Circulating Tumor DNA Predicts Early Recurrence Following Locoregional Therapy for Oligometastatic Colorectal Cancer

 , , , ,
, , , , 
 , , , and
, , , and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
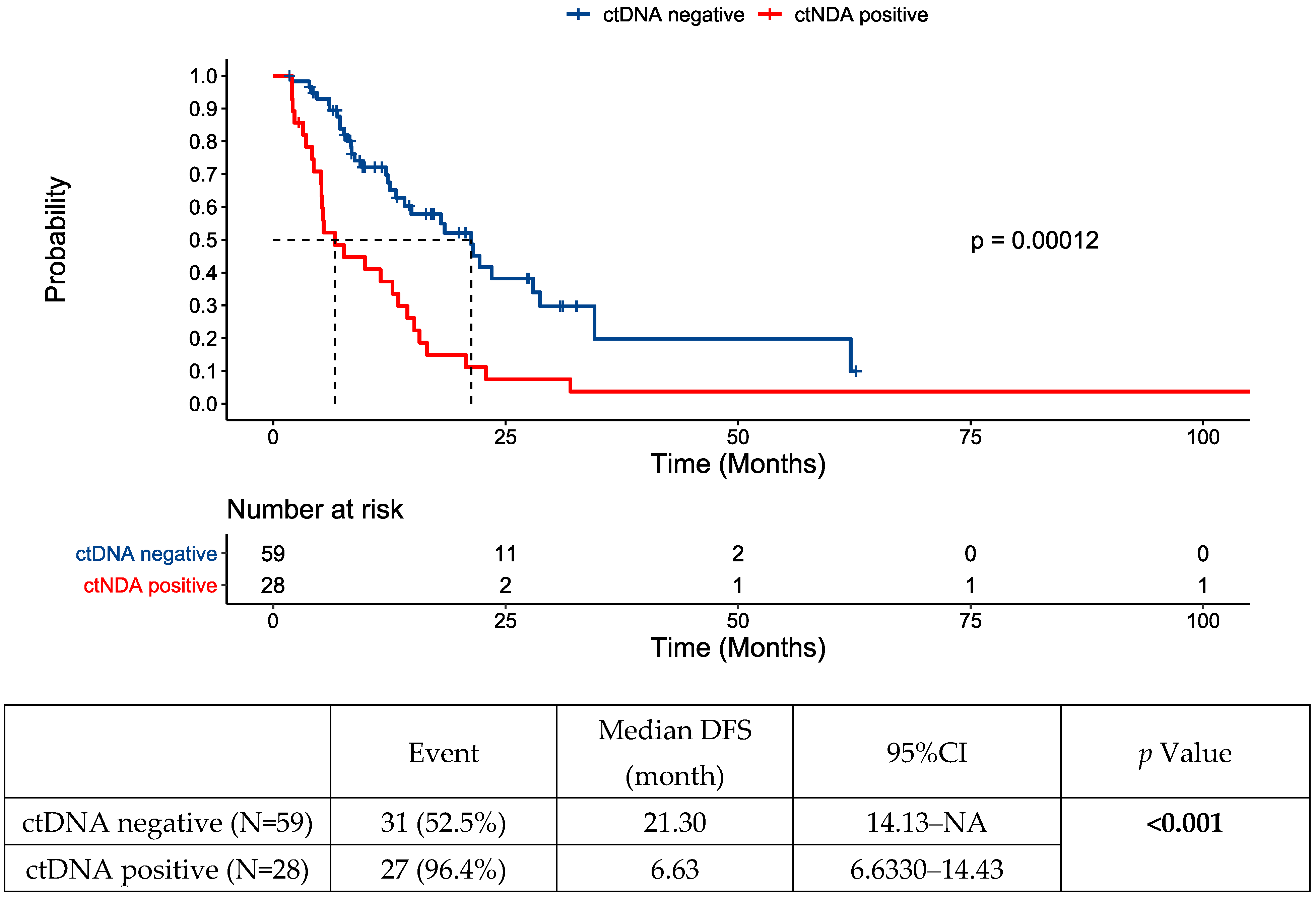
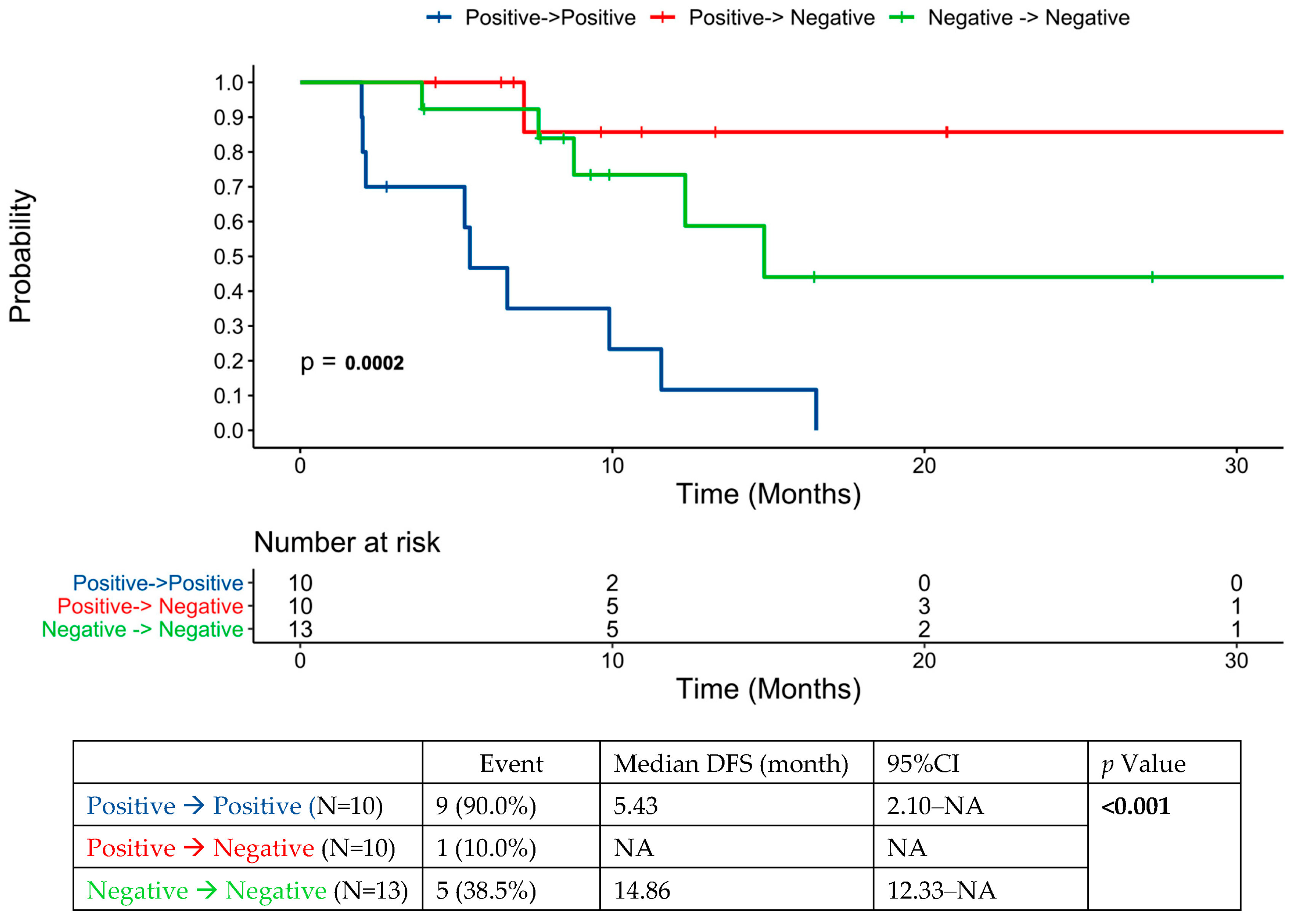
3.1. ctDNA Dynamics
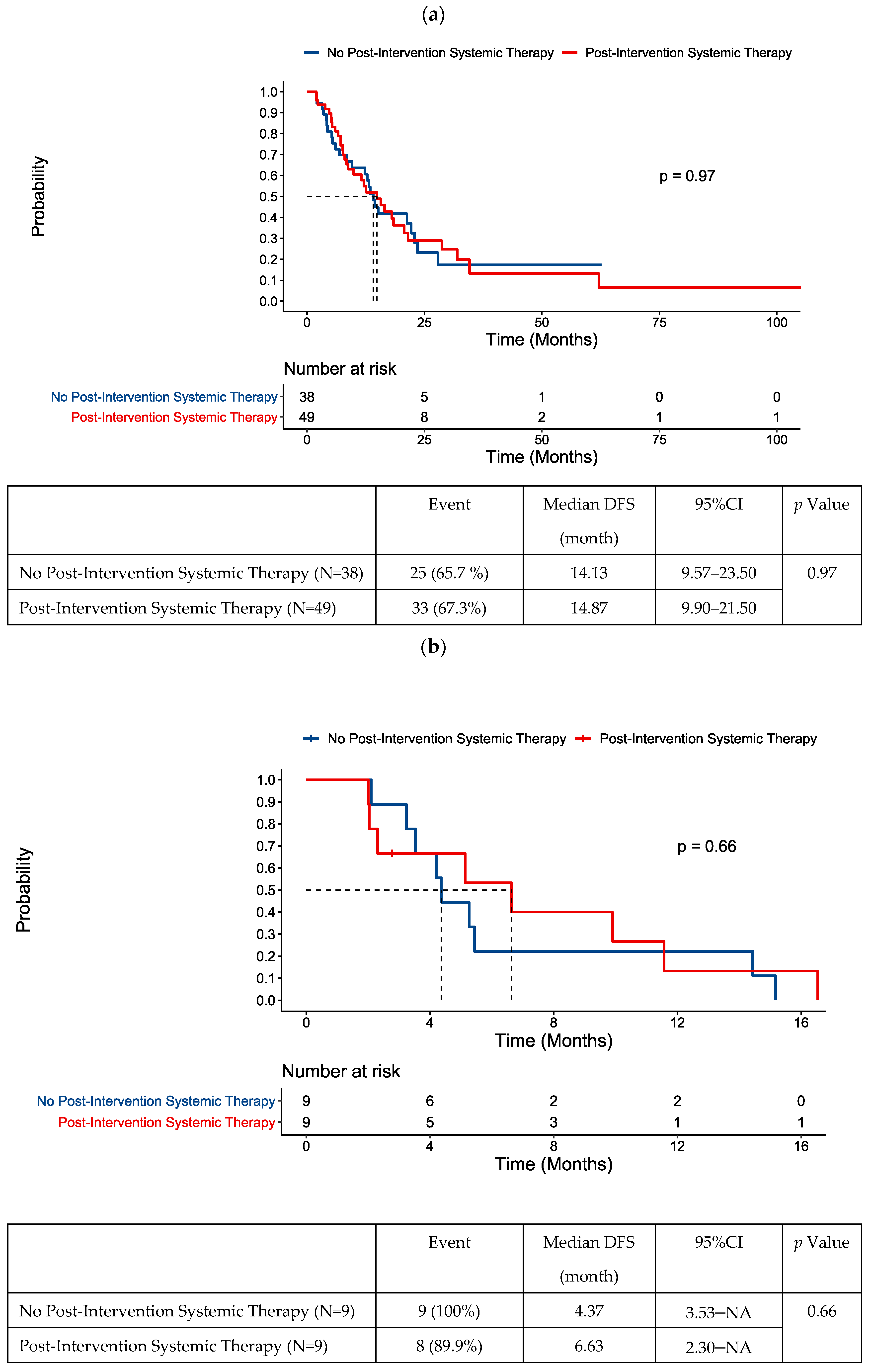
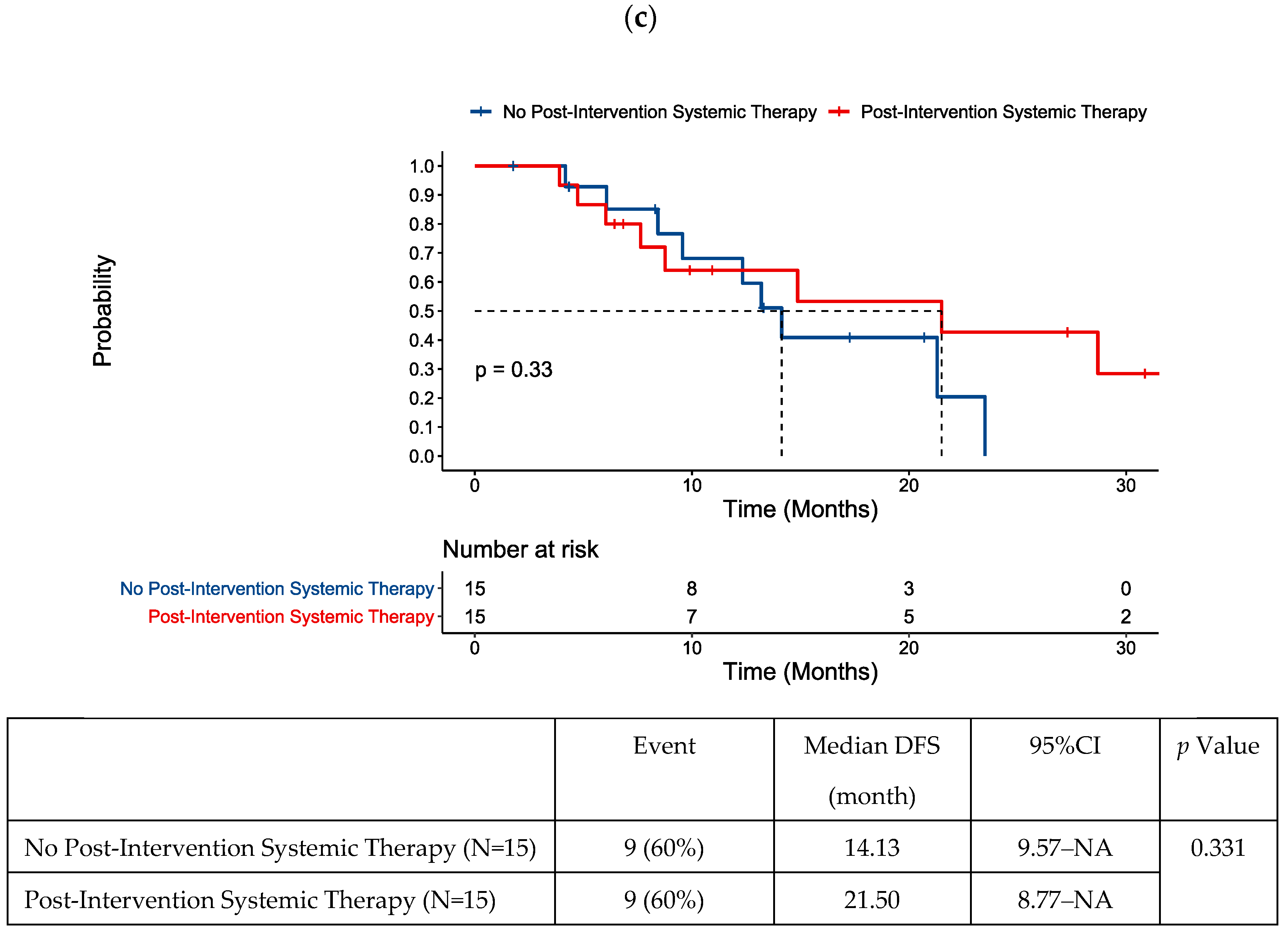
3.2. Assessment in the 8-Week Post-Intervention Window: The Role of Post-Intervention Chemotherapy
3.3. CEA versus ctDNA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Laversanne, M.; Sung, H.; Ferlay, J.; Siegel, R.L.; Soerjomataram, I.; Jemal, A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2024, 74, 229–263. [Google Scholar] [CrossRef] [PubMed]
- Verwaal, V.J.; van Ruth, S.; Witkamp, A.; Boot, H.; van Slooten, G.; Zoetmulder, F.A. Long-term survival of peritoneal carcinomatosis of colorectal origin. Ann. Surg. Oncol. 2005, 12, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Cervantes, A.; Adam, R.; Rosello, S.; Arnold, D.; Normanno, N.; Taieb, J.; Seligmann, J.; De Baere, T.; Osterlund, P.; Yoshino, T.; et al. Metastatic colorectal cancer: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann. Oncol. 2023, 34, 10–32. [Google Scholar] [CrossRef] [PubMed]
- de Baere, T.; Auperin, A.; Deschamps, F.; Chevallier, P.; Gaubert, Y.; Boige, V.; Fonck, M.; Escudier, B.; Palussiere, J. Radiofrequency ablation is a valid treatment option for lung metastases: Experience in 566 patients with 1037 metastases. Ann. Oncol. 2015, 26, 987–991. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.L.; Mangu, P.B.; Choti, M.A.; Crocenzi, T.S.; Dodd, G.D., 3rd; Dorfman, G.S.; Eng, C.; Fong, Y.; Giusti, A.F.; Lu, D.; et al. American Society of Clinical Oncology 2009 clinical evidence review on radiofrequency ablation of hepatic metastases from colorectal cancer. J. Clin. Oncol. 2010, 28, 493–508. [Google Scholar] [CrossRef] [PubMed]
- Kobiela, J.; Spychalski, P.; Marvaso, G.; Ciardo, D.; Dell’Acqua, V.; Kraja, F.; Blazynska-Spychalska, A.; Lachinski, A.J.; Surgo, A.; Glynne-Jones, R.; et al. Ablative stereotactic radiotherapy for oligometastatic colorectal cancer: Systematic review. Crit. Rev. Oncol. Hematol. 2018, 129, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Palma, D.A.; Olson, R.; Harrow, S.; Gaede, S.; Louie, A.V.; Haasbeek, C.; Mulroy, L.; Lock, M.; Rodrigues, G.B.; Yaremko, B.P.; et al. Stereotactic Ablative Radiotherapy for the Comprehensive Treatment of Oligometastatic Cancers: Long-Term Results of the SABR-COMET Phase II Randomized Trial. J. Clin. Oncol. 2020, 38, 2830–2838. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network: Colon Cancer. Version 2.2023. Available online: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed on 9 August 2023).
- Booth, C.M.; Berry, S.R. Perioperative Chemotherapy for Resectable Liver Metastases in Colorectal Cancer: Do We Have a Blind Spot? J. Clin. Oncol. 2021, 39, 3767–3769. [Google Scholar] [CrossRef] [PubMed]
- Kanemitsu, Y.; Shimizu, Y.; Mizusawa, J.; Inaba, Y.; Hamaguchi, T.; Shida, D.; Ohue, M.; Komori, K.; Shiomi, A.; Shiozawa, M.; et al. Hepatectomy Followed by mFOLFOX6 Versus Hepatectomy Alone for Liver-Only Metastatic Colorectal Cancer (JCOG0603): A Phase II or III Randomized Controlled Trial. J. Clin. Oncol. 2021, 39, 3789–3799. [Google Scholar] [CrossRef] [PubMed]
- Nordlinger, B.; Sorbye, H.; Glimelius, B.; Poston, G.J.; Schlag, P.M.; Rougier, P.; Bechstein, W.O.; Primrose, J.N.; Walpole, E.T.; Finch-Jones, M.; et al. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): A randomised controlled trial. Lancet 2008, 371, 1007–1016. [Google Scholar] [CrossRef] [PubMed]
- Sonbol, M.B.; Siddiqi, R.; Uson, P.L.S., Jr.; Pathak, S.; Firwana, B.; Botrus, G.; Almader-Douglas, D.; Ahn, D.H.; Borad, M.J.; Starr, J.; et al. The Role of Systemic Therapy in Resectable Colorectal Liver Metastases: Systematic Review and Network Meta-Analysis. Oncology 2022, 27, 1034–1040. [Google Scholar] [CrossRef] [PubMed]
- Diehl, F.; Schmidt, K.; Choti, M.A.; Romans, K.; Goodman, S.; Li, M.; Thornton, K.; Agrawal, N.; Sokoll, L.; Szabo, S.A.; et al. Circulating mutant DNA to assess tumor dynamics. Nat. Med. 2008, 14, 985–990. [Google Scholar] [CrossRef]
- Kasi, P.M.; Aushev, V.N.; Ensor, J.; Langer, N.; Wang, C.G.; Cannon, T.L.; Berim, L.D.; Feinstein, T.; Grothey, A.; McCollom, J.W.; et al. Circulating tumor DNA (ctDNA) for informing adjuvant chemotherapy (ACT) in stage II/III colorectal cancer (CRC): Interim analysis of BESPOKE CRC study. J. Clin. Oncol. 2024, 42, 9. [Google Scholar] [CrossRef]
- Kotani, D.; Oki, E.; Nakamura, Y.; Yukami, H.; Mishima, S.; Bando, H.; Shirasu, H.; Yamazaki, K.; Watanabe, J.; Kotaka, M.; et al. Molecular residual disease and efficacy of adjuvant chemotherapy in patients with colorectal cancer. Nat. Med. 2023, 29, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Parikh, A.R.; Van Seventer, E.E.; Siravegna, G.; Hartwig, A.V.; Jaimovich, A.; He, Y.; Kanter, K.; Fish, M.G.; Fosbenner, K.D.; Miao, B.; et al. Minimal Residual Disease Detection using a Plasma-only Circulating Tumor DNA Assay in Patients with Colorectal Cancer. Clin. Cancer Res. 2021, 27, 5586–5594. [Google Scholar] [CrossRef] [PubMed]
- Solar Vasconcelos, J.P.; Boutin, M.; Loree, J.M. Circulating tumor DNA in early-stage colon cancer: Ready for prime time or needing refinement? Ther. Adv. Med. Oncol. 2022, 14, 17588359221143975. [Google Scholar] [CrossRef]
- Reinert, T.; Henriksen, T.V.; Christensen, E.; Sharma, S.; Salari, R.; Sethi, H.; Knudsen, M.; Nordentoft, I.; Wu, H.T.; Tin, A.S.; et al. Analysis of Plasma Cell-Free DNA by Ultradeep Sequencing in Patients With Stages I to III Colorectal Cancer. JAMA Oncol. 2019, 5, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Marmorino, F.; Prisciandaro, M.; Giordano, M.; Ortolan, E.; Crucitta, S.; Manca, P.; Antoniotti, C.; Valenti, M.M.; Danesi, R.; Conca, V.; et al. Circulating Tumor DNA as a Marker of Minimal Residual Disease After Radical Resection of Colorectal Liver Metastases. JCO Precis. Oncol. 2022, 6, e2200244. [Google Scholar] [CrossRef] [PubMed]
- Newhook, T.E.; Overman, M.J.; Chun, Y.S.; Dasari, A.; Tzeng, C.D.; Cao, H.S.T.; Raymond, V.; Parseghian, C.; Johnson, B.; Nishioka, Y.; et al. Prospective Study of Perioperative Circulating Tumor DNA Dynamics in Patients Undergoing Hepatectomy for Colorectal Liver Metastases. Ann. Surg. 2023, 277, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Reinert, T.; Petersen, L.M.S.; Henriksen, T.V.; Larsen, M.O.; Rasmussen, M.H.; Johansen, A.F.B.; Ogaard, N.; Knudsen, M.; Nordentoft, I.; Vang, S.; et al. Circulating tumor DNA for prognosis assessment and postoperative management after curative-intent resection of colorectal liver metastases. Int. J. Cancer 2022, 150, 1537–1548. [Google Scholar] [CrossRef] [PubMed]
- Tie, J.; Wang, Y.; Cohen, J.; Li, L.; Hong, W.; Christie, M.; Wong, H.L.; Kosmider, S.; Wong, R.; Thomson, B.; et al. Circulating tumor DNA dynamics and recurrence risk in patients undergoing curative intent resection of colorectal cancer liver metastases: A prospective cohort study. PLoS Med. 2021, 18, e1003620. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Huang, F.; Yang, Y.; Chen, X.; Shen, M.; Zhang, C.; Pan, B.; Wang, B.; Guo, W. Postoperative circulating tumor DNA testing based on tumor naive strategy after liver metastasis surgery in colorectal cancer patients. Front. Oncol. 2023, 13, 1153685. [Google Scholar] [CrossRef] [PubMed]
- Yukami, H.; Nakamura, Y.; Mishima, S.; Ando, K.; Bando, H.; Watanabe, J.; Hirata, K.; Akazawa, N.; Ikeda, M.; Yokota, M.; et al. Circulating tumor DNA (ctDNA) dynamics in patients with colorectal cancer (CRC) with molecular residual disease: Updated analysis from GALAXY study in the CIRCULATE-JAPAN. J. Clin. Oncol. 2024, 42, 6. [Google Scholar] [CrossRef]
- Malla, M.; Loree, J.M.; Kasi, P.M.; Parikh, A.R. Using Circulating Tumor DNA in Colorectal Cancer: Current and Evolving Practices. J. Clin. Oncol. 2022, 40, 2846–2857. [Google Scholar] [CrossRef]
- Tie, J.; Cohen, J.D.; Wang, Y.; Christie, M.; Simons, K.; Lee, M.; Wong, R.; Kosmider, S.; Ananda, S.; McKendrick, J.; et al. Circulating Tumor DNA Analyses as Markers of Recurrence Risk and Benefit of Adjuvant Therapy for Stage III Colon Cancer. JAMA Oncol. 2019, 5, 1710–1717. [Google Scholar] [CrossRef] [PubMed]
- Emiloju, O.E.; Storandt, M.; Zemla, T.; Tran, N.; Jethwa, K.; Mahipal, A.; Mitchell, J.; Thiels, C.; Mathis, K.; McWilliams, R.; et al. Tumor-Informed Circulating Tumor DNA for Minimal Residual Disease Detection in the Management of Colorectal Cancer. JCO Precis. Oncol. 2024, 8, e2300127. [Google Scholar] [CrossRef] [PubMed]
- Maki, H.; Jain, A.J.; Haddad, A.; Lendoire, M.; Chun, Y.S.; Vauthey, J.N. Locoregional treatment for colorectal liver metastases aiming for precision medicine. Ann. Gastroenterol. Surg. 2023, 7, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Tie, J.; Cohen, J.D.; Lahouel, K.; Lo, S.N.; Wang, Y.; Kosmider, S.; Wong, R.; Shapiro, J.; Lee, M.; Harris, S.; et al. Circulating Tumor DNA Analysis Guiding Adjuvant Therapy in Stage II Colon Cancer. N. Engl. J. Med. 2022, 386, 2261–2272. [Google Scholar] [CrossRef] [PubMed]
- Grothey, A.; Sobrero, A.F.; Shields, A.F.; Yoshino, T.; Paul, J.; Taieb, J.; Souglakos, J.; Shi, Q.; Kerr, R.; Labianca, R.; et al. Duration of Adjuvant Chemotherapy for Stage III Colon Cancer. N. Engl. J. Med. 2018, 378, 1177–1188. [Google Scholar] [CrossRef] [PubMed]
- Andre, T.; Meyerhardt, J.; Iveson, T.; Sobrero, A.; Yoshino, T.; Souglakos, I.; Grothey, A.; Niedzwiecki, D.; Saunders, M.; Labianca, R.; et al. Effect of duration of adjuvant chemotherapy for patients with stage III colon cancer (IDEA collaboration): Final results from a prospective, pooled analysis of six randomised, phase 3 trials. Lancet Oncol. 2020, 21, 1620–1629. [Google Scholar] [CrossRef] [PubMed]
- Pietrantonio, F.; Randon, G.; Lonardi, S.; Garattini, S.K.; Tamberi, S.; Giommoni, E.; Donato, S.D.; Fornaro, L.; Brunetti, O.; Vita, F.D.; et al. Ramucirumab plus paclitaxel as switch maintenance versus continuation of oxaliplatin-based chemotherapy in patients (pts) with advanced HER2-negative gastric or gastroesophageal junction (GEJ) cancer: The ARMANI phase III trial. J. Clin. Oncol. 2024, 42, LBA4002. [Google Scholar] [CrossRef]
- Lieu, C.H.; Yu, G.; Kopetz, S.; Puhalla, S.L.; Lucas, P.C.; Sahin, I.H.; Deming, D.A.; Philip, P.A.; Hong, T.S.; Rojas-Khalil, Y.; et al. NRG-GI008: Colon adjuvant chemotherapy based on evaluation of residual disease (CIRCULATE-NORTH AMERICA). J. Clin. Oncol. 2024, 42, TPS243. [Google Scholar] [CrossRef]
- Conroy, T.; Etienne, P.-L.; Rio, E.; Evesque, L.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouche, O.; Boileve, A.; Delaye, M.; et al. Total neoadjuvant therapy with mFOLFIRINOX versus preoperative chemoradiation in patients with locally advanced rectal cancer: 7-year results of PRODIGE 23 phase III trial, a UNICANCER GI trial. J. Clin. Oncol. 2023, 41, LBA3504. [Google Scholar] [CrossRef]
- Cremolini, C.; Antoniotti, C.; Rossini, D.; Lonardi, S.; Loupakis, F.; Pietrantonio, F.; Bordonaro, R.; Latiano, T.P.; Tamburini, E.; Santini, D.; et al. Upfront FOLFOXIRI plus bevacizumab and reintroduction after progression versus mFOLFOX6 plus bevacizumab followed by FOLFIRI plus bevacizumab in the treatment of patients with metastatic colorectal cancer (TRIBE2): A multicentre, open-label, phase 3, randomised, controlled trial. Lancet Oncol. 2020, 21, 497–507. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients N = 87 (%) |
|---|---|
| Median age (IQR), years | 59 (32–86) |
| -<65 | 62 (71) |
| -≥65 | 25 (29) |
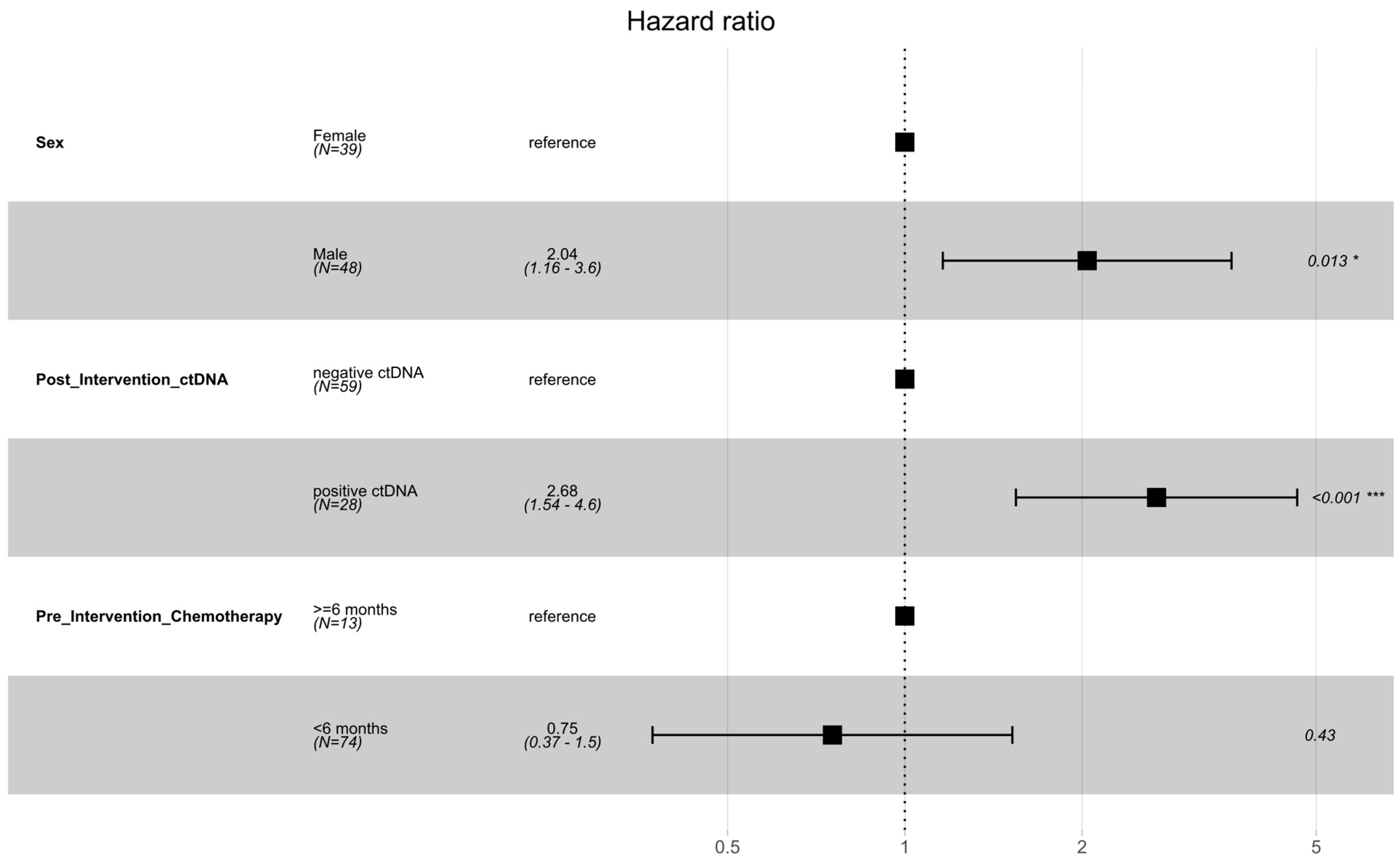
| Sex | |
| -Male | 48 (55) |
| -Female | 39 (45) |
| Ethnicity | |
| -White | 70 (81) |
| -Black | 14 (16) |
| -Other | 3 (3) |
| Molecular profile of tumor | |
| -KRAS/NRAS mutation | |
| • Positive | 36 (46) |
| • Negative | 43 (54) |
| • Unknown | 8 |
| -BRAF mutation | |
| • Positive | 1 (1) |
| • Negative | 75 (99) |
| • Unknown | 11 |
| -MSI/MMR | |
| • dMMR | 2 (2) |
| • pMMR | 85 (98) |
| Initial stage at diagnosis | |
| -Stage I | 4 (5) |
| -Stage II | 8 (9) |
| -Stage III | 23 (26) |
| -Stage IV | 52 (60) |
| Location of primary tumor | |
| -Right-side | 23 (26) |
| -Left side | 64 (74) |
| Pattern of metastatic disease | |
| -Synchronous metastases | 52 (60) |
| -Metachronous metastases | 35 (40) |
| Location of isolated metastatic disease | |
| -Liver | 68 (78) |
| -Lung | 8 (9) |
| -Others | 11 (13) |
| Median amount of pre-intervention systemic therapy (IQR), weeks | 15 (0–58) |
| Pre-intervention systemic therapy regimen | |
| -None | 11 (12) |
| -Single agent chemotherapy | 5 (6) |
| -Doublet chemotherapy | 58 (65) |
| -Triplet chemotherapy | 12 (14) |
| -Other | 3 (3) |
| ctDNA pre-intervention | |
| -Not tested | 54 (62) |
| -Tested | 33 (38) |
| • Positive | 24 (73) |
| • Negative | 9 (27) |
| Type of local therapy to metastatic disease | |
| -Resection | 53 (61) |
| -Ablation | 6 (7) |
| -Stereotactic body radiation therapy | 4 (5) |
| -Multimodality | 24 (27) |
| ctDNA post-intervention | |
| -Positive | 28 (32) |
| -Negative | 59 (68) |
| Median time from definitive therapy to ctDNA test (IQR), weeks | 6.1 (0.4–436.9) |
| -≤8 weeks | 48 (55) |
| ->8 weeks | 39 (45) |
| Post-intervention systemic therapy | |
| -Yes | 49 (56) |
| -No | 38 (44) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
O’Donnell, C.D.J.; Naleid, N.; Siripoon, T.; Zablonski, K.G.; Storandt, M.H.; Selfridge, J.E.; Hallemeier, C.L.; Conces, M.L.; Jethwa, K.R.; Bajor, D.L.; et al. Circulating Tumor DNA Predicts Early Recurrence Following Locoregional Therapy for Oligometastatic Colorectal Cancer. Cancers 2024, 16, 2407. https://doi.org/10.3390/cancers16132407
O’Donnell CDJ, Naleid N, Siripoon T, Zablonski KG, Storandt MH, Selfridge JE, Hallemeier CL, Conces ML, Jethwa KR, Bajor DL, et al. Circulating Tumor DNA Predicts Early Recurrence Following Locoregional Therapy for Oligometastatic Colorectal Cancer. Cancers. 2024; 16(13):2407. https://doi.org/10.3390/cancers16132407
Chicago/Turabian StyleO’Donnell, Conor D. J., Nikolas Naleid, Teerada Siripoon, Kevin G. Zablonski, Michael H. Storandt, Jennifer E. Selfridge, Christopher L. Hallemeier, Madison L. Conces, Krishan R. Jethwa, David L. Bajor, and et al. 2024. "Circulating Tumor DNA Predicts Early Recurrence Following Locoregional Therapy for Oligometastatic Colorectal Cancer" Cancers 16, no. 13: 2407. https://doi.org/10.3390/cancers16132407
APA StyleO’Donnell, C. D. J., Naleid, N., Siripoon, T., Zablonski, K. G., Storandt, M. H., Selfridge, J. E., Hallemeier, C. L., Conces, M. L., Jethwa, K. R., Bajor, D. L., Thiels, C. A., Warner, S. G., Starlinger, P. P., Atwell, T. D., Mitchell, J. L., Mahipal, A., & Jin, Z. (2024). Circulating Tumor DNA Predicts Early Recurrence Following Locoregional Therapy for Oligometastatic Colorectal Cancer. Cancers, 16(13), 2407. https://doi.org/10.3390/cancers16132407