
Proton Beam Therapy for Non-Small Cell Lung Cancer: Current Clinical Evidence and Future Directions

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
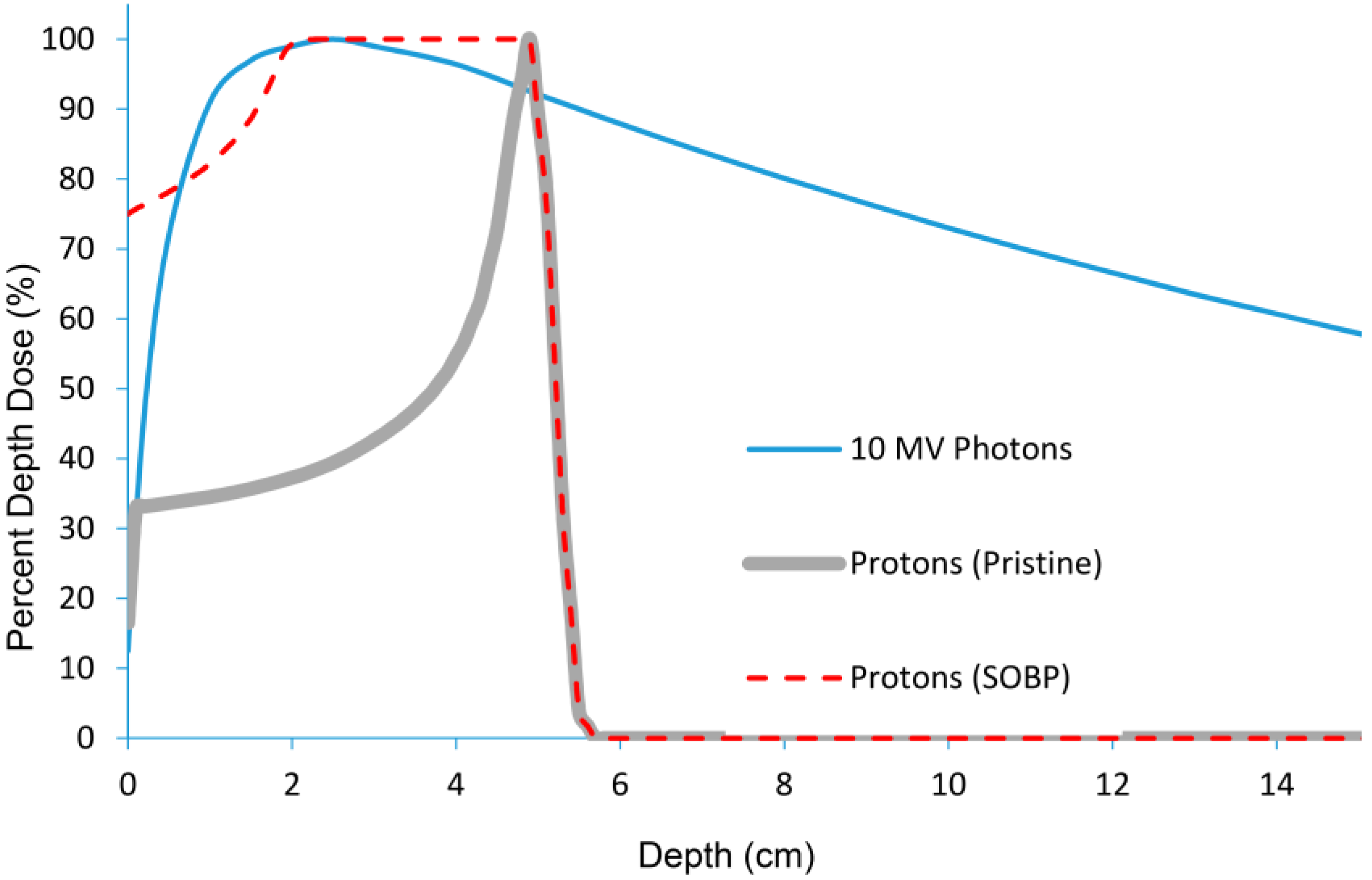
2. A Primer on Proton Beam Therapy Physics

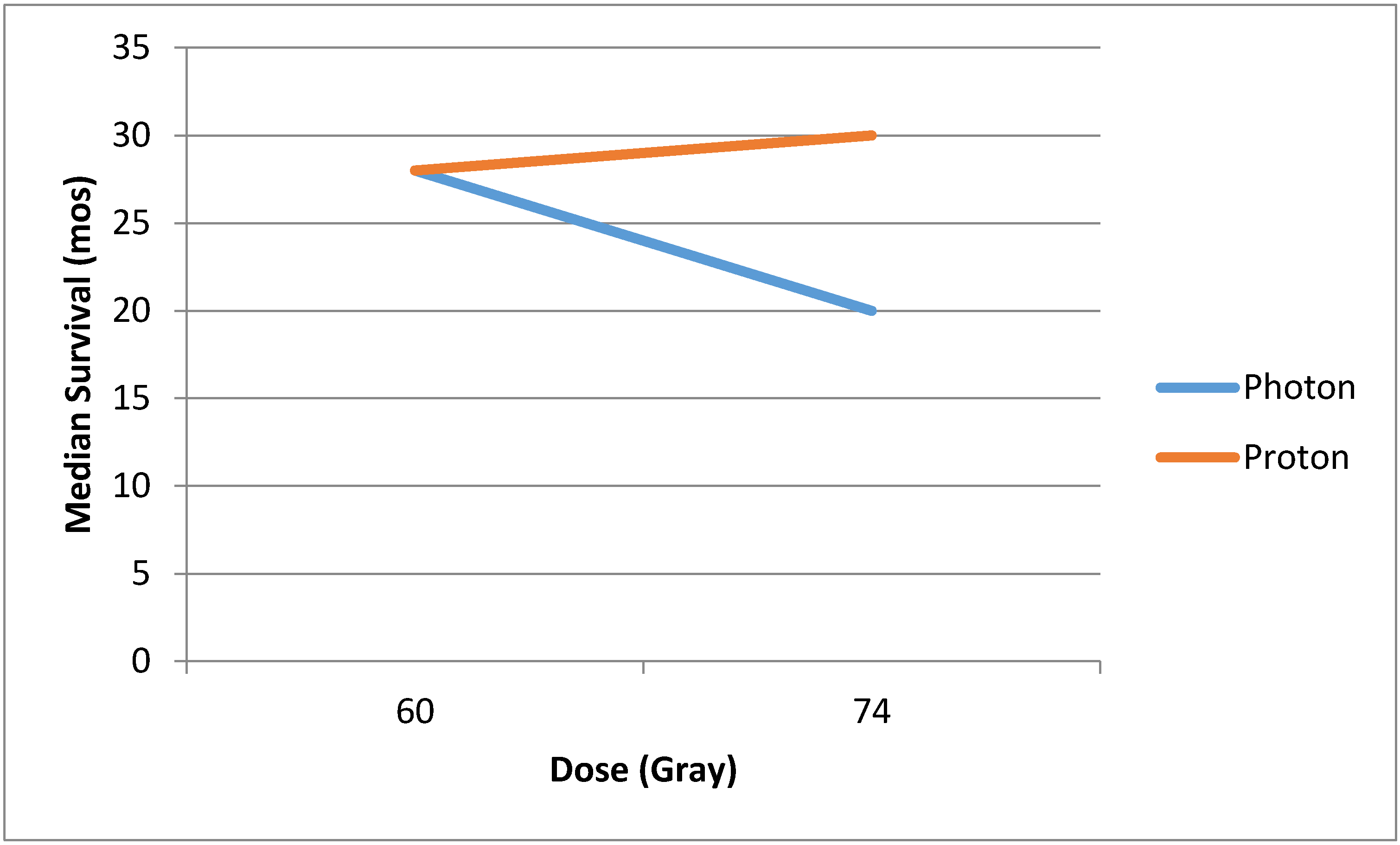
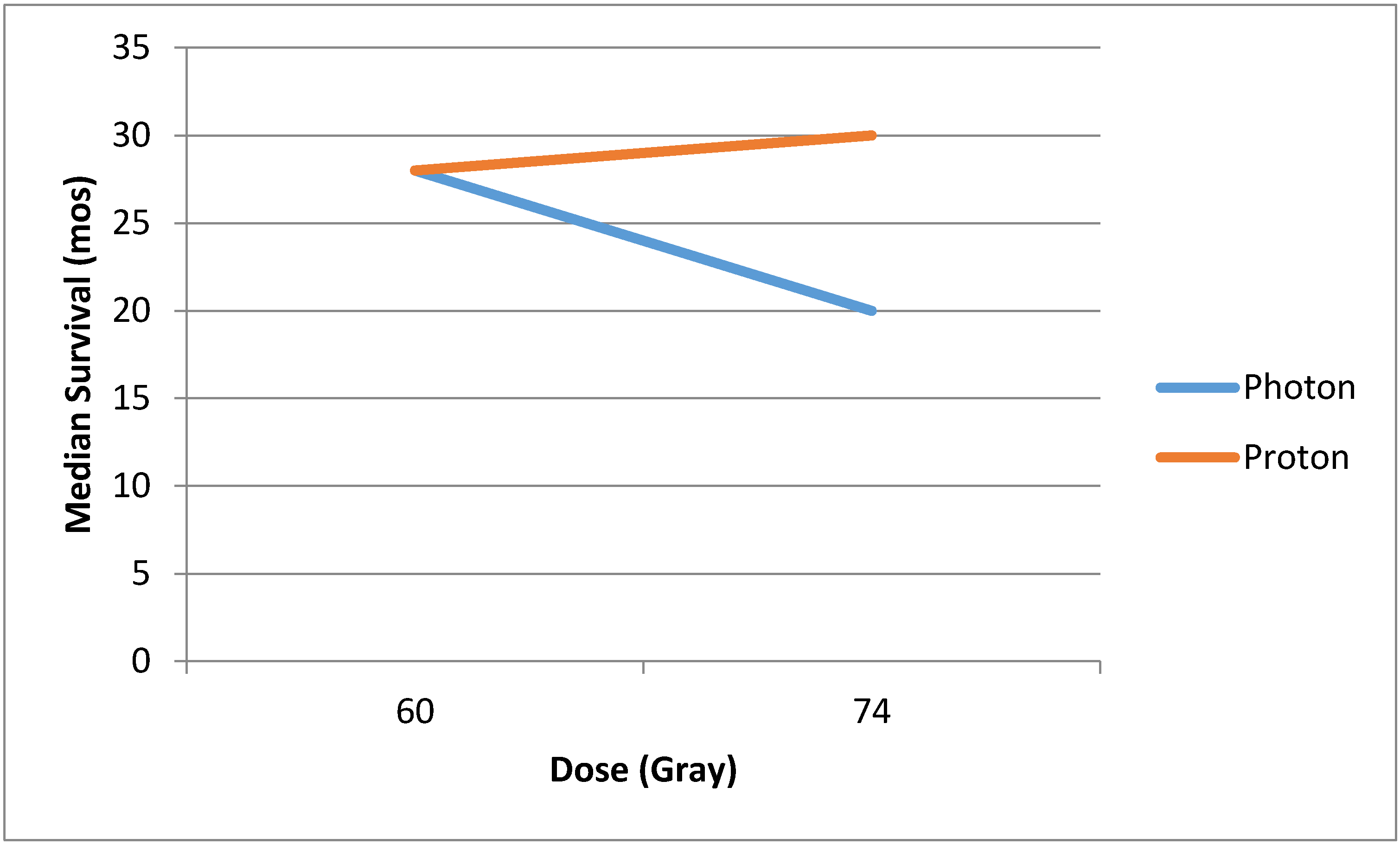
3. Proton Beam Therapy for Locally-Advanced Non-Small Cell Lung Cancer
4. Proton Beam Therapy for Early-Stage Non-Small Cell Lung Cancer
5. Special Situations for Proton Beam Therapy
5.1. Re-Irradiation
5.2. Post-Operative Radiation Therapy for Locally-Advanced NSCLC
6. Caution Using Proton Beam Therapy
6.1. Anatomic Changes
6.2. Motion Management
7. The Future of Proton Beam Therapy Technology: Pencil Beam Scanning
8. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Berman, A.T.; Shea, J.A.; Baffic, C.; Vapiwala, N. Is there a need for resident training in clinical trial design? Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 969–970. [Google Scholar] [CrossRef] [PubMed]
- Zietman, A.L.; Bae, K.; Slater, J.D.; Shipley, W.U.; Efstathiou, J.A.; Coen, J.J.; Bush, D.A.; Lunt, M.; Spiegel, D.Y.; Skowronski, R.; et al. Randomized trial comparing conventional-dose with high-dose conformal radiation therapy in early-stage adenocarcinoma of the prostate: Long-term results from proton radiation oncology group/american college of radiology 95–09. J. Clin. Oncol. 2010, 28, 1106–1111. [Google Scholar] [CrossRef] [PubMed]
- Yock, T.I.; Tarbell, N.J. Technology insight: Proton beam radiotherapy for treatment in pediatric brain tumors. Nat. Clin. Pract. Oncol. 2004, 1, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2015. CA Cancer J. Clin. 2015, 65, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Senan, S.; Oberije, C.; Belderbos, J.; de Dios, N.R.; Bradley, J.D.; Barriger, R.B.; Moreno-Jimenez, M.; Kim, T.H.; Ramella, S.; et al. Predicting esophagitis after chemoradiation therapy for non-small cell lung cancer: An individual patient data meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 690–696. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Senan, S.; Tsujino, K.; Barriger, R.B.; Rengan, R.; Moreno, M.; Bradley, J.D.; Kim, T.H.; Ramella, S.; Marks, L.B.; et al. Predicting radiation pneumonitis after chemoradiation therapy for lung cancer: An international individual patient data meta-analysis. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 444–450. [Google Scholar] [CrossRef] [PubMed]
- Paganetti, H.; Niemierko, A.; Ancukiewicz, M.; Gerweck, L.E.; Goitein, M.; Loeffler, J.S.; Suit, H.D. Relative biological effectiveness (RBE) values for proton beam therapy. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 407–421. [Google Scholar] [CrossRef]
- Curran, W.J., Jr.; Paulus, R.; Langer, C.J.; Komaki, R.; Lee, J.S.; Hauser, S.; Movsas, B.; Wasserman, T.; Rosenthal, S.A.; Gore, E.; et al. Sequential vs. Concurrent chemoradiation for stage III non-small cell lung cancer: Randomized phase III trial RTOG 9410. J. Natl. Cancer Inst. 2011, 103, 1452–1460. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.T.; Rengan, R. New approaches to radiotherapy as definitive treatment for inoperable lung cancer. Semin. Thorac. Cardiovasc. Surg. 2008, 20, 188–197. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Zhang, X.; Wang, X.; Kang, Y.; Riley, B.; Bilton, S.; Mohan, R.; Komaki, R.; Cox, J.D. Significant reduction of normal tissue dose by proton radiotherapy compared with three-dimensional conformal or intensity-modulated radiation therapy in stage I or stage III non-small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Dillman, R.O.; Herndon, J.; Seagren, S.L.; Eaton, W.L., Jr.; Green, M.R. Improved survival in stage III non-small-cell lung cancer: Seven-year follow-up of cancer and leukemia group b (CALGB) 8433 trial. J. Natl. Cancer Inst. 1996, 88, 1210–1215. [Google Scholar] [CrossRef] [PubMed]
- Kong, F.M.; Ten Haken, R.K.; Schipper, M.J.; Sullivan, M.A.; Chen, M.; Lopez, C.; Kalemkerian, G.P.; Hayman, J.A. High-dose radiation improved local tumor control and overall survival in patients with inoperable/unresectable non-small-cell lung cancer: Long-term results of a radiation dose escalation study. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 324–333. [Google Scholar] [CrossRef] [PubMed]
- Auperin, A.; Le Pechoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C.; Paulus, R.; et al. Meta-analysis of concomitant versus sequential radiochemotherapy in locally advanced non-small-cell lung cancer. J. Clin. Oncol. 2010, 28, 2181–2190. [Google Scholar] [CrossRef] [PubMed]
- Machtay, M.; Bae, K.; Movsas, B.; Paulus, R.; Gore, E.M.; Komaki, R.; Albain, K.; Sause, W.T.; Curran, W.J. Higher biologically effective dose of radiotherapy is associated with improved outcomes for locally advanced non-small cell lung carcinoma treated with chemoradiation: An analysis of the radiation therapy oncology group. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Bradley, J.D.; Paulus, R.; Komaki, R.; Masters, G.; Blumenschein, G.; Schild, S.; Bogart, J.; Hu, C.; Forster, K.; Magliocco, A.; et al. Standard-dose vs high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): A randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015, 16, 187–199. [Google Scholar] [PubMed]
- Bonnet, R.B.; Bush, D.; Cheek, G.A.; Slater, J.D.; Panossian, D.; Franke, C.; Slater, J.M. Effects of proton and combined proton/photon beam radiation on pulmonary function in patients with resectable but medically inoperable non-small cell lung cancer. Chest 2001, 120, 1803–1810. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Komaki, R.; Lu, C.; Wen, H.Y.; Allen, P.K.; Tsao, A.; Gillin, M.; Mohan, R.; Cox, J.D. Phase 2 study of high-dose proton therapy with concurrent chemotherapy for unresectable stage III nonsmall cell lung cancer. Cancer 2011, 117, 4707–4713. [Google Scholar] [CrossRef] [PubMed]
- Oshiro, Y.; Mizumoto, M.; Okumura, T.; Hashimoto, T.; Fukumitsu, N.; Ohkawa, A.; Kanemoto, A.; Hashii, H.; Ohno, T.; Sakae, T.; et al. Results of proton beam therapy without concurrent chemotherapy for patients with unresectable stage III non-small cell lung cancer. J. Thorac. Oncol. 2012, 7, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Oshiro, Y.; Okumura, T.; Kurishima, K.; Homma, S.; Mizumoto, M.; Ishikawa, H.; Onizuka, M.; Sakai, M.; Goto, Y.; Hizawa, N.; et al. High-dose concurrent chemo-proton therapy for stage III nsclc: Preliminary results of a phase II study. J. Radiat. Res. 2014, 55, 959–965. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, B.S.; Flampouri, S.; Henderson, R.H.; Pham, D.; Bajwa, A.A.; D’Agostino, H.; Huh, S.N.; Li, Z.; Mendenhall, N.P.; Nichols, R.C. Proton therapy with concurrent chemotherapy for non-small-cell lung cancer: Technique and early results. Clin. Lung Cancer 2012, 13, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Clinical Trials Database. Available online: https://www.clinicaltrials.gov/ct2/show/NCT01993810?term=rtog&recr=Open&rank=01993812 (accessed on 29 January 2015).
- Hoppe, B.S.; Huh, S.; Flampouri, S.; Nichols, R.C.; Oliver, K.R.; Morris, C.G.; Mendenhall, N.P.; Li, Z. Double-scattered proton-based stereotactic body radiotherapy for stage I lung cancer: A dosimetric comparison with photon-based stereotactic body radiotherapy. Radiot. Oncol. 2010, 97, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Macdonald, O.K.; Kruse, J.J.; Miller, J.M.; Garces, Y.I.; Brown, P.D.; Miller, R.C.; Foote, R.L. Proton beam radiotherapy vs three-dimensional conformal stereotactic body radiotherapy in primary peripheral, early-stage non-small-cell lung carcinoma: A comparative dosimetric analysis. Int. J. Radiat. Oncol. Biol. Phys. 2009, 75, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Nakayama, H.; Sugahara, S.; Sakae, T.; Tokuuye, K. Comparisons of dose-volume histograms for proton-beam vs. 3-D conformal x-ray therapy in patients with stage I non-small cell lung cancer. Strahlenther. Onkol. 2009, 185, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Bush, D.A. Proton radiation therapy for lung cancer: Is there enough evidence? Oncology 2010, 24, 1052–1057. [Google Scholar] [PubMed]
- Hata, M.; Tokuuye, K.; Kagei, K.; Sugahara, S.; Nakayama, H.; Fukumitsu, N.; Hashimoto, T.; Mizumoto, M.; Ohara, K.; Akine, Y. Hypofractionated high-dose proton beam therapy for stage I non-small-cell lung cancer: Preliminary results of a phase I/II clinical study. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Nakayama, H.; Sugahara, S.; Tokita, M.; Satoh, H.; Tsuboi, K.; Ishikawa, S.; Tokuuye, K. Proton beam therapy for patients with medically inoperable stage I non-small-cell lung cancer at the university of tsukuba. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 467–471. [Google Scholar] [CrossRef] [PubMed]
- Bush, D.A.; Slater, J.D.; Shin, B.B.; Cheek, G.; Miller, D.W.; Slater, J.M. Hypofractionated proton beam radiotherapy for stage I lung cancer. Chest 2004, 126, 1198–1203. [Google Scholar] [CrossRef] [PubMed]
- Bush, D.A.; Cheek, G.; Zaheer, S.; Wallen, J.; Mirshahidi, H.; Katerelos, A.; Grove, R.; Slater, J.D. High-dose hypofractionated proton beam radiation therapy is safe and effective for central and peripheral early-stage non-small cell lung cancer: Results of a 12-year experience at loma linda university medical center. Int. J. Radiat. Oncol. Biol. Phys. 2013, 86, 964–968. [Google Scholar] [CrossRef] [PubMed]
- Seco, J.; Panahandeh, H.R.; Westover, K.; Adams, J.; Willers, H. Treatment of non-small cell lung cancer patients with proton beam-based stereotactic body radiotherapy: Dosimetric comparison with photon plans highlights importance of range uncertainty. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, 354–361. [Google Scholar] [CrossRef] [PubMed]
- Seco, J.; Gu, G.; Marcelos, T.; Kooy, H.; Willers, H. Proton arc reduces range uncertainty effects and improves conformality compared with photon volumetric modulated arc therapy in stereotactic body radiation therapy for non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Plastaras, J.P.; Berman, A.T.; Freedman, G. Special cases for proton beam radiotherapy: Reirradiation, lymphoma, and breast cancer. Semin. Oncol. 2014, 41, 807–819. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.T.; Ciunci, C.A.; Lin, H.; Both, S.; Langer, C.J.; Varillo, K.; Rengan, R.; Hahn, S.M.; Fagundes, M.D.; Hartsell, W.; et al. Multi-institutional Prospective Study of Reirradiation with Proton Beam Radiotherapy for Non-Small Cell Lung Cancer Paper. In Americal Society of Clinical Oncology Annual Meeting, Chicago, IL, USA, 31 May–4 June 2013.
- McAvoy, S.; Ciura, K.; Wei, C.; Rineer, J.; Liao, Z.; Chang, J.Y.; Palmer, M.B.; Cox, J.D.; Komaki, R.; Gomez, D.R. Definitive reirradiation for locoregionally recurrent non-small cell lung cancer with proton beam therapy or intensity modulated radiation therapy: Predictors of high-grade toxicity and survival outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 819–827. [Google Scholar] [CrossRef] [PubMed]
- Port meta-analysis trialists group. Postoperative radiotherapy in non-small-cell lung cancer: Systematic review and meta-analysis of individual patient data from nine randomised controlled trials. Lancet 1998, 352, 257–263. [Google Scholar]
- Machtay, M.; Lee, J.H.; Shrager, J.B.; Kaiser, L.R.; Glatstein, E. Risk of death from intercurrent disease is not excessively increased by modern postoperative radiotherapy for high-risk resected non-small-cell lung carcinoma. J. Clin. Oncol. 2001, 19, 3912–3917. [Google Scholar] [PubMed]
- Douillard, J.Y.; Rosell, R.; De Lena, M.; Riggi, M.; Hurteloup, P.; Mahe, M.A. Impact of postoperative radiation therapy on survival in patients with complete resection and stage I, II, or IIIA non-small-cell lung cancer treated with adjuvant chemotherapy: The adjuvant navelbine international trialist association (ANITA) randomized trial. Int. J. Radiat. Oncol. Biol. Phys. 2008, 72, 695–701. [Google Scholar] [PubMed]
- Lally, B.E.; Detterbeck, F.C.; Geiger, A.M.; Thomas, C.R., Jr.; Machtay, M.; Miller, A.A.; Wilson, L.D.; Oaks, T.E.; Petty, W.J.; Robbins, M.E.; et al. The risk of death from heart disease in patients with nonsmall cell lung cancer who receive postoperative radiotherapy: Analysis of the surveillance, epidemiology, and end results database. Cancer 2007, 110, 911–917. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.T.; Teo, B.-K.K.; Dolney, D.; Swisher-McClure, S.; Shahnazi, K.; Both, S.; Rengan, R. An in-silico comparison of proton beam and imrt for postoperative radiotherapy in completely resected stage IIIA non-small cell lung cancer. Radiat. Oncol. 2013, 8, 144. [Google Scholar] [CrossRef] [PubMed]
- Remick, J.S.; Gabriel, P.; Kralik, J.; Levin, W.P.; Kucharczuk, J.K.; Pechet, T.T.V.; Rengan, R.; Simone, C.B.; Berman, A.T. First Clinical Report of Proton Beam Therapy Versus Intensity Modulated Radiation Therapy for Post-operative Radiotherapy for Non-small Cell Lung Cancer. In PTCOG Annual Meeting, San Diego, CA, USA, 18–23 May 2015.
- Koay, E.J.; Lege, D.; Mohan, R.; Komaki, R.; Cox, J.D.; Chang, J.Y. Adaptive/nonadaptive proton radiation planning and outcomes in a phase II trial for locally advanced non-small cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2012, 84, 1093–1100. [Google Scholar] [CrossRef] [PubMed]
- Moyers, M.F.; Miller, D.W.; Bush, D.A.; Slater, J.D. Methodologies and tools for proton beam design for lung tumors. Int. J. Radiat. Oncol. Biol. Phys. 2001, 49, 1429–1438. [Google Scholar] [CrossRef]
- Wang, N.; Patyal, B.; Ghebremedhin, A.; Bush, D. Evaluation and comparison of new 4dct based strategies for proton treatment planning for lung tumors. Radiat. Oncol. 2013, 8, 73. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Y.; Li, H.; Zhu, X.R.; Liao, Z.; Zhao, L.; Liu, A.; Li, Y.; Sahoo, N.; Poenisch, F.; Gomez, D.R.; et al. Clinical implementation of intensity modulated proton therapy for thoracic malignancies. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Kesarwala, A.H.; Ko, C.J.; Ning, H.; Xanthopoulos, E.; Haglund, K.E.; O’Meara, W.P.; Simone, C.B., II; Rengan, R. Intensity-modulated proton therapy for elective nodal irradiation and involved-field radiation in the definitive treatment of locally advanced non-small cell lung cancer: A dosimetric study. Clin. Lung Cancer 2015, 16, 237–244. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Berman, A.T.; James, S.S.; Rengan, R. Proton Beam Therapy for Non-Small Cell Lung Cancer: Current Clinical Evidence and Future Directions. Cancers 2015, 7, 1178-1190. https://doi.org/10.3390/cancers7030831
Berman AT, James SS, Rengan R. Proton Beam Therapy for Non-Small Cell Lung Cancer: Current Clinical Evidence and Future Directions. Cancers. 2015; 7(3):1178-1190. https://doi.org/10.3390/cancers7030831
Chicago/Turabian StyleBerman, Abigail T., Sara St. James, and Ramesh Rengan. 2015. "Proton Beam Therapy for Non-Small Cell Lung Cancer: Current Clinical Evidence and Future Directions" Cancers 7, no. 3: 1178-1190. https://doi.org/10.3390/cancers7030831
APA StyleBerman, A. T., James, S. S., & Rengan, R. (2015). Proton Beam Therapy for Non-Small Cell Lung Cancer: Current Clinical Evidence and Future Directions. Cancers, 7(3), 1178-1190. https://doi.org/10.3390/cancers7030831