


The Role of Pelvic Exenteration in Cervical Cancer: A Review of the Literature

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
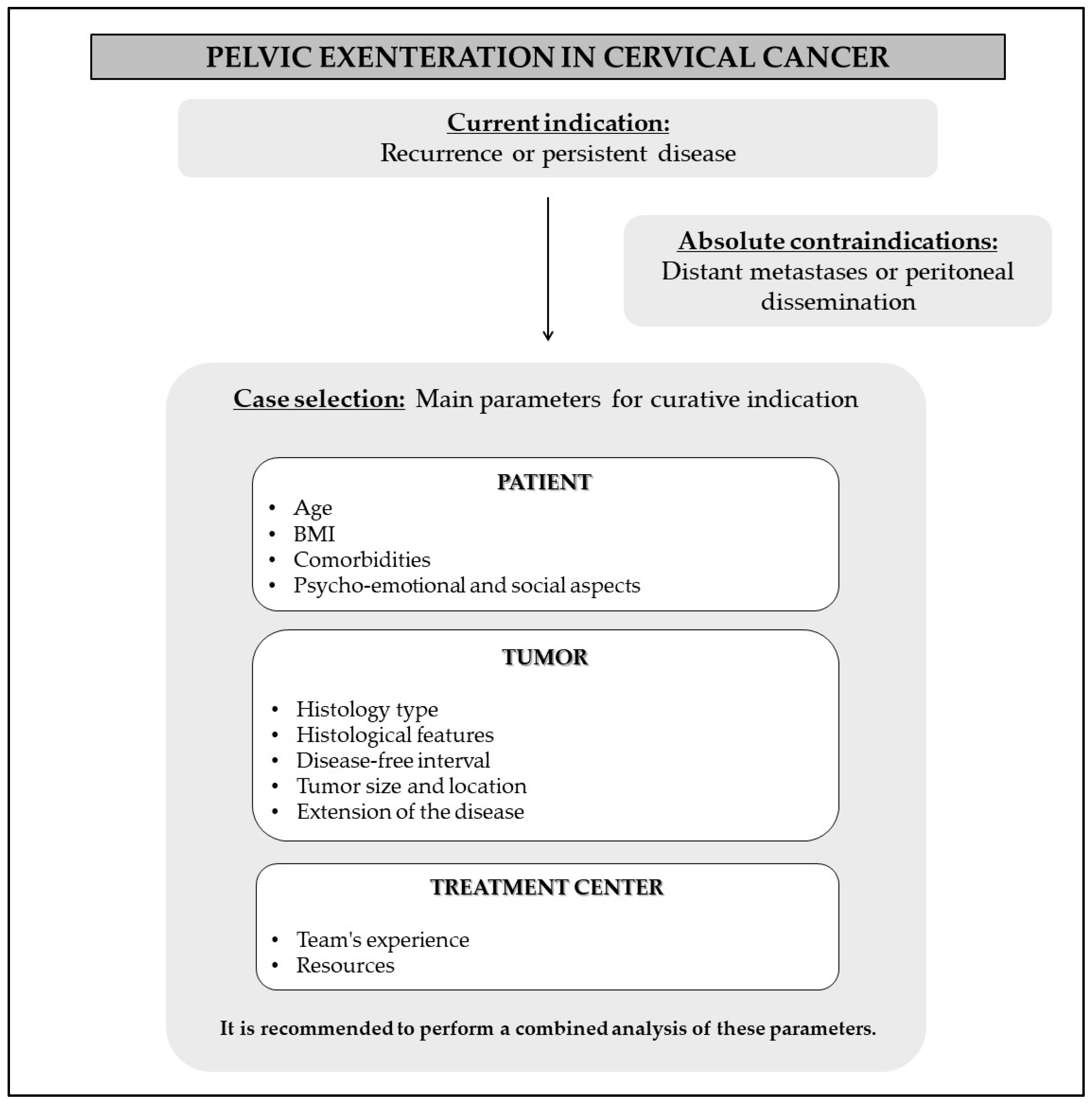
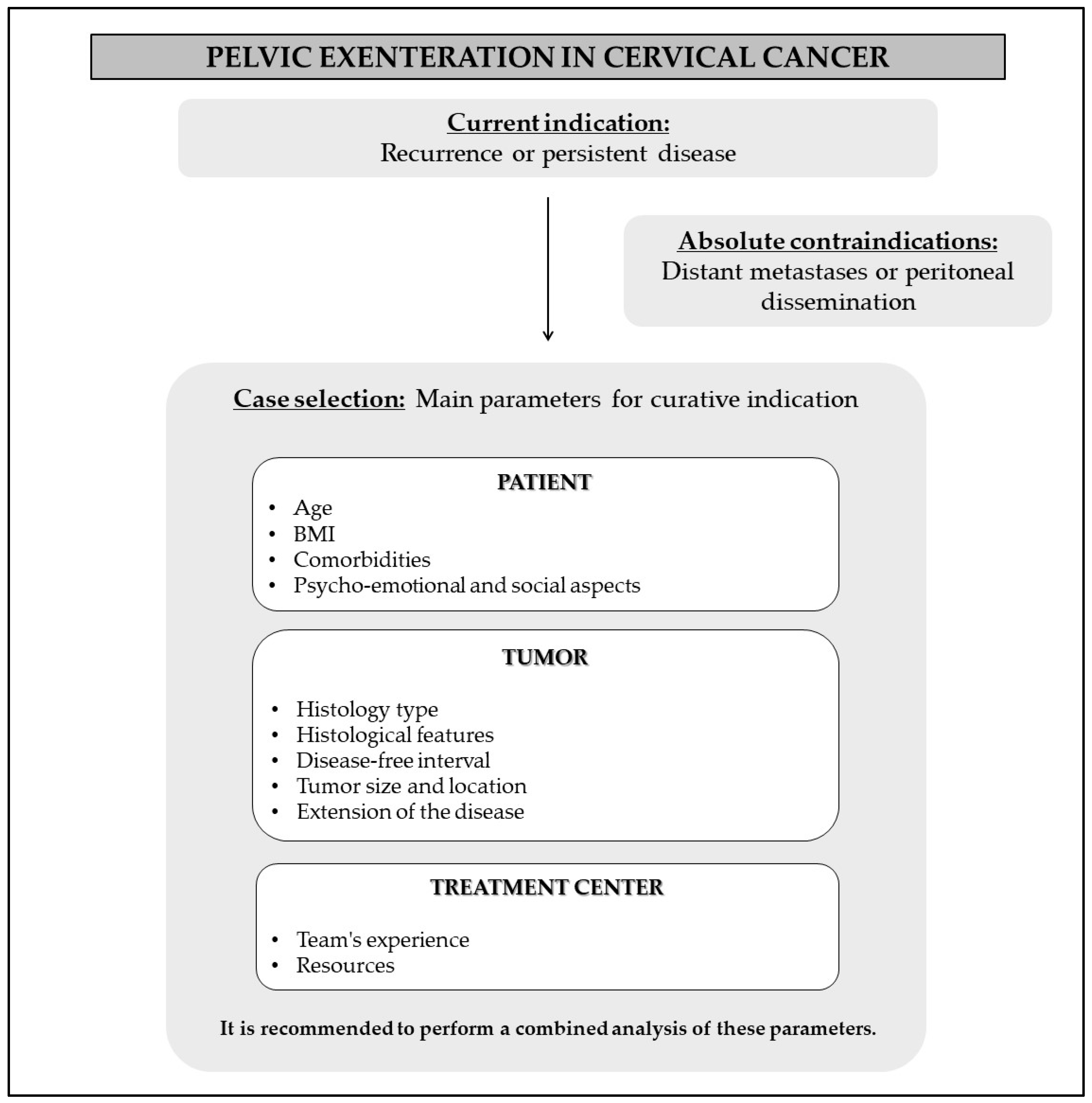
2. Indications and Case Selection
- (1)
- Patient’s clinical condition;
- (2)
- Tumor characteristics;
- (3)
- Resources available at the treatment center.
2.1. Assessment of the Patient’s Clinical Condition
2.2. Evaluation of Tumor Characteristics

{kind=link}
{kind=link}
| Parameters | Recommendation |
|---|---|
| Histology type | The literature presents controversy regarding oncologic outcomes when comparing usual histologies |
| Histological features | Grade 3 and undifferentiated tumors are linked to higher mortality [30]. Perineural invasion is associated with an elevated risk of recurrence [9,30]. The presence of lymphovascular invasion is also connected with worse oncologic outcomes [9,31] |
| Disease-free interval | It’s impact on cancer outcomes remains inconclusive |
| Tumor size and location | Tumors up to 3 cm located in the central region of the pelvis have been associated with a better prognosis [5,21,35] |
| Tumor extension | Achieving negative margins has consistently been identified as one of the key factors enhancing survival after PE [5,9,12,31,33,34]. Even more extensive approaches may involve removal of lateral components of the pelvis, such as muscles, nerves, bones, and great vessels, characterizing extended pelvic resection or extended lateral endopelvic resection [2,3]. |
| Lymph node involvement | It is associated with a worse prognosis [34,41,42,43,44,45]. |
| Small bowel involvement | The presence of implants is an absolute contraindication to the procedure. However, resection due to direct invasion may be considered [47]. |
2.2.1. Physical Examination
2.2.2. Imaging Tests
2.3. Treatment Center Evaluation
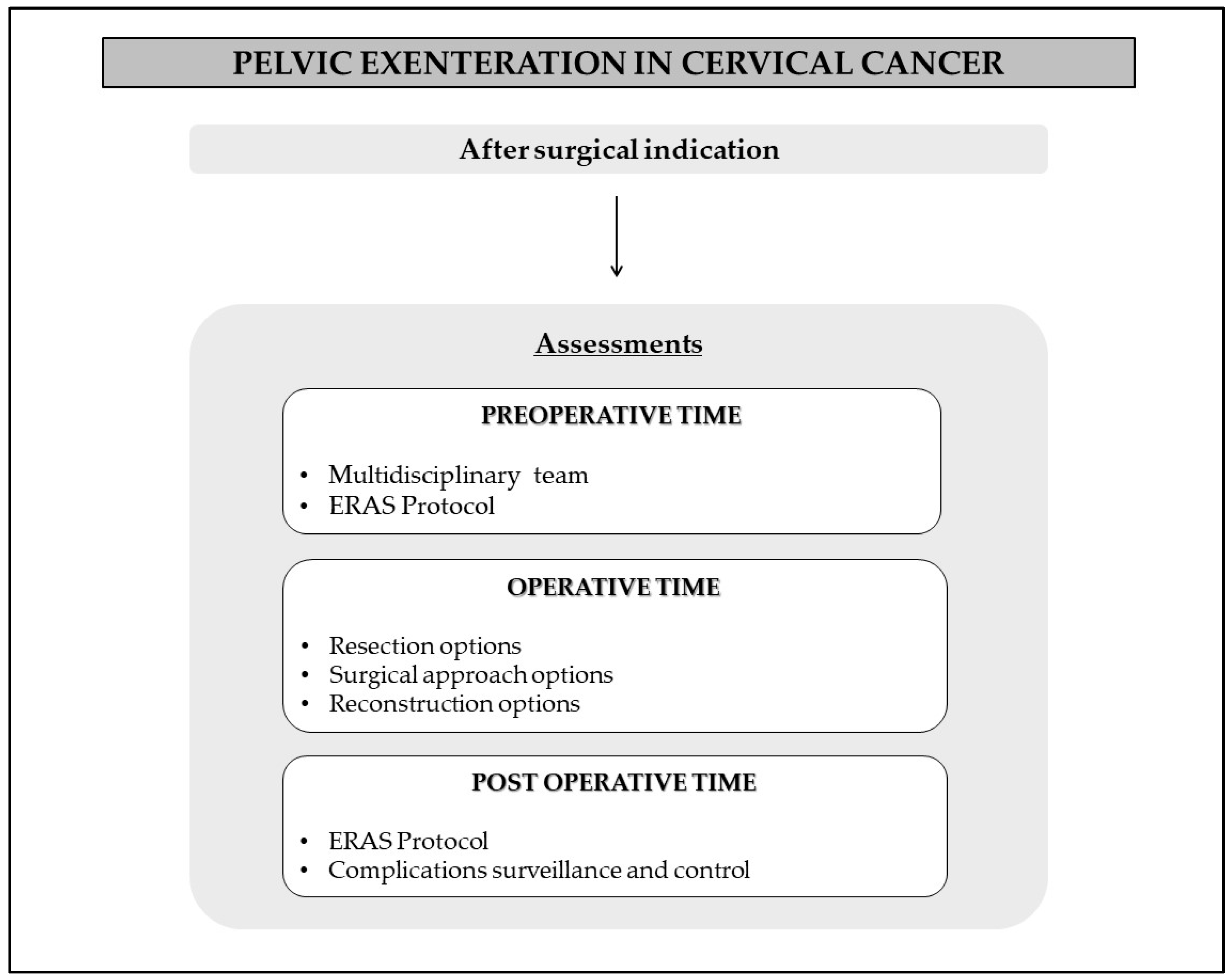
3. Preoperative Time
4. Operative Time
4.1. Resection of the Tumor
4.1.1. PE Classification
4.1.2. Extended Resections
4.2. Surgical Approaches
4.3. Reconstruction Procedures
4.3.1. Urinary Reconstruction
4.3.2. Intestinal Reconstruction
4.3.3. Pelvic Floor Reconstruction
4.3.4. Vaginal Reconstruction
5. Perioperative Time
6. Complications
7. Outcomes
7.1. Survival Analysis
7.2. Impact on Quality of Life
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brunschwig, A. Complete excision of pelvic viscera for advanced carcinoma. A one-stage abdominoperineal operation with end colostomy and bilateral ureteral implantation into the colon above the colostomy. Cancer 1948, 1, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Höckel, M. Laterally extended endopelvic resection: Surgical treatment of infrailiac pelvic wall recurrences of gynecologic malignancies. Am. J. Obstet. Gynecol. 1999, 180, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Vizzielli, G.; Naik, R.; Dostalek, L.; Bizzarri, N.; Kucukmetin, A.; Tinelli, G.; Scambia, G.; Cibula, D. Laterally extended pelvic resection for gynaecological malignancies: A multicentric experience with out-of-the-box surgery. Ann. Surg. Oncol. 2019, 26, 523–530. [Google Scholar] [CrossRef] [PubMed]
- Lago, V.; Poveda, I.; Padilla-Iserte, P.; Simón-Sanz, E.; García-Granero, Á.; Pontones, J.L.; Matute, L.; Domingo, S. Pelvic exenteration in gynecologic cancer: Complications and oncological outcome. Gynecol. Surg. 2019, 16, 1. [Google Scholar] [CrossRef]
- Maggioni, A.; Roviglione, G.; Landoni, F.; Zanagnolo, V.; Peiretti, M.; Colombo, N.; Bocciolone, L.; Biffi, R.; Minig, L.; Morrow, C.P. Pelvic exenteration: Ten-year experience at the European Institute of Oncology in Milan. Gynecol. Oncol. 2009, 114, 64–68. [Google Scholar] [CrossRef]
- Chiantera, V.; Rossi, M.; De Iaco, P.; Koehler, C.; Marnitz, S.; Ferrandina, G.; Legge, F.; Parazzini, F.; Scambia, G.; Schneider, A.; et al. Survival after curative pelvic exenteration for primary or recurrent cervical cancer: A retrospective multicentric study of 167 patients. Int. J. Gynecol. Cancer 2014, 24, 916–922. [Google Scholar] [CrossRef]
- Sharma, S.; Odunsi, K.; Driscoll, D.; Lele, S. Pelvic exenterations for gynecological malignancies: Twenty-year experience at Roswell Park Cancer Institute. Int. J. Gynecol. Cancer 2005, 15, 475–482. [Google Scholar] [CrossRef]
- Mauricio, D.; Zeybek, B.; Tymon-Rosario, J.; Harold, J.; Santin, A.D. Immunotherapy in cervical cancer. Curr. Oncol. Rep. 2021, 23, 61. [Google Scholar] [CrossRef]
- Westin, S.N.; Rallapalli, V.; Fellman, B.; Urbauer, D.L.; Pal, N.; Frumovitz, M.M.; Ramondetta, L.M.; Bodurka, D.C.; Ramirez, P.T.; Soliman, P.T. Overall survival after pelvic exenteration for gynecologic malignancy. Gynecol. Oncol. 2014, 134, 546–551. [Google Scholar] [CrossRef]
- Goldberg, G.L.; Sukumvanich, P.; Einstein, M.H.; Smith, H.O.; Anderson, P.S.; Fields, A.L. Total pelvic exenteration: The Albert Einstein College of Medicine/Montefiore medical center experience (1987 to 2003). Gynecol. Oncol. 2006, 101, 261–268. [Google Scholar] [CrossRef]
- Schmidt, A.M.; Imesch, P.; Fink, D.; Egger, H. Indications and long-term clinical outcomes in 282 patients with pelvic exenteration for advanced or recurrent cervical cancer. Gynecol. Oncol. 2012, 125, 604–609. [Google Scholar] [CrossRef] [PubMed]
- Benn, T.; Brooks, R.A.; Zhang, Q.; Powell, M.A.; Thaker, P.H.; Mutch, D.G.; Zighelboim, I. Pelvic exenteration in gynecologic oncology: A single institution study over 20 years. Gynecol. Oncol. 2011, 122, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, K.; Mandelbaum, R.S.; Adams, C.L.; Roman, L.D.; Wright, J.D. Performance and outcome of pelvic exenteration for gynecologic malignancies: A population-based study. Gynecol. Oncol. 2019, 153, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Marnitz, S.; Köhler, C.; Müller, M.; Behrens, K.; Hasenbein, K.; Schneider, A. Indications for primary and secondary exenterations in patients with cervical cancer. Gynecol. Oncol. 2006, 103, 1023–1030. [Google Scholar] [CrossRef] [PubMed]
- Figo Bhatla, N.; Aoki, D.; Sharma, D.N.; Sankaranarayanan, R. Cancer of the cervix uteri: 2021 update. Int. J. Gynecol. Obstet. 2021, 155, 28–44. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Raspollini, M.R.; Planchamp, F.; Centeno, C.; Chargari, C.; Felix, A.; Fischerová, D.; Jahnn-Kuch, D.; Joly, F.; Kohler, C.; et al. ESGO/ESTRO/ESP Guidelines for the management of patients with cervical cancer–Update 2023. Virchows Arch. 2023, 482, 935–966. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.; Eifel, P.J.; Lu, J.; Grigsby, P.W.; Levenback, C.; Stevens, R.E.; Rotman, M.; Gershenson, D.M.; Mutch, D.G. Pelvic radiation with concurrent chemotherapy compared with pelvic and para-aortic radiation for high-risk cervical cancer. N. Engl. J. Med. 1999, 340, 1137–1143. [Google Scholar] [CrossRef]
- Kroon, H.M.; Dudi-Venkata, N.N.; Bedrikovetski, S.; Thomas, M.L.; Kelly, M.E.; Aalbers, A.G.J.; Abdul Aziz, N.; Abraham-Nordling, M.; Akiyoshi, T.; Alberda, W.; et al. Palliative pelvic exenteration: A systematic review of patient-centered outcomes. Eur. J. Surg. Oncol. 2019, 45, 1787–1795. [Google Scholar] [CrossRef]
- Matthews, C.M.; Morris, M.; Burke, T.W.; Gershenson, D.M.; Wharton, J.T.; Rutledge, F.N. Pelvic exenteration in the elderly patient. Obstet. Gynecol. 1992, 79, 773–777. [Google Scholar] [CrossRef]
- Morley, G.W.; Hopkins, M.P.; Lindenauer, S.M.; Roberts, J.A. Pelvic exenteration, University of Michigan: 100 patients at 5 years. Obstet. Gynecol. 1989, 74, 934–943. [Google Scholar] [CrossRef]
- Shingleton, H.M.; Soong, S.J.; Gelder, M.S.; Hatch, K.D.; Baker, V.V.; Austin, M.J., Jr. Clinical and histopathologic factors predicting recurrence and survival after pelvic exenteration for cancer of the cervix. Obstet. Gynecol. 1989, 73, 1027–1034. [Google Scholar] [CrossRef] [PubMed]
- Straubhar, A.M.; Chi, A.J.; Zhou, Q.C.; Iasonos, A.; Filippova, O.T.; Leitao, M.M., Jr.; Awowole, I.O.; Abu-Rustum, N.R.; Broach, V.A.; Jewell, E.L.; et al. Pelvic exenteration for recurrent or persistent gynecologic malignancies: Clinical and histopathologic factors predicting recurrence and survival in a modern cohort. Gynecol. Oncol. 2021, 163, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Iglesias, D.A.; Westin, S.N.; Rallapalli, V.; Huang, M.; Fellman, B.; Urbauer, D.; Frumovitz, M.; Ramirez, P.T.; Soliman, P.T. The effect of body mass index on surgical outcomes and survival following pelvic exenteration. Gynecol. Oncol. 2012, 125, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Nielsen CK, P.; Sørensen, M.M.; Christensen, H.K.; Funder, J.A. Complications and survival after total pelvic exenteration. Eur. J. Surg. Oncol. 2022, 48, 1362–1367. [Google Scholar] [CrossRef]
- Crozier, M.; Morris, M.; Levenback, C.; Lucas, K.R.; Atkinson, E.N.; Wharton, J.T. Pelvic exenteration for adenocarcinoma of the uterine cervix. Gynecol. Oncol. 1995, 58, 74–78. [Google Scholar] [CrossRef]
- Shingleton, H.M.; Bell, M.C.; Fremgen, A.; Chmiel, J.S.; Russell, A.H.; Jones, W.B.; Winchester, J.D.P.; Clive, R.E. Is there really a difference in survival of women with squamous cell carcinoma, adenocarcinoma, and adenosquamous cell carcinoma of the cervix? Cancer 1995, 76, 1948–1955. [Google Scholar] [CrossRef]
- Grigsby, P.W.; Perez, C.A.; Kuske, R.R.; Camel, H.M.; Kao, M.S.; Galakatos, A.E.; Hederman, M.A. Adenocarcinoma of the uterine cervix: Lack of evidence for a poor prognosis. Radiother. Oncol. 1988, 12, 289–296. [Google Scholar] [CrossRef]
- Baiocchi, G.; Guimaraes, G.C.; Faloppa, C.C.; Kumagai, L.Y.; Oliveira, R.A.R.; Begnami, M.D.; Soares, F.A.; Lopes, A. Does histologic type correlate to outcome after pelvic exenteration for cervical and vaginal cancer? Ann. Surg. Oncol. 2013, 20, 1694–1700. [Google Scholar] [CrossRef]
- Baiocchi, G.; Guimaraes, G.; Oliveira, R.R.; Kumagai, L.; Faloppa, C.; Aguiar, S.; Begnami, M.D.; Soares, F.; Lopes, A. Prognostic factors in pelvic exenteration for gynecological malignancies. Eur. J. Surg. Oncol. 2012, 38, 948–954. [Google Scholar] [CrossRef]
- De Gregorio, N.; de Gregorio, A.; Ebner, F.; Friedl, T.W.P.; Huober, J.; Hefty, R.; Wittau, M.; Janni, W.; Widschwendter, P. Pelvic exenteration as ultimate ratio for gynecologic cancers: Single-center analyses of 37 cases. Arch. Gynecol. Obstet. 2019, 300, 161–168. [Google Scholar] [CrossRef] [PubMed]
- McLean, K.A.; Zhang, W.; Dunsmoor-Su, R.F.; Shah, C.A.; Gray, H.J.; Swensen, R.E.; Goff, B.A. Pelvic exenteration in the age of modern chemoradiation. Gynecol. Oncol. 2011, 121, 131–134. [Google Scholar] [CrossRef] [PubMed]
- Ter Glane, L.; Hegele, A.; Wagner, U.; Boekhoff, J. Pelvic exenteration for recurrent or advanced gynecologic malignancies–Analysis of outcome and complications. Gynecol. Oncol. Rep. 2021, 36, 100757. [Google Scholar] [CrossRef] [PubMed]
- Park, J.Y.; Choi, H.J.; Jeong, S.Y.; Chung, J.; Park, J.K.; Park, S.Y. The role of pelvic exenteration and reconstruction for treatment of advanced or recurrent gynecologic malignancies: Analysis of risk factors predicting recurrence and survival. J. Surg. Oncol. 2007, 96, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Moolenaar, L.; van Rangelrooij, L.; van Poelgeest, M.; van Beurden, M.; van Driel, W.; van Lonkhuijzen, L.; Mom, C.; Zaal, A. Clinical outcomes of pelvic exenteration for gynecologic malignancies. Gynecol. Oncol. 2023, 171, 114–120. [Google Scholar] [CrossRef]
- Smith, B.; Jones, E.L.; Kitano, M.; Gleisner, A.L.; Lyell, N.J.; Cheng, G.; McCarter, M.D.; Abdel-Misih, S.; Backes, F.J. Influence of tumor size on outcomes following pelvic exenteration. Gynecol. Oncol. 2017, 147, 345–350. [Google Scholar] [CrossRef]
- Martin, A.L.; Sinha, S.; Peres, L.C.; Hakam, A.; Chon, H.S.; Hoffman, M.S.; Shahzad, M.M.; Wenham, R.M.; Chern, J.Y. The impact of distance to closest negative margin on survival after pelvic exenteration. Gynecol. Oncol. 2022, 165, 514–521. [Google Scholar] [CrossRef]
- Caceres, A.M.S.M.; Mourton, S.M.; Bochner, B.H.; Gerst, S.R.; Liu, L.; Alektiar, K.M.; Kardos, S.V.; Barakat, R.R.; Boland, P.J.; Chi, D.S. Extended pelvic resections for recurrent uterine and cervical cancer: Out-of-the-box surgery. Int. J. Gynecol. Cancer 2008, 18, 1139–1144. [Google Scholar] [CrossRef]
- Andikyan, V.; Khoury-Collado, F.; Sonoda, Y.; Gerst, S.R.; Alektiar, K.M.; Sandhu, J.S.; Bochner, B.H.; Barakat, R.R.; Boland, P.J.; Chi, D.S. Extended pelvic resections for recurrent or persistent uterine and cervical malignancies: An update on out of the box surgery. Gynecol. Oncol. 2012, 125, 404–408. [Google Scholar] [CrossRef]
- Daix, M.; Gomez, C.M.; Angeles, M.A.; Tock, S.; Gladieff, L.; Gabiache, E.; Mery, E.; Martinez, A.; Cibula, D.; Ferron, G. Extended pelvic resection for gynecological malignancies: A review of out-of-the-box surgery. Gynecol. Oncol. 2022, 165, 393–400. [Google Scholar] [CrossRef]
- Rutledge, F.N.; McGuffee, V.B. Pelvic exenteration: Prognostic significance of regional lymph node metastasis. Gynecol. Oncol. 1987, 26, 374–380. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, M.P.; Morley, G.W. Prognostic factors in advanced stage squamous cell cancer of the cervix. Cancer 1993, 72, 2389–2393. [Google Scholar] [CrossRef] [PubMed]
- Million, R.R.; Rutledge, F.; Fletcher, G.H. Stage IV carcinoma of the cervix with bladder invasion. Am. J. Obstet. Gynecol. 1972, 113, 239–246. [Google Scholar] [CrossRef] [PubMed]
- Roberts, W.S.; Cavanagh, D.; Bryson, S.P.; Lyman, G.H.; Hewitt, S. Major morbidity after pelvic exenteration: A seven-year experience. Obstet. Gynecol. 1987, 69, 617–621. [Google Scholar] [PubMed]
- Barakat, R.R.; Goldman, N.A.; Patel, D.A.; Venkatraman, E.S.; Curtin, J.P. Pelvic exenteration for recurrent endometrial cancer. Gynecol. Oncol. 1999, 75, 99–102. [Google Scholar] [CrossRef] [PubMed]
- Brunschwig, A.; Barber, H.R. Extended pelvic exenteration for advanced cancer of the cervix. Long survivals following added resection of involved small bowel. Cancer 1964, 17, 1267–1270. [Google Scholar] [CrossRef] [PubMed]
- Lambrou, N.C.; Pearson, J.M.; Averette, H.E. Pelvic exenteration of gynecologic malignancy: Indications, and technical and reconstructive considerations. Surg. Oncol. Clin. 2005, 14, 289–300. [Google Scholar] [CrossRef]
- Donati, O.F.; Lakhman, Y.; Sala, E.; Burger, I.A.; Vargas, H.A.; Goldman, D.A.; Andikyan, V.; Park, K.J.; Chi, D.S.; Hricak, H. Role of preoperative MR imaging in the evaluation of patients with persistent or recurrent gynaecological malignancies before pelvic exenteration. Eur. Radiol. 2013, 23, 2906–2915. [Google Scholar] [CrossRef]
- Dresen, R.C.; Kusters, M.; Daniels-Gooszen, A.W.; Cappendijk, V.C.; Nieuwenhuijzen, G.A.P.; Kessels, A.G.H.; de Bruïne, A.P.; Beets, G.L.; Rutten, H.J.T.; Beets-Tan, R.G.H. Absence of tumor invasion into pelvic structures in locally recurrent rectal cancer: Prediction with preoperative MR imaging. Radiology 2010, 256, 143–150. [Google Scholar] [CrossRef]
- Brar, H.; May, T.; Tau, N.; Langer, D.; MacCrostie, P.; Han, K.; Metser, U. Detection of extra-regional tumour recurrence with 18F-FDG-PET/CT in patients with recurrent gynaecological malignancies being considered for radical salvage surgery. Clin. Radiol. 2017, 72, 302–306. [Google Scholar] [CrossRef]
- Burger, I.A.; Vargas, H.A.; Donati, O.F.; Andikyan, V.; Sala, E.; Gonen, M.; Goldman, D.A.; Chi, D.S.; Schöder, H.; Hricak, H. The value of 18F-FDG PET/CT in recurrent gynecologic malignancies prior to pelvic exenteration. Gynecol. Oncol. 2013, 129, 586–592. [Google Scholar] [CrossRef] [PubMed]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced recovery after surgery: A review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef] [PubMed]
- Magrina, J.F. Types of pelvic exenterations: A reappraisal. Gynecol. Oncol. 1990, 37, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Daix, M.; Angeles, M.A.; Leray, H.; Vergriete, K.; Martinez, A.; Ferron, G. Anterior pelvic exenteration and laterally extended pelvic resection: A step by step procedure. Int. J. Gynecol. Cancer 2022, 32, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Causa Andrieu, P.I.; Woo, S.; Rios-Doria, E.; Sonoda, Y.; Ghafoor, S. The role of imaging in pelvic exenteration for gynecological cancers. Br. J. Radiol. 2021, 94, 20201460. [Google Scholar] [CrossRef] [PubMed]
- Höckel, M. Long-term experience with (laterally) extended endopelvic resection (LEER) in relapsed pelvic malignancies. Curr. Oncol. Rep. 2015, 17, 435. [Google Scholar] [CrossRef] [PubMed]
- Solomon, M.J.; Brown, K.G.; Koh, C.E.; Lee, P.; Austin, K.K.; Masya, L. Lateral pelvic compartment excision during pelvic exenteration. Br. J. Surg. 2015, 102, 1710–1717. [Google Scholar] [CrossRef]
- Milne, T.; Solomon, M.J.; Lee, P.; Young, J.M.; Stalley, P.; Harrison, J.D.; Austin, K.K. Sacral resection with pelvic exenteration for advanced primary and recurrent pelvic cancer: A single-institution experience of 100 sacrectomies. Dis. Colon Rectum 2014, 57, 1153–1161. [Google Scholar] [CrossRef]
- Pomel, C.; Rouzier, R.; Pocard, M.; Thoury, A.; Sideris, L.; Morice, P.; Duvillard, P.; Bourgain, J.L.; Castaigne, D. Laparoscopic total pelvic exenteration for cervical cancer relapse. Gynecol. Oncol. 2003, 91, 616–618. [Google Scholar] [CrossRef]
- Lim, P.C. Robotic assisted total pelvic exenteration: A case report. Gynecol. Oncol. 2009, 115, 310–311. [Google Scholar] [CrossRef]
- Puntambekar, S.; Kudchadkar, R.J.; Gurjar, A.M.; Sathe, R.M.; Chaudhari, Y.C.; Agarwal, G.A.; Rayate, N.V. Laparoscopic pelvic exenteration for advanced pelvic cancers: A review of 16 cases. Gynecol. Oncol. 2006, 102, 513–516. [Google Scholar] [CrossRef] [PubMed]
- Puntambekar, S.; Rajamanickam, S.; Agarwal, G.; Joshi, S.; Rayate, N.; Deshmukh, A. Laparoscopic posterior exenteration in advanced gynecologic malignant disease. J. Minim. Invasive Gynecol. 2011, 18, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Puntambekar, S.; Lawande, A.; Desai, R.; Puntambekar, S.; Joshi, G.A.; Joshi, S.N. Initial experience of robotic anterior pelvic exenteration at a single institute. Int. J. Gynecol. Obstet. 2014, 126, 41–44. [Google Scholar] [CrossRef]
- Puntambekar, S.; Sharma, V.; Jamkar, A.V.; Gadkari, Y.; Joshi, G.; Puntambekar, S.; Parikh, H.; Vatsal, S. Our experience of laparoscopic anterior exenteration in locally advanced cervical carcinoma. J. Minim. Invasive Gynecol. 2016, 23, 396–403. [Google Scholar] [CrossRef] [PubMed]
- Bizzarri, N.; Chiantera, V.; Ercoli, A.; Fagotti, A.; Tortorella, L.; Conte, C.; Cappuccio, S.; Di Donna, M.C.; Gallotta, V.; Scambia, G.; et al. Minimally invasive pelvic exenteration for gynecologic malignancies: A multi-institutional case series and review of the literature. J. Minim. Invasive Gynecol. 2019, 26, 1316–1326. [Google Scholar] [CrossRef] [PubMed]
- Xuan, H.T.N.; Deloménie, M.; Ngô, C.; Douard, R.; Bats, A.S.; Timsit, O.; Méjean, A.; Lécuru, F. Pelvic exenteration by robotically-assisted laparoscopy: A feasibility series of 6 cases. Gynecol. Oncol. Rep. 2018, 25, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Martínez, A.; Filleron, T.; Vitse, L.; Querleu, D.; Mery, E.; Balague, G.; Delannes, M.; Soulie, M.; Pomel, C.; Ferron, G. Laparoscopic pelvic exenteration for gynaecological malignancy: Is there any advantage? Gynecol. Oncol. 2011, 120, 374–379. [Google Scholar] [CrossRef]
- Karkia, R.; Tailor, A.; Ellis, P.; Madhuri, T.; Scala, A.; Read, J.; Perry, M.; Patil, K.; Blackburn, A.; Butler-Manuel, S.; et al. Minimally invasive pelvic exenteration for gynaecological malignancy: A single-centre case series and review of the literature. Eur. J. Obstet. Gynecol. Reprod. Biol. 2022, 274, 56–61. [Google Scholar] [CrossRef]
- The PelvEx Collaborative. Minimally invasive surgery techniques in pelvic exenteration: A systematic and meta-analysis review. Surg. Endosc. 2018, 32, 4707–4715. [Google Scholar] [CrossRef]
- Matsuo, K.; Matsuzaki, S.; Mandelbaum, R.S.; Kanao, H.; Chang, E.J.; Klar, M.; Roman, L.D.; Wright, J.D. Utilization and perioperative outcome of minimally invasive pelvic exenteration in gynecologic malignancies: A national study in the United States. Gynecol. Oncol. 2021, 161, 39–45. [Google Scholar] [CrossRef]
- Sozzi, G.; Lauricella, S.; Cucinella, G.; Capozzi, V.A.; Berretta, R.; Di Donna, M.C.; Giallombardo, V.; Scambia, G.; Chiantera, V. Laterally extended endopelvic resection for gynecological malignancies, a comparison between laparoscopic and laparotomic approach. Eur. J. Surg. Oncol. 2023, 49, 107102. [Google Scholar] [CrossRef] [PubMed]
- Lampe, B.; Luengas-Würzinger, V.; Weitz, J.; Roth, S.; Rawert, F.; Schuler, E.; Classen-von Spee, S.; Fix, N.; Baransi, S.; Dizdar, A.; et al. Opportunities and Limitations of Pelvic Exenteration Surgery. Cancers 2021, 13, 6162. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, P.T.; Frumovitz, M.; Pareja, R.; Lopez, A.; Vieira, M.A.; Ribeiro, R. Phase III randomized trial of laparoscopic or robotic versus abdominal radical hysterectomy in patients with early-stage cervical cancer: LACC Trial. Gynecol. Oncol. 2018, 149, 245. [Google Scholar] [CrossRef]
- Bricker, E.M. Bladder substitution after pelvic etisceration. J. Urol. 2002, 167 Pt 2, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, S.; Ferenschild, F.; Solomon, M.; Rodwell, L.; Harrison, J.; Young, J.; Vasilaras, A.; Eisinger, D.; Lee, P.; Byrne, C. Urological leaks after pelvic exenterations comparing formation of colonic and ileal conduits. Eur. J. Surg. Oncol. 2012, 38, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Rink, M.; Kluth, L.; Eichelberg, E.; Fisch, M.; Dahlem, R. Continent catheterizable pouches for urinary diversion. Eur. Urol. Suppl. 2010, 9, 754–762. [Google Scholar] [CrossRef]
- Cody, J.D.; Nabi, G.; Dublin, N.; McClinton, S.; Neal, D.E.; Pickard, R.; Yong, S.M. Urinary diversion and bladder reconstruction/replacement using intestinal segments for intractable incontinence or following cystectomy. Cochrane Database Syst. Rev. 2012. [Google Scholar] [CrossRef]
- Urh, A.; Soliman, P.T.; Schmeler, K.M.; Westin, S.; Frumovitz, M.; Nick, A.M.; Fellman, B.; Urbauer, D.L.; Ramirez, P.T. Postoperative outcomes after continent versus incontinent urinary diversion at the time of pelvic exenteration for gynecologic malignancies. Gynecol. Oncol. 2013, 129, 580–585. [Google Scholar] [CrossRef]
- Kaur, M.; Joniau, S.; D’Hoore, A.; Van Calster, B.; Van Limbergen, E.; Leunen, K.; Penninckx, F.; Van Poppel, H.; Amant, F.; Vergote, I. Pelvic exenterations for gynecological malignancies: A study of 36 cases. Int. J. Gynecol. Cancer 2012, 22. [Google Scholar] [CrossRef]
- Jurado, M.; Alcazar, J.L.; Baixauli, J.; Hernandez-Lizoain, J.L. Low colorectal anastomosis after pelvic exenteration for gynecologic malignancies: Risk factors analysis for leakage. Int. J. Gynecol. Cancer 2011, 21, 397–402. [Google Scholar] [CrossRef]
- Jäger, L.; Nilsson, P.J.; Rådestad, A.F. Pelvic exenteration for recurrent gynecologic malignancy: A study of 28 consecutive pa–tients at a single institution. Int. J. Gynecol. Cancer 2013, 23, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Clavien, P.; Sanabria, J.; Strasberg, S. Proposed classification of complication of surgery with examples of utility in cholecystectomy. Surgery 1992, 111, 518–526. [Google Scholar] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205. [Google Scholar] [CrossRef] [PubMed]
- Ter Glane, L.; Hegele, A.; Wagner, U.; Boekhoff, J. Gynecologic oncology: Pelvic exenteration for advanced or recurring cervical cancer–a single center analysis. Cancer Diagn. Progn. 2022, 2, 308. [Google Scholar] [CrossRef] [PubMed]
- Fotopoulou, C.; Neumann, U.; Kraetschell, R.; Schefold, J.C.; Weidemann, H.; Lichtenegger, W.; Sehouli, J. Long-term clinical outcome of pelvic exenteration in patients with advanced gynecological malignancies. J. Surg. Oncol. 2010, 101, 507–512. [Google Scholar] [CrossRef] [PubMed]
- Tortorella, L.; Casarin, J.; Mara, K.C.; Weaver, A.L.; Multinu, F.; Glaser, G.E.; Cliby, W.A.; Scambia, G.; Mariani, A.; Kumar, A. Prediction of short-term surgical complications in women undergoing pelvic exenterationfor gynecological malignancies. Gynecol. Oncol. 2019, 152, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Haidopoulos, D.; Pergialiotis, V.; Aggelou, K.; Thomakos, N.; Alexakis, N.; Stamatakis, E.; Rodolakis, A. Pelvic exenteration for gynecologic malignancies: The experience of a tertiary center from Greece. Surg. Oncol. 2022, 40, 101702. [Google Scholar] [CrossRef]
- Lewandowska, A.; Szubert, S.; Koper, K.; Koper, A.; Cwynar, G.; Wicherek, L. Analysis of long-term outcomes in 44 patients following pelvic exenteration due to cervical cancer. World J. Surg. Oncol. 2020, 18, 234. [Google Scholar] [CrossRef]
- Soper, J.T.; Berchuck, A.; Creasman, W.T.; Clarke-Pearson, D.L. Pelvic exenteration: Factors associated with major surgical morbidity. Gynecol. Oncol. 1989, 35, 93–98. [Google Scholar] [CrossRef]
- Berek, J.S.; Howe, C.; Lagasse, L.D.; Hacker, N.F. Pelvic exenteration for recurrent gynecologic malignancy: Survival and morbidity analysis of the 45-year experience at UCLA. Gynecol. Oncol. 2005, 99, 153–159. [Google Scholar] [CrossRef]
- Gheorghe, M.; Cozlea, A.L.; Kiss, S.L.; Stanca, M.; Căpîlna, M.E.; Bacalbașa, N.; Moldovan, A.A. Primary pelvic exenteration: Our experience with 23 patients from a single institution. Exp. Ther. Med. 2021, 22, 1060. [Google Scholar] [CrossRef] [PubMed]
- Stanca, M.; Căpîlna, D.M.; Căpîlna, M.E. Long-term survival, prognostic factors, and quality of life of patients undergoing pelvic exenteration for cervical cancer. Cancers 2022, 14, 2346. [Google Scholar] [CrossRef] [PubMed]
- Bouraoui, I.; Bouaziz, H.; Tounsi, N.; Ben Romdhane, R.; Hechiche, M.; Slimane, M.; Rahal, K. Survival after pelvic exenteration for cervical cancer. J. Obstet. Gynecol. India 2022, 72, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Sabiani, L.; Knight, S.; Blache, G.; Jauffret, C.; Buttarelli, M.; Lambaudie, E.; Houvenaeghel, G. Operative Prognostic Scores for Pelvic Exenterations for Gynecological Cancer: When Should we Operate? J. Surg. Res. 2022, 5, 449–455. [Google Scholar] [CrossRef]
- Cibula, D.; Lednický, Š.; Höschlová, E.; Sláma, J.; Wiesnerová, M.; Mitáš, P.; Matějovský, Z.; Schneiderová, M.; Dundr, P.; Němejcová, K.; et al. Quality of life after extended pelvic exenterations. Gynecol. Oncol. 2022, 166, 100–107. [Google Scholar] [CrossRef]
| Parameters | Recommendation |
|---|---|
| Age | Chronological age is not a limiting factor for PE [7,14,19,20,21] |
| Comorbidities | Directly associated with postoperative adverse events, longer hospital stays, and higher mortality [13] |
| BMI | Obesity is directly linked to a higher incidence of postoperative complications [24], just like malnutrition [25] |
| Psycho-emotional and social aspects | The patient must be informed, prepared, and in agreement with the therapeutic proposals |
| Parameters | Recommendation |
|---|---|
| Treatment center | The team’s experience and the resources provided are associated with the success of the treatment |
| Authors | Number of Patients | Cancer | Morbidity | Mortality |
|---|---|---|---|---|
| Maggioni et al., 2009 [5] | 106 | Gynecologic | 66% | 0% (30 days) |
| Fotopoulou et al., 2010 [85] | 47 | Gynecologic | 70.2 (major) | 8.5% |
| Benn et al., 2011 [12] | 54 | Gynecologic | 50% (early) | - |
| 61% (late) | ||||
| Schmidt et al., 2012 [11] | 282 | Cervical | 51% | 5% |
| Westin et al., 2014 [9] | 160 | Gynecologic | 94.4% | 1.3% |
| Matuso et al., 2019 [13] | 2647 | Gynecologic | 68.1% | 1.9% |
| Tortorella et al., 2019 [86] | 138 | Gynecologic | 67% | 2.2% (90 days) |
| Lewandowska et al., 2020 [88] | 44 | Cervical | 25% (major) | 2.3% |
| Ter Glane et al., 2021 [33] | 47 | Gynecologic | 80.9% | 4.3% |
| Ter Glane et al., 2022 [84] | 24 | Cervical | 83.3% | 4.2% |
| Haidopoulos et al., 2022 [87] | 138 | Gynecologic | 12.5% (major) | 2.2% |
| 42% (grade 2+) |
| Authors | Number of Patients | Cancer | Overall Survival |
|---|---|---|---|
| Berek et al., 2005 [90] | 75 | Gynecologic | 54% in 5 years |
| Marnitz et al., 2006 [14] | 55 | Cervical | 36.8% in 5 years |
| Maggioni et al., 2009 [5] | 106 | Gynecologic | 31.6% in 5 years |
| Benn et al., 2011 [12] | 54 | Gynecologic | 34% in 50 months |
| 22% in 100 months | |||
| Kaur et al., 2012 [79] | 36 | Gynecologic | 44% in 5 years |
| Schmidt et al., 2012 [11] | 282 | Cervical | 41% in 5 years |
| Haidopoulus et al., 2012 [87] | 138 | Gynecologic | 44.6% alive in 38.84 months |
| Jager et al., 2013 [81] | 28 | Gynecologic | 70% in 5 years |
| Chiantera et al., 2014 [6] | 167 | Cervical | 38% in 5 years |
| Westin et al., 2014 [9] | 160 | Pelvic | 40% in 5 years |
| Lago et al., 2019 [4] | 23 | Gynecologic | 41.6% in 5 years |
| De Gregório et al., 2019 [31] | 37 | Gynecologic | 46.4% in 5 years |
| Ter Glane et al., 2021 [33] | 47 | Gynecologic | 21.3% in 3 years * |
| Gheorghe et al., 2021 [91] | 23 | Pelvic | 66% in 5 years |
| Stanca et al., 2022 [92] | 47 | Cervical | 48.7% in 5 years |
| Ter Glane et al., 2022 [84] | 24 | Cervical | 23.8% in 5 years |
| Bouraouri et al., 2022 [93] | 41 | Cervical | 51% in 5 years |
| Sibiani et al., 2022 [94] | 277 | Gynecologic | 32.3% in 5 years |
| 36.8% in 3 years | |||
| Moolenaar, et al., 2023 [35] | 90 | Gynecologic | 51.1% in 2 years |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ubinha, A.C.F.; Pedrão, P.G.; Tadini, A.C.; Schmidt, R.L.; Santos, M.H.d.; Andrade, C.E.M.d.C.; Longatto Filho, A.; Reis, R.d. The Role of Pelvic Exenteration in Cervical Cancer: A Review of the Literature. Cancers 2024, 16, 817. https://doi.org/10.3390/cancers16040817
Ubinha ACF, Pedrão PG, Tadini AC, Schmidt RL, Santos MHd, Andrade CEMdC, Longatto Filho A, Reis Rd. The Role of Pelvic Exenteration in Cervical Cancer: A Review of the Literature. Cancers. 2024; 16(4):817. https://doi.org/10.3390/cancers16040817
Chicago/Turabian StyleUbinha, Ana Carla Franco, Priscila Grecca Pedrão, Aline Cássia Tadini, Ronaldo Luis Schmidt, Marcelo Henrique dos Santos, Carlos Eduardo Mattos da Cunha Andrade, Adhemar Longatto Filho, and Ricardo dos Reis. 2024. "The Role of Pelvic Exenteration in Cervical Cancer: A Review of the Literature" Cancers 16, no. 4: 817. https://doi.org/10.3390/cancers16040817
APA StyleUbinha, A. C. F., Pedrão, P. G., Tadini, A. C., Schmidt, R. L., Santos, M. H. d., Andrade, C. E. M. d. C., Longatto Filho, A., & Reis, R. d. (2024). The Role of Pelvic Exenteration in Cervical Cancer: A Review of the Literature. Cancers, 16(4), 817. https://doi.org/10.3390/cancers16040817