
Routes to Diagnosis in Lung Cancer—Do Socio-Demographics Matter? An English Population-Based Study

Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting and Data Sources
2.2. Population
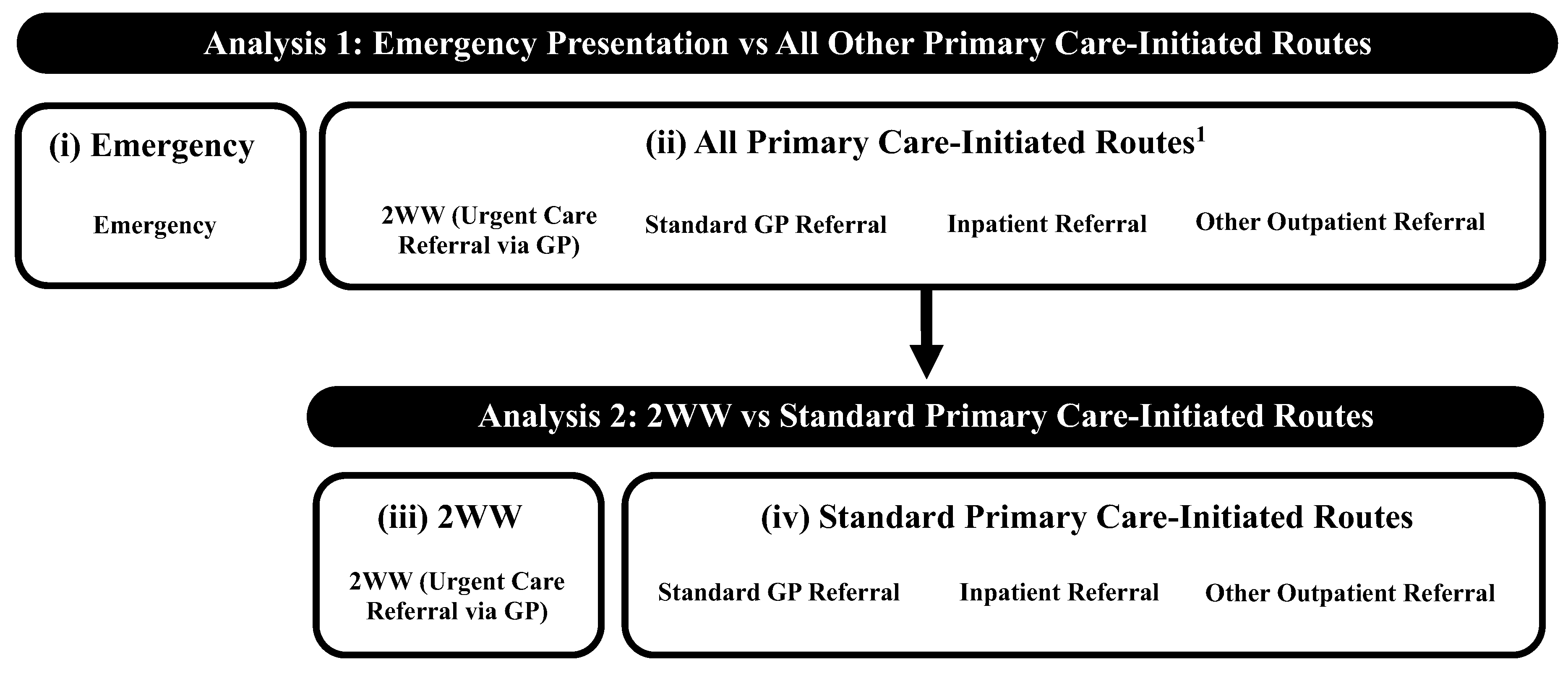
2.3. Outcome Variables
2.4. Explanatory Variables
2.5. Statistical Analyses
2.6. Ethics and Reporting
3. Results
3.1. Patient Characteristics
3.2. Analysis 1: Emergency Presentation vs. All Primary Care-Initiated Routes
3.3. Analysis 2: 2WW vs. Standard Primary Care-Initiated Routes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- The United Kingdom Lung Cancer Coalition. Early Diagnosis Matters: Making the Case for the Early and Rapid Diagnosis of Lung Cancer. 2020. Available online: https://www.uklcc.org.uk/our-reports/january-2020/early-diagnosis-matters (accessed on 4 December 2023).
- McPhail, S.; Johnson, S.; Greenberg, D.; Peake, M.; Rous, B. Stage at diagnosis and early mortality from cancer in England. Br. J. Cancer 2015, 112 (Suppl. 1), S108–S115. [Google Scholar] [CrossRef] [PubMed]
- Arnold, M.; Rutherford, M.; Bardot, A.; Ferlay, J.; Andersson, T.M.-L.; Myklebust, T.Å.; Tervonen, H.; Thursfield, V.; Ransom, D.; Shack, L.; et al. Progress in cancer survival, mortality, and incidence in seven high-income countries 1995-2014 (ICBP SURVMARK-2): A population-based study. Lancet Oncol. 2019, 20, 1493–1505. [Google Scholar] [CrossRef] [PubMed]
- Sanghrajka, A.; Sharp, L.; Rowlands, G. How does socio-economic disadvantage influence the timeliness of lung cancer diagnosis? A systematic review and synthesis of published qualitative studies. Pub. Health. under review.
- Department of Health & Social Care. New Lung Cancer Screening Roll out to Detect Cancer Sooner. 2023. Available online: https://www.gov.uk/government/news/new-lung-cancer-screening-roll-out-to-detect-cancer-sooner (accessed on 4 December 2023).
- Crosbie, P.A.; Balata, H.; Evison, M.; Atack, M.; Bayliss-Brideaux, V.; Colligan, D.; Duerden, R.; Eaglesfield, J.; Edwards, T.; Elton, P.; et al. Implementing lung cancer screening: Baseline results from a community-based “Lung Health Check” pilot in deprived areas of Manchester. Thorax 2019, 74, 405–409. [Google Scholar] [CrossRef]
- Horst, C.; Dickson, J.L.; Tisi, S.; Ruparel, M.; Nair, A.; Devaraj, A.; Janes, S.M. Delivering low-dose CT screening for lung cancer: A pragmatic approach. Thorax 2020, 75, 831–832. [Google Scholar] [CrossRef]
- Department of Health. The NHS Cancer Plan: A Plan for Investment, a Plan for Reform. 2000. Available online: https://image.guardian.co.uk/sys-files/Society/documents/2003/08/26/cancerplan.pdf (accessed on 5 December 2023).
- Round, T.; Ashworth, M.; L’esperance, V.; Møller, H. Cancer detection via primary care urgent referral and association with practice characteristics: A retrospective cross-sectional study in England from 2009/2010 to 2018/2019. Br. J. Gen. Pract. 2021, 71, e826–e835. [Google Scholar] [CrossRef]
- Neal, R.D.; Smith, L. Urgent cancer referrals: How well are they working and can they be improved? Br. J. Gen. Pract. 2021, 71, 390–391. [Google Scholar] [CrossRef]
- National Cancer Institute. Suspected Cancer: Recognition and Referral NICE Guideline NG12. 2023. Available online: https://www.nice.org.uk/guidance/ng12 (accessed on 4 December 2023).
- NHS England. Implementing a Timed Lung Cancer Diagnostic Pathway. 2023. Available online: https://www.england.nhs.uk/long-read/implementing-a-timed-lung-cancer-diagnostic-pathway/ (accessed on 20 February 2024).
- Onwuka, J.U.; Zahed, H.; Feng, X.; Alcala, K.; Erhunmwunsee, L.; Williams, R.M.; Aldrich, M.C.; Ahluwalia, J.S.; Albanes, D.; Arslan, A.A.; et al. Association between socioeconomic position and lung cancer incidence in 16 countries: A prospective cohort consortium study. eClinicalMedicine 2025, 82, 103152. [Google Scholar] [CrossRef]
- Martins, T.; Abel, G.; Ukoumunne, O.C.; Price, S.; Lyratzopoulos, G.; Chinegwundoh, F.; Hamilton, W. Assessing ethnic inequalities in diagnostic interval of common cancers: A population-based UK cohort study. Cancers 2022, 14, 3085. [Google Scholar] [CrossRef]
- Norris, R.P.; Dew, R.; Greystoke, A.; Todd, A.; Sharp, L. Socio-economic inequalities in novel NSCLC treatments during the era of tumor biomarker guided therapy: A population-based cohort study in a publicly funded healthcare system. J. Thorac. Oncol. 2023, 18, 990–1002. [Google Scholar] [CrossRef]
- Martins, T.; Abel, G.; Okumunne, O.C.; Mounce, L.T.A.; Price, S.; Lyratzopoulos, G.; Hamilton, W. Ethnic inequalities in routes to diagnosis of cancer: A population-based UK cohort study. Br. J. Cancer 2022, 127, 863–871. [Google Scholar] [CrossRef] [PubMed]
- O’Dowd, E.L.; McKeever, T.M.; Baldwin, D.R.; Anwar, S.; Powell, H.A.; Gibson, J.E.; Iyen-Omofoman, B.; Hubbard, R.B. What characteristics of primary care and patients are associated with early death in patients with lung cancer in the UK? Thorax 2015, 70, 161–168. [Google Scholar] [CrossRef] [PubMed]
- Beard, E.; Brown, J.; Jackson, S.E.; West, R.; Kock, L.; Boniface, S.; Shahab, L. Independent Associations Between Different Measures of Socioeconomic Position and Smoking Status: A Cross-Sectional Study of Adults in England. Nicotine Tob. Res. 2021, 23, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Lei, F.; Lee, E. Barriers to lung cancer screening with low-dose computed tomography. Oncol. Nurs. Forum. 2019, 46, E60–E71. [Google Scholar] [CrossRef]
- Carter-Harris, L.; Brandzel, S.; Wernli, K.J.; Roth, J.A.; Buist, D.S.M. A qualitative study exploring why individuals opt out of lung cancer screening. Fam. Pract. 2017, 34, 239–244. [Google Scholar] [CrossRef]
- Danckert, B.; Christensen, N.L.; Falborg, A.Z.; Frederiksen, H.; Lyratzopoulos, G.; McPhail, S.; Pederson, A.F.; Ryg, J.; Thomsen, L.A.; Vedsted, P.; et al. Assessing how routes to diagnosis vary by the age of patients with cancer: A nationwide register-based cohort study in Denmark. BMC Cancer 2022, 22, 906. [Google Scholar] [CrossRef]
- Abel, G.A.; Shelton, J.; Johnson, S.; Elliss-Brookes, L.; Lyratzopoulos, G. Cancer-specific variation in emergency presentation by sex, age and deprivation across 27 common and rarer cancers. Br. J. Cancer 2015, 112 (Suppl. S1), S129–S136. [Google Scholar] [CrossRef]
- Danckert, B.; Falborg, A.Z.; Christensen, N.L.; Frederiksen, H.; Lyratzopoulos, G.; McPhail, S.; Ryg, J.; Vedsted, P.; Thomsen, L.A.; Jensen, H. Routes to diagnosis and the association with the prognosis in patients with cancer—A nationwide register-based cohort study in Denmark. Cancer Epidemiol. 2021, 74, 101983. [Google Scholar] [CrossRef]
- Henson, K.E.; Ellis-Brookes, L.; Coupland, V.H.; Payne, E.; Vernon, S.; Rous, B.; Rashbass, J. Data resource profile: National cancer registration dataset in England. Int. J. Epidemiol. 2020, 49, 16–16h. [Google Scholar] [CrossRef]
- Elliss-Brookes, L.; McPhail, S.; Ives, A.; Greenslade, M.; Shelton, J.; Hiom, S.; Richards, M. Routes to diagnosis for cancer—Determining the patient journey using multiple routine data sets. Br. J. Cancer 2012, 107, 1220–1226. [Google Scholar] [CrossRef]
- Union for International Cancer Control. TNM: Classification of Malignant Tumours, 8th ed.; Wiley: New York, NY, USA, 2016. [Google Scholar]
- World Health Organisation. International Classification of Disease for Oncology (ICD-O3), 3rd ed.; Fritz, A., Percy, C., Jack, A., Shanmugaratnam, K., Sobin, L., Parkin, D.M., Whelan, S., Eds.; World Health Organisation: Geneva, Switzerland, 2000. [Google Scholar]
- Deane, J.; Norris, R.; O’Hara, J.; Patterson, J.; Sharp, L. Who presents where? a population-based analysis of socio-demographic inequalities in head and neck cancer patients’ referral routes. Int. J. Environ. Res. Public Health 2022, 19, 16723. [Google Scholar] [CrossRef] [PubMed]
- Department for Communities and Local Government. The English Index of Multiple Deprivation (IMD) 2015—Guidance. 2015. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/464430/English_Index_of_Multiple_Deprivation_2015_-_Guidance.pdf (accessed on 28 August 2021).
- Department for Environment, Food & Rural Affairs. Rural Urban Classification. 2021. Available online: https://www.gov.uk/government/collections/rural-urban-classification#:~:text=The%20six%20categories%20are%3A,population%20resides%20in%20rural%20areas (accessed on 8 February 2024).
- Office for National Statistics. England: Detailed Information on the Administrative Structure Within England. Available online: https://www.ons.gov.uk/methodology/geography/ukgeographies/administrativegeography/england (accessed on 30 August 2021).
- Yu, M.; Feuer, E.J.; Cronin, K.A.; Caporaso, N.E. Use of multiple imputation to correct for bias in lung cancer incidence trends by histologic subtype. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1546–1558. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vanderbroucke, J.P. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Ann. Intern. Med. 2007, 147, 573–577. [Google Scholar] [CrossRef]
- Beckett, P.; Tata, L.J.; Hubbard, R.B. Risk factors and survival outcome for non-elective referral in non-small cell lung cancer patients-analysis based on the national lung cancer audit. Lung Cancer 2014, 83, 396–400. [Google Scholar] [CrossRef]
- McMaughan, D.J.; Oloruntoba, O.; Smith, M.L. Socioeconomic Status and Access to Healthcare: Interrelated Drivers for Healthy Aging. Front. Public Health 2020, 8, 231. [Google Scholar] [CrossRef]
- Public Health England. Local Action on Health Inequalities Improving Health Literacy to Reduce Health Inequalities. 2015. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/460710/4b_Health_Literacy-Briefing.pdf (accessed on 14 April 2025).
- Schumacher, J.R.; Hall, A.G.; Davis, T.C.; Arnold, C.L.; Bennett, R.D.; Wolf, M.S.; Carden, D.L. Potentially Preventable Use of Emergency Services: The Role of Low Health literacy. Med. Care 2013, 51, 654–658. [Google Scholar] [CrossRef]
- Morris, N.S.; Field, T.S.; Wagner, J.L.; Cutrona, S.L.; Roblin, D.W.; Gaglio, B.; Williams, A.E.; Han, P.J.K.; Costanza, M.E.; Mazor, K.M. The association between health literacy and cancer-related attitudes, behaviors, and knowledge. J. Health Commun. 2013, 18 (Suppl. 1), 223–241. [Google Scholar] [CrossRef]
- Office for National Statistics. Adult Smoking Habits in the UK: 2022. 2022. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandlifeexpectancies/bulletins/adultsmokinghabitsingreatbritain/2022 (accessed on 14 December 2023).
- Health Services Safety Investigations Body. Investigations Report: Missed Detection of Lung Cancer on Chest X-Rays of Patients Being Seen in Primary Care. 2021. Available online: https://www.hssib.org.uk/patient-safety-investigations/missed-detection-of-lung-cancer-on-chest-x-rays-of-patients-being-seen-in-primary-care/investigation-report/ (accessed on 14 December 2023).
- Greenwood-Ericksen, M.B.; Kocher, K. Trends in emergency department use by rural and urban populations in the United States. JAMA Netw. Open 2019, 2, e191919. [Google Scholar] [CrossRef]
- Sharp, L.; Donnelly, D.; Hegarty, A.; Carsin, A.-E.; Deady, S.; McCluskey, N.; Gavin, A.; Comber, H. Risk of several cancers is higher in urban areas after adjusting for socioeconomic status. Results from a two-country population-based study of 18 common cancers. J. Urban Health 2014, 91, 510–525. [Google Scholar] [CrossRef]
- Dobson, C.; Deane, J.; MacDonald, S.; Murchie, P.; Ellwood, C.; Angell, L.; Rubin, G. Barriers to early presentation amongst rural residents experiencing symptoms of colorectal cancer: A qualitative interview study. Cancers 2022, 15, 274. [Google Scholar] [CrossRef] [PubMed]
- Bergin, R.J.; Emery, J.; Bollard, R.C.; Falborg, A.Z.; Jensen, H.; Weller, D.; Menon, U.; Vedsted, P.; Thoma, R.J.; Whitfield, K.; et al. Rural–urban disparities in time to diagnosis and treatment for colorectal and breast cancer. Cancer Epidemiol. Biomark. Prev. 2018, 27, 1036–1046. [Google Scholar] [CrossRef] [PubMed]
- Lorenc, T.; Petticrew, M.; Welch, V.; Tugwell, P. What types of interventions generate inequalities? Evidence from systematic reviews. J. Epidemiol. Community Health 2013, 67, 190–193. [Google Scholar] [CrossRef]
- McPhail, S.; Swabb, R.; Johnson, S.A.; Barclay, M.E.; Elkader, H.A.; Alvi, R.; You, H. Risk factors and prognostic implications of diagnosis of cancer within 30 days after an emergency hospital admission (emergency presentation): An international cancer benchmarking partnership (ICBP) population-based study. Lancet Oncol. 2022, 23, 587–600. [Google Scholar] [CrossRef] [PubMed]
- NHS England. Urgent Cancer Diagnostic Services During COVID-19. 2021. Available online: https://www.england.nhs.uk/coronavirus/documents/c0789-urgent-cancer-diagnostic-services-during-covid-19/#:~:text=Urgent%20cancer%20diagnostic%20pathways%20have,be%20seen%20at%20one%20time (accessed on 18 December 2023).


{kind=link}
{kind=link}
| Characteristic | Number (%) |
|---|---|
| Deprivation 1 | |
| 1 (Least Deprived) | 25,302 (13.92) |
| 2 | 32,606 (17.94) |
| 3 | 36,234 (19.93) |
| 4 | 40,685 (22.38) |
| 5 (Most Deprived) | 46,936 (25.82) |
| Sex | |
| Male | 97,827 (53.82) |
| Female | 83,936 (46.18) |
| Age at Diagnosis (Years) | |
| <50 | 4632 (2.55) |
| 50–59 | 16,772 (9.23) |
| 60–69 | 47,667 (26.22) |
| 70–79 | 63,050 (34.69) |
| 80–89 | 42,325 (23.29) |
| 90+ | 7317 (4.03) |
| Ethnicity | |
| White | 168,809 (92.87) |
| Other Ethnic Group 2 | 6256 (3.44) |
| Unknown 3 | 6698 (3.69) |
| Rural/Urban Residence | |
| Rural Village, Hamlet, and Isolated Dwellings | 14,231 (7.83) |
| Rural Town and Fringe | 17,439 (9.59) |
| Urban City and Town | 80,331 (44.20) |
| Extensive Urban Area | 69,762 (38.38) |
| Government Region | |
| North West | 30,903 (17.00) |
| North East | 13,301 (7.32) |
| West Midlands | 18,661 (10.27) |
| Yorkshire and the Humber | 21,535 (11.85) |
| East Midlands | 15,654 (8.61) |
| East of England | 18,765 (10.32) |
| South East | 26,027 (14.32) |
| South West | 17,738 (9.76) |
| London | 19,179 (10.55) |
| Stage at Diagnosis | |
| I | 27,476 (15.12) |
| II | 13,520 (7.44) |
| III | 35,303 (19.42) |
| IV | 88,363 (48.61) |
| Unknown 4 | 17,101 (9.41) |
| Histology | |
| SCLC | 19,125 (10.52) |
| NSCLC 5 | 157,214 (86.49) |
| Other 6 | 5424 (2.98) |
| Multiple Tumours 7 | |
| No | 149,148 (82.06) |
| Yes | 32,615 (17.94) |
| Number of Comorbidities 8 | |
| 0 | 101,797 (56.01) |
| 1–2 | 56,059 (30.84) |
| 3+ | 23,907 (13.15) |
| Discussed at MDT | |
| Yes | 83,489 (45.93) |
| No | 30,631 (16.85) |
| Missing | 67,643 (37.21) |
| Diagnosis Year | |
| 2012 | 36,067 (19.84) |
| 2013 | 36,157 (19.89) |
| 2014 | 36,506 (20.08) |
| 2015 | 36,516 (20.09) |
| 2016 | 36,517 (20.09) |
| Diagnosis Route 9 | |
| Emergency 10 | 64,045 (35.24) |
| Standard GP Referral | 41,788 (22.99) |
| Inpatient Elective | 2976 (1.64) |
| Outpatient (Other) | 21,555 (11.86) |
| 2WW 11 | 51,399 (28.28) |
| All Primary Care-Initiated Routes 12 | 117,718 (64.76) |
| Standard Primary Care-Initiated Routes 13 | 66,319 (36.49) |
| Analysis 1: Emergency Presentation vs. All Primary Care-Initiated Routes | Analysis 2: 2WW vs. Standard Primary Care-Initiated Routes | |||
|---|---|---|---|---|
| Emergency Presentation 1 n = 64,045 (35.24%) | All Primary Care-Initiated Routes 2 n = 117,718 (64.76%) | 2WW 3 n = 51,399 (43.66%) | Standard Primary Care-Initiated Routes 4 n = 66,319 (56.34%) | |
| Deprivation 4,5 | ||||
| 1 (Least Deprived) | 8193 (32.38) | 17,109 (67.62) | 7234 (42.28) | 9875 (57.72) |
| 2 | 10,976 (33.66) | 21,630 (66.34) | 9569 (44.24) | 12,061 (55.76) |
| 3 | 12,751 (35.19) | 23,483 (64.81) | 10,300 (43.86) | 13,183 (56.14) |
| 4 | 14,816 (36.42) | 25,869 (63.58) | 11,476 (44.36) | 14,393 (55.64) |
| 5 (Most Deprived) | 17,309 (36.88) | 29,627 (63.12) | 12,820 (43.27) | 16,807 (56.73) |
| Sex | ||||
| Male | 34,022 (34.78) | 63,805 (65.22) | 27,805 (43.58) | 36,000 (56.42) |
| Female | 30,023 (35.77) | 53,913 (64.23) | 23,594 (43.76) | 30,319 (56.24) |
| Age at Diagnosis (Years) | ||||
| <50 | 1471 (31.76) | 3161 (68.24) | 1276 (40.37) | 1885 (59.63) |
| 50–59 | 4896 (29.19) | 11,876 (70.81) | 5367 (45.19) | 6509 (54.81) |
| 60–69 | 13,466 (28.25) | 34,201 (71.75) | 15,574 (45.54) | 18,627 (54.46) |
| 70–79 | 20,487 (32.49) | 42,563 (67.51) | 18,333 (43.07) | 24,230 (56.93) |
| 80–89 | 19,147 (45.24) | 23,178 (54.76) | 9708 (41.88) | 13,470 (58.12) |
| 90+ | 4578 (62.57) | 2739 (37.43) | 1141 (41.66) | 1598 (58.34) |
| Ethnicity | ||||
| White | 58,809 (34.84) | 110,000 (65.16) | 48,528 (44.12) | 61,472 (55.88) |
| Other Ethnic Group 6 | 2300 (36.76) | 3956 (63.24) | 1396 (35.29) | 2560 (64.71) |
| Unknown 7 | 2936 (43.83) | 3762 (56.17) | 1475 (39.21) | 2287 (60.79) |
| Rural/Urban Residence | ||||
| Rural Village, Hamlet, and Isolated Dwellings | 4478 (31.47) | 9753 (68.53) | 4361 (44.71) | 5392 (55.29) |
| Rural Town and Fringe | 5920 (33.95) | 11,519 (66.05) | 5248 (45.56) | 6271 (54.44) |
| Urban City and Town | 27,978 (34.83) | 52,353 (65.17) | 24,321 (46.46) | 28,032 (53.54) |
| Extensive Urban Area | 25,669 (36.80) | 44,093 (63.20) | 17,469 (39.62) | 26,624 (60.38) |
| Government Region 8 | ||||
| North West | 10,395 (33.64) | 20,508 (66.36) | - | - |
| North East | 4640 (34.88) | 8661 (65.12) | - | - |
| West Midlands | 6642 (35.59) | 12,019 (64.41) | - | - |
| Yorkshire and the Humber | 7803 (36.23) | 13,732 (63.77) | - | - |
| East Midlands | 5559 (35.51) | 10,095 (64.49) | - | - |
| East of England | 6386 (34.03) | 12,379 (65.97) | - | - |
| South East | 8892 (34.16) | 17,135 (65.84) | - | - |
| South West | 6091 (34.34) | 11,647 (65.66) | - | - |
| London | 7637 (39.82) | 11,542 (60.18) | - | - |
| Analysis 1: Emergency Presentation vs. All Primary Care-Initiated Routes 1 | Analysis 2: 2WW Pathway vs. All Other Standard Primary Care-Initiated Routes 2 | |||
|---|---|---|---|---|
| mvOR | 95% CI | mvOR | 95% CI | |
| Deprivation 3 | ||||
| 1 (Least Deprived) | 1.00 | - | 1.00 | - |
| 2 | 1.07 | 1.03–1.11 | 1.08 | 1.04–1.13 |
| 3 | 1.15 | 1.11–1.19 | 1.08 | 1.04–1.12 |
| 4 | 1.22 | 1.18–1.27 | 1.13 | 1.08–1.17 |
| 5 (Most Deprived) | 1.29 | 1.25–1.34 | 1.13 | 1.08–1.17 |
| Sex | ||||
| Male | 1.00 | - | 1.00 | - |
| Female | 1.03 | 1.01– 1.05 | 1.00 | 0.98–1.03 |
| Age at Diagnosis (Years) | ||||
| <50 | 0.93 | 0.87–0.99 | 0.92 | 0.85–0.99 |
| 50–59 | 0.83 | 0.80–0.87 | 1.10 | 1.05–1.14 |
| 60–69 | 0.81 | 0.79–0.83 | 1.10 | 1.07–1.13 |
| 70–79 | 1.00 | - | 1.00 | - |
| 80–89 | 1.73 | 1.68–1.77 | 0.95 | 0.92–0.98 |
| 90+ | 3.49 | 3.32–3.67 | 0.95 | 0.87–1.02 |
| Ethnicity | ||||
| White | 1.00 | - | 1.00 | - |
| Other Ethnic Group 4 | 1.05 | 0.99–1.11 | 0.74 | 0.70–0.80 |
| Unknown 5 | 1.40 | 1.33–1.48 | 0.81 | 0.75–0.86 |
| Rural/Urban Residence | ||||
| Rural Village, Hamlet, and Isolated Dwellings | 0.90 | 0.86–0.94 | 1.27 | 1.21–1.33 |
| Rural Town and Fringe | 0.94 | 0.91–0.98 | 1.29 | 1.24–1.35 |
| Urban City and Town | 0.97 | 0.95–1.00 | 1.33 | 1.29–1.36 |
| Extensive Urban Area | 1.00 | - | 1.00 | - |
| Government Region | ||||
| North West | 1.00 | - | - | - |
| North East | 1.04 | 1.00–1.09 | - | - |
| West Midlands | 1.10 | 1.05–1.14 | - | - |
| Yorkshire and the Humber | 1.13 | 1.09–1.17 | - | - |
| East Midlands | 1.13 | 1.08–1.18 | - | - |
| East of England | 1.06 | 1.02–1.10 | - | - |
| South East | 1.06 | 1.02–1.10 | - | - |
| South West | 1.07 | 1.03–1.12 | - | - |
| London | 1.27 | 1.22–1.32 | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Norris, R.P.; Fuller, E.; Greystoke, A.; Todd, A.; Sharp, L. Routes to Diagnosis in Lung Cancer—Do Socio-Demographics Matter? An English Population-Based Study. Cancers 2025, 17, 1874. https://doi.org/10.3390/cancers17111874
Norris RP, Fuller E, Greystoke A, Todd A, Sharp L. Routes to Diagnosis in Lung Cancer—Do Socio-Demographics Matter? An English Population-Based Study. Cancers. 2025; 17(11):1874. https://doi.org/10.3390/cancers17111874
Chicago/Turabian StyleNorris, Ruth P., Elizabeth Fuller, Alastair Greystoke, Adam Todd, and Linda Sharp. 2025. "Routes to Diagnosis in Lung Cancer—Do Socio-Demographics Matter? An English Population-Based Study" Cancers 17, no. 11: 1874. https://doi.org/10.3390/cancers17111874
APA StyleNorris, R. P., Fuller, E., Greystoke, A., Todd, A., & Sharp, L. (2025). Routes to Diagnosis in Lung Cancer—Do Socio-Demographics Matter? An English Population-Based Study. Cancers, 17(11), 1874. https://doi.org/10.3390/cancers17111874