
Perspectives and Concerns on Late Effects Regarding Sexuality among Adolescents and Young Adults Treated for Testicular Germ Cell Tumor: The PRICELESS-Study—A Qualitative Study

 , , and
, , and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Data Collection
2.3. Data Analysis
2.4. Trustworthiness
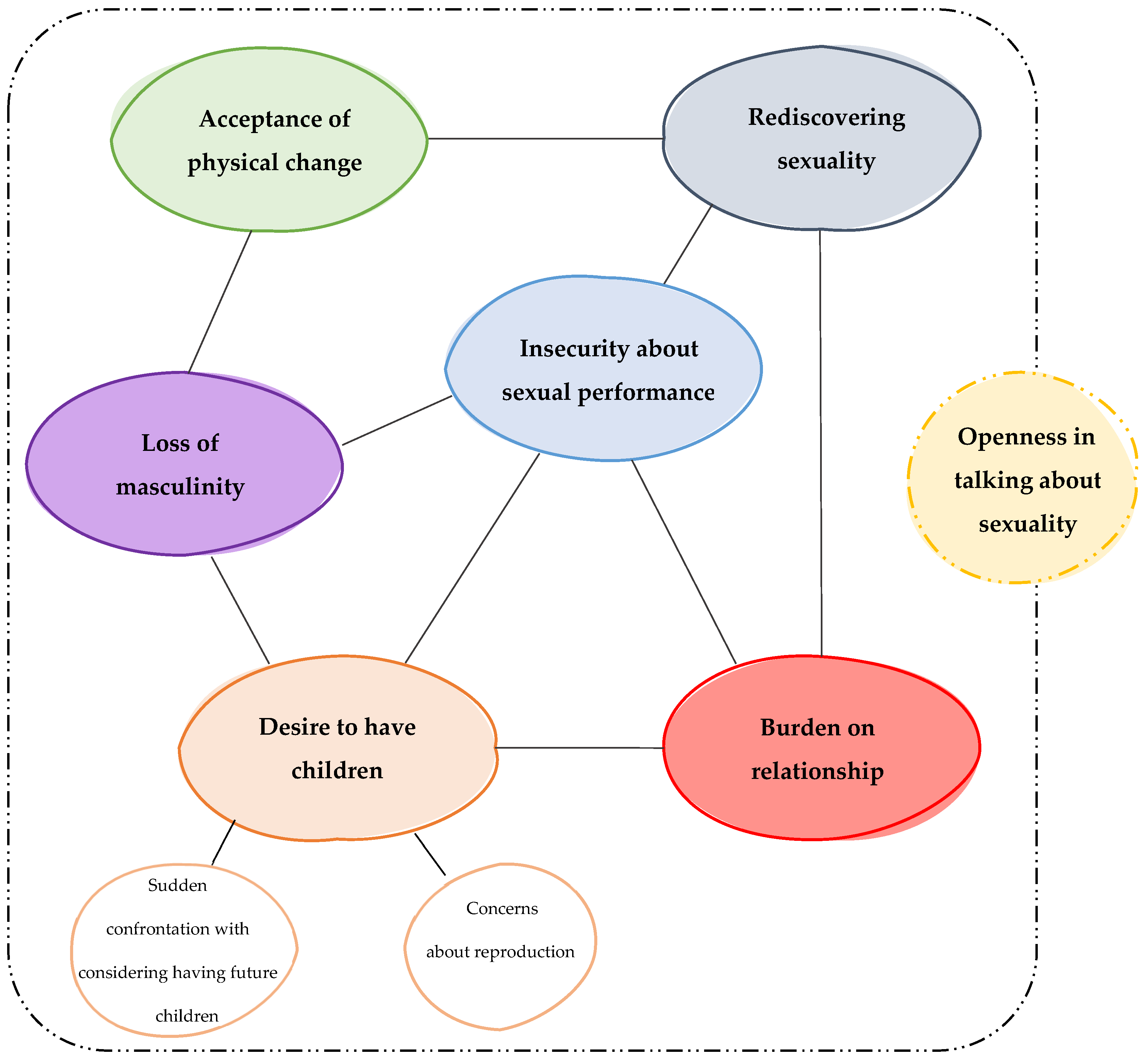
3. Results
3.1. Desire to Have Children
“And of course, they have also indicated that it’s possible that the chemotherapy causes your good cells, including the good sperm cells, to be damaged. And that’s why I started thinking about or worrying about fertility and not necessarily about sexuality itself.”(P5, 25 y/o)
3.1.1. Sudden Confrontation with Considering Having Future Children
“…uh, so they could freeze that [semen] and check if it was still fertile. While I didn’t worry about it at that time, but then you suddenly start thinking a lot about it (…) even if you don’t worry about it, you suddenly have to think about it. I thought that was uh… not annoying, but… weird or something that you suddenly have to think about it.”(P5, 25 y/o)
3.1.2. Uncertainty about Reproduction
“…it’s nice that you have several straws of yours somewhere in the freezer, which you can use at all times.”(P8, 28 y/o)
“Yeah, you’re thinking about it [sexuality], but... yeah, I’m still single so... that’s, well... [silence]... yeah, as long as I’m fertile, that’s- that’s I think the only thing that’s keeping me busy right now.”(P1, 19 y/o)
“No, I’m not stressed about it or anything. We already had a son. So, I was like: “Well… if I’m not fertile anymore, then so be it. And if we want to and have the capacity to conceive a second one, um… then I’m okay with that”.”(P10, 32 y/o)
“So, once it can be done naturally, it would be a nice bonus. I really want that because you prefer not to enter such a [fertility] program.”(P2, 30 y/o)
3.2. Rediscovering Sexuality
“Yes, uncomfortable [first time having sex], a little bit for her too. Especially because then, well, she also looks at it of course and then we shower and then... the other ball, in the beginning especially she found it still a bit scary.”(P9, 27 y/o)
“I think stress in particular and the impact of the uh... diagnosis and the treatment involved has greatly influenced delaying our... sexual... moments.”(P10, 32 y/o)
“It’s like reliving it again, just discovering each other’s bodies or something. (…) It kind of felt like I had to guide her a little.”(P10, 32 y/o)
“Just like I say, when I do it now, I really have to think about… yes… push yourself… (…) yes, push yourself, to pick it up or think about it.”(P6, 39 y/o)
“…the testosterone gel actually determines your whole life. Or at least your sexual life…”(P6, 39 y/o)
3.3. Insecurity about Sexual Performance
“That-that, yes, if it brings uncertainty, let me put it this way, it’s just difficult (...) because then it gets into your head… (...) …and that doesn’t work.”(P2, 30 y/o)
“Look, when I do it now [having sex], it’s really forced. Because it has to, I have to perform, I have to, I have to (…) It’s not emptying my mind being busy with that, no. It is, [I] have to, have to perform. Well, if that happens, then, yes…. then sometimes it just doesn’t work, no.”(P2, 30 y/o)
3.4. Acceptance of Physical Change
“Uh, however, it isn’t nice at all if anyone was touching it, you know. That’s the point. I’m just thinking: “Hey, just stay away from me for a while”. Yes, you know? “Don’t touch me right now”. (…) Yes, I still have that.”(P13, 43 y/o)
“At first, you think I’m going to do that for 100,000% anyway, and after that [treatment] it doesn’t interest you at all. (…) but it becomes a part of you so quickly that you think, “Yeah, I’m not going...” you know. It becomes so secondary because you could have been dead, and then to do something like that…”(P12, 27 y/o)
3.5. Loss of Masculinity
“Yeah… you might feel a little less uh... how to say... a little less complete or something; slightly less of a real guy. You’re actually proud of your balls and your penis, after all. (...) Yes, and if they take one away, you think, “I’m a little less man or so”.”(P11, 30 y/o)
“Before, I was like an alpha male, and now uh… I’m a uh… little sheep. I just named something... a tame lamb. It-it’s such a world of difference.”(P2, 30 y/o)
3.6. Burden on the Relationship
P: “For 90%, it’s gone [confidence in his body].”I: “Yes, gosh (silence). That’s quite something.”P: “Yes, if you are in a relationship and eventually want to have children.”(P2, 30 y/o)
“Yes, she also has her needs, and it’s just part of it [relationship]. (…) Yes, then you’re afraid you’re failing the other [partner].”(P6, 39 y/o)
3.7. Openness in Discussing Sexuality
“And certainly, yes, it still remains a sensitive topic or so. Or a, uh, bit of a taboo. That you talk about that with people...(…)Yeah, because it’s still [something] with your sexuality and stuff. It’s not necessarily a taboo for me when I talk about it with friends, but it’s not something that I just, that I will immediately bring up myself.”(P5, 25 y/o)
“Actually, I only told sometimes when I thought this is going to be a serious one [girlfriend], so then I want to tell it. So, I didn’t even really tell anyone every time I started dating if it might last maybe a week or two weeks. I thought, yeah, you don’t deserve to know it yet.”(P7, 30 y/o)
“P: I think it’s a little easier to say yes. Even though my wife and I talk about it very openly, and she knows it all, to someone else, it’s a kind of a bridge too far sometimes.”“I: Yes, it is indeed a big step to bring it up yourself.”“P: yes, and if someone else says, “Oh, this and this happens very often”, “does that bother you, if not you do…”, I don’t know. I think that will help.”(P11, 30 y/o)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huyghe, E.; Matsuda, T.; Thonneau, P. Increasing Incidence of Testicular Cancer Worldwide: A Review. J. Urol. 2003, 170, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Cheng, L.; Albers, P.; Berney, D.M.; Feldman, D.R.; Daugaard, G.; Gilligan, T.; Looijenga, L.H.J. Testicular Cancer. Nat. Rev. Dis. Primers 2018, 4, 29. [Google Scholar] [CrossRef] [PubMed]
- Hanna, N.H.; Einhorn, L.H. Testicular Cancer—Discoveries and Updates. N. Engl. J. Med. 2014, 371, 2005–2016. [Google Scholar] [CrossRef] [PubMed]
- Global Cancer Observatory. Cancer Today. Available online: https://gco.iarc.fr/today/online-analysis-treemap (accessed on 30 September 2021).
- Park, J.S.; Kim, J.; Elghiaty, A.; Ham, W.S. Recent Global Trends in Testicular Cancer Incidence and Mortality. Medicine 2018, 97, e12390. [Google Scholar] [CrossRef] [PubMed]
- Algaba, F.; Bokemeyer, C.; Boormans, J.; Fischer, S.; Fizazi, K.; Gremmels, H.; Leão, R.; Nicol, D.; Nicolai, N.; Oldenburg, J.; et al. EAU Guidelines on Testicular Cancer; EAU Guidelines Office: Arnhem, The Netherlands, 2021. [Google Scholar]
- Chovanec, M.; Lauritsen, J.; Bandak, M.; Oing, C.; Kier, G.G.; Kreiberg, M.; Rosenvilde, J.; Wagner, T.; Bokemeyer, C.; Daugaard, G. Late Adverse Effects and Quality of Life in Survivors of Testicular Germ Cell Tumour. Nat. Rev. Urol. 2021, 18, 227–245. [Google Scholar] [CrossRef] [PubMed]
- Aziz, N.M. Cancer Survivorship Research: State of Knowledge, Challenges and Opportunities. Acta Oncol. 2007, 46, 417–432. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute (NCI). Definition of Late Effect—NCI Dictionary of Cancer Terms. Available online: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/late-effect (accessed on 22 September 2021).
- Moore, A.; Higgins, A. Testicular Cancer: Addressing the Psychosexual Issues. Br. J. Nurs. 2009, 18, 1182–1186. [Google Scholar] [CrossRef] [PubMed]
- Alexis, O.; Adeleye, A.O.; Worsley, A.J. Men’s Experiences of Surviving Testicular Cancer: An Integrated Literature Review. J. Cancer Surviv. 2020, 14, 284–293. [Google Scholar] [CrossRef]
- Carpentier, M.Y.; Fortenberry, J.D. Romantic and Sexual Relationships, Body Image, and Fertility in Adolescent and Young Adult Testicular Cancer Survivors: A Review of the Literature. J. Adolesc. Health 2010, 47, 115–125. [Google Scholar] [CrossRef]
- Enzlin, R.; Vervoort, S.C.J.M.; Suelmann, B.B.M.; Meijer, R.P.; Teunissen, S.C.C.M.; Zweers, D. The Prevalence and Intensity of Late Effects in Patients with Testicular Germ Cell Tumors: A First Step of Instrument Development Using a Stepwise Approach. Eur. J. Oncol. Nurs. 2023, 64, 102303. [Google Scholar] [CrossRef]
- Arnett, J. Emerging Adulthood: A Theory of Development from the Late Teens through the Twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- Schepisi, G.; De Padova, S.; De Lisi, D.; Casadei, C.; Meggiolaro, E.; Ruffilli, F.; Rosti, G.; Lolli, C.; Ravaglia, G.; Conteduca, V.; et al. Psychosocial Issues in Long-Term Survivors of Testicular Cancer. Front. Endocrinol. 2019, 10, 113. [Google Scholar] [CrossRef]
- Bumbasirevic, U.; Bojanic, N.; Pekmezovic, T.; Janjic, A.; Janicic, A.; Milojevic, B.; Tulic, C. Health-Related Quality of Life, Depression, and Sexual Function in Testicular Cancer Survivors in a Developing Country: A Serbian Experience. Support. Care Cancer 2013, 21, 757–763. [Google Scholar] [CrossRef]
- Flynn, K.E.; Lin, L.; Bruner, D.W.; Cyranowski, J.M.; Hahn, E.A.; Jeffery, D.D.; Reese, J.B.; Reeve, B.B.; Shelby, R.A.; Weinfurt, K.P. Sexual Satisfaction and the Importance of Sexual Health to Quality of Life Throughout the Life Course of US Adults. J. Sex. Med. 2016, 13, 1642. [Google Scholar] [CrossRef]
- World Health Organization. Defining Sexual Health: Report of a Technical Consultation on Sexual Health, 28–31 January 2002, Geneva; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Trotti, A.; Colevas, A.D.; Setser, A.; Basch, E. Patient-Reported Outcomes and the Evolution of Adverse Event Reporting in Oncology. J. Clin. Oncol. 2007, 25, 5121–5127. [Google Scholar] [CrossRef]
- Olsson, C.; Berglund, A.L.; Larsson, M.; Athlin, E. Patient’s Sexuality—A Neglected Area of Cancer Nursing? Eur. J. Oncol. Nurs. 2012, 16, 426–431. [Google Scholar] [CrossRef]
- Papadopoulou, C.; Sime, C.; Rooney, K.; Kotronoulas, G. Sexual Health Care Provision in Cancer Nursing Care: A Systematic Review on the State of Evidence and Deriving International Competencies Chart for Cancer Nurses. Int. J. Nurs. Stud. 2019, 100, 103405. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, L.; Ruan, J.Y.; Cheung, W.Y. Discussions about Reproductive and Sexual Health among Young Adult Survivors of Cancer. Cancer Med. 2016, 5, 1037–1046. [Google Scholar] [CrossRef] [PubMed]
- Frederick, N.N.; Revette, A.; Michaud, A.; Bober, S.L. A Qualitative Study of Sexual and Reproductive Health Communication with Adolescent and Young Adult Oncology Patients. Pediatr. Blood Cancer 2019, 66, e27673. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, V.; Laan, E.T.M.; den Oudsten, B.L. Sexual Health-Related Care Needs among Young Adult Cancer Patients and Survivors: A Systematic Literature Review. J. Cancer Surviv. 2022, 16, 913. [Google Scholar] [CrossRef] [PubMed]
- Holloway, I.; Galvin, K. Qualitative Research in Nursing and Healthcare, 4th ed.; Wiley-Blackwell: Chichester, UK, 2016. [Google Scholar]
- Boeije, H. Analysis in Qualitative Research; SAGE Publications Ltd.: London, UK, 2014. [Google Scholar]
- Moser, A.; Korstjens, I. Series: Practical Guidance to Qualitative Research. Part 1: Introduction. Eur. J. Gen. Pract. 2017, 23, 271–273. [Google Scholar] [CrossRef] [PubMed]
- Hennink, M.M.; Kaiser, B.N.; Marconi, V.C. Code Saturation versus Meaning Saturation: How Many Interviews Are Enough? Qual. Health Res. 2017, 27, 591–608. [Google Scholar] [CrossRef] [PubMed]
- Laursen, B.S. Sexuality in Men after Prostate Cancer Surgery: A Qualitative Interview Study. Scand. J. Caring Sci. 2017, 31, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Granero-Molina, J.; Torrente-Sánchez, M.J.; Ferrer-Márquez, M.; Hernández-Padilla, J.M.; Ruiz-Muelle, A.; López-Entrambasaguas, O.M.; Fernández-Sola, C. Sexuality amongst Heterosexual Men with Morbid Obesity in a Bariatric Surgery Programme: A Qualitative Study. J. Clin. Nurs. 2020, 29, 4258–4269. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using Thematic Analysis in Psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]
- QSR International Pty Ltd. NVivo 2020; QSR International Pty Ltd.: Doncaster, VIC, Australia, 2020. [Google Scholar]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed]
- Lincoln, Y.S.; Guba, E.G. Naturalistic Inquiry; Sage: Newbury Park, CA, USA, 1985. [Google Scholar]
- Ball, M.; Nelson, C.J.; Shuk, E.; Starr, T.D.; Temple, L.; Jandorf, L.; Schover, L.; Mulhall, J.P.; Woo, H.; Jennings, S.; et al. Men’s Experience with Sexual Dysfunction Post Rectal Cancer Treatment: A Qualitative Study. J. Cancer Educ. 2013, 28, 494. [Google Scholar] [CrossRef]
- Hayashi, S.; Oishi, F.; Sato, K.; Fukuda, H.; Ando, S. Sexual Dysfunction Associated with Prostate Cancer Treatment in Japanese Men: A Qualitative Research. Support. Care Cancer 2022, 30, 3201. [Google Scholar] [CrossRef]
- Frederick, N.N.; Recklitis, C.J.; Blackmon, J.E.; Bober, S. Sexual Dysfunction in Young Adult Survivors of Childhood Cancer. Pediatr. Blood Cancer 2016, 63, 1622–1628. [Google Scholar] [CrossRef]
- Ussher, J.M.; Perz, J. Infertility-Related Distress Following Cancer for Women and Men: A Mixed Method Study. Psychooncology 2019, 28, 607–614. [Google Scholar] [CrossRef]
- Benedict, C.; Shuk, E.; Ford, J.S. Fertility Issues in Adolescent and Young Adult Cancer Survivors. J. Adolesc. Young Adult Oncol. 2016, 5, 48. [Google Scholar] [CrossRef]
- Ljungman, L.; Eriksson, L.E.; Flynn, K.E.; Gorman, J.R.; Ståhl, O.; Weinfurt, K.; Wiklander, M.; Lampic, C.; Wettergren, L. Sexual Dysfunction and Reproductive Concerns in Young Men Diagnosed with Testicular Cancer: An Observational Study. J. Sex. Med. 2019, 16, 1049–1059. [Google Scholar] [CrossRef]
- Hopwood, P.; Fletcher, I.; Lee, A.; Al Ghazal, S. A Body Image Scale for Use with Cancer Patients. Eur. J. Cancer 2001, 37, 189–197. [Google Scholar] [CrossRef]
- Carpentier, M.Y.; Fortenberry, J.D.; Ott, M.A.; Brames, M.J.; Einhorn, L.H. Perceptions of Masculinity and Self-Image in Adolescent and Young Adult Testicular Cancer Survivors: Implications for Romantic and Sexual Relationships. Psychooncology 2011, 20, 738. [Google Scholar] [CrossRef]
- Dax, V.; Ftanou, M.; Tran, B.; Lewin, J.; Wallace, R.; Seidler, Z.; Wiley, J.F. The Impact of Testicular Cancer and Its Treatment on Masculinity: A Systematic Review. Psychooncology 2022, 31, 1459. [Google Scholar] [CrossRef]
- Chapple, A.; McPherson, A. The Decision to Have a Prosthesis: A Qualitative Study of Men with Testicular Cancer. Psychooncology 2004, 13, 654–664. [Google Scholar] [CrossRef] [PubMed]
- Catanzariti, F.; Polito, B.; Polito, M. Testicular Prosthesis: Patient Satisfaction and Sexual Dysfunctions in Testis Cancer Survivors. Arch. Ital. Urol. Androl. 2016, 88, 186–188. [Google Scholar] [CrossRef] [PubMed]
- Yossepowitch, O.; Aviv, D.; Wainchwaig, L.; Baniel, J. Testicular Prostheses for Testis Cancer Survivors: Patient Perspectives and Predictors of Long-Term Satisfaction. J. Urol. 2011, 186, 2249–2252. [Google Scholar] [CrossRef] [PubMed]
- Kirchhoff, A.C.; Fowler, B.; Warner, E.L.; Pannier, S.T.; Fair, D.; Spraker-Perlman, H.; Yancey, J.; Bott, B.; Reynolds, C.; Lor Randall, R. Supporting Adolescents and Young Adults with Cancer: Oncology Provider Perceptions of Adolescent and Young Adult Unmet Needs. J. Adolesc. Young Adult Oncol. 2017, 6, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Jonker-Pool, G.; Hoekstra, H.J.; Van Imhoff, G.W.; Sonneveld, D.J.A.; Sleijfer, D.T.; Van Driel, M.F.; Koops, H.S.; Van De Wiel, H.B.M. Male Sexuality after Cancer Treatment—Needs for Information and Support: Testicular Cancer Compared to Malignant Lymphoma. Patient Educ. Couns. 2004, 52, 143–150. [Google Scholar] [CrossRef]
- Rowland, D.L.; Kolba, T.N. The Burden of Sexual Problems: Perceived Effects on Men’s and Women’s Sexual Partners. J. Sex Res. 2017, 55, 226–235. [Google Scholar] [CrossRef]
- Cancer.Net. The Importance of Follow-Up Care. Available online: https://www.cancer.net/survivorship/follow-care-after-cancer-treatment/importance-follow-care (accessed on 1 October 2021).
- Albers, L.F.; Bergsma, F.B.; Mekelenkamp, H.; Pelger, R.C.M.; Manten-Horst, E.; Elzevier, H.W. Discussing Sexual Health with Adolescent and Young Adults with Cancer: A Qualitative Study among Healthcare Providers. J. Cancer Educ. 2020, 37, 133–140. [Google Scholar] [CrossRef] [PubMed]
- van der Baan, F.H.; Koldenhof, J.J.; de Nijs, E.J.; Echteld, M.A.; Zweers, D.; Hesselmann, G.M.; Vervoort, S.C.; Vos, J.B.; de Graaf, E.; Witteveen, P.O.; et al. Validation of the Dutch Version of the Edmonton Symptom Assessment System. Cancer Med. 2020, 9, 6111–6121. [Google Scholar] [CrossRef] [PubMed]
- Weinfurt, K.P.; Lin, L.; Bruner, D.W.; Cyranowski, J.M.; Dombeck, C.B.; Hahn, E.A.; Jeffery, D.D.; Luecht, R.M.; Magasi, S.; Porter, L.S.; et al. Development and Initial Validation of the PROMIS® Sexual Function and Satisfaction Measures Version 2.0. J. Sex. Med. 2015, 12, 1961–1974. [Google Scholar] [CrossRef] [PubMed]
- Sopfe, J.; Marsh, R.; Ziniel, S.I.; Klosky, J.L.; Chow, E.J.; Holliman, B.D.; Peterson, P.N. Evaluation of the v2.0 Brief Profiles for Sexual Function and Satisfaction PROMIS in Adolescent and Young Adult Childhood Cancer Survivors. J. Adolesc. Young Adult Oncol. 2021, 10, 418–424. [Google Scholar] [CrossRef]
- Bruera, E.; Kuehn, N.; Miller, M.J.; Selmser, P.; Macmillan, K. The Edmonton Symptom Assessment System (ESAS): A Simple Method for the Assessment of Palliative Care Patients. J. Palliat. Care 1991, 7, 6–9. [Google Scholar] [CrossRef]

{kind=link}
| Main Topic | Questions, Probes, and Subtopics |
|---|---|
| Diagnosis of TGCT | What affect had the diagnosis of testicular cancer on your life? |
| Late effects regarding sexuality | What changes have you noticed related to sexuality after your treatment?
|
| Value of sexuality in daily life | What is for you the value of sexuality?
|
| Relationships | What kind of change have you noticed in relationships in general?
|
| Discuss sexuality during consultation | Which topics related to sexuality do you think are important to talk about during the consultation?
|
| Characteristic | n (=13) |
|---|---|
| Age 1 (years) (mean, min–max) | 30.3 (19–43) |
| Native country (n, %) | |
| The Netherlands | 13 (100) |
| Marital status 1 (n, %) | |
| Single | 3 (23.1) |
| Relationship/with a partner | 8 (61.5) |
| Married | 2 (15.4) |
| Sexual orientation (n, %) | |
| Heterosexual | 12 (92.3) |
| Homosexual | 1 (7.7) |
| Stage of cancer (n, %) | |
| Stage 1 | 6 (46.2) |
| Stage 2 | 2 (15.4) |
| Stage 3 | 5 (38.5) |
| Treatment type 2 (n, %) | |
| Single radical orchidectomy | 12 (92.3) |
| Double radical orchidectomy | 1 (7.7) |
| Chemotherapy | 6 (46.2) |
| Radiotherapy | 2 (15.4) |
| Additional surgery | 1 (7.7) |
| Follow-up time 1 (months) (mean, min-max) | 32.4 (9–58) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuiper, S.T.; Zweers, D.; Suelmann, B.B.M.; Meijer, R.P.; Vervoort, S.C.J.M. Perspectives and Concerns on Late Effects Regarding Sexuality among Adolescents and Young Adults Treated for Testicular Germ Cell Tumor: The PRICELESS-Study—A Qualitative Study. Cancers 2024, 16, 715. https://doi.org/10.3390/cancers16040715
Kuiper ST, Zweers D, Suelmann BBM, Meijer RP, Vervoort SCJM. Perspectives and Concerns on Late Effects Regarding Sexuality among Adolescents and Young Adults Treated for Testicular Germ Cell Tumor: The PRICELESS-Study—A Qualitative Study. Cancers. 2024; 16(4):715. https://doi.org/10.3390/cancers16040715
Chicago/Turabian StyleKuiper, Stefan T., Daniëlle Zweers, Britt B. M. Suelmann, Richard P. Meijer, and Sigrid C. J. M. Vervoort. 2024. "Perspectives and Concerns on Late Effects Regarding Sexuality among Adolescents and Young Adults Treated for Testicular Germ Cell Tumor: The PRICELESS-Study—A Qualitative Study" Cancers 16, no. 4: 715. https://doi.org/10.3390/cancers16040715
APA StyleKuiper, S. T., Zweers, D., Suelmann, B. B. M., Meijer, R. P., & Vervoort, S. C. J. M. (2024). Perspectives and Concerns on Late Effects Regarding Sexuality among Adolescents and Young Adults Treated for Testicular Germ Cell Tumor: The PRICELESS-Study—A Qualitative Study. Cancers, 16(4), 715. https://doi.org/10.3390/cancers16040715