
Impact of cfDNA Reference Materials on Clinical Performance of Liquid Biopsy NGS Assays
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Reference Materials
2.3. Patient Samples
2.4. cfDNA Isolation
2.5. Kit Design
2.6. Library Preparation and Sequencing
2.7. Bioinformatics Analysis
2.8. Statistical Analysis
3. Results
3.1. Performance Evaluation of Liquid Biopsy NGS Assays
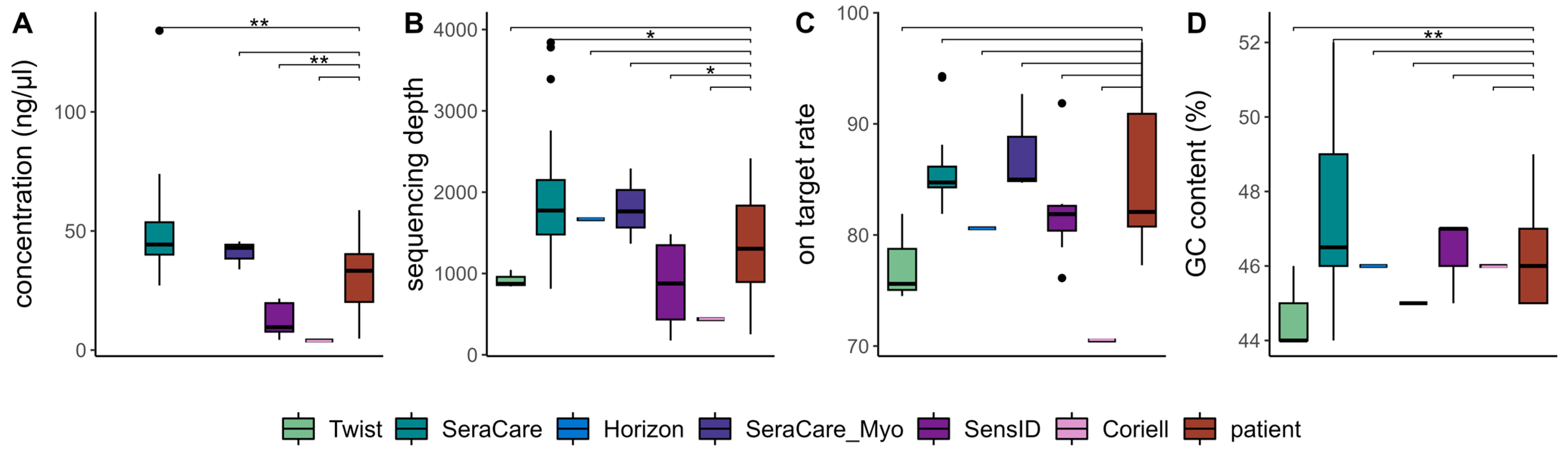
3.2. Quality Metrics of Library Preparation and Sequencing Performance
3.3. Distribution of cfDNA Fragment Length
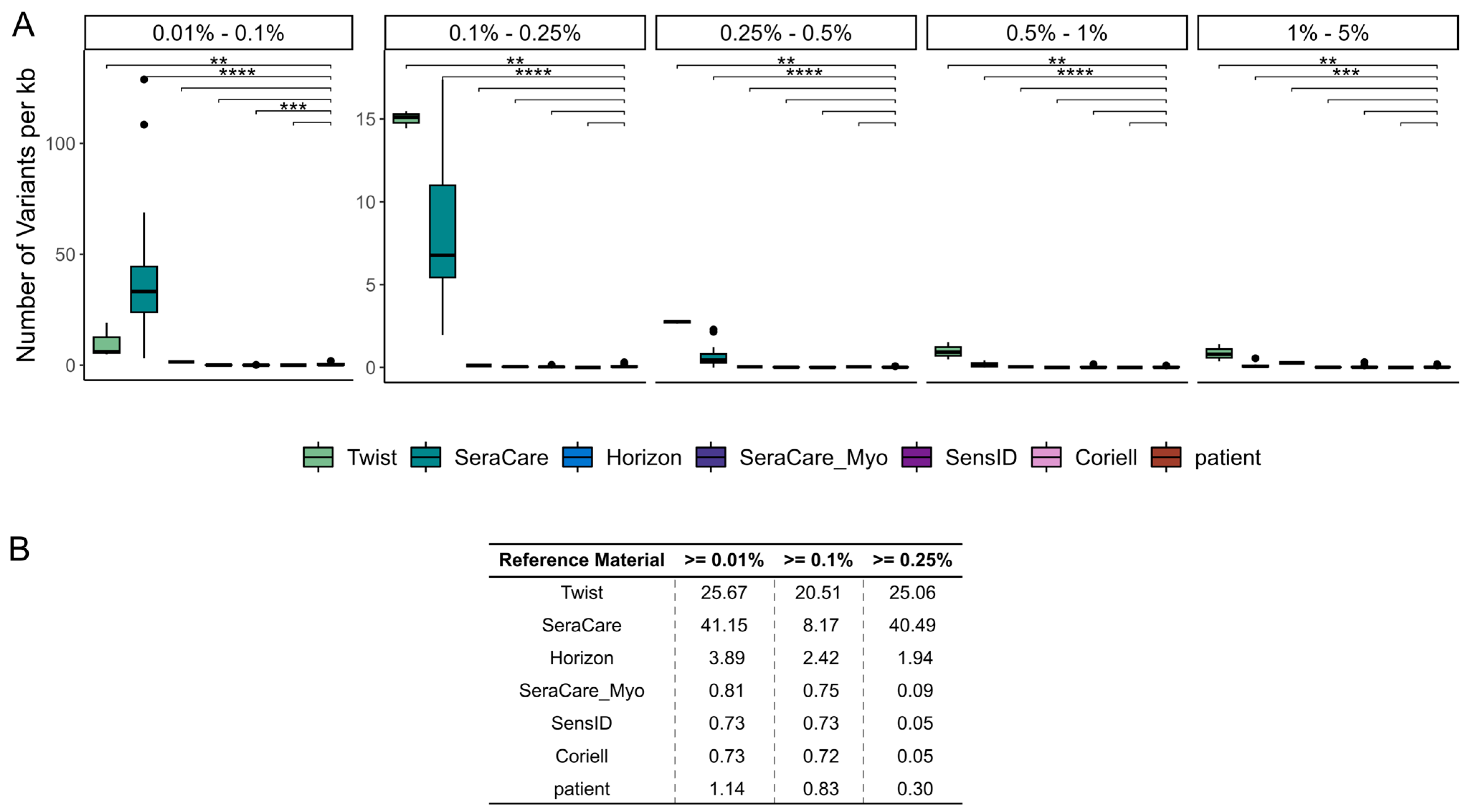
3.4. Variant Detection Rate at Low VAFs
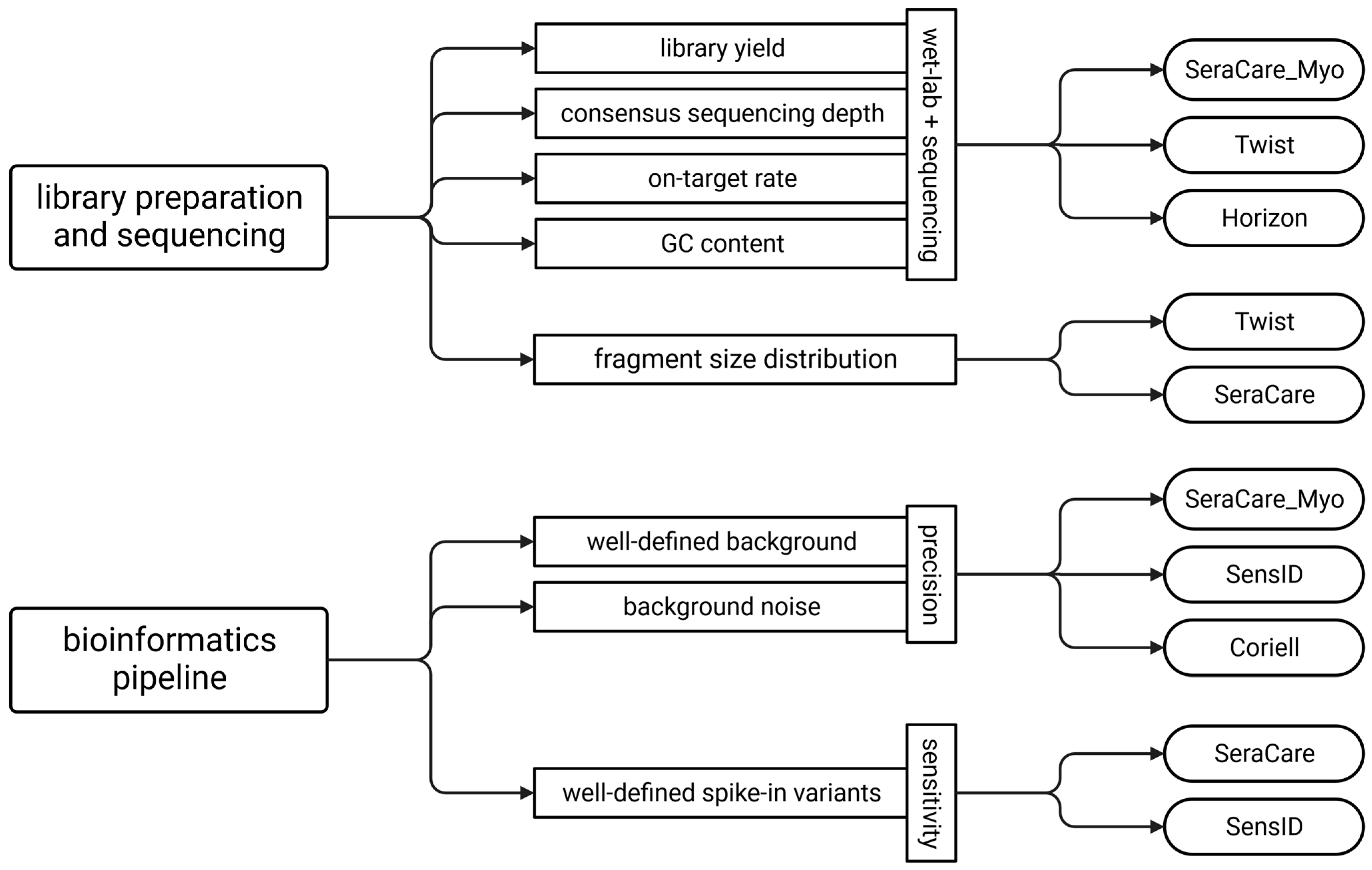
3.5. Guideline for the Selection of Reference Materials
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bożyk, A.; Nicoś, M. The Overview of Perspectives of Clinical Application of Liquid Biopsy in Non-Small-Cell Lung Cancer. Life 2022, 12, 1640. [Google Scholar] [CrossRef] [PubMed]
- Diehl, F.; Li, M.; Dressman, D.; He, Y.; Shen, D.; Szabo, S.; Diaz, L.A.; Goodman, S.N.; David, K.A.; Juhl, H.; et al. Detection and Quantification of Mutations in the Plasma of Patients with Colorectal Tumors. Proc. Natl. Acad. Sci. USA 2005, 102, 16368–16373. [Google Scholar] [CrossRef] [PubMed]
- Pascual, J.; Attard, G.; Bidard, F.-C.; Curigliano, G.; Mattos-Arruda, L.; Diehn, M.; Italiano, A.; Lindberg, J.; Merker, J.D.; Montagut, C.; et al. ESMO Recommendations on the Use of Circulating Tumour DNA Assays for Patients with Cancer: A Report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2022, 33, 750–768. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, F.; Paluch-Shimon, S.; Senkus, E.; Curigliano, G.; Aapro, M.S.; André, F.; Barrios, C.H.; Bergh, J.; Bhattacharyya, G.S.; Biganzoli, L.; et al. 5th ESO-ESMO International Consensus Guidelines for Advanced Breast Cancer (ABC 5). Ann. Oncol. 2020, 31, 1623–1649. [Google Scholar] [CrossRef]
- Mosele, F.; Remon, J.; Mateo, J.; Westphalen, C.B.; Barlesi, F.; Lolkema, M.P.; Normanno, N.; Scarpa, A.; Robson, M.; Meric-Bernstam, F.; et al. Recommendations for the Use of Next-Generation Sequencing (NGS) for Patients with Metastatic Cancers: A Report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2020, 31, 1491–1505. [Google Scholar] [CrossRef]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; van Schil, P.E.; Hellmann, M.D.; et al. Metastatic Non-Small Cell Lung Cancer: ESMO Clinical Practice Guidelines for Diagnosis, Treatment and Follow-Up. Ann. Oncol. 2018, 29, iv192–iv237. [Google Scholar] [CrossRef]
- NCCN. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®); National Comprehensive Cancer Network: Plymouth Meeting, PA, USA, 2021. [Google Scholar]
- Tie, J.; Cohen, J.D.; Lahouel, K.; Lo, S.N.; Wang, Y.; Kosmider, S.; Wong, R.; Shapiro, J.; Lee, M.; Harris, S.; et al. Circulating Tumor DNA Analysis Guiding Adjuvant Therapy in Stage II Colon Cancer. N. Engl. J. Med. 2022, 386, 2261–2272. [Google Scholar] [CrossRef]
- Tie, J.; Cohen, J.D.; Lo, S.N.; Wang, Y.; Li, L.; Christie, M.; Lee, M.; Wong, R.; Kosmider, S.; Skinner, I.; et al. Prognostic Significance of Postsurgery Circulating Tumor DNA in Nonmetastatic Colorectal Cancer: Individual Patient Pooled Analysis of Three Cohort Studies. Int. J. Cancer 2020, 148, 1014–1026. [Google Scholar] [CrossRef]
- Bidard, F.-C.; Hardy-Bessard, A.-C.; Dalenc, F.; Bachelot, T.; Pierga, J.-Y.; de la Motte Rouge, T.; Sabatier, R.; Dubot, C.; Frenel, J.-S.; Ferrero, J.M.; et al. Switch to Fulvestrant and Palbociclib versus No Switch in Advanced Breast Cancer with Rising ESR1 Mutation during Aromatase Inhibitor and Palbociclib Therapy (PADA-1): A Randomised, Open-Label, Multicentre, Phase 3 Trial. Lancet Oncol. 2022, 23, 1367–1377. [Google Scholar] [CrossRef]
- Zaman, F.Y.; Subramaniam, A.; Afroz, A.; Samoon, Z.; Gough, D.; Arulananda, S.; Alamgeer, M. Circulating Tumour DNA (CtDNA) as a Predictor of Clinical Outcome in Non-Small Cell Lung Cancer Undergoing Targeted Therapies: A Systematic Review and Meta-Analysis. Cancers 2023, 15, 2425. [Google Scholar] [CrossRef]
- Hallermayr, A.; Steinke-Lange, V.; Vogelsang, H.; Rentsch, M.; Wit, M.; Haberl, C.; Holinski-Feder, E.; Pickl, J.M.A. Clinical Validity of Circulating Tumor DNA as Prognostic and Predictive Marker for Personalized Colorectal Cancer Patient Management. Cancers 2022, 14, 851. [Google Scholar] [CrossRef] [PubMed]
- Mo, S.; Ye, L.; Wang, D.; Han, L.; Zhou, S.; Wang, H.; Dai, W.; Wang, Y.; Luo, W.; Wang, R.; et al. Early Detection of Molecular Residual Disease and Risk Stratification for Stage I to III Colorectal Cancer via Circulating Tumor DNA Methylation. JAMA Oncol. 2023, 9, 770. [Google Scholar] [CrossRef] [PubMed]
- Hallermayr, A.; Neuhann, T.M.; Steinke-Lange, V.; Scharf, F.; Laner, A.; Ewald, R.; Liesfeld, B.; Holinski-Feder, E.; Pickl, J.M.A. Highly Sensitive Liquid Biopsy Duplex Sequencing Complements Tissue Biopsy to Enhance Detection of Clinically Relevant Genetic Variants. Front. Oncol. 2022, 12, 6734. [Google Scholar] [CrossRef] [PubMed]
- Serio, V.B.; Palmieri, M.; Loberti, L.; Granata, S.; Fallerini, C.; Vaghi, M.; Renieri, A.; Pinto, A.M. Nosological and Theranostic Approach to Vascular Malformation through CfDNA NGS Liquid Biopsy. J. Clin. Med. 2022, 11, 3740. [Google Scholar] [CrossRef] [PubMed]
- Godsey, J.H.; Silvestro, A.; Barrett, J.C.; Bramlett, K.; Chudova, D.; Deras, I.; Dickey, J.; Hicks, J.; Johann, D.J.; Leary, R.; et al. Generic Protocols for the Analytical Validation of Next-Generation Sequencing-Based CtDNA Assays: A Joint Consensus Recommendation of the BloodPAC’s Analytical Variables Working Group. Clin. Chem. 2020, 66, 1156–1166. [Google Scholar] [CrossRef]
- Hallermayr, A.; Benet-Pagès, A.; Steinke-Lange, V.; Mansmann, U.; Rentsch, M.; Holinski-Feder, E.; Pickl, J.M.A. Liquid Biopsy Hotspot Variant Assays: Analytical Validation for Application in Residual Disease Detection and Treatment Monitoring. Clin. Chem. 2021, 67, 1483–1491. [Google Scholar] [CrossRef]
- Ntzifa, A.; Lianidou, E. Pre-Analytical Conditions and Implementation of Quality Control Steps in Liquid Biopsy Analysis. Crit Rev. Clin. Lab. Sci. 2023, 1–22. [Google Scholar] [CrossRef]
- Holdhoff, M.; Schmidt, K.; Donehower, R.; Diaz, L.A. Analysis of Circulating Tumor DNA to Confirm Somatic KRAS Mutations. J. Natl. Cancer Inst. 2009, 101, 1284–1285. [Google Scholar] [CrossRef]
- Diehl, F.; Schmidt, K.; Choti, M.A.; Romans, K.; Goodman, S.; Li, M.; Thornton, K.; Agrawal, N.; Sokoll, L.; Szabo, S.A.; et al. Circulating Mutant DNA to Assess Tumor Dynamics. Nat. Med. 2008, 14, 985–990. [Google Scholar] [CrossRef]
- SeraCare Life Sciences, Inc. SeraseqTM Circulating Tumor DNA-I Reference Materials for Characterizing, Developing and Validating Plasma-Based Assays; Elsevier B.V.: Milford, MA, USA, 2016. [Google Scholar]
- Cherry, P.D. Abstract LB110: Twist Pan-Cancer Synthetic Reference Materials for Cell-Free DNA (CfDNA) Assay Development. Cancer Res. 2022, 82, LB110. [Google Scholar] [CrossRef]
- Schmitt, M.W.; Kennedy, S.R.; Salk, J.J.; Fox, E.J.; Hiatt, J.B.; Loeb, L.A. Detection of Ultra-Rare Mutations by next-Generation Sequencing. Proc. Natl. Acad. Sci. USA 2012, 109, 14508–14513. [Google Scholar] [CrossRef] [PubMed]
- Integrated DNA Technologies. Analysis Guidelines: XGen Prism DNA Library Prep Kit—Processing Sequence Data with Unique Molecular Identifiers (UMIs); Integrated DNA Technologies: Coralville, IA, USA, 2020. [Google Scholar]
- NCCLS. Protocols for Determination of Limits of Detection and Limits of Quantitation Guideline; NCCLS: Wayne, PA, USA, 2004; ISBN 1-56238-551-8. [Google Scholar]
- D’Gama, A.M.; Poduri, A. Brain Somatic Mosaicism in Epilepsy: Bringing Results Back to the Clinic. Neurobiol. Dis. 2023, 181, 106104. [Google Scholar] [CrossRef] [PubMed]
- Bundesärztekammer. Qualitätssicherung Laboratoriumsmedizinischer Untersuchungen—Rili-BÄK; Deutsches Ärzteblatt: Berlin, Germany, 2023. [Google Scholar] [CrossRef]
- Fassunke, J.; Ihle, M.A.; Lenze, D.; Lehmann, A.; Hummel, M.; Vollbrecht, C.; Penzel, R.; Volckmar, A.-L.; Stenzinger, A.; Endris, V.; et al. EGFR T790M Mutation Testing of Non-Small Cell Lung Cancer Tissue and Blood Samples Artificially Spiked with Circulating Cell-Free Tumor DNA: Results of a Round Robin Trial. Virchows Arch. 2017, 471, 509–520. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hallermayr, A.; Keßler, T.; Fujera, M.; Liesfeld, B.; Bernstein, S.; von Ameln, S.; Schanze, D.; Steinke-Lange, V.; Pickl, J.M.A.; Neuhann, T.M.; et al. Impact of cfDNA Reference Materials on Clinical Performance of Liquid Biopsy NGS Assays. Cancers 2023, 15, 5024. https://doi.org/10.3390/cancers15205024
Hallermayr A, Keßler T, Fujera M, Liesfeld B, Bernstein S, von Ameln S, Schanze D, Steinke-Lange V, Pickl JMA, Neuhann TM, et al. Impact of cfDNA Reference Materials on Clinical Performance of Liquid Biopsy NGS Assays. Cancers. 2023; 15(20):5024. https://doi.org/10.3390/cancers15205024
Chicago/Turabian StyleHallermayr, Ariane, Thomas Keßler, Moritz Fujera, Ben Liesfeld, Samuel Bernstein, Simon von Ameln, Denny Schanze, Verena Steinke-Lange, Julia M. A. Pickl, Teresa M. Neuhann, and et al. 2023. "Impact of cfDNA Reference Materials on Clinical Performance of Liquid Biopsy NGS Assays" Cancers 15, no. 20: 5024. https://doi.org/10.3390/cancers15205024
APA StyleHallermayr, A., Keßler, T., Fujera, M., Liesfeld, B., Bernstein, S., von Ameln, S., Schanze, D., Steinke-Lange, V., Pickl, J. M. A., Neuhann, T. M., & Holinski-Feder, E. (2023). Impact of cfDNA Reference Materials on Clinical Performance of Liquid Biopsy NGS Assays. Cancers, 15(20), 5024. https://doi.org/10.3390/cancers15205024