
Lung Cancer Subtyping: A Short Review


 ,
,  ,
, 
Abstract
Simple Summary
Abstract
1. Introduction
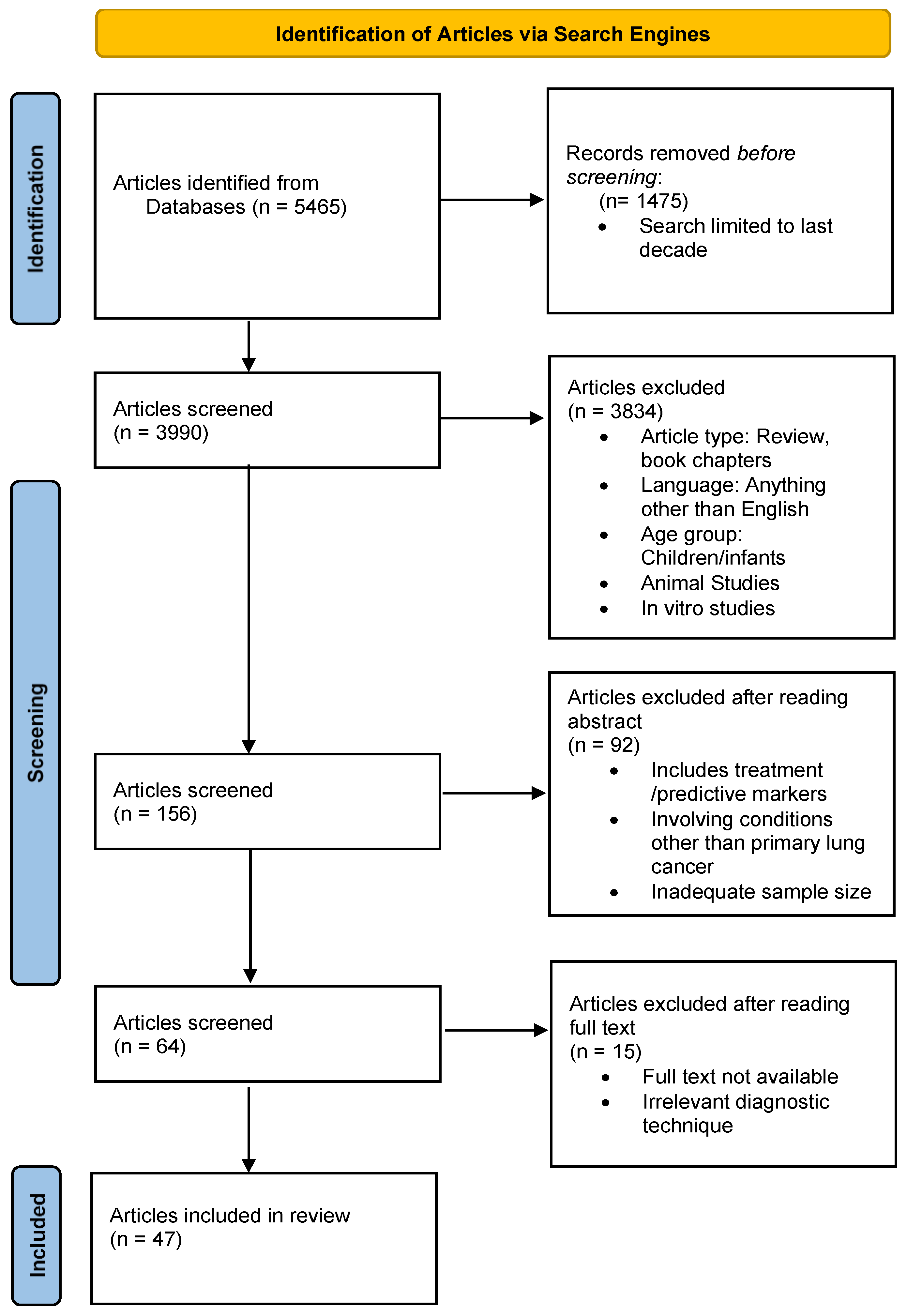
2. Search, Inclusion, and Exclusion Criteria
3. Immunohistochemical Markers
4. Omics Markers
4.1. Transcriptomics
4.2. Proteomics
4.3. Metabolomics
5. Discussion
6. Conclusions and Future Direction
Author Contributions
Funding
Conflicts of Interest
References
- Sharma, R. Mapping of global, regional and national incidence, mortality and mortality-to-incidence ratio of lung cancer in 2020 and 2050. Int. J. Clin. Oncol. 2022, 27, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Thandra, K.C.; Barsouk, A.; Saginala, K.; Aluru, J.S.; Barsouk, A. Epidemiology of lung cancer. Współczesna Onkol. 2021, 25, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Belluomini, L.; Calvetti, L.; Inno, A.; Pasello, G.; Roca, E.; Vattemi, E.; Veccia, A.; Menis, J.; Pilotto, S. SCLC Treatment in the Immuno-Oncology Era: Current Evidence and Unmet Needs. Front. Oncol. 2022, 12, 840783. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Yu, Q.; Song, T.; Wang, Z.; Song, L.; Yang, Y.; Shao, J.; Li, J.; Ni, Y.; Chao, N.; et al. The heterogeneous immune landscape between lung adenocarcinoma and squamous carcinoma revealed by single-cell RNA sequencing. Signal Transduct. Target. Ther. 2022, 7, 289. [Google Scholar] [CrossRef] [PubMed]
- Khodabakhshi, Z.; Mostafaei, S.; Arabi, H.; Oveisi, M.; Shiri, I.; Zaidi, H. Non-small cell lung carcinoma histopathological subtype phenotyping using high-dimensional multinomial multiclass CT radiomics signature. Comput. Biol. Med. 2021, 136, 104752. [Google Scholar] [CrossRef] [PubMed]
- Yabroff, K.R.; Mariotto, A.; Tangka, F.; Zhao, J.; Islami, F.; Sung, H.; Sherman, R.L.; Henley, S.J.; Jemal, A.; Ward, E.M. Annual Report to the Nation on the Status of Cancer, Part 2: Patient Economic Burden Associated With Cancer Care. JNCI J. Natl. Cancer Inst. 2021, 113, 1670–1682. [Google Scholar] [CrossRef] [PubMed]
- Abdullah, D.M.; Ahmed, N.S.; Abdullah, D.M.; Ahmed, N. A Review of most Recent Lung Cancer Detection Techniques using Machine Learning. Int. J. Sci. Bus. 2021, 5, 159–173. [Google Scholar]
- Lamberti, G.; Andrini, E.; Sisi, M.; Rizzo, A.; Parisi, C.; Di Federico, A.; Gelsomino, F.; Ardizzoni, A. Beyond EGFR, ALK and ROS1: Current evidence and future perspectives on newly targetable oncogenic drivers in lung adenocarcinoma. Crit. Rev. Oncol. Hematol. 2020, 156, 103119. [Google Scholar] [CrossRef] [PubMed]
- Guo, H.; Zhang, J.; Qin, C.; Yan, H.; Liu, T.; Hu, H.; Tang, S.; Tang, S.; Zhou, H. Biomarker-Targeted Therapies in Non-Small Cell Lung Cancer: Current Status and Perspectives. Cells 2022, 11, 3200. [Google Scholar] [CrossRef] [PubMed]
- Majeed, U.; Manochakian, R.; Zhao, Y.; Lou, Y. Targeted therapy in advanced non-small cell lung cancer: Current advances and future trends. J. Hematol. Oncol. 2021, 14, 108. [Google Scholar] [CrossRef]
- Yuan, M.; Huang, L.L.; Chen, J.H.; Wu, J.; Xu, Q. The emerging treatment landscape of targeted therapy in non-small-cell lung cancer. Signal Transduct. Target. Ther. 2019, 4, 61. [Google Scholar] [CrossRef] [PubMed]
- Ning, J.; Ge, T.; Jiang, M.; Jia, K.; Wang, L.; Li, W.; Chen, B.; Liu, Y.; Wang, H.; Zhao, S.; et al. Early diagnosis of lung cancer: Which is the optimal choice? Aging 2021, 13, 6214–6227. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Dacic, S.; Wistuba, I.; Sholl, L.; Adusumilli, P.; Bubendorf, L.; Bunn, P.; Cascone, T.; Chaft, J.; Chen, G.; et al. IASLC Multidisciplinary Recommendations for Pathologic Assessment of Lung Cancer Resection Specimens After Neoadjuvant Therapy. J. Thorac. Oncol. 2020, 15, 709–740. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Liu, J.-B.; Hou, L.-K.; Yu, F.; Zhang, J.; Wu, W.; Tang, X.-M.; Sun, F.; Lu, H.-M.; Deng, J.; et al. Liquid biopsy in lung cancer: Significance in diagnostics, prediction, and treatment monitoring. Mol. Cancer 2022, 21, 25. [Google Scholar] [CrossRef] [PubMed]
- Casagrande, G.M.S.; Silva, M.D.O.; Reis, R.M.; Leal, L.F. Liquid Biopsy for Lung Cancer: Up-to-Date and Perspectives for Screening Programs. Int. J. Mol. Sci. 2023, 24, 2505. [Google Scholar] [CrossRef]
- Califf, R.M. Biomarker definitions and their applications. Exp. Biol. Med. 2018, 243, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Travis, W.D.; Brambilla, E.; Nicholson, A.G.; Yatabe, Y.; Austin, J.H.M.; Beasley, M.B.; Chirieac, L.R.; Dacic, S.; Duhig, E.; Flieder, D.B.; et al. The 2015 World Health Organization Classification of Lung Tumors. J. Thorac. Oncol. 2015, 10, 1243–1260. [Google Scholar] [CrossRef] [PubMed]
- Watkins, S. Immunohistochemistry. Curr. Protoc. Cytom. 2009, 48, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Yatabe, Y.; Dacic, S.; Borczuk, A.C.; Warth, A.; Russell, P.A.; Lantuejoul, S.; Beasley, M.B.; Thunnissen, E.; Pelosi, G.; Rekhtman, N.; et al. Best Practices Recommendations for Diagnostic Immunohistochemistry in Lung Cancer. J. Thorac. Oncol. 2019, 14, 377–407. [Google Scholar] [CrossRef] [PubMed]
- Osmani, L.; Askin, F.; Gabrielson, E.; Li, Q.K. Current WHO guidelines and the critical role of immunohistochemical markers in the subclassification of non-small cell lung carcinoma (NSCLC): Moving from targeted therapy to immunotherapy. Semin. Cancer Biol. 2018, 52, 103–109. [Google Scholar] [CrossRef]
- Bodaghi, A.; Fattahi, N.; Ramazani, A. Biomarkers: Promising and valuable tools towards diagnosis, prognosis and treatment of Covid-19 and other diseases. Heliyon 2023, 9, e13323. [Google Scholar] [CrossRef]
- Dong, Z.; Chen, Y. Transcriptomics: Advances and approaches. Sci. China Life Sci. 2013, 56, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Khodadadian, A.; Darzi, S.; Haghi-Daredeh, S.; Eshaghi, F.S.; Babakhanzadeh, E.; Mirabutalebi, S.H.; Nazari, M. Genomics and Transcriptomics: The Powerful Technologies in Precision Medicine. Int. J. Gen. Med. 2020, 13, 627–640. [Google Scholar] [CrossRef] [PubMed]
- Lowe, R.; Shirley, N.; Bleackley, M.; Dolan, S.; Shafee, T. Transcriptomics technologies. PLoS Comput. Biol. 2017, 13, e1005457. [Google Scholar] [CrossRef] [PubMed]
- Suhre, K.; McCarthy, M.I.; Schwenk, J.M. Genetics meets proteomics: Perspectives for large population-based studies. Nat. Rev. Genet. 2021, 22, 19–37. [Google Scholar] [CrossRef] [PubMed]
- Aslam, B.; Basit, M.; Nisar, M.A.; Khurshid, M.; Rasool, M.H. Proteomics: Technologies and Their Applications. J. Chromatogr. Sci. 2017, 55, 182–196. [Google Scholar] [CrossRef] [PubMed]
- Aizat, W.M.; Hassan, M. Proteomics in Systems Biology. Adv. Exp. Med. Biol. 2018, 1102, 31–49. [Google Scholar] [PubMed]
- Al-Amrani, S.; Al-Jabri, Z.; Al-Zaabi, A.; Alshekaili, J.; Al-Khabori, M. Proteomics: Concepts and applications in human medicine. World J. Biol. Chem. 2021, 12, 57–69. [Google Scholar] [CrossRef]
- Muthubharathi, B.C.; Gowripriya, T.; Balamurugan, K. Metabolomics: Small molecules that matter more. Mol. Omics 2021, 17, 210–229. [Google Scholar] [CrossRef]
- Clish, C.B. Metabolomics: An emerging but powerful tool for precision medicine. Cold Spring Harb. Mol. Case Stud 2015, 1, a000588. [Google Scholar] [CrossRef]
- Madama, D.; Martins, R.; Pires, A.S.; Botelho, M.F.; Alves, M.G.; Abrantes, A.M.; Cordeiro, C.R. Metabolomic Profiling in Lung Cancer: A Systematic Review. Metabolites 2021, 11, 630. [Google Scholar] [CrossRef] [PubMed]
- Segers, K.; Declerck, S.; Mangelings, D.; Heyden, Y.V.; Van Eeckhaut, A. Analytical techniques for metabolomic studies: A review. Bioanalysis 2019, 11, 2297–2318. [Google Scholar] [CrossRef] [PubMed]
- Argon, A.; Nart, D.; Veral, A.; Adenokarsinom, A. Skuamöz Hücreli Karsinom ve Küçük Hücreli Dışı Akciğer Kanserlerinde Sitokeratin 5/6, p63 ve TTF-1’in Değeri. Turk. Patoloji Derg. 2015, 31, 81–88. [Google Scholar] [PubMed]
- Kim, M.J.; Shin, H.C.; Shin, K.C.; Ro, J.Y. Best immunohistochemical panel in distinguishing adenocarcinoma from squamous cell carcinoma of lung: Tissue microarray assay in resected lung cancer specimens. Ann. Diagn. Pathol. 2013, 17, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Yassin, F.E.Z.S.E.D. Aldehyde dehyderogenase (ALDH1A1) delineating the normal and cancer stem cells in spectral lung lesions: An immunohistochemical appraisal. Pathol. Res. Pract. 2016, 212, 398–409. [Google Scholar] [CrossRef] [PubMed]
- Nishino, M.; Hoang, M.P.; Della Pelle, P.; Morales-Oyarvide, V.; Huynh, T.G.; Mark, E.J.; Mino-Kenudson, M. Napsin A/p40 antibody cocktail for subtyping non-small cell lung carcinoma on cytology and small biopsy specimens. Cancer Cytopathol. 2016, 124, 472–484. [Google Scholar] [CrossRef] [PubMed]
- Wei, K.; Ye, Z.; Li, Z.; Dang, Y.; Chen, X.; Huang, N.; Bao, C.; Gan, T.; Yang, L.; Chen, G. An immunohistochemical study of cyclin-dependent kinase 5 (CDK5) expression in non-small cell lung cancer (NSCLC) and small cell lung cancer (SCLC): A possible prognostic biomarker. World J. Surg. Oncol. 2016, 14, 34. [Google Scholar] [CrossRef]
- Guo, R.; Tian, Y.; Zhang, N.; Huang, H.; Huang, Y.; Yang, J. Use of dual-marker staining to differentiate between lung squamous cell carcinoma and adenocarcinoma. J. Int. Med. Res. 2019, 48, 300060519893867. [Google Scholar] [CrossRef] [PubMed]
- van Zyl, A.; Schubert, P.T.; Koegelenberg, C.F.N. The utility of TTF-1, napsin A, CK5 and p63 staining in the sub-classification of non-small cell carcinoma of the lung. Cytopathology 2019, 30, 586–591. [Google Scholar] [CrossRef] [PubMed]
- Ao, M.H.; Zhang, H.; Sakowski, L.; Sharma, R.; Illei, P.B.; Gabrielson, E.; Askin, F.; Li, Q.K. The utility of a novel triple marker (combination of TTF1, napsin A, and p40) in the subclassification of non-small cell lung cancer. Hum. Pathol. 2014, 45, 926–934. [Google Scholar] [CrossRef]
- Kawai, T.; Tominaga, S.; Hiroi, S.; Kameda, K.; Ogata, S.; Nakashima, H.; Ozeki, Y.; Nakanishi, K. Expressions of Thyroid Transcription Factor-1, Napsin A, p40, p63, CK5/6 and Desmocollin-3 in Non-Small Cell Lung Cancer, as Revealed by Imprint Cytology Using a Malinol-Based Cell-Transfer Technique. Acta Cytol. 2015, 59, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Tran, L.; Mattsson, J.S.M.; Nodin, B.; Jo, P.; Planck, M.; Jirstro, K.; Botling, J.; Micke, P.; Brunnstro, H. Various Antibody Clones of Napsin A, Thyroid Transcription Factor 1, and p40 and Comparisons With Cytokeratin 5 and p63 in Histopathologic Diagnostics of Non-Small Cell Lung Carcinoma. Appl. Immunohistochem. Mol. Morphol. 2016, 24, 648–659. Available online: www.appliedimmunohist.com (accessed on 5 March 2024). [CrossRef] [PubMed]
- Roudi, R.; Korourian, A.; Shariftabrizi, A.; Madjd, Z. Differential Expression of Cancer Stem Cell Markers ALDH1 and CD133 in Various Lung Cancer Subtypes. Cancer Investig. 2015, 33, 294–302. [Google Scholar] [CrossRef] [PubMed]
- Roudi, R.; Madjd, Z.; Korourian, A.; Mehrazma, M.; Molanae, S.; Sabet, M.N.; Shariftabrizi, A. Clinical significance of putative cancer stem cell marker CD44 in different histological subtypes of lung cancer. Cancer Biomark. 2014, 14, 457–467. [Google Scholar] [CrossRef] [PubMed]
- Geng, Q.; Fan, T.; Zhang, B.; Wang, W.; Xu, Y.; Hu, H. Five microRNAs in plasma as novel biomarkers for screening of early-stage non-small cell lung cancer. Respir. Res. 2014, 15, 149. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Kong, H.; Hou, Y.; Ge, D.; Huang, W.; Ou, J.; Yang, D.; Zhang, L.; Wu, G.; Song, Y. Two plasma microRNA panels for diagnosis and subtype discrimination of lung cancer. Lung Cancer 2018, 123, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.; Liu, Y.; Zhang, J.; Huang, W.; Jiang, H.; Hou, Y.; Xu, C.; Zhai, C.; Gao, X.; Wang, S. The expression of miR-375 is associated with carcinogenesis in three subtypes of lung cancer. PLoS ONE 2015, 10, e0144187. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zhang, Q.; Zhang, M.; Su, W.; Wang, Z.; Li, Y.; Zhang, J.; Beer, D.G.; Yang, S.; Chen, G. Serum microRNA signature is capable of early diagnosis for non-small cell lung cancer. Int. J. Biol. Sci. 2019, 15, 1712. [Google Scholar] [CrossRef]
- Zhang, X.; Tan, J.; Chen, Y.; Ma, S.; Bai, W.; Peng, Y.; Shi, G. Identification of serum MiRNAs as candidate biomarkers for non-small cell lung cancer diagnosis. BMC Pulm. Med. 2022, 22, 479. [Google Scholar] [CrossRef] [PubMed]
- Powrózek, T.; Krawczyk, P.; Kowalski, D.M.; Winiarczyk, K.; Olszyna-Serementa, M.; Milanowski, J. Plasma circulating and microRNA-944 microRNA-3662 as potential histologic type-specific early lung cancer biomarkers. Transl. Res. 2015, 166, 315–323. [Google Scholar] [CrossRef]
- Singh, A.; Kant, R.; Saluja, T.; Tripathi, T.; Srivastava, K.; Naithani, M.; Gupta, A.; Mirza, A.; Prakash, V.; Singh, S. Differential diagnosis of non-small cell lung carcinoma by circulating microRNA. J. Cancer Res. Ther. 2020, 16, 127. [Google Scholar] [PubMed]
- Kumar, S.; Sharawat, S.K.; Ali, A.; Gaur, V.; Malik, P.S.; Kumar, S.; Mohan, A.; Guleria, R. Identification of differentially expressed circulating serum microRNA for the diagnosis and prognosis of Indian non–small cell lung cancer patients. Curr. Probl. Cancer 2020, 44, 100540. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Saikia, J.; Sharawat, S.K.; Malik, P.S.; Kumar, S.; Mohan, A. Analysis of miR-375-3p, miR-197-3p, and miR-15a-5p Expression and Their Clinical Relevance as Biomarkers in Lung Cancer. Technol. Cancer Res. Treat. 2022, 21, 15330338221080980. [Google Scholar] [CrossRef]
- Nadal, E.; Truini, A.; Nakata, A.; Lin, J.; Reddy, R.M.; Chang, A.C.; Ramnath, N.; Gotoh, N.; Beer, D.G.; Chen, G. A novel serum 4-microRNA signature for lung cancer detection. Sci. Rep. 2015, 5, 12464. [Google Scholar] [CrossRef]
- Jin, X.; Chen, Y.; Chen, H.; Fei, S.; Chen, D.; Cai, X.; Liu, L.; Lin, B.; Su, H.; Zhao, L.; et al. Evaluation of Tumor-Derived Exosomal miRNA as Potential Diagnostic Biomarkers for Early-Stage Non–Small Cell Lung Cancer Using Next-Generation Sequencing. Clin. Cancer Res. 2017, 23, 5311–5319. [Google Scholar] [CrossRef]
- Fan, L.; Qi, H.; Teng, J.; Su, B.; Chen, H.; Wang, C.; Xia, Q. Identification of serum miRNAs by nano-quantum dots microarray as diagnostic biomarkers for early detection of non-small cell lung cancer. Tumor Biol. 2016, 37, 7777–7784. [Google Scholar] [CrossRef]
- Saviana, M.; Romano, G.; McElroy, J.; Nigita, G.; Distefano, R.; Toft, R.; Calore, F.; Le, P.; Morales, D.D.V.; Atmajoana, S.; et al. A plasma miRNA-based classifier for small cell lung cancer diagnosis. Front. Oncol. 2023, 13, 1255527. [Google Scholar] [CrossRef]
- Yu, Z.; Chen, X.-Z.; Cui, L.-H.; Si, H.-Z.; Lu, H.-J.; Liu, S.-H. Prediction of lung cancer based on serum biomarkers by gene expression programming methods. Asian Pac. J. Cancer Prev. 2014, 15, 9367–9373. [Google Scholar] [CrossRef]
- Visser, E.; Genet, S.A.A.M.; de Kock, R.P.P.A.; van den Borne, B.E.E.M.; Soud, M.Y.-E.; Belderbos, H.N.A.; Stege, G.; de Saegher, M.E.A.; Westeinde, S.C.V.; Brunsveld, L. Liquid biopsy-based decision support algorithms for diagnosis and subtyping of lung cancer. Lung Cancer 2023, 178, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Korkmaz, E.T.; Koksal, D.; Aksu, F.; Dikmen, Z.G.; Icen, D.; Maden, E.; Onder, S.; Akbiyik, F.; Emri, S. Triple test with tumor markers CYFRA 21.1, HE4, and ProGRP might contribute to diagnosis and subtyping of lung cancer. Clin. Biochem. 2018, 58, 15–19. [Google Scholar] [CrossRef]
- Wen, Z.; Huang, Y.; Ling, Z.; Chen, J.; Wei, X.; Su, R.; Tang, Z.; Wen, Z.; Deng, Y.; Hu, Z. Lack of Efficacy of Combined Carbohydrate Antigen Markers for Lung Cancer Diagnosis. Dis. Markers 2020, 2020, 4716793. [Google Scholar] [CrossRef] [PubMed]
- Trulson, I.; Klawonn, F.; von Pawel, J.; Holdenrieder, S. Improvement of differential diagnosis of lung cancer by use of multiple protein tumor marker combinations. Tumour Biol. 2024, 46, S81–S98. [Google Scholar] [CrossRef] [PubMed]
- Sua, L.F.; Serrano-Gomez, S.J.; Nuñez, M.; Amezquita-Dussan, M.A.; Fernández-Trujillo, L. Diagnostic potential of protein serum biomarkers for distinguishing small and non-small cell lung cancer in patients with suspicious lung lesions. Biomarkers 2024, 29, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.H.; Tian, R.F.; Ren, Q.L.; Chui, H.Y.; Guo, S.T.; Zhang, X.D.; Song, X. Serum protein profiles of patients with lung cancer of different histological types. Asia Pac. J. Clin. Oncol. 2016, 12, 70–76. [Google Scholar] [CrossRef]
- Liang, Y.; Ma, T.; Thakur, A.; Yu, H.; Gao, L.; Shi, P.; Li, X.; Ren, H.; Jia, L.; Zhang, S.; et al. Differentially expressed glycosylated patterns of α-1-antitrypsin as serum biomarkers for the diagnosis of lung cancer. Glycobiology 2015, 25, 331–340. [Google Scholar] [CrossRef]
- Sugár, S.; Bugyi, F.; Tóth, G.; Pápay, J.; Kovalszky, I.; Tornóczky, T.; Drahos, L.; Turiák, L. Proteomic Analysis of Lung Cancer Types—A Pilot Study. Cancers 2022, 14, 2629. [Google Scholar] [CrossRef]
- Rocha, C.M.; Barros, A.S.; Goodfellow, B.J.; Carreira, I.M.; Gomes, A.; Sousa, V.; Bernardo, J.; Carvalho, L.; Gil, A.M.; Duarte, I.F. NMR metabolomics of human lung tumours reveals distinct metabolic signatures for adenocarcinoma and squamous cell carcinoma. Carcinogenesis 2015, 36, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Moreno, P.; Jiménez-Jiménez, C.; Garrido-Rodríguez, M.; Calderón-Santiago, M.; Molina, S.; Lara-Chica, M.; Priego-Capote, F.; Salvatierra, Á.; Munoz, E.; Calzado, M.A. Metabolomic profiling of human lung tumor tissues–nucleotide metabolism as a candidate for therapeutic interventions and biomarkers. Mol. Oncol. 2018, 12, 1778–1796. [Google Scholar] [CrossRef]
- Zang, X.; Zhang, J.; Jiao, P.; Xue, X.; Lv, Z. Non-small cell lung cancer detection and subtyping by UPLC-HRMS-based tissue metabolomics. J. Proteome Res. 2022, 21, 2011–2022. [Google Scholar] [CrossRef]
- You, L.; Fan, Y.; Liu, X.; Shao, S.; Guo, L.; Noreldeen, H.A.A.; Li, Z.; Ouyang, Y.; Li, E.; Pan, X. Liquid chromatography–mass spectrometry-based tissue metabolic profiling reveals major metabolic pathway alterations and potential biomarkers of lung cancer. J. Proteome Res. 2020, 19, 3750–3760. [Google Scholar] [CrossRef]
- Klupczynska, A.; Dereziński, P.; Garrett, T.J.; Rubio, V.Y.; Dyszkiewicz, W.; Kasprzyk, M.; Kokot, Z.J. Study of early stage non-small-cell lung cancer using Orbitrap-based global serum metabolomics. J. Cancer Res. Clin. Oncol. 2017, 143, 649–659. [Google Scholar] [CrossRef] [PubMed]
- Kowalczyk, T.; Kisluk, J.; Pietrowska, K.; Godzien, J.; Kozlowski, M.; Reszeć, J.; Sierko, E.; Naumnik, W.; Mróz, R.; Moniuszko, M. The ability of metabolomics to discriminate non-small-cell lung cancer subtypes depends on the stage of the disease and the type of material studied. Cancers 2021, 13, 3314. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Li, K.; Li, X.; Guan, C.; Sun, T.; Zhang, X. Metabolomic profiling of dried blood spots reveals gender-specific discriminant models for the diagnosis of small cell lung cancer. Aging 2020, 12, 978–995. [Google Scholar] [CrossRef] [PubMed]
- Qi, S.; Wu, Q.; Chen, Z.; Zhang, W.; Zhou, Y.; Mao, K.; Li, J.; Li, Y.; Chen, J.; Huang, Y.; et al. High-resolution metabolomic biomarkers for lung cancer diagnosis and prognosis. Sci. Rep. 2021, 11, 11805. [Google Scholar] [CrossRef] [PubMed]
- Cao, P.; Wu, S.; Guo, W.; Zhang, Q.; Gong, W.; Li, Q.; Zhang, R.; Dong, X.; Xu, S.; Liu, Y.; et al. Precise pathological classification of non-small cell lung adenocarcinoma and squamous carcinoma based on an integrated platform of targeted metabolome and lipidome. Metabolomics 2021, 17, 98. [Google Scholar] [CrossRef] [PubMed]
- Sieminska, J.; Miniewska, K.; Mroz, R.; Sierko, E.; Naumnik, W.; Kisluk, J.; Michalska-Falkowska, A.; Reszec, J.; Kozlowski, M.; Nowicki, L.; et al. First insight about the ability of specific glycerophospholipids to discriminate non-small cell lung cancer subtypes. Front. Mol. Biosci. 2024, 11, 1379631. [Google Scholar] [CrossRef]
- Mazzone, P.J.; Wang, X.-F.; Beukemann, M.; Zhang, Q.; Seeley, M.; Mohney, R.; Holt, T.; Pappan, K.L. Metabolite Profiles of the Serum of Patients with Non–Small Cell Carcinoma. J. Thorac. Oncol. 2016, 11, 72–78. [Google Scholar] [CrossRef]
- Yu, J.; Du, F.; Yang, L.; Chen, L.; He, Y.; Geng, R.; Wu, L.; Xie, B. Identification of potential serum biomarkers for simultaneously classifying lung adenocarcinoma, squamous cell carcinoma and small cell carcinoma. Cancer Biomark. 2021, 30, 331–342. [Google Scholar] [CrossRef]
- Shestakova, K.M.; Moskaleva, N.E.; Boldin, A.A.; Rezvanov, P.M.; Shestopalov, A.V.; Rumyantsev, S.A.; Zlatnik, E.Y.; Novikova, I.A.; Sagakyants, A.B.; Timofeeva, S.V.; et al. Targeted metabolomic profiling as a tool for diagnostics of patients with non-small-cell lung cancer. Sci. Rep. 2023, 13, 11072. [Google Scholar] [CrossRef] [PubMed]
- Bourbonne, V.; Geier, M.; Schick, U.; Lucia, F. Multi-Omics Approaches for the Prediction of Clinical Endpoints after Immunotherapy in Non-Small Cell Lung Cancer: A Comprehensive Review. Biomedicines 2022, 10, 1237. [Google Scholar] [CrossRef]
- Mei, T.; Wang, T.; Zhou, Q. Multi-omics and artificial intelligence predict clinical outcomes of immunotherapy in non-small cell lung cancer patients. Clin. Exp. Med. 2024, 24, 60. [Google Scholar] [CrossRef]
- Abbasian, M.H.; Ardekani, A.M.; Sobhani, N.; Roudi, R. The Role of Genomics and Proteomics in Lung Cancer Early Detection and Treatment. Cancers 2022, 14, 5144. [Google Scholar] [CrossRef]
- Micheletti, C.; Dhuli, K.; Donato, K.; Gadler, M.; Benedetti, S.; Guerri, G.; Cristofoli, F.; Generali, D.; Donofrio, C.A.; Cominetti, M.; et al. Omics sciences and precision medicine in lung cancer. Clin. Ter. 2023, 174, 37–45. [Google Scholar] [PubMed]
- Jia, Z.; Zhang, H.; Ong, C.N.; Patra, A.; Lu, Y.; Lim, C.T.; Venkatesan, T. Detection of Lung Cancer: Concomitant Volatile Organic Compounds and Metabolomic Profiling of Six Cancer Cell Lines of Different Histological Origins. ACS Omega 2018, 3, 5131–5140. [Google Scholar] [CrossRef]
- Ruiying, C.; Zeyun, L.; Yongliang, Y.; Zijia, Z.; Ji, Z.; Xin, T.; Xiaojian, Z. A comprehensive analysis of metabolomics and transcriptomics in non-small cell lung cancer. PLoS ONE 2020, 15, e0232272. [Google Scholar] [CrossRef] [PubMed]
- Stewart, P.A.; Li, J.; Fisher, K.J.; Dhungana, S.; Stewart, D.; Sumner, S.; Gardner, E.; Poirier, J.; Rudin, C.M.; Welsh, E.A. Integrating proteomics and metabolomics characterizes active pathways and potential drug targets in small cell lung cancer. Cancer Res. 2015, 75, 3752. [Google Scholar] [CrossRef]
- Gregorich, Z.R.; Ge, Y. Top-down proteomics in health and disease: Challenges and opportunities. Proteomics 2014, 14, 1195–1210. [Google Scholar] [CrossRef]
- Klupczyńska, A.; Dereziński, P.; Kokot, Z.J. Metabolomics in Medical Sciences--Trends, Challenges and Perspectives. Acta Pol. Pharm. 2015, 72, 629–641. [Google Scholar] [PubMed]
- Kosmides, A.K.; Kamisoglu, K.; Calvano, S.E.; Corbett, S.A.; Androulakis, I.P. Metabolomic fingerprinting: Challenges and opportunities. Crit. Rev. Biomed. Eng. 2013, 41, 205–221. [Google Scholar] [CrossRef]
- Linning, E.; Lu, L.; Li, L.; Yang, H.; Schwartz, L.H.; Zhao, B. Radiomics for Classification of Lung Cancer Histological Subtypes Based on Nonenhanced Computed Tomography. Acad. Radiol. 2019, 26, 1245–1252. [Google Scholar]
- Zhou, M.; Leung, A.; Echegaray, S.; Gentles, A.; Shrager, J.B.; Jensen, K.C.; Berry, G.J.; Plevritis, S.K.; Rubin, D.L.; Napel, S.; et al. Non–Small Cell Lung Cancer Radiogenomics Map Identifies Relationships between Molecular and Imaging Phenotypes with Prognostic Implications. Radiology 2018, 286, 307–315. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study | Sample Size/Type | Markers | Methods | Results | Conclusion |
|---|---|---|---|---|---|
| Argon et al. [33] | 120/ Lung tissue | TTF1, CK5/6, P63 | TMA | Discriminator:
| TTF-1 is a reliable marker for subtyping lung cancer. CK5/6 and P63 can be used as adjuncts for final diagnosis. |
| Kim et al. [34] | 129/ Lung, stomach, colon, vaginal tissue | Napsin A, TTF-1, p63, CK5/6 COX-2, HMWCK, CD141, p27, MOC-31, CEA, Rb protein | TMA | Discriminator:
| Researchers elected a combined panel of Napsin A, TTF1, CK5/6, and p63 as the best option to differentiate between ADC and SCC. |
| Yassin et al. [35] | 105/ Lung tissue | ALDH1A1 | TMA | ADC:
| There is a strong association between ALDH1 expression, histological subtype, and the grade of tumors in NSCLC. |
| Nishino et al. [36] | 241/ Lung tissue | TTF1, NapA, CK5/6, and P40 | TMA | SCC:
| A cocktail of Nap A/p40 can be used to accurately subtype preoperative small biopsy and cytology specimens. |
| Wei et al. [37] | 395/ Lung tissue | CDK5 | TMA | CDK5 positivity in lung cancer samples highly exceeded that in normal lung tissue (51.5% vs. 20%). The positive rates were found to be higher in advanced cases, cases of lymphatic metastases, and cases with a poorer histological grade, AUC = 0.685. | CDK5 positivity is a good diagnostic marker for lung cancer. |
| Guo et al. [38] | 58/ Lung tissue | p40/Nap A CK5/6/TTF1 | TMA | 100% of SCC cases showed p40 (nuclear) and CK5/6 (cytoplasmic) positivity, 93.8% of the ADC cases showed TTF1 (nuclear) positivity, and 87.5% cases showed Nap A (cytoplasmic) positivity. p40 and Napsin A dual-marker set showed 100% nuclear positivity and cytoplasmic negativity in SCC, while CK5/6 and TTF1 dual staining exhibited 100% cytoplasmic positivity and nuclear negativity in SCC. The single- and dual-marker panels revealed identical results. | Dual-marker stains could be an economical and simple novel approach to differentiating subtypes of NSCLC and could be an alternative to the more conventional single-marker IHC panels. |
| Zyl et al. [39] | 271/ FNA and FFPE | TTF-1, Napsin A, CK5, and P63 | TMA | ADC:
| Napsin A and TTF1 are acceptable markers for ADC, whereas CK5 and P63 are good markers for SCC. |
| Ao et al. [40] | 200/ Lung tissue | Triple-marker panel (consisting of TTF-1, Napsin A, and p40 | TMA | ADC:
| The triple-marker panel could be very helpful for the accurate subclassification of NSCLCs and would also aid in tissue preservation for further necessary molecular testing. |
| Kawai et al. [41] | 215/ Lung tissue | TTF1, Napsin A, p63, CK5/6, desmocollin-3 | TMA |
Discriminators:
| Napsin A and P63 could be very helpful in the histological categorization of NSCLC. |
| Tran et al. [42] | 557/ Lung tissue | CK5, p63, p40, Napsin A, TTF-1 | TMA | IHC markers of SCC identification and NSCLC exclusion:
| CK5 and p40 are good diagnostic markers for SCC and superior to p63. |
| Roudi et al. [43] | 133/ Lung tissue | ALDH1 CD133 | TMA |
| ALDH1 and CD133 could be used as novel biomarkers for lung cancer subtyping. |
| Roudi et al. [44] | 195/ Lung tissue | CD44 | TMA |
| CD44 could potentially serve as a novel diagnostic biomarker and might also be used to formulate targeted therapies. |
| Study | Sample Size/Type | Marker | Method | Results | Conclusion |
|---|---|---|---|---|---|
| Geng et al. [45] | 50/ Blood | miR-20a, miR-223, miR-21, miR-221, miR-145 | RT-PCR | Best candidates: miR-20a (AUC = 0.89) miR-223 (AUC = 0.94) miR-155 (AUC = 0.92) | These five miRNAs could individually work as noninvasive biomarkers for early stage NSCLC. |
| Lu et al. [46] | 1132/ Plasma | Six miRNAs | qRT-PCR | miR-17, miR-190b, and miR-375 could discriminate between SCLC and NSCLC. Training set AUC = 0.878 Validation set AUC = 0.869 The subdivision of NSCLC was not possible. | These panels could potentially serve as effective markers for the early diagnosis and subtyping of lung cancer. |
| Jin et al. [47] | 78/ Macrodissected frozen lung tissue | miR-365 | qRT-PCR | miR-365 was upregulated in SCLC and ADC. miR-365 was downregulated in SCC. | miR-365 is higher in SCLC and ADC and lower in SCC. |
| Yang et al. [48] | 175/ Blood | Eight circulating miRNAs | qRT-PCR | A panel of four miRNAs (miR-146b, miR-205, miR-29c, miR-30b, and miR-337) was best for the early diagnosis of NSCLC. For ADC:
| This panel can be utilized for the early diagnosis of NSCLC and is a better predictor for ADC than SCC. |
| Zhang et al. [49] | 147/ Serum | 16 miRNAs | qRT-PCR | NSCLC patients had significantly higher miR-3149 and miR-4769.3p (AUC 0.830 and 0.735, respectively). The values were similar in both ADC and SCC. | miR-3149 and miR-4769.3p performed well as diagnostic markers for NSCLC. |
| Powrozek et al. [50] | 90/ plasma | miR-944 miR-3662 | RT-PCR | Both miRNAs were higher in cancerous samples compared to the non-cancer cohort. miR-944 had a greater accuracy for operable SCC (AUC = 0.982), and miR-3662 for ADC (AUC = 0.926). | miR-944 and miR-3662 could serve as potent biomarkers for lung cancer diagnosis in the future. |
| Singh et al. [51] | 80/ Blood | Six miRNAs | qRT-PCR | mir-2116 and mir-449c were upregulated only in AC. mir-2115, mir-548q, and mir-2117 were higher only in SCC. mir-2115 and mir-449c were highest in SCC and AC, respectively. | These markers (specifically mir-2115 and mir-449c) could be effective in the differential diagnosis of NSCLC within the scope of noninvasive approaches. |
| Kumar et al. [52] | 115/ Serum | 10 miRNAs | RT-PCR | miR-15a-5p, miR-320a, miR-25-3p, let-7e-5p, miR-192-5p, let-7d-5p miR-148a-3p, and miR-92a-3p were lower in NSCLC patients. SCC patients had lower levels of miR-375 and miR-10b-5p compared to controls. There was no significant difference in these markers between ADC and controls. | miRNA-based assays could assist in the diagnosis and prognosis of NSCLC. |
| Kumar et al. [53] | 161/ Tissue samples | miR-375-3p miR-197-3p | TaqMan advanced miRNA assays | miR-375-3p and miR-197-3p were upregulated in tumor resectates compared to healthy controls. miR-375-3p was upregulated in tissue samples. miR-375-3p was the best diagnostic marker
| Lung carcinogenesis might be linked with the excessive expression of miR-375-3p and miR-197-3p. The expression of miR-375-3p may assist in predicting therapeutic response. |
| Nadal et al. [54] | 94/ Serum | Four miRNAs | qRT-PCR | A combined panel could diagnose NSCLC. AUC = 0.993 | This miRNA signature could act as a clinically helpful tool for the determination of lung cancer in patients. |
| Jin et al. [55] | 88/ Serum | MiRNA | RNA sequencing | ADC patients had significantly upregulated levels of 11 and downregulated levels of 13 miRNAs (miR-181a-5p, miR-30a-3p, miR-30e-3p, and miR-361-5p were specific for ADC). SCC patients had upregulated levels of six and lower levels of eight miRNAs (miR-10b-5p, miR-15b-5p, and miR-320b for SCC). The three-miRNA combined panel was a good diagnostic marker for NSCLC, ADC, and SCC, with AUCs of 0.899, 0.936, and 0.911, respectively. | The three-miRNA combined panel showed promise as a good diagnostic marker for NSCLC, ADC, and SCC |
| Fan et al. [56] | 152/ Plasma | 12 miRNAs | qRT-PCR fluorescence quantum dot liquid bead array | Six miRNAs (miR-16-5p, miR-20a-5p, miR-92-3p, miR-15b-5p, miR-17b-5p, miR-19-3p) were able to distinguish between the two groups. miR-15b-5p, miR-16-5p, and miR-20a-5p were the best discriminants for NSCLC. | These six markers could be explored as an avenue for noninvasive NSCLC diagnosis. |
| Saviana et al. [57] | 144/ Plasma | Seven circulating cell-free miRNAs | RNA sequencing qRT-PCR | miR-375-3p is the most competent discriminant for SCLC.
| Cell-free miRNA circulation shows promise as low cost, noninvasive, and reliable biomarker for SCLC diagnosis. |
| Study | Sample Size/Type | Marker | Method | Results | Conclusion |
|---|---|---|---|---|---|
| Yu et al. [58] | 180/ Serum | CEA NSE CPR LDH Cyfra 21-1 | Mass spectrometry | GEP 3 (CEA + NSE + Cyfra 21-1) Accuracy: 94.8% | A panel consisting of CEA, NSE, and CYFRA 21-1 was found to be superior for classifying lung cancer. |
| Visser et al. [59] | 1096/ Blood | Eight protein tumor markers (CA125, CA15.3, CEA, CYFRA 21-1, HE4, NSE, proGRP, SCCA) ctDNA mutations in EGFR, KRAS, and BRAF | Electrochemiluminescent assays Droplet digital PCR | CYFRA 21-1 had the best overall performance in identifying NSCLC.
CYFRA 21-1, CEA, proGRP, and NSE performed better than CYFRA 21-1 alone for NSCLC diagnosis.
| These models have clinical value and may help in LC diagnostics. |
| Korkmaz et al. [60] | 129/ Venous blood | Six tumor markers: ProGRP SCCAg CYFRA 21.1 HE4 CgA NSE | Mass spectrometry | ProGRP levels were found to be higher in SCLC. CYFRA 21.1 and SCCAg levels were higher in NSCLC. CYFRA 21.1 (p < 0.001, r = 0.394), HE4 (p = 0.014, r = 0.279), and CgA (p = 0.023, r = 0.259) levels had a positive correlation with the stage of NSCLC. Pro GRP was the best discriminator between subtypes.
| A panel of three tumor markers, CYFRA 21.1, HE4, and ProGRP, may play a role in differentiating LC from benign lung disease as well as subtyping SCLC. |
| Wen et al. [61] | 250/ Blood | CEA, CYFRA 21, NSE | Mass spectrometry | The CEA level was the highest in ADC.
NSE (AUC: 0.819; sensitivity: 69.0%) and CEA (AUC: 0.808; sensitivity: 60.7%) were the most related to SCLC. | Tumor markers could diagnose different lung cancer types. |
| Trulson et al. [62] | 490/ Serum | CYFRA 21-1 CEA, NSE ProGRP SCC, CA 125 CA 15-3 CA 19-9 CA 72-4 | Mass spectrometry | SCLC vs. NSCLC Pro GRP and NSE AUCs were 0.86 and 0.83, respectively. A two-marker panel (NSE and ProGRP) and a three-marker combination (NSE, ProGRP, and CEA) performed better; AUC = 0.97. ADC vs. SCC Low SCC and high CA15-3 AUC = 0.75 | A combination of serum tumor markers could be useful in assessing different subtypes of lung cancer. |
| Sua et al. [63] | 93/ Serum | Pro-GRP, CEA, CYFRA 21-1, SCC-Ag, and NSE | Mass spectrometry | Median levels of Pro-GRP, CEA, CYFRA 21-1, SCC-Ag, and NSE were higher in malignant lung disease than benign lung disease Discriminators: NSCLC Panel of Pro-GRP, CEA, CYFRA 21-1, SCC-Ag, and NSE AUC = 81.1% Sensitivity = 74.5% Specificity = 78.8% SCLC CYFRA 21-1 + Pro-GRP + NSE AUC = 97.3% Sensitivity = 88.8% Specificity = 98.9% | Individual biomarkers could be limited in the differential diagnosis of lung cancer, and although the exploration of combined markers could be fruitful, tissue diagnosis should not be delayed. |
| Yang et al. [64] | 183/ Serum | Protein mass-to-change ratio (M/Z) peak | SELDI-TOF-MS | Overall, 48 protein peaks were differentially expressed in lung cancer patients compared to healthy individuals. For SCC, there was an increase in the M/Z peaks at 1205, 4673, and 1429 and a decrease in the peak M/Z 4279. For ADC, M/Z 1205, 4673, 1429, and 4279 were at the intermediate levels and showed the lowest levels of M/Z 1205 and 4673. Best discriminators: SCCs vs. SCLC and ADC M/Z 1205 (AUC 0.84 and 0.82, respectively) SCLC vs. ADC M/Z 4279 AUC = 0.87 SCCs vs. SCLC Combination of M/Z 1205 and M/Z 4279 AUC = 0.91 | Protein profiles could be used to facilitate the classification of lung cancer and could be especially helpful for patients with tumors in hard-to-reach anatomical sites or for those unable to undergo a tissue biopsy before treatment can start. |
| Liang et al. [65] | 48/ Serum | Glyco patterns of A1AT | Lectin microarray Lectin-based ELISA | Discriminator: ADC vs. subtypes Fucosylated A1AT AUC = 0.844 Specificity = 69%, Sensitivity = 85.7% SCLC vs. NSCLC Poly-LacNAc AUC = 0.70 Specificity = 80.4% Sensitivity = 52.6% | Specific glycopatterns of A1AT could be used as novel biomarkers for the classification of lung cancer. |
| Sugar et al. [66] | 71/ Lung tissue | Number of differentially expressed proteins | Nano UHPLC-MS (MS) | Number of differential proteins: ADC: 61 (eukaryotic translation initiation factor 1 and matrix-metalloproteinase proteins (MMP2 and MMP19)) SCC: 35 (Fascin) SCLC: 99 (IgG heavy constant gamma 2 and RAB10) | Proteomic profiles show promise as potential diagnostic markers. |
| Study | Sample Size/Type | Marker | Method | Results | Conclusion |
|---|---|---|---|---|---|
| Rocha et al. [67] | 100/ Plasma | n PC, GPC, UDP/UTP, and peptides vs. lactate, glutamate, alanine, GSH, and creatine | HRMAS NMR spectroscopy | Higher levels of n PC, GPC, UDP/UTP, and peptides were observed in ADC. Higher levels of lactate, glutamate, alanine, GSH, and creatine were observed in SCC. Accuracy: 81.3% | Different subtypes of LC exhibit distinct molecular patterns. |
| Moreno et al. [68] | 136/ Lung tissue | Nucleotides | Mass spectrometry | 5,6-dihydrouracil was discriminatory for ADC and 20-O-methylguanosine and 5-methyluri-dine for SCC. | Lung cancer histotypes can be determined by metabolomic profiling |
| Zang et al. [69] | 227/ Lung tissue | Valine, sphingosine, glutamic acid γ-methyl ester, lyso phosphatidylcholine (LPC) (16:0), LPC (18:1), leucine derivatives | UPLC-HRMS | Discriminators ADC: Valine, sphingosine, glutamic acid γ-methyl ester, and lysophosphatidylcholine (LPC) (16:0) SCC: Valine, sphingosine, LPC (18:1), and leucine derivatives For a five-metabolite panel Accuracy: 96.8% Sensitivity: 98.2% Specificity: 85.7% | This panel shows a promising prospect for NSCLC tissue detection and subtyping. |
| You et al. [70] | 131/ Lung tissue | 241 metabolites | LC-MS | Panel of creatine, myoinositol, and LPE 16:0 AUC = 0.934 | This panel could serve as an excellent adjunct diagnostic tool for subtyping for lung cancer. |
| Klupczynska et al. [71] | 75/ Serum | Amino acids (histidine, leucine, methionine, and tyrosine), organic acids (pyroglutamic acid, malic acid), carnitine, acylcarnitines (valerylcarnitine and propionylcarnitine), alpha-N-phenylacetyl-L-glutamine, thiomorpholine 3-carboxylate, 1-amino-propan-2-ol/trimethylamine N-oxide/2-amino-1-propanol | ORBITRAP-based methodology Ultra-high-performance liquid chromatography–quadrupole- Orbitrap high- resolution mass spectrometry | AUC = 0.836 for discrimination between lung cancer and normal tissue No statistically significant difference was observed between subtypes. | Orbitrap-based global metabolic profiling could be a useful diagnostic and therapeutic strategy in NSCLC. |
| Kowalczyk et al. [72] | 137/ Lung tissue and plasma | Amino acids, fatty acids, carnitines, lyso glycerophospholipids, sphingomyelins, plasmalogens glycerophospholipids, metabolites related to N-acyl ethanolamine (NAE) biosynthesis, glycerophospho (N-acyl) ethanolamines (GP-NAE) | LC-MS | Tissue samples were a better medium for differentiating early stage ADC and SCC. Serum samples were better for advanced disease- Early stage SCC had higher levels of creatine, creatinine, xanthine, and dihydrothymine. ADC had greater levels of fatty acids, carnitines, glycerophospholipids, lyso glycerophospholipids, amines, amino acids, and amides. Fatty acids, carnitines, and fatty-acid amides were discriminatory for advanced cases. | Metabolites can differentiate between NSCLC histotypes. |
| Yu et al. [73] | 114/Dried blood | Metabolites (PI (18:0/18:0), Cer (d18:1/22:0 OH), 2-AG, IMP, Cholic acid, PE (18:1/20:4), 5-methyltetrahydrofolic acid, desmosterol, 4,5-dihydroorotic acid, 9-HETE) | LC-MS/MS | SCLC Male: (PI (18:0/18:0), Cer (d18:1/22:0 OH), 2-AG, IMP, and cholic acid AUC = 0.95 Female: PE (18:1/20:4), 5-methyltetrahydrofolic acid, desmosterol, 4,5-dihydroorotic acid, and 9-HETE AUC = 0.94 | Metabolomic profiling of DBSs could be helpful in the diagnosis of SCLC. |
| Qi et al. [74] | 173/Plasma | Metabolites (Amino acids, fatty acids, acylcarnitines) | High-resolution LC-MS | Palmitic acid, heptadecanoic acid, ornithine, pentadecanoic acid, and acylcarnitine C8:1 were the most effective subtype classifiers. | Plasma metabolites could be a useful tool for the screening and classification of lung cancer. |
| Cao et al. [75] | 128/Plasma | 1191 metabolites, including lipids | LC-ESI -QTRAP- MS/MS | Number of differential metabolites between ADC and SCC: 16 upregulated 3 downregulated Best discriminators: 2-(methylthio) ethanol, cortisol, D-glyceric acid, and N-acetylhistamine AUC = 0.946 Sensitivity = 92.0% Specificity = 92.9% | Their research could contribute to the growing evidence of metabolomic biomarkers as NSCLC discriminants. |
| Sieminska et al. [76] | 122/Lung tissue 101/Plasma | Lipid markers | LC-MS | Discriminants: ADC Upregulated plasma levels of LPA 20:4, LPA 18:1, and LPA 18:2; PC 16:0/18:2; OH, PC 18:0/20:4; OH, PC 16:0/20:4; OOH Upregulated tumor levels of PC 16:0/18:2, PC 16:0/4:0, CHO Best performers: LPA 20:4 (AUC = 0.851) PC 16:0/20:4 (AUC = 0.825) Combined panel (AUC = 0.873) | This research provides insight that oxPCs and LPAs could act as potential markers for ADC and SCC. |
| Mazzone et al. [77] | 284/Serum | Serum metabolites | Non-targeted UPLC-MS/MS and GC/MS | Overall, 149 metabolites were differentially present in the lung cancer group compared to the controls. ADC patients showed different levels of 65 metabolites (5 specific). SCC patients showed different levels of 50 metabolites with 3 specific ones. | The differences in the concentrations of various metabolites could be used as new biomarkers for NSCLC subtyping and to discover novel therapeutic targets. |
| Yu et al. [78] | 143/Blood | Various metabolites | 1H NMR UPLC- MS/MS | SAM, CEA, NSE, and SCC were best suited for differentiation. Accuracy = 92.3% AUC = 0.97 | The model can be used to discriminate between lung cancer subtypes. |
| Shestakova et al. [79] | 200/Plasma | Amino acids Tryptophan metabolism intermediates Acylcarnitine | Targeted metabolomic techniques | Metabolites involved in the tryptophan metabolism, TCA cycle, urea cycle, and lipid metabolism pathways were distinctive. Model of combined markers and ratios: AUC = 0.96 | Metabolomics integrated with bioinformatics could work as a valuable diagnostic tool for NSCLC. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siddique, F.; Shehata, M.; Ghazal, M.; Contractor, S.; El-Baz, A. Lung Cancer Subtyping: A Short Review. Cancers 2024, 16, 2643. https://doi.org/10.3390/cancers16152643
Siddique F, Shehata M, Ghazal M, Contractor S, El-Baz A. Lung Cancer Subtyping: A Short Review. Cancers. 2024; 16(15):2643. https://doi.org/10.3390/cancers16152643
Chicago/Turabian StyleSiddique, Farzana, Mohamed Shehata, Mohammed Ghazal, Sohail Contractor, and Ayman El-Baz. 2024. "Lung Cancer Subtyping: A Short Review" Cancers 16, no. 15: 2643. https://doi.org/10.3390/cancers16152643
APA StyleSiddique, F., Shehata, M., Ghazal, M., Contractor, S., & El-Baz, A. (2024). Lung Cancer Subtyping: A Short Review. Cancers, 16(15), 2643. https://doi.org/10.3390/cancers16152643