
Chronic Lymphocytic Leukemia Care and Beyond: Navigating the Needs of Long-Term Survivors



{kind=link}
{kind=link}
Simple Summary
Abstract
1. Introduction
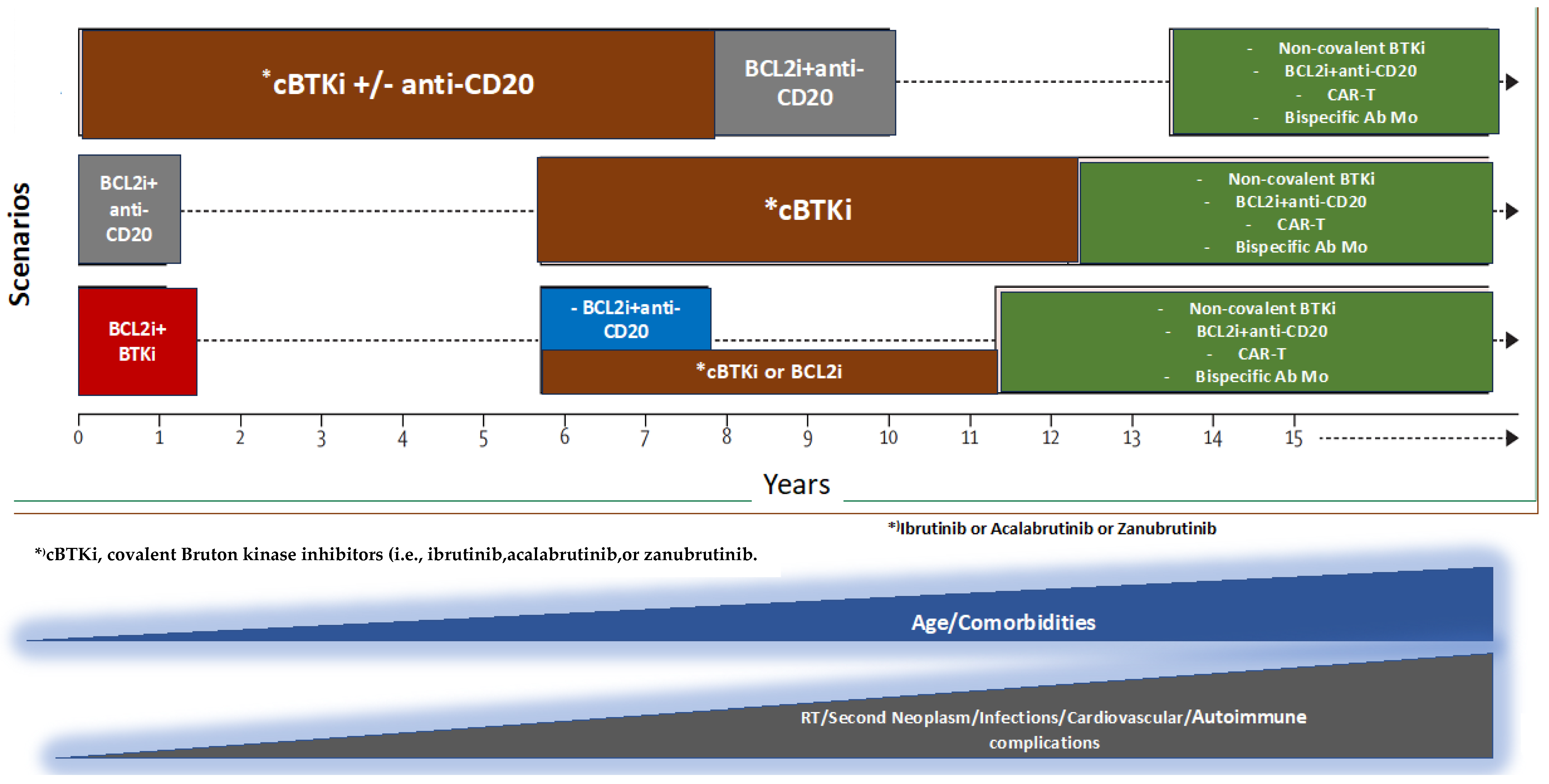
2. The Changing Treatment Landscape of CLL: A Success Story
3. Challenges Faced by Long-Term CLL Survivors
4. The Management of CLL-Related Immune Dysfunction
5. The Cardiovascular Complications of BTKis: Risks and Management
6. Second Primary Malignancies: Prevalence and Implications for Screening and Long-Term Care
7. Bone Health in CLL: Addressing Fracture Risk and the Potential of BTK Inhibitors
8. Managing Frailty in CLL
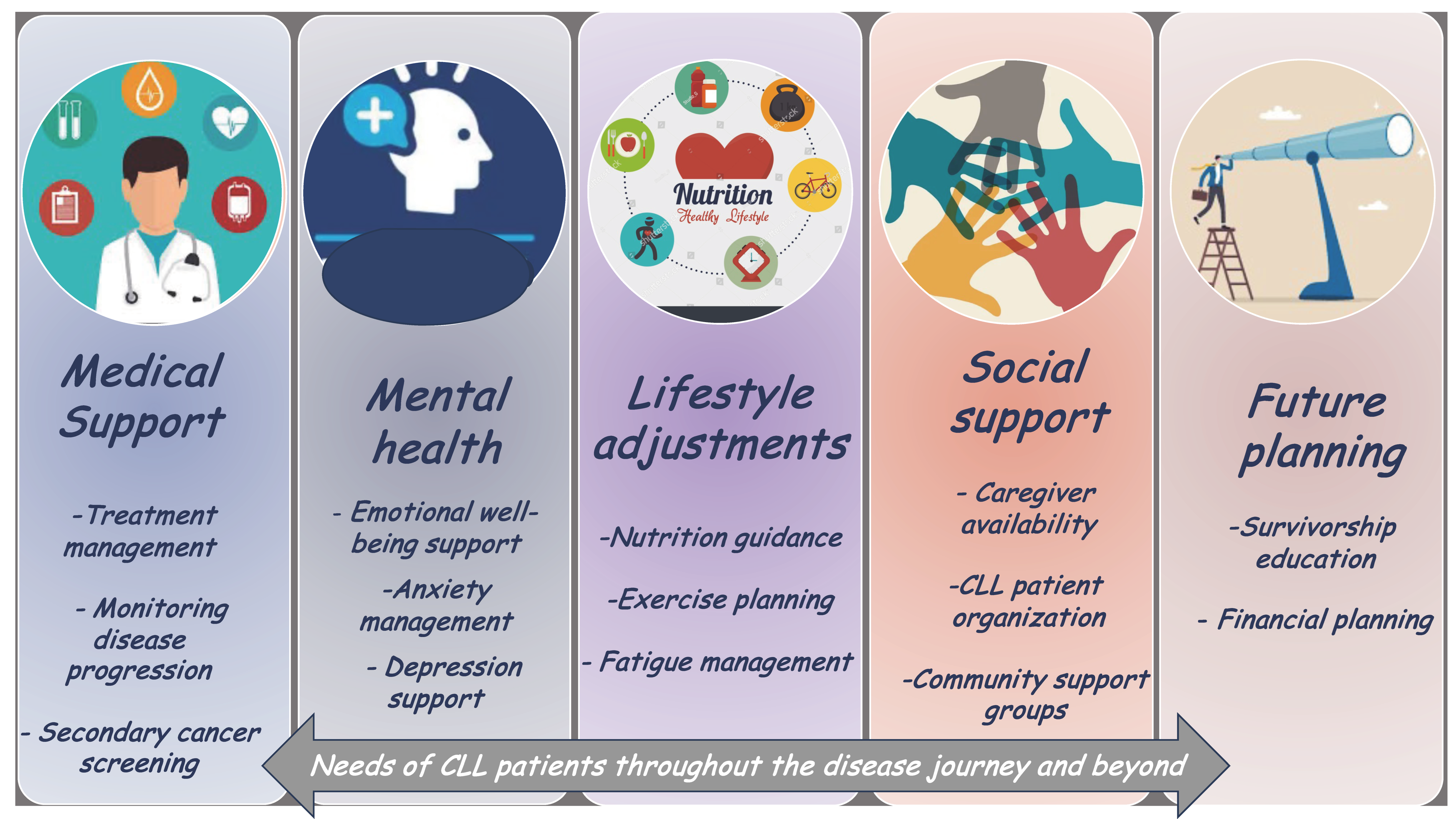
9. Enhancing the Quality of Life for CLL Patients
10. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- SEER*Explorer: An Interactive Website for SEER Cancer Statistics; Surveillance Research Program, National Cancer Institute: Bethesda, MD, USA, 2023. Available online: https://seer.cancer.gov/statistics-network/explorer/ (accessed on 30 December 2024).
- Jain, N.; Wierda, W.G.; O’Brien, S. Chronic lymphocytic leukaemia. Lancet 2024, 404, 694–706. [Google Scholar] [CrossRef]
- Hemminki, K.; Hemminki, J.; Försti, A.; Sud, A. Survival trends in hematological malignancies in the Nordic countries through 50 years. Blood Cancer J. 2022, 12, 150. [Google Scholar] [CrossRef]
- van der Straten, L.; Maas, C.C.H.M.; Levin, M.D.; Visser, O.; Posthuma, E.F.M.; Doorduijn, J.K.; Langerak, A.W.; Kater, A.P.; Dinmohamed, A.G. Long-term trends in the loss in expectation of life after a diagnosis of chronic lymphocytic leukemia: A population-based study in the Netherlands, 1989-2018. Blood Cancer J. 2022, 12, 72. [Google Scholar] [CrossRef] [PubMed]
- Kajüter, H.; Wellmann, I.; Khil, L.; Jöckel, K.H.; Zhang, C.; Fink, A.M.; Hallek, M.; Stang, A. Survival of patients with chronic lymphocytic leukemia before and after the introduction of chemoimmunotherapy in Germany. Blood Cancer J. 2021, 11, 174. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Achenbach, S.J.; Rabe, K.G.; Shanafelt, T.D.; Call, T.G.; Ding, W.; Kenderian, S.S.; Muchtar, E.; Leis, J.F.; Koehler, A.B.; et al. Cause of death in patients with newly diagnosed chronic lymphocytic leukemia (CLL) stratified by the CLL-International Prognostic Index. Blood Cancer J. 2021, 11, 140. [Google Scholar] [CrossRef]
- Fedele, P.L.; Opat, S. Chronic Lymphocytic Leukemia: Time to Care for the Survivors. J. Clin. Oncol. 2024, 42, 2005–2011. [Google Scholar] [CrossRef]
- Catovsky, D.; Richards, S.; Matutes, E.; Oscier, D.; Dyer, M.; Bezares, R.F.; Pettitt, A.R.; Hamblin, T.; Milligan, D.W.; Child, J.A.; et al. Assessment of fludarabine plus cyclophosphamide for patients with chronic lymphocytic leukaemia (the LRF CLL4 Trial): A randomised controlled trial. Lancet 2007, 370, 230–239. [Google Scholar] [CrossRef] [PubMed]
- Eichhorst, B.F.; Busch, R.; Hopfinger, G.; Pasold, R.; Hensel, M.; Steinbrecher, C.; Siehl, S.; Jäger, U.; Bergmann, M.; Stilgenbauer, S.; et al. Fludarabine plus cyclophosphamide versus fludarabine alone in first-line therapy of younger patients with chronic lymphocytic leukemia. Blood 2006, 107, 885–891. [Google Scholar] [CrossRef]
- Flinn, I.W.; Neuberg, D.S.; Grever, M.R.; Dewald, G.W.; Bennett, J.M.; Paietta, E.M.; Hussein, M.A.; Appelbaum, F.R.; Larson, R.A.; Moore, D.F., Jr.; et al. Phase III trial of fludarabine plus cyclophosphamide compared with fludarabine for patients with previously untreated chronic lymphocytic leukemia: US Intergroup Trial E2997. J. Clin. Oncol. 2007, 25, 793–798. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.; Bahlo, J.; Fink, A.M.; Goede, V.; Herling, C.D.; Cramer, P.; Langerbeins, P.; von Tresckow, J.; Engelke, A.; Maurer, C.; et al. Long-term remissions after FCR chemoimmunotherapy in previously untreated patients with CLL: Updated results of the CLL8 trial. Blood 2016, 127, 208–215. [Google Scholar] [CrossRef]
- Fischer, K.; Cramer, P.; Busch, R.; Böttcher, S.; Bahlo, J.; Schubert, J.; Pflüger, K.H.; Schott, S.; Goede, V.; Isfort, S.; et al. Bendamustine in combination with rituximab for previously untreated patients with chronic lymphocytic leukemia: A multicenter phase II trial of the German Chronic Lymphocytic Leukemia Study Group. J. Clin. Oncol. 2012, 30, 3209–3216. [Google Scholar] [CrossRef] [PubMed]
- Goede, V.; Fischer, K.; Busch, R.; Engelke, A.; Eichhorst, B.; Wendtner, C.M.; Chagorova, T.; de la Serna, J.; Dilhuydy, M.S.; Illmer, T.; et al. Obinutuzumab plus chlorambucil in patients with CLL and coexisting conditions. N. Engl. J. Med. 2014, 370, 1101–1110. [Google Scholar] [CrossRef] [PubMed]
- Hallek, M.; Fischer, K.; Fingerle-Rowson, G.; Fink, A.M.; Busch, R.; Mayer, J.; Hensel, M.; Hopfinger, G.; Hess, G.; von Grünhagen, U.; et al. Addition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: A randomised, open-label, phase 3 trial. Lancet 2010, 376, 1164–1174. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.A.; Bazinet, A.; Wierda, W.G.; Tam, C.S.; O’Brien, S.M.; Saha, S.; Peterson, C.B.; Plunkett, W.; Keating, M.J. Sustained remissions in CLL after frontline FCR treatment with very-long-term follow-up. Blood 2023, 142, 1784–1788. [Google Scholar] [CrossRef] [PubMed]
- Davids, M.S. Functional cure reported in CLL. Blood 2023, 142, 1761–1763. [Google Scholar] [CrossRef]
- Scarfò, L.; Chatzikonstantinou, T.; Rigolin, G.M.; Quaresmini, G.; Motta, M.; Vitale, C.; Garcia-Marco, J.A.; Hernández-Rivas, J.Á.; Mirás, F.; Baile, M.; et al. COVID-19 severity and mortality in patients with chronic lymphocytic leukemia: A joint study by ERIC, the European Research Initiative on CLL, and CLL Campus. Leukemia 2020, 34, 2354–2363. [Google Scholar] [CrossRef]
- Molica, S.; Tam, C.; Polliack, A. Current perspectives regarding SARS-CoV-2 vaccination in chronic lymphocytic leukemia. Hematol. Oncol. 2022, 40, 313–319. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Wang, X.V.; Hanson, C.A.; Paietta, E.M.; O’Brien, S.; Barrientos, J.; Jelinek, D.F.; Braggio, E.; Leis, J.F.; Zhang, C.C.; et al. Long-term outcomes for ibrutinib-rituximab and chemoimmunotherapy in CLL: Updated results of the E1912 trial. Blood 2022, 140, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Eichhorst, B.; Niemann, C.U.; Kater, A.P.; Fürstenau, M.; von Tresckow, J.; Zhang, C.; Robrecht, S.; Gregor, M.; Juliusson, G.; Thornton, P.; et al. First-Line Venetoclax Combinations in Chronic Lymphocytic Leukemia. N. Engl. J. Med. 2023, 388, 1739–1754. [Google Scholar] [CrossRef]
- Eichhorst, B.; Ghia, P.; Niemann, C.U.; Kater, A.P.; Gregor, M.; Hallek, M.; Jerkeman, M.; Buske, C.; ESMO Guidelines Committee. ESMO Clinical Practice Guideline interim update on new targeted therapies in the first line and at relapse of chronic lymphocytic leukaemia. Ann. Oncol. 2024, 35, 762–768. [Google Scholar] [CrossRef]
- Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Version 1.2025—October 1, 2024 Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. Available online: https://www.nccn.org/professionals/physician_gls/pdf/cll.pdf (accessed on 30 December 2024).
- Burger, J.A.; Tedeschi, A.; Barr, P.M.; Robak, T.; Owen, C.; Ghia, P.; Bairey, O.; Hillmen, P.; Bartlett, N.L.; Li, J.; et al. Ibrutinib as initial therapy for patients with chronic lymphocytic leukemia. N. Engl. J. Med. 2015, 373, 2425–2437. [Google Scholar] [CrossRef] [PubMed]
- Barr, P.M.; Owen, C.; Robak, T.; Tedeschi, A.; Bairey, O.; Burger, J.A.; Hillmen, P.; Coutre, S.E.; Dearden, C.; Grosicki, S.; et al. Up to 8-year follow-up from RESONATE-2: First-line ibrutinib treatment for patients with chronic lymphocytic leukemia. Blood Adv. 2022, 6, 3440–3450. [Google Scholar] [CrossRef] [PubMed]
- Moreno, C.; Greil, R.; Demirkan, F.; Tedeschi, A.; Anz, B.; Larratt, L.; Simkovic, M.; Samoilova, O.; Novak, J.; Ben-Yehuda, D.; et al. Ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab in firstline treatment of chronic lymphocytic leukaemia (iLLUMINATE): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2019, 20, 43–56. [Google Scholar] [CrossRef]
- Moreno, C.; Greil, R.; Demirkan, F.; Tedeschi, A.; Anz, B.; Larratt, L.; Simkovic, M.; Novak, J.; Strugov, V.; Gill, D.; et al. First-line treatment of chronic lymphocytic leukemia with ibrutinib plus obinutuzumab versus chlorambucil plus obinutuzumab: Final analysis of the randomized, phase III iLLUMINATE trial. Haematologica 2022, 107, 2108–2120. [Google Scholar] [CrossRef]
- Woyach, J.A.; Ruppert, A.S.; Heerema, N.A.; Zhao, W.; Booth, A.M.; Ding, W.; Bartlett, N.L.; Brander, D.M.; Barr, P.M.; Rogers, K.A.; et al. Ibrutinib regimens versu chemoimmunotherapy in older patients with untreated CLLN. Engl. J. Med. 2018, 379, 2517–2528. [Google Scholar] [CrossRef] [PubMed]
- Woyach, J.A.; Perez Burbano, G.; Ruppert, A.S.; Miller, C.; Heerema, N.A.; Zhao, W.; Wall, A.; Ding, W.; Bartlett, N.L.; Brander, D.M.; et al. Long-term results of Alliance A041202 show continued advantage of ibrutinib-based regimens compared with bendamustine plus rituximab (BR) chemoimmunotherapy. Blood 2024, 143, 1616–1627. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Wang, X.V.; Kay, N.E.; Hanson, C.A.; O’Brien, S.; Barrientos, J.; Jelinek, D.F.; Braggio, E.; Leis, J.F.; Zhang, C.C.; et al. Ibrutinib-rituximab or chemoimmunotherapy for chronic lymphocytic leukemia. N. Engl. J. Med. 2019, 381, 432–443. [Google Scholar] [CrossRef] [PubMed]
- Sharman, J.P.; Egyed, M.; Jurczak, W.; Skarbnik, A.; Pagel, J.M.; Flinn, I.W.; Kamdar, M.; Munir, T.; Walewska, R.; Corbett, G.; et al. Acalabrutinib with or without obinutuzumab versus chlorambucil and obinutuzumab for treatment-naive chronic lymphocytic leukaemia (ELEVATE TN): A randomised, controlled, phase 3 trial. Lancet 2020, 395, 1278–1291. [Google Scholar] [CrossRef] [PubMed]
- Sharman, J.P.; Egyed, M.; Jurczak, W.; Skarbnik, I.; Patel, K.; Flinn, I.W.; Kamdar, M.; Munir, T.; Walewska, R.; Hughes, M.; et al. Acalabrutinib ± obinutuzumab vs obinutuzumab + chlorambucil in treatment-naïve chronic lymphocytic leukemia: 6-year follow-up of Elevate-TN. Blood 2023, 142 (Suppl. 1), 636. [Google Scholar] [CrossRef]
- Tam, C.S.; Brown, J.R.; Kahl, B.S.; Ghia, P.; Giannopoulos, K.; Jurczak, W.; Šimkovič, M.; Shadman, M.; Österborg, A.; Laurenti, L.; et al. Zanubrutinib versus bendamustine and rituximab in untreated chronic lymphocytic leukaemia and smalllymphocytic lymphoma (SEQUOIA): A randomised, controlled, phase 3 trial. Lancet Oncol. 2022, 23, 1031–1043. [Google Scholar] [CrossRef]
- Fischer, K.; Al-Sawaf, O.; Bahlo, J.; Fink, A.M.; Tandon, M.; Dixon, M.; Robrecht, S.; Warburton, S.; Humphrey, K.; Samoylova, O.; et al. Venetoclax and Obinutuzumab in patients with CLL and coexisting conditions. N. Engl. J. Med. 2019, 380, 2225–2236. [Google Scholar] [CrossRef] [PubMed]
- Munir, T.; Cairns, D.A.; Bloor, A.; Allsup, D.; Cwynarski, K.; Pettitt, A.; Paneesha, S.; Fox, C.P.; Eyre, T.A.; Forconi, F.; et al. Chronic lymphocytic leukemia therapy guided by measurable residual disease. N. Engl. J. Med. 2024, 390, 326–337. [Google Scholar] [CrossRef] [PubMed]
- Al-Sawaf, O.; Zhang, C.; Jin, H.Y.; Robrecht, S.; Choi, Y.; Balasubramanian, S.; Kotak, A.; Chang, Y.M.; Fink, A.M.; Tausch, E.; et al. Transcriptomic profiles and 5-year results from the randomized CLL14 study of venetoclax plus obinutuzumab versus chlorambucil plus obinutuzumab in chronic lymphocytic leukemia. Nat. Commun. 2023, 14, 2147–2156. [Google Scholar] [CrossRef]
- Burger, J.; Barr, P.; Robak, T.; Owen, C.; Tedeschi, A.; Sarma, A.; Patten, P.E.M.; Grosicki, S.; McCarthy, H.; Offner, F.; et al. Final Analysis of the RESONATE-2 Study: Up to 10 Years of Follow-Up of First-Line Ibrutinib Treatment in Patients With Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. Clin. Lymphoma Myeloma Leuk. Vol. 2024, 24 (Suppl. 1), S1–S678. [Google Scholar]
- Ghia, P.; Owen, C.; Allan, J.N.; Barrientos, J.C.; Barr, P.M.; Shi, C.; Szoke, A.; Abbazio, C.; Krigsfeld, G.S.; Burger, J.A. First-line ibrutinib treatment in patients with chronic lymphocytic leukemia is associated with overall survival rates similar to those of an age-matched general population: A pooled post hoc analysis. Hemasphere 2024, 8, e74. [Google Scholar] [CrossRef] [PubMed]
- Molica, S.; Shanafelt, T.; Allsup, D.; Giannarelli, D. Impact of targeted agents on survival of CLL patients age > 65 relative to age and sex matched population. Am. J. Hematol. 2023, 99, 480–483. [Google Scholar] [CrossRef] [PubMed]
- Forconi, F.; Moss, P. Perturbation of the normal immune system in patients with CLL. Blood 2015, 126, 573–581. [Google Scholar] [CrossRef]
- Moreira, J.; Rabe, K.G.; Cerhan, J.R.; Kay, N.E.; Wilson, J.W.; Call, T.G.; Leis, J.F.; Jelinek, D.F.; Schwager, S.M.; Bowen, D.A.; et al. Infectious complications among individuals with clinical monoclonal B-cell lymphocytosis (MBL): A cohort study of newly diagnosed cases compared to controls. Leukemia 2013, 27, 136–141. [Google Scholar] [CrossRef]
- Galitzia, A.; Maccaferri, M.; Mauro, F.R.; Murru, R.; Marasca, R. Chronic Lymphocytic Leukemia: Management of Adverse Events in the Era of Targeted Agents. Cancers 2024, 16, 1996. [Google Scholar] [CrossRef]
- Vassilopoulos, S.; Shehadeh, F.; Kalligeros, M.; Tran, Q.L.; Schiffman, F.; Mylonakis, E. Targeted therapies in CLL/SLL and the cumulative incidence of infection: A systematic review and meta-analysis. Front. Pharmacol. 2022, 13, 989830. [Google Scholar] [CrossRef] [PubMed]
- Chong, E.A.; Kumashie, K.G.; Chong, E.R.; Fabrizio, J.; Gupta, A.; Svoboda, J.; Barta, S.K.; Walsh, K.M.; Napier, E.B.; Lundberg, R.K.; et al. Immunologic Predictors of Vaccine Responsiveness in Patients With Lymphoma and Chronic Lymphocytic Leukemia. J. Infect. Dis. 2024, 230, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Visentin, A.; Chatzikonstantinou, T.; Scarfò, L.; Kapetanakis, A.; Demosthenous, C.; Karakatsoulis, G.; Minga, E.; Chamou, D.; Allsup, D.; Cabrero, A.A.; et al. The evolving landscape of, COVID-19 and post-COVID condition in patients with chronic lymphocytic leukemia: A study by ERIC, the European research initiative on CLL. Am. J. Hematol. 2023, 98, 1856–1868. [Google Scholar] [CrossRef]
- Mikulska, M.; Cesaro, S.; de Lavallade, H.; Di Blasi, R.; Einarsdottir, S.; Gallo, G.; Rieger, C.; Engelhard, D.; Lehrnbecher, T.; Ljungman, P.; et al. Vaccination of patients with haematological malignancies who did not have transplantations: Guidelines from the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis. 2019, 19, e188–e199. [Google Scholar] [CrossRef] [PubMed]
- Tomasulo, E.; Paul, S.; Mu, R.; Tian, X.; Chen, J.; Pleyer, C.; Wiestner, A.; Sun, C. Interruption of BTK inhibitor improves response to SARS-CoV-2 booster vaccination in patients with, CLL. Leuk. Lymphoma 2023, 64, 2306–2315. [Google Scholar] [CrossRef] [PubMed]
- Solman, I.G.; Blum, L.K.; Hoh, H.Y.; Kipps, T.J.; Burger, J.A.; Barrientos, J.C.; O’Brien, S.; Mulligan, S.P.; Kay, N.E.; Hillmen, P.; et al. Ibrutinib restores immune cell numbers and function in first-line and relapsed/refractory chronic lymphocytic leukemia. Leuk. Res. 2020, 97, 106432. [Google Scholar] [CrossRef]
- Moreno, C.; Solman, I.G.; Tam, C.S.; Grigg, A.; Scarfò, L.; Kipps, T.J.; Srinivasan, S.; Mali, R.S.; Zhou, C.; Dean, J.P.; et al. Immune restoration with ibrutinib plus venetoclax in first-line chronic lymphocytic leukemia: The phase 2 CAPTIVATE study. Blood Adv. 2023, 7, 5294–5303. [Google Scholar] [CrossRef]
- Parikh, S.A.; Leis, J.F.; Chaffee, K.G.; Call, T.G.; Hanson, C.A.; Ding, W.; Chanan-Khan, A.A.; Bowen, D.; Conte, M.; Schwager, S.; et al. Hypogammaglobulinemia in newly diagnosed chronic lymphocytic leukemia: Natural history, clinical correlates, and outcomes. Cancer 2015, 121, 2883–2891. [Google Scholar] [CrossRef]
- Khan, S.; Allsup, D.; Molica, S. An updated perspective on immunoglobulin replacement in chronic lymphocytic leukaemia in the era of targeted therapies. Front. Oncol. 2023, 13, 1135812. [Google Scholar] [CrossRef] [PubMed]
- Chai, K.L.; Wong, J.; Weinkove, R.; Keegan, A.; Crispin, P.; Stanworth, S.; Morrissey, C.O.; Wood, E.M.; McQuilten, Z.K. Interventions to reduce infections in patients with hematological malignancies: A systematic review and meta-analysis. Blood Adv. 2023, 7, 20–31. [Google Scholar] [CrossRef]
- Larsson, K.; Mattsson, M.; Ebrahim, F.; Glimelius, I.; Höglund, M. High prevalence and incidence of cardiovascular disease in chronic lymphocytic leukaemia: A nationwide population-based study. Br. J. Haematol. 2020, 190, e245–e248. [Google Scholar] [CrossRef] [PubMed]
- Larsson, K.; Söderling, J.; Höglund, M.; Glimelius, I.; Mattsson, M. Cardiovascular disease in patients with chronic lymphocytic leukemia: A Swedish nationwide register study with matched comparators. Am. J. Hematol. 2022, 97, E255–E257. [Google Scholar] [CrossRef]
- Dickerson, T.; Wiczer, T.; Waller, A.; Philippon, J.; Porter, K.; Haddad, D.; Guha, A.; Rogers, K.A.; Bhat, S.; Byrd, J.C.; et al. Hypertension and incident cardiovascular events following ibrutinib initiation. Blood 2019, 134, 1919–1928. [Google Scholar] [CrossRef] [PubMed]
- Fernandez Turizo, M.J.; Kim, E.; Zhang, C.; Yankama, T.; Von Keudell, G.; Sermer, D.J.; Mejías-De Jesús, C.; Asnani, A. Pre-existing cardiovascular disease is associated with an increased risk of cardiovascular events during Bruton tyrosine kinase inhibitor therapy. Oncologist 2024, oyae229, Online ahead of print. [Google Scholar] [CrossRef]
- Brown, J.R.; Moslehi, J.; O’Brien, S.; Ghia, P.; Hillmen, P.; Cymbalista, F.; Shanafelt, T.D.; Fraser, G.; Rule, S.; Kipps, T.J.; et al. Characterization of atrial fibrillation adverse events reported in ibrutinib randomized controlled registration trials. Haematologica 2017, 102, 1796–1805. [Google Scholar] [CrossRef] [PubMed]
- Diamond, A.; Bensken, W.P.; Vu, L.; Dong, W.; Koroukian, S.M.; Caimi, P. Ibrutinib Is Associated With Increased Cardiovascular Events and Major Bleeding in Older CLL Patients. JACC CardioOncol. 2023, 5, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Byrd, J.C.; Hillmen, P.; Ghia, P.; Kater, A.P.; Chanan-Khan, A.; Furman, R.R.; O’Brien, S.; Yenerel, M.N.; Illés, A.; Kay, N.; et al. Acalabrutinib versus ibrutinib in previously treated chronic lymphocytic leukemia: Results of the first randomized phase III trial. J. Clin. Oncol. 2021, 39, 3441–3452. [Google Scholar] [CrossRef]
- Tam, C.S.; Opat, S.; D’Sa, S.; Jurczak, W.; Lee, H.P.; Cull, G.; Owen, R.G.; Marlton, P.; Wahlin, B.E.; Sanz, R.G.; et al. A randomized phase 3 trial of zanubrutinib vs ibrutinib in symptomatic Waldenström macroglobulinemia: The ASPEN study. Blood 2020, 136, 2038–2050. [Google Scholar] [CrossRef]
- Brown, J.R.; Eichhorst, B.; Hillmen, P.; Jurczak, W.; Kaźmierczak, M.; Lamanna, N.; O’Brien, S.M.; Tam, C.S.; Qiu, L.; Zhou, K.; et al. Zanubrutinib or ibrutinib in relapsed or refractory chronic lymphocytic leukemia. N. Engl. J. Med. 2023, 388, 319–332. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.R.; Eichhorst, B.; Lamanna, N.; O’Brien, S.M.; Tam, C.S.; Qiu, L.; Jurczak, W.; Zhou, K.; Šimkovič, M.; Mayer, J.; et al. Sustained Benefit of Zanubrutinib vs Ibrutinib in Patients With R/RCLL/SLL: Final Comparative Analysis of ALPINE. Blood 2024, 144, 2706–2717. [Google Scholar] [CrossRef] [PubMed]
- Lampson, B.L.; Yu, L.; Glynn, R.J.; Barrientos, J.C.; Jacobsen, E.D.; Banerji, V.; Jones, J.A.; Walewska, R.; Savage, K.J.; Michaud, G.F.; et al. Ventricular arrhythmias and sudden death in patients taking ibrutinib. Blood 2017, 129, 2581–2584. [Google Scholar] [CrossRef] [PubMed]
- Sharman, J.P.; Ghia, P.; Miranda, P.; Bajwa, N.; Rule, S.; Shaw, B.; Seymour, J.F. Analysis of ventricular arrhythmias and sudden death from prospective, randomized clinical trials of acalabrutinib. Br. J. Haematol. 2024, 205, 529–533. [Google Scholar] [CrossRef]
- Quartermaine, C.; Ghazi, S.M.; Yasin, A.; Awan, F.T.; Fradley, M.; Wiczer, T.; Kalathoor, S.; Ferdousi, M.; Krishan, S.; Habib, A.; et al. Cardiovascular Toxicities of BTK Inhibitors in Chronic Lymphocytic Leukemia: JACC: CardioOncology State-of-the-Art Review. JACC CardioOncol. 2023, 5, 570–590. [Google Scholar] [CrossRef]
- Abdel-Qadir, H.; Sabrie, N.; Leong, D.; Pang, A.; Austin, P.C.; Prica, A.; Nanthakumar, K.; Calvillo-Argüelles, O.; Lee, D.S.; Thavendiranathan, P. Cardiovascular risk associated with ibrutinib use in chronic lymphocytic leukemia: A population-based cohort study. J. Clin. Oncol. 2021, 39, 3453–3462. [Google Scholar] [CrossRef]
- Zheng, Y.; Guo, X.; Chen, C.; Chi, L.; Guo, Z.; Liang, J.; Wei, L.; Chen, X.; Ye, X.; He, J. Cardiovascular Toxicities of Ibrutinib: A Pharmacovigilance Study Based on the United States Food and Drug Administration Adverse Event Reporting System Database. Pharmaceuticals 2023, 16, 98. [Google Scholar] [CrossRef]
- Brown, J.R.; Byrd, J.C.; Ghia, P.; Sharman, J.P.; Hillmen, P.; Stephens, D.M.; Sun, C.; Jurczak, W.; Pagel, J.M.; Ferrajoli, A.; et al. Cardiovascular adverse events in patients with chronic lymphocytic leukemia receiving acalabrutinib monotherapy: Pooled analysis of 762 patients. Haematologica 2022, 107, 1335–1346. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Awan, F.T.; Addison, D.; Alfraih, F.; Baratta, S.J.; Campos, R.N.; Cugliari, M.S.; Goh, Y.T.; Ionin, V.A.; Mundnich, S.; Sverdlov, A.L.; et al. International consensus statement on the management of cardiovascular risk of Bruton’s tyrosine kinase inhibitors in CLL. Blood Adv. 2022, 6, 5516–5525. [Google Scholar] [CrossRef]
- AlAsmari, A.F.; Alghamdi, A.; Ali, N.; Almeaikl, M.A.; Hakami, H.M.; Alyousef, M.K.; AlSwayyed, M.; Alharbi, M.; Alqahtani, F.; Alasmari, F.; et al. Venetoclax Induces Cardiotoxicity through Modulation of Oxidative-Stress-Mediated Cardiac Inflammation and Apoptosis via NF-κB and BCL-2 Pathway. Int. J. Mol. Sci. 2022, 23, 6260. [Google Scholar] [CrossRef]
- Johnson, I.M.; Bezerra, E.D.; Farrukh, F.; McCullough, K.; Al-Kali, A.; Alkhateeb, H.B.; Begna, K.; Litzow, M.R.; Hogan, W.J.; Shah, M.V.; et al. Cardiac events in patients with acute myeloid leukemia treated with venetoclax in combination with hypomethylating agents. Blood Adv. 2022, 6, 5227–5231. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V.; Ailawadhi, S.; Bojanini, L.; Mehta, A.; Biswas, S.; Sher, T.; Roy, V.; Vishnu, P.; Marin-Acevedo, J.; Alegria, V.R.; et al. Trends in the risk of second primary malignancies among survivors of chronic lymphocytic leukemia. Blood Cancer J. 2019, 9, 75. [Google Scholar] [CrossRef]
- van der Straten, L.; Levin, M.D.; Dinnessen, M.A.W.; Visser, O.; Posthuma, E.F.M.; Doorduijn, J.K.; Langerak, A.W.; Kater, A.P.; Dinmohamed, A.G. Risk of second primary malignancies in patients with chronic lymphocytic leukemia: A population-based study in the Netherlands, 1989–2019. Blood Cancer J. 2023, 13, 15. [Google Scholar] [CrossRef] [PubMed]
- Chatzikonstantinou, T.; Scarfò, L.; Karakatsoulis, G.; Minga, E.; Chamou, D.; Iacoboni, G.; Kotaskova, J.; Demosthenous, C.; Smolej, L.; Mulligan, S.; et al. Other malignancies in the history of CLL: An international multicenter study conducted by ERIC, the European Research Initiative on CLL, in HARMONY. EClinicalMedicine 2023, 65, 102307. [Google Scholar] [CrossRef] [PubMed]
- Cramer, P.; Isfort, S.; Bahlo, J.; Stilgenbauer, S.; Döhner, H.; Bergmann, M.; Stauch, M.; Kneba, M.; Lange, E.; Langerbeins, P.; et al. Outcome of advanced chronic lymphocytic leukemia following different first-line and relapse therapies: A meta-analysis of five prospective trials by the German CLL Study Group (GCLLSG). Haematologica 2015, 100, 1451–1459. [Google Scholar] [CrossRef]
- Bond, D.A.; Huang, Y.; Fisher, J.L.; Ruppert, A.S.; Owen, D.H.; Bertino, E.M.; Rogers, K.A.; Bhat, S.A.; Grever, M.R.; Jaglowski, S.M.; et al. Second cancer incidence in CLL patients receiving BTK inhibitors. Leukemia 2020, 34, 3197–3205. [Google Scholar] [CrossRef]
- Falchi, L.; Vitale, C.; Keating, M.J.; Lerner, S.; Wang, X.; Elhor Gbito, K.Y.; Strom, S.; Wierda, W.G.; Ferrajoli, A. Incidence and prognostic impact of other cancers in a population of long-term survivors of chronic lymphocytic leukemia. Ann. Oncol. 2016, 27, 1100–1106. [Google Scholar] [CrossRef]
- Olszewski, A.J.; Gutman, R.; Eaton, C.B. Increased risk of axial fractures in patients with untreated chronic lymphocytic leukemia: A population-based analysis. Haematologica 2016, 101, e488–e491. [Google Scholar] [CrossRef] [PubMed]
- Ferrajoli, A.; Keating, M.J.; Manshouri, T.; Giles, F.J.; Dey, A.; Estrov, Z.; Koller, C.A.; Kurzrock, R.; Thomas, D.A.; Faderl, S.; et al. The clinical significance of tumor necrosis factor-alpha plasma level in patients having chronic lymphocytic leukemia. Blood 2002, 100, 1215–1219. [Google Scholar] [CrossRef] [PubMed]
- Lai, R.; O’Brien, S.; Maushouri, T.; Rogers, A.; Kantarjian, H.; Keating, M.; Albitar, M. Prognostic value of plasma interleukin-6 levels in patients with chronic lymphocytic leukemia. Cancer 2002, 95, 1071–1075. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.J.; Dozmorov, I.; Li, W.; Yancopoulos, S.; Sison, C.; Centola, M.; Jain, P.; Allen, S.L.; Kolitz, J.E.; Rai, K.R.; et al. Identification of outcome-correlated cytokine clusters in chronic lymphocytic leukemia. Blood 2011, 118, 5201–5210. [Google Scholar] [CrossRef]
- Schmiedel, B.J.; Scheible, C.A.; Nuebling, T.; Kopp, H.G.; Wirths, S.; Azuma, M.; Schneider, P.; Jung, G.; Grosse-Hovest, L.; Salih, H.R. RANKL expression, function, and therapeutic targeting in multiple myeloma and chronic lymphocytic leukemia. Cancer Res. 2013, 73, 683–694. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; Drake, M.T.; Maurer, M.J.; Allmer, C.; Rabe, K.G.; Slager, S.L.; Weiner, G.J.; Call, T.G.; Link, B.K.; Zent, C.S.; et al. Vitamin D insufficiency and prognosis in chronic lymphocytic leukemia. Blood 2011, 117, 1492–1498. [Google Scholar] [CrossRef]
- Molica, S.; Digiesi, G.; Antenucci, A.; Levato, L.; Mirabelli, R.; Molica, M.; Gentile, M.; Giannarelli, D.; Sperduti, I.; Morabito, F.; et al. Vitamin D insufficiency predicts time to first treatment (TFT) in early chronic lymphocytic leukemia (CLL). Leuk. Res. 2012, 36, 443–447. [Google Scholar] [CrossRef]
- Jaksic, V.P.; SorićJelena, E.; Andric, A.; Iaksic, J.; Korunic, R.H.; Mitrovic, Z.; Jaksic, O. Vertebral fractures in patients with B-cell chronic lymphocytic leukemia before and after ibrutinib treatment. XX International workshop on chronic lymphocytic leukemia. Leuk. Lymphoma 2023, 64 (Suppl. 1), S101. [Google Scholar]
- Ariza, Y.; Murata, M.; Ueda, Y.; Yoshizawa, T. Bruton’s tyrosine kinase (Btk) inhibitor tirabrutinib suppresses osteoclastic bone resorption. Bone Rep. 2019, 10, 100201. [Google Scholar] [CrossRef]
- Pokhrel, N.K.; Kim, Y.G.; Kim, H.J.; Kim, H.J.; Lee, J.H.; Choi, S.Y.; Kwon, T.G.; Lee, H.J.; Kim, J.Y.; Lee, Y. A novel Bruton’s tyrosine kinase inhibitor, acalabrutinib, suppresses osteoclast differentiation and Porphyromonas gingivalis lipopolysaccharide-induced alveolar bone resorption. J. Periodontol. 2019, 90, 546–554. [Google Scholar] [CrossRef]
- Giannoni, P.; Marini, C.; Cutrona, G.; Sambuceti, G.M.; Fais, F.; de Totero, D. Unraveling the Bone Tissue Microenvironment in Chronic Lymphocytic Leukemia. Cancers 2023, 15, 5058. [Google Scholar] [CrossRef]
- Molica, S.; Brugiatelli, M.; Morabito, F.; Ferrara, F.; Iannitto, E.; Di Renzo, N.; Capalbo, S.; Musto, P.; Di Raimondo, F. Treatment of elderly patients with chronic lymphocytic leukemia: An unmet cinical need. Expert. Rev. Hematol. 2013, 6, 441–449. [Google Scholar] [CrossRef] [PubMed]
- Molica, S. Defining treatment success in chronic lymphocytic leukemia: Exploring surrogate markers, comorbidities, and patient-centered endpoints. Expert. Rev. Hematol. 2024, 17, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Goede, V. Frailty is also a target for targeted drugs in CLL. Blood 2023, 142, 1107–1108. [Google Scholar] [CrossRef] [PubMed]
- van der Straten, L.; Stege, C.A.M.; Kersting, S.; Nasserinejad, K.; Dubois, J.; Dobber, J.A.; Mellink, C.H.M.; van der Kevie-Kersemaekers, A.F.; Evers, L.M.; de Boer, F.; et al. Fixed-duration venetoclax plus obinutuzumab improves quality of life and geriatric impairments in FCR-unfit patients with CLL. Blood 2023, 142, 1131–1142. [Google Scholar] [PubMed]
- Martino, E.A.; Mauro, F.R.; Reda, G.; Laurenti, L.; Visentin, A.; Frustaci, A.; Vigna, E.; Pepe, S.; Catania, G.; Loseto, G.; et al. Ibrutinib as first line therapy in chronic lymphocytic leukemia patients over 80 years old: A retrospective real-life multicenter Italian cohort. Hematol. Oncol. 2024, 42, e3249. [Google Scholar] [CrossRef]
- Simon, F.; Ligtvoet, R.; Nösslinger, T.; Bohn, J.P.; Von Tresckow, J.; Liersch, R.; Gaska, T.; Jentsch-Ullrich, K.; Koenigsmann, M.; Wolff, T.; et al. Safety of acalabrutinib treatment in very old (≥80 y) and/or frail patients with chronic lymphocytic leukemia—interim safety analysis of the ongoing phase II CLL-Frail trial. Hematol. Oncol. 2023, 41 (Suppl. 1), 468–469; [Google Scholar] [CrossRef]
- González-Gascón-Y-Marín, I.; Ballesteros-Andrés, M.; Martínez-Flores, S.; Rodríguez-Vicente, A.E.; Pérez-Carretero, C.; Quijada-Álamo, M.; Rodríguez-Sánchez, A.; Hernández-Rivas, J.Á. The Five “Ws” of Frailty Assessment and Chronic Lymphocytic Leukemia: Who, What, Where, Why, and When. Cancers 2023, 15, 4391. [Google Scholar] [CrossRef] [PubMed]
- Crowder, S.L.; Hoogland, A.I.; Small, B.J.; Carpenter, K.M.; Fischer, S.M.; Li, D.; Kinney, A.Y.; Welniak, T.L.; Brownstein, N.; Reich, R.R.; et al. Associations among frailty and quality of life in older patients with cancer treated with chemotherapy. J. Geriatr. Oncol. 2022, 13, 1149–1155. [Google Scholar] [CrossRef]
- Johnson, P.C.; Woyach, J.A.; Ulrich, A.; Marcotte, V.; Nipp, R.D.; Lage, D.E.; Nelson, A.M.; Newcomb, R.A.; Rice, J.; Lavoie, M.W.; et al. Geriatric assessment measures are predictive of outcomes in chronic lymphocytic leukemia. J. Geriatr. Oncol. 2023, 14, 101538. [Google Scholar] [CrossRef] [PubMed]
- Soumerai, J.D.; Barrientos, J.C.; Ahn, I.E.; Coombs, C.C.; Gladstone, D.E.; Hoffmann, M.S.; Kittai, A.S.; Jacobs, R.W.; Lipsky, A.; Patel, K.; et al. Consensus Recommendations from the 2024 Lymphoma Research Foundation Workshop on Treatment Selection Sequencing in CLL or SLL. Blood Adv, 2024; bloodadvances.2024014474. [Google Scholar] [CrossRef]
- Molica, S.; Allsup, D.; Polliack, A.; Giannarelli, D. The net clinical benefit of targeted agents in the upfront treatment of elderly/unfit chronic lymphocytic leukemia patients: Results of network meta-analysis. Eur. J. Haematol. 2023, 110, 774–777. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Bowen, D.; Venkat, C.; Slager, S.L.; Zent, C.S.; Kay, N.E.; Reinalda, M.; Sloan, J.A.; Call, T.G. Quality of life in chronic lymphocytic leukemia: An international survey of 1482 patients. Br. J. Haematol. 2007, 139, 255–264. [Google Scholar] [CrossRef] [PubMed]
- Holzner, B.; Fischhofer, M.; Kemmler, G.; Kopp, M.; Sperner-Unterweger, B.; Krugmann, J.; Dirnhofer, S.; Greil, R. Quality of life of patients with chronic lymphocytic leukemia: Results of a longitudinal investigation over 1 yr. Eur. J. Haematol. 2004, 72, 381–389. [Google Scholar] [CrossRef]
- Waweru, C.; Kaur, S.; Sharma, S.; Mishra, N. Health-related quality of life and economic burden of chronic lymphocytic leukemia in the era of novel targeted agents. Curr. Med. Res. Opin. 2020, 36, 1481–1495. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.; Moghaddam, N.; Tickle, A. Examining anxiety and depression in haematology cancer patients in ongoing treatment and under watchful waiting: A systematic review and meta-analysis. Eur. J. Cancer Care 2022, 31, e13678. [Google Scholar] [CrossRef]
- Fifer, S.; Godsell, J.; Opat, S.; Hamad, N.; Lasica, M.; Forsyth, C.; Morand, L.; Smeaton, E.; Winton, S.; Puig, A.; et al. Understanding the experience, treatment preferences and goals of people living with chronic lymphocytic leukemia (CLL) in Australia. BMC Cancer 2024, 24, 831. [Google Scholar] [CrossRef] [PubMed]
- Deering, K.L.; Sundaram, M.; Harshaw, Q.; Trudeau, J.; Barrientos, J.C. Health-related quality of life and treatment satisfaction in Chronic Lymphocytic Leukemia (CLL) patients on ibrutinib compared to other CLL treatments in a real-world US cross sectional study. PLoS ONE 2022, 17, e0270291. [Google Scholar] [CrossRef] [PubMed]
- Tam, C.S.; Lamanna, N.; O’Brien, S.M.; Qiu, L.; Yang, K.; Barnes, G.; Wu, K.; Salmi, T.; Brown, J.R. Health-related quality of life outcomes associated with zanubrutinib versus ibrutinib monotherapy in patients with relapsed/refractory chronic lymphocytic leukemia and small lymphocytic lymphoma: Results from the ALPINE Trial. Curr. Med. Res. Opin. 2023, 39, 1497–1503. [Google Scholar] [CrossRef]
- Molica, S.; Bombaci, F.; Cuneo, A.; Gaidano, G.; Ghia, P.; Mauro, F.R.; Tedeschi, A.; Trentin, L.; Amadori, S.; Foà, R. Living with chronic lymphocytic leukemia (CLL): A quantitative cross-sectional study of italian patients’ experiences on behalf of ail (associazione italiana contro le leucemie-linfomi e mielomi). EPOSTER 2020, 4, EP1743. [Google Scholar]
- Molica, S.; Shanafelt, T.D.; Allsup, D.; Giannarelli, D. Impact of Targeted Agents on Survival of Chronic Lymphocytic Leukemia Patients Fit for Fludarabine, Cyclophosphamide, and Rituximab (FCR) Relative to Age- and Sex-Matched Population. Cancers 2024, 16, 1085. [Google Scholar] [CrossRef] [PubMed]
- Villavicencio, A.; Solans, M.; Zacarías-Pons, L.; Vidal, A.; Puigdemont, M.; Roncero, J.M.; Saez, M.; Marcos-Gragera, R. Comorbidities at Diagnosis, Survival, and Cause of Death in Patients with Chronic Lymphocytic Leukemia: A Population-Based Study. Int. J. Environ. Res. Public Health 2021, 18, 701. [Google Scholar] [CrossRef] [PubMed]
- Shanafelt, T.D.; Kay, N.E. Comprehensive management of the CLL patient: A holistic approach. Hematology Am. Soc. Hematol. Educ. Program. 2007, 2007, 324–331. [Google Scholar] [CrossRef]
- Scheffold, A.; Stilgenbauer, S. Revolution of Chronic Lymphocytic Leukemia Therapy: The Chemo-Free Treatment Paradigm. Curr. Oncol. Rep. 2020, 22, 16. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zanardo, E.; Lejeune, D.; De Nigris, E.; Sarpong, E.; Farooqui, M.; Laliberté, F. Treatment Patterns, Healthcare Resource Utilization, and Costs of Patients with Chronic Lymphocytic Leukemia or Small Lymphocytic Lymphoma in the US. Oncologist 2024, 29, e360–e371. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molica, S.; Allsup, D. Chronic Lymphocytic Leukemia Care and Beyond: Navigating the Needs of Long-Term Survivors. Cancers 2025, 17, 119. https://doi.org/10.3390/cancers17010119
Molica S, Allsup D. Chronic Lymphocytic Leukemia Care and Beyond: Navigating the Needs of Long-Term Survivors. Cancers. 2025; 17(1):119. https://doi.org/10.3390/cancers17010119
Chicago/Turabian StyleMolica, Stefano, and David Allsup. 2025. "Chronic Lymphocytic Leukemia Care and Beyond: Navigating the Needs of Long-Term Survivors" Cancers 17, no. 1: 119. https://doi.org/10.3390/cancers17010119
APA StyleMolica, S., & Allsup, D. (2025). Chronic Lymphocytic Leukemia Care and Beyond: Navigating the Needs of Long-Term Survivors. Cancers, 17(1), 119. https://doi.org/10.3390/cancers17010119