
Development and Assessment of Nomogram Based on AFP Response for Patients with Unresectable Hepatocellular Carcinoma Treated with Immune Checkpoint Inhibitors


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Treatment Strategy for HCC
2.3. Follow-up
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
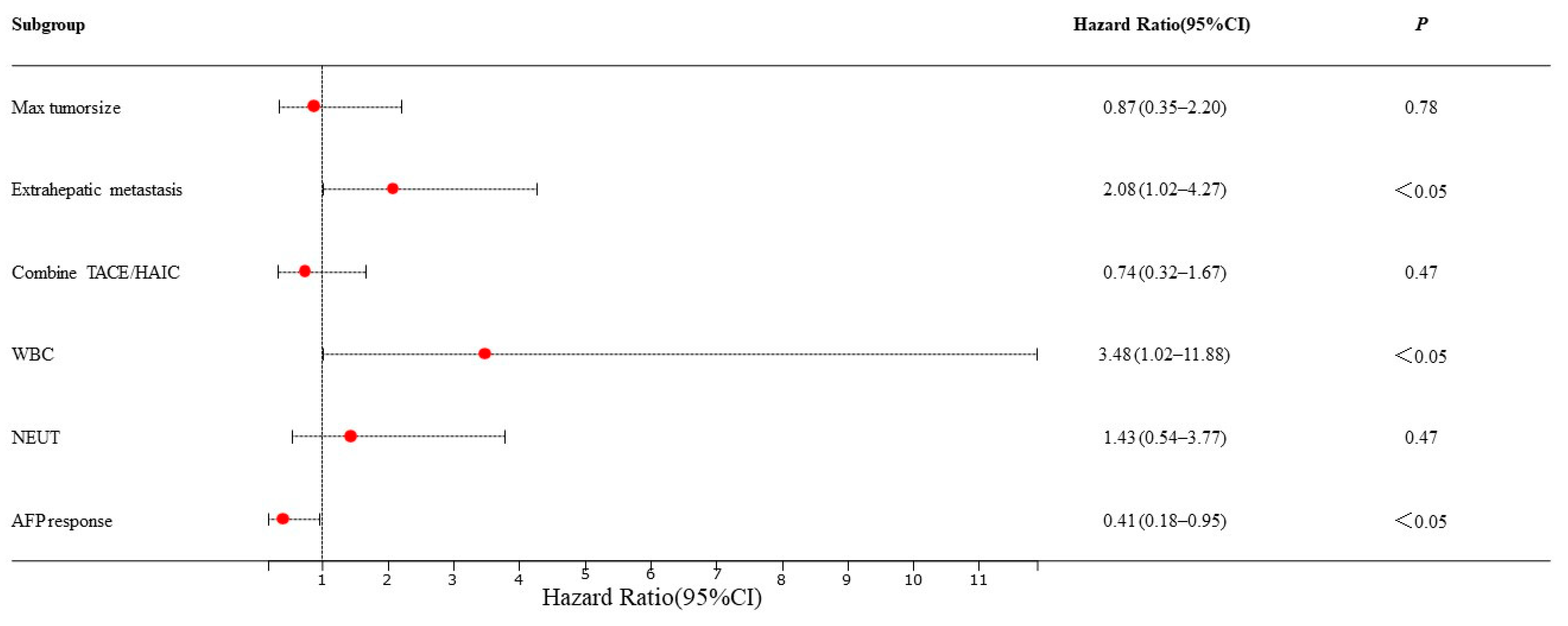
3.2. Independent Predictors of PFS and Predictive Nomogram Construction (Training Set)
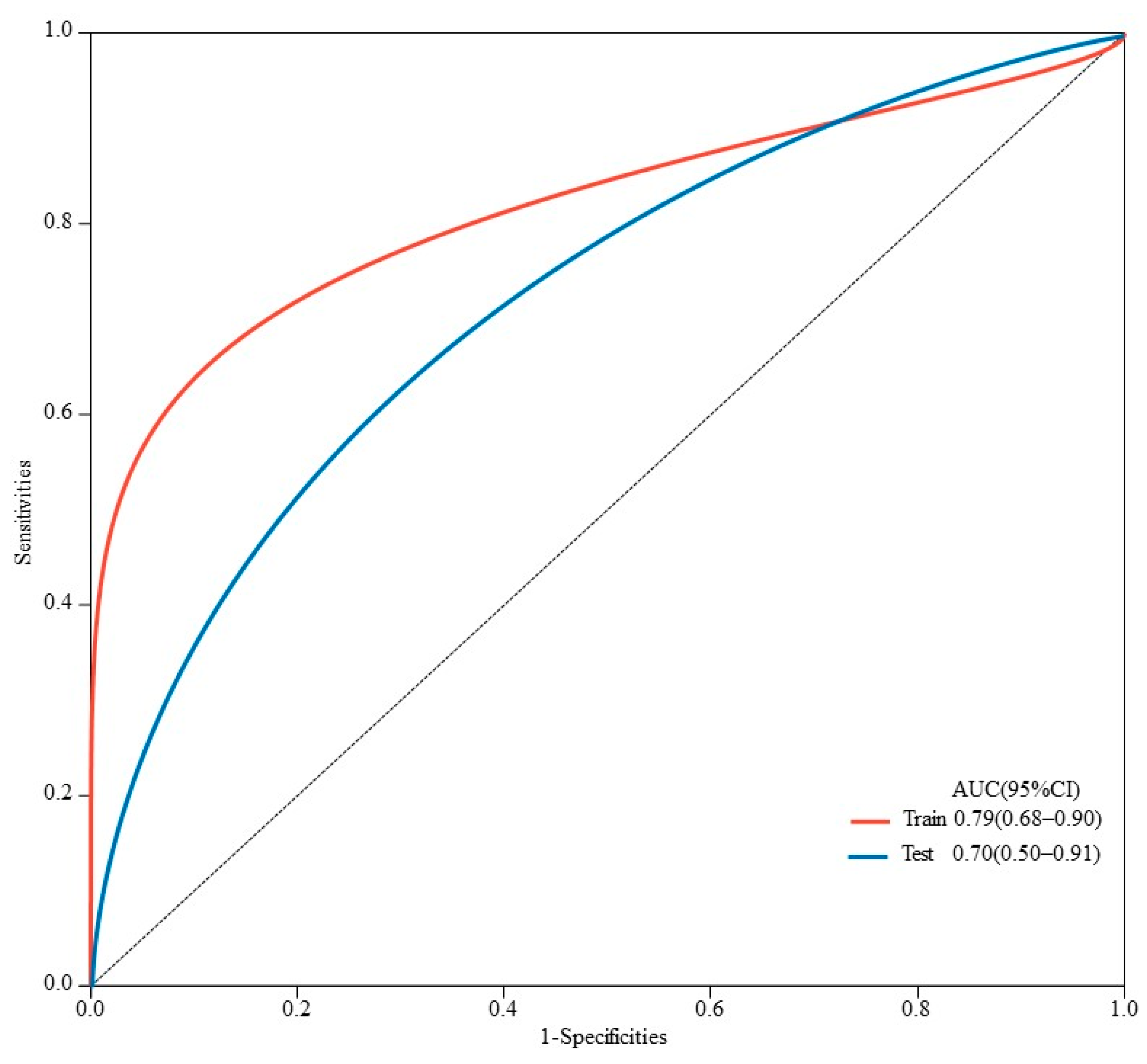
3.3. Model Performance and Validation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC strategy for prognosis prediction and treatment recommendation: The 2022 update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Zhu, A.X. Systemic therapy of advanced hepatocellular carcinoma: How hopeful should we be? Oncologist 2006, 11, 790–800. [Google Scholar] [CrossRef]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.F.; de Oliveira, A.C.; Santoro, A.; Raoul, J.L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [PubMed]
- Pinter, M.; Peck-Radosavljevic, M. Review article: Systemic treatment of hepatocellular carcinoma. Aliment. Pharmacol. Ther. 2018, 48, 598–609. [Google Scholar] [CrossRef] [PubMed]
- Pinter, M.; Jain, R.K.; Duda, D.G. The Current Landscape of Immune Checkpoint Blockade in Hepatocellular Carcinoma: A Review. JAMA Oncol. 2021, 7, 113–123. [Google Scholar] [CrossRef]
- El-Khoueiry, A.B.; Sangro, B.; Yau, T.; Crocenzi, T.S.; Kudo, M.; Hsu, C.; Kim, T.Y.; Choo, S.P.; Trojan, J.; Welling, T.H.R.; et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): An open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet 2017, 389, 2492–2502. [Google Scholar] [CrossRef]
- Chan, S.L.; Wong, N.; Lam, W.K.J.; Kuang, M. Personalized treatment for hepatocellular carcinoma: Current status and future perspectives. J. Gastroenterol. Hepatol. 2022, 37, 1197–1206. [Google Scholar] [CrossRef]
- Cheng, A.L.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.Y.; Lim, H.Y.; Kudo, M.; Breder, V.; Merle, P.; et al. Updated efficacy and safety data from IMbrave150: Atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J. Hepatol. 2022, 76, 862–873. [Google Scholar] [CrossRef]
- Zhu, A.X.; Finn, R.S.; Edeline, J.; Cattan, S.; Ogasawara, S.; Palmer, D.; Verslype, C.; Zagonel, V.; Fartoux, L.; Vogel, A.; et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): A non-randomised, open-label phase 2 trial. Lancet Oncol. 2018, 19, 940–952. [Google Scholar] [CrossRef]
- Ang, C.; Klempner, S.J.; Ali, S.M.; Madison, R.; Ross, J.S.; Severson, E.A.; Fabrizio, D.; Goodman, A.; Kurzrock, R.; Suh, J.; et al. Prevalence of established and emerging biomarkers of immune checkpoint inhibitor response in advanced hepatocellular carcinoma. Oncotarget 2019, 10, 4018–4025. [Google Scholar] [CrossRef]
- Sangro, B.; Melero, I.; Wadhawan, S.; Finn, R.S.; Abou-Alfa, G.K.; Cheng, A.L.; Yau, T.; Furuse, J.; Park, J.W.; Boyd, Z.; et al. Association of inflammatory biomarkers with clinical outcomes in nivolumab-treated patients with advanced hepatocellular carcinoma. J. Hepatol. 2020, 73, 1460–1469. [Google Scholar] [CrossRef]
- Le, D.T.; Uram, J.N.; Wang, H.; Bartlett, B.R.; Kemberling, H.; Eyring, A.D.; Skora, A.D.; Luber, B.S.; Azad, N.S.; Laheru, D.; et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N. Engl. J. Med. 2015, 372, 2509–2520. [Google Scholar] [CrossRef] [PubMed]
- Harding, J.J.; Nandakumar, S.; Armenia, J.; Khalil, D.N.; Albano, M.; Ly, M.; Shia, J.; Hechtman, J.F.; Kundra, R.; El Dika, I.; et al. Prospective Genotyping of Hepatocellular Carcinoma: Clinical Implications of Next-Generation Sequencing for Matching Patients to Targeted and Immune Therapies. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2019, 25, 2116–2126. [Google Scholar] [CrossRef] [PubMed]
- Mitsuhashi, N.; Kobayashi, S.; Doki, T.; Kimura, F.; Shimizu, H.; Yoshidome, H.; Ohtsuka, M.; Kato, A.; Yoshitomi, H.; Nozawa, S.; et al. Clinical significance of alpha-fetoprotein: Involvement in proliferation, angiogenesis, and apoptosis of hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2008, 23, e189–e197. [Google Scholar] [CrossRef] [PubMed]
- Shao, Y.Y.; Liu, T.H.; Hsu, C.; Lu, L.C.; Shen, Y.C.; Lin, Z.Z.; Cheng, A.L.; Hsu, C.H. Early alpha-foetoprotein response associated with treatment efficacy of immune checkpoint inhibitors for advanced hepatocellular carcinoma. Liver Int. Off. J. Int. Assoc. Study Liver 2019, 39, 2184–2189. [Google Scholar] [CrossRef]
- Hsu, W.F.; Chuang, P.H.; Chen, C.K.; Wang, H.W.; Tsai, M.H.; Su, W.P.; Chen, H.Y.; Yang, C.Y.; Lin, C.C.; Huang, G.T.; et al. Predictors of response and survival in patients with unresectable hepatocellular carcinoma treated with nivolumab: Real-world experience. Am. J. Cancer Res. 2020, 10, 4547–4560. [Google Scholar]
- Lee, P.C.; Chao, Y.; Chen, M.H.; Lan, K.H.; Lee, C.J.; Lee, I.C.; Chen, S.C.; Hou, M.C.; Huang, Y.H. Predictors of Response and Survival in Immune Checkpoint Inhibitor-Treated Unresectable Hepatocellular Carcinoma. Cancers 2020, 12, 182. [Google Scholar] [CrossRef]
- Tian, B.W.; Yan, L.J.; Ding, Z.N.; Liu, H.; Meng, G.X.; Xue, J.S.; Han, C.L.; Dong, Z.R.; Hong, J.G.; Chen, Z.Q.; et al. Early alpha-fetoprotein response predicts prognosis of immune checkpoint inhibitor and targeted therapy for hepatocellular carcinoma: A systematic review with meta-analysis. Expert Rev. Gastroenterol. Hepatol. 2023, 17, 73–83. [Google Scholar] [CrossRef]
- EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.I.; Lim, J.; Shim, J.H. Role of the alpha-fetoprotein response in immune checkpoint inhibitor-based treatment of patients with hepatocellular carcinoma. J. Cancer Res. Clin. Oncol. 2021, 148, 2069–2077. [Google Scholar] [CrossRef] [PubMed]
- Pinato, D.J.; Mauri, F.A.; Spina, P.; Cain, O.; Siddique, A.; Goldin, R.; Victor, S.; Pizio, C.; Akarca, A.U.; Boldorini, R.L.; et al. Clinical implications of heterogeneity in PD-L1 immunohistochemical detection in hepatocellular carcinoma: The Blueprint-HCC study. Br. J. Cancer 2019, 120, 1033–1036. [Google Scholar] [CrossRef]
- Topalian, S.L.; Taube, J.M.; Anders, R.A.; Pardoll, D.M. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat. Rev. Cancer 2016, 16, 275–287. [Google Scholar] [CrossRef]
- Hansen, A.R.; Siu, L.L. PD-L1 Testing in Cancer: Challenges in Companion Diagnostic Development. JAMA Oncol. 2016, 2, 15–16. [Google Scholar] [CrossRef]
- Galle, P.R.; Foerster, F.; Kudo, M.; Chan, S.L.; Llovet, J.M.; Qin, S.; Schelman, W.R.; Chintharlapalli, S.; Abada, P.B.; Sherman, M.; et al. Biology and significance of alpha-fetoprotein in hepatocellular carcinoma. Liver Int. Off. J. Int. Assoc. Study Liver 2019, 39, 2214–2229. [Google Scholar] [CrossRef]
- Zhu, A.X.; Kang, Y.K.; Yen, C.J.; Finn, R.S.; Galle, P.R.; Llovet, J.M.; Assenat, E.; Brandi, G.; Pracht, M.; Lim, H.Y.; et al. Ramucirumab after sorafenib in patients with advanced hepatocellular carcinoma and increased α-fetoprotein concentrations (REACH-2): A randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019, 20, 282–296. [Google Scholar] [CrossRef]
- Peng, S.Y.; Chen, W.J.; Lai, P.L.; Jeng, Y.M.; Sheu, J.C.; Hsu, H.C. High alpha-fetoprotein level correlates with high stage, early recurrence and poor prognosis of hepatocellular carcinoma: Significance of hepatitis virus infection, age, p53 and beta-catenin mutations. Int. J. Cancer 2004, 112, 44–50. [Google Scholar] [CrossRef]
- Terentiev, A.A.; Moldogazieva, N.T. Alpha-fetoprotein: A renaissance. Tumour Biol. J. Int. Soc. Oncodev. Biol. Med. 2013, 34, 2075–2091. [Google Scholar] [CrossRef]
- Shan, Y.F.; Huang, Y.L.; Xie, Y.K.; Tan, Y.H.; Chen, B.C.; Zhou, M.T.; Shi, H.Q.; Yu, Z.P.; Song, Q.T.; Zhang, Q.Y. Angiogenesis and clinicopathologic characteristics in different hepatocellular carcinoma subtypes defined by EpCAM and α-fetoprotein expression status. Med. Oncol. 2011, 28, 1012–1016. [Google Scholar] [CrossRef] [PubMed]
- Fukumura, D.; Kloepper, J.; Amoozgar, Z.; Duda, D.G.; Jain, R.K. Enhancing cancer immunotherapy using antiangiogenics: Opportunities and challenges. Nat. Rev. Clin. Oncol. 2018, 15, 325–340. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Sun, W.; Ding, X.; Li, W.; Chen, J. Prognostic model of immune checkpoint inhibitors combined with anti-angiogenic agents in unresectable hepatocellular carcinoma. Front. Immunol. 2022, 13, 1060051. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.C.; Hsu, C.; Shao, Y.Y.; Chao, Y.; Yen, C.J.; Shih, I.L.; Hung, Y.P.; Chang, C.J.; Shen, Y.C.; Guo, J.C.; et al. Differential Organ-Specific Tumor Response to Immune Checkpoint Inhibitors in Hepatocellular Carcinoma. Liver Cancer 2019, 8, 480–490. [Google Scholar] [CrossRef]
- Scheiner, B.; Pomej, K.; Kirstein, M.M.; Hucke, F.; Finkelmeier, F.; Waidmann, O.; Himmelsbach, V.; Schulze, K.; von Felden, J.; Fründt, T.W.; et al. Prognosis of patients with hepatocellular carcinoma treated with immunotherapy—Development and validation of the CRAFITY score. J. Hepatol. 2022, 76, 353–363. [Google Scholar] [CrossRef]
- Dharmapuri, S.; Özbek, U.; Lin, J.Y.; Sung, M.; Schwartz, M.; Branch, A.D.; Ang, C. Predictive value of neutrophil to lymphocyte ratio and platelet to lymphocyte ratio in advanced hepatocellular carcinoma patients treated with anti-PD-1 therapy. Cancer Med. 2020, 9, 4962–4970. [Google Scholar] [CrossRef]
- Zhang, Y.; Lu, L.; He, Z.; Xu, Z.; Xiang, Z.; Nie, R.C.; Lin, W.; Chen, W.; Zhou, J.; Yin, Y.; et al. C-Reactive Protein Levels Predict Responses to PD-1 Inhibitors in Hepatocellular Carcinoma Patients. Front. Immunol. 2022, 13, 808101. [Google Scholar] [CrossRef]
- Guthrie, G.J.; Charles, K.A.; Roxburgh, C.S.; Horgan, P.G.; McMillan, D.C.; Clarke, S.J. The systemic inflammation-based neutrophil-lymphocyte ratio: Experience in patients with cancer. Crit. Rev. Oncol. Hematol. 2013, 88, 218–230. [Google Scholar] [CrossRef]
- Michael, M.; Goldstein, D.; Clarke, S.J.; Milner, A.D.; Beale, P.; Friedlander, M.; Mitchell, P. Prognostic factors predictive of response and survival to a modified FOLFOX regimen: Importance of an increased neutrophil count. Clin. Color. Cancer 2006, 6, 297–304. [Google Scholar] [CrossRef]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef]
- Diakos, C.I.; Charles, K.A.; McMillan, D.C.; Clarke, S.J. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014, 15, e493–e503. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.L.; Fulgenzi, C.A.M.; D’Alessio, A.; Cheon, J.; Nishida, N.; Saeed, A.; Wietharn, B.; Cammarota, A.; Pressiani, T.; Personeni, N.; et al. Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios as Prognostic Biomarkers in Unresectable Hepatocellular Carcinoma Treated with Atezolizumab plus Bevacizumab. Cancers 2022, 14, 5834. [Google Scholar] [CrossRef]
- Hsu, W.F.; Lai, H.C.; Chen, C.K.; Wang, H.W.; Chuang, P.H.; Tsai, M.H.; Chen, S.H.; Chu, C.S.; Su, W.P.; Chou, J.W.; et al. Combined CRAFITY score and α-fetoprotein response predicts treatment outcomes in patients with unresectable hepatocellular carcinoma receiving anti-programmed death-1 blockade-based immunotherapy. Am. J. Cancer Res. 2023, 13, 654–668. [Google Scholar] [PubMed]
- Chen, Q.; Deng, Y.; Zhao, C.; Huang, Z.; Zhang, W.; Yang, Y.; Bai, Y.; Tu, J.; Li, B.; Wu, W.; et al. Nomogram for tumour response based on prospective cohorts of hepatocellular carcinoma patients receiving immunotherapy combined with targeted therapy: Development and validation. Ann. Transl. Med. 2023, 11, 199. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.; Liu, M.; Zhai, X.; Li, X.; Jin, B.; Liu, Y. Development and validation of prognostic risk prediction models for hepatocellular carcinoma patients treated with immune checkpoint inhibitors based on a systematic review and meta-analysis of 47 cohorts. Front. Immunol. 2023, 14, 1215745. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Feng, J.; Kuang, T.; Chai, D.; Qiu, Z.; Deng, W.; Dong, K.; Zhao, K.; Wang, W. Blood biomarkers predict outcomes in patients with hepatocellular carcinoma treated with immune checkpoint Inhibitors: A pooled analysis of 44 retrospective sudies. Int. Immunopharmacol. 2023, 118, 110019. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Training Set (n = 84) | Validation Set (n = 36) | p-Value |
|---|---|---|---|
| Gender | |||
| Male | 75 (89.29) | 35 (97.22) | 0.15 |
| Female | 9 (10.71) | 1 (2.78) | |
| Age (year) | |||
| <60 | 63 (75.00) | 25 (69.44) | 0.53 |
| ≥60 | 21 (25.00) | 11 (30.56) | |
| HBV | |||
| Negative | 2 (2.38) | 2 (5.56) | 0.38 |
| Positive | 82 (97.62) | 34 (94.44) | |
| Tumor number | |||
| <3 | 29 (34.52) | 4 (11.11) | 0.01 |
| ≥3 | 55 (65.48) | 32 (88.89) | |
| Max tumor size | |||
| <5 cm | 35 (41.67) | 9 (25.00) | 0.08 |
| ≥5 cm | 49 (58.33) | 27 (75.00) | |
| Portal vein invasion | |||
| Negative | 44 (52.38) | 15 (41.67) | 0.28 |
| Positive | 40 (47.62) | 21 (58.33) | |
| Extrahepatic metastasis | |||
| Negative | 34 (40.48) | 15 (41.67) | 0.90 |
| Positive | 50 (59.52) | 21 (58.33) | |
| Child-Pugh class | |||
| A | 66 (78.57) | 29 (80.56) | 0.81 |
| B | 18 (21.43) | 7 (19.44) | |
| BCLC stage | |||
| II | 11 (13.10) | 8 (22.22) | 0.21 |
| III | 73 (86.90) | 28 (77.78) | |
| Combine TACE/HAIC | |||
| No | 20 (23.81) | 4 (11.11) | 0.11 |
| Yes | 64 (76.19) | 32 (88.89) | |
| PLT | |||
| <100 × 109/L | 11 (13.10) | 5 (13.89) | 0.91 |
| ≥100 × 109/L | 73 (86.90) | 31 (86.11) | |
| ALB | |||
| <35 g/L | 30 (35.71) | 11 (30.56) | 0.59 |
| ≥35 g/L | 54 (64.29) | 25 (69.44) | |
| ALT | |||
| <40 U/L | 46 (54.76) | 21 (58.33) | 0.72 |
| ≥40 U/L | 38 (45.24) | 15 (41.67) | |
| TBIL | |||
| <34.2 μmol/L | 80 (95.24) | 33 (91.67) | 0.44 |
| ≥34.2 μmol/L | 4 (4.76) | 3 (8.33) | |
| PT | |||
| <14 s | 75 (89.29) | 33 (91.67) | 0.69 |
| ≥14 s | 9 (10.71) | 3 (8.33) | |
| WBC | |||
| <10 × 109/L | 76 (90.48) | 34 (94.44) | 0.47 |
| ≥10 × 109/L | 8 (9.52) | 2 (5.56) | |
| NEUT | |||
| <6.4 × 109/L | 72 (85.71) | 34 (94.44) | 0.17 |
| ≥6.4 × 109/L | 12 (14.29) | 2 (5.56) | |
| MONO | |||
| <0.5 × 109/L | 42 (50.00) | 21 (58.33) | 0.40 |
| ≥0.5 × 109/L | 42 (50.00) | 15 (41.67) | |
| Baseline AFP | |||
| <400 μg/L | 43 (51.19) | 19 (52.78) | 0.87 |
| ≥400 μg/L | 41 (48.81) | 17 (47.22) | |
| AFP response | |||
| No | 45 (53.57) | 17 (47.22) | 0.52 |
| Yes | 39 (46.43) | 19 (52.78) | |
| NLR | 3.14 (2.41, 4.51) | 2.90 (2.04, 4.13) | 0.14 |
| PLR | 134.65 (96.17, 206.67) | 154.62 (117.42, 199.42) | 0.25 |
| MLR | 0.42 (0.31, 0.60) | 0.41 (0.30, 0.47) | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Shen, H.; Zheng, R.; Sun, Y.; Xie, X.; Lu, M.-D.; Liu, B.; Huang, G. Development and Assessment of Nomogram Based on AFP Response for Patients with Unresectable Hepatocellular Carcinoma Treated with Immune Checkpoint Inhibitors. Cancers 2023, 15, 5131. https://doi.org/10.3390/cancers15215131
Zhang Y, Shen H, Zheng R, Sun Y, Xie X, Lu M-D, Liu B, Huang G. Development and Assessment of Nomogram Based on AFP Response for Patients with Unresectable Hepatocellular Carcinoma Treated with Immune Checkpoint Inhibitors. Cancers. 2023; 15(21):5131. https://doi.org/10.3390/cancers15215131
Chicago/Turabian StyleZhang, Yi, Hui Shen, Ruiying Zheng, Yueting Sun, Xiaoyan Xie, Ming-De Lu, Baoxian Liu, and Guangliang Huang. 2023. "Development and Assessment of Nomogram Based on AFP Response for Patients with Unresectable Hepatocellular Carcinoma Treated with Immune Checkpoint Inhibitors" Cancers 15, no. 21: 5131. https://doi.org/10.3390/cancers15215131
APA StyleZhang, Y., Shen, H., Zheng, R., Sun, Y., Xie, X., Lu, M.-D., Liu, B., & Huang, G. (2023). Development and Assessment of Nomogram Based on AFP Response for Patients with Unresectable Hepatocellular Carcinoma Treated with Immune Checkpoint Inhibitors. Cancers, 15(21), 5131. https://doi.org/10.3390/cancers15215131