
Somatic Copy Number Alterations in Circulating Cell-Free DNA as a Prognostic Biomarker for Hepatocellular Carcinoma: Insights from a Proof-of-Concept Study

 , , , , , , , , ,
, , , , , , , , , 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Plasma Collection and ccfDNA Extraction
2.3. Shallow Whole Genome Sequencing and Bioinformatic Analysis
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. ctDNA Evaluation
3.2.1. CLD and Cirrhosis
3.2.2. HCC Patients
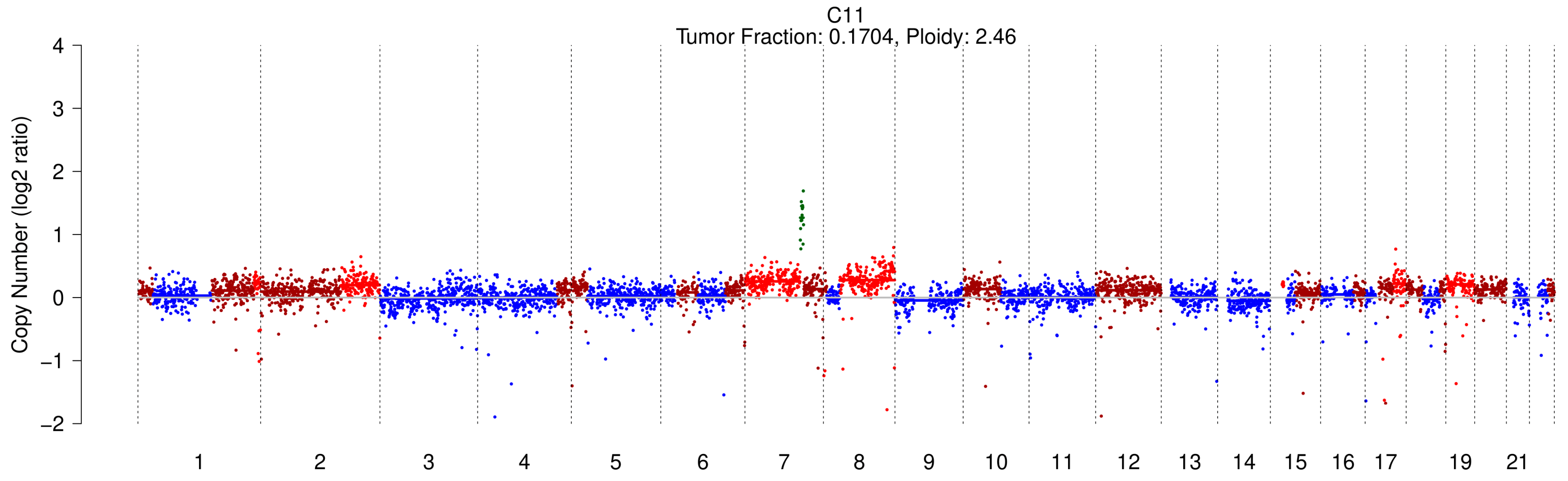
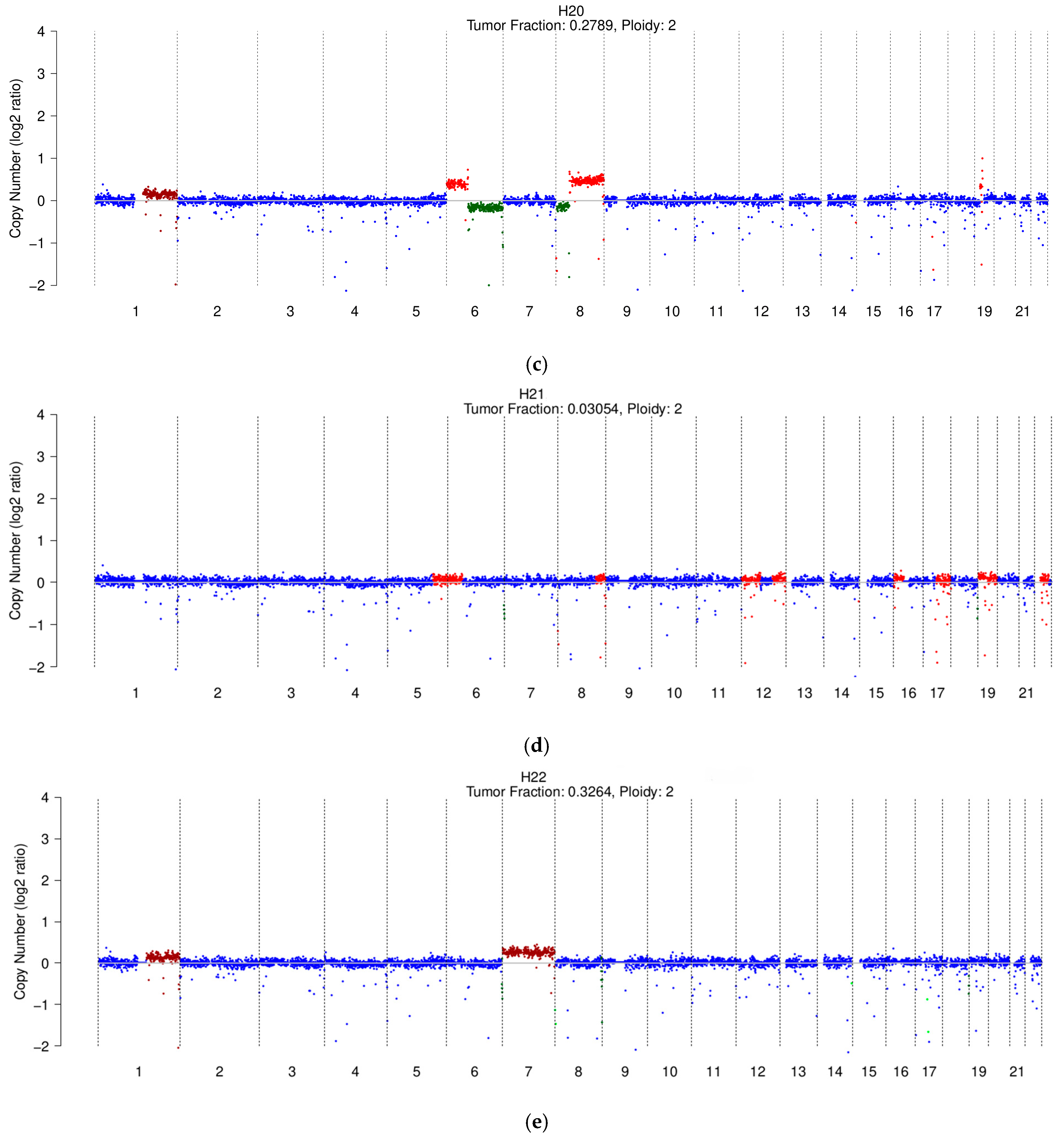
3.3. Copy Number Profiles in Cirrhosis and HCC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| HCC | Hepatocellular carcinoma |
| AFP | Alpha-fetoprotein |
| TF | Tumor fraction |
| ccfDNA | Circulating cell-free DNA |
| sWGS | Shallow whole genome sequencing |
| ctDNA | Circulating tumor DNA |
| SCNAs | Somatic copy number alterations |
| CNVs | Copy number variations |
| HBV | Hepatitis B virus |
| HDV | Hepatitis D virus |
| HCV | Hepatitis C virus |
| LB | Liquid biopsy |
| IQR | Interquartile range |
| CLD | Chronic liver disease |
| CSPH | Clinically significant portal hypertension |
| CR | Complete response |
| PR | Partial response |
| SD | Stable disease |
| PD | Progression disease |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Pelizzaro, F.; Vitale, A.; Sartori, A.; Vieno, A.; Penzo, B.; Russo, F.P.; Frigo, A.C.; Giannini, E.G.; Piccinnu, M.; Rapaccini, G.L.; et al. Surveillance as Determinant of Long-Term Survival in Non-Transplanted Hepatocellular Carcinoma Patients. Cancers 2021, 13, 897. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Zhang, K.H. New Blood Biomarkers for the Diagnosis of AFP-Negative Hepatocellular Carcinoma. Front. Oncol. 2020, 10, 1316. [Google Scholar] [PubMed]
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Galle, P.R.; Foerster, F.; Kudo, M.; Chan, S.L.; Llovet, J.M.; Qin, S.; Schelman, W.R.; Chintharlapalli, S.; Abada, P.B.; Sherman, M.; et al. Biology and Significance of Alpha-Fetoprotein in Hepatocellular Carcinoma. Liver Int. 2019, 39, 2214–2229. [Google Scholar]
- Trevisani, F.; D’Intino, P.E.; Morselli-Labate, A.M.; Mazzella, G.; Accogli, E.; Caraceni, P.; Domenicali, M.; De Notariis, S.; Roda, E.; Bernardi, M. Serum Alpha-Fetoprotein for Diagnosis of Hepatocellular Carcinoma in Patients with Chronic Liver Disease: Influence of HBsAg and Anti-HCV Status. J. Hepatol. 2001, 34, 570–575. [Google Scholar]
- Sun, X.; Mei, J.; Lin, W.; Yang, Z.; Peng, W.; Chen, J.; Zhang, Y.; Xu, L.; Chen, M. Reductions in AFP and PIVKA-II Can Predict the Efficiency of Anti-PD-1 Immunotherapy in HCC Patients. BMC Cancer 2021, 21, 775. [Google Scholar] [CrossRef]
- Zhu, A.X.; Dayyani, F.; Yen, C.J.; Ren, Z.; Bai, Y.; Meng, Z.; Pan, H.; Dillon, P.; Shivani, M.; Gaillard, V.; et al. Alpha-Fetoprotein (AFP) Kinetics as a Potential Surrogate Biomarker in Patients (Pts) with Hepatocellular Carcinoma (HCC) Treated with Atezolizumab (Atezo) + Bevacizumab (Bev). In Proceedings of the ILCA Annual Conference, Vitual, 11–13 September 2020. [Google Scholar]
- Wang, X.; Zhang, Y.; Yang, N.; He, H.; Tao, X.; Kou, C.; Jiang, J. Evaluation of the Combined Application of AFP, AFP-L3%, and DCP for Hepatocellular Carcinoma Diagnosis: A Meta-Analysis. Biomed Res. Int. 2020, 2020, 5087643. [Google Scholar] [CrossRef]
- Chaiteerakij, R.; Addissie, B.D.; Roberts, L.R. Update on Biomarkers of Hepatocellular Carcinoma. Clin. Gastroenterol. Hepatol. 2015, 13, 237–245. [Google Scholar]
- Campani, C.; Zucman-Rossi, J.; Nault, J.C. Genetics of Hepatocellular Carcinoma: From Tumor to Circulating DNA. Cancers 2023, 15, 817. [Google Scholar] [CrossRef]
- Lehrich, B.M.; Zhang, J.; Monga, S.P.; Dhanasekaran, R. Battle of the Biopsies: Role of Tissue and Liquid Biopsy in Hepatocellular Carcinoma. J. Hepatol. 2024, 80, 515–530. [Google Scholar] [PubMed]
- Labgaa, I.; Villanueva, A.; Dormond, O.; Demartines, N.; Melloul, E. The Role of Liquid Biopsy in Hepatocellular Carcinoma Prognostication. Cancers 2021, 13, 659. [Google Scholar] [CrossRef] [PubMed]
- Ye, Q.; Ling, S.; Zheng, S.; Xu, X. Liquid Biopsy in Hepatocellular Carcinoma: Circulating Tumor Cells and Circulating Tumor DNA. Mol. Cancer 2019, 18, 114. [Google Scholar] [PubMed]
- Pelizzaro, F.; Cardin, R.; Penzo, B.; Pinto, E.; Vitale, A.; Cillo, U.; Russo, F.P.; Farinati, F. Liquid Biopsy in Hepatocellular Carcinoma: Where Are We Now? Cancers 2021, 13, 2274. [Google Scholar] [CrossRef]
- Garin, E.; Tselikas, L.; Guiu, B.; Chalaye, J.; Edeline, J.; De Baere, T.; Assenat, E.; Tacher, V.; Robert, C.; Terroir-Cassou-Mounat, M.; et al. Personalised versus Standard Dosimetry Approach of Selective Internal Radiation Therapy in Patients with Locally Advanced Hepatocellular Carcinoma (DOSISPHERE-01): A Randomised, Multicentre, Open-Label Phase 2 Trial. Lancet Gastroenterol. Hepatol. 2021, 6, 17–29. [Google Scholar] [CrossRef]
- Stejskal, P.; Goodarzi, H.; Srovnal, J.; Hajdúch, M.; van’t Veer, L.J.; Magbanua, M.J.M. Circulating Tumor Nucleic Acids: Biology, Release Mechanisms, and Clinical Relevance. Mol. Cancer 2023, 22, 15. [Google Scholar]
- Magbanua, M.J.M.; Brown Swigart, L.; Ahmed, Z.; Sayaman, R.W.; Renner, D.; Kalashnikova, E.; Hirst, G.L.; Yau, C.; Wolf, D.M.; Li, W.; et al. Clinical Significance and Biology of Circulating Tumor DNA in High-Risk Early-Stage HER2-Negative Breast Cancer Receiving Neoadjuvant Chemotherapy. Cancer Cell 2023, 41, 1091–1102.e4. [Google Scholar] [CrossRef]
- Egger, M.E.; Alexander, E.; Van Meter, T.; Kong, M.; Maung, A.A.; Valdes, R.; Hall, M.B.; Linder, M.W. Corresponding CtDNA and Tumor Burden Dynamics in Metastatic Melanoma Patients on Systemic Treatment. Transl. Oncol. 2024, 42, 101883. [Google Scholar] [CrossRef]
- Yi, X.; Ma, J.; Guan, Y.; Chen, R.; Yang, L.; Xia, X. The Feasibility of Using Mutation Detection in CtDNA to Assess Tumor Dynamics. Int. J. Cancer 2017, 140, 2642–2647. [Google Scholar]
- Tao, K.; Bian, Z.; Zhang, Q.; Guo, X.; Yin, C.; Wang, Y.; Zhou, K.; Wan, S.; Shi, M.; Bao, D.; et al. Machine Learning-Based Genome-Wide Interrogation of Somatic Copy Number Aberrations in Circulating Tumor DNA for Early Detection of Hepatocellular Carcinoma. EBioMedicine 2020, 56, 102811. [Google Scholar] [CrossRef]
- Adalsteinsson, V.A.; Ha, G.; Freeman, S.S.; Choudhury, A.D.; Stover, D.G.; Parsons, H.A.; Gydush, G.; Reed, S.C.; Rotem, D.; Rhoades, J.; et al. Scalable Whole-Exome Sequencing of Cell-Free DNA Reveals High Concordance with Metastatic Tumors. Nat. Commun. 2017, 8, 1324. [Google Scholar] [CrossRef] [PubMed]
- Sogbe, M.; Bilbao, I.; Marchese, F.P.; Zazpe, J.; De Vito, A.; Pozuelo, M.; D’avola, D.; Iñarrairaegui, M.; Berasain, C.; Arechederra, M.; et al. Prognostic Value of Ultra-Low-Pass Whole-Genome Sequencing of Circulating Tumor DNA in Hepatocellular Carcinoma under Systemic Treatment. Clin. Mol. Hepatol. 2024, 30, 177–190. [Google Scholar] [CrossRef] [PubMed]
- Bruix, J.; Sherman, M.; Llovet, J.M.; Beaugrand, M.; Lencioni, R.; Burroughs, A.K.; Christensen, E.; Pagliaro, L.; Colombo, M.; Rodés, J.; et al. Clinical Management of Hepatocellular Carcinoma. Conclusions of the Barcelona-2000 EASL Conference. European Association for the Study of the Liver. J. Hepatol. 2001, 35, 421–430. [Google Scholar] [PubMed]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC Strategy for Prognosis Prediction and Treatment Recommendation: The 2022 Update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Ally, A.; Balasundaram, M.; Carlsen, R.; Chuah, E.; Clarke, A.; Dhalla, N.; Holt, R.A.; Jones, S.J.M.; Lee, D.; Ma, Y.; et al. Comprehensive and Integrative Genomic Characterization of Hepatocellular Carcinoma. Cell 2017, 169, 1327–1341.e23. [Google Scholar] [CrossRef]
- Campani, C.; Imbeaud, S.; Ziol, M.; Nahon, P.; Sidali, S.; Demory, A.; Seror, O.; Taly, V.; Laurent-Puig, P.; Ganne-Carrié, N.; et al. Dynamic Evolution of Circulating Tumor DNA in Patients with Hepatocellular Carcinoma across Tumor Stages and Treatments. Dig. Liver Dis. 2023, 55, S213–S214. [Google Scholar] [CrossRef]
- Lian, S.; Lu, C.; Li, F.; Yu, X.; Ai, L.; Wu, B.; Gong, X.; Zhou, W.; Liang, X.; Zhan, J.; et al. Monitoring Hepatocellular Carcinoma Using Tumor Content in Circulating Cell-Free DNA. Clin. Cancer Res. 2024, 30, 2772–2779. [Google Scholar] [CrossRef]
- Lee, T.Y.; Wu, J.C.; Yu, S.H.; Lin, J.T.; Wu, M.S.; Wu, C.Y. The Occurrence of Hepatocellular Carcinoma in Different Risk Stratifications of Clinically Noncirrhotic Nonalcoholic Fatty Liver Disease. Int. J. Cancer 2017, 141, 1307–1314. [Google Scholar] [CrossRef]
- Do, A.L.; Wong, C.R.; Nguyen, L.H.; Nguyen, V.G.; Trinh, H.; Nguyen, M.H. Hepatocellular Carcinoma Incidence in Noncirrhotic Patients with Chronic Hepatitis B and Patients with Cirrhosis of All Etiologies. J. Clin. Gastroenterol. 2014, 48, 644–649. [Google Scholar] [CrossRef]
- Fateen, W.; Johnson, P.J.; Wood, H.M.; Zhang, H.; He, S.; El-Meteini, M.; Wyatt, J.I.; Aithal, G.P.; Quirke, P. Characterisation of Dysplastic Liver Nodules Using Low-Pass DNA Sequencing and Detection of Chromosome Arm-Level Abnormalities in Blood-Derived Cell-Free DNA. J. Pathol. 2021, 255, 30–40. [Google Scholar] [CrossRef]
- Tokuhisa, Y.; Iizuka, N.; Sakaida, I.; Moribe, T.; Fujita, N.; Miura, T.; Tamatsukuri, S.; Ishitsuka, H.; Uchida, K.; Terai, S.; et al. Circulating Cell-Free DNA as a Predictive Marker for Distant Metastasis of Hepatitis C Virus-Related Hepatocellular Carcinoma. Br. J. Cancer 2007, 97, 1399–1403. [Google Scholar] [CrossRef] [PubMed]
- Iizuka, N.; Sakaida, I.; Moribe, T.; Fujita, N.; Miura, T.; Stark, M.; Tamatsukuri, S.; Ishitsuka, H.; Uchida, K.; Terai, S.; et al. Elevated Levels of Circulating Cell-Free DNA in the Blood of Patients with Hepatitis C Virus-Associated Hepatocellular Carcinoma. Anticancer Res. 2006, 26, 4713–4719. [Google Scholar] [PubMed]
- Yan, L.; Chen, Y.; Zhou, J.; Zhao, H.; Zhang, H.; Wang, G. Diagnostic Value of Circulating Cell-Free DNA Levels for Hepatocellular Carcinoma. Int. J. Infect. Dis. 2018, 67, 92–97. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Chen, L.; Zhang, Z.; Zhang, X.; Lu, X.; Liu, W.; Shi, G.; Ge, Y.; Gao, P.; Yang, Y.; et al. Genome-Wide Mapping of 5-Hydroxymethylcytosines in Circulating Cell-Free DNA as a Non-Invasive Approach for Early Detection of Hepatocellular Carcinoma. Gut 2019, 68, 2195–2205. [Google Scholar] [CrossRef]
- Lin, N.; Lin, Y.; Xu, J.; Liu, D.; Li, D.; Meng, H.; Gallant, M.A.; Kubota, N.; Roy, D.; Li, J.S.; et al. A Multi-Analyte Cell-Free DNA–Based Blood Test for Early Detection of Hepatocellular Carcinoma. Hepatol. Commun. 2022, 6, 1753–1763. [Google Scholar] [CrossRef]
- Ersoy, O. Very High Alpha-Fetoprotein in a Young Man Due to Concomitant Presentation of Hepatocellular Carcinoma and Sertoli Cell Testis Tumor. World J. Gastroenterol. 2005, 11, 7051–7053. [Google Scholar] [CrossRef]
- Ren, N.; Qin, L.X.; Tu, H.; Liu, Y.K.; Zhang, B.H.; Tang, Z.Y. The Prognostic Value of Circulating Plasma DNA Level and Its Allelic Imbalance on Chromosome 8p in Patients with Hepatocellular Carcinoma. J. Cancer Res. Clin. Oncol. 2006, 132, 399–407. [Google Scholar] [CrossRef]
- Yang, Y.J.; Chen, H.; Huang, P.; Li, C.H.; Dong, Z.H.; Hou, Y.L. Quantification of Plasma HTERT DNA in Hepatocellular Carcinoma Patients by Quantitative Fluorescent Polymerase Chain Reaction. Clin. Investig. Med. 2011, 34, E238–E244. [Google Scholar] [CrossRef]
- Huang, Z.; Hua, D.; Hu, Y.; Cheng, Z.; Zhou, X.; Xie, Q.; Wang, Q.; Wang, F.; Du, X.; Zeng, Y. Quantitation of Plasma Circulating DNA Using Quantitative PCR for the Detection of Hepatocellular Carcinoma. Pathol. Oncol. Res. 2012, 18, 271–276. [Google Scholar] [CrossRef]
- Chen, H.; Sun, L.Y.; Zheng, H.Q.; Zhang, Q.F.; Jin, X.M. Total Serum DNA and DNA Integrity: Diagnostic Value in Patients with Hepatitis B Virus-Related Hepatocellular Carcinoma. Pathology 2012, 44, 318–324. [Google Scholar] [CrossRef]
- Piciocchi, M.; Cardin, R.; Vitale, A.; Vanin, V.; Giacomin, A.; Pozzan, C.; Maddalo, G.; Cillo, U.; Guido, M.; Farinati, F. Circulating Free DNA in the Progression of Liver Damage to Hepatocellular Carcinoma. Hepatol. Int. 2013, 7, 1050–1057. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhou, K.; Wang, X.; Liu, Y.; Guo, D.; Bian, Z.; Su, L.; Liu, K.; Gu, X.; Guo, X.; et al. Multiple-Level Copy Number Variations in Cell-Free DNA for Prognostic Prediction of HCC with Radical Treatments. Cancer Sci. 2021, 112, 4772–4784. [Google Scholar] [CrossRef] [PubMed]
- Cai, Z.; Chen, G.; Zeng, Y.; Dong, X.; Li, Z.; Huang, Y.; Xin, F.; Qiu, L.; Xu, H.; Zhang, W.; et al. Comprehensive Liquid Profiling of Circulating Tumor DNA and Protein Biomarkers in Long-Term Follow-up Patients with Hepatocellular Carcinoma. Clin. Cancer Res. 2019, 25, 5284–5294. [Google Scholar] [CrossRef] [PubMed]
- Matsumae, T.; Kodama, T.; Myojin, Y.; Maesaka, K.; Sakamori, R.; Takuwa, A.; Oku, K.; Motooka, D.; Sawai, Y.; Oshita, M.; et al. Circulating Cell-Free DNA Profiling Predicts the Therapeutic Outcome in Advanced Hepatocellular Carcinoma Patients Treated with Combination Immunotherapy. Cancers 2022, 14, 3367. [Google Scholar] [CrossRef]
- Hirai, M.; Kinugasa, H.; Nouso, K.; Yamamoto, S.; Terasawa, H.; Onishi, Y.; Oyama, A.; Adachi, T.; Wada, N.; Sakata, M.; et al. Prediction of the Prognosis of Advanced Hepatocellular Carcinoma by TERT Promoter Mutations in Circulating Tumor DNA. J. Gastroenterol. Hepatol. 2021, 36, 1118–1125. [Google Scholar] [CrossRef]
- Fujii, Y.; Ono, A.; Hayes, C.N.; Aikata, H.; Yamauchi, M.; Uchikawa, S.; Kodama, K.; Teraoka, Y.; Fujino, H.; Nakahara, T.; et al. Identification and Monitoring of Mutations in Circulating Cell-Free Tumor DNA in Hepatocellular Carcinoma Treated with Lenvatinib. J. Exp. Clin. Cancer Res. 2021, 40, 215. [Google Scholar] [CrossRef]
- Nakatsuka, T.; Nakagawa, H.; Hayata, Y.; Wake, T.; Yamada, T.; Nishibatake Kinoshita, M.; Nakagomi, R.; Sato, M.; Minami, T.; Uchino, K.; et al. Post-Treatment Cell-Free DNA as a Predictive Biomarker in Molecular-Targeted Therapy of Hepatocellular Carcinoma. J. Gastroenterol. 2021, 56, 456–469. [Google Scholar] [CrossRef]
- Ikeda, S.; Lim, J.S.; Kurzrock, R. Analysis of Tissue and Circulating Tumor DNA by Next-Generation Sequencing of Hepatocellular Carcinoma: Implications for Targeted Therapeutics. Mol. Cancer Ther. 2018, 17, 1114–1122. [Google Scholar] [CrossRef]
- Xia, Y.; Tang, W.; Qian, X.; Li, X.; Cheng, F.; Wang, K.; Zhang, F.; Zhang, C.; Li, D.; Song, J.; et al. Efficacy and Safety of Camrelizumab plus Apatinib during the Perioperative Period in Resectable Hepatocellular Carcinoma: A Single-Arm, Open Label, Phase II Clinical Trial. J. Immunother. Cancer 2022, 10, e004656. [Google Scholar] [CrossRef]
- Hsu, C.-H.; Lu, S.; Abbas, A.; Guan, Y.; Zhu, A.X.; Aleshin, A.; Lee, K.-H.; Lee, M.S.; Mahipal, A.; Ryoo, B.-Y.; et al. Longitudinal and Personalized Detection of Circulating Tumor DNA (CtDNA) for Monitoring Efficacy of Atezolizumab plus Bevacizumab in Patients with Unresectable Hepatocellular Carcinoma (HCC). J. Clin. Oncol. 2020, 38, 3531. [Google Scholar] [CrossRef]
- Zhao, K.; Zhao, Y.; Zhu, J.Y.; Dong, H.; Cong, W.M.; Yu, Y.; Wang, H.; Zhu, Z.Z.; Xu, Q. A Panel of Genes Identified as Targets for 8q24.13-24.3 Gain Contributing to Unfavorable Overall Survival in Patients with Hepatocellular Carcinoma. Curr. Med. Sci. 2018, 38, 590–596. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Cheng, Y.; Zhang, C.; Fu, S.; He, G.; Cai, L.; Qiu, L.; Huang, K.; Chen, Q.; Xie, W.; et al. Co-Amplification of Genes in Chromosome 8q24: A Robust Prognostic Marker in Hepatocellular Carcinoma. J. Gastrointest. Oncol. 2021, 12, 1086–1100. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Chronic Hepatitis (n = 13) | Cirrhosis (n = 24) | HCC (n = 23) | |
|---|---|---|---|
| Sex-n (%) | |||
| Male | 7 (53.8%) | 14 (58.3%) | 17 (73.9%) |
| Female | 6 (46.2%) | 10 (41.7%) | 6 (26.1%) |
| Age at the time of the sample—median (IQR) | 54.0 (26–70) | 60.7 (44–86) | 66.7 (45–84) |
| Etiology-n (%) | |||
| Viral | 13 (100%) | 10 (41.7%) | 13 (56.5%) |
| Alcohol | - | 5 (20.8%) | 5 (21.7%) |
| Viral + Alcohol | - | 2 (8.3%) | 3 (13.0%) |
| MetALD | - | 3 (12.5%) | 2 (8.7%) |
| MASLD | - | 3 (12.5%) | - |
| Other | - | 1 (4.2%) | - |
| MELD—median (IQR) | - | 12 (7–20) | 10 (7–24) |
| CHILD-n (%) | - | ||
| A | 18 (75.0%) | 19 (82.6%) | |
| B | 4 (16.7%) | 3 (13.0%) | |
| C | 2 (8.3%) | 1 (4.4%) | |
| CSPH-n (%) | - | ||
| Yes | 16 (66.7%) | 17 (73.9%) | |
| No | 8 (33.3%) | 6 (26.1%) | |
| AFP (ng/mL)—median (IQR) | 2.1 (0.7–4.6) | 6.3 (2.0–38.1) | 6.2 (3.0–152.8) |
| HCC during FU-n (%) | 0 | 4 (16.7%) | - |
| HCC at the time of the sample-n (%) | - | - | |
| Active | 19 (82.6%) | ||
| No active | 4 (17.4%) | ||
| N° of nodules—median (IQR) | - | - | 2.9 (0–15.0) |
| Size of nodules (mm)—median (IQR) | - | - | 31.8 (12.0–110.0) |
| Metastasis-n (%) | - | - | 1 (4.3%) |
| BCLC-n (%) | |||
| 0 | 2 (8.7%) | ||
| A | 10 (43.8%) | ||
| B | 4 (17.4%) | ||
| C | 3 (13.0%) | ||
| D | - | ||
| Previously treated for HCC-n (%) | - | - | |
| Yes | 14 (60.9%) | ||
| No | 9 (39.1%) | ||
| mRECIST *-n (%) | - | - | CR 4 (28.6%) PR 4 (28.6%) SD 2 (14.2%) PD 4 (28.6%) |
| Deaths-n (%) | 0 | 4 (16.7%) | 3 (13.0%) |
| Median FU (months)—median (IQR) | 388.7 (4.0–1428.0) | 71.7 (2.0–1493.0) | 35.1 (1.0–116.0) |
| Altered profile-n (%) | 0 | 1 (5.0%) | 5 (21.7%) |
| Patient | AFP (ng/mL) | N° of Nodules | Size of Nodules (mm) | Metastasis | BCLC | Dead | OS (Months) | TF (%) | PD |
|---|---|---|---|---|---|---|---|---|---|
| H18 | 22,700.0 | 5 | 21.0 | Yes | C | No | 26.0 | 31.0% | Yes |
| H19 | 3.0 | 3 | 20.0 | No | A | No | 25.0 | 14.6% | Yes |
| H20 | 470.0 | 15 | 15.0 | No | C | Yes | 9.0 | 27.9% | Yes |
| H21 | 4.6 | 5 | 17.0 | No | B | Yes | 17.0 | 3.1% | Yes |
| H22 | 8.6 | 6 | 55.0 | No | C | Yes | 1.0 | 32.6% | Yes |
| Variable | Overall (n = 23) | Undetectable ctDNA (n = 18) | Detectable ctDNA (n = 5) | p |
|---|---|---|---|---|
| Sex-n (%) | 0.133 | |||
| Males | 17 (73.9) | 12 (66.7) | 5 (100) | |
| Females | 6 (26.1) | 6 (43.3) | 0 (0) | |
| Age at the time of the sample—median (IQR) | 65 (60–72) | 67 (59–76) | 61 (52–69) | 0.257 |
| Etiology-n (%) | 0.461 | |||
| Alcohol | 5 (21.7) | 5 (27.8) | 0 (0) | |
| MetALD | 2 (8.7) | 1 (5.6) | 1 (20.0) | |
| Viral | 13 (56.5) | 10 (55.6) | 3 (60.0) | |
| Viral + Alcohol | 3 (13.0) | 2 (11.1) | 1 (20.0) | |
| AFP (ng/mL)—median (IQR) | 6.2 (3.0–152.8) | 5.6 (2.8–74.9) | 8.6 (3.8–11585) | 0.359 |
| MELD—median (IQR) | 9 (8–12) | 9 (8–12) | 10 (8–17) | 0.403 |
| CHILD-n (%) | 0.109 | |||
| A | 19 (82.6) | 15 (83.3) | 4 (80.0) | |
| B | 3 (13.0) | 3 (16.7) | 0 (0) | |
| C | 1 (4.3) | 0 (0) | 1 (20.0) | |
| CHILD—median (IQR) | 6 (5–7) | 6 (5–7) | 6 (5–9) | 0.257 |
| Number of nodules—median (IQR) | 2 (1–5) | 1 (1–4) | 4.7 (1–11) | 0.005 |
| Max size—median (IQR) | 22.0 (16.5–43) | 24.0 (17.0–46.0) | 20.0 (16.0–38.0) | 0.500 |
| CSPH †-n (%) | 0.423 | |||
| Yes | 17 (73.9) | 14 (77.8) | 3 (60.0) | |
| No | 6 (26.1) | 4 (22.2) | 2 (40.0) | |
| Metastasis-n (%) | 0.138 | |||
| Yes | 1 (4.3) | 0 (0) | 1 (20.0) | |
| No | 22 (94.7) | 18 (100) | 4 (80.0) | |
| BCLC-n (%) | 0.010 | |||
| 0 | 2 (8.7) | 2 (11.1) | 0 (0) | |
| A | 10 (43.5) | 9 (50.0) | 1 (20.0) | |
| B | 4 (17.4) | 3 (16.7) | 1 (20.0) | |
| C | 3 (13.0) | 0 (0) | 3 (60.0) | |
| mRECIST-n (%) | 0.001 | |||
| CR | 4 (17.4) | 4 (22.2) | 0 (0) | |
| PR | 4 (17.4) | 4 (22.2) | 0 (0) | |
| SD | 2 (8.7) | 2 (11.1) | 0 (0) | |
| PD | 4 (17.4) | 0 (0) | 4 (80.0) | |
| Progression-n (%) | <0.0001 | |||
| Yes | 4 (17.4) | 0 (0) | 4 (80.0) | |
| No | 10 (60.9) | 10 (55.6) | 0 (0) | |
| Status ‡-n (%) | 0.246 | |||
| Active | 4 (17.4) | 14 (77.8) | 5 (100) | |
| No active | 10 (43.5) | 4 (22.2) | 0 (0) | |
| Previously treated-n (%) | 0.322 | |||
| Yes | 14 (60.9) | 10 (55.6) | 4 (80.0) | |
| No | 9 (39.1) | 8 (44.4) | 1 (20.0) | |
| Death-n (%) | <0.0001 | |||
| Yes | 3 (13.0) | 0 (0) | 3 (60.0) | |
| No | 20 (87.0) | 18 (100) | 2 (40.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pinto, E.; Lazzarini, E.; Pelizzaro, F.; Gambato, M.; Santarelli, L.; Potente, S.; Zanaga, P.; Zappitelli, T.; Cardin, R.; Burra, P.; et al. Somatic Copy Number Alterations in Circulating Cell-Free DNA as a Prognostic Biomarker for Hepatocellular Carcinoma: Insights from a Proof-of-Concept Study. Cancers 2025, 17, 1115. https://doi.org/10.3390/cancers17071115
Pinto E, Lazzarini E, Pelizzaro F, Gambato M, Santarelli L, Potente S, Zanaga P, Zappitelli T, Cardin R, Burra P, et al. Somatic Copy Number Alterations in Circulating Cell-Free DNA as a Prognostic Biomarker for Hepatocellular Carcinoma: Insights from a Proof-of-Concept Study. Cancers. 2025; 17(7):1115. https://doi.org/10.3390/cancers17071115
Chicago/Turabian StylePinto, Elisa, Elisabetta Lazzarini, Filippo Pelizzaro, Martina Gambato, Laura Santarelli, Sara Potente, Paola Zanaga, Teresa Zappitelli, Romilda Cardin, Patrizia Burra, and et al. 2025. "Somatic Copy Number Alterations in Circulating Cell-Free DNA as a Prognostic Biomarker for Hepatocellular Carcinoma: Insights from a Proof-of-Concept Study" Cancers 17, no. 7: 1115. https://doi.org/10.3390/cancers17071115
APA StylePinto, E., Lazzarini, E., Pelizzaro, F., Gambato, M., Santarelli, L., Potente, S., Zanaga, P., Zappitelli, T., Cardin, R., Burra, P., Farinati, F., Romualdi, C., Boscarino, D., Tosello, V., Indraccolo, S., & Russo, F. P. (2025). Somatic Copy Number Alterations in Circulating Cell-Free DNA as a Prognostic Biomarker for Hepatocellular Carcinoma: Insights from a Proof-of-Concept Study. Cancers, 17(7), 1115. https://doi.org/10.3390/cancers17071115