Simple Summary
We delve into the intricate relationship between bisphosphonates, commonly used for treating osteoporosis and tumors, and their potential side effect: bisphosphonate-related osteonecrosis of the jaws (BRONJ) after dental procedures. We explore how bisphosphonates affect bone density and resorption, emphasizing their impact on dental treatments. Dental patients on bisphosphonates face a heightened risk of BRONJ, especially post-invasive dental procedures. Although topical applications enhance dental implant success and aid in periodontal treatment, systemic administration significantly raises BRONJ risk. Preventive measures involve maintaining oral health and considering alternative treatments. This review underscores the need for further research to refine protocols and ensure the safety of dental procedures for bisphosphonate-treated patients.
Abstract
Bisphosphonates are widely used to treat osteoporosis and malignant tumors due to their effectiveness in increasing bone density and inhibiting bone resorption. However, their association with bisphosphonate-related osteonecrosis of the jaws (BRONJ) following invasive dental procedures poses a significant challenge. This review explores the functions, mechanisms, and side effects of bisphosphonates, emphasizing their impact on dental procedures. Dental patients receiving bisphosphonate treatment are at higher risk of BRONJ, necessitating dentists’ awareness of these risks. Topical bisphosphonate applications enhance dental implant success, by promoting osseointegration and preventing osteoclast apoptosis, and is effective in periodontal treatment. Yet, systemic administration (intravenous or intraoral) significantly increases the risk of BRONJ following dental procedures, particularly in inflamed conditions. Prevention and management of BRONJ involve maintaining oral health, considering alternative treatments, and careful pre-operative and post-operative follow-ups. Future research could focus on finding bisphosphonate alternatives with fewer side effects or developing combinations that reduce BRONJ risk. This review underscores the need for further exploration of bisphosphonates and their implications in dental procedures.
1. Introduction
Bisphosphonates, a class of medications frequently employed to treat bone-related diseases, function by enhancing bone formation, improving bone density, and inhibiting osteoclast activity and bone resorption [1,2,3]. Structurally, bisphosphonates consist of two phosphonate groups linked by a carbon atom, rendering them resistant to degradation in acidic environments or by pyrophosphatases [4,5]. Figure 1 illustrates the general chemical structure of bisphosphonates, with the attached carbon chains (denoted as R and R’) varying depending on the specific type of bisphosphonate [6]. These medications can be administered orally or intravenously. Intravenous bisphosphonates, being more potent, are utilized for conditions like Paget’s disease, bone pain, and malignant tumors, while oral bisphosphonates are commonly used to treat osteoporosis, particularly in the elderly [1,7]. The most common oral bisphosphonates include alendronate and risedronate, whereas pamidronate and zoledronate are usually administered intravenously; some bisphosphonates are given both orally and intravenously, depending on the treatment and patient’s physical conditions [8]. Despite their efficacy, bisphosphonates are associated with upper gastrointestinal side effects, such as dysphagia, nausea, vomiting, and dyspepsia [9]. Their strong affinity for bone hydroxyapatites prevents bone degeneration and calcification, impacting bone development [10]. By impeding osteoclast recruitment, reducing activity, and inducing osteoclast apoptosis, bisphosphonates effectively decrease osteoclast activity and numbers [1,11,12]. Osteoporosis, a progressive skeletal disorder resulting in bone tissue loss and increased fragility, necessitates bisphosphonate treatment to strengthen bones and prevent fractures [2,13]. However, the use of bisphosphonates is associated with a severe side effect, especially relevant in dentistry: bisphosphonate-related osteonecrosis of the jaws (BRONJ) [8,14]. BRONJ typically occurs after invasive dental procedures, such as tooth extraction, oral trauma, or infections, particularly in the maxilla and mandible, where bisphosphonates tend to accumulate [8,12]. It manifests as visible necrotic bone in the jaws lasting more than eight weeks in individuals undergoing bisphosphonate therapy; the untreated bone can be seen and identified radiographically [12,15,16]. Even minor injuries can lead to impaired jawbone tissue repair in this state [16]. Given the widespread use of bisphosphonates in cancer treatment and managing osteoporosis—especially prevalent among the elderly—dental procedures pose significant challenges. When major dental procedures are necessary for patients receiving bisphosphonate therapy, careful management is crucial to ensure the success of treatment, as well as the health and safety of the patient. In this paper, we aim to address the interconnectedness of bisphosphonate, BRONJ, and their relations to dental procedures, namely implants, extractions, endodontics, periodontal treatment, and prosthodontics. We narrowed the scope of our search to only include statistics from studies published after 2010, in order to ensure the recency of the findings. Additionally, we suggested clinical guidelines and procedures to better mitigate the risks of BRONJ in bisphosphonate patients.
Figure 1.
Chemical structure of bisphosphonates. The “R” and “R’” refers to long carbon chains that differ depending on the type of bisphosphonate.
2. BRONJ: Mechanisms, Clinical Stages, and Effective Management Strategies
2.1. Mechanisms
The intricate mechanisms underlying BRONJ are not yet fully understood. However, its development is believed to result from various contributing factors. Figure 2 visually outlines the intricate interconnections among these factors, shedding light on the complex nature of BRONJ.
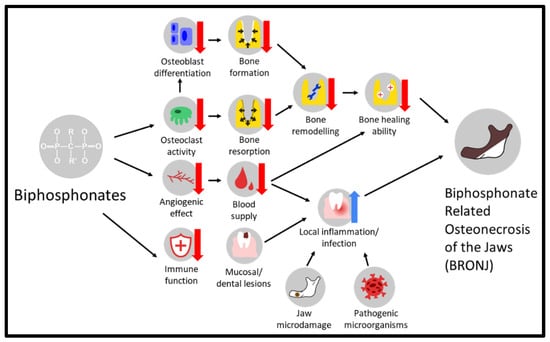
Figure 2.
An overview of potential factors contributing to the development of BRONJ.
2.1.1. Bone Remodeling Inhibition
One prevailing theory revolves around the inhibition of bone remodeling. Bisphosphonates exhibit a strong affinity for hydroxyapatite crystals, the primary constituents of bone mineral [17,18]. This affinity results in the induction of apoptosis and suppression of the activity of osteoclasts, the cells responsible for bone resorption [18,19,20]. By impeding osteoclast function, bisphosphonates disrupt the natural process of bone remodeling, causing delays and impairments in bone healing, particularly following invasive dental surgeries [21]. Furthermore, bisphosphonates indirectly hinder the differentiation of osteoblasts due to the absence of cytokines released by osteoclasts. This disruption further compromises the bone’s ability to heal and escalates the risk of osteonecrosis [18]. Notably, an analysis of human bone specimens from patients undergoing bisphosphonate treatment reveals an increased presence of nonfunctional osteoclasts surrounding necrotic bones, reinforcing the hypothesis of bone remodeling inhibition as a significant factor in the development of BRONJ [22,23]. This intricate interplay between bisphosphonates, osteoclasts, and osteoblasts underscores the complexity of BRONJ’s pathogenesis. The inhibition of bone remodeling disrupts the delicate balance between bone resorption and formation, playing a pivotal role in the onset and progression of this condition. The combination of apoptosis induction, osteoclast suppression, and impaired osteoblast differentiation creates a microenvironment conducive to osteonecrosis, highlighting the multifaceted nature of BRONJ’s development [18,19,20,21,22,23].
2.1.2. Angiogenesis Inhibition
Bisphosphonates are known to interfere with angiogenesis, inhibiting the formation of new blood vessels within the jawbone [24]. This impaired blood supply can impede proper bone healing, making the tissue more susceptible to infections and necrosis [23]. Studies conducted on animals have demonstrated a reduction in arterial area, venous area, and overall vascularity in periodontal tissues during the onset of BRONJ [25,26]. Remarkably, research indicates a higher incidence of BRONJ in individuals simultaneously using anti-resorptive agents (such as bisphosphonates) and anti-angiogenic agents [27,28]. The cumulative evidence highlights the significant impact of bisphosphonates on diminishing vascularity in jawbones. This decrease in blood vessel formation compromises the natural healing capacity of bones, elevating the risk of complications such as infections and necrosis. This intricate relationship between the inhibition of angiogenesis and the development of BRONJ underscores the necessity for a comprehensive understanding of vascular dynamics in bone tissue, particularly concerning bisphosphonate treatments [24,25,26,27,28]. It emphasizes the importance of ongoing research to delve deeper into these interactions, enabling healthcare professionals to make informed decisions and implement targeted strategies when managing patients undergoing bisphosphonate therapy. This knowledge is paramount in enhancing patient outcomes and ensuring the safety and efficacy of treatments in the realm of bone-related conditions and cancer therapies.
2.1.3. Inflammation or Infection
Another hypothesis centers on the immunosuppressive effects of bisphosphonates on the body’s immune system [29]. These effects have the potential to compromise the jawbone tissues’ ability to defend against infections. Mucosal or dental lesions associated with bisphosphonates can trigger local inflammation, leading to infections that spread to the bone and exacerbate osteonecrosis [30]. Several factors contribute to the specificity of bisphosphonate-related osteonecrosis in the jaw. Firstly, the mandibular and maxilla bones are thinly covered by a mucoperiosteal layer, offering limited protection against oral pathogens [30]. Furthermore, the jawbone is prone to repetitive microtraumas due to occlusion and chewing activities. This ongoing bone remodeling process facilitates a higher accumulation of bisphosphonates, magnifying their impact [30]. Specifically, within the jaw, the alveolar crest undergoes a faster rate of remodeling compared to other bones, resulting in the accumulation of one of the highest concentrations of bisphosphonates [17,30]. This complex interplay between immunosuppression, recurrent microtraumas, and the unique anatomical characteristics of the jawbone underscores the specific vulnerability of the jaw to bisphosphonate-related osteonecrosis. Understanding these intricate factors is essential for developing targeted and effective preventive strategies and treatment approaches [29,30]. Continued research in this area is vital to advancing our knowledge and enhancing the care and safety of individuals undergoing bisphosphonate therapy.
2.2. Clinical Manifestations and Staging
In clinical settings, BRONJ exhibits a range of symptoms, the severity of which can vary. These symptoms commonly include jaw pain, mobility of teeth, exposed jawbone, soft tissue damage or ulceration, numbness of the lower lip (hypoesthesia), non-healing extraction sockets, and swelling or inflammation in the jaw and gum area [31,32]. The progression of BRONJ is categorized into distinct stages. Table 1 provides a concise summary of the key points of each stage.

Table 1.
A summary table of the symptoms and clinical stages of BRONJ, according to AAOMS and SICMF-SIPMO.
According to the American Association of Oral and Maxillofacial Surgeons’ (AAOMS) Position Paper, four stages can be observed:
Stage 0: This stage is characterized by nonspecific symptoms such as pain and swelling, lacking clinical evidence of exposed bone or necrotic tissue [32,33].
Stage 1: Patients in this stage are asymptomatic but exhibit exposed and necrotic bone within the mouth, persisting for more than eight weeks without signs of infection [32,33].
Stage 2: In this stage, there is exposed and necrotic bone (fistulae) that can be probed down to the bone. This condition is associated with pain and infection, indicating a more advanced level of tissue involvement [32,33].
Stage 3: The most severe stage involves extensive exposed and necrotic bone (fistulae) that can be probed down to the bone. It is associated with active infection and additional complications such as pathological fractures of the jaw, representing a critical and challenging clinical scenario [32,33].
Alternatively, a different approach to BRONJ staging has been proposed by the Italian Society of Maxillofacial Surgery and the Italian Society of Oral Pathology and Medicine, jointly known as the SICMF-SIPMO. In particular, the criteria proposed by SICMF-SIPMO emphasizes the importance of radiological symptoms that can be observed via CT scans, whereas AAOMS considers only clinical symptoms [34]. SICMF-SIPMO does not have a stage 0, and classifies stages in the following way:
Stage 1: Focal, patients exhibit at least one minor clinical symptom; CT scans showing bone condensation limited to only the alveolar process [34].
Stage 2: Diffused, patients exhibit at least one minor clinical symptom; CT scans showing bone condensation spreading to the basal bone area [34].
Stage 3: Severe, patients exhibit one or more major clinical symptoms; CT scans showing large scale damage, such as fractures or osteolysis, of the surrounding facial bones, (e.g., mandible, maxilla, zygomatic or hard palate) [34].
Regardless of the differences in the staging criteria, these progressive stages highlight the varying degrees of tissue involvement and clinical complexity in BRONJ cases. Understanding these stages is essential for accurate diagnosis, appropriate management, and tailored treatment planning for affected individuals [32,33].
2.3. Risk Factors
As previously stated, bisphosphonates serve as the primary trigger for BRONJ. Nevertheless, the development of BRONJ is influenced by various additional risk factors.
2.3.1. Accumulated Dosage (Prolonged Treatment Duration)
The accumulation of medication over time often occurs during extended treatment, a situation more frequently encountered in cancer patients [35]. Extensive research on individuals undergoing cancer treatment has unequivocally established a direct link between the prevalence of BRONJ and the duration of exposure to bisphosphonate drugs. This research underscores the significantly heightened risk associated with prolonged treatment periods [35]. Consequently, it is imperative to emphasize the critical importance of monitoring the duration of bisphosphonate therapy, especially in cancer patients, in order to mitigate the potential occurrence of BRONJ. This correlation emphasizes the need for vigilant oversight and careful management of patients undergoing extended bisphosphonate treatments. It calls for a collaborative effort between oncologists and dental professionals, working closely together to ensure a nuanced and balanced approach. Such an approach must not only take into account the therapeutic benefits these treatments offer, but also carefully weigh them against the potential risks associated with their prolonged use [35]. By doing so, healthcare providers can optimize patient outcomes while minimizing the adverse effects, thereby enhancing the overall quality of care for individuals requiring extended bisphosphonate therapy.
2.3.2. Dental Surgical Procedures
The association between dental extraction and osteonecrosis of the jaw has been firmly established. Patients with dentures face a heightened risk in this regard [36]. Clinical studies revealed a significant increase in the risk of developing BRONJ following dental extraction, with figures ranging from 33 to 333 times higher compared to non-extraction cases [37]. Moreover, tooth extraction was found to trigger osteonecrosis in 38% of patients [38]. Several studies have emphasized the role of concurrent dental diseases or dentoalveolar procedures in elevating the risk of BRONJ [38,39]. It is worth noting that whether BRONJ manifests after invasive oral surgical procedures in patients on bisphosphonates often hinges on the expertise and technique employed by the dentist [37,39,40]. This body of evidence highlights the critical need for meticulous dental care and skilled dental practitioners when treating patients undergoing bisphosphonate therapy, especially those requiring dental extractions or similar interventions [36,37,38,39,40]. Details about the interconnectedness of BRONJ and specific dental procedures will be addressed in detail in the next section.
2.3.3. Malignancy
Cancer chemotherapy medications and the presence of malignancies significantly elevate the risk of jaw osteonecrosis [41]. Cancer cells often metastasize to the bones, necessitating the use of bisphosphonates to alleviate symptoms and impede further damage. Paradoxically, the essential administration of bisphosphonates to manage bone complications in cancer patients simultaneously heightens the risk of developing BRONJ [42,43,44]. This double-edged relationship between cancer treatments, bisphosphonate usage, and the increased susceptibility to BRONJ underscores the intricate challenges faced in managing cancer-related bone issues. Balancing the therapeutic benefits of bisphosphonates with the potential complications, especially in cancer patients, necessitates careful consideration and close monitoring to mitigate the risk of BRONJ effectively [41,42,43,44].
2.4. Prevention and Management
Given the high occurrence rate of jaw osteonecrosis in patients with malignant diseases (92%), it is imperative to establish effective prevention and management strategies [35,37]. A structured approach can be taken to address patients at different stages of bisphosphonate treatment. For individuals about to commence intravenous bisphosphonate therapy, the primary objective is to minimize the risk of BRONJ by optimizing dental health [45]. Ideally, bisphosphonate therapy initiation should be delayed until dental health is thoroughly optimized, a decision that requires collaboration among the treating physician, dentist, and specialists. During this stage, the focus should be retaining restorable teeth and completing necessary surgeries 4 to 6 weeks before initiating bisphosphonate treatment, allowing adequate time for osseous healing; patients should actively cooperate with regular evaluations and promptly report any symptoms potentially related to BRONJ [33,45]. The next stage involves patients already receiving bisphosphonates, but without evidence of osteonecrosis [33,45]. Here, maintaining excellent oral hygiene remains crucial, with a focus on preserving teeth whenever possible. If tooth extraction becomes necessary, retaining the tooth root is recommended, to minimize trauma to the bone and oral tissues. Additionally, patients exposed to bisphosphonates like zoledronic acid and pamidronate should avoid dental implant procedures, minimizing the risk of complications. The final stage pertains to patients diagnosed with established BRONJ [33,45]. In these cases, panoramic and tomographic imaging are essential for accurate assessment. However, due to the unpredictable response of these cases to bisphosphonates, surgical treatment is challenging and should be delayed. During this stage, trimming soft tissues helps minimize exposure and promotes healing. The primary objectives at this stage include pain elimination and infection control, highlighting the critical importance of comprehensive and personalized management strategies [37,46,47]. This systematic approach is vital for enhancing the quality of care and outcomes for patients dealing with BRONJ.
3. Bisphosphonates’ Impact on Dental Procedures
3.1. Dental Implants
Implantology, a dental procedure involving the placement of dental implants in the maxillary or mandibular bone, is vital for restoring missing teeth, supporting chewing function, and preserving aesthetics [48]. Key to the success of dental implants is the process of osseointegration, the formation of integration between bone and titanium implants, a process influenced by factors like bone characteristics, tobacco use, and the patient’s overall health [49,50]. Bisphosphonates, commonly used for medical treatments, can be administered systematically or topically, the latter involving localized application, such as coating the surface of dental implants [51]. Studies have shown positive outcomes when bisphosphonates are coated on implants, enhancing osseointegration and delaying osteoclast apoptosis, ultimately extending the preservation time of marginal bone around implants [51,52,53]. These findings indicate the potential benefits of topical bisphosphonate applications, presenting a promising avenue for clinical consideration. However, the impact of BRONJ on dental implants depends on the method of administration. Research indicates that patients using intraoral bisphosphonates for less than five years pose a low risk for BRONJ following dental implantation, especially when operative care is meticulously observed [54]. In contrast, intravenous bisphosphonate therapy carries a higher risk, making dental implant placement a high-risk situation for these patients [55]. To ensure implant safety, pre-operation measures such as drug withdrawal evaluation, antibiotic usage, and follow-up protocols are essential [3,56]. Additionally, combining treatments, such as using plasma rich in platelet (PRP), platelet-rich fibrin (PRF), and plasma rich in growth factors (PRGF), enhances wound closure and aids in the implant healing process [57,58,59]. In conclusion, the method and duration of bisphosphonate administration significantly influences dental implant outcomes and the risk of developing BRONJ. Continued research and in-depth studies are imperative to gain a comprehensive understanding of bisphosphonate effects on implantology. Dentists must remain vigilant, thoroughly evaluating patient conditions, and maintaining rigorous follow-up protocols post-implantation, especially for patients undergoing bisphosphonate treatments, to mitigate the risk of BRONJ and ensure the success of dental implant procedures.
3.2. Extraction
Based on research and statistical findings, BRONJ typically manifests following tooth extraction [60]. Most studies suggest that the development of BRONJ is influenced by various contributing factors. One study revealed that patients currently undergoing intravenous bisphosphonate therapy did not exhibit a higher risk for BRONJ compared to patients who had completed or temporarily paused their intravenous bisphosphonate therapy [61]. However, the risk of BRONJ significantly increases when tooth extraction involves an osteotomy, particularly a mandible osteotomy [61]. Several investigations propose that common infectious diseases are also contributing factors to the development of BRONJ [62,63]. For instance, preexisting pathological inflammatory conditions like baseline osteomyelitis and periapical periodontitis are risk factors that may induce the development of BRONJ following tooth extraction [64,65]. Otto et al. concluded that tooth extraction itself might not be the primary cause of BRONJ but rather the complications, such as infections associated with the procedure, contribute to its development [65]. On the contrary, Song et al. found that "tooth extraction alone" could lead to BRONJ, while inflammation induced by pulp exposure worsened BRONJ by causing more bone necrosis [65]. BRONJ did not develop when inflammation was present without a tooth extraction procedure [65]. In this case, tooth extraction appears to act as a trigger, but other factors can influence the severity of BRONJ. Similarly, tooth extraction was reported to be the leading cause of BRONJ among patients with bisphosphonate therapy, with a relative risk “5.3–53 times higher” than bisphosphonate patients who do not undergo tooth extraction [66]. Since extractions appear to be a high-risk trigger for the development of BRONJ in bisphosphonate patients, it is recommended to avoid extractions, if possible, but only under conditions that allow for the lesion or inflammation to be resolved with alternative treatments [66].
On the other hand, although patients administered bisphosphonates are currently classified as high-risk, some believe tooth extraction can be performed safely following established guidelines [62,63]. An experimental study indicated that the application of bFGF, a growth factor, can promote healing in tooth sockets after extraction and prevent the development of BRONJ. Researchers suggested that bFGF might counteract the interference of bisphosphonates with bone healing. Specifically, bFGF prevents the inhibition of healing, thereby reducing the risk of BRONJ after tooth extraction [60]. Treatment with PRGF, another growth factor, can restore the osteoblast/osteoclast homeostatic cycles, counteracting and minimizing the effects of bisphosphonates on osteoclasts, thus reducing the risk of BRONJ development in patients [67]. In another case, a patient with BRONJ was treated by removing infected tissue and suspending bisphosphonate usage, with no signs of recurrence after a year [68]. While the precise role of tooth extraction in the development of BRONJ may still require further investigation, it is evident that maintaining good oral health is beneficial in preventing severe BRONJ, either by decreasing its severity or by reducing the risk of its development.
3.3. Endodontics
Due to the high risk of developing BRONJ following tooth extraction in bisphosphonate patients, endodontics is commonly seen as an alternative treatment method. Endodontics could preserve the tooth, preventing the need for extraction and significantly decreasing the risk of apical periodontitis, both of which majorly contribute to the development of BRONJ [69]. However, endodontics itself could also contribute to BRONJ. During root canal shaping and cleaning, the inner pulp and dentin of the tooth is directly exposed to the oral environment and the microorganisms within [69]. Moreover, soft tissue damage can occur while cleaning the root or when applying a rubber dam, also increasing the risk of BRONJ [70].
Exploring this relationship inversely, bisphosphonates impact the outcome of endodontic treatments. After root canal treatment, periapical lesions heal via a bone remodeling process, but this process would be inhibited by bisphosphonates [70]. The lack of bone modelling delays the healing process, and, if coupled with microleakage or incomplete seals, could increase the risk inflammation, thus also increasing the risk of BRONJ developing [70,71].
That being said, it appears endodontic procedures performed on bisphosphonate patients generally have high success rates. Studies have found a high tooth survival rates of endodontic teeth of bisphosphonate patients of around 70%, with no significant difference compared to the control group; extractions were only deemed necessary in the case of tooth fractures and periodontal inflammation [72,73]. Oral bisphosphonates were not found to pose a significant risk to the successful healing following endodontic treatment [74]. On the other hand, IV bisphosphonates may interfere with the healing of root canal procedures: Dereci et al. found endodontic procedures to be more successful in patients receiving IV bisphosphonates less than a year compared to those that have been for a longer period; however, this study has a small sample size, and the generalizability of the results may be limited [75]. Although endodontic procedures in bisphosphonate patients may not be without risks, it appears that it might be a suitable alternative for tooth extraction in bisphosphonate patients, if conditions permit.
3.4. Periodontal Treatment
Periodontitis is the inflammation of the gingiva caused by bacterial flora, which could lead to the destructive of gingival tissues, or tooth loss, in more severe cases [76]. It can be caused by both local and systemic factors, and is easily influenced by factors such as immunity, oral hygiene habits, and many more [77]. Periodontitis is traditionally treated via a procedure known as scaling and root planning (SRP), which physically removes the pathogenic microorganisms causing the inflammation [76]. However, many studies have found adjunctive bisphosphonate therapy to be effective in the treating periodontitis, due to the bisphosphonates’ ability to inhibit proinflammatory cytokines and the resorption of alveolar bone, providing a different approach to periodontal treatment [78,79,80,81]. Bisphosphonates have been administered intravenously or applied locally, in gel-form (often using alendronate specifically) for these purposes [82,83]. According to several review articles, a vast number of studies with locally applied bisphosphonates (applied after traditional SRP) showed significant improvements to patients’ periodontal conditions, resulting in decreased probing pocket depth [76,78]. Similar results were found for bisphosphonates administered systemically, whether orally or intravenously, with oral bisphosphonates showing greater improvement compared to IVs [76]. Although both systemic and local bisphosphonates demonstrate effectiveness, locally applied bisphosphonates are preferred due to having fewer side effects [78]. Based on these results, it seems quite promising to utilize bisphosphonates in conjunction with SRP for periodontal treatment. There has not yet been a comparison of effectiveness between locally and systemically applied bisphosphonates for periodontal treatment, which is a potential area for further research.
However, periodontitis itself is closely correlated with BRONJ. According to Thumbigere-Math et al., a high percentage of patients with BRONJ had periodontal disease, ranging from 41–84% [84]. BRONJ patients were found to have less alveolar bone support and fewer teeth remaining, which are both indirect measures of periodontal health [84]. Microorganisms causing periodontitis have also been found in BRONJ lesions from multiple studies [85,86]. The American Association of Oral and Maxillofacial Surgeons’ Position Paper (2022 Update) also cites “pre-existing inflammatory dental disease such as periodontal disease” as a risk factor for BRONJ [23].
It is quite interesting to consider bisphosphonates being related to periodontal disease and BRONJ from two perspectives. On one hand, bisphosphonates are the solution; they can help improve periodontal disease through decreasing inflammatory cytokines and inhibiting bone resorption [78,79,80,81]. But on the other hand, bisphosphonates coupled with periodontal diseases poses the risk of BRONJ developing. A recent study, conducted in 2021, found results indicating that the use of systemic bisphosphonates along with periodontal disease leads to the development of BRONJ in rats [21]. They proposed a possible mechanism: the inflammation from periodontal disease coupled with the decreased osteoclastic activity due to bisphosphonates exposes the alveolar bone to a high concentration of inflammatory cytokines and microorganisms, both of which increases the risk of BRONJ developing [21].
Taken together, this raises the following question: is it worth it to introduce bisphosphonates—for the sake of improving periodontal conditions—into a patient who has no prior history of using bisphosphonates, thus presenting the possibility of developing BRONJ? Without dental bisphosphonate treatment, these patients have no risk of BRONJ, even with their present periodontitis conditions. However, periodontitis is a problem that significantly affects the oral and general health of the patient; it should be addressed regardless of its connection to BRONJ. Based on the data, bisphosphonates seem to be quite effective to use in conjunction with SRP, but some researchers have suggested against using it for reasons relating to BRONJ [78]. The decision of whether or not bisphosphonates should be applied in the treatment of periodontitis should be a mutual agreement between doctors and patients, and should be made after careful consideration of the patient’s health conditions and other relevant factors.
3.5. Prosthodontics
The relationship between bisphosphonates and prosthodontics, whether fixed or removable, has not been studied in depth, and a consensus cannot be reached regarding its role in the development of BRONJ. Some studies identified the use of dentures as a risk factor for BRONJ developing, attributing the reason to denture trauma [87,88,89]. Contrarily, other researchers stated that prosthodontic management does not pose a high risk, especially when compared with aforementioned invasive oral surgical procedures, namely extractions and implants, even suggesting that patients who have developed BRONJ can still undergo prosthodontic rehabilitation for aesthetic and functional purposes [90]. Nevertheless, it is beneficial to minimize the pressure of the dental prosthesis on the mucosa to minimize the risk of BRONJ, or to avoid worsening the condition [87,90]. Removable dentures were identified to be more likely to cause mucosa trauma, compared to fixed dentures [90]. A heat-polymerized resilient denture liner as a denture base material has been suggested to prevent localized stresses and distributing the load more evenly over the whole base, potentially providing a preventative measure for patients requiring prosthodontics [87]. It is critical that patients with dentures attend dentist appointments regularly. Any discomfort should be promptly reported so poorly fitting dentures can be adjusted or replaced to minimize soft tissue trauma [89]. Ali et al. recommended closely monitoring the denture-bearing tissues and prosthesis at 2–3-month intervals [90].
4. Discussion
In this review, we have explored the impact of bisphosphonates on dental procedures, focusing on dental implants, extractions, endodontics, periodontal treatment, and prosthodontics. The findings presented here provide valuable insights into the complexities surrounding bisphosphonate administration and its effects on oral health.
4.1. Administration Routes and Effect on Dental Procedures
Dental procedures are affected by bisphosphonates differently, but general trends can be suggested based on current research. In terms of systemic bisphosphonates, it has been found that BRONJ has higher incidence rates in bisphosphonate patients if they were administered intravenously, compared to oral bisphosphonates, regardless of the dental procedure performed [54,55,66]. We cannot be conclusive that the differences are caused by the route of administration alone; other factors, such as differing health conditions of patients who require IV or oral bisphosphonates could also play a role. However, a recent study has found that IV administration of bisphosphonates seem to have a greater effect on osteoclastic activity—compared to oral bisphosphonates at the same dosage—that seems to “aggravate” the conditions of BRONJ [91].
As opposed to systemic bisphosphonates, locally applied bisphosphonates seem to be an overall positive addition to dental procedures. Studies show that it positively improves implant osseointegration and periodontal treatment [51,52,53,78,79,81]. There has been no record of BRONJ occurring after applying bisphosphonates locally, and the general consensus seems to be that locally applied bisphosphonates pose no serious side effects to the patient [52,78]. Current literature does not seem to explain the mechanisms or reasons behind this phenomenon; this gap in knowledge is an important area in need of further research.
4.2. Interconnectedness of Risk Factors of BRONJ
Additionally, although tooth extractions are commonly viewed as a major contributing factor to BRONJ, some researchers believe the involvement of tooth extractions is overstated. For one, Kishimoto et al. proposes that most tooth extraction are necessary because of periodontal inflammation [92]. Hence, it may appear that tooth extraction is the leading cause of BRONJ, when other factors, such as periodontal disease, could also be contributing to its development. It seems possible that extractions are not the sole reason for BRONJ, and BRONJ sometimes develop even in the absence of extractions; however, the act of extracting seems to be a major trigger that greatly increases the risk of BRONJ developing soon after [65]. It is also important to note that the process of tooth extraction was found to increase inflammatory cytokine levels—a major risk factor of BRONJ—which would not be present in the absence of extractions; thus, perhaps the act of extraction does play a significant role in BRONJ [93]. Regardless of whether it is extractions themselves or the combination of extractions and periodontal inflammation increasing the incidence rate of BRONJ, it is crucial not to delay extractions due to fear of BRONJ developing. The untreated inflammation poses a serious risk for BRONJ and may lead to other oral health conditions. If the patient’s circumstances allow for it, endodontic treatment could be used as an alternative to extraction, decreasing the risk of microdamage or trauma that could trigger BRONJ.
4.3. Clinical Guidelines for Minimizing Risks
Due to the prevalence of bisphosphonates used in medical treatment, it seems necessary to propose guidelines for preventative measures and clinical recommendations to help minimize the risk of BRONJ. A summary of pre-procedural and post-procedural guidelines for both patients and doctors can be found in Table 2. Generally agreed upon guidelines include: identifying and treating infection or potential infection sites, performing high-risk operations (e.g., tooth extractions, dental implants) prior to starting bisphosphonate therapy, maintaining good oral and general health, using antimicrobial mouthwash (e.g., chlorhexidine) prior and following procedures, thoroughly sanitizing equipment, and minimizing trauma during dental procedures [24,70]. These preventative measures were found to significantly reduce risk of BRONJ developing [94,95].
Table 2.
A summary of clinical guidelines for minimizing risk of BRONJ.
The need or effectiveness for a drug holiday is considered controversial. Some researchers support it for the purposes or minimizing BRONJ risk, while others believe it interferes with the original intention of the bisphosphonate treatment in addition to increasing the risk of bone fractures during the dental procedure, especially in the case of osteoporosis patients [23]. Additionally, antibiotics have been suggested to decrease local inflammation and reduce inflammatory cytokines prior and following major dental procedures [93,96,97]. While antibiotics might be useful, there is debate regarding their necessity, addressing concerns surrounding antimicrobial resistance [98]. The overuse of antibiotics in dentistry is a phenomenon not limited to BRONJ, and bisphosphonate patients are at a significantly higher risk of developing devastating side effects; thus, antibiotic use does not seem unjustified in this case, but ultimately, it is the doctor’s decision.
The usage of anesthetic agents without vasoconstricting effects has also been suggested [70,99]. As bisphosphonates already have angiogenic effects that increase risk of BRONJ, some researchers want to prevent further reducing blood flow to the operated area [70,99]. However, this comes with greater risks, such as extreme blood loss for the patient, and thus, is not generally incorporated in dental procedures.
5. Conclusions
In conclusion, while bisphosphonates offer significant benefits in various medical and dental treatments, their impact on oral health and other dental procedures necessitates careful consideration. Systemic administration of bisphosphonates generally poses a risk of BRONJ developing following major dental procedures, such as implants and extractions; thus, endodontics could be a lower-risk alternative for extractions, if conditions permit. Local applications of bisphosphonate greatly increase the success rates of periodontal treatment and implant osseointegration. Continued research in this field is essential to refine protocols, ensuring the safety and success of dental procedures for patients undergoing bisphosphonate treatments.
Author Contributions
E.S.L., M.-C.T., J.-X.L., C.W., Y.-N.C., A.-C.L., Y.-F.L., C.-Y.F., C.-Y.W. and I.-T.L. designed and conceived this review. E.S.L., M.-C.T., J.-X.L., C.W., Y.-N.C., A.-C.L., Y.-F.L., C.-Y.F., C.-Y.W. and I.-T.L. drafted the manuscript and prepared the figures. E.S.L., M.-C.T., J.-X.L., C.W., Y.-N.C., A.-C.L., Y.-F.L., C.-Y.F., C.-Y.W. and I.-T.L. edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the College of Oral Medicine, Taipei Medical University, Taiwan, grant number TMUCOM202202.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available in this article.
Acknowledgments
We thank Wei-Ning Lin for her suggestions on manuscript layout.
Conflicts of Interest
The authors declare that there are no conflicts of interest regarding the publication of this article.
References
- Berardi, D.; Carlesi, T.; Rossi, F.; Calderini, M.; Volpi, R.; Perfetti, G. Potential applications of biphosphonates in dental surgical implants. Int. J. Immunopathol. Pharmacol. 2007, 20, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Ashrafi, M.; Gholamian, F.; Doblare, M. A comparison between the effect of systemic and coated drug delivery in osteoporotic bone after dental implantation. Med. Eng. Phys. 2022, 107, 103859. [Google Scholar] [CrossRef] [PubMed]
- López-Cedrún, J.L.; Sanromán, J.F.; García, A.; Peñarrocha, M.; Feijoo, J.F.; Limeres, J.; Diz, P. Oral bisphosphonate-related osteonecrosis of the jaws in dental implant patients: A case series. Br. J. Oral Maxillofac. Surg. 2013, 51, 874–879. [Google Scholar] [CrossRef]
- Cheng, A.; Mavrokokki, A.; Carter, G.; Stein, B.; Fazzalari, N.L.; Wilson, D.F.; Goss, A.N. The dental implications of bisphosphonates and bone disease. Aust. Dent. J. 2005, 50, S4–S13. [Google Scholar] [CrossRef]
- Montoya-Carralero, J.M.; Parra-Mino, P.; Ramírez-Fernández, P.; Morata-Murcia, I.M.; Mompeán-Gambín Mdel, C.; Calvo-Guirado, J.L. Dental implants in patients treated with oral bisphosphonates: A bibliographic review. Med. Oral Patol. Oral Cir. Bucal. 2010, 15, e65–e69. [Google Scholar] [CrossRef][Green Version]
- Roelofs, A.J.; Ebetino, F.H.; Reszka, A.A.; Russell, R.G.G.; Rogers, M.J. Bisphosphonates: Mechanisms of action. In Principles of Bone Biology; Academic Press: Cambridge, MA, USA, 2008; pp. 1737–1767. [Google Scholar]
- Jain, V.; Seith, A.; Manchanda, S.; Pillai, R.; Sharma, D.; Mathur, V. Effect of intravenous administration of zoledronic acid on jaw bone density in cases having skeletal metastasis: A prospective clinical study. J. Indian Prosthodont. Soc. 2019, 19, 203–209. [Google Scholar] [CrossRef]
- De-Freitas, N.R.; Lima, L.B.; de-Moura, M.B.; Veloso-Guedes, C.C.; Simamoto-Júnior, P.C.; de-Magalhães, D. Bisphosphonate treatment and dental implants: A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e644–e651. [Google Scholar] [CrossRef]
- Psimma, C.; Psimma, Z.; Willems, H.C.; Klüter, W.J.; van der Maarel-Wierink, C.D. Oral bisphosphonates: Adverse effects on the oral mucosa not related to the jaw bones. A scoping review. Gerodontology 2022, 39, 330–338. [Google Scholar] [CrossRef]
- Vuorimies, I.; Arponen, H.; Valta, H.; Tiesalo, O.; Ekholm, M.; Ranta, H.; Evälahti, M.; Mäkitie, O.; Waltimo-Sirén, J. Timing of dental development in osteogenesis imperfecta patients with and without bisphosphonate treatment. Bone 2017, 94, 29–33. [Google Scholar] [CrossRef]
- Mendes, V.; dos Santos, G.O.; Calasans-Maia, M.D.; Granjeiro, J.M.; Moraschini, V. Impact of bisphosphonate therapy on dental implant outcomes: An overview of systematic review evidence. Int. J. Oral Maxillofac. Surg. 2019, 48, 373–381. [Google Scholar] [CrossRef]
- Nieckula, P.; Stempniewicz, A.; Tubaja, M. Prophylaxis of osteonecrosis in the case of patients treated with bisphosphonates: A review paper. Dent. Med. Probl. 2018, 55, 425–429. [Google Scholar] [PubMed]
- Ata-Ali, J.; Ata-Ali, F.; Peñarrocha-Oltra, D.; Galindo-Moreno, P. What is the impact of bisphosphonate therapy upon dental implant survival? A systematic review and meta-analysis. Clin. Oral Implants Res. 2016, 27, e38–e46. [Google Scholar] [CrossRef] [PubMed]
- Chadha, G.K.; Ahmadieh, A.; Kumar, S.; Sedghizadeh, P.P. Osseointegration of dental implants and osteonecrosis of the jaw in patients treated with bisphosphonate therapy: A systematic review. J. Oral Implantol. 2013, 39, 510–520. [Google Scholar] [CrossRef] [PubMed]
- Serra, M.P.; Llorca, C.S.; Donat, F.J. Oral implants in patients receiving bisphosphonates: A review and update. Med. Oral Patol. Oral Cir. Bucal. 2008, 13, E755–E760. [Google Scholar]
- Vidal-Gutiérrez, X.; Gómez-Clavel, J.F.; Gaitán-Cepeda, L.A. Dental extraction following zoledronate, induces osteonecrosis in rat’s jaw. Med. Oral Patol. Oral Cir. Bucal. 2017, 22, e177–e184. [Google Scholar]
- Singh, M.; Gonegandla, G.S. Bisphosphonate-induced osteonecrosis of the jaws (BIONJ). J. Maxillofac. Oral Surg. 2020, 19, 162–167. [Google Scholar] [CrossRef]
- AlDhalaan, N.A.; BaQais, A.; Al-Omar, A. Medication-related osteonecrosis of the jaw: A review. Cureus 2020, 12, e6944. [Google Scholar] [CrossRef]
- Favia, G.; Tempesta, A.; Limongelli, L.; Crincoli, V.; Maiorano, E. Medication-related osteonecrosis of the jaw: Surgical or non-surgical treatment? Oral Dis. 2018, 24, 238–242. [Google Scholar] [CrossRef]
- Kuroshima, S.; Sasaki, M.; Murata, H.; Sawase, T. Medication-related osteonecrosis of the jaw-like lesions in rodents: A comprehensive systematic review and meta-analysis. Gerodontology 2019, 36, 313–324. [Google Scholar] [CrossRef]
- Kuroshima, S.; Sasaki, M.; Sawase, T. Medication-related osteonecrosis of the jaw: A literature review. J. Oral Biosci. 2019, 61, 99–104. [Google Scholar] [CrossRef]
- Wehrhan, F.; Gross, C.; Creutzburg, K.; Amann, K.; Ries, J.; Kesting, M.; Geppert, C.I.; Weber, M. Osteoclastic expression of higher-level regulators NFATc1 and BCL6 in medication-related osteonecrosis of the jaw secondary to bisphosphonate therapy: A comparison with osteoradionecrosis and osteomyelitis. J. Transl. Med. 2019, 17, 69. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Aghaloo, T.; Carlson, E.R.; Ward, B.B.; Kademani, D. American association of oral and maxillofacial surgeons’ position paper on medication-related osteonecrosis of the jaws—2022 update. J. Oral Maxillofac. Surg. 2022, 80, 920–943. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Ivanovski, S.; Slevin, M.; Hamlet, S.; Pop, T.S.; Brinzaniuc, K.; Petcu, E.B.; Miroiu, R.I. Bisphosphonate-related osteonecrosis of jaw (BRONJ): Diagnostic criteria and possible pathogenic mechanisms of an unexpected anti-angiogenic side effect. Vasc. Cell 2013, 5, 1. [Google Scholar] [CrossRef]
- Bi, Y.; Gao, Y.; Ehirchiou, D.; Cao, C.; Kikuiri, T.; Le, A.; Shi, S.; Zhang, L. Bisphosphonates cause osteonecrosis of the jaw-like disease in mice. Am. J. Pathol. 2010, 177, 280–290. [Google Scholar] [CrossRef] [PubMed]
- Gkouveris, I.; Hadaya, D.; Soundia, A.; Bezouglaia, O.; Chau, Y.; Dry, S.M.; Pirih, F.Q.; Aghaloo, T.L.; Tetradis, S. Vasculature submucosal changes at early stages of osteonecrosis of the jaw (ONJ). Bone 2019, 123, 234–245. [Google Scholar] [CrossRef]
- Rugani, P.; Walter, C.; Kirnbauer, B.; Acham, S.; Begus-Nahrman, Y.; Jakse, N. Prevalence of medication-related osteonecrosis of the jaw in patients with breast cancer, prostate cancer, and multiple myeloma. Dent. J. 2016, 4, 32. [Google Scholar] [CrossRef]
- Srivastava, A.; Nogueras Gonzalez, G.M.; Geng, Y.; Won, A.M.; Myers, J.; Li, Y.; Chambers, M.S. Medication-related osteonecrosis of the jaw in patients treated concurrently with antiresorptive and antiangiogenic agents: Systematic review and meta-analysis. J. Immunother. Precis Oncol. 2021, 4, 196–207. [Google Scholar] [CrossRef]
- Hoefert, S.; Schmitz, I.; Weichert, F.; Gaspar, M.; Eufinger, H. Macrophages and bisphosphonate-related osteonecrosis of the jaw (BRONJ): Evidence of local immunosuppression of macrophages in contrast to other infectious jaw diseases. Clin. Oral Investig. 2015, 19, 497–508. [Google Scholar] [CrossRef]
- Lombard, T.; Neirinckx, V.; Rogister, B.; Gilon, Y.; Wislet, S. Medication-related osteonecrosis of the jaw: New insights into molecular mechanisms and cellular therapeutic approaches. Stem. Cells Int. 2016, 2016, 8768162. [Google Scholar] [CrossRef]
- Ferneini, E.M. Medication-Related Osteonecrosis of the Jaw (MRONJ). J. Oral Maxillofac. Surg. 2021, 79, 1801–1802. [Google Scholar] [CrossRef]
- Kawahara, M.; Kuroshima, S.; Sawase, T. Clinical considerations for medication-related osteonecrosis of the jaw: A comprehensive literature review. Int. J. Implant Dent. 2021, 7, 47. [Google Scholar] [CrossRef] [PubMed]
- Nicolatou-Galitis, O.; Schiødt, M.; Mendes, R.A.; Ripamonti, C.; Hope, S.; Drudge-Coates, L.; Niepel, D.; van den Wyngaert, T. Medication-related osteonecrosis of the jaw: Definition and best practice for prevention, diagnosis, and treatment. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 117–135. [Google Scholar] [CrossRef] [PubMed]
- De Cicco, D.; Boschetti, C.E.; Santagata, M.; Colella, G.; Staglianò, S.; Gaggl, A.; Bottini, G.B.; Vitagliano, R.; D’Amato, S. Medication-Related Osteonecrosis of the Jaws: A Comparison of SICMF-SIPMO and AAOMS Guidelines. Diagnostics 2023, 13, 2137. [Google Scholar] [CrossRef] [PubMed]
- Bamias, A.; Kastritis, E.; Bamia, C.; Moulopoulos, L.A.; Melakopoulos, I.; Bozas, G.; Koutsoukou, V.; Gika, D.; Anagnostopoulos, A.; Papadimitriou, C.; et al. Osteonecrosis of the jaw in cancer after treatment with bisphosphonates: Incidence and risk factors. J. Clin. Oncol. 2005, 23, 8580–8587. [Google Scholar] [CrossRef]
- Kyrgidis, A.; Vahtsevanos, K.; Koloutsos, G.; Andreadis, C.; Boukovinas, I.; Teleioudis, Z.; Patrikidou, A.; Triaridis, S. Biphosphonate related osteonecrosis of the jaws: Risk factors in breast cancer patients. A case control study. J. Clin. Oncol. 2008, 26, 4634–4638. [Google Scholar] [CrossRef]
- Assael, L.A. Oral bisphosphonates as a cause of bisphosphonate-related osteonecrosis of the jaws: Clinical findings, assessment of risks, and preventive strategies. J. Oral Maxillofac. Surg. 2009, 67, 35–43. [Google Scholar] [CrossRef]
- Marx, R.E.; Sawatari, Y.; Fortin, M.; Broumand, V. Bisphosphonate-induced exposed bone (osteonecrosis/osteopetrosis) of the jaws: Risk factors, recognition, prevention, and treatment. J. Oral Maxillofac. Surg. 2005, 63, 1567–1575. [Google Scholar] [CrossRef]
- Ruggiero, S.L.; Dodson, T.B.; Assael, L.A.; Landesberg, R.; Marx, R.E.; Mehrotra, B. American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws—2009 update. J. Oral Maxillofac. Surg. 2009, 67, 2–12. [Google Scholar]
- Vahtsevanos, K.; Kyrgidis, A.; Verrou, E.; Katodritou, E.; Triaridis, S.; Andreadis, C.G.; Boukovinas, I.; Koloutsos, G.E.; Teleioudis, Z.; Kitikidou, K.; et al. Longitudinal Cohort Study of Risk Factors in Cancer Patients of Bisphosphonate-Related Osteonecrosis of the Jaw. J. Clin. Oncol. 2009, 27, 5356–5362. [Google Scholar] [CrossRef]
- Schwartz, H.C. Osteonecrosis of the jaws: A complication of cancer chemotherapy. Head Neck Surg. 1982, 4, 251–253. [Google Scholar] [CrossRef]
- Hoff, A.O.; Toth, B.; Hu, M.; Hortobagyi, G.N.; Gagel, R.F. Epidemiology and risk factors for osteonecrosis of the jaw in cancer patients. Ann. N. Y. Acad. Sci. 2011, 1218, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Dodson, T.B. Intravenous bisphosphonate therapy and bisphosphonate-related osteonecrosis of the jaws. J. Oral Maxillofac. Surg. 2009, 67, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Otto, S.; Schreyer, C.; Hafner, S.; Mast, G.; Ehrenfeld, M.; Stürzenbaum, S.; Pautke, C. Bisphosphonate-related osteonecrosis of the jaws—Characteristics, risk factors, clinical features, localization and impact on oncological treatment. J. Cranio-Maxillofac. Surg. 2012, 40, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Fantasia, J.; Carlson, E. Bisphosphonate-related osteonecrosis of the jaw: Background and guidelines for diagnosis, staging and management. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 102, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Campisi, G.; Mauceri, R.; Bertoldo, F.; Bettini, G.; Biasotto, M.; Colella, G.; Consolo, U.; di Fede, O.; Favia, G.; Fusco, V.; et al. Medication-related osteonecrosis of jaws (MRONJ) prevention and diagnosis: Italian consensus update 2020. Int. J. Environ. Res. Public Health 2020, 17, 5998. [Google Scholar] [CrossRef]
- Grewal, V.S.; Fayans, E.P. Bisphosphonate-associated osteonecrosis: A clinician’s reference to patient management. Todays FDA 2008, 20, 38–41, 43–46. [Google Scholar]
- Albrektsson, T.; Brånemark, P.I.; Hansson, H.A.; Lindström, J. Osseointegrated titanium implants: Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef]
- Baqain, Z.H.; Moqbel, W.Y.; Sawair, F.A. Early dental implant failure: Risk factors. Br. J. Oral Maxillofac. Surg. 2012, 50, 239–243. [Google Scholar] [CrossRef]
- Fiorillo, L.; Cicciù, M.; Tözüm, T.F.; D’Amico, C.; Oteri, G.; Cervino, G. Impact of bisphosphonate drugs on dental implant healing and peri-implant hard and soft tissues: A systematic review. BMC Oral Health 2022, 22, 291. [Google Scholar] [CrossRef]
- Najeeb, S.; Zafar, M.S.; Khurshid, Z.; Zohaib, S.; Hasan, S.M.; Khan, R.S. Bisphosphonate releasing dental implant surface coatings and osseointegration: A systematic review. J. Taibah Univ. Med. Sci. 2017, 12, 369–375. [Google Scholar] [CrossRef]
- Jobke, B.; Milovanovic, P.; Amling, M.; Busse, B. Bisphosphonate-osteoclasts: Changes in osteoclast morphology and function induced by antiresorptive nitrogen-containing bisphosphonate treatment in osteoporosis patients. Bone 2014, 59, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Abtahi, J.; Henefalk, G.; Aspenberg, P. Randomised trial of bisphosphonate-coated dental implants: Radiographic follow-up after five years of loading. Int. J. Oral Maxillofac. Surg. 2016, 45, 1564–1569. [Google Scholar] [CrossRef] [PubMed]
- Madrid, C.; Sanz, M. What impact do systemically administrated bisphosphonates have on oral implant therapy? A systematic review. Clin. Oral Implants Res. 2009, 20 (Suppl. S4), 87–95. [Google Scholar] [CrossRef] [PubMed]
- Holzinger, D.; Seemann, R.; Matoni, N.; Ewers, R.; Millesi, W.; Wutzl, A. Effect of dental implants on bisphosphonate-related osteonecrosis of the jaws. J. Oral Maxillofac. Surg. 2014, 72, 1937.e1–1938.e8. [Google Scholar] [CrossRef] [PubMed]
- Gelazius, R.; Poskevicius, L.; Sakavicius, D.; Grimuta, V.; Juodzbalys, G. Dental implant placement in patients on bisphosphonate therapy: A systematic review. J. Oral Maxillofac. Res. 2018, 9, e2. [Google Scholar] [CrossRef]
- Bocanegra-Pérez, S.; Vicente-Barrero, M.; Knezevic, M.; Castellano-Navarro, J.M.; Rodríguez-Bocanegra, E.; Rodríguez-Millares, J.; Pérez-Plasencia, D.; Ramos-Macías, A. Use of platelet-rich plasma in the treatment of bisphosphonate-related osteonecrosis of the jaw. Int. J. Oral Maxillofac. Surg. 2012, 41, 1410–1415. [Google Scholar] [CrossRef]
- Curi, M.M.; Cossolin, G.S.I.; Koga, D.H.; Zardetto, C.; Christianini, S.; Feher, O.; Cardoso, C.L.; dos Santos, M.O. Bisphosphonate-related osteonecrosis of the jaws–an initial case series report of treatment combining partial bone resection and autologous platelet-rich plasma. J. Oral Maxillofac. Surg. 2011, 69, 2465–2472. [Google Scholar] [CrossRef]
- Nisi, M.; La Ferla, F.; Karapetsa, D.; Gennai, S.; Ramaglia, L.; Graziani, F.; Gabriele, M. Conservative surgical management of patients with bisphosphonate-related osteonecrosis of the jaws: A series of 120 patients. Br. J. Oral Maxillofac. Surg. 2016, 54, 930–935. [Google Scholar] [CrossRef]
- Imada, M.; Yagyuu, T.; Ueyama, Y.; Maeda, M.; Yamamoto, K.; Kurokawa, S.; Jo, J.I.; Tabata, Y.; Tanaka, Y.; Kirita, T. Prevention of tooth extraction-triggered bisphosphonate-related osteonecrosis of the jaws with basic fibroblast growth factor: An experimental study in rats. PLoS ONE 2019, 14, e0211928. [Google Scholar] [CrossRef]
- Bodem, J.P.; Kargus, S.; Eckstein, S.; Saure, D.; Engel, M.; Hoffmann, J.; Freudlsperger, C. Incidence of bisphosphonate-related osteonecrosis of the jaw in high-risk patients undergoing surgical tooth extraction. J. Craniomaxillofac. Surg. 2015, 43, 510–514. [Google Scholar] [CrossRef]
- Otto, S.; Troltzsch, M.; Jambrovic, V.; Panya, S.; Probst, F.; Ristow, O.; Ehrenfeld, M.; Pautke, C. Tooth extraction in patients receiving oral or intravenous bisphosphonate administration: A trigger for BRONJ development? J. Craniomaxillofac. Surg. 2015, 43, 847–854. [Google Scholar] [CrossRef] [PubMed]
- Soutome, S.; Otsuru, M.; Hayashida, S.; Murata, M.; Yanamoto, S.; Sawada, S.; Kojima, Y.; Funahara, M.; Iwai, H.; Umeda, M.; et al. Relationship between tooth extraction and development of medication-related osteonecrosis of the jaw in cancer patients. Sci. Rep. 2021, 11, 17226. [Google Scholar] [CrossRef] [PubMed]
- Saia, G.; Blandamura, S.; Bettini, G.; Tronchet, A.; Totola, A.; Bedogni, G.; Ferronato, G.; Nocini, P.F.; Bedogni, A. Occurrence of bisphosphonate-related osteonecrosis of the jaw after surgical tooth extraction. J. Oral Maxillofac. Surg. 2010, 68, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Alshaikh, A.; Kim, T.; Kim, S.; Dang, M.; Mehrazarin, S.; Shin, K.H.; Kang, M.; Park, N.H.; Kim, R.H. Preexisting periapical inflammatory condition exacerbates tooth extraction-induced bisphosphonate-related osteonecrosis of the jaw lesions in mice. J. Endod. 2016, 42, 1641–1646. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, T.; Yamori, M.; Ishizaki, T.; Asai, K.; Goto, K.; Takahashi, K.; Nakayama, T.; Bessho, K. Increased incidence of osteonecrosis of the jaw after tooth extraction in patients treated with bisphosphonates: A cohort study. Int. J. Oral Maxillofac. Surg. 2012, 41, 1397–1403. [Google Scholar] [CrossRef]
- Mozzati, M.; Arata, V.; Gallesio, G. Tooth extraction in patients on zoledronic acid therapy. Oral Oncol. 2012, 48, 817–821. [Google Scholar] [CrossRef]
- Ribeiro, N.R.; Silva Lde, F.; Santana, D.M.; Nogueira, R.L. Bisphosphonate-related osteonecrosis of the jaw after tooth extraction. J. Craniofac. Surg. 2015, 26, e606–e608. [Google Scholar] [CrossRef]
- Narayanan, L.L.; Vaishnavi, C. Endodontic microbiology. J. Conserv. Dent. 2010, 13, 233–239. [Google Scholar] [CrossRef]
- AlRahabi, M.K.; Ghabbani, H.M. Clinical impact of bisphosphonates in root canal therapy. Saudi Med. J. 2018, 39, 232–238. [Google Scholar] [CrossRef]
- Xu, R.; Guo, D.; Zhou, X.; Sun, J.; Zhou, Y.; Fan, Y.; Zhou, X.; Wan, M.; Du, W.; Zheng, L. Disturbed bone remodelling activity varies in different stages of experimental, gradually progressive apical periodontitis in rats. Int. J. Oral Sci. 2019, 11, 27. [Google Scholar] [CrossRef]
- Zamparini, F.; Pelliccioni, G.A.; Spinelli, A.; Gissi, D.B.; Gandolfi, M.G.; Prati, C. Root canal treatment of compromised teeth as alternative treatment for patients receiving bisphosphonates: 60-month results of a prospective clinical study. Int. Endod. J. 2021, 54, 156–171. [Google Scholar] [CrossRef] [PubMed]
- Pirani, C.; Friedman, S.; Gatto, M.R.; Iacono, F.; Tinarelli, V.; Gandolfi, M.G.; Prati, C. Survival and periapical health after root canal treatment with carrier-based root fillings: Five-year retrospective assessment. Int. Endod. J. 2018, 51, e178–e188. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, A.; Glickman, G.; He, J. A Retrospective Clinical and Radiographic Study on Healing of Periradicular Lesions in Patients Taking Oral Bisphosphonates. J. Endod. 2009, 35, 1525–1528. [Google Scholar] [CrossRef] [PubMed]
- Dereci, Ö.; Orhan, E.O.; Irmak, Ö.; Ay, S. The effect of the duration of intravenous zolendronate medication on the success of non-surgical endodontic therapy: A retrospective study. BMC Oral Health 2016, 16, 9. [Google Scholar] [CrossRef]
- Muniz, F.; Silva, B.F.D.; Goulart, C.R.; Silveira, T.M.D.; Martins, T.M. Effect of adjuvant bisphosphonates on treatment of periodontitis: Systematic review with meta-analyses. J. Oral Biol. Craniofac. Res. 2021, 11, 158–168. [Google Scholar] [CrossRef]
- Mehrotra, N.; Singh, S. Periodontitis. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2023. [Google Scholar]
- Akram, Z.; Abduljabbar, T.; Kellesarian, S.V.; Abu Hassan, M.I.; Javed, F.; Vohra, F. Efficacy of bisphosphonate as an adjunct to nonsurgical periodontal therapy in the management of periodontal disease: A systematic review. Br. J. Clin. Pharmacol. 2017, 83, 444–454. [Google Scholar] [CrossRef]
- Badran, Z.; Kraehenmann, M.A.; Guicheux, J.; Soueidan, A. Bisphosphonates in periodontal treatment: A review. Oral Health Prev. Dent. 2009, 7, 3–12. [Google Scholar]
- Chen, J.A.-O.; Chen, Q.A.-O.; Hu, B.A.-O.; Wang, Y.A.-O.; Song, J.A.-O. Effectiveness of alendronate as an adjunct to scaling and root planing in the treatment of periodontitis: A meta-analysis of randomized controlled clinical trials. J. Periodontal Implant. Sci. 2016, 46, 382–395. [Google Scholar] [CrossRef]
- Li, C.L.; Lu, W.W.; Seneviratne, C.J.; Leung, W.K.; Zwahlen, R.A.; Zheng, L.W. Role of periodontal disease in bisphosphonate-related osteonecrosis of the jaws in ovariectomized rats. Clin. Oral Implant. Res. 2016, 27, 1–6. [Google Scholar] [CrossRef]
- Dutra, B.C.; Oliveira, A.; Oliveira, P.A.D.; Manzi, F.R.; Cortelli, S.C.; Cota, L.O.M.; Costa, F.O. Effect of 1% sodium alendronate in the non-surgical treatment of periodontal intraosseous defects: A 6-month clinical trial. J. Appl. Oral Sci. 2017, 25, 310–317. [Google Scholar] [CrossRef]
- Gupta, A.; Govila, V.; Pant, V.A.; Gupta, R.; Verma, U.P.; Ahmad, H.; Mohan, S. A randomized controlled clinical trial evaluating the efficacy of zoledronate gel as a local drug delivery system in the treatment of chronic periodontitis: A clinical and radiological correlation. Natl. J. Maxillofac. Surg. 2018, 9, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Thumbigere-Math, V.; Michalowicz, B.S.; Hodges, J.S.; Tsai, M.L.; Swenson, K.K.; Rockwell, L.; Gopalakrishnan, R. Periodontal disease as a risk factor for bisphosphonate-related osteonecrosis of the jaw. J. Periodontol. 2014, 85, 226–233. [Google Scholar] [CrossRef] [PubMed]
- Badros, A.; Weikel, D.; Salama, A.; Goloubeva, O.; Schneider, A.; Rapoport, A.; Fenton, R.; Gahres, N.; Sausville, E.; Ord, R.; et al. Osteonecrosis of the Jaw in Multiple Myeloma Patients: Clinical Features and Risk Factors. J. Clin. Oncol. 2006, 24, 945–952. [Google Scholar] [CrossRef] [PubMed]
- Sedghizadeh, P.P.; Kumar, S.K.S.; Gorur, A.; Schaudinn, C.; Shuler, C.F.; Costerton, J.W. Identification of Microbial Biofilms in Osteonecrosis of the Jaws Secondary to Bisphosphonate Therapy. J. Oral Maxillofac. Surg. 2008, 66, 767–775. [Google Scholar] [CrossRef]
- Göllner, M.; Holst, S.; Fenner, M.; Schmitt, J. Prosthodontic treatment of a patient with bisphosphonate-induced osteonecrosis of the jaw using a removable dental prosthesis with a heat-polymerized resilient liner: A clinical report. J. Prosthet. Dent. 2010, 103, 196–201. [Google Scholar] [CrossRef]
- Kizub, D.A.; Miao, J.; Schubert, M.M.; Paterson, A.H.G.; Clemons, M.; Dees, E.C.; Ingle, J.N.; Falkson, C.I.; Barlow, W.E.; Hortobagyi, G.N.; et al. Risk factors for bisphosphonate-associated osteonecrosis of the jaw in the prospective randomized trial of adjuvant bisphosphonates for early-stage breast cancer (SWOG 0307). Support Care Cancer 2021, 29, 2509–2517. [Google Scholar] [CrossRef]
- Kalra, S.; Jain, V. Dental complications and management of patients on bisphosphonate therapy: A review article. J. Oral Biol. Craniofac. Res. 2013, 3, 25–30. [Google Scholar] [CrossRef]
- Ali, I.E.; Sumita, Y. Medication-related osteonecrosis of the jaw: Prosthodontic considerations. Jpn. Dent. Sci. Rev. 2022, 58, 9–12. [Google Scholar] [CrossRef]
- Kim, H.W.; Lee, M.W.; Lee, J.H.; Kim, M.Y. Comparison of the Effect of Oral Versus Intravenous Bisphosphonate Administration on Osteoclastogenesis in Advanced-Stage Medication-Related Osteonecrosis of the Jaw Patients. J. Clin. Med. 2021, 10, 2988. [Google Scholar] [CrossRef]
- Kishimoto, H.; Noguchi, K.; Takaoka, K. Novel insight into the management of bisphosphonate-related osteonecrosis of the jaw (BRONJ). Jpn. Dent. Sci. Rev. 2019, 55, 95–102. [Google Scholar] [CrossRef]
- Soma, T.; Iwasaki, R.; Sato, Y.; Kobayashi, T.; Nakamura, S.; Kaneko, Y.; Ito, E.; Okada, H.; Watanabe, H.; Miyamoto, K.; et al. Tooth extraction in mice administered zoledronate increases inflammatory cytokine levels and promotes osteonecrosis of the jaw. J. Bone Miner. Metab. 2021, 39, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, M.A.; Kastritis, E.; Bamia, C.; Melakopoulos, I.; Gika, D.; Roussou, M.; Migkou, M.; Eleftherakis-Papaiakovou, E.; Christoulas, D.; Terpos, E.; et al. Reduction of osteonecrosis of the jaw (ONJ) after implementation of preventive measures in patients with multiple myeloma treated with zoledronic acid. Ann. Oncol. 2009, 20, 117–120. [Google Scholar] [CrossRef] [PubMed]
- Ripamonti, C.I.; Maniezzo, M.; Campa, T.; Fagnoni, E.; Brunelli, C.; Saibene, G.; Bareggi, C.; Ascani, L.; Cislaghi, E. Decreased occurrence of osteonecrosis of the jaw after implementation of dental preventive measures in solid tumour patients with bone metastases treated with bisphosphonates. The experience of the National Cancer Institute of Milan. Ann. Oncol. 2009, 20, 137–145. [Google Scholar] [CrossRef]
- Montefusco, V.; Gay, F.; Spina, F.; Miceli, R.; Maniezzo, M.; Teresa Ambrosini, M.; Farina, L.; Piva, S.; Palumbo, A.; Boccadoro, M.; et al. Antibiotic prophylaxis before dental procedures may reduce the incidence of osteonecrosis of the jaw in patients with multiple myeloma treated with bisphosphonates. Leuk. Lymphoma 2008, 49, 2156–2162. [Google Scholar] [CrossRef]
- Bermúdez-Bejarano, E.B.; Serrera-Figallo, M.; Gutiérrez-Corrales, A.; Romero-Ruiz, M.M.; Castillo-de-Oyagüe, R.; Gutiérrez-Pérez, J.L.; Torres-Lagares, D. Prophylaxis and antibiotic therapy in management protocols of patients treated with oral and intravenous bisphosphonates. J. Clin. Exp. Dent. 2017, 9, e141–e149. [Google Scholar] [PubMed]
- Oberoi, S.S.; Dhingra, C.; Sharma, G.; Sardana, D. Antibiotics in dental practice: How justified are we. Int. Dent. J. 2015, 65, 4–10. [Google Scholar] [CrossRef] [PubMed]
- Campisi, G.; di Fede, O.; Musciotto, A.; Lo Casto, A.; Lo Muzio, L.; Fulfaro, F.; Badalamenti, G.; Russo, A.; Gebbia, N. Bisphosphonate-related osteonecrosis of the jaw (BRONJ): Run dental management designs and issues in diagnosis. Ann. Oncol. 2007, 18 (Suppl. S6), vi168–vi172. [Google Scholar] [CrossRef]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).