
Association between Head and Neck Cancer and Increased Risk of Ischemic Heart Disease: A Retrospective Cohort Study Using National Population Data


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Ethical Statement
2.2. Nationwide Population-Based Cohort Dataset
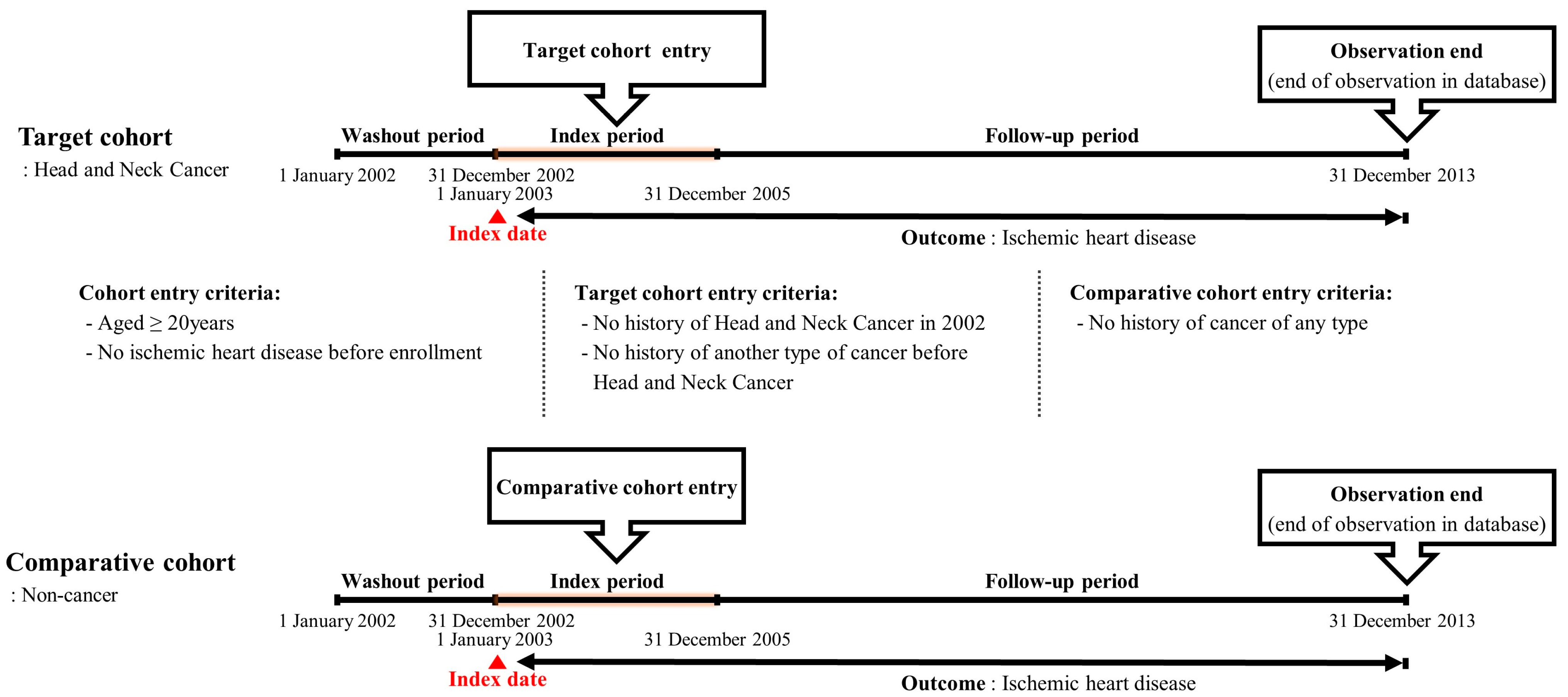
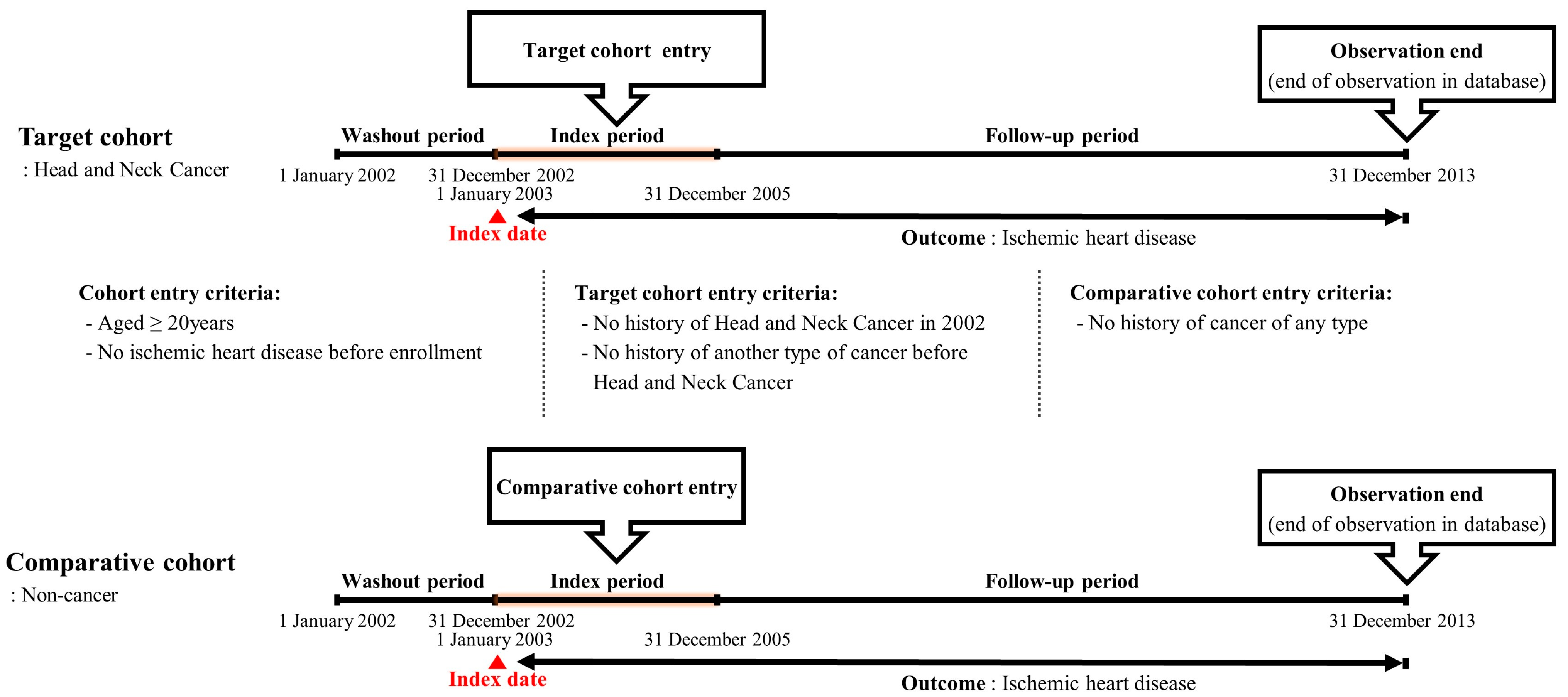
2.3. Study Design: A Retrospective Cohort Approach
2.4. Statistical Analysis
3. Results
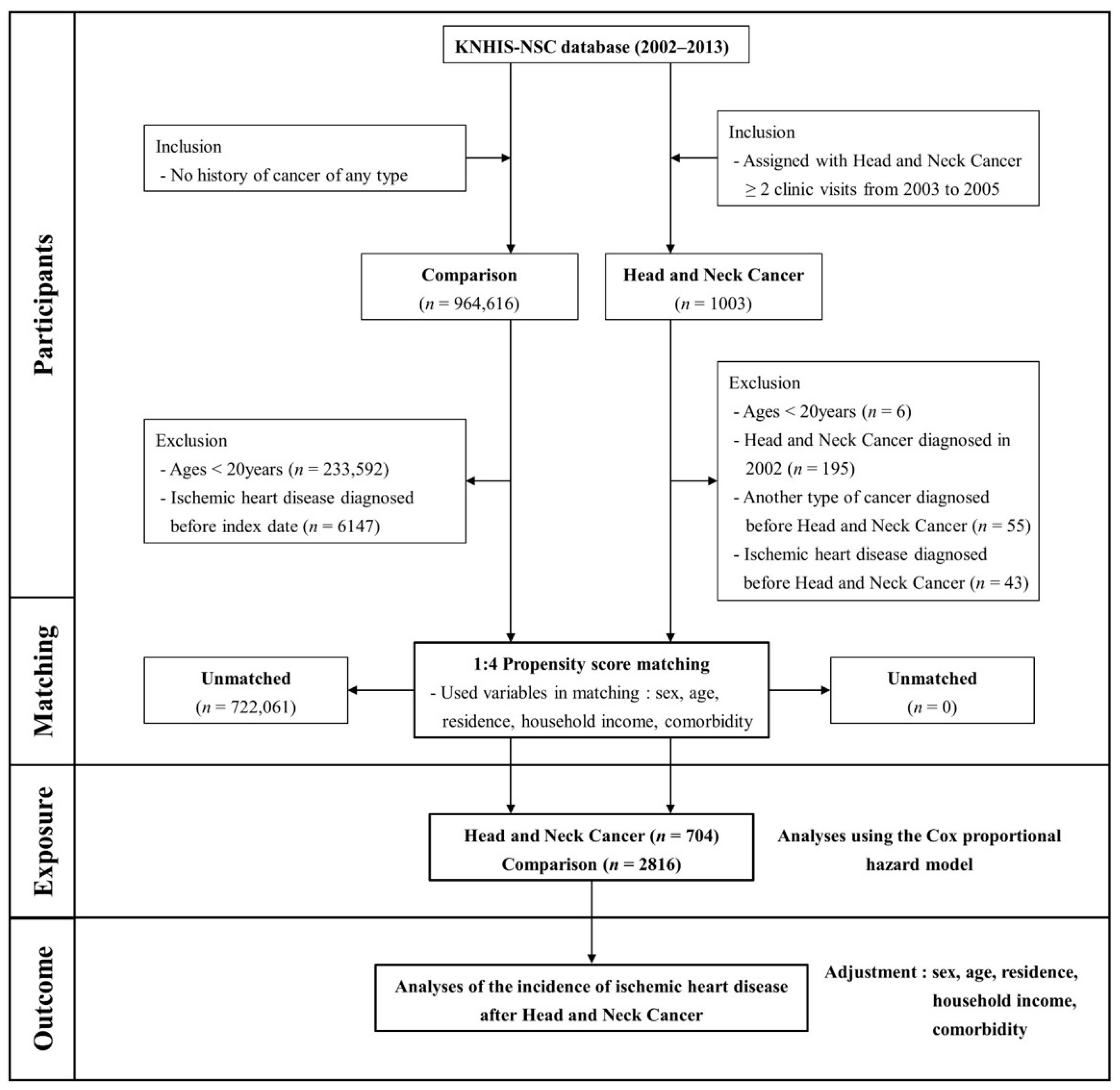
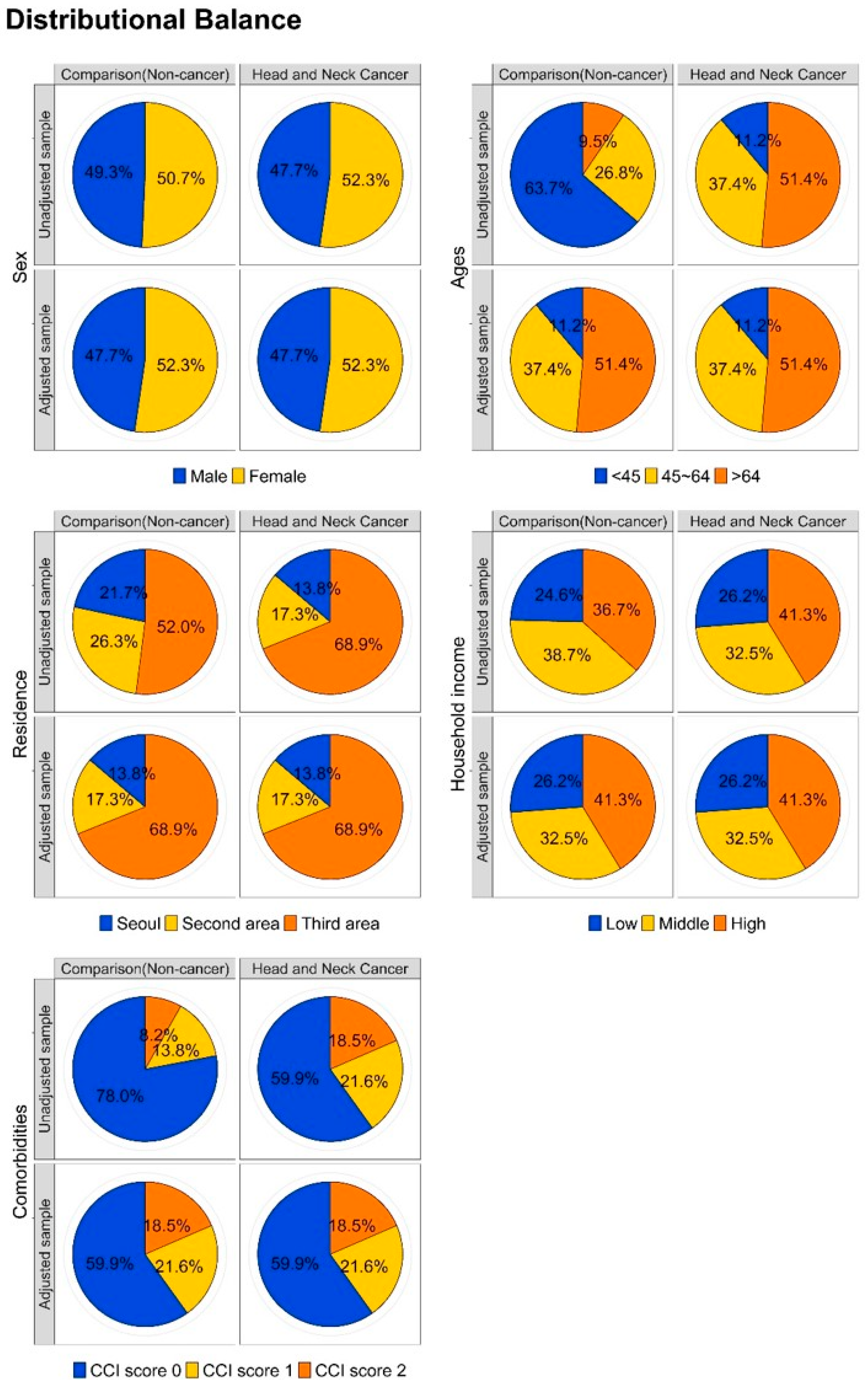
3.1. Comparing the Comparative and Target Cohorts
3.2. Effect of Head and Neck Cancer on Subsequent Ischemic Heart Disease Development
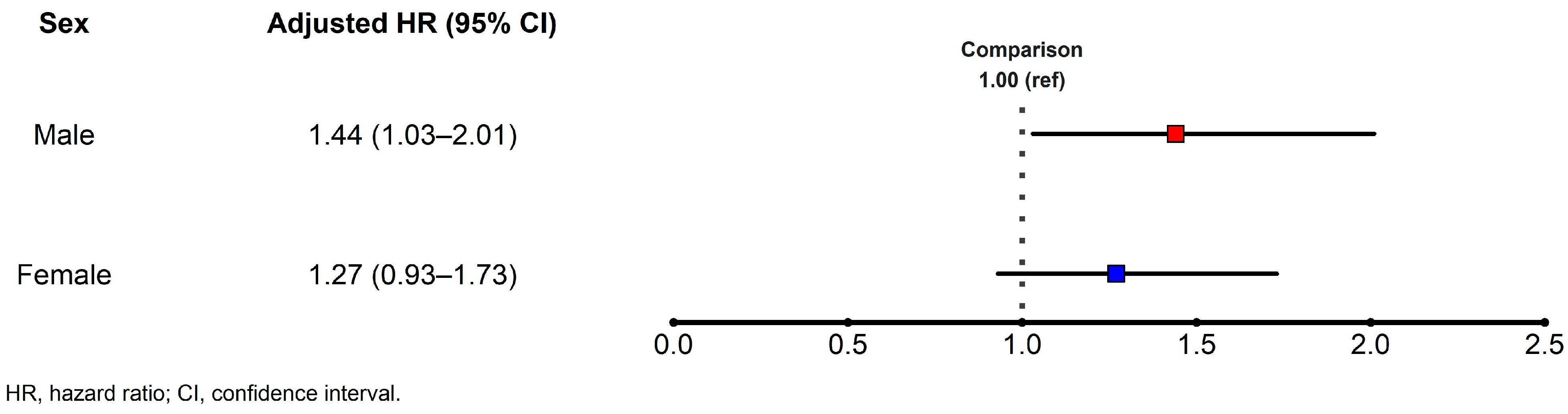
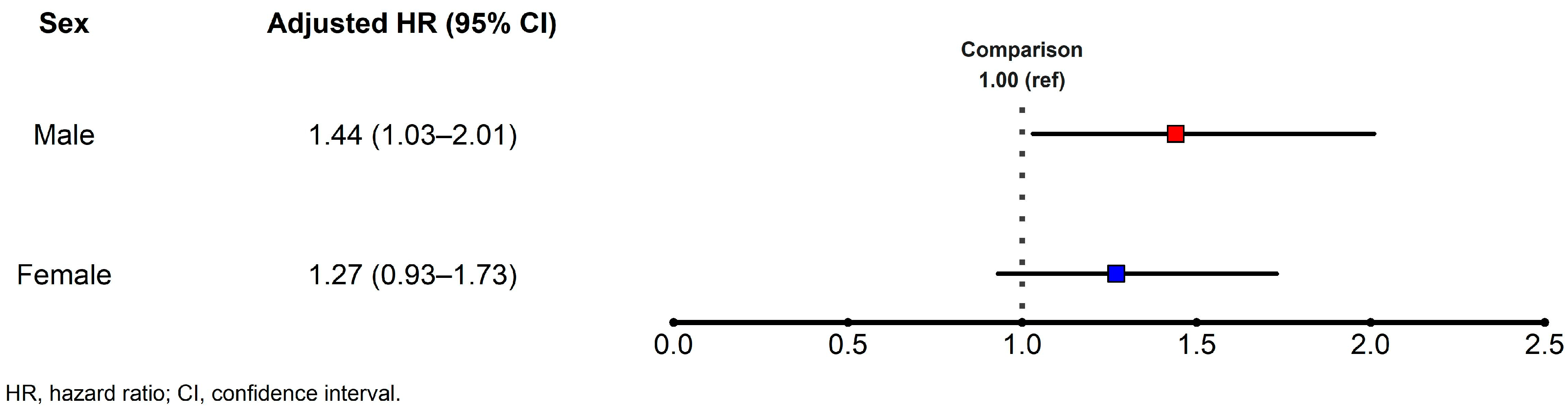
3.3. Risk of Ischemic Heart Disease Events in Various Subgroups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fidler, M.M.; Bray, F.; Soerjomataram, I. The global cancer burden and human development: A review. Scand J. Public Health 2018, 46, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Soerjomataram, I. The changing global burden of cancer: Transitions in human development and implications for cancer prevention and control. In Cancer: Disease Control Priorities, 3rd ed.; Gelband, H., Jha, P., Sankaranarayanan, R., Horton, S., Eds.; World Bank: Washington, DC, USA, 2015; Volume 3. [Google Scholar]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; He, F.; Hu, Y.; Wang, Q.; Wang, D.; Sha, Y.; Wu, J. Cancer incidence and mortality and risk factors in member countries of the ‘Belt and Road’ initiative. BMC Cancer 2022, 22, 582. [Google Scholar] [CrossRef] [PubMed]
- Pulumati, A.; Pulumati, A.; Dwarakanath, B.S.; Verma, A.; Papineni, R.V.L. Technological advancements in cancer diagnostics: Improvements and limitations. Cancer Rep. 2023, 6, e1764. [Google Scholar] [CrossRef] [PubMed]
- Debela, D.T.; Muzazu, S.G.; Heraro, K.D.; Ndalama, M.T.; Mesele, B.W.; Haile, D.C.; Kitui, S.K.; Manyazewal, T. New approaches and procedures for cancer treatment: Current perspectives. SAGE Open Med. 2021, 9, 20503121211034366. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.M.J.; Koyama, S.; Honigberg, M.C.; Surakka, I.; Haidermota, S.; Ganesh, S.; Patel, A.P.; Bhattacharya, R.; Lee, H.; Kim, H.C.; et al. Genetic, sociodemographic, lifestyle, and clinical risk factors of recurrent coronary artery disease events: A population-based cohort study. Eur. Heart J. 2023, 44, 3456–3465. [Google Scholar] [CrossRef] [PubMed]
- Armenian, S.H.; Armstrong, G.T.; Aune, G.; Chow, E.J.; Ehrhardt, M.J.; Ky, B.; Moslehi, J.; Mulrooney, D.A.; Nathan, P.C.; Ryan, T.D.; et al. Cardiovascular disease in survivors of childhood cancer: Insights into epidemiology, pathophysiology, and prevention. J. Clin. Oncol. 2018, 36, 2135–2144. [Google Scholar] [CrossRef] [PubMed]
- Carrillo-Estrada, M.; Bobrowski, D.; Carrasco, R.; Nadler, M.B.; Kalra, S.; Thavendiranathan, P.; Abdel-Qadir, H. Coronary artery disease in patients with cancer: Challenges and opportunities for improvement. Curr. Opin. Cardiol. 2021, 36, 597–608. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.; Loccoh, E.C.; Sanchez, R.; Ruz, P.; Anaba, U.; Williams, T.M.; Slivnick, J.; Vallakati, A.; Baliga, R.; Ayan, A.; et al. Contemporary understandings of cardiovascular disease after cancer radiotherapy: A focus on ischemic heart disease. Curr. Cardiol. Rep. 2020, 22, 151. [Google Scholar] [CrossRef]
- Murphy, A.C.; Koshy, A.N.; Yudi, M.B. Ischaemic heart disease and Cancer: Competing malignant conditions. BMC Cardiovasc. Disord. 2020, 20, 254. [Google Scholar] [CrossRef]
- Koene, R.J.; Prizment, A.E.; Blaes, A.; Konety, S.H. Shared risk factors in cardiovascular disease and cancer. Circulation 2016, 133, 1104–1114. [Google Scholar] [CrossRef]
- Berton, G.; Cordiano, R.; Cavuto, F.; Bagato, F.; Mahmoud, H.T.; Pasquinucci, M. Association between plasma lipid levels during acute coronary syndrome and long-term malignancy risk. The ABC-4* study on heart disease. BMC Cardiovasc. Disord. 2019, 19, 119. [Google Scholar] [CrossRef]
- Armstrong, G.T.; Oeffinger, K.C.; Chen, Y.; Kawashima, T.; Yasui, Y.; Leisenring, W.; Stovall, M.; Chow, E.J.; Sklar, C.A.; Mulrooney, D.A.; et al. Modifiable risk factors and major cardiac events among adult survivors of childhood cancer. J. Clin. Oncol. 2013, 31, 3673–3680. [Google Scholar] [CrossRef]
- Das, D.; Asher, A.; Ghosh, A.K. Cancer and coronary artery disease: Common associations, diagnosis and management challenges. Curr. Treat. Options Oncol. 2019, 20, 46. [Google Scholar] [CrossRef]
- Florido, R.; Daya, N.R.; Ndumele, C.E.; Koton, S.; Russell, S.D.; Prizment, A.; Blumenthal, R.S.; Matsushita, K.; Mok, Y.; Felix, A.S.; et al. Cardiovascular disease risk among cancer survivors: The atherosclerosis risk in communities (ARIC) study. J. Am. Coll. Cardiol. 2022, 80, 22–32. [Google Scholar] [CrossRef]
- Velusamy, R.; Nolan, M.; Murphy, A.; Thavendiranathan, P.; Marwick, T.H. Screening for coronary artery disease in cancer survivors: JACC: CardioOncology state-of-the-art review. JACC CardioOncol 2023, 5, 22–38. [Google Scholar] [CrossRef]
- Lenneman, C.G.; Sawyer, D.B. Cardio-oncology: An update on cardiotoxicity of cancer-related treatment. Circ. Res. 2016, 118, 1008–1020. [Google Scholar] [CrossRef]
- Barsouk, A.; Aluru, J.S.; Rawla, P.; Saginala, K.; Barsouk, A. Epidemiology, risk factors, and prevention of head and neck squamous cell carcinoma. Med. Sci. 2023, 11, 42. [Google Scholar] [CrossRef]
- Vigneswaran, N.; Williams, M.D. Epidemiologic trends in head and neck cancer and aids in diagnosis. Oral Maxillofac. Surg. Clin. N. Am. 2014, 26, 123–141. [Google Scholar] [CrossRef]
- Sun, L.; Brody, R.; Candelieri, D.; Lynch, J.A.; Cohen, R.B.; Li, Y.; Getz, K.D.; Ky, B. Risk of cardiovascular events among patients with head and neck cancer. JAMA Otolaryngol. Head Neck Surg. 2023, 149, 717–725. [Google Scholar] [CrossRef]
- Mukherjee, A.; Wiener, H.W.; Griffin, R.L.; Lenneman, C.; Chatterjee, A.; Nabell, L.M.; Lewis, C.E.; Shrestha, S. Traditional risk factors and cancer-related factors associated with cardiovascular disease risk in head and neck cancer patients. Front. Cardiovasc. Med. 2022, 9, 1024846. [Google Scholar] [CrossRef]
- Seong, S.C.; Kim, Y.Y.; Park, S.K.; Khang, Y.H.; Kim, H.C.; Park, J.H.; Kang, H.J.; Do, C.H.; Song, J.S.; Lee, E.J.; et al. Cohort profile: The National Health Insurance Service-National Health Screening Cohort (NHIS-HEALS) in Korea. BMJ Open 2017, 7, e016640. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.S.; Park, S.H.; Shin, S.A.; Kim, K. Cohort profile: The National Health Insurance Service-National Sample Cohort (NHIS-NSC), South Korea. Int. J. Epidemiol. 2017, 46, e15. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Gearing, R.E.; Mian, I.A.; Barber, J.; Ickowicz, A. A methodology for conducting retrospective chart review research in child and adolescent psychiatry. J. Can. Acad. Child. Adolesc. Psychiatry 2006, 15, 126–134. [Google Scholar]
- Oh, C.M.; Lee, D.; Kong, H.J.; Lee, S.; Won, Y.J.; Jung, K.W.; Cho, H. Causes of death among cancer patients in the era of cancer survivorship in Korea: Attention to the suicide and cardiovascular mortality. Cancer Med. 2020, 9, 1741–1752. [Google Scholar] [CrossRef]
- Addison, D.; Seidelmann, S.B.; Janjua, S.A.; Emami, H.; Staziaki, P.V.; Hallett, T.R.; Szilveszter, B.; Lu, M.T.; Cambria, R.P.; Hoffmann, U.; et al. Human papillomavirus status and the risk of cerebrovascular events following radiation therapy for head and neck cancer. J. Am. Heart Assoc. 2017, 6, e006453. [Google Scholar] [CrossRef]
- Lin, P.Y.; Cheng, P.C.; Hsu, W.L.; Lo, W.C.; Hsieh, C.H.; Shueng, P.W.; Liao, L.J. Risk of CVD following radiotherapy for head and neck cancer: An updated systematic review and meta-analysis. Front. Oncol. 2022, 12, 820808. [Google Scholar] [CrossRef]
- Mukherjee, A.; Wiener, H.W.; Griffin, R.L.; Lenneman, C.; Chatterjee, A.; Nabell, L.M.; Lewis, C.E.; Shrestha, S. Racial and rural-urban disparities in cardiovascular risk factors among patients with head and neck cancer in a clinical cohort. Head Neck 2022, 44, 1563–1575. [Google Scholar] [CrossRef]
- Lee, Y.A.; Li, S.; Chen, Y.; Li, Q.; Chen, C.; Hsu, W.; Lou, P.; Zhu, C.; Pan, J.; Shen, H.; et al. Tobacco smoking, alcohol drinking, betel quid chewing, and the risk of head and neck cancer in an East Asian population. Head Neck 2019, 41, 92–102. [Google Scholar] [CrossRef]
- Hashibe, M.; Brennan, P.; Chuang, S.-C.; Boccia, S.; Castellsague, X.; Chen, C.; Curado, M.P.; Maso, L.D.; Daudt, A.W.; Fabianova, E.; et al. Interaction between tobacco and alcohol use and the risk of head and neck cancer: Pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Cancer Epidemiol. Biomark. Prev. 2009, 18, 541–550. [Google Scholar] [CrossRef]
- Carton, M.; Barul, C.; Menvielle, G.; Cyr, D.; Sanchez, M.; Pilorget, C.; Trétarre, B.; Stücker, I.; Luce, D.; ICARE Study Group. Occupational exposure to solvents and risk of head and neck cancer in women: A population-based case-control study in France. BMJ Open 2017, 7, e012833. [Google Scholar] [CrossRef]
- Conway, D.; Hovanec, J.; Ahrens, W.; Ross, A.; Holcatova, I.; Lagiou, P.; Serraino, D.; Canova, C.; Richiardi, L.; Healy, C.; et al. Occupational socioeconomic risk associations for head and neck cancer in Europe and South America: Individual participant data analysis of pooled case-control studies within the INHANCE Consortium. J. Epidemiol. Community Health 2021, 75, 779–787. [Google Scholar] [CrossRef]
- Čonkaš, J.; Sabol, M.; Ozretić, P. “Toxic Masculinity”: What is known about the role of androgen receptors in head and neck squamous cell carcinoma. Int. J. Mol. Sci. 2023, 24, 3766. [Google Scholar] [CrossRef]
- Qin, C.; Lu, Y.; Zhang, H.; Zhang, Z.; Xu, W.; Wen, S.; Gao, W.; Wu, Y. Biological roles and clinical significance of estrogen and androgen receptors in head and neck cancers. J. Cancer 2022, 13, 2189–2199. [Google Scholar] [CrossRef]
- Radoï, L.; Paget-Bailly, S.; Cyr, D.; Papadopoulos, A.; Guida, F.; Schmaus, A.; Cénée, S.; Menvielle, G.; Carton, M.; Lapôtre-Ledoux, B.; et al. Tobacco smoking, alcohol drinking and risk of oral cavity cancer by subsite: Results of a French population-based case-control study, the ICARE study. Eur. J. Cancer Prev. 2013, 22, 268–276. [Google Scholar] [CrossRef]
- Binazzi, A.; Ferrante, P.; Marinaccio, A. Occupational exposure and sinonasal cancer: A systematic review and meta-analysis. BMC Cancer 2015, 15, 49. [Google Scholar] [CrossRef]
- Mannetje, A.T.; Kogevinas, M.; Luce, D.; Demers, P.A.; Bégin, D.; Bolm-Audorff, U.; Boffetta, P. Sinonasal cancer, occupation, and tobacco smoking in European women and men. Am. J. Ind. Med. 1999, 36, 101–107. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Comparative Cohort (n = 2816) | Target Cohort (n = 704) | p-Value |
|---|---|---|---|
| Sex | 1.000 | ||
| Male | 1344 (47.7%) | 336 (47.7%) | |
| Female | 1472 (52.3%) | 368 (52.3%) | |
| Ages (years) | 1.000 | ||
| <45 | 316 (11.2%) | 79 (11.2%) | |
| 45–64 | 1052 (37.4%) | 263 (37.4%) | |
| ≥64 | 1448 (51.4%) | 362 (51.4%) | |
| Residence | 1.000 | ||
| Seoul | 388 (13.8%) | 97 (13.8%) | |
| Second area | 488 (17.3%) | 122 (17.3%) | |
| Third area | 1940 (68.9%) | 485 (68.9%) | |
| Household income | 1.000 | ||
| Low (0–30%) | 736 (26.1%) | 184 (26.1%) | |
| Middle (30–70%) | 916 (32.5%) | 229 (32.5%) | |
| High (70–100%) | 1164 (41.3%) | 291 (41.3%) | |
| CCI | 1.000 | ||
| 0 | 1688 (59.9%) | 422 (59.9%) | |
| 1 | 608 (21.6%) | 152 (21.6%) | |
| ≥2 | 520 (18.5%) | 130 (18.5%) |
| Variables | N | Case | Median Follow-Up Period | Person Year | Incidence |
|---|---|---|---|---|---|
| Comparative cohort | 2816 | 349 | 8.997 years | 23,563.2 | 14.81 |
| Target cohort | 704 | 96 | 8.329 years | 4817.7 | 19.93 |
| HR (95%CI) | Model 1 | Model 2 | Model 3 | Model 4 |
|---|---|---|---|---|
| Comparative cohort | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) | 1.00 (ref) |
| Target cohort | 1.33 (1.06–1.67) | 1.34 (1.07–1.68) | 1.34 (1.07–1.68) | 1.33 (1.06–1.67) |
| Time (Year) | Ischemic Heart Disease | Ischemic Heart Disease |
|---|---|---|
| Model 1 (95% CI) | Model 4 (95% CI) | |
| 1 | 1.07 (0.61–1.90) | 1.08 (0.61–1.90) |
| 2 | 1.20 (0.79–1.83) | 1.21 (0.79–1.83) |
| 3 | 1.38 (0.97–1.96) | 1.38 (0.97–1.97) |
| 4 | 1.48 (1.10–2.01) | 1.49 (1.10–2.02) |
| 5 | 1.35 (1.01–1.81) | 1.36 (1.02–1.81) |
| 6 | 1.31 (1.00–1.72) | 1.32 (1.00–1.73) |
| 7 | 1.43 (1.11–1.84) | 1.44 (1.12–1.85) |
| 8 | 1.39 (1.09–1.77) | 1.39 (1.09–1.77) |
| 9 | 1.40 (1.11–1.77) | 1.40 (1.12–1.77) |
| 10 | 1.36 (1.08–1.70) | 1.36 (1.08–1.71) |
| 11 | 1.33 (1.06–1.67) | 1.33 (1.06–1.67) |
| Variables | N | Case | Person Year | Incidence Rate | Model 1 (95% CI) | Model 2 (95% CI) |
|---|---|---|---|---|---|---|
| Cancer type | ||||||
| Comparison | 2816 | 349 | 23,563.2 | 14.81 | 1.00 (ref) | 1.00 (ref) |
| Oral cavity | 495 | 76 | 3489.4 | 21.78 | 1.46 (1.14–1.87) | 1.40 (1.09–1.80) |
| Salivary gland | 23 | 3 | 144.8 | 20.71 | 1.37 (0.44–4.28) | 2.37 (0.75–7.48) |
| Oropharynx | 24 | 3 | 169.6 | 17.69 | 1.18 (0.38–3.69) | 1.29 (0.41–4.04) |
| Nasopharynx | 39 | 2 | 232.5 | 8.60 | 0.57 (0.14–2.29) | 0.71 (0.18–2.86) |
| Hypopharynx | 13 | 1 | 87.8 | 11.40 | 0.76 (0.11–5.43) | 0.66 (0.09–4.69) |
| Sinonasal tract | 16 | 3 | 91.8 | 32.69 | 2.16 (0.69–6.74) | 3.53 (1.12–11.13) |
| Larynx | 94 | 8 | 601.9 | 13.29 | 0.89 (0.44–1.79) | 0.89 (0.44–1.80) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, C.; Yu, H.; Kim, D.-K. Association between Head and Neck Cancer and Increased Risk of Ischemic Heart Disease: A Retrospective Cohort Study Using National Population Data. Cancers 2024, 16, 1352. https://doi.org/10.3390/cancers16071352
Kim C, Yu H, Kim D-K. Association between Head and Neck Cancer and Increased Risk of Ischemic Heart Disease: A Retrospective Cohort Study Using National Population Data. Cancers. 2024; 16(7):1352. https://doi.org/10.3390/cancers16071352
Chicago/Turabian StyleKim, Chulho, Hyunjae Yu, and Dong-Kyu Kim. 2024. "Association between Head and Neck Cancer and Increased Risk of Ischemic Heart Disease: A Retrospective Cohort Study Using National Population Data" Cancers 16, no. 7: 1352. https://doi.org/10.3390/cancers16071352
APA StyleKim, C., Yu, H., & Kim, D.-K. (2024). Association between Head and Neck Cancer and Increased Risk of Ischemic Heart Disease: A Retrospective Cohort Study Using National Population Data. Cancers, 16(7), 1352. https://doi.org/10.3390/cancers16071352