

Diagnostic Capability and Improved Clinical Management of 18F-DCFPyL-PSMA PET/CT in Occult Biochemical Recurrence of Prostate Cancer After Prostatectomy

 ,
,  , ,
, ,
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Imaging Protocol and Analysis
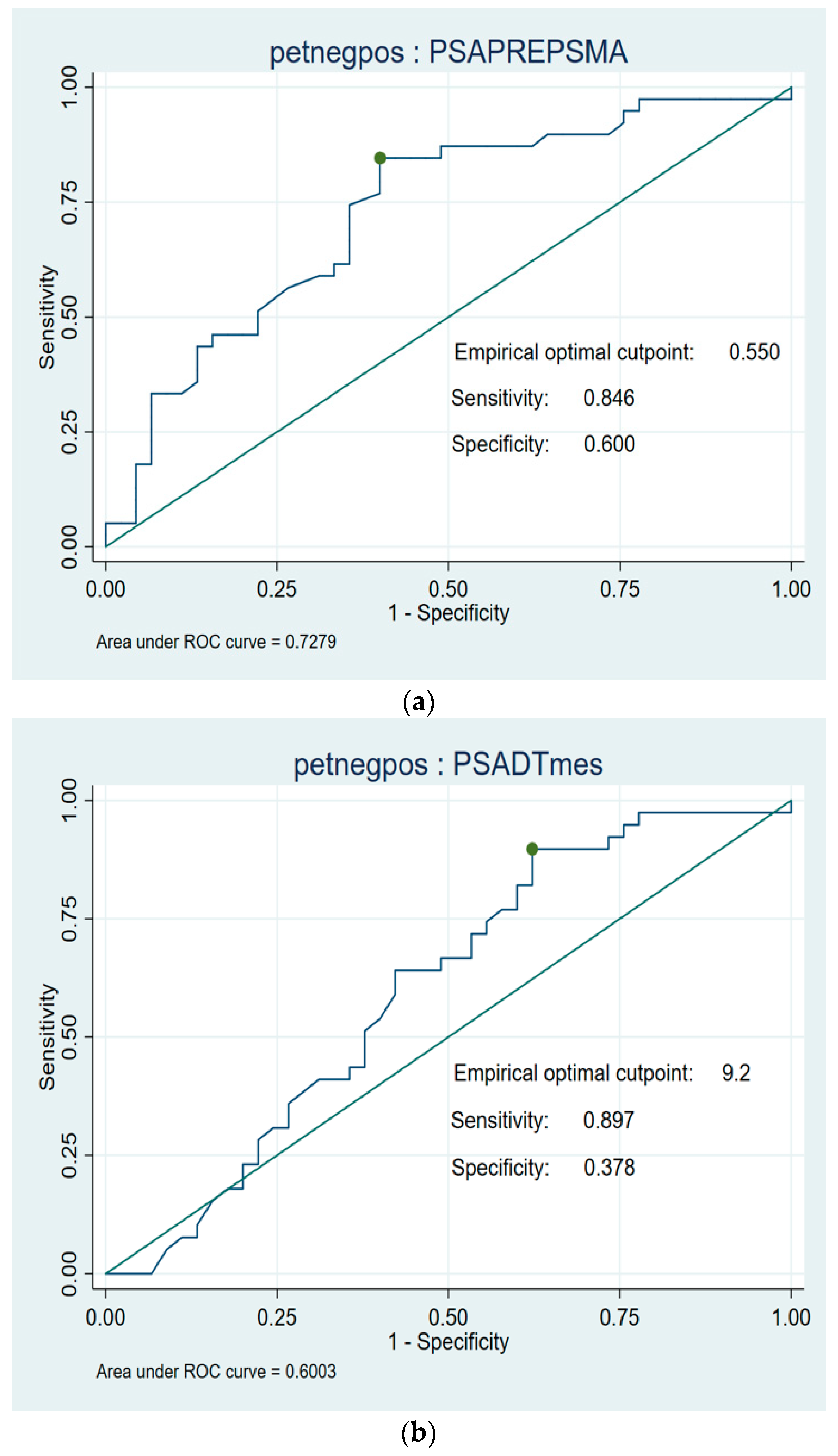
2.2. Statistical Analysis
3. Results
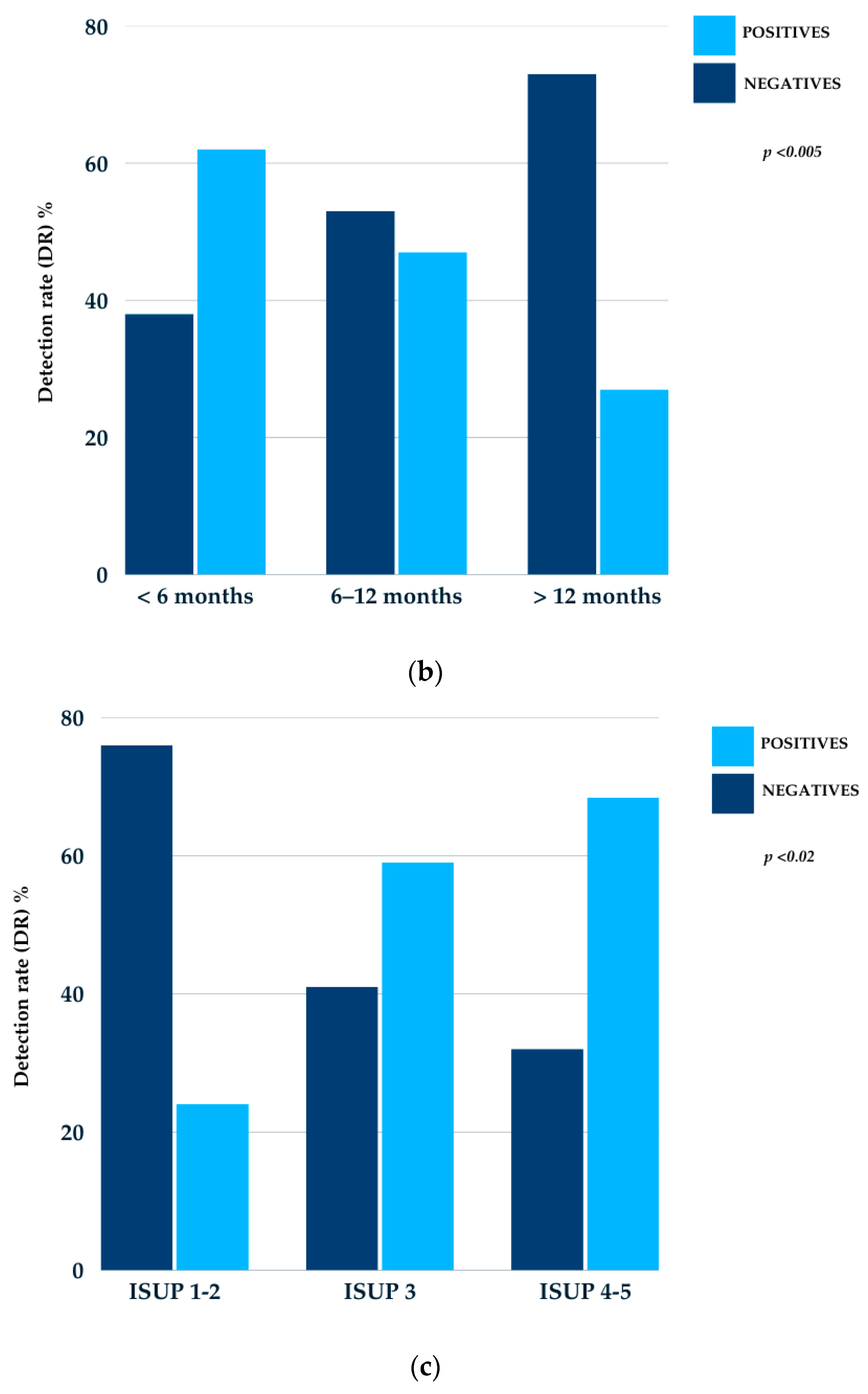
3.1. 18F-DCFPyL PET/CT Detection Rate
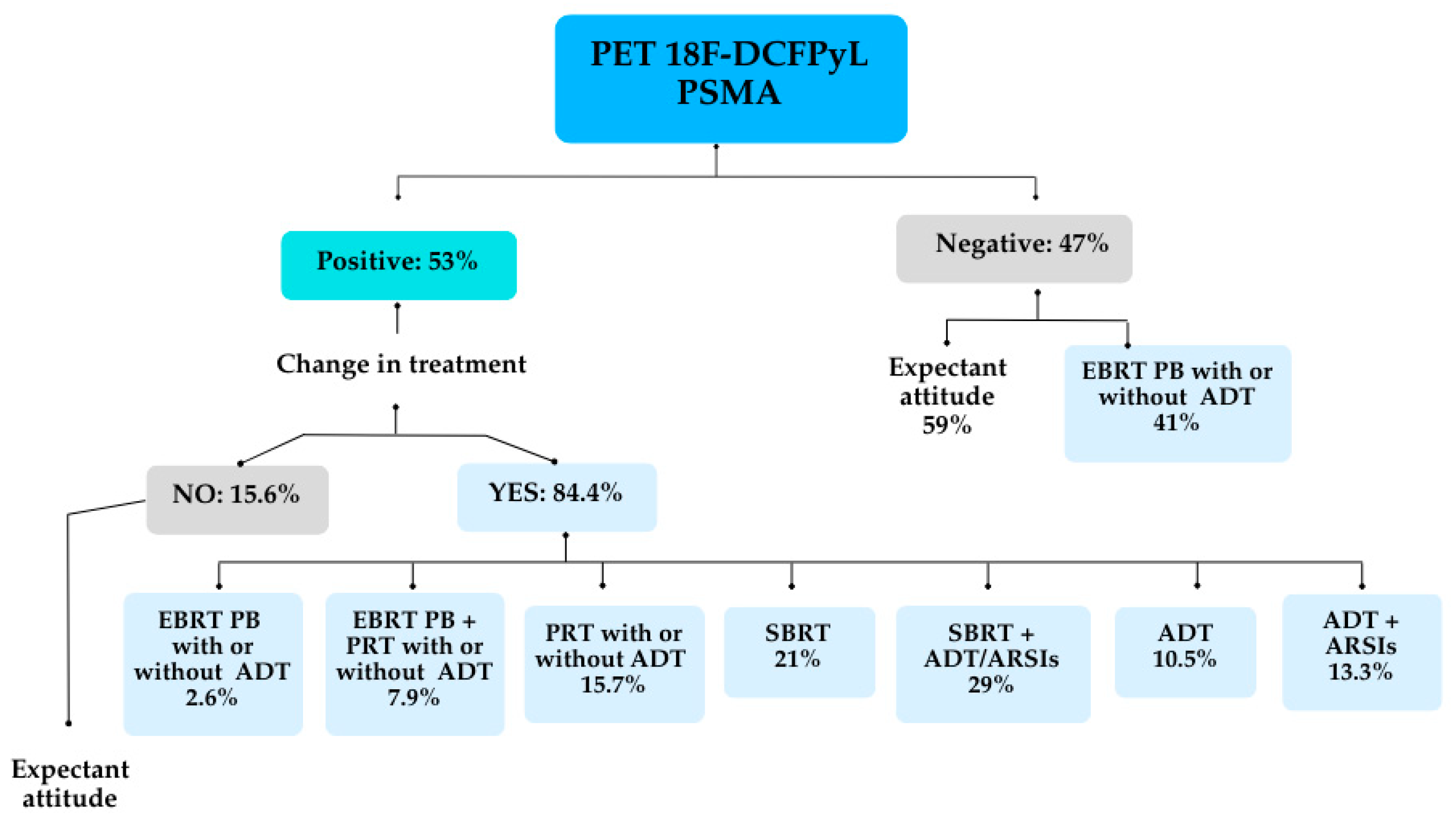
3.2. Changes in Therapeutic Decisions and Overall Clinical Management
4. Discussion
Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| EBRT | External bean radiation therapy |
| PB | Prostate bed |
| ADT | Androgen deprivation therapy |
| PRT | Pelvis radiation therapy |
| SBRT | Stereotactic body radiation therapy |
| ARSIs | Androgen receptor signaling inhibitors |
| PLND | Pelvic lymph node dissection |
| AUC | Area under the curve |
References
- Han, M.; Partin, A.W.; Zahurak, M.; Piantadosi, S.; Epstein, J.I.; Walsh, P.C. Biochemical (Prostate Specific Antigen) Recurrence Probability Following Radical Prostatectomy for Clinically Localized Prostate Cancer. J. Urol. 2003, 169, 517–523. [Google Scholar] [CrossRef]
- Pompe, R.S.; Karakiewicz, P.I.; Tian, Z.; Mandel, P.; Steuber, T.; Schlomm, T.; Salomon, G.; Graefen, M.; Huland, H.; Tilki, D. Oncologic and Functional Outcomes after Radical Prostatectomy for High or Very High Risk Prostate Cancer: European Validation of the Current NCCN® Guideline. J. Urol. 2017, 198, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Roach, M., III; Hanks, G.; Thames, H., Jr.; Schellhammer, P.; Shipley, W.U.; Sokol, G.H.; Sandler, H. Defining Biochemical Failure Following Radiotherapy with or without Hormonal Therapy in Men with Clinically Localized Prostate Cancer: Recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Vargas, H.A.; Martin-Malburet, A.G.; Takeda, T.; Corradi, R.B.; Eastham, J.; Wibmer, A.; Sala, E.; Zelefsky, M.J.; Weber, W.A.; Hricak, H. Localizing Sites of Disease in Patients with Rising Serum Prostate-Specific Antigen up to 1 ng/mL Following Prostatectomy: How Much Information Can Conventional Imaging Provide? Urol. Oncol. 2016, 34, 413.e1–413.e7. [Google Scholar] [CrossRef]
- Venkatesan, A.M.; Mudairu-Dawodu, E.; Duran, C.; Stafford, R.J.; Yan, Y.; Wei, W.; Kundra, V. Detecting Recurrent Prostate Cancer Using Multiparametric MRI, Influence of PSA and Gleason Grade. J. Cancer Imaging 2020, 20, 10. [Google Scholar] [CrossRef]
- Turkbey, B.; Albert, P.S.; Kurdziel, K.; Choyke, P.L. Imaging Localized Prostate Cancer: Current Approaches and New Developments. Am. J. Roentgenol. 2010, 195, 350–360. [Google Scholar] [CrossRef]
- Monteiro, F.S.M.; Schutz, F.A.; Morbeck, I.A.P.; Bastos, D.A.; de Padua, F.V.; Costa, L.A.G.A.; Maia, M.C.; Rinck, J.A., Jr.; Zequi, S.C.; da Trindade, K.M.; et al. Consensus on Treatment and Follow-Up for Biochemical Recurrence in Castration-Sensitive Prostate Cancer: A Report From the First Global Prostate Cancer Consensus Conference for Developing Countries. JCO Glob. Oncol. 2021, 7, 538–544. [Google Scholar] [CrossRef]
- Van den Broeck, T.; van den Bergh, R.C.N.; Briers, E.; Cornford, P.; Cumberbatch, M.; Tilki, D.; De Santis, M.; Fanti, S.; Fossati, N.; Gillessen, S.; et al. Biochemical Recurrence in Prostate Cancer: The European Association of Urology Prostate Cancer Guidelines Panel Recommendations. Eur. Urol. 2019, 76, 8–20. [Google Scholar] [CrossRef]
- Simon, N.I.; Parker, C.; Hope, T.A.; Paller, C.J. Best Approaches and Updates for Prostate Cancer Biochemical Recurrence. Am. Soc. Clin. Oncol. Educ. Book 2022, 42, 1–8. [Google Scholar] [CrossRef]
- Tendulkar, R.D.; Agrawal, S.; Gao, T.; Efstathiou, J.A.; Pisansky, T.M.; Michalski, J.M.; Koontz, B.F.; Hamstra, D.A.; Feng, F.Y.; Liauw, S.L.; et al. Contemporary Update of a Multi-Institutional Predictive Nomogram for Salvage Radiotherapy After Radical Prostatectomy. J. Clin. Oncol. 2016, 34, 3648–3654. [Google Scholar] [CrossRef]
- Parker, C.C.; Clarke, N.W.; Cook, A.D.; Kynaston, H.G.; Petersen, P.M.; Catton, C.; Cross, W.; Logue, J.; Parulekar, W.; Payne, H.; et al. Timing of Radiotherapy after Radical Prostatectomy (RADICALS-RT): A Randomised, Controlled Phase 3 Trial. Lancet 2020, 396, 982–991. [Google Scholar] [CrossRef] [PubMed]
- Pfister, D.; Bolla, M.; Briganti, A.; Carroll, P.; Cozzarini, C.; Joniau, S.; van Poppel, H.; Roach, M.; Stephenson, A.; Wiegel, T.; et al. Early Salvage Radiotherapy Following Radical Prostatectomy. Eur. Urol. 2013, 64, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Jackson, W.C.; Suresh, K.; Tumati, V.; Dess, R.T.; Soni, P.D.; Zhao, S.G.; Zumsteg, Z.S.; Hannan, R.; Hollenbeck, B.K.; George, A.; et al. Impact of Biochemical Failure After Salvage Radiation Therapy on Prostate Cancer-Specific Mortality: Competition Between Age and Time to Biochemical Failure. Eur. Urol. Oncol. 2019, 2, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Tumati, V.; Jackson, W.C.; Abugharib, A.E.; Raj, G.; Roehrborn, C.; Lotan, Y.; Courtney, K.; Bagrodia, A.; Gahan, J.C.; Zumsteg, Z.S. Natural History of ‘Second’ Biochemical Failure After Salvage Radiation Therapy for Prostate Cancer: A Multi-Institution Study. BJU Int. 2017, 120, 768–776. [Google Scholar] [CrossRef]
- Wang, R.; Shen, G.; Huang, M.; Tian, R. The Diagnostic Role of 18F-Choline, 18F-Fluciclovine, and 18F-PSMA PET/CT in the Detection of Prostate Cancer With Biochemical Recurrence: A Meta-Analysis. Front. Oncol. 2021, 11, 684629. [Google Scholar] [CrossRef]
- Nanni, C.; Zanoni, L.; Pultrone, C.; Schiavina, R.; Brunocilla, E.; Lodi, F.; Malizia, C.; Ferrari, M.; Rigatti, P.; Fonti, C.; et al. (18F)-FACBC (Anti-1-Amino-3-(18F)-Fluorocyclobutane-1-Carboxylic Acid) Versus (11C)-Choline PET/CT in Prostate Cancer Relapse: Results of a Prospective Trial. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1405–1414. [Google Scholar] [CrossRef]
- Graziani, T.; Ceci, F.; Castellucci, P.; Polverari, G.; Lima, G.M.; Lodi, F.; Morganti, A.G.; Ardizzoni, A.; Schiavina, R.; Fanti, S. (¹¹C)-Choline PET/CT for Restaging Prostate Cancer: Results from 4,426 Scans in a Single-Centre Patient Series. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1971–1979. [Google Scholar] [CrossRef]
- Plaza López, P.J.; Puertas, E.; Aguiló, J.J.; Suárez-Piñera, M.; Domenech, B.; Mestre-Fusco, A.; Casals, J.; Chícharo de Fleitas, J.R. ⁶⁸Ga-PSMA-11 PET/CT in Patients with Occult Biochemical Recurrence of Prostate Carcinoma and Negative 18F-Choline PET/CT: Preliminary Assessment of Its Clinical Use. Actas Urol. Esp. (Engl. Ed.) 2021, 45, 353–358. [Google Scholar] [CrossRef]
- Hofman, M.S.; Lawrentschuk, N.; Francis, R.J.; Tang, C.; Vela, I.; Thomas, P.; Rutherford, N.; Martin, J.M.; Frydenberg, M.; Shakher, R.; et al. Prostate-Specific Membrane Antigen PET-CT in Patients with High-Risk Prostate Cancer Before Curative-Intent Surgery or Radiotherapy (proPSMA): A Prospective, Randomised, Multicentre Study. Lancet 2020, 395, 1208–1216. [Google Scholar] [CrossRef]
- Afshar-Oromieh, A.; Avtzi, E.; Giesel, F.L.; Holland-Letz, T.; Linhart, H.G.; Eder, M.; Eisenhut, M.; Boxler, S.; Hadaschik, B.A.; Kratochwil, C.; et al. The Diagnostic Value of PET/CT Imaging with the 68Ga-Labelled PSMA Ligand HBED-CC in the Diagnosis of Recurrent Prostate Cancer. Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 197–209. [Google Scholar] [CrossRef]
- Huang, S.; Ong, S.; McKenzie, D.; Mirabelli, A.; Chen, D.C.; Chengodu, T.; Murphy, D.G.; Hofman, M.S.; Lawrentschuk, N.; Perera, M. Comparison of 18F-Based PSMA Radiotracers with [⁶⁸Ga]Ga-PSMA-11 in PET/CT Imaging of Prostate Cancer—A Systematic Review and Meta-Analysis. Prostate Cancer Prostatic Dis. 2024, 27, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Fendler, W.P.; Eiber, M.; Beheshti, M.; Bomanji, J.; Calais, J.; Ceci, F.; Cho, S.Y.; Fanti, S.; Giesel, F.L.; Goffin, K.; et al. PSMA PET/CT: Joint EANM Procedure Guideline/SNMMI Procedure Standard for Prostate Cancer Imaging 2.0. Eur. J. Nucl. Med. Mol. Imaging 2023, 50, 1466–1486. [Google Scholar] [CrossRef] [PubMed]
- Rowe, S.P.; Gorin, M.A.; Pomper, M.G. Imaging of Prostate-Specific Membrane Antigen Using [18F]DCFPyL. Clin. Positron Imaging 2017, 10, 177–187. [Google Scholar] [CrossRef] [PubMed]
- Rowe, S.P.; Macura, K.J.; Mena, E.; Blackford, A.L.; Nadal, R.; Antonarakis, E.S.; Eisenberger, M.; Carducci, M.; Fan, H.; Dannals, R.F.; et al. PSMA-Based [18F]DCFPyL PET/CT Is Superior to Conventional Imaging for Lesion Detection in Patients with Metastatic Prostate Cancer. Mol. Imaging Biol. 2016, 18, 411–419. [Google Scholar] [CrossRef]
- Pienta, K.J.; Gorin, M.A.; Rowe, S.P.; Carroll, P.R.; Pouliot, F.; Probst, S.; Saperstein, L.; Preston, M.A.; Alva, A.S.; Patnaik, A.; et al. A Phase 2/3 Prospective Multicenter Study of the Diagnostic Accuracy of Prostate-Specific Membrane Antigen PET/CT with 18F-DCFPyL in Prostate Cancer Patients (OSPREY). J. Urol. 2021, 205, 1557–1564. [Google Scholar] [CrossRef]
- Belliveau, C.; Benhacene-Boudam, M.-K.; Juneau, D.; Plouznikoff, N.; Olivié, D.; Alley, S.; Barkati, M.; Delouya, G.; Taussky, D.; Lambert, C.; et al. F18-DCFPyL PSMA-PET/CT Versus MRI: Identifying the Prostate Cancer Region Most at Risk of Radiation Therapy Recurrence for Tumor Dose Escalation. Prostate Cancer Radiother. Oncol. 2024, 13, 163–169. [Google Scholar] [CrossRef]
- Mottet, N.; Van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer-2020 Update. Part 1: Screening, Diagnosis, and Local Treatment with Curative Intent. Eur. Urol. 2020, 79, 243–262. [Google Scholar] [CrossRef]
- Cornford, P.; van den Bergh, R.C.N.; Briers, E.; Van den Broeck, T.; Cumberbatch, M.G.; De Santis, M.; Fanti, S.; Fossati, N.; Gandaglia, G.; Gillessen, S.; et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II—2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur. Urol. 2021, 79, 263–282. [Google Scholar] [CrossRef]
- Ceci, F.; Oprea-Lager, D.E.; Emmett, L.; Adam, J.A.; Bomanji, J.; Czernin, J.; Eiber, M.; Haberkorn, U.; Hofman, M.S.; Hope, T.A.; et al. E-PSMA: The EANM Standardized Reporting Guidelines v1.0 for PSMA-PET. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2466–2473. [Google Scholar] [CrossRef]
- Eiber, M.; Herrmann, K.; Calais, J.; Hadaschik, B.; Giesel, F.L.; Hartenbach, M.; Hope, T.; Reiter, R.; Maurer, T.; Weber, W.A.; et al. Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE): Proposed miTNM Classification for the Interpretation of PSMA-Ligand PET/CT. J. Nucl. Med. 2018, 59, 469–478. [Google Scholar] [CrossRef]
- Seifert, R.; Emmett, L.; Rowe, S.P.; Herrmann, K.; Hadaschik, B.; Calais, J.; Giesel, F.L.; Reiter, R.; Maurer, T.; Heck, M.; et al. Second Version of the Prostate Cancer Molecular Imaging Standardized Evaluation Framework Including Response Evaluation for Clinical Trials (PROMISE V2). Eur. Urol. 2023, 83, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.R.; Pullambhatla, M.; Byun, Y.; Nimmagadda, S.; Green, G.; Fox, J.J.; Horti, A.; Mease, R.C.; Pomper, M.G. 68Ga-labeled inhibitors of prostate-specific membrane antigen (PSMA) for imaging prostate cancer. J. Med. Chem. 2010, 53, 5333–5341. [Google Scholar] [CrossRef]
- Eder, M.; Schäfer, M.; Bauder-Wüst, U.; Hull, W.-E.; Wängler, C.; Mier, W.; Haberkorn, U.; Eisenhut, M. 68Ga-complex lipophilicity and the targeting property of a urea-based PSMA inhibitor for PET imaging. Bioconjug. Chem. 2012, 23, 688–697. [Google Scholar] [CrossRef]
- Chow, K.M.; So, W.Z.; Lee, H.J.; Lee, A.; Yap, D.W.T.; Takwoingi, Y.; Tay, K.J.; Tuan, J.; Thang, S.P.; Lam, W.; et al. Head-to-head comparison of the diagnostic accuracy of prostate-specific membrane antigen positron emission tomography and conventional imaging modalities for initial staging of intermediate- to high-risk prostate cancer: A systematic review and meta-analysis. Eur. Urol. 2023, 84, 36–48. [Google Scholar] [CrossRef]
- Morris, M.J.; Rowe, S.P.; Gorin, M.A.; Saperstein, L.; Pouliot, F.; Josephson, D.; Wong, J.Y.C.; Pantel, A.R.; Cho, S.Y.; Gage, K.L.; et al. Diagnostic Performance of 18F-DCFPyL-PET/CT in Men with Biochemically Recurrent Prostate Cancer: Results from the CONDOR Phase III, Multicenter Study. Clin. Cancer Res. 2021, 27, 3674–3682. [Google Scholar] [CrossRef]
- Fendler, W.P.; Calais, J.; Eiber, M.; Flavell, R.R.; Mishoe, A.; Feng, F.Y.; Nguyen, H.G.; Reiter, R.E.; Rettig, M.B.; Okamoto, S.; et al. Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. JAMA Oncol. 2019, 5, 856–863. [Google Scholar] [CrossRef]
- Aydin, A.M.; Haberal, B.; Artykov, M.; Bilen, C.Y.; Yazici, S. Clinicopathological Predictors of Positive 68Ga-PSMA-11 PET/CT in PSA-Only Recurrence of Localized Prostate Cancer Following Definitive Therapy. Ann. Nucl. Med. 2019, 33, 305–313. [Google Scholar] [CrossRef]
- Hoffmann, M.A.; Buchholz, H.-G.; Wieler, H.J.; Miederer, M.; Rosar, F.; Fischer, N.; Müller-Hübenthal, J.; Trampert, L.; Pektor, S.; Schreckenberger, M. PSA and PSA Kinetics Thresholds for the Presence of 68Ga-PSMA-11 PET/CT-Detectable Lesions in Patients With Biochemical Recurrent Prostate Cancer. Cancers 2020, 12, 398. [Google Scholar] [CrossRef]
- Ceci, F.; Uprimny, C.; Nilica, B.; Geraldo, L.; Kendler, D.; Kroiss, A.; Bektic, J.; Horninger, W.; Lukas, P.; Decristoforo, C.; et al. {68}Ga-PSMA PET/CT for Restaging Recurrent Prostate Cancer: Which Factors Are Associated with PET/CT Detection Rate? Eur. J. Nucl. Med. Mol. Imaging 2015, 42, 1284–1294. [Google Scholar] [CrossRef]
- Perera, M.; Papa, N.; Christidis, D.; Wetherell, D.; Hofman, M.S.; Murphy, D.G.; Bolton, D.; Lawrentschuk, N. Sensitivity, Specificity, and Predictors of Positive 68Ga-Prostate-Specific Membrane Antigen Positron Emission Tomography in Advanced Prostate Cancer: A Systematic Review and Meta-Analysis. Eur. Urol. 2016, 70, 926–937. [Google Scholar] [CrossRef]
- Treglia, G.; Annunziata, S.; Pizzuto, D.A.; Giovanella, L.; Prior, J.O.; Ceriani, L. Detection Rate of {18}F-Labeled PSMA PET/CT in Biochemical Recurrent Prostate Cancer: A Systematic Review and a Meta-Analysis. Cancers 2019, 11, 710. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh, A.; da Cunha, M.L.; Wagner, J.; Haberkorn, U.; Debus, N.; Weber, W.; Eiber, M.; Holland-Letz, T.; Rauscher, I. Performance of [68Ga]Ga-PSMA-11 PET/CT in Patients with Recurrent Prostate Cancer after Prostatectomy—A Multi-Centre Evaluation of 2533 Patients. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2925–2934. [Google Scholar] [CrossRef] [PubMed]
- Grubmüller, B.; Baltzer, P.; D’Andrea, D.; Korn, S.; Haug, A.R.; Hacker, M.; Grubmüller, K.H.; Goldner, G.M.; Wadsak, W.; Pfaff, S.; et al. 68Ga-PSMA-11 Ligand PET Imaging in Patients with Biochemical Recurrence after Radical Prostatectomy—Diagnostic Performance and Impact on Therapeutic Decision-Making. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Hegemann, N.-S.; Fendler, W.P.; Buchner, A.; Stief, C.; Rogowski, P.; Niyazi, M.; Eze, C.; Li, M.; Bartenstein, P.; Belka, C.; et al. Detection Level and Pattern of Positive Lesions Using PSMA PET/CT for Staging Prior to Radiation Therapy. Radiat. Oncol. 2017, 12, 180. [Google Scholar] [CrossRef]
- Mena, E.; Lindenberg, M.L.; Turkbey, I.B.; Shih, J.H.; Harmon, S.A.; Lim, I.; Lin, F.; Adler, S.; Eclarinal, P.; McKinney, Y.L.; et al. 18F-DCFPyL PET/CT Imaging in Patients with Biochemically Recurrent Prostate Cancer After Primary Local Therapy. J. Nucl. Med. 2019, 60, 54–60. [Google Scholar] [CrossRef]
- Calais, J.; Kishan, A.U.; Cao, M.; Fendler, W.P.; Eiber, M.; Herrmann, K.; Ceci, F.; Reiter, R.E.; Rettig, M.B.; Hegde, J.V.; et al. Potential Impact of 68Ga-PSMA-11 PET/CT on the Planning of Definitive Radiation Therapy for Prostate Cancer. J. Nucl. Med. 2018, 59, 1327–1333. [Google Scholar] [CrossRef]
- Roach, P.J.; Francis, R.; Emmett, L.; Hsiao, E.; Kneebone, A.; Hruby, G.; Eade, T.; Nguyen, Q.A.; Thompson, B.D.; Cusick, T.; et al. The Impact of 68Ga-PSMA PET/CT on Management Intent in Prostate Cancer: Results of an Australian Prospective Multicenter Study. J. Nucl. Med. 2017, 58, 1316–1322. [Google Scholar] [CrossRef]
- Emmett, L.; van Leeuwen, P.J.; Nandurkar, R.; Scheltema, M.J.; Cusick, T.; Hruby, G.; Kneebone, A.; Eade, T.; Fogarty, G.; Jagavkar, R.; et al. Treatment Outcomes from 68Ga-PSMA PET/CT-Informed Salvage Radiation Treatment in Men with Rising PSA After Radical Prostatectomy: Prognostic Value of a Negative PSMA PET. J. Nucl. Med. 2017, 58, 1345–1349. [Google Scholar] [CrossRef]
- Song, H.; Harrison, C.; Duan, H.; Guja, K.; Hatami, N.; Franc, B.L.; Moradi, F.; Mari Aparici, C.; Davidzon, G.A.; Iagaru, A. Prospective Evaluation of 18F-DCFPyL PET/CT in Biochemically Recurrent Prostate Cancer in an Academic Center: A Focus on Disease Localization and Changes in Management. J. Nucl. Med. 2020, 61, 826–832. [Google Scholar] [CrossRef]
- Ng, M.; Guerrieri, M.; Wong, L.M.; Taubman, K.; Sutherland, T.; Benson, A.; Byrne, G.; Koschel, S.; Yap, K.; Starmans, M.; et al. Changes in Management After 18F-DCFPyL PSMA PET in Patients Undergoing Postprostatectomy Radiotherapy, with Early Biochemical Response Outcomes. J. Nucl. Med. 2022, 63, 414–421. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Value |
|---|---|
| Age | 48–74 years |
| Median age | 69 years |
| Mean diagnosis PSA | 11.24 ng/mL |
| TNM | |
| T2 a-b | 7 |
| T2c | 36 |
| T3a | 21 |
| T3b | 20 |
| T4 | 1 |
| Nx | 32 |
| N0 | 49 |
| N1 | 4 |
| Mx | 32 |
| M0 | 53 |
| Histological characteristics | |
| Gleason score < 8 | 37 |
| Gleason score > 8 | 48 |
| ISUP 1–2 | 25 |
| ISUP 3 | 22 |
| ISUP 4–5 | 38 |
| Primary treatment | |
| PR | 41 |
| PR + PLND | 44 |
| Radiotherapy | |
| NO | 40 |
| Adjuvant | 12 |
| Salvage | 33 |
| ADT | |
| Yes | 33 |
| No | 52 |
| Median PSA (pre-DCFPyL PET/CT) | 0.59 ng/mL (0.29–1.0) |
| Mean DT-PSA (pre-DCFPyL PET/CT) | 7.2 months (3–9.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amorelli, F.; Foro, P.; Blanco, J.S.; Ocanto, A.; Natali, A.; Fumado, L.; Plaza, P. Diagnostic Capability and Improved Clinical Management of 18F-DCFPyL-PSMA PET/CT in Occult Biochemical Recurrence of Prostate Cancer After Prostatectomy. Cancers 2025, 17, 1272. https://doi.org/10.3390/cancers17081272
Amorelli F, Foro P, Blanco JS, Ocanto A, Natali A, Fumado L, Plaza P. Diagnostic Capability and Improved Clinical Management of 18F-DCFPyL-PSMA PET/CT in Occult Biochemical Recurrence of Prostate Cancer After Prostatectomy. Cancers. 2025; 17(8):1272. https://doi.org/10.3390/cancers17081272
Chicago/Turabian StyleAmorelli, Francesco, Palmira Foro, Juan Sebastian Blanco, Abrahams Ocanto, Augusto Natali, Lluis Fumado, and Pedro Plaza. 2025. "Diagnostic Capability and Improved Clinical Management of 18F-DCFPyL-PSMA PET/CT in Occult Biochemical Recurrence of Prostate Cancer After Prostatectomy" Cancers 17, no. 8: 1272. https://doi.org/10.3390/cancers17081272
APA StyleAmorelli, F., Foro, P., Blanco, J. S., Ocanto, A., Natali, A., Fumado, L., & Plaza, P. (2025). Diagnostic Capability and Improved Clinical Management of 18F-DCFPyL-PSMA PET/CT in Occult Biochemical Recurrence of Prostate Cancer After Prostatectomy. Cancers, 17(8), 1272. https://doi.org/10.3390/cancers17081272