

Atypical Ductal Hyperplasia and Lobular In Situ Neoplasm: High-Risk Lesions Challenging Breast Cancer Prevention

 ,
,  , ,
, ,  , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bahl, M. Management of High-Risk Breast Lesions. Radiol. Clin. N. Am. 2021, 59, 29–40. [Google Scholar] [CrossRef] [PubMed]
- Bratthauer, G.L.; Tavassoli, F.A. Lobular intraepithelial neoplasia: Previously unexplored aspects assessed in 775 cases and their clinical implications. Virchows Arch. 2002, 440, 134–138. [Google Scholar] [CrossRef] [PubMed]
- Lee, A. Guidelines for Non-Operative Diagnostic Procedures and Reporting in Breast Cancer Screening. August 2021. Available online: https://www.rcpath.org/static/4b16f19c-f7bd-456c-b212f557f8040f66/G150-Non-op-reporting-breast-cancer-screening.pdf (accessed on 17 December 2020).
- Hartmann, L.C.; Degnim, A.C.; Santen, R.J.; Dupont, W.D.; Ghosh, K. Atypical hyperplasia of the breast–risk assessment and management options. N. Engl. J. Med. 2015, 372, 78–89. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, L.C.; Radisky, D.C.; Frost, M.H.; Santen, R.J.; Vierkant, R.A.; Benetti, L.L.; Tarabishy, Y.; Ghosh, K.; Visscher, D.W.; Degnim, A.C. Understanding the premalignant potential of atypical hyperplasia through its natural history: A longitudinal cohort study. Cancer Prev. Res. 2014, 7, 211–217. [Google Scholar] [CrossRef] [PubMed]
- Lewin, A.A.; Mercado, C.L. Atypical Ductal Hyperplasia and Lobular Neoplasia: Update and Easing of Guidelines. AJR Am. J. Roentgenol. 2020, 214, 265–275. [Google Scholar] [CrossRef] [PubMed]
- Brem, R.F.; Lechner, M.C.; Jackman, R.J.; Rapelyea, J.A.; Evans, W.P.; Philpotts, L.E.; Hargreaves, J.; Wasden, S. Lobular neoplasia at percutaneous breast biopsy: Variables associated with carcinoma at surgical excision. AJR Am. J. Roentgenol. 2008, 190, 637–641. [Google Scholar] [CrossRef]
- Gulla, S.; Lancaster, R.; De Los Santos, J. High-Risk Breast Lesions and Current Management. Semin. Roentgenol. 2018, 53, 252–260. [Google Scholar] [CrossRef]
- Rageth, C.J.; O’Flynn, E.A.; Comstock, C.; Kurtz, C.; Kubik, R.; Madjar, H.; Lepori, D.; Kampmann, G.; Mundinger, A.; Baege, A.; et al. First International Consensus Conference on lesions of uncertain malignant potential in the breast (B3 lesions). Breast Cancer Res. Treat. 2016, 159, 203–213. [Google Scholar] [CrossRef]
- Giannotti, E.; James, J.J.; Chen, Y.; Sun, R.; Karuppiah, A.; Yemm, J.; Lee, A.H.S. Effectiveness of percutaneous vacuum-assisted excision (VAE) of breast lesions of uncertain malignant potential (B3 lesions) as an alternative to open surgical biopsy. Eur. Radiol. 2021, 31, 9540–9547. [Google Scholar] [CrossRef]
- Rageth, C.J.; O’Flynn, E.A.M.; Pinker, K.; Kubik-Huch, R.A.; Mundinger, A.; Decker, T.; Tausch, C.; Dammann, F.; Baltzer, P.A.; Fallenberg, E.M.; et al. Second International Consensus Conference on lesions of uncertain malignant potential in the breast (B3 lesions). Breast Cancer Res. Treat. 2019, 174, 279–296. [Google Scholar] [CrossRef]
- Hoffmann, O.; Stamatis, G.A.; Bittner, A.K.; Arnold, G.; Schnabel, R.; Krüger, K.; Kimmig, R.; Heubner, M. B3-lesions of the breast and cancer risk—An analysis of mammography screening patients. Mol. Clin. Oncol. 2016, 4, 705–708. [Google Scholar] [CrossRef] [PubMed]
- Ellis, I.O.; Humphreys, S.; Michell, M.; Pinder, S.E.; Wells, C.A.; Zakhour, H.D.; UK National Coordinating Commmittee for Breast Screening Pathology; European Commission Working Group on Breast Screening Pathology. Best Practice No 179. Guidelines for breast needle core biopsy handling and reporting in breast screening assessment. J. Clin. Pathol. 2004, 57, 897–902. [Google Scholar] [CrossRef] [PubMed]
- Sharma, N.; Wilkinson, L.S.; Pinder, S.E. The B3 conundrum-the radiologists’ perspective. Br. J. Radiol. 2017, 90, 20160595. [Google Scholar] [CrossRef] [PubMed]
- McLachlan, C.; Jackson, M.; Valencia, A. Evaluating the use of vacuum-assisted excisions in the management of B3 breast lesions. Br. J. Radiol. 2023, 96, 20230528. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Fatah, T.M.; Powe, D.G.; Hodi, Z.; Lee, A.H.; Reis-Filho, J.S.; Ellis, I.O. High frequency of coexistence of columnar cell lesions, lobular neoplasia, and low grade ductal carcinoma in situ with invasive tubular carcinoma and invasive lobular carcinoma. Am. J. Surg. Pathol. 2007, 31, 417–426. [Google Scholar] [CrossRef] [PubMed]
- Ugurlu, M.U.; Yoldemir, T.; Gulluoglu, B.M. Assessment and management of B3 breast lesions with atypia: A focused review. Climacteric 2020, 23, 17–23. [Google Scholar] [CrossRef]
- Elfgen, C.; Leo, C.; Kubik-Huch, R.A.; Muenst, S.; Schmidt, N.; Quinn, C.; McNally, S.; van Diest, P.J.; Mann, R.M.; Bago-Horvath, Z.; et al. Third International Consensus Conference on lesions of uncertain malignant potential in the breast (B3 lesions). Virchows Arch. 2023, 483, 5–20. [Google Scholar] [CrossRef]
- Rageth, C.J.; Rubenov, R.; Bronz, C.; Dietrich, D.; Tausch, C.; Rodewald, A.K.; Varga, Z. Atypical ductal hyperplasia and the risk of underestimation: Tissue sampling method, multifocality, and associated calcification significantly influence the diagnostic upgrade rate based on subsequent surgical specimens. Breast Cancer 2019, 26, 452–458. [Google Scholar] [CrossRef]
- Tan, P.H.; Ellis, I.; Allison, K.; Brogi, E.; Fox, S.B.; Lakhani, S.; Lazar, A.J.; Morris, E.A.; Sahin, A.; Salgado, R.; et al. The 2019 WHO classification of tumours of the breast. Histopathology 2020, 77, 181–185. [Google Scholar] [CrossRef]
- Forester, N.D.; Lowes, S.; Mitchell, E.; Twiddy, M. High risk (B3) breast lesions: What is the incidence of malignan-cy for individual lesion subtypes? A systematic review and meta-analysis. Eur. J. Surg. Oncol. 2019, 45, 519–527. [Google Scholar] [CrossRef]
- Catanzariti, F.; Avendano, D.; Cicero, G.; Garza-Montemayor, M.; Sofia, C.; Venanzi Rullo, E.; Ascenti, G.; Pinker-Domenig, K.; Marino, M.A. High-risk lesions of the breast: Concurrent diagnostic tools and management recommendations. Insights Imaging 2021, 12, 63. [Google Scholar] [CrossRef] [PubMed]
- Brem, R.F. Management of Breast Atypical Ductal Hyperplasia: Now and the Future. Radiology 2020, 294, 87–88. [Google Scholar] [CrossRef] [PubMed]
- Page, D.L.; Dupont, W.D.; Rogers, L.W.; Rados, M.S. Atypical hyperplastic lesions of the female breast. A long-term follow-up study. Cancer 1985, 55, 2698–2708. [Google Scholar] [CrossRef] [PubMed]
- Tavassoli, F.A.; Norris, H.J. A comparison of the results of long-term follow-up for atypical intraductal hyper-plasia and intraductal hyperplasia of the breast. Cancer 1990, 65, 518–529. [Google Scholar] [CrossRef] [PubMed]
- Schiaffino, S.; Calabrese, M.; Melani, E.F.; Trimboli, R.M.; Cozzi, A.; Carbonaro, L.A.; Di Leo, G.; Sardanelli, F. Upgrade Rate of Percutaneously Diagnosed Pure Atypical Ductal Hyperplasia: Systematic Review and Meta-Analysis of 6458 Lesions. Radiology 2020, 294, 76–86. [Google Scholar] [CrossRef] [PubMed]
- Beute, B.J.; Kalisher, L.; Hutter, R.V. Lobular carcinoma in situ of the breast: Clinical, pathologic, and mammo-graphic features. AJR Am. J. Roentgenol. 1991, 157, 257–265. [Google Scholar] [CrossRef]
- Christgen, M.; Steinemann, D.; Kühnle, E.; Länger, F.; Gluz, O.; Harbeck, N.; Kreipe, H. Lobular breast cancer: Clinical, molecular and morphological characteristics. Pathol. Res. Pract. 2016, 212, 583–597. [Google Scholar] [CrossRef]
- Maxwell, A.J.; Clements, K.; Dodwell, D.J.; Evans, A.J.; Francis, A.; Hussain, M.; Morris, J.; Pinder, S.E.; Sawyer, E.J.; Thomas, J.; et al. The radiological features, diagnosis and management of screen-detected lobular neoplasia of the breast: Findings from the Sloane Project. Breast 2016, 27, 109–115. [Google Scholar] [CrossRef]
- Hussain, M.; Cunnick, G.H. Management of lobular carcinoma in-situ and atypical lobular hyperplasia of the breast—A review. Eur. J. Surg. Oncol. 2011, 37, 279–289. [Google Scholar] [CrossRef]
- Nicosia, L.; Latronico, A.; Addante, F.; De Santis, R.; Bozzini, A.C.; Montesano, M.; Frassoni, S.; Bagnardi, V.; Maz-zarol, G.; Pala, O.; et al. Atypical Ductal Hyperplasia after Vacuum-Assisted Breast Biopsy: Can We Reduce the Upgrade to Breast Cancer to an Acceptable Rate? Diagnostics 2021, 11, 1120. [Google Scholar] [CrossRef]
- Hennessy, G.; Boland, M.R.; Bambrick, M.; Crone, L.; Lloyd, A.; Abdelwahab, S.; Downey, E.; Staunton, M.; Hambly, N.; Mhuircheartaigh, N.N.; et al. Value of Long-Term Follow-up in Surgically Excised Lesions of Uncertain Malignant Potential in the Breast—Is 5 Years Necessary? Clin. Breast Cancer 2022, 22, 699–704. [Google Scholar] [CrossRef]
- Bellini, C.; Nori Cucchiari, J.; Di Naro, F.; De Benedetto, D.; Bicchierai, G.; Franconeri, A.; Renda, I.; Bianchi, S.; Susini, T. Breast Lesions of Uncertain Malignant Potential (B3) and the Risk of Breast Cancer Development: A Long-Term Follow-Up Study. Cancers 2023, 15, 3521. [Google Scholar] [CrossRef]
- Rahman, W.T.; Helvie, M.A. Breast Cancer Screening in Average and High-Risk Women. Best Pract. Res. Clin. Obstet. Gynaecol. 2022, 83, 3–14. [Google Scholar] [CrossRef]
- Mann, R.M.; Balleyguier, C.; Baltzer, P.A.; Bick, U.; Colin, C.; Cornford, E.; Evans, A.; Fallenberg, E.; Forrai, G.; Fuchsjäger, M.H.; et al. Breast MRI: EUSOBI Recommendations for Women’s Information. Eur. Radiol. 2015, 25, 3669–3678. [Google Scholar] [CrossRef]
- Bianchi, S.; Bendinelli, B.; Saladino, V.; Vezzosi, V.; Brancato, B.; Nori, J.; Palli, D. Non-Malignant Breast Papillary Lesions—B3 Diagnosed on Ultrasound—Guided 14-Gauge Needle Core Biopsy: Analysis of 114 Cases from a Single Institution and Review of the Literature. Pathol. Oncol. Res. 2015, 21, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Girardi, V.; Guaragni, M.; Ruzzenenti, N.; Palmieri, F.; Fogazzi, G.; Cozzi, A.; Lucchini, D.; Buffoli, A.; Schiaffino, S.; Sardanelli, F. B3 Lesions at Vacuum-Assisted Breast Biopsy under Ultrasound or Mammography Guidance: A Single-Center Experience on 3634 Consecutive Biopsies. Cancers 2021, 13, 5443. [Google Scholar] [CrossRef] [PubMed]
- Pashayan, N.; Antoniou, A.C.; Lee, A.; Wolfson, M.; Chiquette, J.; Eloy, L.; Eisen, A.; Stockley, T.L.; Nabi, H.; Brooks, J.D.; et al. Should Age-Dependent Absolute Risk Thresholds Be Used for Risk Stratification in Risk-Stratified Breast Cancer Screening? J. Pers. Med. 2021, 11, 916. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | Level | ADH (n = 120) | LIN 1/2 (n = 126) | p-Value |
|---|---|---|---|---|
| Age at VABB, median (min–max) | 52 (31–78) | 49 (37–70) | 0.056 | |
| Dimension of lesion, median (min–max) | 15 (5–100) | 13 (3–80) | 0.17 | |
| Missing | 0 | 21 | ||
| Disease-only specimen with micro, n (%) | No | 50 (51.5) | 86 (81.9) | <0.001 |
| Yes | 47 (48.5) | 19 (18.1) | ||
| Missing | 23 | 21 |
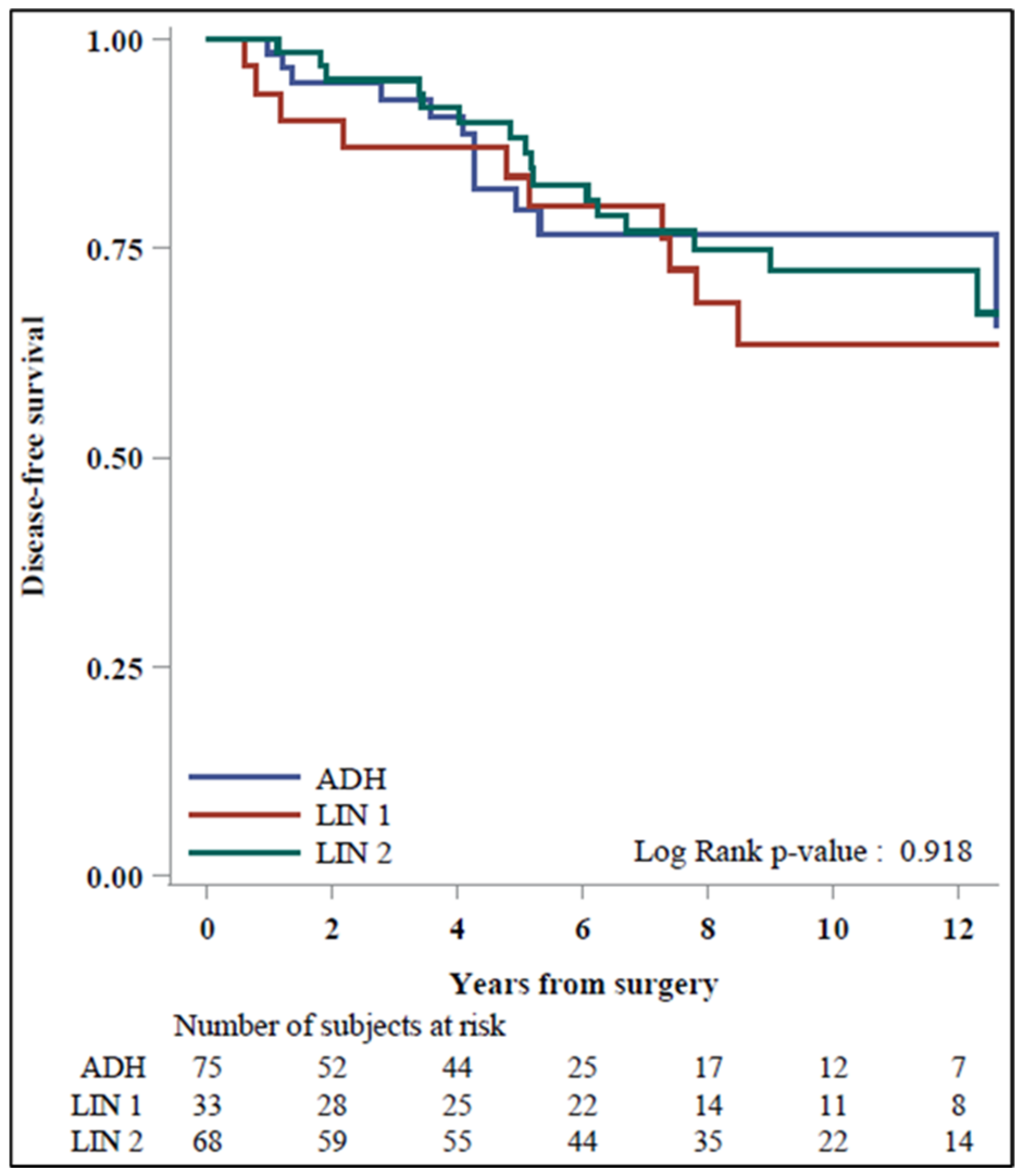
| At Surgery | ADH | LIN 1/2 | LIN 1 | LIN 2 |
|---|---|---|---|---|
| n (% col) | ||||
| No Upgrade (B2 or B3) | 75 (63) | 101 (80) | 33 (83) | 68 (79) |
| B2 | 36 (30) | 32 (25) | 15 (38) | 17 (20) |
| B3 | 39 (33) | 69 (55) | 18 (45) | 51 (59) |
| Upgrade (B5a or B5b) | 45 (38) | 25 (20) | 7 (18) | 18 (21) |
| B5a | 35 (29) | 8 (6) | 2 (5) | 6 (7) |
| B5b | 10 (8) | 17 (13) | 5 (13) | 12 (14) |
| Total | 120 | 126 | 40 | 86 |
| p-Value | ||
|---|---|---|
| Upgrade vs. No Upgrade | ADH vs. LIN 1/2 | 0.002 |
| ADH vs. LIN 1 | 0.019 | |
| ADH vs. LIN 2 | 0.011 | |
| B5a vs. No Upgrade | ADH vs. LIN 1/2 | <0.001 |
| ADH vs. LIN 1 | 0.002 | |
| ADH vs. LIN 2 | <0.001 | |
| B5b vs. No Upgrade | ADH vs. LIN 1/2 | 0.58 |
| ADH vs. LIN 1 | 0.78 | |
| ADH vs. LIN 2 | 0.54 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nicosia, L.; Mariano, L.; Pellegrino, G.; Ferrari, F.; Pesapane, F.; Bozzini, A.C.; Frassoni, S.; Bagnardi, V.; Pupo, D.; Mazzarol, G.; et al. Atypical Ductal Hyperplasia and Lobular In Situ Neoplasm: High-Risk Lesions Challenging Breast Cancer Prevention. Cancers 2024, 16, 837. https://doi.org/10.3390/cancers16040837
Nicosia L, Mariano L, Pellegrino G, Ferrari F, Pesapane F, Bozzini AC, Frassoni S, Bagnardi V, Pupo D, Mazzarol G, et al. Atypical Ductal Hyperplasia and Lobular In Situ Neoplasm: High-Risk Lesions Challenging Breast Cancer Prevention. Cancers. 2024; 16(4):837. https://doi.org/10.3390/cancers16040837
Chicago/Turabian StyleNicosia, Luca, Luciano Mariano, Giuseppe Pellegrino, Federica Ferrari, Filippo Pesapane, Anna Carla Bozzini, Samuele Frassoni, Vincenzo Bagnardi, Davide Pupo, Giovanni Mazzarol, and et al. 2024. "Atypical Ductal Hyperplasia and Lobular In Situ Neoplasm: High-Risk Lesions Challenging Breast Cancer Prevention" Cancers 16, no. 4: 837. https://doi.org/10.3390/cancers16040837
APA StyleNicosia, L., Mariano, L., Pellegrino, G., Ferrari, F., Pesapane, F., Bozzini, A. C., Frassoni, S., Bagnardi, V., Pupo, D., Mazzarol, G., De Camilli, E., Sangalli, C., Venturini, M., Pizzamiglio, M., & Cassano, E. (2024). Atypical Ductal Hyperplasia and Lobular In Situ Neoplasm: High-Risk Lesions Challenging Breast Cancer Prevention. Cancers, 16(4), 837. https://doi.org/10.3390/cancers16040837