
Diagnosis and Evaluation of Aggressiveness Using Circulating Plasma miRNAs in Papillary Thyroid Microcarcinoma

 , , , , and
, , , , and
Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Ethics Approval
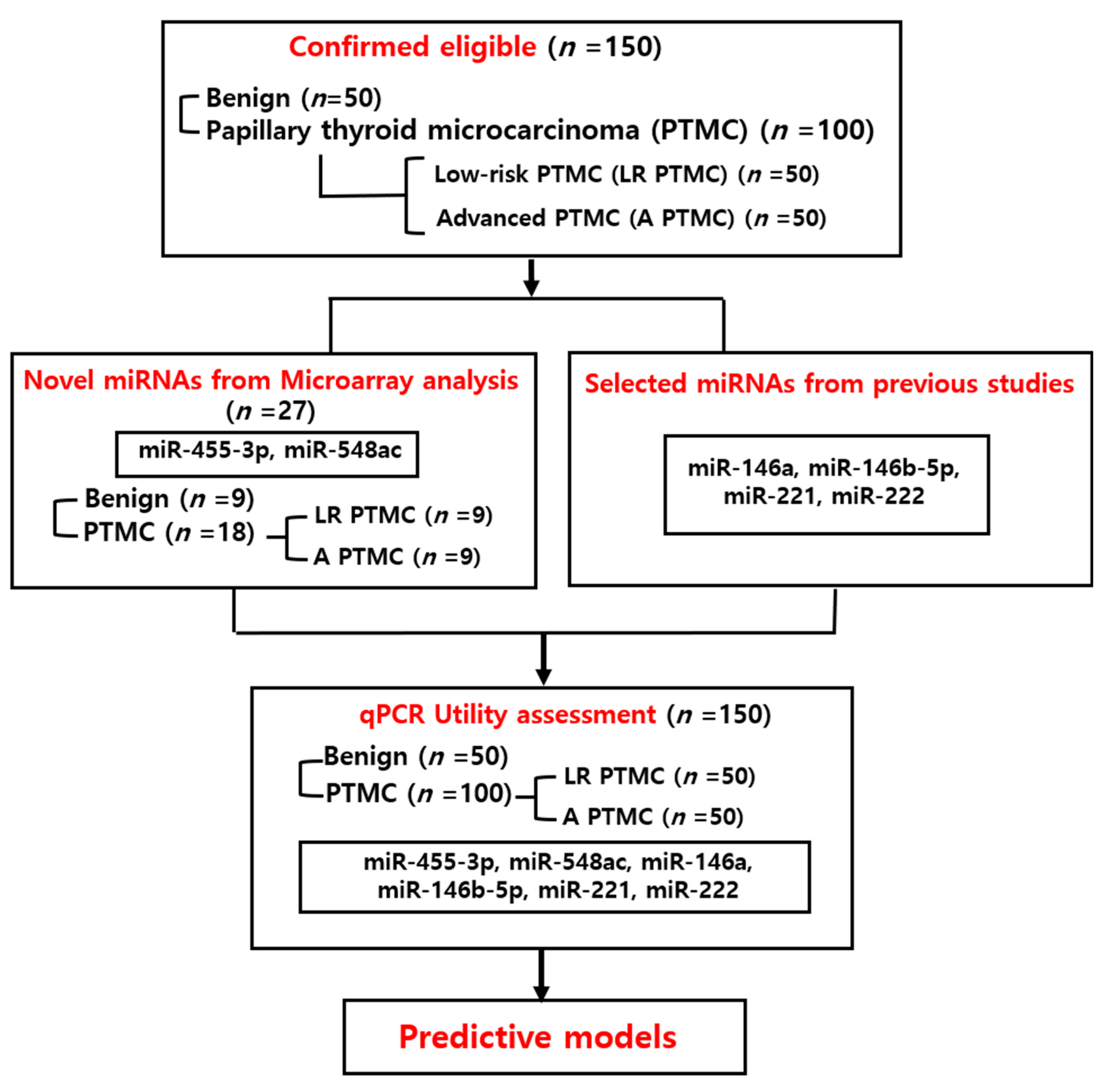
2.2. Subjects
2.3. Selection of miRNAs
2.4. Microarray
2.5. RNA Isolation
2.6. Reverse Transcriptase Reactions
2.7. Quantitative Real-Time PCR
2.8. Statistics Analysis
3. Results
3.1. Comparison of Benign and PTMC
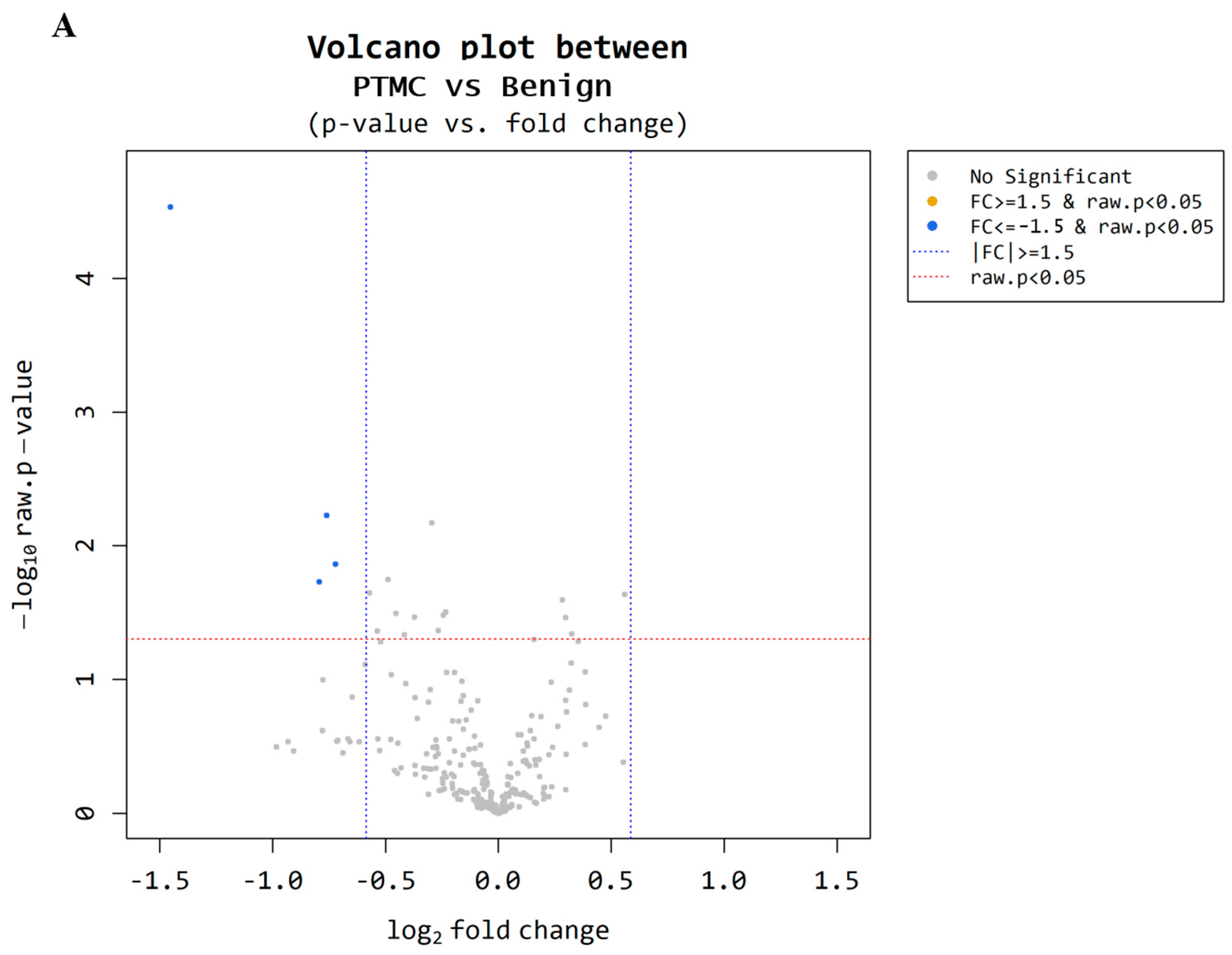
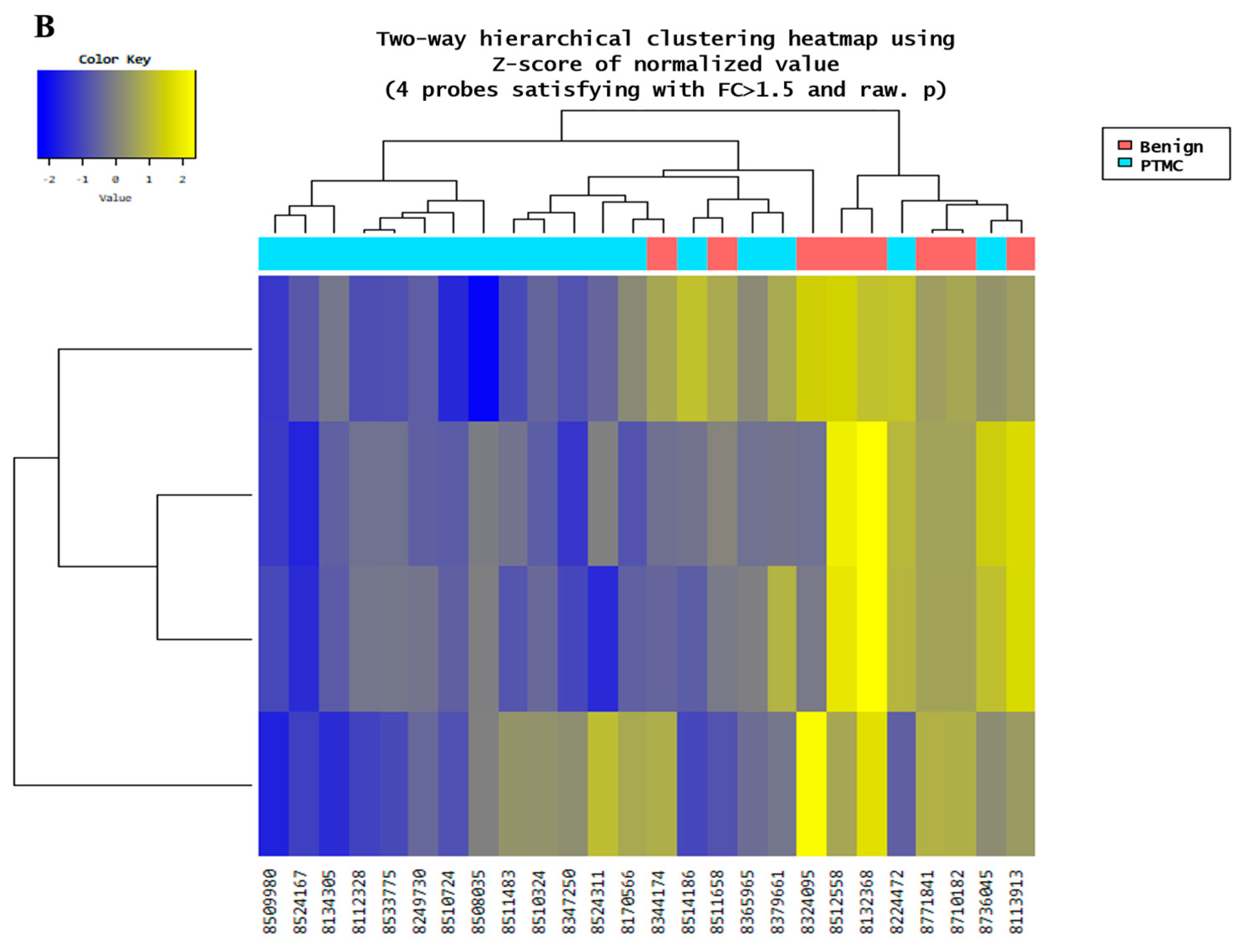
3.1.1. Microarray Analysis Performed on the Benign Nodules and PTMC Groups
3.1.2. Plasma miRNA TaqMan Assay Performed on the Benign Nodules and PTMC Groups
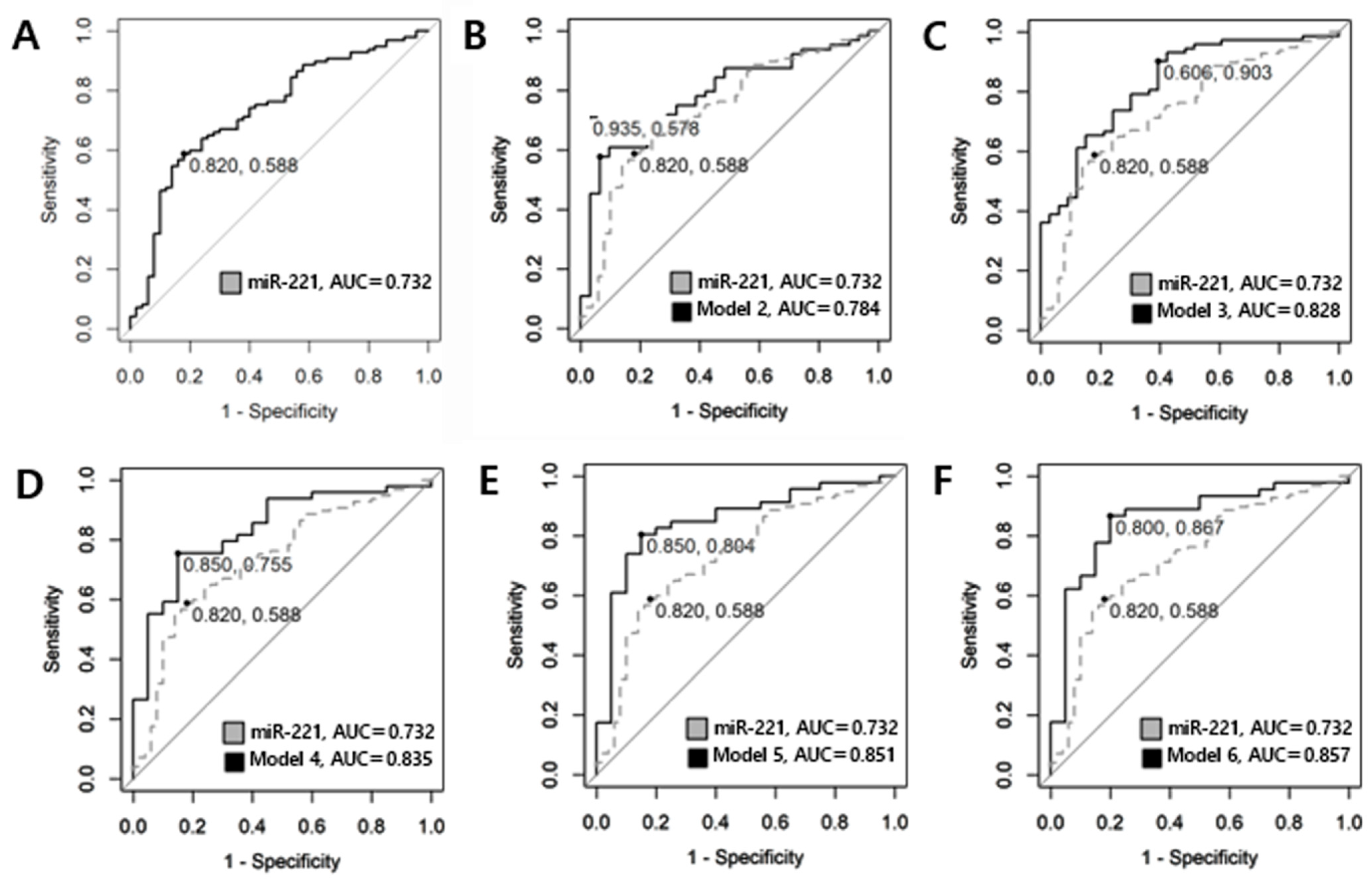
3.1.3. Differentiation Between Benign Nodules and PTMC Groups by ROC Curve
3.2. Low-Risk PTMC and Advanced PTMC
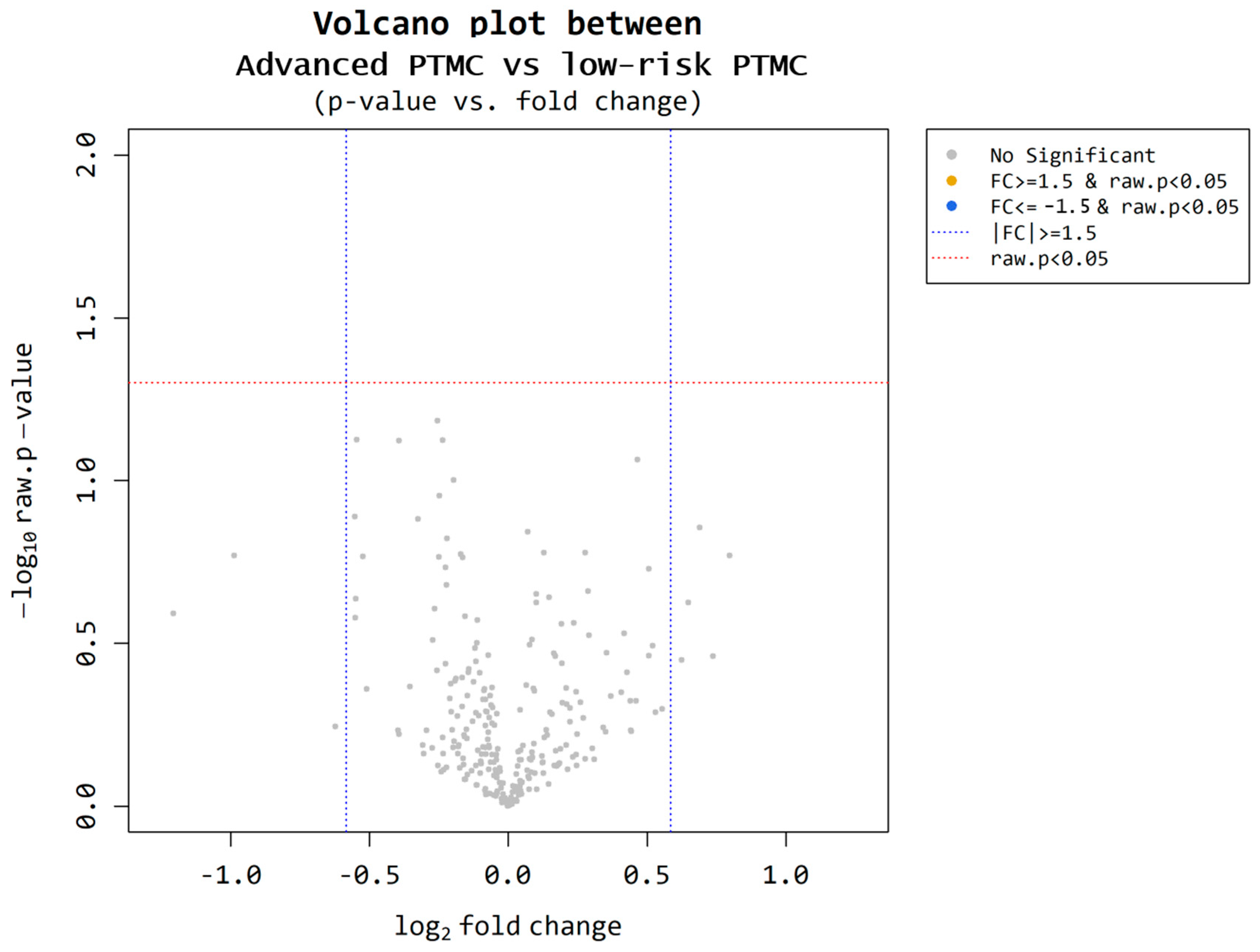
3.2.1. Microarrays Performed on the Low-Risk and Advanced PTMC Groups
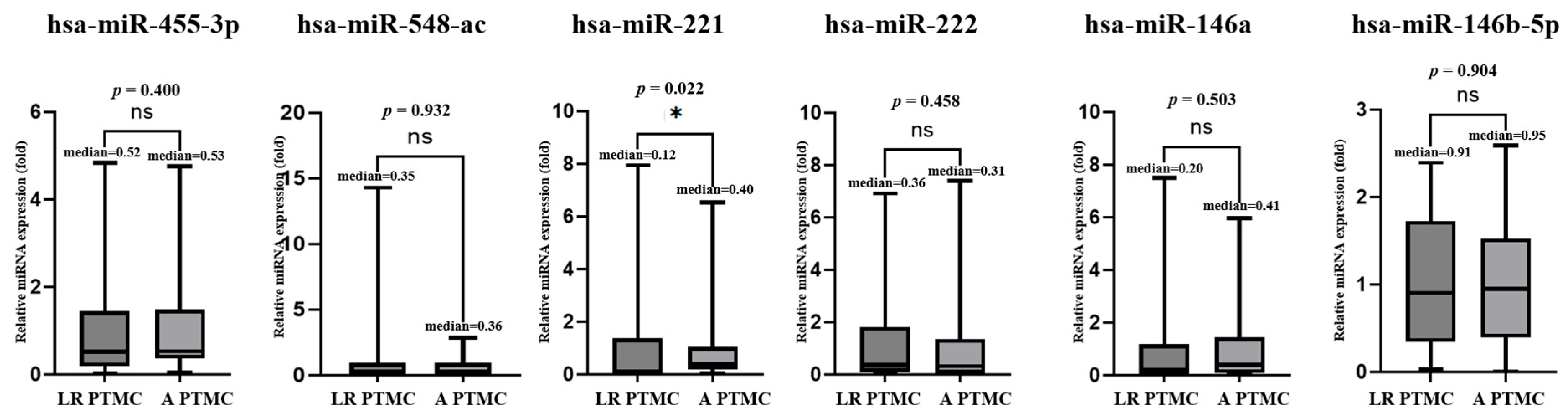
3.2.2. Plasma miRNA TaqMan Assay Performed on the Low-Risk and Advanced PTMC Groups
3.2.3. Differentiation Between Low-RISK and ADVANCED PTMC by ROC Curve
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| PTC | Papillary thyroid carcinoma |
| PTMC | Papillary thyroid microcarcinoma |
| US | Ultrasonography |
| LND | Lateral neck dissection |
| RAI | Radioactive iodine |
| miRNA | MicroRNA |
| ETE | Extrathyroidal extension |
| RT-PCR | Real-time polymerase chain reaction |
| AUC | Area under the curve |
| ROC | Receiver operating characteristic |
| TT | Total thyroidectomy |
| CCND | Central compartment neck dissection. |
| FNA | Fine needle aspiration |
References
- Orlandella, F.M.; Imperlini, E.; Pane, K.; Luciano, N.; Braile, M.; De Stefano, A.E.; Iervolino, P.L.C.; Ruocco, A.; Orrù, S.; Franzese, M.; et al. miR-331-5p affects motility of thyroid cancer cell lines and regulates BID expression. Biomedicines 2024, 12, 658. [Google Scholar] [CrossRef]
- Boucai, L.; Zafereo, M.; Cabanillas, M.E. Thyroid Cancer: A Review. JAMA 2024, 331, 425–435. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. SEER Cancer Statistics Review [Internet]; National Cancer Institute: Bethesda, MD, USA, 2023; Available online: https://seer.cancer.gov/statfacts/ (accessed on 13 May 2025).
- Pizzato, M.; Li, M.; Vignat, J.; Laversanne, M.; Singh, D.; La Vecchia, C.; Vaccarella, S. The epidemiological landscape of thyroid cancer worldwide: GLOBOCAN estimates for incidence and mortality rates in 2020. Lancet Diabetes Endocrinol. 2022, 10, 264–272. [Google Scholar] [CrossRef]
- Patel, K.N.; Yip, L.; Lubitz, C.C.; Grubbs, E.G.; Miller, B.S.; Shen, W.; Angelos, P.; Chen, H.; Doherty, G.M.; Fahey, T.J.; et al. The American Association of Endocrine Surgeons Guidelines for the Definitive Surgical Management of Thyroid Disease in Adults. Ann. Surg. 2020, 271, e21–e93. [Google Scholar] [CrossRef]
- Oharram, L.; Al-Alawi, Y.; Hariri, N.; Ghorbel, I.; Hamoud, E. Overdiagnosis and overtreatment of papillary thyroid carcinoma: A multidisciplinary review. Thyroid Res. Pract. 2021, 18, 111–115. [Google Scholar] [CrossRef]
- Sugitani, I. Active surveillance of low-risk papillary thyroid microcarcinoma. Best Pract. Res. Clin. Endocrinol. Metab. 2023, 37, 101630. [Google Scholar] [CrossRef]
- He, L.; Hannon, G.J. MicroRNAs: Small RNAs with a big role in gene regulation. Nat. Rev. Genet. 2004, 5, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Budakoti, M.; Panwar, A.S.; Molpa, D.; Singh, R.K.; Büsselberg, D.; Mishra, A.P.; Coutinho, H.D.M.; Nigam, M. Micro-RNA: The darkhorse of cancer. Cell Signal 2021, 83, 109995. [Google Scholar] [CrossRef]
- Sempere, L.F.; Azmi, A.S.; Moore, A. microRNA-based diagnostic and therapeutic applications in cancer medicine. Wiley Interdiscip. Rev. RNA 2021, 12, e1662. [Google Scholar] [CrossRef]
- Mastronikolis, N.; Tsiambas, E.; Roukas, D.; Fotiades, P.; Chrysovergis, A.; Papanikolaou, V.; Kyrodimos, E.; Mastronikoli, S.; Niotis, A.; Ragos, V. Micro-RNAs signatures in papillary thyroid carcinoma. J. BUON 2020, 25, 2144–2146. [Google Scholar]
- Lodewijk, L.; Prins, A.M.; Kist, J.W.; Valk, G.D.; Kranenburg, O.; BorelRinkes, I.H.M.; Vriens, M.R. The value of miRNA in diagnosing thyroid cancer: A systematic review. Cancer Biomark. 2012, 11, 229–238. [Google Scholar] [CrossRef]
- Toraih, E.A.; Fawzy, M.S.; Ning, B.; Zerfaoui, M.; Errami, Y.; Ruiz, E.M.; Hussein, M.H.; Haidari, M.; Bratton, M.; Tortelote, G.G.; et al. A miRNA-based prognostic model to trace thyroid cancer recurrence. Cancers 2022, 14, 4128. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Z.; Li, H.; Wang, J.; Sun, C. miR-146a and miR-146b in the diagnosis and prognosis of papillary thyroid carcinoma. Oncol. Rep. 2017, 38, 2735–2740. [Google Scholar] [CrossRef] [PubMed]
- Liang, L.; Zheng, X.; Hu, M.; Cui, Y.; Zhong, Q.; Wang, S.; Huang, F. MiRNA-221/222 in thyroid cancer: A meta-analysis. Clin. Chim. Acta 2018, 484, 284–292. [Google Scholar] [CrossRef]
- Shen, H.; Lin, Z.; Shi, H.; Wu, L.; Ma, B.; Li, H.; Yin, B.; Tang, J.; Yu, H.; Yin, X. MiR-221/222 promote migration and invasion, and inhibit autophagy and apoptosis by modulating ATG10 in aggressive papillary thyroid carcinoma. 3 Biotech 2020, 10, 339. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.S.; Lim, Y.S.; Lee, J.C.; Wang, S.G.; Park, H.Y.; Kim, S.Y.; Lee, B.J. Differential expression levels of plasma-derived miR-146b and miR-155 in papillary thyroid cancer. Oral Oncol. 2015, 51, 77–83. [Google Scholar] [CrossRef]
- Liu, Y.; Geng, H.; Liu, X.; Cao, M.; Zhang, X. A meta-analysis of circulating microRNAs in the diagnosis of papillary thyroid carcinoma. PLoS ONE 2021, 16, e0251676. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef]
- Papaioannou, M.; Chorti, A.G.; Chatzikyriakidou, A.; Giannoulis, K.; Bakkar, S.; Papavramidis, T.S. MicroRNAs in Papillary Thyroid Cancer: What Is New in Diagnosis and Treatment. Front. Oncol. 2021, 11, 755097. [Google Scholar] [CrossRef]
- Ruiz-Pozo, V.A.; Cadena-Ullauri, S.; Guevara-Ramírez, P.; Paz-Cruz, E.; Tamayo-Trujillo, R.; Zambrano, A.K. Differential microRNA expression for diagnosis and prognosis of papillary thyroid cancer. Front. Med. 2023, 10, 1139362. [Google Scholar] [CrossRef]
- Jasim, S.; Dean, D.S.; Gharib, H. Fine-NeedleAspirationoftheThyroidGland. In Endotext; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., Dungan, K., Grossman, A., Hershman, J.M., Kaltsas, G., Koch, C., Kopp, P., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2023. [Google Scholar]
- Lee, E.K.; Park, Y.J.; Jung, C.K.; Na, D.G. A Narrative Review of the 2023 Korean Thyroid Association Management Guideline for Patients with Thyroid Nodules. Endocrinol. Metab. 2024, 39, 61–72. [Google Scholar] [CrossRef]
- Ho, P.T.B.; Clark, I.M.; Le, L.T.T. MicroRNA-Based Diagnosis and Therapy. Int. J. Mol. Sci. 2022, 23, 7167. [Google Scholar] [CrossRef]
- Backes, C.; Meese, E.; Keller, A. Specific miRNA Disease Biomarkers in Blood, Serum and Plasma: Challenges and Prospects. Mol. Diagn. Ther. 2016, 20, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Kanaan, Z.; Rai, S.N.; Eichenberger, M.R.; Roberts, H.; Keskey, B.; Pan, J.; Galandiuk, S. Plasma miR-21: A potential diagnostic marker of colorectal cancer. Ann. Surg. 2012, 256, 544–551. [Google Scholar] [CrossRef]
- Qi, P.; Cheng, S.; Wang, H.; Li, N.; Chen, Y.; Gao, C. Serum microRNAs as biomarkers for hepatocellular carcinoma in Chinese patients with chronic hepatitis B virus infection. PLoS ONE 2011, 6, e28486. [Google Scholar] [CrossRef]
- Batra, J.S.; Girdhani, S.; Hlatky, L. A Quest to Identify Prostate Cancer Circulating Biomarkers with a Bench-to-Bedside Potential. J. Biomark. 2014, 2014, 321680. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Liu, H.; Zou, H.; Chen, R.; Dou, Y.; Sheng, S.; Dai, S.; Ai, J.; Melson, J.; Kittles, R.A.; et al. Evaluation of Plasma miR-21 and miR-152 as Diagnostic Biomarkers for Common Types of Human Cancers. J. Cancer 2016, 7, 490–499. [Google Scholar] [CrossRef]
- Fichtlscherer, S.; De Rosa, S.; Fox, H.; Schwietz, T.; Fischer, A.; Liebetrau, C.; Weber, M.; Hamm, C.W.; Röxe, T.; Müller-Ardogan, M.; et al. Circulating microRNAs in patients with coronary artery disease. Circ. Res. 2010, 107, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Corral-Fernández, N.E.; Salgado-Bustamante, M.; Martínez-Leija, M.E.; Cortez-Espinosa, N.; García-Hernández, M.H.; Reynaga-Hernández, E.; Quezada-Calvillo, R.; Portales-Pérez, D.P. Dysregulated miR-155 expression in peripheral blood mononuclear cells from patients with type2 diabetes. Exp. Clin. Endocrinol. Diabetes 2013, 121, 347–353. [Google Scholar]
- Chou, C.K.; Liu, R.T.; Kang, H.Y. MicroRNA-146b: A Novel Biomarker and Therapeutic Target for Human Papillary Thyroid Cancer. Int. J. Mol. Sci. 2017, 18, 636. [Google Scholar] [CrossRef]
- Han, P.A.; Weng, C.H.; Khawaja, H.T.; Nagarajan, N.; Schneider, E.B.; Umbricht, C.B.; Witwer, K.W.; Zeiger, M.A. MicroRNA Expression and Association with Clinicopathologic Features in Papillary Thyroid Cancer: A Systematic Review. Thyroid 2015, 25, 1322–1329. [Google Scholar]
- Kondrotiene, A.; Dauksa, A.; Pamedytyte, D.; Kazokaite, M.; Zvirbliene, A.; Dauksiene, D.; Simanaviciene, V.; Klimaite, R.; Golubickaite, I.; Stakaitis, R.; et al. Papillary Thyroid Carcinoma Tissue miR-146b, -21, -221, -222, -181b Expression in Relation with Clinicopathological Features. Diagnostics 2021, 11, 418. [Google Scholar] [CrossRef] [PubMed]
- Geropoulos, G.; Psarras, K.; Papaioannou, M.; Giannis, D.; Meitanidou, M.; Kapriniotis, K.; Symeonidis, N.; Pavlidis, E.T.; Pavlidis, T.E.; Sapalidis, K.; et al. Circulating microRNAs and Clinicopathological Findings of Papillary Thyroid Cancer: A Systematic Review. In Vivo 2022, 36, 1551–1569. [Google Scholar] [CrossRef] [PubMed]
- Qiao, D.H.; He, X.M.; Deng, X.; Ji, Y.C.; Yang, H.; Cheng, L.; Zhou, X.Y. Aberrant expression of five miRNAs in papillary thyroid carcinomas. J. Clin. Lab. Anal. 2021, 35, e23907. [Google Scholar] [CrossRef]
- Alexander, E.K.; Kennedy, G.C.; Baloch, Z.W.; Cibas, E.S.; Chudova, D.; Diggans, J.; Friedman, L.; Kloos, R.T.; LiVolsi, V.A.; Mandel, S.J. Molecular testing for the indeterminate thyroid nodule. N. Engl. J. Med. 2012, 367, 705–715. [Google Scholar] [CrossRef]
- Steward, D.L.; Carty, S.E.; Sippel, R.S.; Yang, S.P.; Sosa, J.A.; Sipos, J.A.; Figge, J.J.; Mandel, S.; Haugen, B.R.; Burman, K.D.; et al. Performance of a multigene genomic classifier in thyroid nodules with indeterminate cytology: A prospective multicenter study. JAMA Oncol. 2019, 5, 204–212. [Google Scholar] [CrossRef]
- Markopoulos, G.S.; Roupakia, E.; Tokamani, M.; Alabasi, G.; Sandaltzopoulos, R.; Marcu, K.B.; Kolettas, E. Roles of NF-κB signaling in the regulation of miRNAs impacting on inflammation in cancer. Biomedicines 2018, 6, 40. [Google Scholar] [CrossRef]
- Zhang, Y.; Pan, J.; Xu, D.; Yang, Z.; Sun, J.; Sun, L.; Wu, Y.; Qiao, H. Combination of serum microRNAs and ultrasound profile as predictive biomarkers of diagnosis and prognosis for papillary thyroid microcarcinoma. Oncol. Rep. 2018, 40, 3611–3624. [Google Scholar] [CrossRef]
- Peng, Y.; Li, C.; Luo, D.; Ding, J.; Zhang, W.; Pan, G. Expression profile and clinical significance of microRNAs in papillary thyroid carcinoma. Molecules 2014, 19, 11586–11600. [Google Scholar] [CrossRef]
- D’Amico, G.; Santonocito, R.; Grech, G.; Graceffa, G.; Cipolla, C.; Scalia, F.; Raccosta, S.; Manno, M.; Conwayde Macario, E.; Macario, A.J.L.; et al. MiRNAs in Extracellular Vesicles as Biomarkers in Plasma of Papillary Thyroid Cancer Patients: A Proof-of-Concept Study. Biology 2024, 13, 743. [Google Scholar] [CrossRef]
- Toraih, E.A.; Elshazli, R.M.; Trinh, L.N.; Hussein, M.H.; Attia, A.A.; Ruiz, E.M.L.; Zerfaoui, M.; Fawzy, M.S.; Kandil, E. Diagnostic and prognostic performance of liquid biopsy-derived exosomal microRNAs in thyroid cancer patients: A systematic review and meta-analysis. Cancers 2021, 13, 4295. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Benign (n = 50) | Low-Risk PTMC (n = 50) | Advanced PTMC (n = 50) |
|---|---|---|---|
| Gender | |||
| Male | 13 | 13 | 13 |
| Female | 37 | 37 | 37 |
| Age (yr, mean ± SD) | 48.56 (±12.34) | 48.51 (±11.53) | 48.74 (±11.70) |
| Tumor size (cm ± SD) | 2.38 (±1.34) | 0.66 (±0.17) | 0.67 (±0.18) |
| Multifocality, n (%) | |||
| Yes | - | 22 (44) | 22 (44) |
| No | - | 28 (56) | 28 (56) |
| ETE, n(%) | |||
| No | - | 42(84) | 31(62) |
| Minimal | - | 8(16) | 18(36) |
| Gross | 0 (0) | 1(2) | |
| CLNM, n (%) | |||
| Yes | - | 4 (8) | 47 (94) |
| No | - | 46 (92) | 3 (6) |
| LLNM, n (%) | |||
| Yes | - | 0 (0) | 20 (40) |
| No | - | 50 (100) | 30 (60) |
| BRAF mutation, n (%) | |||
| Not tested | - | 40 (80) | 39 (78) |
| Positive | - | 1 (2) | 7 (14) |
| Negative | - | 9 (18) | 4 (8) |
| Number of LN metastasis cases Average n (min,max) | 0 (0,0) | 0.04 (0,1) | 8.42 (5,20) |
| Surgery, n (%) | |||
| HT | 31 (62) | 2 (4) | 0 (0) |
| HT with CCND ** | 11 (22) | 16 (32) | 5 (10) |
| TT | 3 (6) | 0 (0) | 0 (0) |
| TT with CCND ** | 5 (10) | 32 (64) | 25 (50) |
| TT with CCND, LND | 0 (0) | 0 (0) | 20 (40) |
| Characteristics | Benign (n = 9) | Low-Risk PTMC (n = 9) | Advanced PTMC (n = 9) |
|---|---|---|---|
| Gender | |||
| Male | 2 | 2 | 2 |
| Female | 7 | 7 | 7 |
| Age (years, mean ± SD) | 50.89 (±10.71) | 49.22 (±10.70) | 47.78 (±10.49) |
| Tumor size (cm ± SD) | 2.84 (±1.60) | 0.63 (±0.19) | 0.7 (±0.16) |
| Multifocality, n(%) | |||
| Yes | - | 2 | 2 |
| No | - | 7 | 7 |
| miRNA Base | PTMC/Benign Fold Change | PTMC/Benign Raw p-Value |
|---|---|---|
| has-miR-455-3p | −2.736502 | 0.00002907 |
| has-miR-548ac | −1.694879 | 0.00591083 |
| - | −1.734454 | 0.01860101 |
| - | −1.648868 | 0.01374299 |
| Model | miRNA | AUC (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | Cut-Off Value (Log Transformed) | p-Value | BIC |
|---|---|---|---|---|---|---|---|
| 1 | miRNA-455-3p | 0.512 (0.386, 0.638) | 0.522 (0.418, 0.642) | 0.613 (0.419, 0.774) | −0.774 | 0.579 | 131.5 |
| 1 | miRNA-548ac | 0.578 (0.458, 0.697) | 0.533 (0.427, 0.640) | 0.647 (0.500, 0.794) | −1.465 | 0.903 | 142.8 |
| 1 | miRNA-146a | 0.508 (0.410, 0.606) | 0.387 (0.290, 0.484) | 0.735 (0.592, 0.857) | −1.648 | 0.564 | 192.8 |
| 1 | miRNA-146b | 0.640 (0.547, 0.734) | 0.480 (0.378, 0.582) | 0.780 (0.660, 0.880) | 0.419 | 0.003 | 192.3 |
| 1 | miRNA-221 | 0.732 (0.646, 0.819) | 0.588 (0.485, 0.691) | 0.820 (0.720, 0.920) | −0.424 | <0.001 | 176.8 |
| 1 | miRNA-222 | 0.703 (0.612, 0.793) | 0.626 (0.525, 0.717) | 0.714 (0.571, 0.837) | −0.852 | <0.001 | 179.8 |
| 2 | miRNA-455-3p + miRNA-221 | 0.784 (0.690, 0.879) | 0.578 (0.469, 0.703) | 0.935 (0.839, 1.000) | - | <0.001 | 112.6 |
| 3 | miRNA-548ac + miRNA-221 + miRNA-222 | 0.828 (0.745, 0.911) | 0.903 (0.833, 0.958) | 0.606 (0.424, 0.758) | - | <0.001 | 115.5 |
| 4 | miRNA-455-3p + miRNA-548ac + miRNA-221 + miRNA-222 | 0.835 (0.732, 0.938) | 0.755 (0.633, 0.857) | 0.850 (0.700, 1.000) | - | <0.001 | 93.7 |
| 5 | miRNA-455-3p + miRNA-548ac + miRNA-146a + miRNA-221 + miRNA-222 | 0.851 (0.748, 0.954) | 0.804 (0.674, 0.913) | 0.850 (0.650, 1.000) | - | <0.001 | 90.1 |
| 6 | miRNA-455-3p + miRNA-548ac + miRNA-146a + miRNA-146b +miRNA-221 + miRNA-222 | 0.857 (0.753, 0.960) | 0.867 (0.756, 0.956) | 0.800 (0.600, 0.950) | - | <0.001 | 88.6 |
| Model | miRNA | AUC (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | Cut-Off Value (Log Transformed) | p-Value | BIC |
|---|---|---|---|---|---|---|---|
| 1 | miRNA-455.3p | 0.560 (0.419, 0.701) | 0.943 (0.857, 1.000) | 0.250 (0.125, 0.406) | −1.804 | 0.203 | 99.3 |
| 1 | miRNA-548ac | 0.506 (0.373, 0.639) | 0.400 (0.257, 0.571) | 0.700 (0.550, 0.850) | −0.797 | 0.468 | 112.3 |
| 1 | miRNA-146a | 0.540 (0.421, 0.659) | 0.614 (0.455, 0.750) | 0.531 (0.388, 0.673) | −1.146 | 0.254 | 137.3 |
| 1 | miRNA-146b | 0.519 (0.403, 0.635) | 0.521 (0.375, 0.667) | 0.580 (0.460, 0.720) | 0.433 | 0.373 | 144.9 |
| 1 | miRNA-221 | 0.636 (0.518, 0.754) | 0.900 (0.820, 0.980) | 0.468 (0.319, 0.596) | −1.524 | 0.011 | 135.3 |
| 1 | miRNA-222 | 0.543 (0.428, 0.658) | 0.245 (0.122, 0.367) | 0.880 (0.780, 0.960) | −2.284 | 0.772 | 145.7 |
| 2 | miRNA.455-3p + miRNA-221 | 0.681 (0.540, 0.821) | 0.971 (0.914, 1.000) | 0.448 (0.276, 0.621) | 0.006 | 92.8 | |
| 3 | miRNA-455-3p + miRNA-221 + mRNA-222 | 0.748 (0.624, 0.873) | 0.794 (0.647, 0.912) | 0.621 (0.448, 0.793) | <0.001 | 91.3 | |
| 4 | miRNA-455-3p + miRNA-146b + miRNA-221+ miRNA-222 | 0.770 (0.649, 0.891) | 0.818 (0.667, 0.939) | 0.655 (0.483, 0.828) | <0.001 | 91.7 | |
| 5 | miRNA-455-3p + miRNA-146a + miRNA-146b + miRNA-221 + miRNA-222 | 0.757 (0.629, 0.886) | 0.759 (0.586, 0.897) | 0.724 (0.552, 0.862) | <0.001 | 92.6 | |
| 6 | miRNA.455-3p + miRNA-548ac + miRNA-146a + miRNA-146b + miRNA-221 + miRNA-222 | 0.763 (0.623, 0.903) | 0.739 (0.565, 0.913) | 0.727 (0.545, 0.909) | 0.001 | 77.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, J.; Kim, J.M.; Shin, S.-C.; Cheon, Y.-i.; Kim, B.H.; Kim, M.; Kim, S.S.; Lee, B.-J. Diagnosis and Evaluation of Aggressiveness Using Circulating Plasma miRNAs in Papillary Thyroid Microcarcinoma. Cancers 2025, 17, 2079. https://doi.org/10.3390/cancers17132079
Jang J, Kim JM, Shin S-C, Cheon Y-i, Kim BH, Kim M, Kim SS, Lee B-J. Diagnosis and Evaluation of Aggressiveness Using Circulating Plasma miRNAs in Papillary Thyroid Microcarcinoma. Cancers. 2025; 17(13):2079. https://doi.org/10.3390/cancers17132079
Chicago/Turabian StyleJang, Jiwon, Ji Min Kim, Sung-Chan Shin, Yong-il Cheon, Bo Hyun Kim, Mijin Kim, Sang Soo Kim, and Byung-Joo Lee. 2025. "Diagnosis and Evaluation of Aggressiveness Using Circulating Plasma miRNAs in Papillary Thyroid Microcarcinoma" Cancers 17, no. 13: 2079. https://doi.org/10.3390/cancers17132079
APA StyleJang, J., Kim, J. M., Shin, S.-C., Cheon, Y.-i., Kim, B. H., Kim, M., Kim, S. S., & Lee, B.-J. (2025). Diagnosis and Evaluation of Aggressiveness Using Circulating Plasma miRNAs in Papillary Thyroid Microcarcinoma. Cancers, 17(13), 2079. https://doi.org/10.3390/cancers17132079