
Time Relationship between the Occurrence of a Thromboembolic Event and the Diagnosis of Hematological Malignancies


Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Delluc, A.; Ianotto, J.-C.; Tromeur, C.; De Moreuil, C.; Couturaud, F.; Lacut, K.; Le Moigne, E.; Louis, P.; Thereaux, J.; Metges, J.-P.; et al. Real-World Incidence of Cancer Following a First Unprovoked Venous Thrombosis: Results from the EPIGETBO Study. Thromb. Res. 2018, 164, 79–84. [Google Scholar] [CrossRef] [PubMed]
- White, R.H.; Chew, H.K.; Zhou, H.; Parikh-Patel, A.; Harris, D.; Harvey, D.; Wun, T. Incidence of Venous Thromboembolism in the Year Before the Diagnosis of Cancer in 528 693 Adults. Arch. Intern. Med. 2005, 165, 1782. [Google Scholar] [CrossRef] [PubMed]
- Douketis, J.D.; Gu, C.; Piccioli, A.; Ghirarduzzi, A.; Pengo, V.; Prandoni, P. The Long-Term Risk of Cancer in Patients with a First Episode of Venous Thromboembolism. J. Thromb. Haemost. 2009, 7, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Taccone, F.S.; Jeangette, S.M.; Blecic, S.A. First-Ever Stroke as Initial Presentation of Systemic Cancer. J. Stroke Cerebrovasc. Dis. 2008, 17, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Selvik, H.A.; Bjerkreim, A.T.; Thomassen, L.; Waje-Andreassen, U.; Naess, H.; Kvistad, C.E. When to Screen Ischaemic Stroke Patients for Cancer. Cerebrovasc. Dis. 2018, 45, 42–47. [Google Scholar] [CrossRef]
- Quintas, S.; Rogado, J.; Gullón, P.; Pacheco-Barcia, V.; Dotor García-Soto, J.; Reig-Roselló, G.; Mondéjar, R.; Colomer, R.; Vivancos, J. Predictors of Unknown Cancer in Patients with Ischemic Stroke. J. Neurooncol. 2018, 137, 551–557. [Google Scholar] [CrossRef]
- Robertson, L.; Yeoh, S.E.; Stansby, G.; Agarwal, R. Effect of Testing for Cancer on Cancer- and Venous Thromboembolism (VTE)-Related Mortality and Morbidity in People with Unprovoked VTE. Cochrane Database Syst. Rev. 2017, 8, CD010837. [Google Scholar] [CrossRef]
- Fang, J.; Wu, J.; Hong, G.; Zheng, L.; Yu, L.; Liu, X.; Lin, P.; Yu, Z.; Chen, D.; Lin, Q.; et al. Cancer Screening in Hospitalized Ischemic Stroke Patients: A Multicenter Study Focused on Multiparametric Analysis to Improve Management of Occult Cancers. EPMA J. 2024, 15, 53–66. [Google Scholar] [CrossRef]
- Pernod, G.; Cohen, A.; Mismetti, P.; Sanchez, O.; Mahé, I.; Innovte Cat Working Group. Cancer-Related Arterial Thromboembolic Events. Arch. Cardiovasc. Dis. 2024, 117, 101–113. [Google Scholar] [CrossRef]
- Martens, K.L.; Li, A.; La, J.; May, S.B.; Swinnerton, K.N.; Tosi, H.; Elbers, D.C.; Do, N.V.; Brophy, M.T.; Gaziano, J.M.; et al. Epidemiology of Cancer-Associated Venous Thromboembolism in Patients With Solid and Hematologic Neoplasms in the Veterans Affairs Health Care System. JAMA Netw. Open 2023, 6, e2317945. [Google Scholar] [CrossRef]
- Miroddi, M.; Sterrantino, C.; Simmonds, M.; Caridi, L.; Calapai, G.; Phillips, R.S.; Stewart, L.A. Systematic Review and Meta-analysis of the Risk of Severe and Life-threatening Thromboembolism in Cancer Patients Receiving anti-EGFR Monoclonal Antibodies (Cetuximab or Panitumumab). Int. J. Cancer 2016, 139, 2370–2380. [Google Scholar] [CrossRef] [PubMed]
- Arnold, D.; Fuchs, C.S.; Tabernero, J.; Ohtsu, A.; Zhu, A.X.; Garon, E.B.; Mackey, J.R.; Paz-Ares, L.; Baron, A.D.; Okusaka, T.; et al. Meta-Analysis of Individual Patient Safety Data from Six Randomized, Placebo-Controlled Trials with the Antiangiogenic VEGFR2-Binding Monoclonal Antibody Ramucirumab. Ann. Oncol. 2017, 28, 2932–2942. [Google Scholar] [CrossRef] [PubMed]
- Haguet, H.; Douxfils, J.; Mullier, F.; Chatelain, C.; Graux, C.; Dogné, J.-M. Risk of Arterial and Venous Occlusive Events in Chronic Myeloid Leukemia Patients Treated with New Generation BCR-ABL Tyrosine Kinase Inhibitors: A Systematic Review and Meta-Analysis. Expert Opin. Drug Saf. 2017, 16, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.P.; Hisada, Y.M.; Kasthuri, R.S.; Reeves, B.N.; Mackman, N. Cancer Therapy–Associated Thrombosis. ATVB 2021, 41, 1291–1305. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, J.; Lenihan, D.; Armenian, S.; Barac, A.; Blaes, A.; Cardinale, D.; Carver, J.; Dent, S.; Ky, B.; Lyon, A.R.; et al. Defining Cardiovascular Toxicities of Cancer Therapies: An International Cardio-Oncology Society (IC-OS) Consensus Statement. Eur. Heart J. 2021, 43, 280–299. [Google Scholar] [CrossRef]
- Sørensen, H.T.; Pedersen, L.; van Es, N.; Büller, H.R.; Horváth-Puhó, E. Impact of Venous Thromboembolism on the Mortality in Patients with Cancer: A Population-Based Cohort Study. Lancet Reg. Health Eur. 2023, 34, 100739. [Google Scholar] [CrossRef]
- Mulder, F.I.; Horváth-Puhó, E.; van Es, N.; Pedersen, L.; Büller, H.R.; Bøtker, H.E.; Sørensen, H.T. Arterial Thromboembolism in Cancer Patients: A Danish Population-Based Cohort Study. JACC CardioOncol. 2021, 3, 205–218. [Google Scholar] [CrossRef]
- Hsu, C.; Patell, R.; Zwicker, J.I. The Prevalence of Thrombocytopenia in Patients with Acute Cancer-Associated Thrombosis. Blood Adv. 2023, 7, 4721–4727. [Google Scholar] [CrossRef]
- Wang, T.-F.; Leader, A.; Sanfilippo, K.M. Thrombosis and Bleeding in Hematological Malignancy. Best. Pract. Res. Clin. Haematol. 2022, 35, 101353. [Google Scholar] [CrossRef]
- Giustozzi, M.; Connors, J.M.; Ruperez Blanco, A.B.; Szmit, S.; Falvo, N.; Cohen, A.T.; Huisman, M.; Bauersachs, R.; Dentali, F.; Becattini, C.; et al. Clinical Characteristics and Outcomes of Incidental Venous Thromboembolism in Cancer Patients: Insights from the Caravaggio Study. J. Thromb. Haemost. 2021, 19, 2751–2759. [Google Scholar] [CrossRef]
- Navi, B.B.; Reiner, A.S.; Kamel, H.; Iadecola, C.; Okin, P.M.; Elkind, M.S.V.; Panageas, K.S.; DeAngelis, L.M. Risk of Arterial Thromboembolism in Patients With Cancer. J. Am. Coll. Cardiol. 2017, 70, 926–938. [Google Scholar] [CrossRef] [PubMed]
- Giustozzi, M.; Agnelli, G.; del Toro-Cervera, J.; Klok, F.A.; Rosovsky, R.P.; Martin, A.-C.; Herold, J.; Tzoran, I.; Szmit, S.; Bertoletti, L.; et al. Direct Oral Anticoagulants for the Treatment of Acute Venous Thromboembolism Associated with Cancer: A Systematic Review and Meta-Analysis. Thromb. Haemost. 2020, 120, 1128–1136. [Google Scholar] [CrossRef] [PubMed]
- Falanga, A.; Leader, A.; Ambaglio, C.; Bagoly, Z.; Castaman, G.; Elalamy, I.; Lecumberri, R.; Niessner, A.; Pabinger, I.; Szmit, S.; et al. EHA Guidelines on Management of Antithrombotic Treatments in Thrombocytopenic Patients With Cancer. HemaSphere 2022, 6, e750. [Google Scholar] [CrossRef] [PubMed]
- Bohacekova, M.; Kaldararova, M.; Valkovicova, T.; Remkova, A.; Vesely, J.; Simkova, I. Risk Factors Detection in Chronic Thromboembolic Pulmonary Hypertension, a Tool for Risk Quantification? Bratisl. Lekárske Listy 2016, 117, 577–582. [Google Scholar] [CrossRef]
- Montani, D.; Thoré, P.; Mignard, X.; Jaïs, X.; Boucly, A.; Jevnikar, M.; Seferian, A.; Jutant, E.-M.; Cottin, V.; Fadel, E.; et al. Clinical Phenotype and Outcomes of Pulmonary Hypertension Associated with Myeloproliferative Neoplasms: A Population-Based Study. Am. J. Respir. Crit. Care Med. 2023, 208, 600–612. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, A.; Scandura, J.; Masciulli, A.; Krichevsky, S.; Gavazzi, A.; Barbui, T. Prevalence and Risk Factors for Pulmonary Hypertension Associated with Chronic Myeloproliferative Neoplasms. Eur. J. Haematol. 2021, 106, 250–259. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. Eur. Heart J. 2022, 43, 3618–3731. [Google Scholar] [CrossRef]
- Falanga, A.; Ay, C.; Di Nisio, M.; Gerotziafas, G.; Jara-Palomares, L.; Langer, F.; Lecumberri, R.; Mandala, M.; Maraveyas, A.; Pabinger, I.; et al. Venous Thromboembolism in Cancer Patients: ESMO Clinical Practice Guideline. Ann. Oncol. 2023, 34, 452–467. [Google Scholar] [CrossRef]
- Key, N.S.; Khorana, A.A.; Kuderer, N.M.; Bohlke, K.; Lee, A.Y.Y.; Arcelus, J.I.; Wong, S.L.; Balaban, E.P.; Flowers, C.R.; Gates, L.E.; et al. Venous Thromboembolism Prophylaxis and Treatment in Patients With Cancer: ASCO Guideline Update. J. Clin. Oncol. 2023, 41, 3063–3071. [Google Scholar] [CrossRef]
- Sanfilippo, K.M.; Luo, S.; Wang, T.; Fiala, M.; Schoen, M.; Wildes, T.M.; Mikhael, J.; Kuderer, N.M.; Calverley, D.C.; Keller, J.; et al. Predicting Venous Thromboembolism in Multiple Myeloma: Development and Validation of the IMPEDE VTE Score. Am. J Hematol. 2019, 94, 1176–1184. [Google Scholar] [CrossRef]
- Khorana, A.A.; Kuderer, N.M.; Culakova, E.; Lyman, G.H.; Francis, C.W. Development and Validation of a Predictive Model for Chemotherapy-Associated Thrombosis. Blood 2008, 111, 4902–4907. [Google Scholar] [CrossRef] [PubMed]
- Khorana, A.A.; Soff, G.A.; Kakkar, A.K.; Vadhan-Raj, S.; Riess, H.; Wun, T.; Streiff, M.B.; Garcia, D.A.; Liebman, H.A.; Belani, C.P.; et al. Rivaroxaban for Thromboprophylaxis in High-Risk Ambulatory Patients with Cancer. N. Engl. J. Med. 2019, 380, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Carrier, M.; Abou-Nassar, K.; Mallick, R.; Tagalakis, V.; Shivakumar, S.; Schattner, A.; Kuruvilla, P.; Hill, D.; Spadafora, S.; Marquis, K.; et al. Apixaban to Prevent Venous Thromboembolism in Patients with Cancer. N. Engl. J. Med. 2019, 380, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Paterno, G.; Palmieri, R.; Forte, V.; Del Prete, V.; Gurnari, C.; Guarnera, L.; Mallegni, F.; Pascale, M.R.; Buzzatti, E.; Mezzanotte, V.; et al. Predictors of Early Thrombotic Events in Adult Patients with Acute Myeloid Leukemia: A Real-World Experience. Cancers 2022, 14, 5640. [Google Scholar] [CrossRef] [PubMed]
- Lyman, G.H.; Eckert, L.; Wang, Y.; Wang, H.; Cohen, A. Venous Thromboembolism Risk in Patients With Cancer Receiving Chemotherapy: A Real-World Analysis. Oncologist 2013, 18, 1321–1329. [Google Scholar] [CrossRef]
- Libourel, E.J.; Klerk, C.P.W.; van Norden, Y.; de Maat, M.P.M.; Kruip, M.J.; Sonneveld, P.; Löwenberg, B.; Leebeek, F.W.G. Disseminated Intravascular Coagulation at Diagnosis Is a Strong Predictor for Thrombosis in Acute Myeloid Leukemia. Blood 2016, 128, 1854–1861. [Google Scholar] [CrossRef]
- Khorana, A.A. Venous Thromboembolism and Prognosis in Cancer. Thromb. Res. 2010, 125, 490–493. [Google Scholar] [CrossRef]
- Ku, G.H.; White, R.H.; Chew, H.K.; Harvey, D.J.; Zhou, H.; Wun, T. Venous Thromboembolism in Patients with Acute Leukemia: Incidence, Risk Factors, and Effect on Survival. Blood 2009, 113, 3911–3917. [Google Scholar] [CrossRef] [PubMed]
- Faiz, A.S.; Sridharan, A.; Guo, S.; Lin, Y.; Philipp, C.S. Risk Factors and Mortality Associated with Venous Thromboembolism in the Elderly US Population with Acute Lymphocytic Leukemia. Thromb. Update 2024, 14, 100155. [Google Scholar] [CrossRef]
- Johannesdottir, S.A.; Horváth-Puhó, E.; Dekkers, O.M.; Cannegieter, S.C.; Jørgensen, J.O.L.; Ehrenstein, V.; Vandenbroucke, J.P.; Pedersen, L.; Sørensen, H.T. Use of Glucocorticoids and Risk of Venous Thromboembolism: A Nationwide Population-Based Case-Control Study. JAMA Intern. Med. 2013, 173, 743. [Google Scholar] [CrossRef]
- Orsi, F.A.; Lijfering, W.M.; Geersing, G.; Rosendaal, F.R.; Dekkers, O.M.; Le Cessie, S.; Cannegieter, S.C. Glucocorticoid Use and Risk of First and Recurrent Venous Thromboembolism: Self-controlled Case-series and Cohort Study. Br. J. Haematol. 2021, 193, 1194–1202. [Google Scholar] [CrossRef]
- Raskob, G.E.; van Es, N.; Verhamme, P.; Carrier, M.; Di Nisio, M.; Garcia, D.; Grosso, M.A.; Kakkar, A.K.; Kovacs, M.J.; Mercuri, M.F.; et al. Edoxaban for the Treatment of Cancer-Associated Venous Thromboembolism. N. Engl. J. Med. 2018, 378, 615–744. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Becattini, C.; Meyer, G.; Muñoz, A.; Huisman, M.V.; Connors, J.M.; Cohen, A.; Bauersachs, R.; Brenner, B.; Torbicki, A.; et al. Apixaban for the Treatment of Venous Thromboembolism Associated with Cancer. N. Engl. J. Med. 2020, 382, 1599–1607. [Google Scholar] [CrossRef]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. 2022 ESC Guidelines on Cardio-Oncology Developed in Collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur. Heart J. 2022, 43, 4229–4361. [Google Scholar] [CrossRef]
- Giustozzi, M.; Curcio, A.; Weijs, B.; Field, T.S.; Sudikas, S.; Katholing, A.; Wallenhorst, C.; Weitz, J.I.; Martinez, C.; Cohen, A.T. Variation in the Association between Antineoplastic Therapies and Venous Thromboembolism in Patients with Active Cancer. Thromb. Haemost. 2020, 120, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, J. Vascular Toxic Effects of Cancer Therapies. Nat. Rev. Cardiol. 2020, 17, 503–522. [Google Scholar] [CrossRef] [PubMed]
- Verso, M.; Agnelli, G.; Munoz, A.; Connors, J.M.; Sanchez, O.; Huisman, M.; Brenner, B.; Gussoni, G.; Cohen, A.T.; Becattini, C. Recurrent Venous Thromboembolism and Major Bleeding in Patients with Localised, Locally Advanced or Metastatic Cancer: An Analysis of the Caravaggio Study. Eur. J. Cancer 2022, 165, 136–145. [Google Scholar] [CrossRef]
- Feldman, S.; Gupta, D.; Navi, B.B.; Grace Ho, K.-W.; Willeit, P.; Devlin, S.; Bolton, K.L.; Arcila, M.E.; Mantha, S. Tumor Genomic Profile Is Associated With Arterial Thromboembolism Risk in Patients With Solid Cancer. JACC CardioOncol. 2023, 5, 246–255. [Google Scholar] [CrossRef]
- Moik, F.; Chan, W.-S.E.; Wiedemann, S.; Hoeller, C.; Tuchmann, F.; Aretin, M.-B.; Fuereder, T.; Zöchbauer-Müller, S.; Preusser, M.; Pabinger, I.; et al. Incidence, Risk Factors, and Outcomes of Venous and Arterial Thromboembolism in Immune Checkpoint Inhibitor Therapy. Blood 2021, 137, 1669–1678. [Google Scholar] [CrossRef]
- Mulder, F.I.; Horváth-Puhó, E.; van Es, N.; van Laarhoven, H.W.M.; Pedersen, L.; Moik, F.; Ay, C.; Büller, H.R.; Sørensen, H.T. Venous Thromboembolism in Cancer Patients: A Population-Based Cohort Study. Blood 2021, 137, 1959–1969. [Google Scholar] [CrossRef]
- Wang, J.; Kim, Y.D.; Kim, C.H. Incidence and Risk of Various Types of Arterial Thromboembolism in Patients With Cancer. Mayo Clin. Proc. 2021, 96, 592–600. [Google Scholar] [CrossRef] [PubMed]
- Aboumsallem, J.P.; Moslehi, J.; de Boer, R.A. Reverse Cardio-Oncology: Cancer Development in Patients With Cardiovascular Disease. J. Am. Heart Assoc. 2020, 9, e013754. [Google Scholar] [CrossRef]
- Imran, S.; Rao, M.S.; Shah, M.H.; Gaur, A.; Guernaoui, A.E.; Roy, S.; Roy, S.; Bharadwaj, H.R.; Awuah, W.A. Evolving Perspectives in Reverse Cardio-Oncology: A Review of Current Status, Pathophysiological Insights, and Future Directives. Curr. Probl. Cardiol. 2024, 49, 102389. [Google Scholar] [CrossRef]
- Liang, Z.; He, Y.; Hu, X. Cardio-Oncology: Mechanisms, Drug Combinations, and Reverse Cardio-Oncology. Int. J. Mol. Sci. 2022, 23, 10617. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.; Bavishi, A.; Hibler, E.A.; Yang, E.H.; Parashar, S.; Okwuosa, T.; DeCara, J.M.; Brown, S.-A.; Guha, A.; Sadler, D.; et al. Interconnected Clinical and Social Risk Factors in Breast Cancer and Heart Failure. Front. Cardiovasc. Med. 2022, 9, 847975. [Google Scholar] [CrossRef]
- Di Fusco, S.A.; Cianfrocca, C.; Bisceglia, I.; Spinelli, A.; Alonzo, A.; Mocini, E.; Gulizia, M.M.; Gabrielli, D.; Oliva, F.; Imperoli, G.; et al. Potential Pathophysiologic Mechanisms Underlying the Inherent Risk of Cancer in Patients with Atherosclerotic Cardiovascular Disease. Int. J. Cardiol. 2022, 363, 190–195. [Google Scholar] [CrossRef]
- Koelwyn, G.J.; Aboumsallem, J.P.; Moore, K.J.; de Boer, R.A. Reverse Cardio-Oncology: Exploring the Effects of Cardiovascular Disease on Cancer Pathogenesis. J. Mol. Cell Cardiol. 2022, 163, 1–8. [Google Scholar] [CrossRef] [PubMed]
- de Wit, S.; de Boer, R.A. From Studying Heart Disease and Cancer Simultaneously to Reverse Cardio-Oncology. Circulation 2021, 144, 93–95. [Google Scholar] [CrossRef]
- Lyon, A.R.; Dent, S.; Stanway, S.; Earl, H.; Brezden-Masley, C.; Cohen-Solal, A.; Tocchetti, C.G.; Moslehi, J.J.; Groarke, J.D.; Bergler-Klein, J.; et al. Baseline cardiovascular risk assessment in cancer patients scheduled to receive cardiotoxic cancer therapies: A position statement and new risk assessment tools from the Cardio-Oncology Study Group of the Heart Failure Association of the European Society of Cardiology in collaboration with the International Cardio-Oncology Society. Eur. J. Heart Fail. 2020, 22, 1945–1960. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Number | Percentage | ||
|---|---|---|---|
| Sex | Men | 673 | 52.46 |
| Older age | ≥70 years | 390 | 30.4 |
| Hematological malignancies | AML | 270 | 21.04 |
| NHL | 250 | 19.49 | |
| MM | 223 | 17,38 | |
| CLL | 101 | 7.87 | |
| ALL | 76 | 5.92 | |
| MDS | 70 | 5.46 | |
| HL | 56 | 4.36 | |
| CML | 51 | 3.98 | |
| Chronic myeloproliferative disease | 48 | 3.74 | |
| Other rarer (together) | 138 | ||
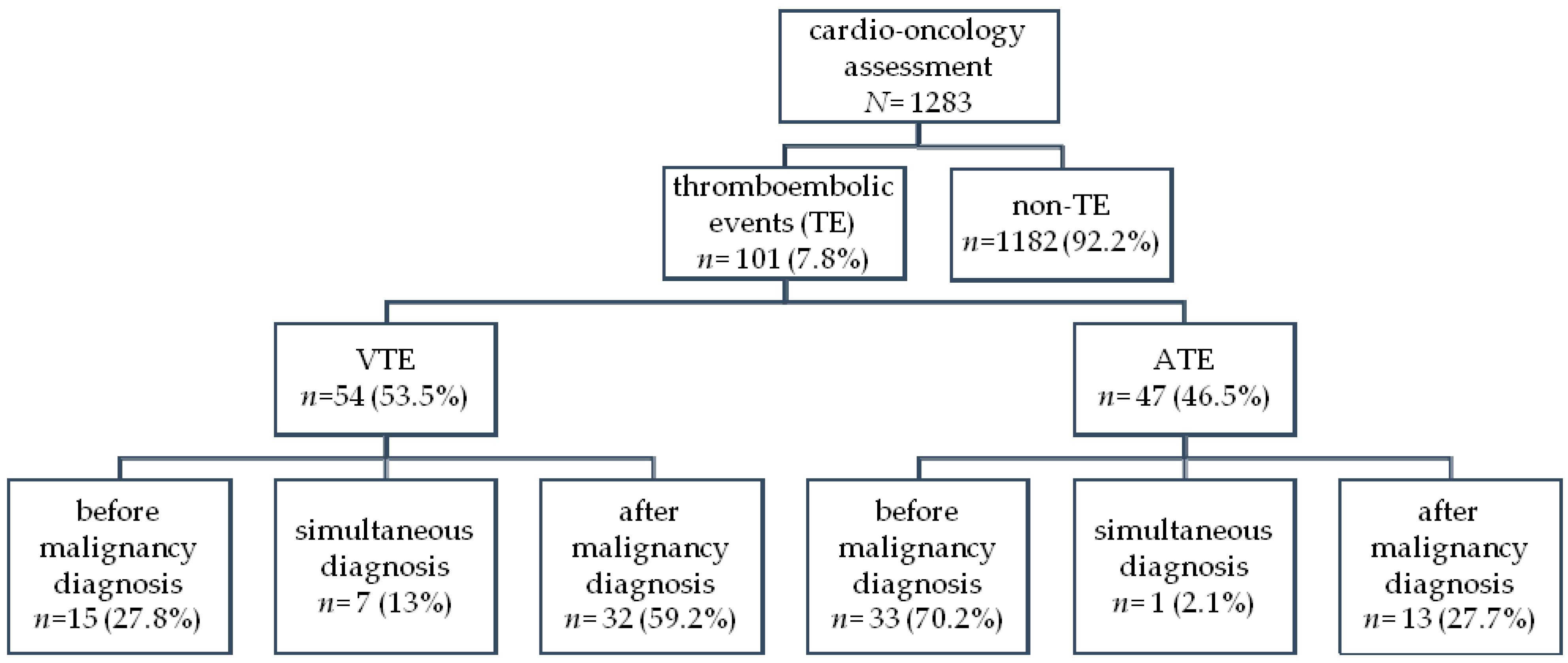
| Thromboembolism | All | 101 | 7.87 |
| VTE | 54 | 4.21 | |
| ATE | 47 | 3.66 | |
| Coexisting diseases | Hypertension | 521 | 40.61 |
| Arrhythmia | 203 | 15.82 | |
| AF | 105 | 8.18 | |
| HF | 142 | 11.07 | |
| IHD | 107 | 8.34 | |
| DM | 128 | 9.98 |
| VTE | ATE | |||
|---|---|---|---|---|
| Frequency | p-Value | Frequency | p-Value | |
| All | 54 of 1283 4.21% | - | 47 of 1283 3.66% | - |
| AML | 17 of 270 6.30% | 0.055 | 8 of 270 2.96% | 0.491 |
| NHL | 7 of 250 2.80% | 0.216 | 6 of 250 2.40% | 0.236 |
| MM | 10 of 223 4.48% | 0.822 | 11 of 223 4.93% | 0.267 |
| CLL | 3 of 101 2.97% | 0.698 * | 6 of 101 5.94% | 0.204 |
| ALL | 7 of 76 9.21% | 0.025 | 2 of 76 2.63% | 0.858 * |
| MDS | 1 of 70 1.43% | 0.376 * | 3 of 70 4.29% | 0.966 * |
| HL | 0 of 56 0% | 0.206 * | 1 of 56 1.79% | 0.688 * |
| CML | 0 of 51 0% | 0.241 * | 4 of 51 7.84% | 0.215 * |
| Chronic myeloproliferative disease | 7 of 48 14.58% | 0.0003 | 4 of 48 8.33% | 0.173 * |
| All ATE | ATE before Diagnosis of Malignancy | ATE after Diagnosis of Malignancy | |
|---|---|---|---|
| Older age (≥70 y) | OR = 3.55 (1.96–6.44) p = 0.00003 | OR = 4.17 (2.03–8.57) p = 0.0001 | NS |
| Hypertension | OR = 4.5 (2.31–8.76) p < 0.00001 | OR=5.67 (2.44–13.16) p = 0.00005 | NS |
| Arrhythmia | OR = 2.61 (1.39–4.92) p = 0.003 | OR = 3.17 (1.53–6.55) p=0.002 | NS |
| AF | NS | NS | NS |
| HF | OR = 3.28 (1.69–6.38) p = 0.0004 | OR = 4.92 (2.37–10.24) p = 0.00002 | NS |
| IHD | OR = 83.74 (37.63–186.32) p < 0.00001 | OR = 108.94 (37.32–317.98) p < 0.00001 | OR = 30.21 (9.29–98.2) p < 0.00001 |
| DM | NS | NS | NS |
| All VTE | VTE before Diagnosis of Malignancy | VTE after Diagnosis of Malignancy | |
|---|---|---|---|
| AML | NS | NS | NS |
| ALL | OR = 2.5 (1.09–5.75) p = 0.03 | NS | OR = 3.05 (1.24–7.53) p = 0.015 |
| Chronic myeloproliferative disease | OR = 4.32 (1.84–10.13) p = 0.0008 | OR = 6.79 (1.85–24.95) p = 0.004 | OR = 3.12 (1.06–9.16) p = 0.04 |
| Older age (≥70 y) | NS | NS | NS |
| Hypertension | NS | NS | NS |
| Arrhythmia | NS | NS | NS |
| AF | NS | NS | NS |
| HF | NS | NS | NS |
| IHD | NS | NS | NS |
| DM | OR = 2.43 (1.22–4.85) p = 0.01 | NS | OR = 2.42 (1.09–5.38) p = 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kępski, J.; Szmit, S.; Lech-Marańda, E. Time Relationship between the Occurrence of a Thromboembolic Event and the Diagnosis of Hematological Malignancies. Cancers 2024, 16, 3196. https://doi.org/10.3390/cancers16183196
Kępski J, Szmit S, Lech-Marańda E. Time Relationship between the Occurrence of a Thromboembolic Event and the Diagnosis of Hematological Malignancies. Cancers. 2024; 16(18):3196. https://doi.org/10.3390/cancers16183196
Chicago/Turabian StyleKępski, Jarosław, Sebastian Szmit, and Ewa Lech-Marańda. 2024. "Time Relationship between the Occurrence of a Thromboembolic Event and the Diagnosis of Hematological Malignancies" Cancers 16, no. 18: 3196. https://doi.org/10.3390/cancers16183196
APA StyleKępski, J., Szmit, S., & Lech-Marańda, E. (2024). Time Relationship between the Occurrence of a Thromboembolic Event and the Diagnosis of Hematological Malignancies. Cancers, 16(18), 3196. https://doi.org/10.3390/cancers16183196