
Intraoperative Assessment of Breast Cancer Tissues after Breast-Conserving Surgery Based on Mapping the Attenuation Coefficients in 3D Cross-Polarization Optical Coherence Tomography

 ,
,  ,
,  , , and
, , and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Human Breast Specimens after BCS
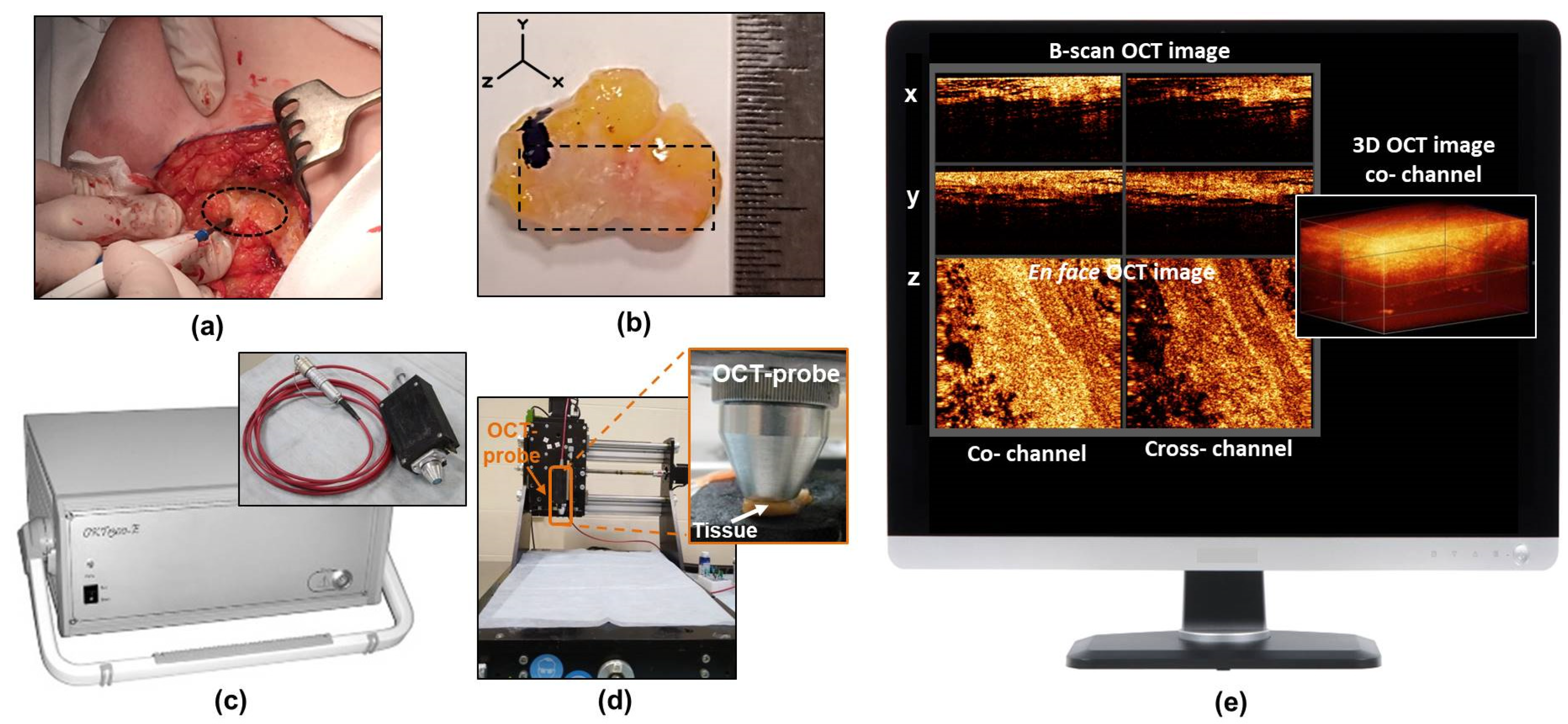
2.2. CP OCT Setup and Data Acquisition
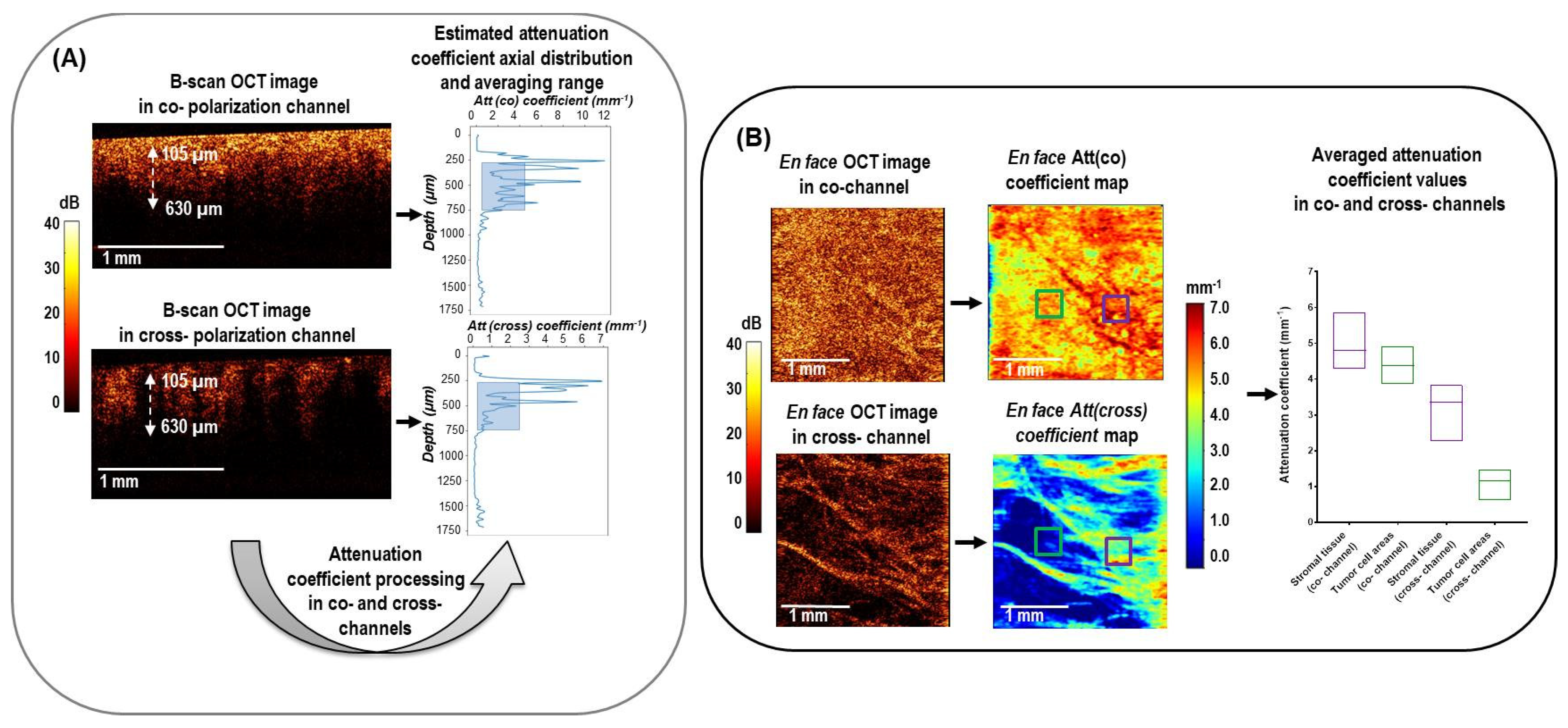
2.3. CP OCT Data Processing
2.4. Histological Study
2.5. Correlation of the CP OCT Data with Histology and Region of Interest Selection
2.6. Statistical Analysis
3. Results
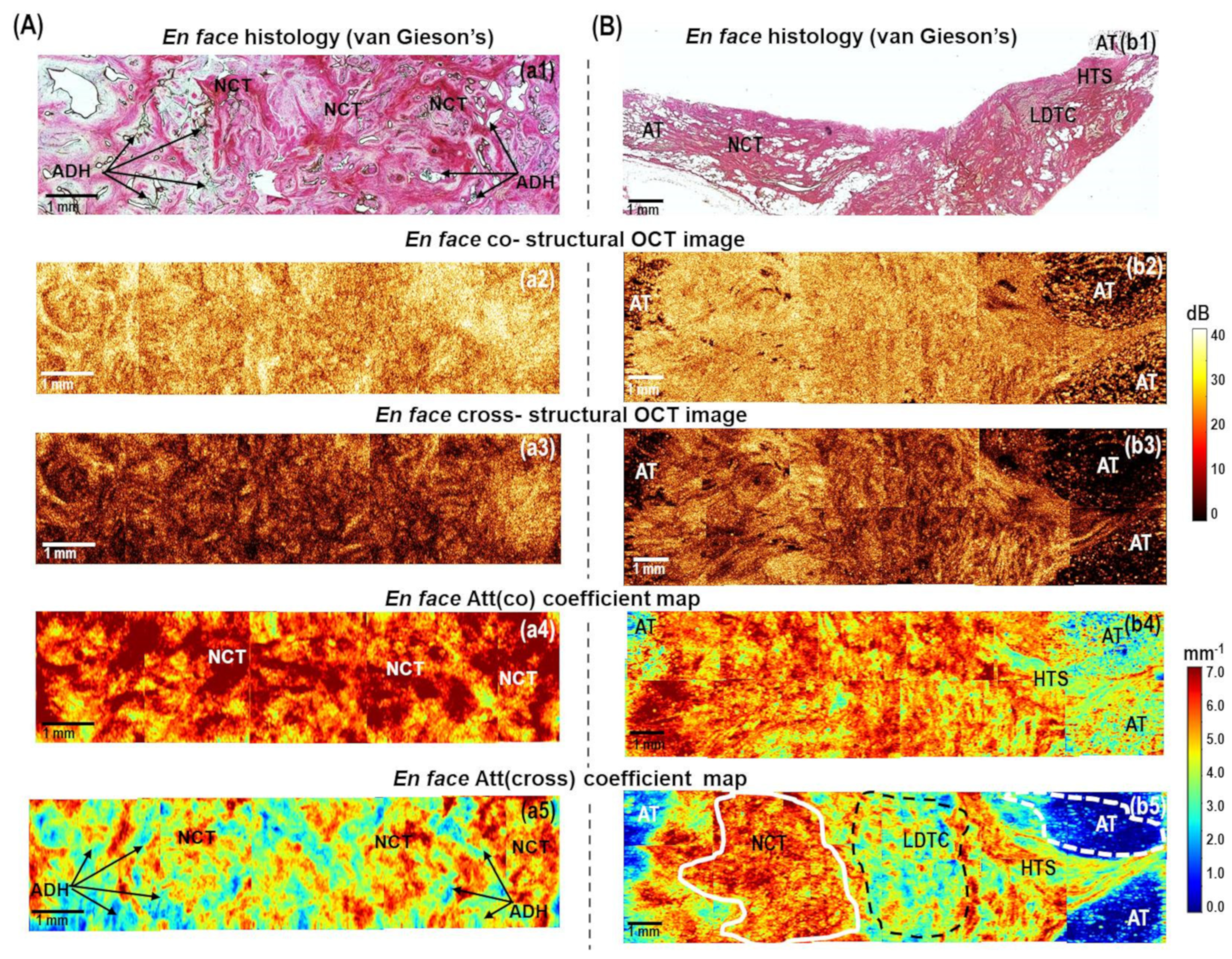
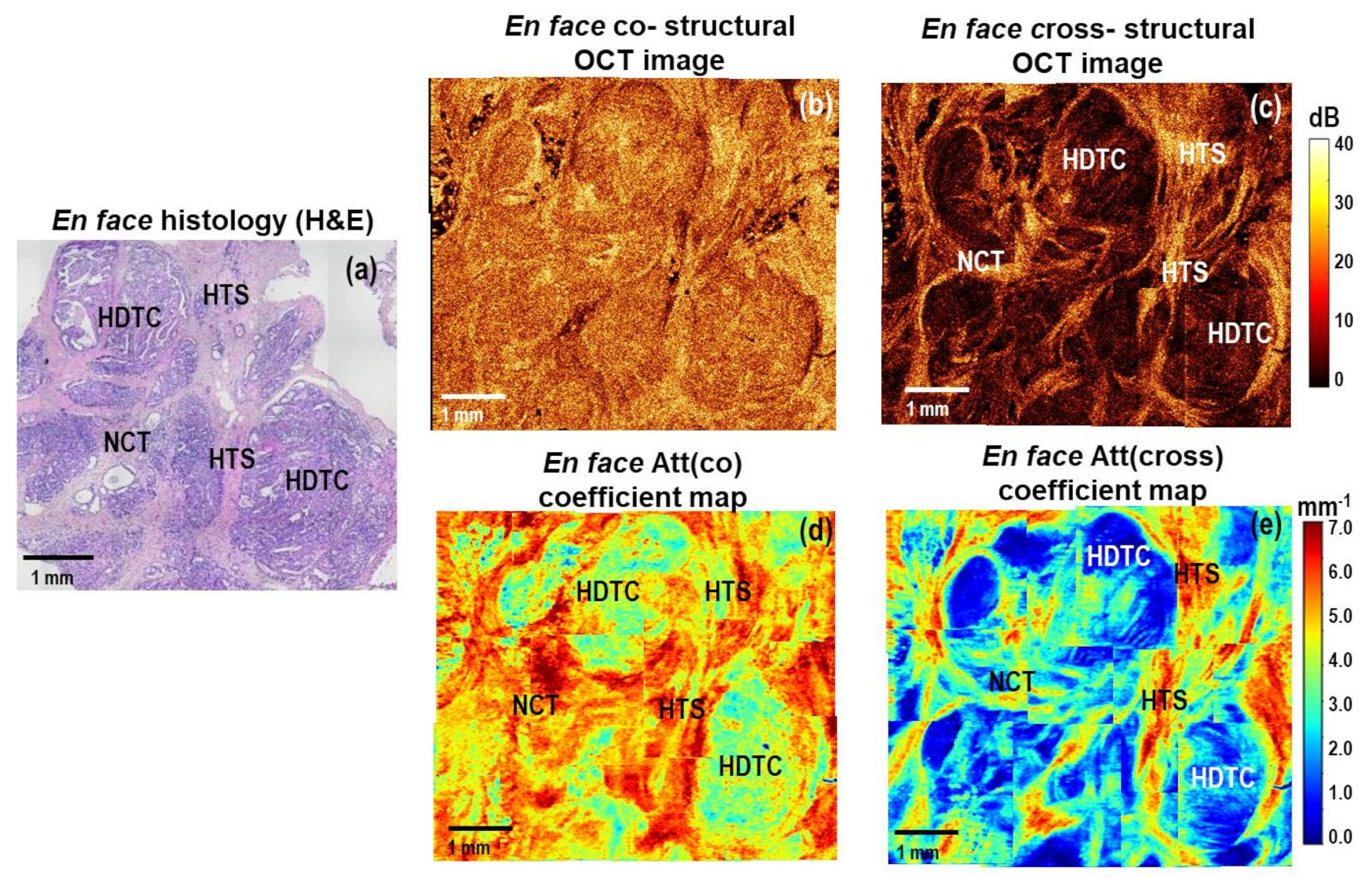
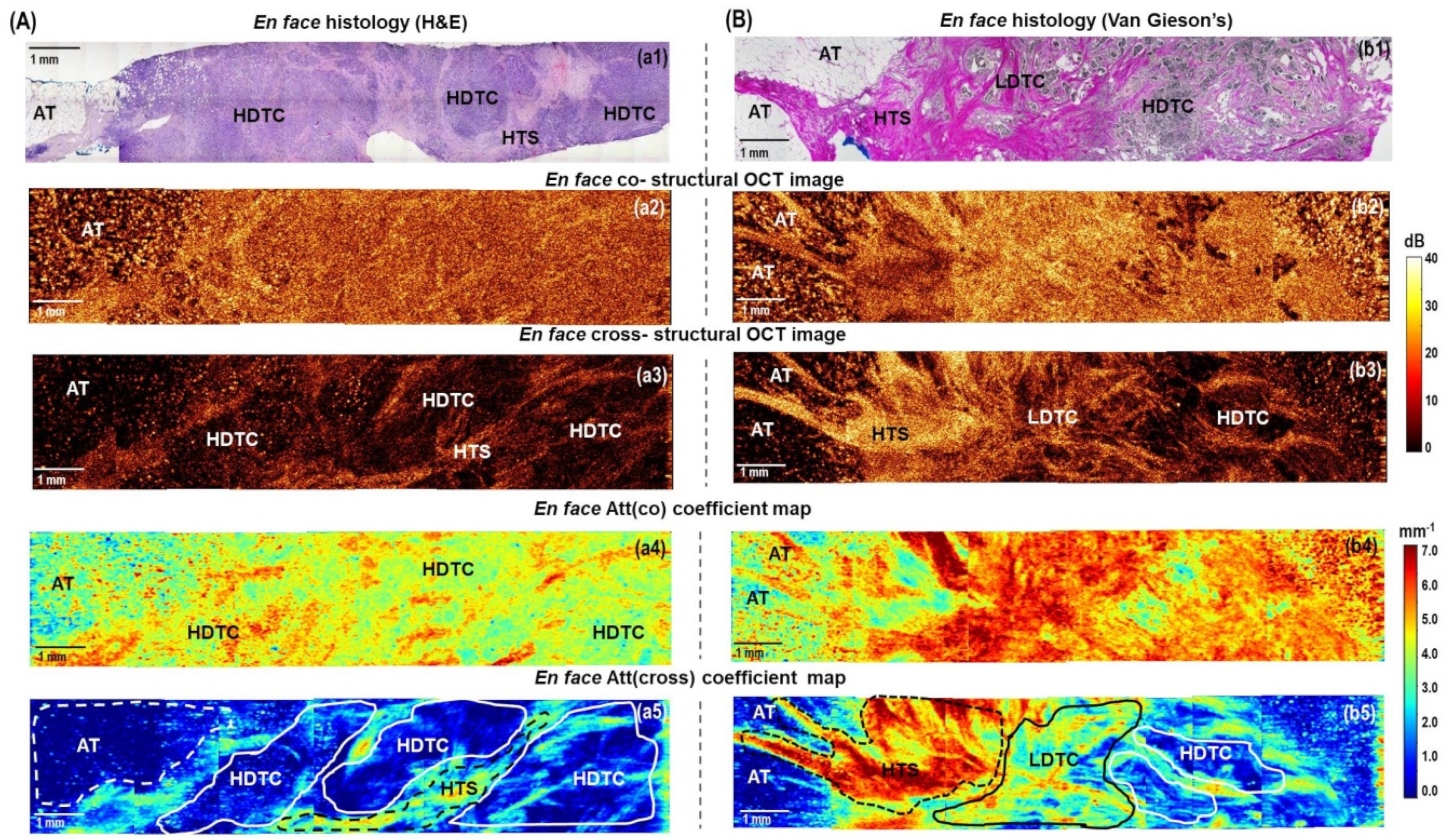
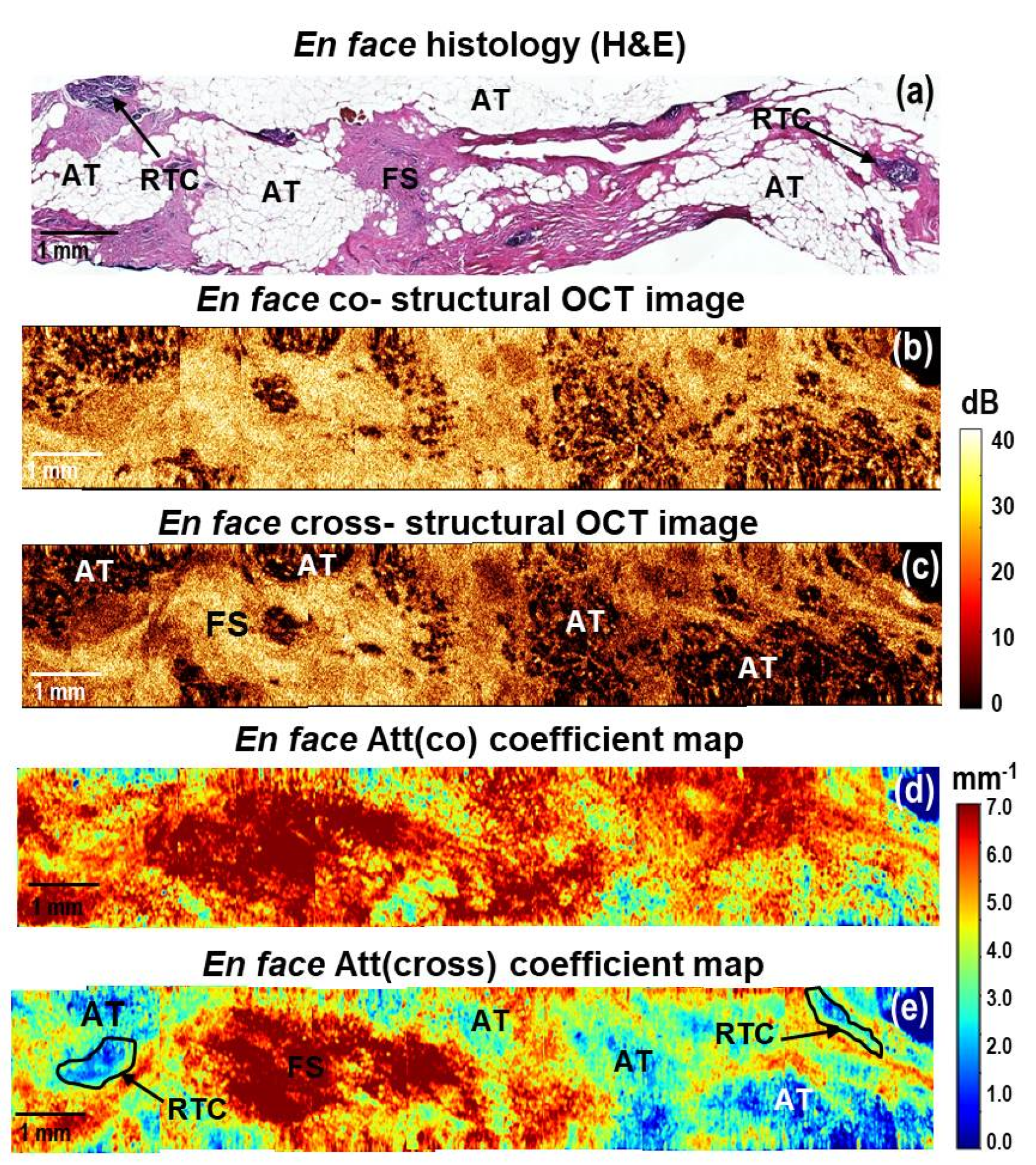
3.1. Color-Coded Attenuation Coefficient Maps in Differentiation of Breast Cancer Subtypes
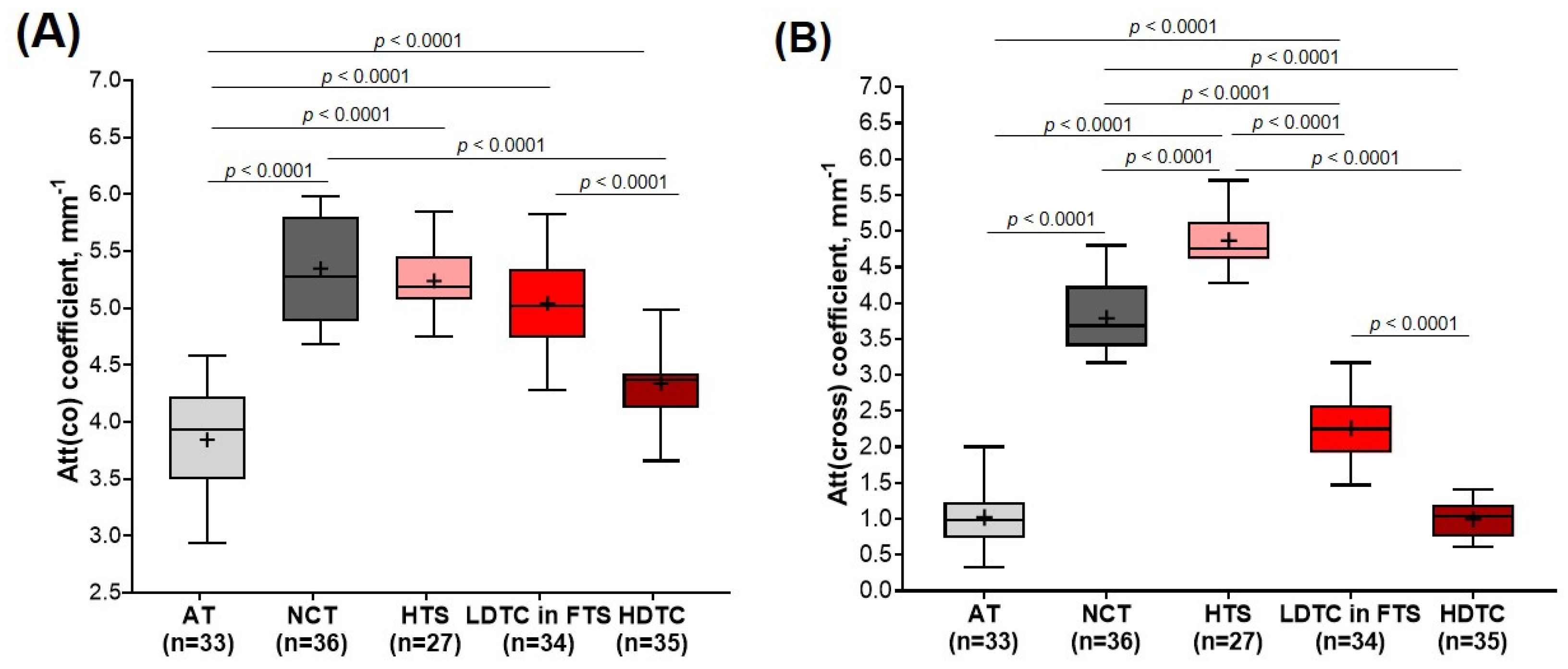
3.2. Comparison of Attenuation Coefficients for Breast Tissue Types Differentiation
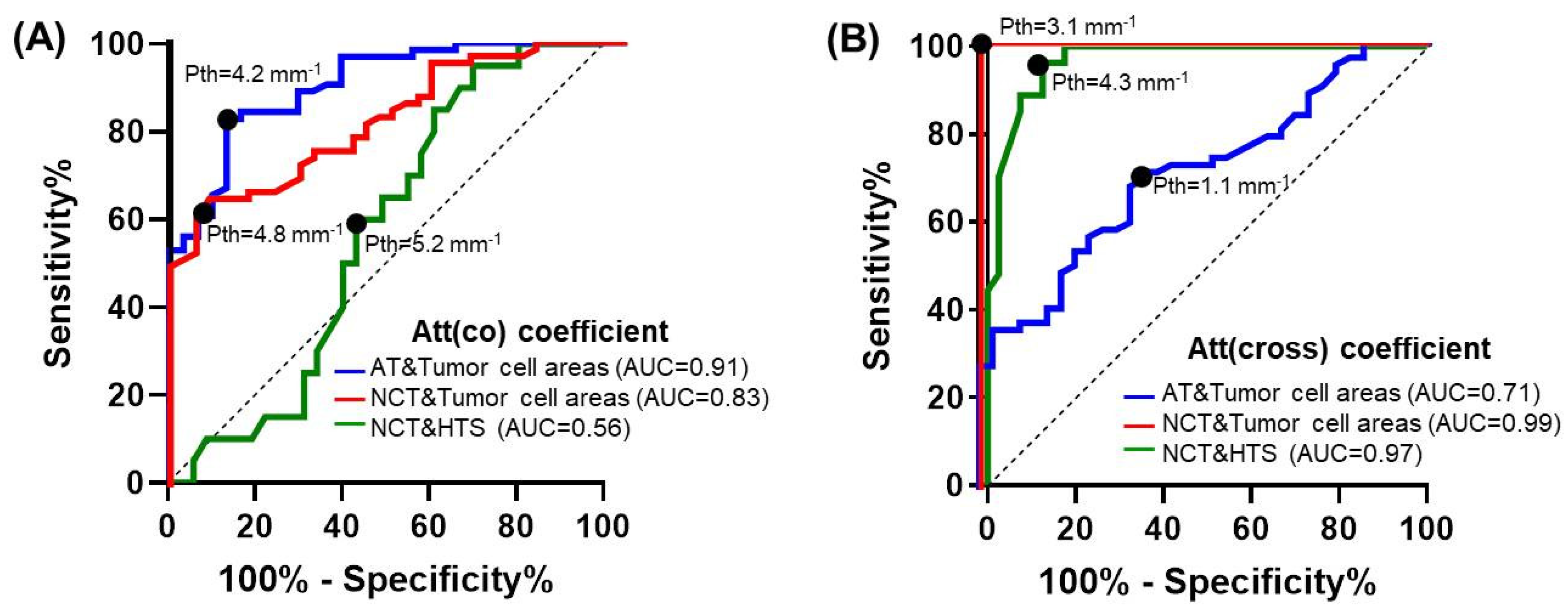
3.3. Diagnostic Accuracy of Attenuation Coefficients for Breast Tissue Type Differentiation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, L.; Gathani, T. Understanding Breast Cancer as a Global Health Concern. BJR 2022, 95, 20211033. [Google Scholar] [CrossRef] [PubMed]
- Fajdic, J.; Djurovic, D.; Gotovac, N.; Hrgovic, Z. Criteria and Procedures for Breast Conserving Surgery. Acta Inf. Med. 2013, 21, 16. [Google Scholar] [CrossRef] [PubMed]
- Bundred, J.R.; Michael, S.; Stuart, B.; Cutress, R.I.; Beckmann, K.; Holleczek, B.; Dahlstrom, J.E.; Gath, J.; Dodwell, D.; Bundred, N.J. Margin Status and Survival Outcomes after Breast Cancer Conservation Surgery: Prospectively Registered Systematic Review and Meta-Analysis. BMJ 2022, 378, e070346. [Google Scholar] [CrossRef]
- Houssami, N.; Macaskill, P.; Luke Marinovich, M.; Morrow, M. The Association of Surgical Margins and Local Recurrence in Women with Early-Stage Invasive Breast Cancer Treated with Breast-Conserving Therapy: A Meta-Analysis. Ann. Surg. Oncol. 2014, 21, 717–730. [Google Scholar] [CrossRef]
- Azu, M.; Abrahamse, P.; Katz, S.J.; Jagsi, R.; Morrow, M. What Is an Adequate Margin for Breast-Conserving Surgery? Surgeon Attitudes and Correlates. Ann. Surg. Oncol. 2010, 17, 558–563. [Google Scholar] [CrossRef]
- Morrow, M. Breast Conservation and Negative Margins: How Much Is Enough? Breast 2009, 18, S84–S86. [Google Scholar] [CrossRef]
- Aleskandarany, M.A.; Vandenberghe, M.E.; Marchiò, C.; Ellis, I.O.; Sapino, A.; Rakha, E.A. Tumour Heterogeneity of Breast Cancer: From Morphology to Personalised Medicine. Pathobiology 2018, 85, 23–34. [Google Scholar] [CrossRef]
- Iwao, K. Molecular Classification of Primary Breast Tumors Possessing Distinct Prognostic Properties. Hum. Mol. Genet. 2002, 11, 199–206. [Google Scholar] [CrossRef]
- De Glas, N.A.; Kiderlen, M.; Liefers, G.-J. Survival after Lumpectomy and Mastectomy for Early Stage Invasive Breast Cancer: The Effect of Age and Hormone Receptor Status: Correspondence. Cancer 2013, 119, 3253–3254. [Google Scholar] [CrossRef]
- Rezai, M.; Kern, P. Targeted Breast Surgery Targeting Breast Cancer. In Breast Cancer Essentials; Rezai, M., Kocdor, M.A., Canturk, N.Z., Eds.; Springer International Publishing: Cham, Switzerland, 2021; pp. 245–252. ISBN 9783030731465. [Google Scholar]
- Esbona, K.; Li, Z.; Wilke, L.G. Intraoperative Imprint Cytology and Frozen Section Pathology for Margin Assessment in Breast Conservation Surgery: A Systematic Review. Ann. Surg. Oncol. 2012, 19, 3236–3245. [Google Scholar] [CrossRef] [PubMed]
- Maloney, B.W.; McClatchy, D.M.; Pogue, B.W.; Paulsen, K.D.; Wells, W.A.; Barth, R.J. Review of Methods for Intraoperative Margin Detection for Breast Conserving Surgery. J. Biomed. Opt. 2018, 23, 100901. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, F.; Boolbol, S.K.; Gittleman, M.; Karni, T.; Tafra, L.; Feldman, S.; Police, A.; Friedman, N.B.; Karlan, S.; Holmes, D.; et al. A Randomized Prospective Study of Lumpectomy Margin Assessment with Use of MarginProbe in Patients with Nonpalpable Breast Malignancies. Ann. Surg. Oncol. 2014, 21, 1589–1595. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.Q.; Bydlon, T.M.; Kennedy, S.A.; Caldwell, M.L.; Gallagher, J.E.; Junker, M.; Wilke, L.G.; Barry, W.T.; Geradts, J.; Ramanujam, N. Optical Spectral Surveillance of Breast Tissue Landscapes for Detection of Residual Disease in Breast Tumor Margins. PLoS ONE 2013, 8, e69906. [Google Scholar] [CrossRef] [PubMed]
- Abeytunge, S.; Li, Y.; Larson, B.; Peterson, G.; Seltzer, E.; Toledo-Crow, R.; Rajadhyaksha, M. Confocal Microscopy with Strip Mosaicing for Rapid Imaging over Large Areas of Excised Tissue. J. Biomed. Opt. 2013, 18, 061227. [Google Scholar] [CrossRef] [PubMed]
- Keller, M.D.; Vargis, E.; de Matos Granja, N.; Wilson, R.H.; Mycek, M.-A.; Kelley, M.C.; Mahadevan-Jansen, A. Development of a Spatially Offset Raman Spectroscopy Probe for Breast Tumor Surgical Margin Evaluation. J. Biomed. Opt. 2011, 16, 077006. [Google Scholar] [CrossRef] [PubMed]
- Boppart, S.A.; Luo, W.; Marks, D.L.; Singletary, K.W. Optical Coherence Tomography: Feasibility for Basic Research and Image-Guided Surgery of Breast Cancer. Breast Cancer Res. Treat. 2004, 84, 85–97. [Google Scholar] [CrossRef]
- Schmidt, H.; Connolly, C.; Jaffer, S.; Oza, T.; Weltz, C.R.; Port, E.R.; Corben, A. Evaluation of Surgically Excised Breast Tissue Microstructure Using Wide-field Optical Coherence Tomography. Breast J. 2020, 26, 917–923. [Google Scholar] [CrossRef]
- Ha, R.; Friedlander, L.C.; Hibshoosh, H.; Hendon, C.; Feldman, S.; Ahn, S.; Schmidt, H.; Akens, M.K.; Fitzmaurice, M.; Wilson, B.C.; et al. Optical Coherence Tomography: A Novel Imaging Method for Post-lumpectomy Breast Margin Assessment-A Multi-reader Study. Acad. Radiol. 2018, 25, 279–287. [Google Scholar] [CrossRef]
- Nguyen, F.T.; Zysk, A.M.; Chaney, E.J.; Kotynek, J.G.; Oliphant, U.J.; Bellafiore, F.J.; Rowland, K.M.; Johnson, P.A.; Boppart, S.A. Intraoperative Evaluation of Breast Tumor Margins with Optical Coherence Tomography. Cancer Res. 2009, 69, 8790–8796. [Google Scholar] [CrossRef]
- Erickson-Bhatt, S.J.; Nolan, R.M.; Shemonski, N.D.; Adie, S.G.; Putney, J.; Darga, D.; McCormick, D.T.; Cittadine, A.J.; Zysk, A.M.; Marjanovic, M.; et al. Real-Time Imaging of the Resection Bed Using a Handheld Probe to Reduce Incidence of Microscopic Positive Margins in Cancer Surgery. Cancer Res. 2015, 75, 3706–3712. [Google Scholar] [CrossRef] [PubMed]
- Villiger, M.; Lorenser, D.; McLaughlin, R.A.; Quirk, B.C.; Kirk, R.W.; Bouma, B.E.; Sampson, D.D. Deep Tissue Volume Imaging of Birefringence through Fibre-Optic Needle Probes for the Delineation of Breast Tumour. Sci. Rep. 2016, 6, 28771. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Gan, Y.; Chang, E.; Hibshoosh, H.; Feldman, S.; Hendon, C. Visualization and Tissue Classification of Human Breast Cancer Images Using Ultrahigh-Resolution OCT: Visualization and Tissue Classification of Human Breast. Lasers Surg. Med. 2017, 49, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Dabbs, D.J. Brest Pathology; Elsevier: London, UK, 2012. [Google Scholar]
- Provenzano, P.P.; Eliceiri, K.W.; Campbell, J.M.; Inman, D.R.; White, J.G.; Keely, P.J. Collagen Reorganization at the Tumor-Stromal Interface Facilitates Local Invasion. BMC Med. 2006, 4, 38. [Google Scholar] [CrossRef]
- Uddin, M.N.; Wang, X. Identification of Key Tumor Stroma-Associated Transcriptional Signatures Correlated with Survival Prognosis and Tumor Progression in Breast Cancer. Breast Cancer 2022, 29, 541–561. [Google Scholar] [CrossRef]
- Kennedy, K.M.; Zilkens, R.; Allen, W.M.; Foo, K.Y.; Fang, Q.; Chin, L.; Sanderson, R.W.; Anstie, J.; Wijesinghe, P.; Curatolo, A.; et al. Diagnostic Accuracy of Quantitative Micro-Elastography for Margin Assessment in Breast-Conserving Surgery. Cancer Res. 2020, 80, 1773–1783. [Google Scholar] [CrossRef]
- Gubarkova, E.V.; Sovetsky, A.A.; Zaitsev, V.Y.; Matveyev, A.L.; Vorontsov, D.A.; Sirotkina, M.A.; Matveev, L.A.; Plekhanov, A.A.; Pavlova, N.P.; Kuznetsov, S.S.; et al. OCT-Elastography-Based Optical Biopsy for Breast Cancer Delineation and Express Assessment of Morphological/Molecular Subtypes. Biomed. Opt. Express 2019, 10, 2244. [Google Scholar] [CrossRef]
- Foo, K.Y.; Chin, L.; Zilkens, R.; Lakhiani, D.D.; Fang, Q.; Sanderson, R.; Dessauvagie, B.F.; Latham, B.; McLaren, S.; Saunders, C.M.; et al. Three-dimensional Mapping of the Attenuation Coefficient in Optical Coherence Tomography to Enhance Breast Tissue Microarchitecture Contrast. J. Biophotonics 2020, 13, e201960201. [Google Scholar] [CrossRef]
- South, F.A.; Chaney, E.J.; Marjanovic, M.; Adie, S.G.; Boppart, S.A. Differentiation of Ex Vivo Human Breast Tissue Using Polarization-Sensitive Optical Coherence Tomography. Biomed. Opt. Express 2014, 5, 3417. [Google Scholar] [CrossRef]
- Patel, R.; Khan, A.; Quinlan, R.; Yaroslavsky, A.N. Polarization-Sensitive Multimodal Imaging for Detecting Breast Cancer. Cancer Res. 2014, 74, 4685–4693. [Google Scholar] [CrossRef]
- Liu, Y.; Adamson, R.; Galan, M.; Hubbi, B.; Liu, X. Quantitative Characterization of Human Breast Tissue Based on Deep Learning Segmentation of 3D Optical Coherence Tomography Images. Biomed. Opt. Express 2021, 12, 2647. [Google Scholar] [CrossRef] [PubMed]
- Foo, K.Y.; Newman, K.; Fang, Q.; Gong, P.; Ismail, H.M.; Lakhiani, D.D.; Zilkens, R.; Dessauvagie, B.F.; Latham, B.; Saunders, C.M.; et al. Multi-Class Classification of Breast Tissue Using Optical Coherence Tomography and Attenuation Imaging Combined via Deep Learning. Biomed. Opt. Express 2022, 13, 3380. [Google Scholar] [CrossRef] [PubMed]
- Kansal, S.; Bhattacharya, J.; Srivastava, V. Automated Full-Field Polarization-Sensitive Optical Coherence Tomography Diagnostic Systems for Breast Cancer. Appl. Opt. 2020, 59, 7688. [Google Scholar] [CrossRef]
- Zhu, D.; Wang, J.; Marjanovic, M.; Chaney, E.J.; Cradock, K.A.; Higham, A.M.; Liu, Z.G.; Gao, Z.; Boppart, S.A. Differentiation of Breast Tissue Types for Surgical Margin Assessment Using Machine Learning and Polarization-Sensitive Optical Coherence Tomography. Biomed. Opt. Express 2021, 12, 3021. [Google Scholar] [CrossRef] [PubMed]
- Gelikonov, V.M.; Romashov, V.N.; Shabanov, D.V.; Ksenofontov, S.Y.; Terpelov, D.A.; Shilyagin, P.A.; Gelikonov, G.V.; Vitkin, I.A. Cross-Polarization Optical Coherence Tomography with Active Maintenance of the Circular Polarization of a Sounding Wave in a Common Path System. Radiophys. Quantum Electron. 2018, 60, 897–911. [Google Scholar] [CrossRef]
- Gubarkova, E.V.; Kiseleva, E.B.; Sirotkina, M.A.; Vorontsov, D.A.; Achkasova, K.A.; Kuznetsov, S.S.; Yashin, K.S.; Matveyev, A.L.; Sovetsky, A.A.; Matveev, L.A.; et al. Diagnostic Accuracy of Cross-Polarization OCT and OCT-Elastography for Differentiation of Breast Cancer Subtypes: Comparative Study. Diagnostics 2020, 10, 994. [Google Scholar] [CrossRef]
- Yashin, K.S.; Kiseleva, E.B.; Gubarkova, E.V.; Moiseev, A.A.; Kuznetsov, S.S.; Shilyagin, P.A.; Gelikonov, G.V.; Medyanik, I.A.; Kravets, L.Y.; Potapov, A.A.; et al. Cross-Polarization Optical Coherence Tomography for Brain Tumor Imaging. Front. Oncol. 2019, 9, 201. [Google Scholar] [CrossRef]
- Kiseleva, E.; Kirillin, M.; Feldchtein, F.; Vitkin, A.; Sergeeva, E.; Zagaynova, E.; Streltzova, O.; Shakhov, B.; Gubarkova, E.; Gladkova, N. Differential Diagnosis of Human Bladder Mucosa Pathologies in Vivo with Cross-Polarization Optical Coherence Tomography. Biomed. Opt. Express 2015, 6, 1464. [Google Scholar] [CrossRef]
- Yashin, K.S.; Kiseleva, E.B.; Moiseev, A.A.; Kuznetsov, S.S.; Timofeeva, L.B.; Pavlova, N.P.; Gelikonov, G.V.; Medyanik, I.A.; Kravets, L.Y.; Zagaynova, E.V.; et al. Quantitative Nontumorous and Tumorous Human Brain Tissue Assessment Using Microstructural Co- and Cross-Polarized Optical Coherence Tomography. Sci. Rep. 2019, 9, 2024. [Google Scholar] [CrossRef]
- Gubarkova, E.V.; Moiseev, A.A.; Kiseleva, E.B.; Vorontsov, D.A.; Kuznetsov, S.S.; Vorontsov, A.Y.; Gelikonov, G.V.; Sirotkina, M.A.; Gladkova, N.D. Tissue Optical Properties Estimation from Cross-Polarization OCT Data for Breast Cancer Margin Assessment. Laser Phys. Lett. 2020, 17, 075602. [Google Scholar] [CrossRef]
- Moiseev, A.A.; Achkasova, K.A.; Kiseleva, E.B.; Yashin, K.S.; Potapov, A.L.; Bederina, E.L.; Kuznetsov, S.S.; Sherstnev, E.P.; Shabanov, D.V.; Gelikonov, G.V.; et al. Brain White Matter Morphological Structure Correlation with Its Optical Properties Estimated from Optical Coherence Tomography (OCT) Data. Biomed. Opt. Express 2022, 13, 2393. [Google Scholar] [CrossRef] [PubMed]
- Tyulyandin, S.A.; Zhukova, L.G.; Koroleva, I.A.; Parokonnaya, A.A.; Semiglazova, T.Y.; Stenina, M.B.; Frolova, M.A. Practical recommendations for drug treatment of breast cancer. Malig. Tumors Pract. Guidel. RUSSCO 2021, 11, 119–157. [Google Scholar]
- Cardoso, F.; Kyriakides, S.; Ohno, S.; Penault-Llorca, F.; Poortmans, P.; Rubio, I.T.; Zackrisson, S.; Senkus, E. Early Breast Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2019, 30, 1194–1220. [Google Scholar] [CrossRef]
- Vermeer, K.A.; Mo, J.; Weda, J.J.A.; Lemij, H.G.; De Boer, J.F. Depth-Resolved Model-Based Reconstruction of Attenuation Coefficients in Optical Coherence Tomography. Biomed. Opt. Express 2014, 5, 322. [Google Scholar] [CrossRef]
- Symmans, W.F.; Peintinger, F.; Hatzis, C.; Rajan, R.; Kuerer, H.; Valero, V.; Assad, L.; Poniecka, A.; Hennessy, B.; Green, M.; et al. Measurement of Residual Breast Cancer Burden to Predict Survival After Neoadjuvant Chemotherapy. JCO 2007, 25, 4414–4422. [Google Scholar] [CrossRef]
- Pritt, B.; Tessitore, J.J.; Weaver, D.L.; Blaszyk, H. The effect of tissue fixation and processing on breast cancer size. Hum. Pathol. 2005, 36, 756–760. [Google Scholar] [CrossRef]
- Drexler, W.; Liu, M.; Kumar, A.; Kamali, T.; Unterhuber, A.; Leitgeb, R.A. Optical Coherence Tomography Today: Speed, Contrast, and Multimodality. J. Biomed. Opt. 2014, 19, 071412. [Google Scholar] [CrossRef]
- Hsiung, P.L.; Nambiar, P.R.; Fujimoto, J.G. Effect of tissue preservation on imaging using ultrahigh resolution optical coherence tomography. J. Biomed. Opt. 2005, 10, 064033. [Google Scholar] [CrossRef]
- Feuerman, M.; Miller, A.R. Relationships between Statistical Measures of Agreement: Sensitivity, Specificity and Kappa: Statistical Measures of Agreement. J. Eval. Clin. Pract. 2008, 14, 930–933. [Google Scholar] [CrossRef]
- Zimmermann, A. Tumor Stroma, Desmoplasia, and Stromagenesis. In Tumors and Tumor-like Lesions of the Hepatobiliary Tract; Springer International Publishing: Cham, Switzerland, 2017; pp. 3409–3440. ISBN 9783319269542. [Google Scholar]
- Hirabayashi, K.; Kawanishi, A.; Morimachi, M.; Yamada, M.; Takanashi, Y.; Hori, S.; Serizawa, A.; Saika, T.; Nakagohri, T.; Nakamura, N. Hyalinized Stroma Is a Characteristic Feature of Pancreatic Intraductal Oncocytic Papillary Neoplasm: An Immunohistochemical Study. Ann. Diagn. Pathol. 2020, 49, 151639. [Google Scholar] [CrossRef]
- Leitgeb, R.; Placzek, F.; Rank, E.; Krainz, L.; Haindl, R.; Li, Q.; Liu, M.; Andreana, M.; Unterhuber, A.; Schmoll, T.; et al. Enhanced Medical Diagnosis for DOCTors: A Perspective of Optical Coherence Tomography. J. Biomed. Opt. 2021, 26, 100601. [Google Scholar] [CrossRef] [PubMed]
- Moran, M.S.; Schnitt, S.J.; Giuliano, A.E.; Harris, J.R.; Khan, S.A.; Horton, J.; Klimberg, S.; Chavez-MacGregor, M.; Freedman, G.; Houssami, N.; et al. Society of Surgical Oncology–American Society for Radiation Oncology Consensus Guideline on Margins for Breast-Conserving Surgery With Whole-Breast Irradiation in Stages I and II Invasive Breast Cancer. JCO 2014, 32, 1507–1515. [Google Scholar] [CrossRef] [PubMed]
- Morrow, M.; Van Zee, K.J.; Solin, L.J.; Houssami, N.; Chavez-MacGregor, M.; Harris, J.R.; Horton, J.; Hwang, S.; Johnson, P.L.; Marinovich, M.L.; et al. Society of Surgical Oncology–American Society for Radiation Oncology–American Society of Clinical Oncology Consensus Guideline on Margins for Breast-Conserving Surgery With Whole-Breast Irradiation in Ductal Carcinoma in Situ. Pract. Radiat. Oncol. 2016, 6, 287–295. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xu, Y.; Boppart, S.A. Review of Optical Coherence Tomography in Oncology. J. Biomed. Opt. 2017, 22, 121711. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AUC (95% CI) | Sensitivity (95% CI) | Specificity (95% CI) | Diagnostic Accuracy (95% CI) | The Optimal Cutoff (Pth), Yielding Maximal Sum of Sensitivity and Specificity | |
|---|---|---|---|---|---|
| Attenuation (co) coefficient | |||||
| Tumor cell areas vs. Adipose tissue | 0.91 (0.85; 0.96) | 84% (74%; 91%) | 84% (68%; 93%) | 83% (78%; 86%) | >4.2 mm−1 |
| Tumor cell areas vs. Non-tumorous connective tissue | 0.83 (0.75; 0.90) | 65% (53%; 75%) | 91% (77%; 97%) | 78% (71%; 90%) | <4.8 mm−1 |
| Hyalinized tumor stroma vs. Non-tumorous connective tissue | 0.56 (0.44; 0.68) | 60% (39%; 78%) | 56% (45%; 68%) | 58% (45%; 70%) | <5.2 mm−1 |
| Attenuation (cross) coefficient | |||||
| Tumor cell areas vs. Adipose tissue | 0.71 (0.61; 0.82) | 68% (56%; 78%) | 66% (50%; 80%) | 67% (67%; 88%) | >1.1 mm−1 |
| Tumor cell areas vs. Non-tumorous connective tissue | 0.99 (0.99; 1.0) | 98% (91%; 99%) | 99% (91%; 1.0%) | 99% (98%; 1.0%) | <3.1 mm−1 |
| Hyalinized tumor stroma vs. Non-tumorous connective tissue | 0.97 (0.93; 1.0) | 96% (82%; 99%) | 87% (74%; 94%) | 91% (84%; 97%) | >4.3 mm−1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gubarkova, E.; Kiseleva, E.; Moiseev, A.; Vorontsov, D.; Kuznetsov, S.; Plekhanov, A.; Karabut, M.; Sirotkina, M.; Gelikonov, G.; Gamayunov, S.; et al. Intraoperative Assessment of Breast Cancer Tissues after Breast-Conserving Surgery Based on Mapping the Attenuation Coefficients in 3D Cross-Polarization Optical Coherence Tomography. Cancers 2023, 15, 2663. https://doi.org/10.3390/cancers15092663
Gubarkova E, Kiseleva E, Moiseev A, Vorontsov D, Kuznetsov S, Plekhanov A, Karabut M, Sirotkina M, Gelikonov G, Gamayunov S, et al. Intraoperative Assessment of Breast Cancer Tissues after Breast-Conserving Surgery Based on Mapping the Attenuation Coefficients in 3D Cross-Polarization Optical Coherence Tomography. Cancers. 2023; 15(9):2663. https://doi.org/10.3390/cancers15092663
Chicago/Turabian StyleGubarkova, Ekaterina, Elena Kiseleva, Alexander Moiseev, Dmitry Vorontsov, Sergey Kuznetsov, Anton Plekhanov, Maria Karabut, Marina Sirotkina, Grigory Gelikonov, Sergey Gamayunov, and et al. 2023. "Intraoperative Assessment of Breast Cancer Tissues after Breast-Conserving Surgery Based on Mapping the Attenuation Coefficients in 3D Cross-Polarization Optical Coherence Tomography" Cancers 15, no. 9: 2663. https://doi.org/10.3390/cancers15092663
APA StyleGubarkova, E., Kiseleva, E., Moiseev, A., Vorontsov, D., Kuznetsov, S., Plekhanov, A., Karabut, M., Sirotkina, M., Gelikonov, G., Gamayunov, S., Vorontsov, A., Krivorotko, P., & Gladkova, N. (2023). Intraoperative Assessment of Breast Cancer Tissues after Breast-Conserving Surgery Based on Mapping the Attenuation Coefficients in 3D Cross-Polarization Optical Coherence Tomography. Cancers, 15(9), 2663. https://doi.org/10.3390/cancers15092663