
13N-Ammonia PET-CT for Evaluating Response to Antiangiogenic Therapy and Prognosis in Patients with Advanced Hepatocellular Carcinoma: A Pilot Study

 , , , , , , and
, , , , , , and
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
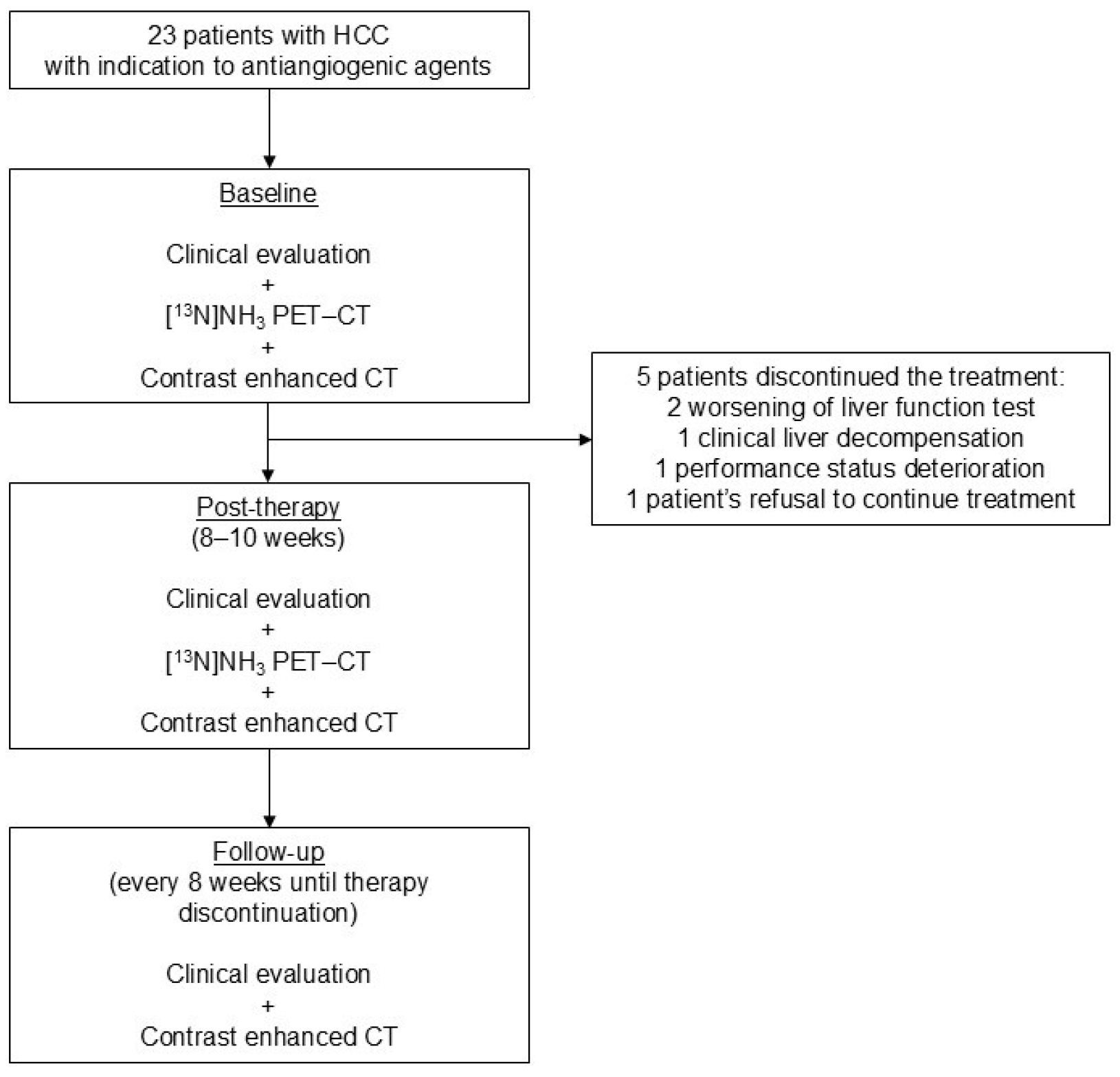
2.1. Patients
2.2. 13N-Ammonia PET-CT
2.3. Antiangiogenic Therapy
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
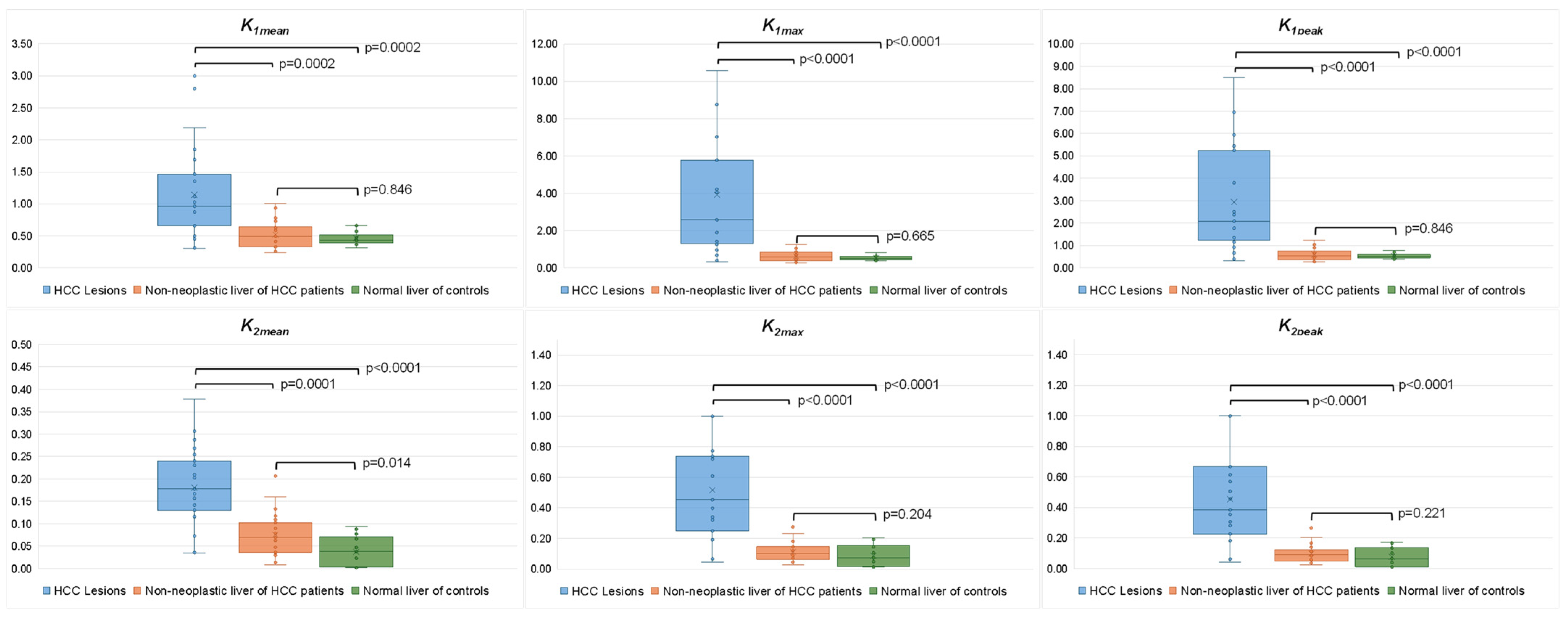
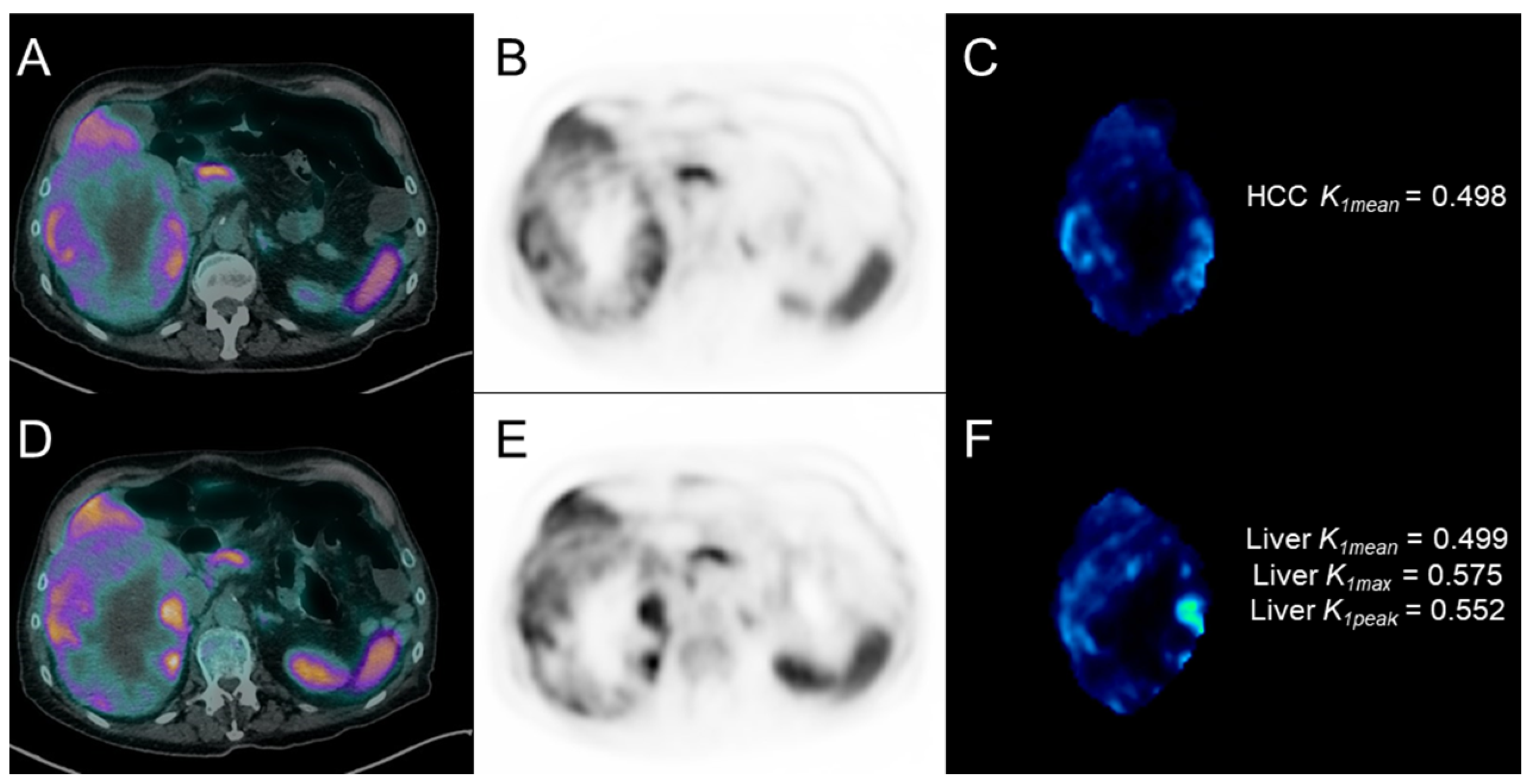
3.2. Kinetic PET Parameters in HCC Lesions and Non-Neoplastic Liver Parenchyma
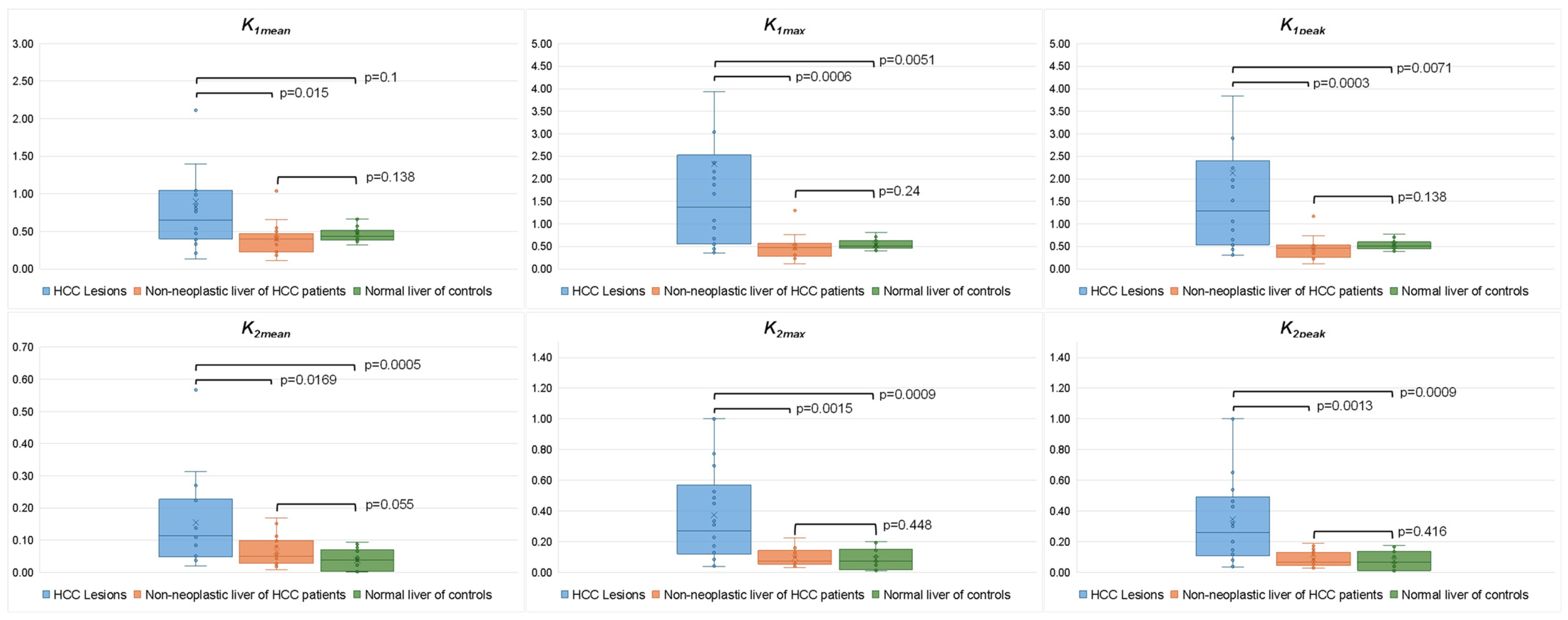
3.3. Kinetic PET Parameters and Clinical Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236, Erratum in: J. Hepatol. 2019, 70, 817. [Google Scholar]
- Golfieri, R.; Bargellini, I.; Spreafico, C.; Trevisani, F. Patients with Barcelona Clinic Liver Cancer Stages B and C Hepatocellular Carcinoma: Time for a Subclassification. Liver Cancer 2019, 8, 78–91. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Cabibbo, G.; Giannini, E.; Piscaglia, F.; Trevisani, F.; Daniele, B.; Belli, G.; Viganò, L.; Cappabianca, S.; Romanini, L.; Volterrani, L.; et al. Raccomandazioni Multisocietarie Italiane (AISF, AIOM, IT-IHPBA, SIC, SIRM, SITO) per la Gestione Clinica Integrata del Paziente con Epatocarcinoma (HCC). Available online: https://sirm.org/wp-content/uploads/2021/04/304-Documento-intersocietario-AISF-AIOM-IT-IHPBA-SIC-SIRM-SITO-2016-HCC-raccomandazioni-multisocietarie.pdf (accessed on 23 December 2024).
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Kudo, M.; Montal, R.; Finn, R.S.; Castet, F.; Ueshima, K.; Nishida, N.; Haber, P.K.; Hu, Y.; Chiba, Y.; Schwartz, M.; et al. Objective Response Predicts Survival in Advanced Hepatocellular Carcinoma Treated with Systemic Therapies. Clin. Cancer Res. 2022, 28, 3443–3451. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef]
- Molecular Imaging and Contrast Agent Database (MICAD). Bethesda (MD): National Center for Biotechnology Information (US); 2004–2013. Available online: https://www.ncbi.nlm.nih.gov/books/NBK5330/ (accessed on 23 December 2024).
- Fathala, A.; Aboulkheir, M.; Shoukri, M.M.; Alsergani, H. Diagnostic accuracy of 13N-ammonia myocardial perfusion imaging with PET-CT in the detection of coronary artery disease. Cardiovasc. Diagn. Ther. 2019, 9, 35–42. [Google Scholar] [CrossRef]
- Khangembam, B.C.; Karunanithi, S.; Sharma, P.; Kc, S.S.; Kumar, R.; Julka, P.K.; Kumar, R.; Bal, C. Perfusion-metabolism coupling in recurrent gliomas: A prospective validation study with 13N-ammonia and 18F-fluorodeoxyglucose PET/CT. Neuroradiology 2014, 56, 893–902. [Google Scholar] [CrossRef]
- Albano, D.; Giubbini, R.; Bertagna, F. 13N-NH3 PET/CT in oncological disease. Jpn. J. Radiol. 2019, 37, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Schelstraete, K.; Simons, M.; Deman, J.; Vermeulen, F.L.; Slegers, G.; Vandecasteele, C.; Goethals, P.; De Schryver, A. Uptake of 13N-ammonia by human tumours as studied by positron emission tomography. Br. J. Radiol. 1982, 55, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Scolozzi, V.; Giancipoli, R.G.; Inzani, F.; Ponziani, F.R.; Taralli, S. Splenic and lung metastases of hepatocellular carcinoma detected at 13N-ammonia PET/CT. Rev. Esp. Med. Nucl. Imagen Mol. 2023, 42, 416–417. [Google Scholar] [CrossRef]
- Wennerberg, A.E.; Nalesnik, M.A.; Coleman, W.B. Hepatocyte paraffin 1: A monoclonal antibody that reacts with hepatocytes and can be used for differential diagnosis of hepatic tumors. Am. J. Pathol. 1993, 143, 1050–1054. [Google Scholar]
- Di Tommaso, L.; Franchi, G.; Park, Y.N.; Fiamengo, B.; Destro, A.; Morenghi, E.; Montorsi, M.; Torzilli, G.; Tommasini, M.; Terracciano, L.; et al. Diagnostic value of HSP70, glypican 3, and glutamine synthetase in hepatocellular nodules in cirrhosis. Hepatology 2007, 45, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Shibata, T.; Yamamoto, K.; Hayashi, N.; Yonekura, Y.; Nagara, T.; Saji, H.; Mukai, T.; Konishi, J. Dynamic positron emission tomography with 13N-ammonia in liver tumors. Eur. J. Nucl. Med. 1988, 14, 607–611. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, N.; Tamaki, N.; Yonekura, Y.; Senda, M.; Saji, H.; Yamamoto, K.; Konishi, J.; Torizuka, K. Imaging of the hepatocellular carcinoma using dynamic positron emission tomography with nitrogen-13 ammonia. J. Nucl. Med. 1985, 26, 254–257. [Google Scholar] [PubMed]
- Alpert, N.M.; Eriksson, L.; Chang, J.Y.; Bergstrom, M.; Litton, J.E.; Correia, J.A.; Bohm, C.; Ackerman, R.H.; Taveras, J.M. Strategy for the measurement of regional cerebral blood flow using short-lived tracers and emission tomography. J. Cereb. Blood Flow. Metab. 1984, 4, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Meyer, E. Simultaneous correction for tracer arrival delay and dispersion in CBF measurements by the H215O autoradiographic method and dynamic PET. J. Nucl. Med. 1989, 30, 1069–1078. [Google Scholar]
- Bujang, M.A.; Adnan, T.H. Requirements for Minimum Sample Size for Sensitivity and Specificity Analysis. J. Clin. Diagn. Res. 2016, 10, YE01–YE06. [Google Scholar] [CrossRef] [PubMed]
- Berndt, N.; Eckstein, J.; Heucke, N.; Wuensch, T.; Gajowski, R.; Stockmann, M.; Meierhofer, D.; Holzhütter, H.G. Metabolic heterogeneity of human hepatocellular carcinoma: Implications for personalized pharmacological treatment. FEBS J. 2021, 288, 2332–2346. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.; Shen, J.; Yan, J.; Bott, A.J.; Maimouni, S.; Daguplo, H.Q.; Wang, Y.; Khayati, K.; Guo, J.Y.; Zhang, L.; et al. Glutamine synthetase limits β-catenin-mutated liver cancer growth by maintaining nitrogen homeostasis and suppressing mTORC1. J. Clin. Investig. 2022, 132, e161408. [Google Scholar] [CrossRef] [PubMed]
- Ippolito, D.; Querques, G.; Okolicsanyi, S.; Talei Franzesi, C.; Pecorelli, A.; Lombardi, S.; Orsini, E.; Strazzabosco, M.; Sironi, S. Dynamic contrast enhanced perfusion CT imaging: A diagnostic biomarker tool for survival prediction of tumour response to antiangiogenetic treatment in patients with advanced HCC lesions. Eur. J. Radiol. 2018, 106, 62–68. [Google Scholar] [CrossRef]
- Zocco, M.A.; Garcovich, M.; Lupascu, A.; Di Stasio, E.; Roccarina, D.; Annicchiarico, B.E.; Riccardi, L.; Ainora, M.E.; Ponziani, F.; Caracciolo, G.; et al. Early prediction of response to sorafenib in patients with advanced hepatocellular carcinoma: The role of dynamic contrast enhanced ultrasound. J. Hepatol. 2013, 59, 1014–1021. [Google Scholar] [CrossRef] [PubMed]
- Faivre, S.; Rimassa, L.; Finn, R.S. Molecular therapies for HCC: Looking outside the box. J. Hepatol. 2020, 72, 342–352. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Zhu, A.X. Targeting angiogenesis in hepatocellular carcinoma: Focus on VEGF and bevacizumab. Expert. Rev. Anticancer. Ther. 2009, 9, 503–509. [Google Scholar] [CrossRef] [PubMed]
- de Langen, A.J.; van den Boogaart, V.; Lubberink, M.; Backes, W.H.; Marcus, J.T.; van Tinteren, H.; Pruim, J.; Brans, B.; Leffers, P.; Dingemans, A.M.; et al. Monitoring response to antiangiogenic therapy in non-small cell lung cancer using imaging markers derived from PET and dynamic contrast-enhanced MRI. J. Nucl. Med. 2011, 52, 48–55. [Google Scholar] [CrossRef] [PubMed]
- Corpechot, C.; Barbu, V.; Wendum, D.; Kinnman, N.; Rey, C.; Poupon, R.; Housset, C.; Rosmorduc, O. Hypoxia-induced VEGF and collagen I expressions are associated with angiogenesis and fibrogenesis in experimental cirrhosis. Hepatology 2002, 35, 1010–1021. [Google Scholar] [CrossRef] [PubMed]
- Iwakiri, Y.; Shah, V.; Rockey, D.C. Vascular pathobiology in chronic liver disease and cirrhosis—Current status and future directions. J. Hepatol. 2014, 61, 912–924. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics (n = 23) | Value (%) |
|---|---|
| Age (years) | 68.2 ± 15.3 |
| Male gender | 21 (91.3%) |
| Cirrhosis | 23 (100%) |
| Etiology | |
| HCV | 6 (26.1%) |
| HBV | 5 (21.7%) |
| Alcohol | 5 (21.7%) |
| NAFLD | 5 (21.7%) |
| HCV + alcohol | 1 (4.3%) |
| Cryptogenic | 1 (4.3%) |
| Extrahepatic spread at baseline CT | 13 (56.5%) |
| Portal vein tumor thrombosis at baseline CT | 5 (21.7%) |
| Child-Pugh score | |
| A | 18 (78.2%) |
| B | 2 (8.7%) |
| N/A | 3 (13.1%) |
| BCLC | |
| B | 6 (26.1%) |
| C | 17 (73.9%) |
| ECOG performance status | |
| 0 | 12 (52.2%) |
| 1 | 9 (39.1%) |
| 2 | 2 (8.7%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scolozzi, V.; Nicoletti, A.; Capotosti, A.; Ponziani, F.R.; Taralli, S.; Genco, E.; Leccisotti, L.; Moretti, R.; Indovina, L.; Pompili, M.; et al. 13N-Ammonia PET-CT for Evaluating Response to Antiangiogenic Therapy and Prognosis in Patients with Advanced Hepatocellular Carcinoma: A Pilot Study. Cancers 2025, 17, 656. https://doi.org/10.3390/cancers17040656
Scolozzi V, Nicoletti A, Capotosti A, Ponziani FR, Taralli S, Genco E, Leccisotti L, Moretti R, Indovina L, Pompili M, et al. 13N-Ammonia PET-CT for Evaluating Response to Antiangiogenic Therapy and Prognosis in Patients with Advanced Hepatocellular Carcinoma: A Pilot Study. Cancers. 2025; 17(4):656. https://doi.org/10.3390/cancers17040656
Chicago/Turabian StyleScolozzi, Valentina, Alberto Nicoletti, Amedeo Capotosti, Francesca Romana Ponziani, Silvia Taralli, Enza Genco, Lucia Leccisotti, Roberto Moretti, Luca Indovina, Maurizio Pompili, and et al. 2025. "13N-Ammonia PET-CT for Evaluating Response to Antiangiogenic Therapy and Prognosis in Patients with Advanced Hepatocellular Carcinoma: A Pilot Study" Cancers 17, no. 4: 656. https://doi.org/10.3390/cancers17040656
APA StyleScolozzi, V., Nicoletti, A., Capotosti, A., Ponziani, F. R., Taralli, S., Genco, E., Leccisotti, L., Moretti, R., Indovina, L., Pompili, M., & Calcagni, M. L. (2025). 13N-Ammonia PET-CT for Evaluating Response to Antiangiogenic Therapy and Prognosis in Patients with Advanced Hepatocellular Carcinoma: A Pilot Study. Cancers, 17(4), 656. https://doi.org/10.3390/cancers17040656