
The Evolving Landscape of Leptomeningeal Cancer from Solid Tumors: A Systematic Review of Clinical Trials

 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
3. Results
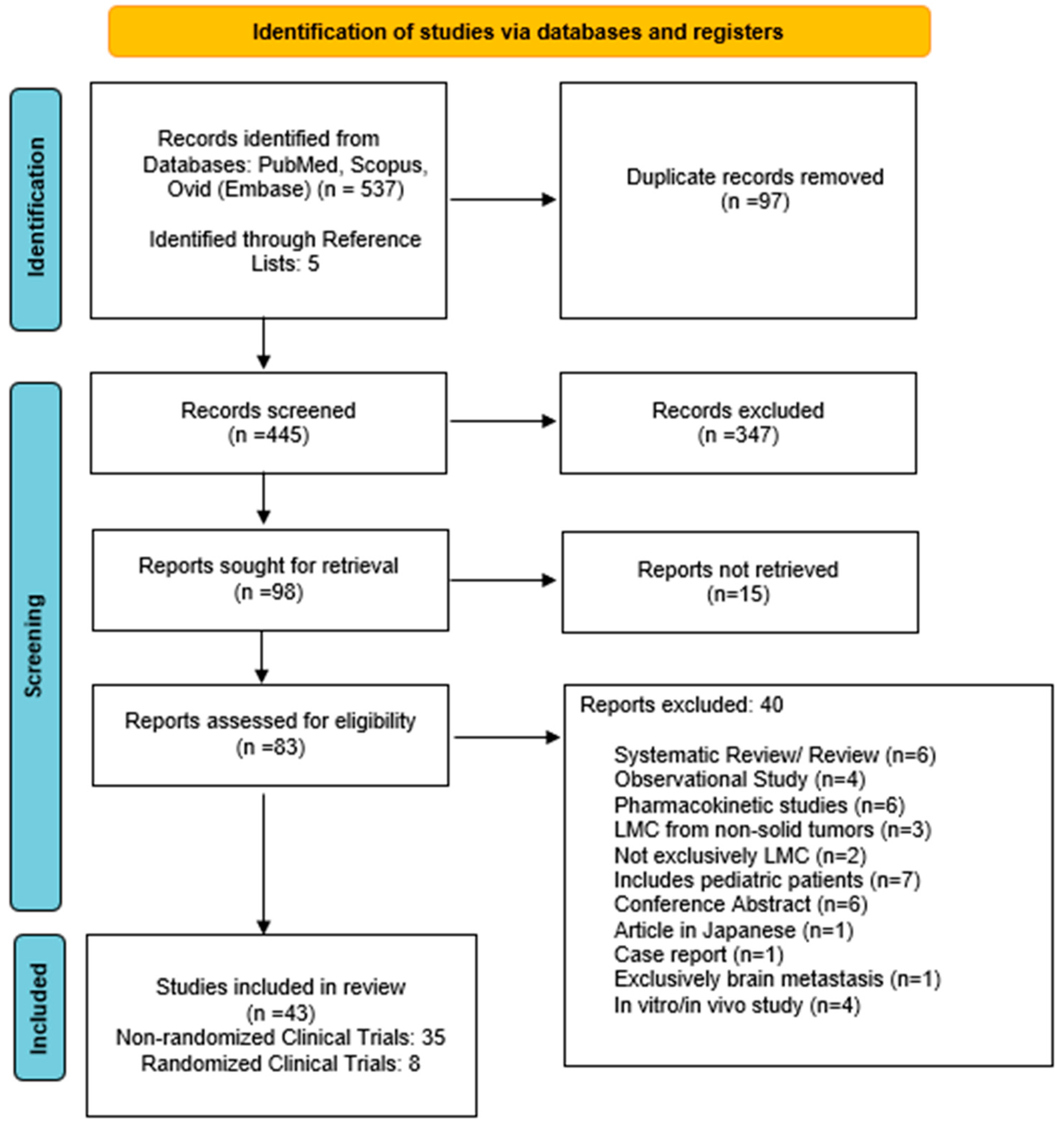
3.1. Literature Search
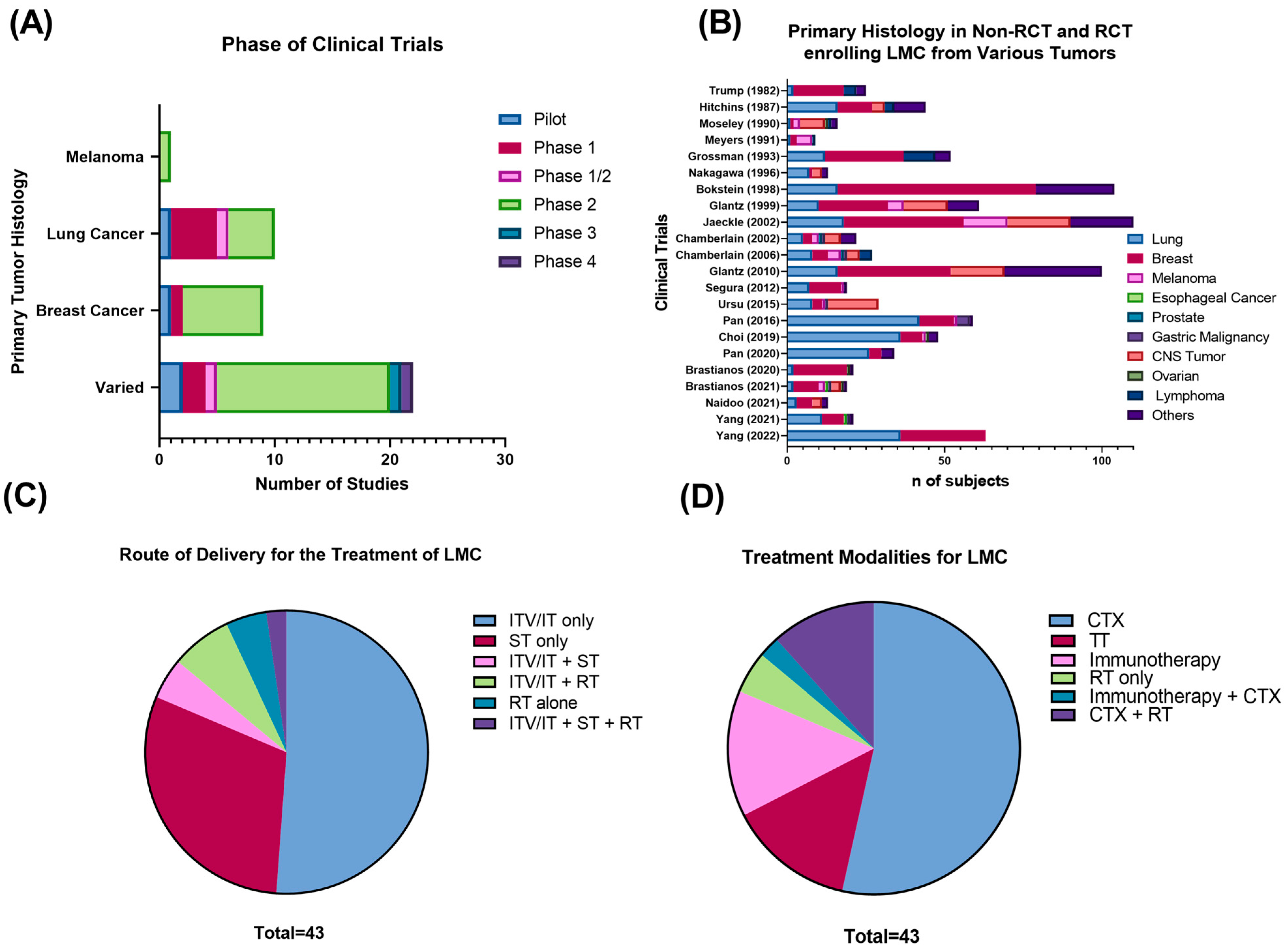
3.2. Clinical Trials
3.3. Cytotoxic Chemotherapy
3.3.1. Non-Randomized Clinical Trials
3.3.2. Randomized Clinical Trials (RCTs)

{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Primary Tumor | Phase | Treatment | (n) | Age (Years) | Median KPS/ECOG | BM (n) | mPFS (Months) | mOS (Months) | Response Criteria | Response Rate |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Le Rhun (2019) [49] | Breast | 2 | Systemic treatment alone | 37 | 47.5 | 80 | 15 | 2 | 4 | Neurological clinical evaluation, MRI, CSF negative conversion | Clinical improvement (1), MRI response (3), complete CSF response (5) |
| Systemic treatment + IT liposomal cytarabine | 36 | 50.9 | 80 | 8 | 2.4 | 7.3 | Clinical improvement (6), MRI response (7), complete CSF response (10) | ||||
| Boogerd (2004) [50] | Breast | 2 | ITV MTX + systemic chemotherapy and IFRT | 17 | NA | 64 | 2 | 5.2 | 4.2 | Neurological clinical evaluation | Improvement (7), stable (3), no response (7) |
| Systemic chemotherapy and IFRT | 18 | NA | 71 | 1 | 5.5 | 6.9 | Improvement (7), stable (5), no response (6) | ||||
| Yang (2022) [51] | Varied | 2 | pCSI | 42 | 57 | 80 | 28 | 7.5 | 9.9 | Neurological clinical evaluation, imaging (stable) | RR: 30/42 (71.4%) |
| IFRT | 21 | 61 | 80 | 15 | 2.3 | 6 | RR: 5/21 (23.8%) | ||||
| Cole (2003) [45] | Varied | 2 | ITV MTX | 30 | 49 | NA | NA | 1 | 2.56 | Quality-adjusted survival without symptoms or toxicity (Q-Twist) in days | 70 days |
| ITV DepoCyt | 31 | 49 | NA | NA | 1.9 | 3.45 | 131 days | ||||
| Glantz (2010) [46] | Varied | 4 | ITV MTX | 48 | NA | NA | 20 | 1.23 | NA | Doubling of PFS between groups | - |
| ITV DepoCyt | 52 | NA | NA | 23 | 1.15 | NA | - | ||||
| Glantz (1999) [44] | Varied | 2 | IT MTX | 30 | 49 | 70 | NA | 0.986 | 2.6 | Clinical response, negative conversion of CSF cytology | RR: 20% |
| IT DepoCyt | 31 | 49 | 60 | NA | 1.9 | 3.5 | RR: 26% | ||||
| Grossman (1993) [48] | Varied | 2 | ITV MTX | 28 | NA | 2 | NA | NA | 3.6 | Clinical response, negative conversion of CSF cytology, neuroimaging (CT and myelography) | Complete RR: 21% |
| ITV thiotepa | 24 | NA | 2 | NA | NA | 3.24 | Complete RR: 4% | ||||
| Hitchins (1987) [47] | Varied | 2 | IT MTX | 22 | 55 | NA | 6 | NA | 2.7 | Clinical response, negative conversion of CSF cytology, neuroimaging (CT and myelography), | RR: 61% |
| IT MTX + Ara-C | 20 | 55 | NA | NA | 1.6 | RR: 45% |
3.3.3. Impact of the Route and Rate of Intra-CSF Administration in Leptomeningeal Cancer
3.3.4. ITV vs. Systemic Chemotherapy and the Utility of Combination Chemotherapy
3.4. Targeted Therapy
3.4.1. NSCLC: EGFR TKI Inhibitors
3.4.2. Breast Cancer: HER2 Targeted Therapy
3.5. Immunotherapy
3.5.1. Immune-Checkpoint Inhibitors Nivolumab, Ipilimumab, and Pembrolizumab
3.5.2. Anti-VEGF Immunotherapy
3.5.3. Other Types of Immunotherapies
3.6. Radiotherapy
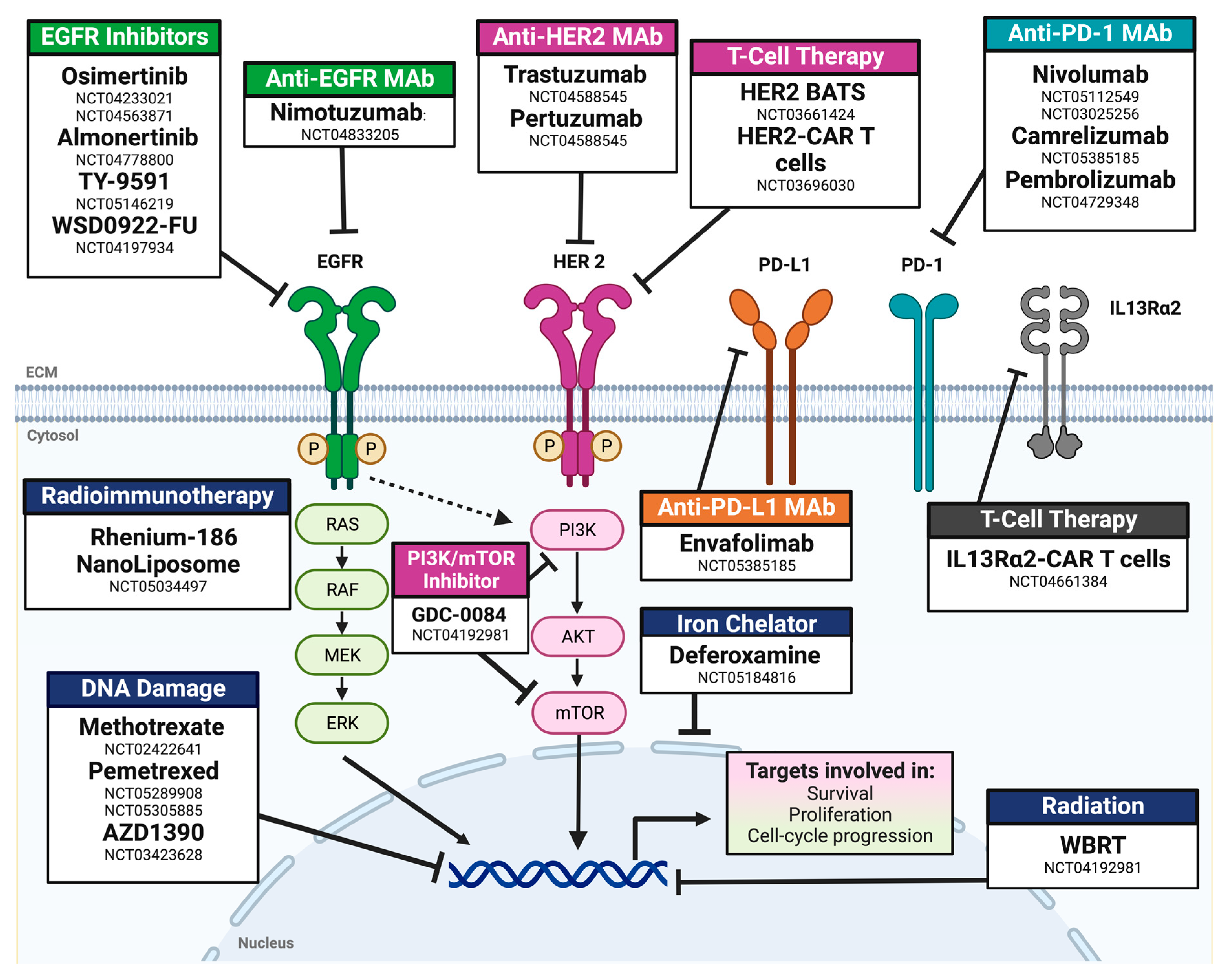
3.7. Review of Actively Enrolling Clinical Trials
4. Discussion
Current Limitations for Conducting Clinical Trials in Leptomeningeal Cancer and Future Perspectives
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wang, N.; Bertalan, M.S.; Brastianos, P.K. Leptomeningeal metastasis from systemic cancer: Review and update on management. Cancer 2018, 124, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Le Rhun, E.; Weller, M.; Brandsma, D.; Van den Bent, M.; de Azambuja, E.; Henriksson, R.; Boulanger, T.; Peters, S.; Watts, C.; Wick, W.; et al. EANO-ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up of patients with leptomeningeal metastasis from solid tumours. Ann. Oncol. 2017, 28, iv84–iv99. [Google Scholar] [CrossRef]
- Nayar, G.; Ejikeme, T.; Chongsathidkiet, P.; Elsamadicy, A.A.; Blackwell, K.L.; Clarke, J.M.; Lad, S.P.; Fecci, P.E. Leptomeningeal disease: Current diagnostic and therapeutic strategies. Oncotarget 2017, 8, 73312–73328. [Google Scholar] [CrossRef] [PubMed]
- Sener, U.; Kumthekar, P.; Boire, A. Advances in the diagnosis, evaluation, and management of leptomeningeal disease. Neurooncol. Adv. 2021, 3, v86–v95. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, J.P.; Kumthekar, P.; Dixit, K.S.; Stupp, R.; Lukas, R.V. Leptomeningeal metastasis from solid tumors. J. Neurol. Sci. 2020, 411, 116706. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- U.S. Department of Human Health Services. Common Terminology Criteria for Adverse Events (CTCAE) v4.0. Available online: http://www.eortc.be/services/doc/ctc/ctcae_4.03_2010-06-14_quickreference_5x7.pdf (accessed on 23 July 2022).
- Chamberlain, M.; Kormanik, P. Leptomeningeal metastases due to melanoma. Int. J. Oncol. 1996, 9, 505–510. [Google Scholar] [CrossRef]
- Kumthekar, P.; Tang, S.C.; Brenner, A.J.; Kesari, S.; Piccioni, D.E.; Anders, C.; Carrillo, J.; Chalasani, P.; Kabos, P.; Puhalla, S.; et al. ANG1005, a Brain-Penetrating Peptide-Drug Conjugate, Shows Activity in Patients with Breast Cancer with Leptomeningeal Carcinomatosis and Recurrent Brain Metastases. Clin. Cancer Res. 2020, 26, 2789–2799. [Google Scholar] [CrossRef]
- Melisko, M.E.; Assefa, M.; Hwang, J.; DeLuca, A.; Park, J.W.; Rugo, H.S. Phase II study of irinotecan and temozolomide in breast cancer patients with progressing central nervous system disease. Breast Cancer Res. Treat. 2019, 177, 401–408. [Google Scholar] [CrossRef]
- Mrugala, M.M.; Kim, B.; Sharma, A.; Johnson, N.; Graham, C.; Kurland, B.F.; Gralow, J. Phase II Study of Systemic High-dose Methotrexate and Intrathecal Liposomal Cytarabine for Treatment of Leptomeningeal Carcinomatosis From Breast Cancer. Clin. Breast Cancer 2019, 19, 311–316. [Google Scholar] [CrossRef]
- Bonneau, C.; Paintaud, G.; Trédan, O.; Dubot, C.; Desvignes, C.; Dieras, V.; Taillibert, S.; Tresca, P.; Turbiez, I.; Li, J.; et al. Phase I feasibility study for intrathecal administration of trastuzumab in patients with HER2 positive breast carcinomatous meningitis. Eur. J. Cancer. 2018, 95, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.F.; Lin, C.H.; Kuo, C.H.; Chen, W.W.; Yeh, D.C.; Liao, H.W.; Huang, S.M.; Cheng, A.L.; Lu, Y.S. A pilot study of bevacizumab combined with etoposide and cisplatin in breast cancer patients with leptomeningeal carcinomatosis. BMC Cancer 2015, 15, 299. [Google Scholar] [CrossRef] [PubMed]
- Orlando, L.; Curigliano, G.; Colleoni, M.; Fazio, N.; Nole, F.; Martinelli, G.; Cinieri, S.; Graffeo, R.; Peruzzotti, G.; Goldhirsch, A. Intrathecal chemotherapy in carcinomatous meningitis from breast cancer. Anticancer Res. 2002, 22, 3057–3059. [Google Scholar] [PubMed]
- Esteva, F.J.; Soh, L.T.; Holmes, F.A.; Plunkett, W.; Meyers, C.A.; Forman, A.D.; Hortobagyi, G.N. Phase II trial and pharmacokinetic evaluation of cytosine arabinoside for leptomeningeal metastases from breast cancer. Cancer Chemother. Pharmacol. 2000, 46, 382–386. [Google Scholar] [CrossRef]
- Lu, Z.Q.; Cai, J.; Wang, X.; Wei, J.P.; Zeng, Z.M.; Huang, L.; Liu, A.W. Osimertinib combined with bevacizumab for leptomeningeal metastasis from EGFR-mutation non-small cell lung cancer: A phase II single-arm prospective clinical trial. Thorac. Cancer 2021, 12, 172–180. [Google Scholar] [CrossRef]
- Fan, C.; Zhao, Q.; Li, L.; Shen, W.; Du, Y.; Teng, C.; Gao, F.; Song, X.; Jiang, Q.; Huang, D.; et al. Efficacy and Safety of Intrathecal Pemetrexed Combined With Dexamethasone for Treating Tyrosine Kinase Inhibitor-Failed Leptomeningeal Metastases From EGFR-Mutant NSCLC-a Prospective, Open-Label, Single-Arm Phase 1/2 Clinical Trial (Unique Identifier: ChiCTR1800016615). J. Thorac. Oncol. 2021, 16, 1359–1368. [Google Scholar] [CrossRef]
- Nosaki, K.; Yamanaka, T.; Hamada, A.; Shiraishi, Y.; Harada, T.; Himeji, D.; Kitazaki, T.; Ebi, N.; Shimose, T.; Seto, T.; et al. Erlotinib for Non-Small Cell Lung Cancer with Leptomeningeal Metastases: A Phase II Study (LOGIK1101). Oncologist 2020, 25, e1869–e1878. [Google Scholar] [CrossRef]
- Park, S.; Lee, M.H.; Seong, M.; Kim, S.T.; Kang, J.H.; Cho, B.C.; Lee, K.H.; Cho, E.K.; Sun, J.M.; Lee, S.H.; et al. A phase II, multicenter, two cohort study of 160 mg osimertinib in EGFR T790M-positive non-small-cell lung cancer patients with brain metastases or leptomeningeal disease who progressed on prior EGFR TKI therapy. Ann. Oncol. 2020, 31, 1397–1404. [Google Scholar] [CrossRef]
- Yang, J.C.H.; Kim, S.W.; Kim, D.W.; Lee, J.S.; Cho, B.C.; Ahn, J.S.; Lee, D.H.; Kim, T.M.; Goldman, J.W.; Natale, R.B.; et al. Osimertinib in Patients With Epidermal Growth Factor Receptor Mutation-Positive Non-Small-Cell Lung Cancer and Leptomeningeal Metastases: The BLOOM Study. J. Clin. Oncol. 2020, 38, 538–547. [Google Scholar] [CrossRef]
- Nanjo, S.; Hata, A.; Okuda, C.; Kaji, R.; Okada, H.; Tamura, D.; Irie, K.; Okada, H.; Fukushima, S.; Katakami, N. Standard-dose osimertinib for refractory leptomeningeal metastases in T790M-positive EGFR-mutant non-small cell lung cancer. Br. J. Cancer 2018, 118, 32–37. [Google Scholar] [CrossRef]
- Pan, Z.; Yang, G.; Cui, J.; Li, W.; Li, Y.; Gao, P.; Jiang, T.; Sun, Y.; Dong, L.; Song, Y.; et al. A Pilot Phase 1 Study of Intrathecal Pemetrexed for Refractory Leptomeningeal Metastases From Non-small-cell Lung Cancer. Front. Oncol. 2019, 9, 838. [Google Scholar] [CrossRef] [PubMed]
- Tamiya, A.; Tamiya, M.; Nishihara, T.; Shiroyama, T.; Nakao, K.; Tsuji, T.; Takeuchi, N.; Isa, S.I.; Omachi, N.; Okamoto, N.; et al. Cerebrospinal Fluid Penetration Rate and Efficacy of Afatinib in Patients with EGFR Mutation-positive Non-small Cell Lung Cancer with Leptomeningeal Carcinomatosis: A Multicenter Prospective Study. Anticancer Res. 2017, 37, 4177–4182. [Google Scholar] [CrossRef] [PubMed]
- Jackman, D.M.; Cioffredi, L.A.; Jacobs, L.; Sharmeen, F.; Morse, L.K.; Lucca, J.; Plotkin, S.R.; Marcoux, P.J.; Rabin, M.S.; Lynch, T.J.; et al. A phase I trial of high dose gefitinib for patients with leptomeningeal metastases from non-small cell lung cancer. Oncotarget 2015, 6, 4527–4536. [Google Scholar] [CrossRef]
- Chamberlain, M.C.; Kormanik, P. Carcinoma meningitis secondary to non-small cell lung cancer: Combined modality therapy. Arch Neurol. 1998, 55, 506–512. [Google Scholar] [CrossRef]
- Yang, T.J.; Wijetunga, N.A.; Yamada, J.; Wolden, S.; Mehallow, M.; Goldman, D.A.; Zhang, Z.; Young, R.J.; Kris, M.G.; Yu, H.A.; et al. Clinical trial of proton craniospinal irradiation for leptomeningeal metastases. Neuro Oncol. 2021, 23, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Naidoo, J.; Schreck, K.C.; Fu, W.; Hu, C.; Carvajal-Gonzalez, A.; Connolly, R.M.; Santa-Maria, C.A.; Lipson, E.J.; Holdhoff, M.; Forde, P.M.; et al. Pembrolizumab for patients with leptomeningeal metastasis from solid tumors: Efficacy, safety, and cerebrospinal fluid biomarkers. J. ImmunoTherapy Cancer 2021, 9, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Brastianos, P.K.; Strickland, M.R.; Lee, E.Q.; Wang, N.; Cohen, J.V.; Chukwueke, U.; Forst, D.A.; Eichler, A.; Overmoyer, B.; Lin, N.U.; et al. Phase II study of ipilimumab and nivolumab in leptomeningeal carcinomatosis. Nat. Commun. 2021, 12, 5954. [Google Scholar] [CrossRef]
- Brastianos, P.K.; Lee, E.Q.; Cohen, J.V.; Tolaney, S.M.; Lin, N.U.; Wang, N.; Chukwueke, U.; White, M.D.; Nayyar, N.; Kim, A.; et al. Single-arm, open-label phase 2 trial of pembrolizumab in patients with leptomeningeal carcinomatosis. Nat. Med. 2020, 26, 1280–1284. [Google Scholar] [CrossRef]
- Pan, Z.; Yang, G.; He, H.; Cui, J.; Li, W.; Yuan, T.; Chen, K.; Jiang, T.; Gao, P.; Sun, Y.; et al. Intrathecal pemetrexed combined with involved-field radiotherapy as a first-line intra-CSF therapy for leptomeningeal metastases from solid tumors: A phase I/II study. Ther. Adv. Med. Oncol. 2020, 12, 1758835920937953. [Google Scholar] [CrossRef]
- Choi, Y.H.; Gwak, H.S.; Joo, J.; Kwon, J.W.; Shin, S.H.; Yoo, H.; Lee, J.H.; Youn, J.H. Efficacy of Slow Rate Ventriculolumbar Perfusion Chemotherapy for Leptomeningeal Carcinomatosis: Interim Result of a Phase II Study. Brain Tumor. Res. Treat 2019, 7, 85–91. [Google Scholar] [CrossRef]
- Pan, Z.; Yang, G.; He, H.; Zhao, G.; Yuan, T.; Li, Y.; Shi, W.; Gao, P.; Dong, L.; Li, Y. Concurrent radiotherapy and intrathecal methotrexate for treating leptomeningeal metastasis from solid tumors with adverse prognostic factors: A prospective and single-arm study. Int. J. Cancer 2016, 139, 1864–1872. [Google Scholar] [CrossRef] [PubMed]
- Ursu, R.; Taillibert, S.; Banissi, C.; Vicaut, E.; Bailon, O.; Le Rhun, E.; Guillamo, J.S.; Psimaras, D.; Tibi, A.; Sacko, A.; et al. Immunotherapy with CpG-ODN in neoplastic meningitis: A phase I trial. Cancer Sci. 2015, 106, 1212–1218. [Google Scholar] [CrossRef] [PubMed]
- Segura, P.P.; Gil, M.; Balañá, C.; Chacón, I.; Langa, J.M.; Martín, M.; Bruna, J. Phase II trial of temozolomide for leptomeningeal metastases in patients with solid tumors. J. Neurooncol. 2012, 109, 137–142. [Google Scholar] [CrossRef]
- Chamberlain, M.C.; Tsao-Wei, D.D.; Groshen, S. Phase II trial of intracerebrospinal fluid etoposide in the treatment of neoplastic meningitis. Cancer 2006, 106, 2021–2027. [Google Scholar] [CrossRef]
- Chamberlain, M.C. A phase II trial of intra-cerebrospinal fluid alpha interferon in the treatment of neoplastic meningitis. Cancer 2002, 94, 2675–2680. [Google Scholar] [CrossRef]
- Jaeckle, K.A.; Batchelor, T.; O’Day, S.J.; Phuphanich, S.; New, P.; Lesser, G.; Cohn, A.; Gilbert, M.; Aiken, R.; Heros, D.; et al. An open label trial of sustained-release cytarabine (DepoCyt) for the intrathecal treatment of solid tumor neoplastic meningitis. J. Neurooncol. 2002, 57, 231–239. [Google Scholar] [CrossRef]
- Bokstein, F.; Lossos, A.; Siegal, T. Leptomeningeal metastases from solid tumors: A comparison of two prospective series treated with and without intra-cerebrospinal fluid chemotherapy. Cancer 1998, 82, 1756–1763. [Google Scholar] [CrossRef]
- Nakagawa, H.; Fujita, T.; Kubo, S.; Izumoto, S.; Nakajima, Y.; Tsuruzono, K.; Tokiyoshi, K.; Hayakawa, T. Ventriculolumbar perfusion chemotherapy with methotrexate and cytosine arabinoside for meningeal carcinomatosis: A pilot study in 13 patients. Surg. Neurol. 1996, 45, 256–264. [Google Scholar] [CrossRef]
- Meyers, C.A.; Obbens, E.A.; Scheibel, R.S.; Moser, R.P. Neurotoxicity of intraventricularly administered alpha-interferon for leptomeningeal disease. Cancer 1991, 68, 88–92. [Google Scholar] [CrossRef]
- Moseley, R.P.; Davies, A.G.; Richardson, R.B.; Zalutsky, M.; Carrell, S.; Fabre, J.; Slack, N.; Bullimore, J.; Pizer, B.; Papanastassiou, V.; et al. Intrathecal administration of 131I radiolabelled monoclonal antibody as a treatment for neoplastic meningitis. Br. J. Cancer 1990, 62, 637–642. [Google Scholar] [CrossRef]
- Trump, D.L.; Grossman, S.A.; Thompson, G.; Murray, K.; Wharam, M. Treatment of neoplastic meningitis with intraventricular thiotepa and methotrexate. Cancer Treat Rep. 1982, 66, 1549–1551. [Google Scholar] [PubMed]
- Adjei, A.A. Pharmacology and mechanism of action of pemetrexed. Clin. Lung Cancer 2004, 5 (Suppl. 2), S51–S55. [Google Scholar] [CrossRef] [PubMed]
- Glantz, M.J.; Jaeckle, K.A.; Chamberlain, M.C.; Phuphanich, S.; Recht, L.; Swinnen, L.J.; Maria, B.; LaFollette, S.; Schumann, G.B.; Cole, B.F.; et al. A randomized controlled trial comparing intrathecal sustained-release cytarabine (DepoCyt) to intrathecal methotrexate in patients with neoplastic meningitis from solid tumors. Clin. Cancer Res. 1999, 5, 3394–3402. [Google Scholar] [PubMed]
- Cole, B.F.; Glantz, M.J.; Jaeckle, K.A.; Chamberlain, M.C.; Mackowiak, J.I. Quality-of-life-adjusted survival comparison of sustained-release cytosine arabinoside versus intrathecal methotrexate for treatment of solid tumor neoplastic meningitis. Cancer 2003, 97, 3053–3060. [Google Scholar] [CrossRef]
- Glantz, M.J.; Van Horn, A.; Fisher, R.; Chamberlain, M.C. Route of intracerebrospinal fluid chemotherapy administration and efficacy of therapy in neoplastic meningitis. Cancer 2010, 116, 1947–1952. [Google Scholar] [CrossRef]
- Hitchins, R.N.; Bell, D.R.; Woods, R.L.; Levi, J.A. A prospective randomized trial of single-agent versus combination chemotherapy in meningeal carcinomatosis. J. Clin. Oncol. 1987, 5, 1655–1662. [Google Scholar] [CrossRef]
- Grossman, S.A.; Finkelstein, D.M.; Ruckdeschel, J.C.; Trump, D.L.; Moynihan, T.; Ettinger, D.S. Randomized prospective comparison of intraventricular methotrexate and thiotepa in patients with previously untreated neoplastic meningitis. Eastern Cooperative Oncology Group. J. Clin. Oncol. 1993, 11, 561–569. [Google Scholar] [CrossRef]
- Le Rhun, E.; Wallet, J.; Mailliez, A.; Le Deley, M.C.; Rodrigues, I.; Boulanger, T.; Lorgis, V.; Barrière, J.; Robin, Y.M.; Weller, M.; et al. Intrathecal liposomal cytarabine plus systemic therapy versus systemic chemotherapy alone for newly diagnosed leptomeningeal metastasis from breast cancer. Neuro Oncol. 2020, 22, 524–538. [Google Scholar] [CrossRef]
- Boogerd, W.; van den Bent, M.J.; Koehler, P.J.; Heimans, J.J.; van der Sande, J.J.; Aaronson, N.K.; Hart, A.A.; Benraadt, J.; Vecht Ch, J. The relevance of intraventricular chemotherapy for leptomeningeal metastasis in breast cancer: A randomised study. Eur. J. Cancer 2004, 40, 2726–2733. [Google Scholar] [CrossRef]
- Yang, J.T.; Wijetunga, N.A.; Pentsova, E.; Wolden, S.; Young, R.J.; Correa, D.; Zhang, Z.; Zheng, J.; Steckler, A.; Bucwinska, W.; et al. Randomized Phase II Trial of Proton Craniospinal Irradiation Versus Photon Involved-Field Radiotherapy for Patients With Solid Tumor Leptomeningeal Metastasis. J. Clin. Oncol. 2022, 40, 3858–3867. [Google Scholar] [CrossRef]
- Buszek, S.M.; Chung, C. Radiotherapy in Leptomeningeal Disease: A Systematic Review of Randomized and Non-randomized Trials. Front. Oncol. 2019, 9, 1224. [Google Scholar] [CrossRef]
- Gill, C.M.; Brastianos, P.K. Management of leptomeningeal carcinomatosis and challenges of trial design. Curr. Opin. Oncol. 2019, 31, 508–513. [Google Scholar] [CrossRef] [PubMed]
- Chamberlain, M.; Junck, L.; Brandsma, D.; Soffietti, R.; Rudà, R.; Raizer, J.; Boogerd, W.; Taillibert, S.; Groves, M.D.; Le Rhun, E.; et al. Leptomeningeal metastases: A RANO proposal for response criteria. Neuro Oncol. 2017, 19, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.; Fong, C.; Luthra, A.; Smith, S.A.; DiNatale, R.G.; Nandakumar, S.; Walch, H.; Chatila, W.K.; Madupuri, R.; Kundra, R.; et al. Genomic characterization of metastatic patterns from prospective clinical sequencing of 25,000 patients. Cell 2022, 185, 563–575.e511. [Google Scholar] [CrossRef] [PubMed]
- Colclough, N.; Chen, K.; Johnström, P.; Strittmatter, N.; Yan, Y.; Wrigley, G.L.; Schou, M.; Goodwin, R.; Varnäs, K.; Adua, S.J.; et al. Preclinical Comparison of the Blood-brain barrier Permeability of Osimertinib with Other EGFR TKIs. Clin. Cancer Res. 2021, 27, 189–201. [Google Scholar] [CrossRef] [PubMed]
- Chajon, E.; Castelli, J.; Marsiglia, H.; De Crevoisier, R. The synergistic effect of radiotherapy and immunotherapy: A promising but not simple partnership. Crit. Rev. Oncol. Hematol. 2017, 111, 124–132. [Google Scholar] [CrossRef]
- Amin, S.; Baine, M.J.; Meza, J.L.; Lin, C. Association of Immunotherapy With Survival Among Patients With Brain Metastases Whose Cancer Was Managed With Definitive Surgery of the Primary Tumor. JAMA Netw. Open 2020, 3, e2015444. [Google Scholar] [CrossRef]



| Author (Year) | Primary Tumor | Phase | Treatment | (n) | Age (Years) | Median KPS/ECOG | BM (n) | mPFS (Months) | mOS (Months) | Response Criteria | Response Rate |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Kumthekar (2020) [9] | Breast | 2 | IV ANG1005 | 28 | 47.5 | 80 | 28 | 3.4 | 8 | CNS RECIST v1.1 | Intracranial ORR: (15%) stable/improved intracranial disease (77%) |
| Melisko (2019) [10] | Breast | 2 | IV irinotecan and TMZ | 8 | NA | NA | 7 | NA | 3 | NA in LMC subset | NA |
| Mrugala (2019) [11] | Breast | 2 | IV MTX and IT DepoCyt | 3 | 50 | 70 | 2 | 1.4 | 8.2 | Radiographic criteria (MRI), CSF cytology | NA |
| Bonneau (2018) [12] | Breast | 1 | IT trastuzumab | 16 | 57 | 80 | 14 | NA | 7.3 | Clinical, radiographic (RECIST v1.1), CSF cytology. | Clinical response: Responsive (3), stable (7), progressive (4), NA (2). Radiological response: Stable (9), progressive (5), NA (2) CSF cytology response: Responsive (2), Stable (6) Progressive (4), NA (4) |
| Wu (2015) [13] | Breast | Pilot | IV BEEP | 8 | 55 | 60 | 7 | 4.7 | 4.7 | -CSF cytology, clinically stable or improved | 3/5 (60%) |
| Orlando (2002) [14] | Breast | 2 | Day: 1 IT thiotepa + MTX, IT hydrocortisone, Day 2: IT cytarabine, IT MTX, IT hydrocortisone, and oral folinic acid | 13 | 45 | NA | 5 | NA | 2.07 | Complete: -CSF cytology + clinically stable Partial: decreased CSF cytology + clinically improved Failure: no decrease in CSF cytology + clinically stable or progression | 0 |
| Esteva (2000) [15] | Breast | 2 | ITV Ara-C | 10 | 49 | NA | 2 | NA | 5.7 | Complete: -CSF cytology > 4 weeks, clinically responsive Partial: -CSF cytology < 4 weeks, clinically responsive Failure: -CSF cytology, partial remission after 6 weeks, clinical progression after 3 weeks | Response: Complete (2), Partial (4), Treatment failure (3) |
| Lu (2021) [16] | EGFRmut NSCLC | 2 | Oral osimertinib (80 mg) + IV bevacizumab | 14 | 61 | NA | 11 | 9.3 | 12.6 | RANO LM radiological criteria | Response (7), Stable (6) Progression (1) LM ORR: 50% |
| Fan (2021) [17] | EGFRmut NSCLC | 1/2 | IT premetrexed + dexamethasone | 30 | 54 | 40–60 | NA | NA | 9 | Neurological signs and symptoms and KPS | RR: 87%, stable (1), Progressive (2), not evaluable (3) |
| Nosaki (2020) [18] | NSCLC | 2 | Oral erlotinib | 21 | 64 | 2 | NA | 2.2 | 3.4 | Negative conversion of CSF cytology | CSF RR: 30% |
| Park (2020) [19] | EGFRmut NSCLC | 2 | Oral osimertinib (160 mg) | 40 | 59 | 1 | NA | 8 | 13.3 | RECIST v1.1 | ICD complete response: 92.5%, ECD complete response: 85% |
| Yang (2020) [20] | EGFRmut NSCLC | 1 | Oral osimertinib (160 mg) | 41 | 59 | 2 | 29 | 8.6 | 11 | RECIST v1.1 and RANO criteria | LM ORR: 27% |
| Nanjo (2018) [21] | EGFRmut NSCLC | Pilot | Oral osimertinib (80 mg) | 13 | 67 | 2 | NA | 7.2 | Not reached | Clinical response, -conversion of CSF cytology, neuroimaging findings and RECIST v1.1 (extra CNS tumor) | CNS radiological RR: improved (8), stable (3), progressed (1), not evaluable (1). Clinical RR: improved (4), stable (8), worsened (n = 1) |
| Pan (2019) [22] | Lung | 1 | IT pemetrexed | 13 | 55 | 30 | NA | 2.5 | 3.8 | RANO criteria | Clinical RR: 31% (4/13) |
| Tamiya (2017) [23] | Lung | 1 | Oral afatinib | 11 | 66 | 2 | NA | 2 | 3.8 | RECIST v1.1 | ORR: 27.3% |
| Jackman (2015) [24] | EGFRmut NSCLC | 1 | High-dose oral gifetinib | 7 | 51 | 2 | brain | 750 mg: 1.9, 1000 mg: 2.5 | 750 mg: 1.9 1000 mg: 3.7 | Clinical neurological improvement, CSF clearance, radiological response (resolution of LM metastasis on MRI) | Clinical improvement (4/7). CSF clearance: 2/7 partial, 1/7 complete |
| Chamberlain (1998) [25] | NSCLC | 2 | ITV therapy (MTX: 32, cytarabine: 16, thiotepa: 6) | 32 | 57 | 90 | 9 | NA | 5 | Clinical response, -CSF cytology | MTX RR: 17 (43%), second-line Ara-C RR: 8 (50%), third line thiotepa RR: 2 (33%) |
| Chamberlain (1996) [8] | Melanoma | 2 | ITV MTX/Ara-C/thiotepa + RT | 16 | 47 | 80 | NA | NA | 4 | CSF cytology | RR: complete (2), partial (4), progressive (3) |
| Yang (2021) [26] | Varied | 1 | pCSI | 21 | 52 | 70 | 11 | 7 | 8 | RANO-LM criteria | 6-month CNS RR: 63% 1-year CNS RR: 19% |
| Naidoo (2021) [27] | Varied | 2 | IV pembrolizumab | 13 | 57 | 0 | NA | 2.9 | 4.9 | Clinical response, -CSF cytology, neuroimaging findings | CNS RR: 38% (5/13) progressive disease: 61.5% (8/13) |
| Brastianos (2021) [28] | Varied | 2 | IV ipilimumab and nivolumab | 18 | 54 | NA | 13 | 1.94 | 2.9 | 3-month OS, iRANO and RECIST v1.1 criteria | iRANO: Complete (1), stable (7),progression (4) not evaluable (6) RECIST: partial (1), stable (3), progression (3), not evaluable (11) |
| Brastianos (2020) [29] | Varied | 2 | IV pembrolizumab | 20 | 51.5 | NA | NA | 2.6 | 3.6 | 3-month OS, iRANO and RECIST v1.1 criteria | iRANO: RR stable (11), progressive (5), not evaluable (4) RECIST RR: stable (10), progression (1), not evaluable (9) |
| Pan (2020) [30] | Varied | 1/2 | IT pemetrexed + IFRT | 34 | 56 | 40 | 6 | 3.5 | 5.5 | RANO-LM criteria | Clinical RR: 52.9% (18/34) CSF RR: 32% (8/25) Imaging response: 33% (9/25) |
| Choi (2019) [31] | Varied | 2 | Slow VLP IT MTX | 47 | 59 | 70 | NA | NA | 5.3 | ICP normalization | ICP normalized: 13/22 (59%) |
| Pan (2016) [32] | Varied | 2 | IT MTX + RT | 59 | 55 | 40 | NA | NA | 6.5 | Clinical response (KPS, symptoms) | Complete response (14), obvious response (29), partial (8), stable (5), progressive (3) |
| Ursu (2015) [33] | Varied | 1 | IT CpG-28 | 29 | 56 | 70 | NA | 1.75 | 3.75 | Clinical and imaging response | Clinical improvement (4) Radiological response (3) |
| Segura (2012) [34] | Varied | 2 | Oral TMZ | 19 | 51 | 70 | NA | 0.92 | 1.4 | RECIST, corticosteroid use, clinical response, and CSF cytology | RECIST response: Complete = 0, partial = 2 (11%) stable = 1 (5%), progressive = 16/19 (84%) |
| Chamberlain (2006) [35] | Varied | 2 | ITV etoposide | 27 | 55 | NA | NA | 11% at 6-months | 2.5 | Clinical response, negative conversion of CSF cytology | Clinically stable and + CSF (+) = 12 (44%). Neurologically stable/improved/CSF (-) = 7/27 (26%) Complete response = 1/27 Partial response = 6/27 |
| Chamberlain (2002) [36] | Varied | 2 | ITV alpha interferon | 22 | 56 | NA | NA | NA | 4.14 | Clinical response, negative conversion of CSF cytology | Partial response (10), progressive disease (12) |
| Jaeckle (2002) [37] | Varied | 3 | ITV/IT DepoCyt | 110 | 50 | 70 | NA | 1.8 | 3.12 | Clinical response, negative conversion of CSF cytology | CSF RR: 19/70 (27%, 95% CI: 17–39%). Rate of neurological progression: 69/110 (63%) |
| Bokstein (1998) [38] | Varied | 2 | RT + ITV and systemic chemotherapy vs. RT + systemic chemotherapy | 104 | NA | NA | NA | NA | 4 | Clinical response, negative conversion of CSF cytology, neuroimaging findings | RT+ ITV + systemic chemo complete RR: 24/28 (86%) RT + Systemic chemo alone: 20/27 (74%) (p >0.05) |
| Nakagawa (1996) [39] | Varied | Pilot | IT VLP | 13 | 54 | NA | NA | NA | 7 | Good: (-) CSF + clinical improvement Moderate: CSF + clinical improvement Minor: CSF or clinical improvement Non-responder: without improvement | Good: 6/13 Moderate: 3/13 Minor: 2/13 None: 2/13 |
| Meyers (1991) [40] | Varied | 2 | ITV leukocyte α interferon | 9 | 50 | NA | NA | NA | 4 | Negative CSF cytology | CSF RR: 4/9 (44%) |
| Moseley (1990) [41] | Varied | Pilot | IT 131I radiolabeled mAb | 15 | NA | NA | 0 | NA | 12 | Clinical response, negative conversion of CSF cytology, imaging | Clinical RR: 5/9, CSF RR: 5/9, imaging RR: 5/9 |
| Trump (1982) [42] | Varied | 2 | ITV thiotepa and MTX + RT | 25 | 50 | NA | 10 | NA | 5.29 | Clinical response, negative conversion of CSF cytology | Clinical response: complete (4), partial (5), stable (13), progressive (3) CSF: 13/17 complete RR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marenco-Hillembrand, L.; Bamimore, M.A.; Rosado-Philippi, J.; Perdikis, B.; Abarbanel, D.N.; Quinones-Hinojosa, A.; Chaichana, K.L.; Sherman, W.J. The Evolving Landscape of Leptomeningeal Cancer from Solid Tumors: A Systematic Review of Clinical Trials. Cancers 2023, 15, 685. https://doi.org/10.3390/cancers15030685
Marenco-Hillembrand L, Bamimore MA, Rosado-Philippi J, Perdikis B, Abarbanel DN, Quinones-Hinojosa A, Chaichana KL, Sherman WJ. The Evolving Landscape of Leptomeningeal Cancer from Solid Tumors: A Systematic Review of Clinical Trials. Cancers. 2023; 15(3):685. https://doi.org/10.3390/cancers15030685
Chicago/Turabian StyleMarenco-Hillembrand, Lina, Michael A. Bamimore, Julio Rosado-Philippi, Blake Perdikis, David N. Abarbanel, Alfredo Quinones-Hinojosa, Kaisorn L. Chaichana, and Wendy J. Sherman. 2023. "The Evolving Landscape of Leptomeningeal Cancer from Solid Tumors: A Systematic Review of Clinical Trials" Cancers 15, no. 3: 685. https://doi.org/10.3390/cancers15030685
APA StyleMarenco-Hillembrand, L., Bamimore, M. A., Rosado-Philippi, J., Perdikis, B., Abarbanel, D. N., Quinones-Hinojosa, A., Chaichana, K. L., & Sherman, W. J. (2023). The Evolving Landscape of Leptomeningeal Cancer from Solid Tumors: A Systematic Review of Clinical Trials. Cancers, 15(3), 685. https://doi.org/10.3390/cancers15030685