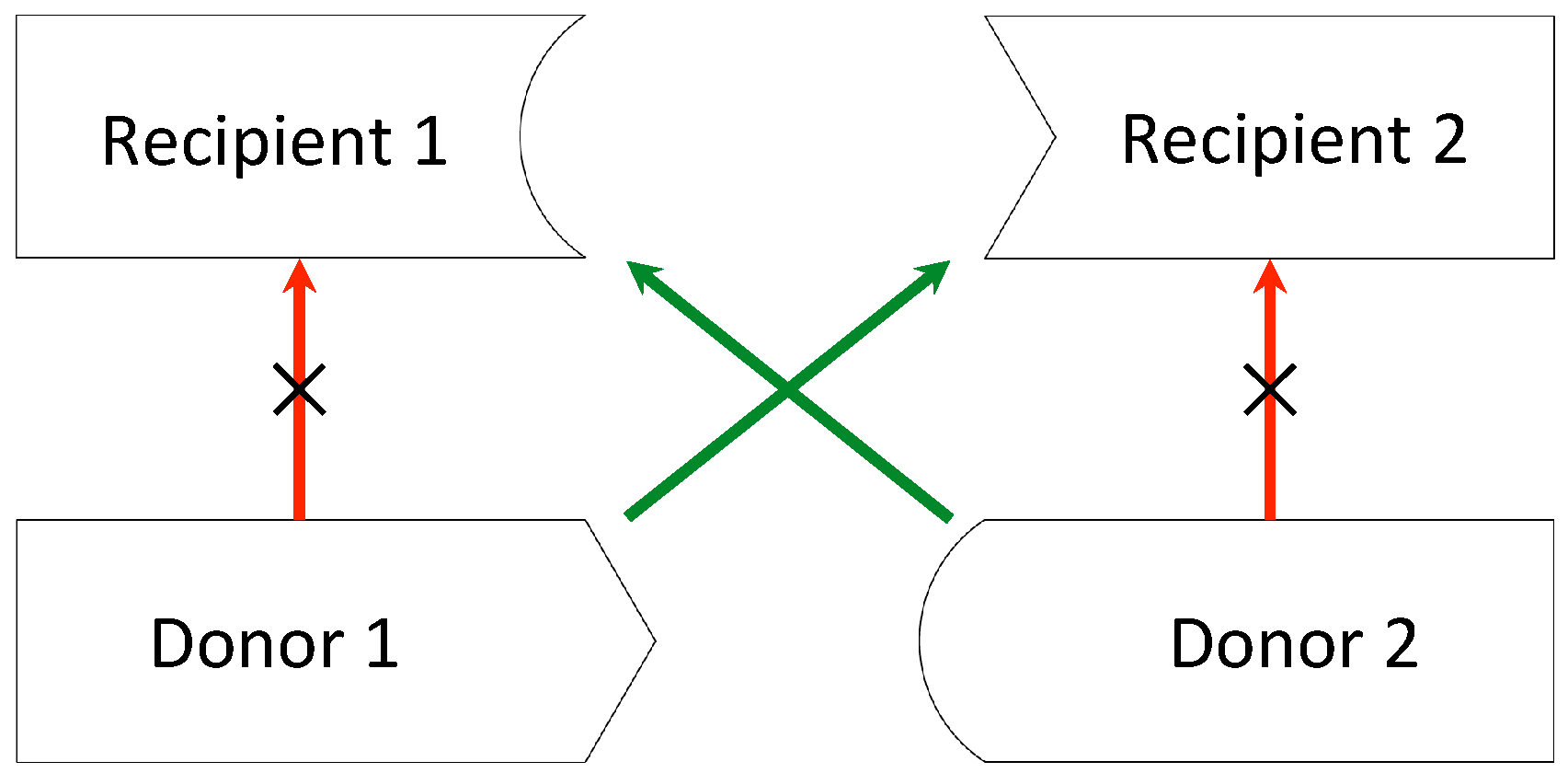
1.2. Kidney Exchange
1.3. Mathematical Aspects
- An exchange can involve only two pairs (pairwise exchange);
- Each patient is indifferent between all compatible donors and between all incompatible donors. The own donor is strictly preferred to any other incompatible donor, and any compatible donor is considered to be strictly better than the own donor (0–1 preferences).
- It considers the set of all maximum-cardinality matchings;
- It selects those matchings that assign a kidney to the patient with the highest priority in the priority ordering. Among this subgroup of matchings, it selects those that also match the patient who is ranked second in the priority ordering, and so on.
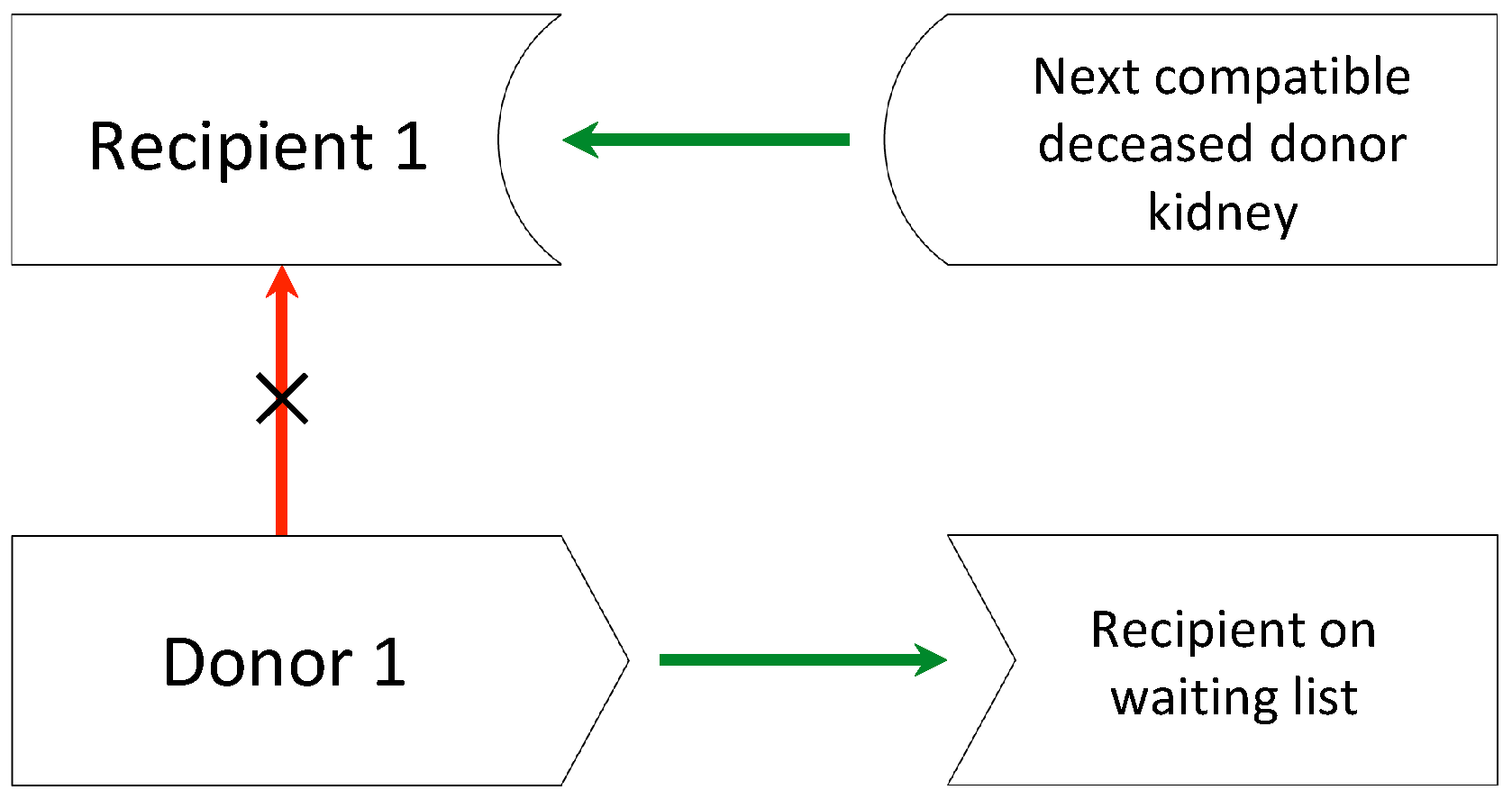
- There are no constraints on the size of exchanges, and list exchanges are allowed;
- Recipients have heterogenous preferences over compatible kidneys, which are supposed to be strict and based on different factors, such as HLA match, donor’s age, and so on.
- Initially, all kidneys are available;
- In each round, each couple points towards its patient’s favourite option (a donor of the pool or a high priority on the waiting list).
- –
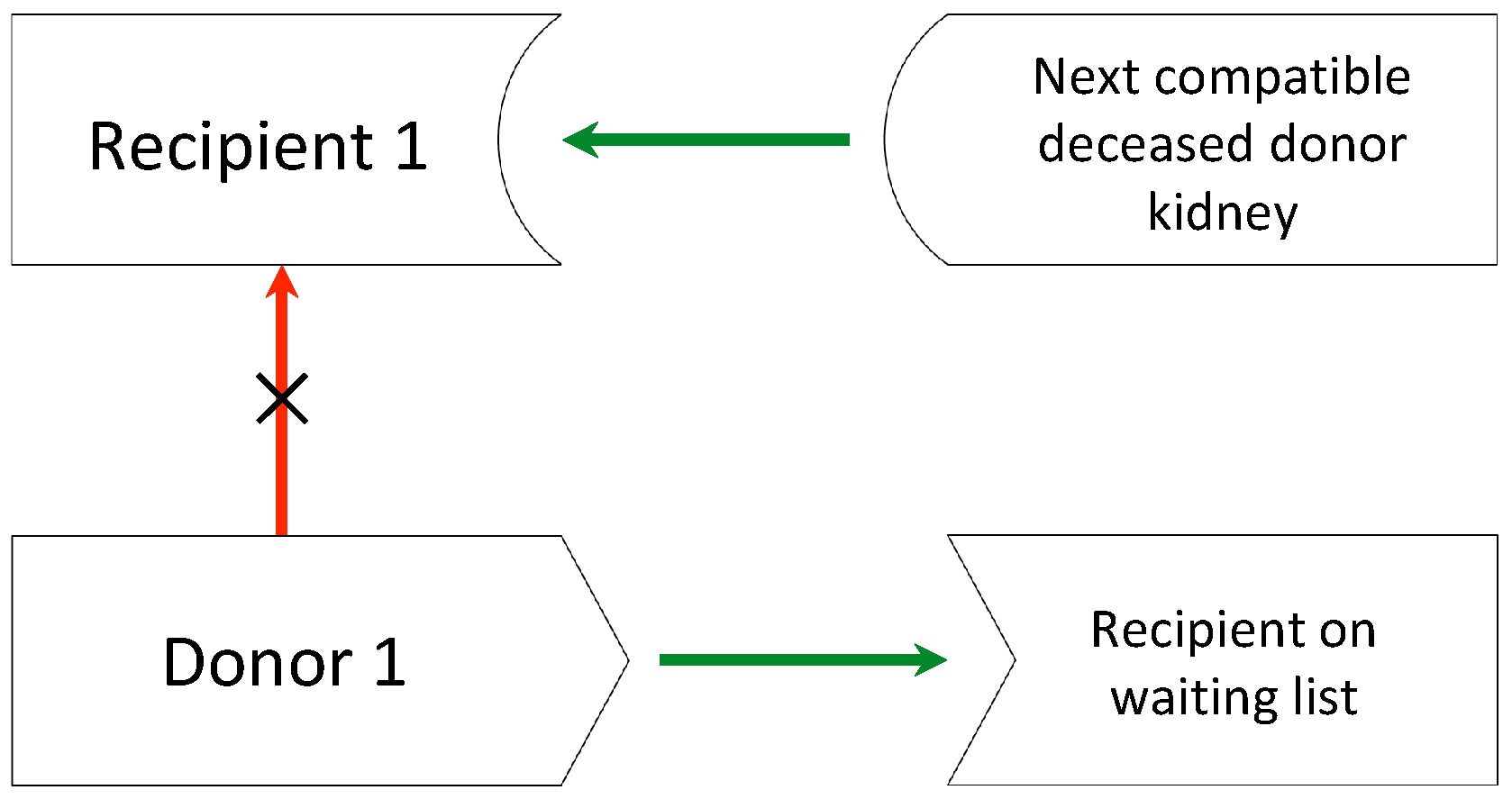
- There can be either a cycle, a w-chain (i.e., chains in which the last patient points towards the waiting list option), or both. Whenever a cycle is formed, the corresponding transplants are carried out until there are no cycles left, but only w-chains.
- –
- The algorithm selects one chain following a preselected rule and carrying out transplantations on that chain and so on. Some selection rules and their implications are discussed in [15].
- At the end of the procedure, the TTCC mechanism assigns each patient a kidney or a high priority in the waiting list for a kidney from a deceased donor.
2. Materials and Methods
- Only pairwise exchanges are allowed (priority mechanism);
- There are no constraints on the size of exchanges, and list exchanges are also allowed (TTCC).
2.1. Dataset
2.2. Implementation
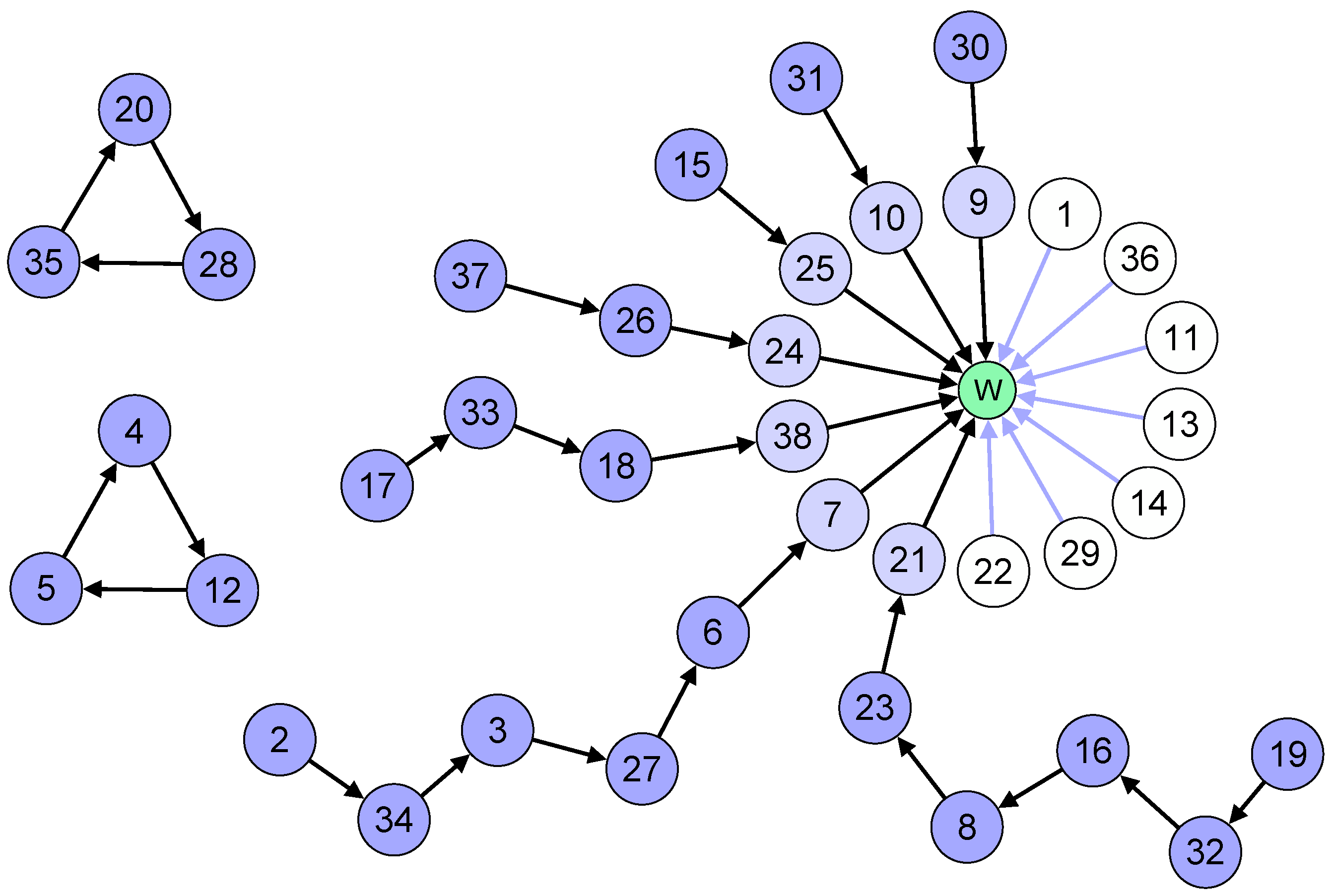
3. Results
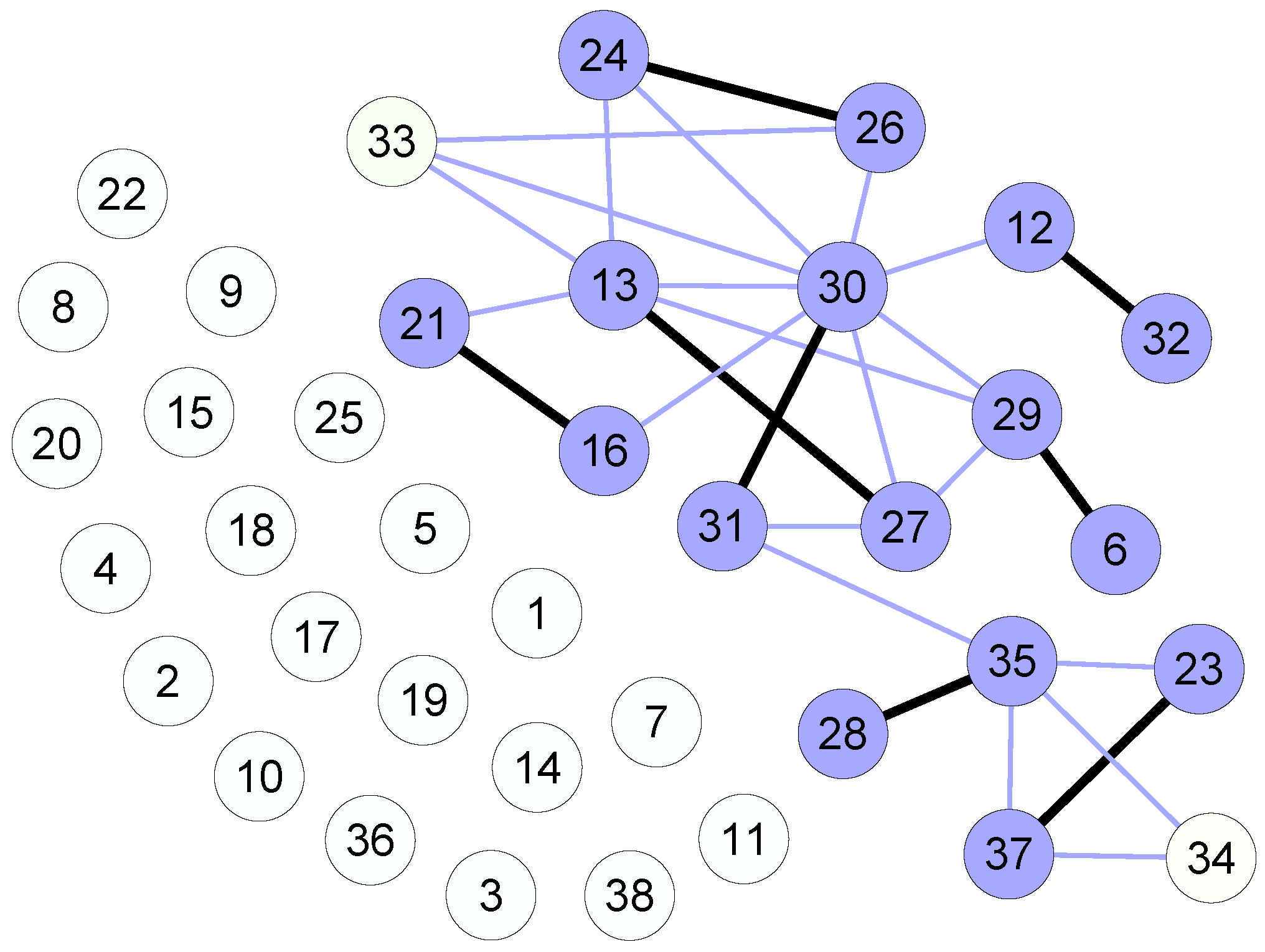
- Twenty patients are mutually incompatible with any donor, for them there is no way to receive a transplant;
- Of the 18 patients left, 16 will be matched, and two will not.
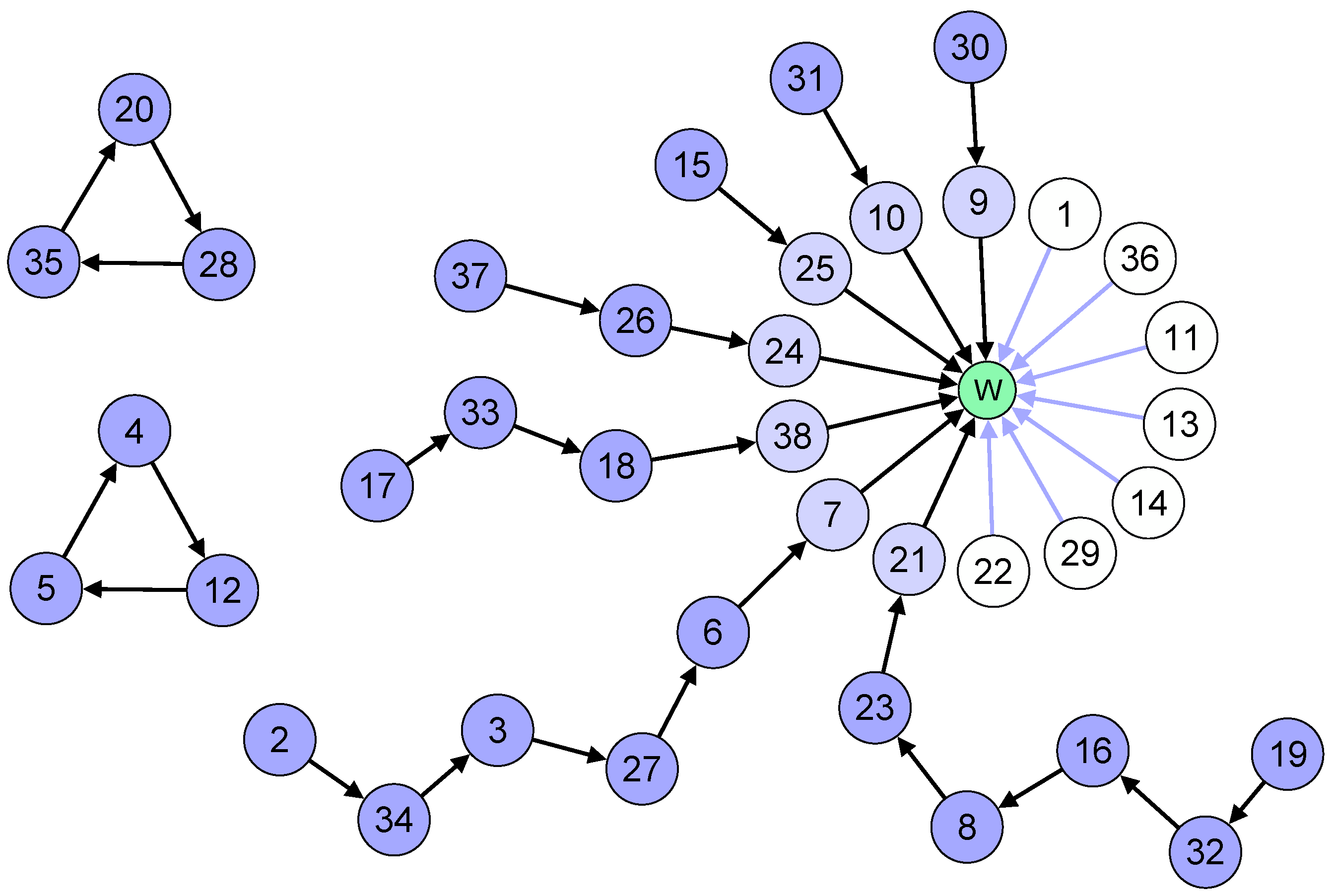
- Two cycles of three patients each will form;
- Seven patients point directly to the waiting list and are not involved in any cycle or chain;
- Seven chains will form: three of length two, one of length three, one of length four two of length six;
- As a result, 24 patients will receive a kidney from a living donor, and seven will get high priority on the waiting list.
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| HLA | Human Leukocyte Antigen |
| PRA | Panel Reactive Antibody |
| TTCC | Top Trading Cycles and Chains |
References
- Garibotto, G.; Pontremoli, R. Manuale di Nefrologia, 1st ed.; Minerva Medica: Torino, Italy, 2012. [Google Scholar]
- Abbas, A.K.; Lichtman, A.H.; Pillai, S. Transplantation Immunology. In Cellular and Molecular Immunology, 6th ed.; Elsevier/Saunders: Philadelphia, PA, USA, 2007. [Google Scholar]
- Wongsaroj, P.; Kahwaji, J.; Vo, A.; Jordan, S.C. Modern approaches to incompatible kidney transplantation. World J. Nephrol. 2015, 4, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Heeger, P.S.; Dinavahi, R. Transplant immunology for non-immunologist. Mt. Sinai J. Med. 2012, 79, 376–387. [Google Scholar] [CrossRef] [PubMed]
- Aull, M.J.; Kapur, S. Kidney paired donation and its potential impact on transplantation. Surg. Clin. N. Am. 2013, 93, 1407–1421. [Google Scholar] [CrossRef] [PubMed]
- Glorie, K.; Haase-Kromwijk, B.; van de Klundert, J.; Wagelmans, A.; Weimar, W. Allocation and matching in kidney exchange programs. Transpl. Int. 2014, 27, 333–343. [Google Scholar] [CrossRef] [PubMed]
- Chkhotua, A. Paired kidney donation: Outcomes, limitations, and future perspectives. Transplant. Proc. 2012, 44, 1790–1792. [Google Scholar] [CrossRef] [PubMed]
- Rapaport, F.T. The case for a living emotionally related international kidney donor exchange registry. Transplant. Proc. 1986, 18, 5–9. [Google Scholar] [PubMed]
- De Klerk, M.; Keizer, K.M.; Claas, F.H.J.; Witvliet, M.; Haase-Kromwijk, B.J.; Weimar, W. The Dutch national living donor kidney exchange program. Am. J. Transplant. 2005, 5, 2302–2305. [Google Scholar] [CrossRef] [PubMed]
- Mierzejewska, B.; Durlik, M.; Lisik, W.; Baum, C.; Schroder, P.; Kopke, J.; Rees, M.; Stepkowski, S. Current approaches in national kidney paired donation programs. Ann. Transplant. 2013, 18, 112–124. [Google Scholar] [CrossRef] [PubMed]
- Barsotti, M.; Boggi, U.; Tregnaghi, C.; Paleologo, G.; Nerucci, B.; Bianchi, A.; Vistoli, F.; Croce, C.; Amorese, G.; Mariotti, M.L.; et al. Living donor kidney transplant: The crossover modality. G. Ital. Nefrol. 2009, 26, 488–498. [Google Scholar] [PubMed]
- Den Hartogh, G. Trading with the waiting-list: The justice of living donor list exchange. Bioethics 2010, 24, 190–198. [Google Scholar] [CrossRef] [PubMed]
- Zenios, S.A.; Woodle, E.S.; Ross, L.F. Primum non nocere: Avoiding harm to vulnerable wait list candidates in an indirect kidney exchange. Transplantation 2001, 72, 648–654. [Google Scholar] [CrossRef] [PubMed]
- Roth, A.E.; Sönmez, T.; Ünver, M.U. Pairwise kidney exchange. J. Econ. Theor. 2005, 125, 151–188. [Google Scholar] [CrossRef]
- Roth, A.E.; Sönmez, T.; Ünver, M.U. Kidney exchange. Q. J. Econ. 2004, 119, 457–488. [Google Scholar] [CrossRef]
- Ünver, M.U. Dynamic kidney exchange. Rev. Econ. Stud. 2010, 77, 372–414. [Google Scholar] [CrossRef]
- Ferrari, P.; Weimar, W.; Johnson, R.J.; Lim, W.H.; Tinckam, K.J. Kidney paired donation: Principles, protocols and programs. Nephrol. Dial. Transplant. 2015, 30, 1276–1285. [Google Scholar] [CrossRef] [PubMed]
- Edmonds, J. Maximum matching and a polyhedron with 0,1 vertices. J. Res. Nat. Bur. Stand. 1965, 69, 125–130. [Google Scholar] [CrossRef]
- Edmonds, J. Path, trees and flowers. Can. J. Math. 1965, 17, 449–467. [Google Scholar] [CrossRef]
- 60 Lives, 30 Kidneys, All Linked. Available online: http://www.webcitation.org/6gRckXL3y (accessed on 1 April 2016).
- Centro Nazionale Trapianti—Comunicato Stampa del 10 Aprile 2015. Available online: http://www.webcitation.org/6gRcwxUmi (accessed on 1 April 2016).
- Anderson, R.; Ashlagi, I.; Gamarnik, D.; Roth, A.E. Finding long chains in kidney exchange using the traveling salesman problem. Proc. Natl. Acad. Sci. USA 2015, 112, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.; Ashlagi, I.; Gamarnik, D.; Rees, M.; Roth, A.E.; Sönmez, T.; Ünver, M.U. Kidney Exchange and the Alliance for Paired Donation: Operations Research Changes the Way Kidneys Are Transplanted. Interfaces 2015, 45, 26–42. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Recipients | Donors | ||
|---|---|---|---|---|
| No. | (%) | No. | (%) | |
| Sex | ||||
| Female | 23 | (61) | 18 | (47) |
| Male | 15 | (39) | 20 | (53) |
| Blood type | ||||
| O | 21 | (55) | 19 | (50) |
| A | 15 | (39) | 17 | (45) |
| B | 1 | (3) | 2 | (5) |
| AB | 1 | (3) | 0 | (0) |
| PRA distribution | ||||
| Low PRA (<15%) | 10 | (26) | ||
| Medium PRA (15%–79%) | 14 | (37) | ||
| High PRA (>80%) | 14 | (37) | ||
| Condition | Points | |
|---|---|---|
| Points based on age difference between donor and recipient | Less than 10 years | 3.5 |
| 10–20 years | 2 | |
| 20–30 years | 1 | |
| More than 30 years | 0 | |
| Points based on number of HLA antigens matches between donor and recipient | 1 | 0.5 |
| 2 | 1 | |
| 3 | 1.5 | |
| 4 | 2 | |
| 5 | 2.5 | |
| 6 | 3 | |
| Bonus points | Same transplant center | 5 |
| Blood group identity | 0.5 | |
| Six HLA antigens matches | 6 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salvioli, M.; Lucchetti, R.; Torelli, R. Simulating the Impact of Crossover Kidney Transplantation on the Nord Italia Transplant Program. Games 2016, 7, 30. https://doi.org/10.3390/g7040030
Salvioli M, Lucchetti R, Torelli R. Simulating the Impact of Crossover Kidney Transplantation on the Nord Italia Transplant Program. Games. 2016; 7(4):30. https://doi.org/10.3390/g7040030
Chicago/Turabian StyleSalvioli, Monica, Roberto Lucchetti, and Rosanna Torelli. 2016. "Simulating the Impact of Crossover Kidney Transplantation on the Nord Italia Transplant Program" Games 7, no. 4: 30. https://doi.org/10.3390/g7040030
APA StyleSalvioli, M., Lucchetti, R., & Torelli, R. (2016). Simulating the Impact of Crossover Kidney Transplantation on the Nord Italia Transplant Program. Games, 7(4), 30. https://doi.org/10.3390/g7040030