
Personalized Medicine in Infant Population with Cancer: Pharmacogenetic Pilot Study of Polymorphisms Related to Toxicity and Response to Chemotherapy

 , ,
, ,  , , , , ,
, , , , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
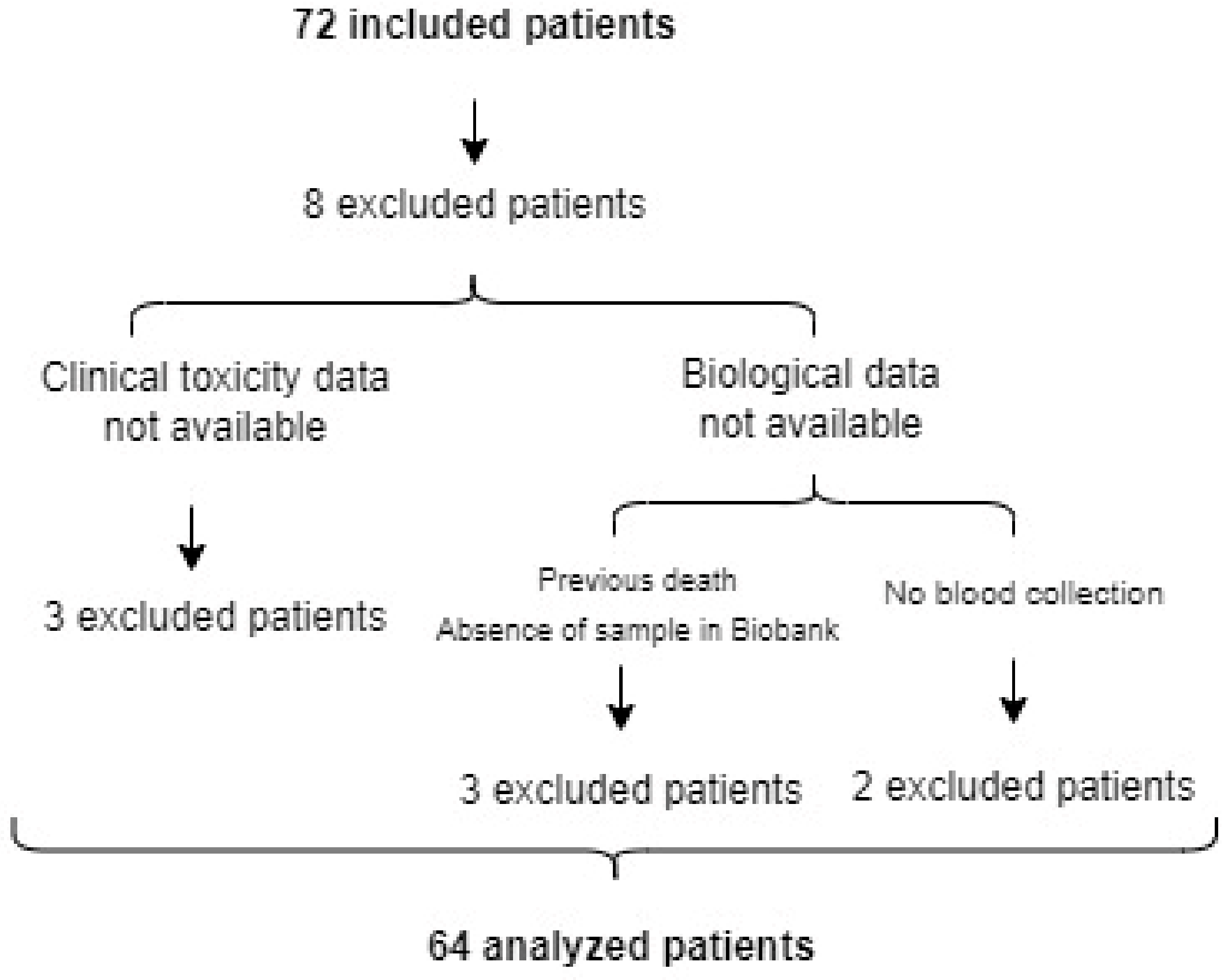
2.1. Study Design
2.2. Clinical Parameters
2.2.1. Drugs and Therapeutic Schemes
2.2.2. Clinical and Analytical Toxicity. Survival Data
2.3. Genetic Variants
2.3.1. SNPs Selection
2.3.2. Samples and DNA Extraction
2.3.3. Genotyping
2.4. Statistics
3. Results
3.1. Descriptive Data
3.1.1. Chemotherapy Drugs Administered
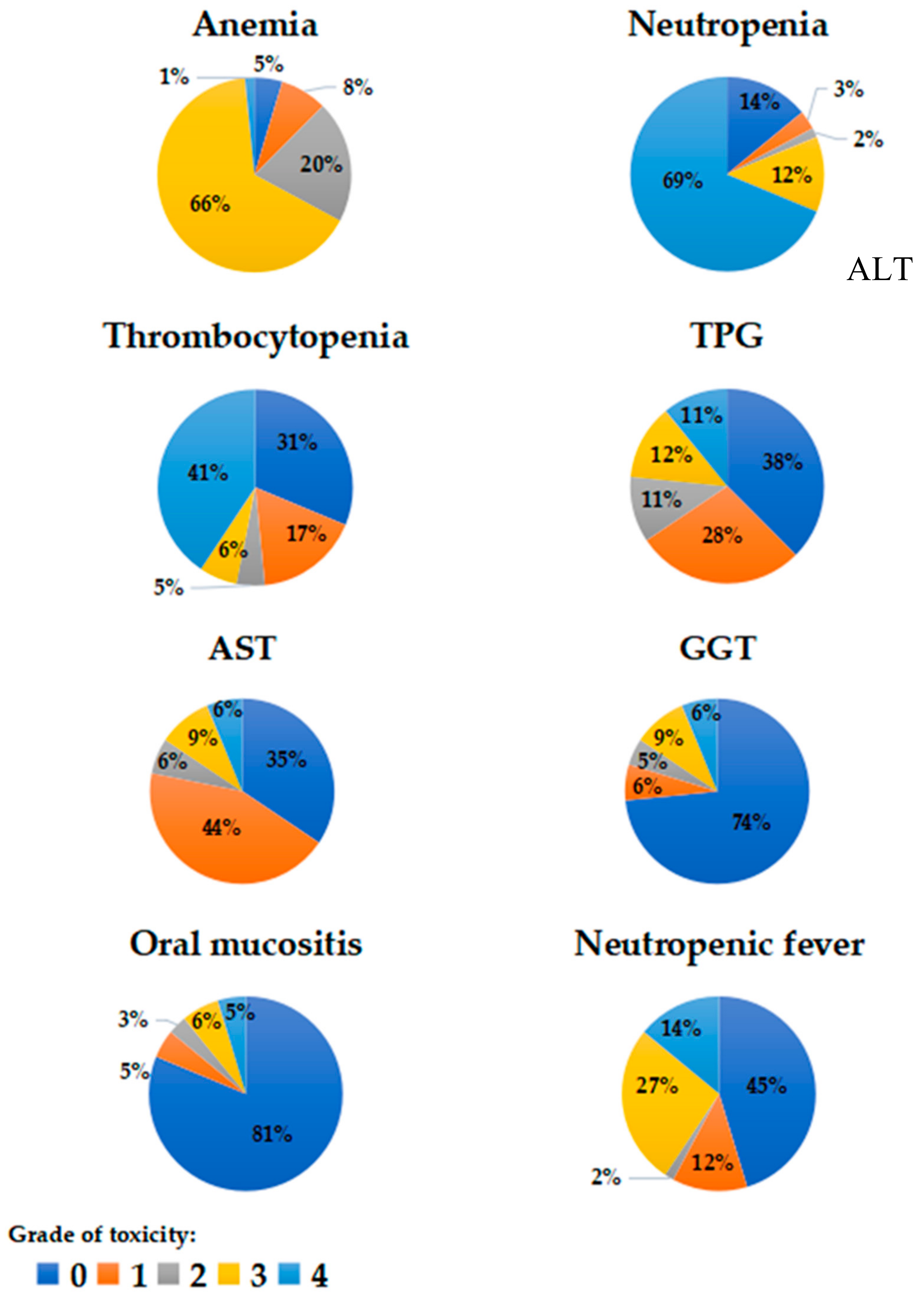
3.1.2. Clinical and Analytical Toxicities
3.1.3. Genotyping
3.2. Correlation between Genetic Polymorphisms and Toxicity
3.3. Correlation between Polymorphisms and Survival
3.3.1. Overall Survival (OS)
3.3.2. Event-Free Survival
4. Discussion
4.1. Hematological Toxicities
4.2. Survival
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Registro Español de Tumores Infantiles RETI-SEHOP. Available online: https://www.uv.es/rnti/informes.html (accessed on 24 November 2022).
- Spear, B.B.; Heath-Chiozzi, M.; Huff, J. Clinical application of pharmacogenetics. Trends Mol. Med. 2001, 7, 201–204. [Google Scholar] [CrossRef] [PubMed]
- Lazarou, J.; Pomeranz, B.H.; Corey, P.N. Incidence of Adverse Drug Reactions in Hospitalized Patients. J. Am. Med. Assoc. 1998, 279, 1200–1205. [Google Scholar] [CrossRef] [PubMed]
- Elzagallaai, A.A.; Greff, M.J.E.; Rieder, M.J. Adverse Drug Reactions in Children: The Double-Edged Sword of Therapeutics. Clin. Pharmacol. Ther. 2017, 101, 725–735. [Google Scholar] [CrossRef] [PubMed]
- Impicciatore, P.; Choonara, I.; Clarkson, A.; Provasi, D.; Pandolfini, C.; Bonati, M. Incidence of adverse drug reactions in paediatric in/out-patients: A systematic review and meta-analysis of prospective studies. Br. J. Clin. Pharmacol. 2001, 52, 77–83. [Google Scholar] [CrossRef]
- Aagaard, L.; Christensen, A.; Hansen, E.H. Information about adverse drug reactions reported in children: A qualitative review of empirical studies. Br. J. Clin. Pharmacol. 2010, 70, 481–491. [Google Scholar] [CrossRef]
- Van Driest, S.L.; McGregor, T.L. Pharmacogenetics in clinical pediatrics: Challenges and strategies. Pers. Med. 2013, 10, 661–671. [Google Scholar] [CrossRef]
- Korbel, L.; George, M.; Kitzmiller, J. Clinically Relevant Pharmacogenomic Testing in Pediatric Practice. Clin. Pediatr. 2014, 53, 831–838. [Google Scholar] [CrossRef]
- Dotta, A.; Chukhlantseva, N. Ontogeny and drug metabolism in newborns. J. Matern. Neonatal Med. 2012, 25, 75–76. [Google Scholar] [CrossRef]
- Agunod, M.; Yamaguchi, N.; Lopez, R.; Luhby, A.L.; Glass, G.B.J. Correlative study of hydrochloric acid, pepsin, and intrinsic factor secretion in newborns and infants. Am. J. Dig. Dis. 1969, 14, 400–414. [Google Scholar] [CrossRef]
- Hyman, P.E.; Clarke, D.D.; Everett, S.L.; Sonne, B.; Stewart, D.; Harada, T.; Walsh, J.H.; Taylor, I.L. Gastric acid secretory function in preterm infants. J. Pediatr. 1985, 106, 467–471. [Google Scholar] [CrossRef]
- Lu, H.; Rosenbaum, S. Developmental Pharmacokinetics in Pediatric Populations. J. Pediatr. Pharmacol. Ther. 2014, 19, 262–276. [Google Scholar] [CrossRef]
- Mlakar, V.; Curtis, P.H.-D.; Uppugunduri, C.R.S.; Krajinovic, M.; Ansari, M. Pharmacogenomics in Pediatric Oncology: Review of Gene—Drug Associations for Clinical Use. Int. J. Mol. Sci. 2016, 17, 1502. [Google Scholar] [CrossRef]
- Kearns, G.L. Acetaminophen poisoning in children: Treat early and long enough. J. Pediatr. 2002, 140, 495–498. [Google Scholar] [CrossRef]
- Fernandez, E.; Perez, R.; Hernandez, A.; Tejada, P.; Arteta, M.; Ramos, J.T. Factors and Mechanisms for Pharmacokinetic Differences between Pediatric Population and Adults. Pharmaceutics 2011, 3, 53–72. [Google Scholar] [CrossRef]
- Huang, A.; Xu, S.; Cai, X. Empirical Bayesian elastic net for multiple quantitative trait locus mapping. Heredity 2015, 114, 107–115. [Google Scholar] [CrossRef]
- Zou, H.; Hastie, T. Regularization and variable selection via the elastic net. J. R. Stat. Soc. Ser. B Stat. Methodol. 2005, 67, 301–320. [Google Scholar] [CrossRef]
- Mostafa-Hedeab, G.; Elborai, Y.; Ebid, G.T.A. Effects of Methylene Tetrahydro Folate Reductase Gene Polymorphisms on Methotrexate Toxicity in Egyptian Pediatric Acute Lymphocytic Leukaemia Patients. Iran. J. Pharm. Res. 2020, 19, 387–393. [Google Scholar] [CrossRef]
- Han, J.-Y.; Shin, E.S.; Lee, Y.-S.; Ghang, H.Y.; Kim, S.-Y.; Hwang, J.-A.; Kim, J.Y.; Lee, J.S. A genome-wide association study for irinotecan-related severe toxicities in patients with advanced non-small-cell lung cancer. Pharm. J. 2012, 13, 417–422. [Google Scholar] [CrossRef]
- Gregers, J.; Gréen, H.; Christensen, I.J.; Dalhoff, K.; Schroeder, H.; Carlsen, N.; Rosthoej, S.; Lausen, B.; Schmiegelow, K.; Peterson, C. Polymorphisms in the ABCB1 gene and effect on outcome and toxicity in childhood acute lymphoblastic leukemia. Pharm. J. 2015, 15, 372–379. [Google Scholar] [CrossRef]
- Brown, A.L.; Lupo, P.J.; Okcu, M.F.; Lau, C.C.; Rednam, S.; Scheurer, M.E. SOD2 genetic variant associated with treatment-related ototoxicity in cisplatin-treated pediatric medulloblastoma. Cancer Med. 2015, 4, 1679–1686. [Google Scholar] [CrossRef]
- Olivera, G.G.; Yáñez, Y.; Gargallo, P.; Sendra, L.; Aliño, S.F.; Segura, V.; Sanz, M.Á.; Cañete, A.; Castel, V.; De Mora, J.F.; et al. MTHFR and VDR Polymorphisms Improve the Prognostic Value of MYCN Status on Overall Survival in Neuroblastoma Patients. Int. J. Mol. Sci. 2020, 21, 2714. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Li, W.; Zhu, J.; Chen, H.; Guan, J.; Zhou, D.; Zhen, Z.; Sun, F.; Huang, J.; Wang, J.; et al. Influence of MTHFR C677T and A1298C polymorphisms on the survival of pediatric patients with non-Hodgkin lymphoma. Leuk. Lymphoma 2021, 62, 2374–2382. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Du, M.; Vallis, J.; Shariati, M.; Parfrey, P.S.; Mclaughlin, J.R.; Wang, P.P.; Zhu, Y. The Roles of MTRR and MTHFR Gene Polymorphisms in Colorectal Cancer Survival. Nutrients 2022, 14, 4594. [Google Scholar] [CrossRef] [PubMed]
- Sheng, Y.; Li, F.; Qin, Z. TNF Receptor 2 Makes Tumor Necrosis Factor a Friend of Tumors. Front. Immunol. 2018, 9, 1170. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Deng, Z.; Yin, J.; Wang, S.; Lu, D.; Wen, X.; Li, X.; Xiao, D.; Hu, C.; Chen, X.; et al. The association of genetic variations in DNA repair pathways with severe toxicities in NSCLC patients undergoing platinum-based chemotherapy. Int. J. Cancer 2017, 141, 2336–2347. [Google Scholar] [CrossRef]
- Zhang, R.; Jia, M.; Xue, H.; Xu, Y.; Wang, M.; Zhu, M.; Sun, M.; Chang, J.; Wei, Q. Genetic variants in ERCC1 and XPC predict survival outcome of non-small cell lung cancer patients treated with platinum-based therapy. Sci. Rep. 2017, 7, 10702. [Google Scholar] [CrossRef] [PubMed]
- Amirimani, B.; Ning, B.; Deitz, A.C.; Weber, B.L.; Kadlubar, F.F.; Rebbeck, T.R. Increased transcriptional activity of theCYP3A4*1B promoter variant. Environ. Mol. Mutagen. 2003, 42, 299–305. [Google Scholar] [CrossRef]
- Schulte, R.R.; Choi, L.; Utreja, N.; Van Driest, S.L.; Stein, C.M.; Ho, R.H. Effect of SLCO1B1 Polymorphisms on High-Dose Methotrexate Clearance in Children and Young Adults with Leukemia and Lymphoblastic Lymphoma. Clin. Transl. Sci. 2021, 14, 343–353. [Google Scholar] [CrossRef]
- Iskierka-Jażdżewska, E.; Hus, M.; Giannopoulos, K.; Mądro, E.; Hołojda, J.; Piotrowska, M.; Zaucha, J.M.; Piszczek, W.; Szeremet, A.; Wojciechowska, M.; et al. Efficacy and toxicity of compassionate ibrutinib use in relapsed/refractory chronic lymphocytic leukemia in Poland: Analysis of the Polish Adult Leukemia Group (PALG). Leuk. Lymphoma 2017, 58, 2485–2488. [Google Scholar] [CrossRef]
- Ciccolini, J.; Evrard, A.; M’Batchi, L.; Pourroy, B.; Mercier, C.; Iliadis, A.; Lacarelle, B.; Verschuur, A.; Ouafik, L.; André, N. CDA deficiency as a possible culprit for life-threatening toxicities after cytarabine plus 6-mercaptopurine therapy: Pharmacogenetic investigations. Pharmacogenomics 2012, 13, 393–397. [Google Scholar] [CrossRef]
- Laverdière, C.; Chiasson, S.; Costea, I.; Moghrabi, A.; Krajinovic, M. Polymorphism G80A in the reduced folate carrier gene and its relationship to methotrexate plasma levels and outcome of childhood acute lymphoblastic leukemia. Blood 2002, 100, 3832–3834. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 1-A ANEMIA | |||
|---|---|---|---|
| GENE | SNP | VARIANT | ODDS RATIO |
| ATIC | rs16853826 | GG | 1.14 |
| MTHFR | rs1801131 | GT | 1.73 |
| DPYD | rs1801158 | TC | 1.08 |
| TNFRSF11B | rs2073618 | GG | 1.42 |
| UGT1A | rs4124874 | TT | 1.13 |
| ABCB1 | rs1045642 | GG | 0.91 |
| ITPA | rs1127354 | CC | 0.91 |
| FCGRA1 | rs1801274 | AG | 0.81 |
| ESR1 | rs2234693 | TT | 0.85 |
| XRCC1 | rs25487 | TT | 0.87 |
| CDA | rs3215400 | del.C | 0.86 |
| ATIC | rs4673993 | TT | 0.73 |
| 1-B NEUTROPENIA | |||
| GENE | SNP | VARIANT | ODDS RATIO |
| C8ORF34 | rs1517114 | GC | 1.50 |
| MTHFR | rs1801133 | GA | 1.02 |
| XPC | rs2228001 | GT | 4.63 |
| CDA | rs3215400 | del.del | 1.20 |
| ABCC2 | rs3740066 | TC | 1.03 |
| CYP2C19 | rs4244285 | AG | 1.15 |
| ABCB1 | rs1045642 | GG | 0.57 |
| ERCC1 | rs11615 | GG | 0.80 |
| C8ORF34 | rs1517114 | GG | 0.85 |
| ATIC | rs16853826 | GA | 0.52 |
| FCGR2A | rs1801274 | GG | 0.88 |
| MTRR | rs1801394 | GG | 0.75 |
| XRCC1 | rs25487 | TT | 0.93 |
| CDA | rs3215400 | del.C | 0.78 |
| MTR | rs3768142 | TT | 0.70 |
| FCGR3A | rs396991 | CA | 0.82 |
| CYP2B6 | rs4802101 | TT | 0.85 |
| 1-C THROMBOCYTOPENIA | |||
| GENE | SNP | VARIANT | ODDS RATIO |
| ABCB1 | rs1045642 | AG | 1.70 |
| C8ORF34 | rs1517114 | GC | 1.45 |
| MTHFR | rs1801131 | GT | 1.41 |
| MTHFR | rs1801133 | GG | 1.32 |
| MTRR | rs1801394 | AG | 1.06 |
| TNFRSF11B | rs2073618 | GG | 1.77 |
| XPC | rs2228001 | GT | 1.40 |
| CYP2B6 | rs4802101 | TC | 1.70 |
| SOD2 | rs4880 | GG | 1.73 |
| MTHFR | rs1801131 | TT | 0.79 |
| ATIC | rs16853826 | GA | 0.75 |
| ESR1 | rs2234693 | TT | 0.77 |
| CDA | rs3215400 | del.C | 0.79 |
| FCGR3A | rs396991 | CC | 0.93 |
| ATIC | rs4673993 | TT | 0.73 |
| SLC22A1 | rs683369 | CG | 0.74 |
| ABCC2 | rs8187710 | GG | 0.38 |
| 2-A GLOBAL SURVIVAL | |||
|---|---|---|---|
| GENE | SNP | VARIANT | HAZARD RATIO |
| ATIC | rs16853826 | GG | 1.22 |
| SLC19A1 | rs1051266 | TT | 1.06 |
| MTHFR | rs1801133 | GG | 3.12 |
| MTRR | rs1801394 | AG | 1.32 |
| TNFRSF11B | rs2073618 | GG | 1.84 |
| XPC | rs2228001 | GT | 1.68 |
| XPC | rs2228001 | TT | 1.10 |
| ENOSF1 | rs2612091 | CT | 1.05 |
| CYP3A4 | rs2740574 | CT | 2.92 |
| ERCC1 | rs3212986 | CC | 1.19 |
| CDA | rs3215400 | del.del | 1.90 |
| SLC01B1 | rs4149015 | GA | 3.96 |
| CYP2C19 | rs4244285 | AG | 1.09 |
| SOD2 | rs4880 | AG | 1.34 |
| SLC19A1 | rs1051266 | CT | 0.70 |
| TP53 | rs1042522 | GG | 0.09 |
| TP53 | rs1042522 | CG | 0.19 |
| ITPA | rs1127354 | CC | 0.59 |
| NQO1 | rs1800566 | GG | 0.56 |
| MTRR | rs1801394 | GG | 0.41 |
| SLC22A2 | rs316019 | CC | 0.25 |
| MTR | rs3768142 | GT | 0.95 |
| FCGR3A | rs396991 | CC | 0.48 |
| UGT1A | rs4124874 | GT | 0.77 |
| SLC01B1 | rs4149015 | GG | 0.26 |
| FOLH1 | rs61886492 | GG | 0.15 |
| 2-B EVENT-FREE SURVIVAL | |||
| GENE | SNP | VARIANT | HAZARD RATIO |
| SLC19A1 | rs1051266 | TT | 1.61 |
| UMP | rs1801019 | CG | 1.05 |
| XRCC1 | rs25487 | TT | 1.39 |
| ENOSF1 | rs2612091 | CT | 1.08 |
| SLC22A2 | rs316019 | CC | 1.16 |
| CDA | rs3215400 | del.del | 2.19 |
| CYP3A5 | rs776746 | CT | 1.28 |
| TP53 | rs1042522 | CG | 0.85 |
| SLC01B1 | rs11045879 | TT | 0.72 |
| ITPA | rs1127354 | CC | 0.67 |
| CYP3A4 | rs2740574 | TT | 0.59 |
| SLC01B1 | rs4149056 | TT | 0.87 |
| ABCC2 | rs8187710 | GG | 0.63 |
| TRANSPORT PROTEINS | |||
|---|---|---|---|
| Solute Carrier Family (SLC) | |||
| GENE | SNP | VARIANT | EFFECT |
| SLC01B1 | rs4149015 | GA-GG | OS |
| SLC19A1 | rs1051266 | TT | EFS |
| SLC22A2 | rs316019 | CC | OS |
| ATP-binding cassette family (ABC) | |||
| GENE | SNP | VARIANT | EFFECT |
| ABCB1 | rs1045642 | AG, GG | Tbp, Np |
| ABCC2 | rs8187710 | GG | Tbp, EFS |
| METABOLIC ENZYMES | |||
| Phase I | |||
| GENE | SNP | VARIANT | EFFECT |
| CYP2B6 | rs4802101 | TC | Tbp |
| CYP3A4 | rs2740574 | TT, CT | EFS, OS |
| FOLH1 | rs61886492 | GG | OS |
| NQO1 | rs1800566 | GG | OS |
| SOD2 | rs4880 | GG | Tbp |
| CDA | rs3215400 | del.del | EFS, OS |
| ITPA | rs1127354 | CC | OS |
| Phase II | |||
| MTHFR | rs1801131 | GT | An |
| rs1801133 | GG | OS | |
| MTRR | rs1801394 | GG-AG | OS |
| ATIC | rs16853826 | GA | Np |
| DNA REPAIR GENE/TUMOR SUPPRESSOR GENE | |||
| GENE | SNP | VARIANT | EFFECT |
| TP53 | rs1042522 | CG-GG | OS |
| XPC | rs2228001 | GT | Np, OS |
| C8ORF34 | rs1517114 | GC | Np |
| GENES WITH OTHER FUNCTIONS | |||
| GENE | SNP | VARIANT | EFFECT |
| TNFRSF11B | rs2073618 | GG | Tbp, OS |
| FCGR3A | rs396991 | CC | OS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urtasun, A.; Olivera, G.G.; Sendra, L.; Aliño, S.F.; Berlanga, P.; Gargallo, P.; Hervás, D.; Balaguer, J.; Juan-Ribelles, A.; Andrés, M.d.M.; et al. Personalized Medicine in Infant Population with Cancer: Pharmacogenetic Pilot Study of Polymorphisms Related to Toxicity and Response to Chemotherapy. Cancers 2023, 15, 1424. https://doi.org/10.3390/cancers15051424
Urtasun A, Olivera GG, Sendra L, Aliño SF, Berlanga P, Gargallo P, Hervás D, Balaguer J, Juan-Ribelles A, Andrés MdM, et al. Personalized Medicine in Infant Population with Cancer: Pharmacogenetic Pilot Study of Polymorphisms Related to Toxicity and Response to Chemotherapy. Cancers. 2023; 15(5):1424. https://doi.org/10.3390/cancers15051424
Chicago/Turabian StyleUrtasun, Andrea, Gladys G. Olivera, Luis Sendra, Salvador F. Aliño, Pablo Berlanga, Pablo Gargallo, David Hervás, Julia Balaguer, Antonio Juan-Ribelles, María del Mar Andrés, and et al. 2023. "Personalized Medicine in Infant Population with Cancer: Pharmacogenetic Pilot Study of Polymorphisms Related to Toxicity and Response to Chemotherapy" Cancers 15, no. 5: 1424. https://doi.org/10.3390/cancers15051424
APA StyleUrtasun, A., Olivera, G. G., Sendra, L., Aliño, S. F., Berlanga, P., Gargallo, P., Hervás, D., Balaguer, J., Juan-Ribelles, A., Andrés, M. d. M., Cañete, A., & Herrero, M. J. (2023). Personalized Medicine in Infant Population with Cancer: Pharmacogenetic Pilot Study of Polymorphisms Related to Toxicity and Response to Chemotherapy. Cancers, 15(5), 1424. https://doi.org/10.3390/cancers15051424