



A Machine Learning-Based Online Prediction Tool for Predicting Short-Term Postoperative Outcomes Following Spinal Tumor Resections

Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Guidelines
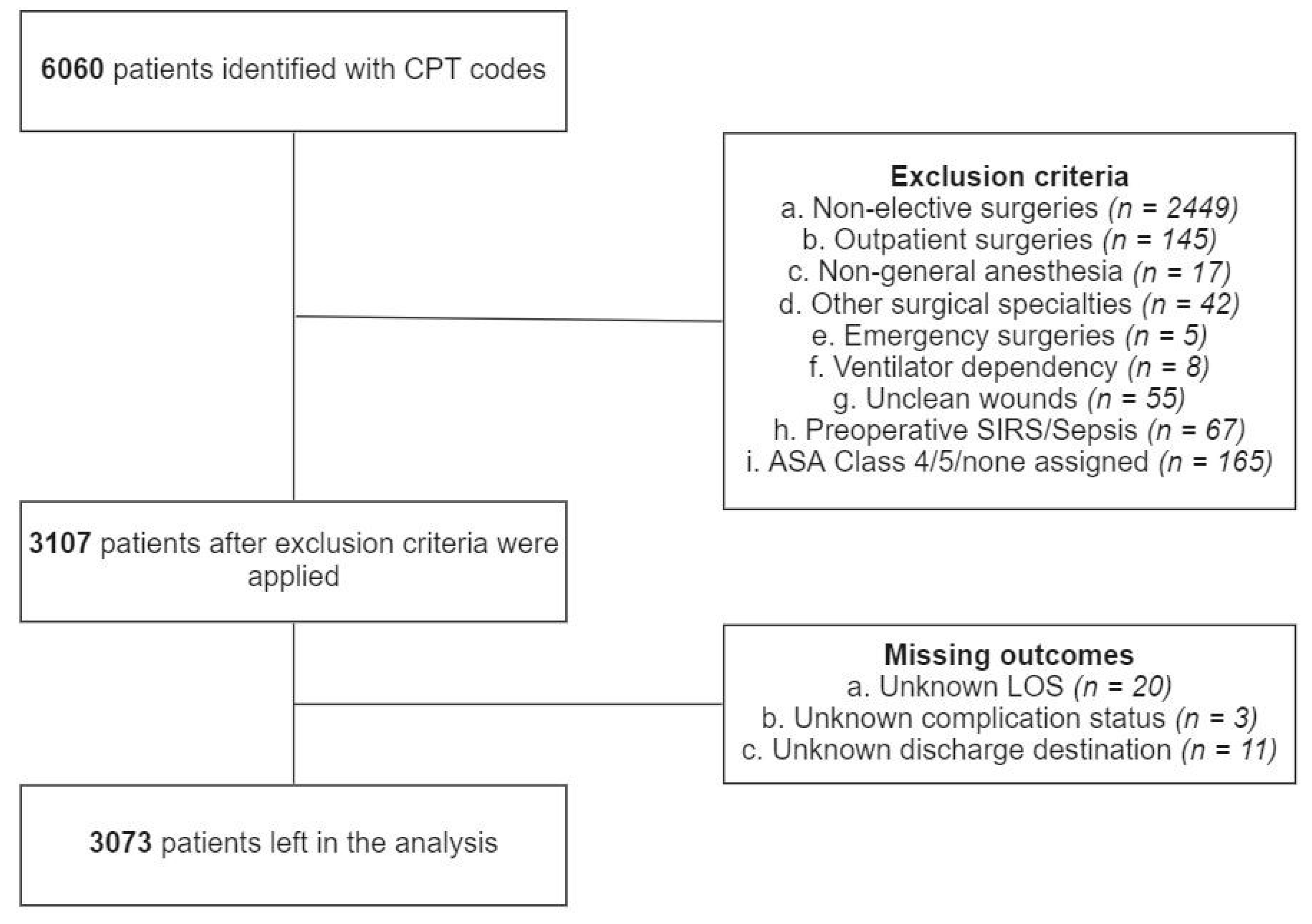
2.3. Study Population
2.4. Predictor Variables
2.5. Outcome of Interest
2.6. Data Preprocessing
2.7. Training, Validation, and Test Sets
2.8. Modeling
2.9. Performance Evaluation
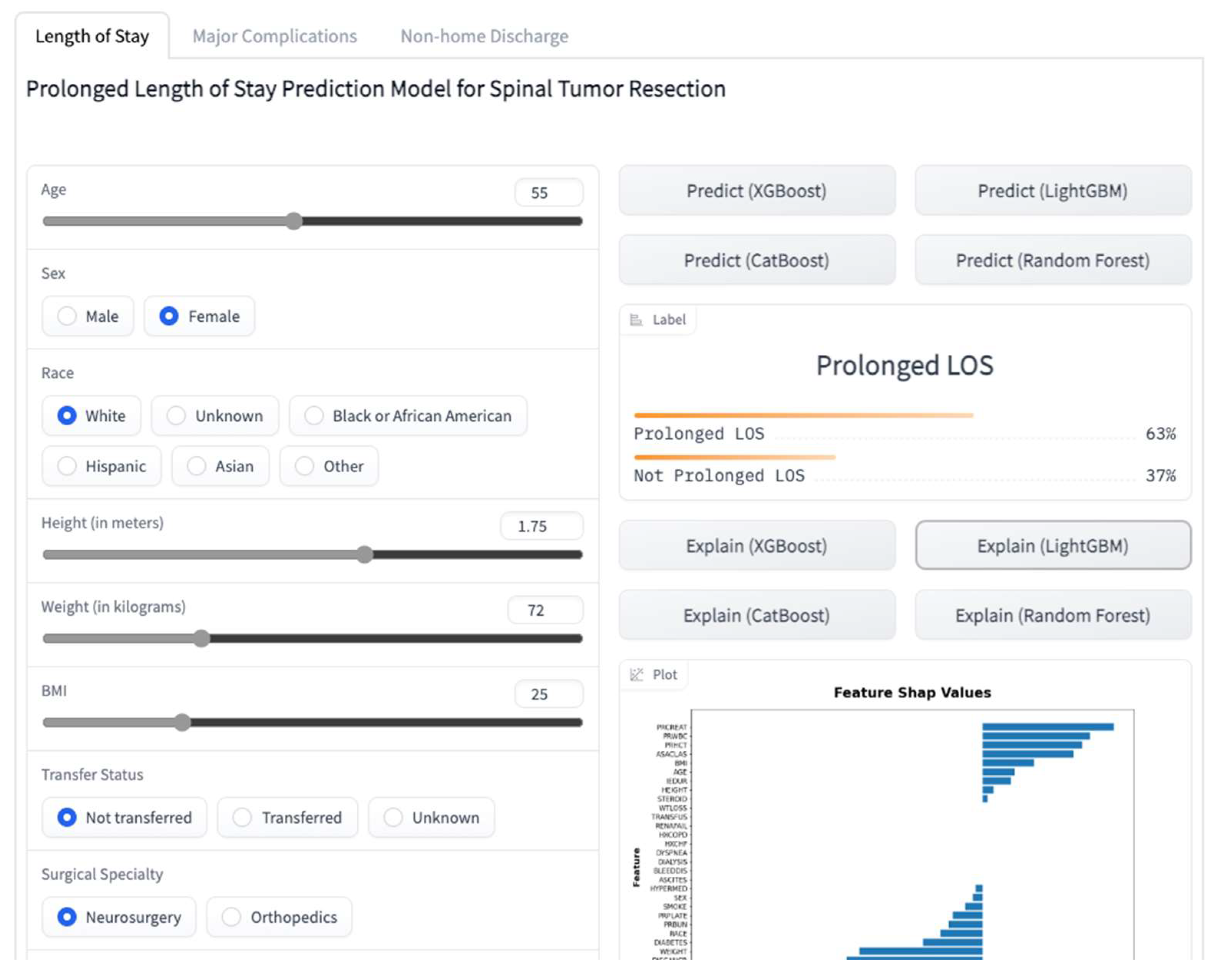
2.10. Online Prediction Tool
2.11. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Statement
Source Code
References
- Duong, L.M.; McCarthy, B.J.; McLendon, R.E.; Dolecek, T.A.; Kruchko, C.; Douglas, L.L.; Ajani, U.A. Descriptive Epidemiology of Malignant and Nonmalignant Primary Spinal Cord, Spinal Meninges, and Cauda Equina Tumors, United States, 2004–2007. Cancer 2012, 118, 4220–4227. [Google Scholar] [CrossRef] [PubMed]
- Sharma, M.; Sonig, A.; Ambekar, S.; Nanda, A. Discharge Dispositions, Complications, and Costs of Hospitalization in Spinal Cord Tumor Surgery: Analysis of Data from the United States Nationwide Inpatient Sample, 2003–2010. J. Neurosurg. Spine 2014, 20, 125–141. [Google Scholar] [CrossRef] [PubMed]
- Kaloostian, P.E.; Zadnik, P.L.; Etame, A.B.; Vrionis, F.D.; Gokaslan, Z.L.; Sciubba, D.M. Surgical Management of Primary and Metastatic Spinal Tumors. Cancer Control 2014, 21, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Schairer, W.W.; Carrer, A.; Sing, D.C.; Chou, D.; Mummaneni, P.V.; Hu, S.S.; Berven, S.H.; Burch, S.; Tay, B.; Deviren, V.; et al. Hospital Readmission Rates after Surgical Treatment of Primary and Metastatic Tumors of the Spine. Spine 2014, 39, 1801–1808. [Google Scholar] [CrossRef]
- Galgano, M.; Fridley, J.; Oyelese, A.; Telfian, A.; Kosztowski, T.; Choi, D.; Gokaslan, Z.L. Surgical Management of Spinal Metastases. Expert Rev. Anticancer. Ther. 2018, 18, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Wei, W.; Xu, F.; Wang, Y.; Liu, Y.; Fu, C. Clinical Therapy of Metastatic Spinal Tumors. Front. Surg. 2021, 8, 626873. [Google Scholar] [CrossRef] [PubMed]
- Barzilai, O.; Robin, A.M.; O’Toole, J.E.; Laufer, I. Minimally Invasive Surgery Strategies. Neurosurg. Clin. North Am. 2020, 31, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Camino Willhuber, G.; Elizondo, C.; Slullitel, P. Analysis of Postoperative Complications in Spinal Surgery, Hospital Length of Stay, and Unplanned Readmission: Application of Dindo-Clavien Classification to Spine Surgery. Glob. Spine J. 2019, 9, 279–286. [Google Scholar] [CrossRef]
- Slattery, C.; Verma, K. Outcome Measures in Adult Spine Surgery: How Do We Identify the Outcomes of Greatest Utility for Research? Clin. Spine Surg. A Spine Publ. 2019, 32, 164–165. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Patel, R.S.; Wang, S.S.Y.; Tan, J.Y.H.; Singla, A.; Chen, Z.; Ravikumar, N.; Tan, A.; Kumar, N.; Hey, D.H.W.; et al. Factors Influencing Extended Hospital Stay in Patients Undergoing Metastatic Spine Tumour Surgery and Its Impact on Survival. J. Clin. Neurosci. 2018, 56, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Pennington, Z.; Sundar, S.J.; Lubelski, D.; Alvin, M.D.; Benzel, E.C.; Mroz, T.E. Cost and Quality of Life Outcome Analysis of Postoperative Infections after Posterior Lumbar Decompression and Fusion. J. Clin. Neurosci. 2019, 68, 105–110. [Google Scholar] [CrossRef]
- Zhou, R.P.; Mummaneni, P.V.; Chen, K.-Y.; Lau, D.; Cao, K.; Amara, D.; Zhang, C.; Dhall, S.; Chou, D. Outcomes of Posterior Thoracic Corpectomies for Metastatic Spine Tumors: An Analysis of 90 Patients. World Neurosurg. 2019, 123, e371–e378. [Google Scholar] [CrossRef] [PubMed]
- Ahn, A.; Phan, K.; Cheung, Z.B.; White, S.J.W.; Kim, J.S.; Cho, S.K.-W. Predictors of Discharge Disposition Following Laminectomy for Intradural Extramedullary Spinal Tumors. World Neurosurg. 2019, 123, e427–e432. [Google Scholar] [CrossRef]
- Kim, J.S.; Merrill, R.K.; Arvind, V.; Kaji, D.; Pasik, S.D.; Nwachukwu, C.C.; Vargas, L.; Osman, N.S.; Oermann, E.K.; Caridi, J.M.; et al. Examining the Ability of Artificial Neural Networks Machine Learning Models to Accurately Predict Complications Following Posterior Lumbar Spine Fusion. Spine 2018, 43, 853–860. [Google Scholar] [CrossRef]
- Cruz, J.A.; Wishart, D.S. Applications of Machine Learning in Cancer Prediction and Prognosis. Cancer Inf. 2007, 2, 59–77. [Google Scholar] [CrossRef]
- Kuhle, S.; Maguire, B.; Zhang, H.; Hamilton, D.; Allen, A.C.; Joseph, K.S.; Allen, V.M. Comparison of Logistic Regression with Machine Learning Methods for the Prediction of Fetal Growth Abnormalities: A Retrospective Cohort Study. BMC Pregnancy Childbirth 2018, 18, 333. [Google Scholar] [CrossRef] [PubMed]
- Oermann, E.K.; Rubinsteyn, A.; Ding, D.; Mascitelli, J.; Starke, R.M.; Bederson, J.B.; Kano, H.; Lunsford, L.D.; Sheehan, J.P.; Hammerbacher, J.; et al. Using a Machine Learning Approach to Predict Outcomes after Radiosurgery for Cerebral Arteriovenous Malformations. Sci. Rep. 2016, 6, 21161. [Google Scholar] [CrossRef]
- Lee, S.-I.; Celik, S.; Logsdon, B.A.; Lundberg, S.M.; Martins, T.J.; Oehler, V.G.; Estey, E.H.; Miller, C.P.; Chien, S.; Dai, J.; et al. A Machine Learning Approach to Integrate Big Data for Precision Medicine in Acute Myeloid Leukemia. Nat. Commun. 2018, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Khuri, S.F.; Henderson, W.G.; Daley, J.; Jonasson, O.; Jones, S.R.; Campbell, D.A.J.; Fink, A.S.; Mentzer, R.M.J.; Steeger, J.E.; Study, P.S.I. of the P.S. in S. The Patient Safety in Surgery Study: Background, Study Design, and Patient Populations. J. Am. Coll. Surg. 2007, 204, 1089–1102. [Google Scholar] [CrossRef]
- Hall, B.L.; Hamilton, B.H.; Richards, K.; Bilimoria, K.Y.; Cohen, M.E.; Ko, C.Y. Does Surgical Quality Improve in the American College of Surgeons National Surgical Quality Improvement Program: An Evaluation of All Participating Hospitals. Ann. Surg. 2009, 250, 363–376. [Google Scholar] [CrossRef]
- Ingraham, A.M.; Richards, K.E.; Hall, B.L.; Ko, C.Y. Quality Improvement in Surgery: The American College of Surgeons National Surgical Quality Improvement Program Approach. Adv. Surg. 2010, 44, 251–267. [Google Scholar] [CrossRef] [PubMed]
- Ingraham, A.M.; Cohen, M.E.; Bilimoria, K.Y.; Dimick, J.B.; Richards, K.E.; Raval, M.V.; Fleisher, L.A.; Hall, B.L.; Ko, C.Y. Association of Surgical Care Improvement Project Infection-Related Process Measure Compliance with Risk-Adjusted Outcomes: Implications for Quality Measurement. J. Am. Coll. Surg. 2010, 211, 705–714. [Google Scholar] [CrossRef] [PubMed]
- About ACS NSQIP. Available online: https://www.facs.org/quality-programs/data-and-registries/acs-nsqip/about-acs-nsqip/ (accessed on 29 September 2022).
- Collins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a Multivariable Prediction Model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD Statement. BMC Med. 2015, 13, 1. [Google Scholar] [CrossRef]
- Luo, W.; Phung, D.; Tran, T.; Gupta, S.; Rana, S.; Karmakar, C.; Shilton, A.; Yearwood, J.; Dimitrova, N.; Ho, T.B.; et al. Guidelines for Developing and Reporting Machine Learning Predictive Models in Biomedical Research: A Multidisciplinary View. J. Med. Internet Res. 2016, 18, e323. [Google Scholar] [CrossRef]
- Bovonratwet, P.; Ondeck, N.T.; Nelson, S.J.; Cui, J.J.; Webb, M.L.; Grauer, J.N. Comparison of Outpatient vs Inpatient Total Knee Arthroplasty: An ACS-NSQIP Analysis. J. Arthroplast. 2017, 32, 1773–1778. [Google Scholar] [CrossRef]
- Basques, B.A.; Ibe, I.; Samuel, A.M.; Lukasiewicz, A.M.; Webb, M.L.; Bohl, D.D.; Grauer, J.N. Predicting Postoperative Morbidity and Readmission for Revision Posterior Lumbar Fusion. Clin. Spine Surg. 2017, 30, E770. [Google Scholar] [CrossRef]
- Sood, A.; Abdollah, F.; Sammon, J.D.; Kapoor, V.; Rogers, C.G.; Jeong, W.; Klett, D.E.; Hanske, J.; Meyer, C.P.; Peabody, J.O.; et al. An Evaluation of the Timing of Surgical Complications Following Nephrectomy: Data from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP). World J. Urol. 2015, 33, 2031–2038. [Google Scholar] [CrossRef] [PubMed]
- Sklearn.Impute.KNNImputer. Available online: https://scikit-learn/stable/modules/generated/sklearn.impute.KNNImputer.html (accessed on 29 September 2022).
- Beretta, L.; Santaniello, A. Nearest Neighbor Imputation Algorithms: A Critical Evaluation. BMC Med. Inform. Decis. Mak. 2016, 16, 74. [Google Scholar] [CrossRef]
- Sklearn.Preprocessing.RobustScaler. Available online: https://scikit-learn/stable/modules/generated/sklearn.preprocessing.RobustScaler.html (accessed on 29 September 2022).
- Sklearn.Preprocessing.MinMaxScaler. Available online: https://scikit-learn/stable/modules/generated/sklearn.preprocessing.MinMaxScaler.html (accessed on 29 September 2022).
- Sklearn.Preprocessing.OrdinalEncoder. Available online: https://scikit-learn/stable/modules/generated/sklearn.preprocessing.OrdinalEncoder.html (accessed on 29 September 2022).
- ADASYN—Version 0.9.1. Available online: https://imbalanced-learn.org/stable/references/generated/imblearn.over_sampling.ADASYN.html (accessed on 29 September 2022).
- He, H.; Bai, Y.; Garcia, E.A.; Li, S. ADASYN: Adaptive Synthetic Sampling Approach for Imbalanced Learning. In Proceedings of the 2008 IEEE International Joint Conference on Neural Networks (IEEE World Congress on Computational Intelligence), Hong Kong, China, 1–6 June 2008; pp. 1322–1328. [Google Scholar]
- Hanley, J.A.; McNeil, B.J. The Meaning and Use of the Area under a Receiver Operating Characteristic (ROC) Curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef]
- Saito, T.; Rehmsmeier, M. The Precision-Recall Plot Is More Informative than the ROC Plot When Evaluating Binary Classifiers on Imbalanced Datasets. PLoS ONE 2015, 10, e0118432. [Google Scholar] [CrossRef]
- Galbusera, F.; Casaroli, G.; Bassani, T. Artificial Intelligence and Machine Learning in Spine Research. JOR Spine 2019, 2, e1044. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Yang, X.; Wang, H.; Gu, Y.; Feng, J.; Qin, X.; Feng, C.; Li, Y.; Liu, L.; Fan, G.; et al. Development and Validation of a Personalized Prognostic Prediction Model for Patients with Spinal Cord Astrocytoma. Front. Med. 2022, 8, 802471. [Google Scholar] [CrossRef]
- Karhade, A.V.; Thio, Q.C.B.S.; Ogink, P.T.; Shah, A.A.; Bono, C.M.; Oh, K.S.; Saylor, P.J.; Schoenfeld, A.J.; Shin, J.H.; Harris, M.B.; et al. Development of Machine Learning Algorithms for Prediction of 30-Day Mortality After Surgery for Spinal Metastasis. Neurosurgery 2019, 85, E83–E91. [Google Scholar] [CrossRef] [PubMed]
- Massaad, E.; Williams, N.; Hadzipasic, M.; Patel, S.S.; Fourman, M.S.; Kiapour, A.; Schoenfeld, A.J.; Shankar, G.M.; Shin, J.H. Performance Assessment of the Metastatic Spinal Tumor Frailty Index Using Machine Learning Algorithms: Limitations and Future Directions. Neurosurg. Focus 2021, 50, E5. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.C.; Ho, A.L.; Feng, A.Y.; Medress, Z.A.; Pendharkar, A.V.; Rezaii, P.; Ratliff, J.K.; Desai, A.M. Prediction of Discharge Status and Readmissions after Resection of Intradural Spinal Tumors. Neurospine 2022, 19, 133–145. [Google Scholar] [CrossRef]
- Zhong, H.; Poeran, J.; Gu, A.; Wilson, L.A.; Gonzalez Della Valle, A.; Memtsoudis, S.G.; Liu, J. Machine Learning Approaches in Predicting Ambulatory Same Day Discharge Patients after Total Hip Arthroplasty. Reg. Anesth. Pain Med. 2021, 46, 779–783. [Google Scholar] [CrossRef]
- Lopez, C.D.; Gazgalis, A.; Peterson, J.R.; Confino, J.E.; Levine, W.N.; Popkin, C.A.; Lynch, T.S. Machine Learning Can Accurately Predict Overnight Stay, Readmission, and 30-Day Complications Following Anterior Cruciate Ligament Reconstruction. Arthroscopy 2022, in press. [Google Scholar] [CrossRef]
- Harris, A.H.S.; Trickey, A.W.; Eddington, H.S.; Seib, C.D.; Kamal, R.N.; Kuo, A.C.; Ding, Q.; Giori, N.J. A Tool to Estimate Risk of 30-Day Mortality and Complications After Hip Fracture Surgery: Accurate Enough for Some but Not All Purposes? A Study From the ACS-NSQIP Database. Clin. Orthop. Relat. Res. 2022, 480, 2335–2346. [Google Scholar] [CrossRef]
- Kalagara, S.; Eltorai, A.E.M.; Durand, W.M.; DePasse, J.M.; Daniels, A.H. Machine Learning Modeling for Predicting Hospital Readmission Following Lumbar Laminectomy. J. Neurosurg. Spine 2019, 30, 344–352. [Google Scholar] [CrossRef]
- Rolston, J.D.; Han, S.J.; Chang, E.F. Systemic Inaccuracies in the National Surgical Quality Improvement Program Database: Implications for Accuracy and Validity for Neurosurgery Outcomes Research. J. Clin. Neurosci. 2017, 37, 44–47. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
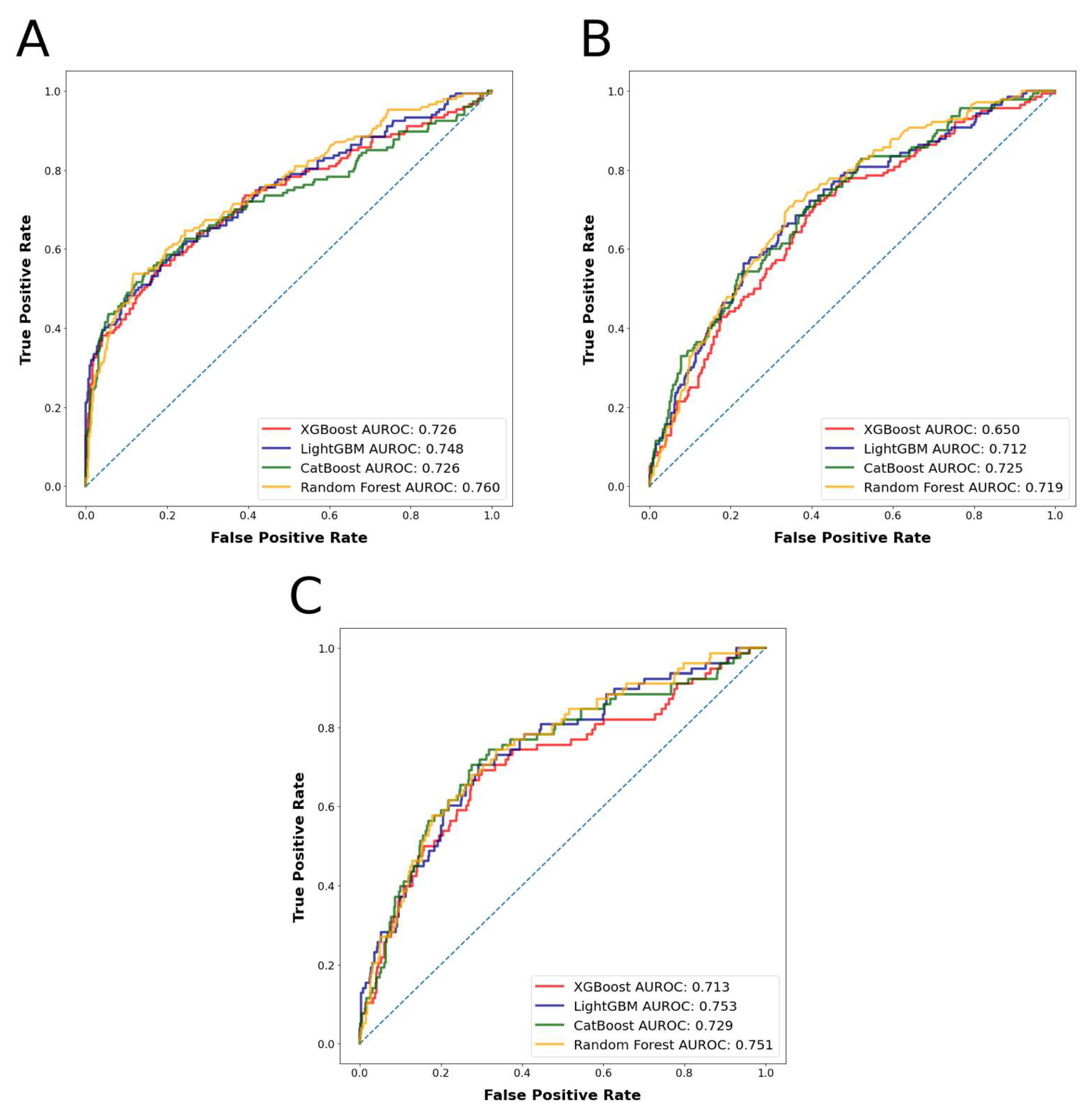
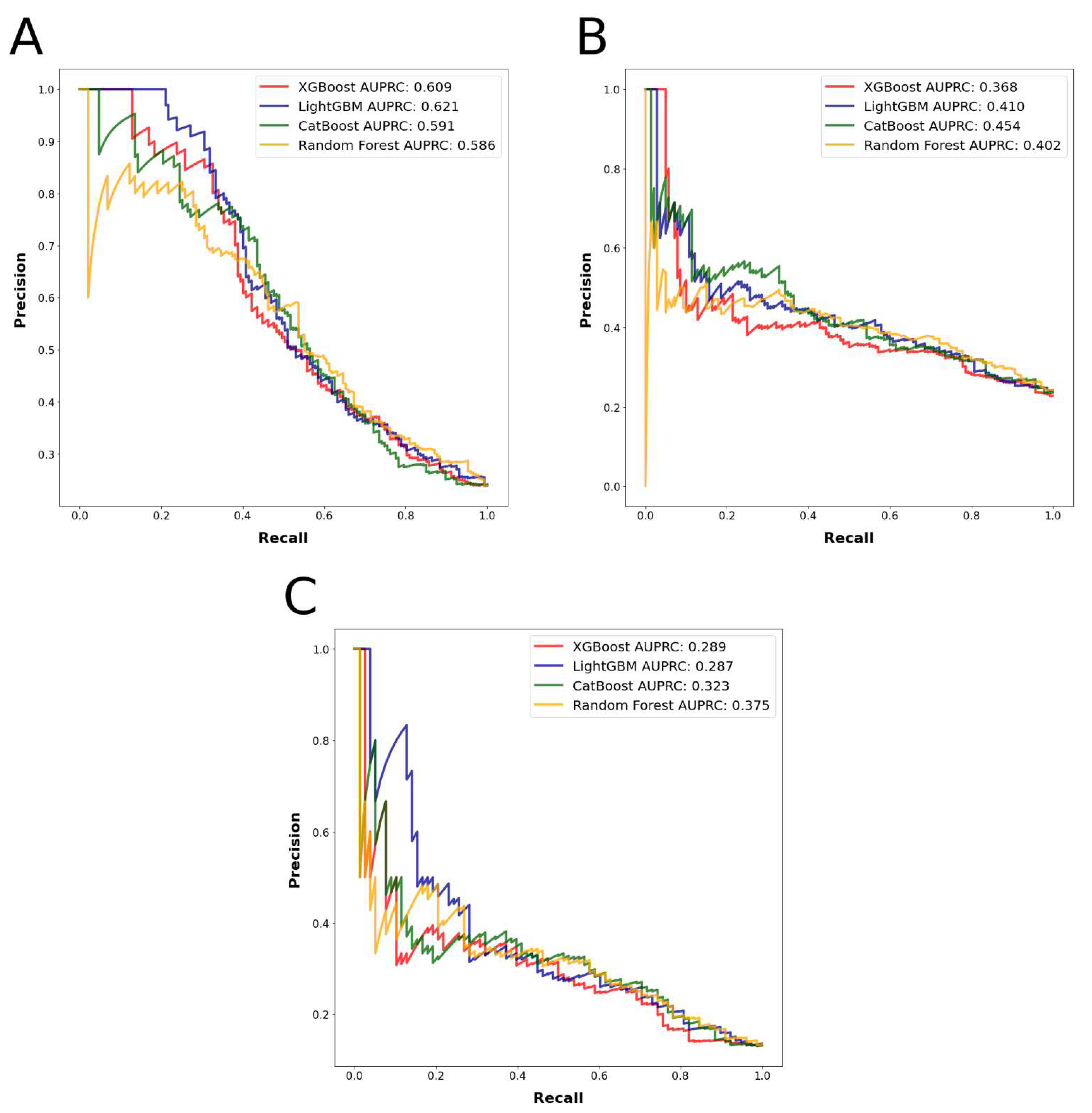
| Outcome | Algorithm | P | R | F1 | MCC | AUPRC | ACC | AUROC |
|---|---|---|---|---|---|---|---|---|
| LOS | XGB | 0.503 | 0.565 | 0.532 | 0.398 | 0.609 | 0.789 | 0.744 |
| LGB | 0.449 | 0.641 | 0.528 | 0.423 | 0.621 | 0.808 | 0.748 | |
| CB | 0.469 | 0.645 | 0.543 | 0.437 | 0.591 | 0.811 | 0.726 | |
| RF | 0.490 | 0.621 | 0.548 | 0.431 | 0.586 | 0.807 | 0.760 | |
| Mean | 0.478 | 0.618 | 0.538 | 0.422 | 0.602 | 0.804 | 0.745 | |
| NHD | XGB | 0.307 | 0.381 | 0.340 | 0.173 | 0.368 | 0.728 | 0.650 |
| LGB | 0.343 | 0.475 | 0.398 | 0.262 | 0.410 | 0.764 | 0.712 | |
| CB | 0.436 | 0.477 | 0.455 | 0.304 | 0.454 | 0.763 | 0.725 | |
| RF | 0.414 | 0.436 | 0.425 | 0.261 | 0.402 | 0.745 | 0.719 | |
| Mean | 0.375 | 0.442 | 0.405 | 0.250 | 0.408 | 0.750 | 0.701 | |
| MC | XGB | 0.192 | 0.405 | 0.261 | 0.212 | 0.293 | 0.862 | 0.718 |
| LGB | 0.192 | 0.375 | 0.254 | 0.197 | 0.305 | 0.857 | 0.726 | |
| CB | 0.244 | 0.373 | 0.295 | 0.222 | 0.321 | 0.852 | 0.728 | |
| RF | 0.256 | 0.377 | 0.305 | 0.231 | 0.318 | 0.852 | 0.749 | |
| Mean | 0.221 | 0.383 | 0.279 | 0.216 | 0.309 | 0.856 | 0.730 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karabacak, M.; Margetis, K. A Machine Learning-Based Online Prediction Tool for Predicting Short-Term Postoperative Outcomes Following Spinal Tumor Resections. Cancers 2023, 15, 812. https://doi.org/10.3390/cancers15030812
Karabacak M, Margetis K. A Machine Learning-Based Online Prediction Tool for Predicting Short-Term Postoperative Outcomes Following Spinal Tumor Resections. Cancers. 2023; 15(3):812. https://doi.org/10.3390/cancers15030812
Chicago/Turabian StyleKarabacak, Mert, and Konstantinos Margetis. 2023. "A Machine Learning-Based Online Prediction Tool for Predicting Short-Term Postoperative Outcomes Following Spinal Tumor Resections" Cancers 15, no. 3: 812. https://doi.org/10.3390/cancers15030812
APA StyleKarabacak, M., & Margetis, K. (2023). A Machine Learning-Based Online Prediction Tool for Predicting Short-Term Postoperative Outcomes Following Spinal Tumor Resections. Cancers, 15(3), 812. https://doi.org/10.3390/cancers15030812