

Persistence of Telemedicine Usage for Breast and Prostate Cancer after the Peak of the COVID-19 Pandemic
 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sirintrapun, S.J.; Lopez, A.M. Telemedicine in Cancer Care. In American Society of Clinical Oncology Educational Book; American Society of Clinical Oncology: Alexandria, VA, USA, 2018; Volume 38, pp. 540–545. [Google Scholar]
- Shirke, M.M.; Shaikh, S.A.; Harky, A. Implications of Telemedicine in Oncology during the COVID-19 Pandemic. Acta Biomed. 2020, 91, e2020022. [Google Scholar]
- Daggubati, L.C.; Eichberg, D.G.; Ivan, M.E.; Hanft, S.; Mansouri, A.; Komotar, R.J.; D’Amico, R.S.; Zacharia, B.E. Telemedicine for Outpatient Neurosurgical Oncology Care: Lessons Learned for the Future During the COVID-19 Pandemic. World Neurosurg. 2020, 139, e859–e863. [Google Scholar] [CrossRef]
- Bizot, A.; Karimi, M.; Rassy, E.; Heudel, P.E.; Levy, C.; Vanlemmens, L.; Uzan, C.; Deluche, E.; Genet, D.; Saghatchian, M.; et al. Multicenter evaluation of breast cancer patients’ satisfaction and experience with oncology telemedicine visits during the COVID-19 pandemic. Br. J. Cancer 2021, 125, 1486–1493. [Google Scholar] [CrossRef]
- Doolittle, G.C.; Spaulding, A.O. Providing access to oncology care for rural patients via telemedicine. J. Oncol. Pract. 2006, 2, 228. [Google Scholar] [CrossRef] [PubMed]
- Shaverdian, N.; Gillespie, E.F.; Cha, E.; Kim, S.Y.; Benvengo, S.; Chino, F.; Kang, J.J.; Li, Y.; Atkinson, T.M.; Lee, N.; et al. Impact of telemedicine on patient satisfaction and perceptions of care quality in radiation oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 1174–1180. [Google Scholar] [CrossRef]
- Pang, N.-Q.; Lau, J.; Fong, S.-Y.; Wong, C.Y.-H.; Tan, K.-K. Telemedicine acceptance among older adult patients with cancer: Scoping review. J. Med. Internet Res. 2022, 24, e28724. [Google Scholar] [CrossRef] [PubMed]
- Orazem, M.; Oblak, I.; Spanic, T.; Ratosa, I. Telemedicine in Radiation Oncology Post–COVID-19 Pandemic: There Is No Turning Back; Elsevier: Amsterdam, The Netherlands, 2020; pp. 411–415. [Google Scholar]
- West, H.J.; Barzi, A.; Wong, D. Telemedicine in Cancer Care Beyond the COVID-19 Pandemic: Oncology 2.0? Curr. Oncol. Rep. 2022, 24, 1843–1850. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.Y.; Mehrotra, A.; Huskamp, H.A.; Uscher-Pines, L.; Ganguli, I.; Barnett, M.L. Trends in Outpatient Care Delivery and Telemedicine During the COVID-19 Pandemic in the US. JAMA Intern. Med. 2021, 181, 388–391. [Google Scholar] [CrossRef] [PubMed]
- Ftouni, R.; AlJardali, B.; Hamdanieh, M.; Ftouni, L.; Salem, N. Challenges of Telemedicine during the COVID-19 pandemic: A systematic review. BMC Med. Inf. Decis. Mak. 2022, 22, 207. [Google Scholar] [CrossRef]
- Panet, F.; Tétreault-Langlois, M.; Morin, V.; Sultanem, K.; Melnychuk, D.; Panasci, L. The risks associated with the widespread use of telemedicine in oncology: Four cases and review of the literature. Cancer Rep. 2022, 5, e1531. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Wagle, N.S.; Jemal, A. Cancer statistics, 2023. CA Cancer J. Clin. 2023, 73, 17–48. [Google Scholar] [CrossRef]
- Xia, C.; Dong, X.; Li, H.; Cao, M.; Sun, D.; He, S.; Yang, F.; Yan, X.; Zhang, S.; Li, N.; et al. Cancer statistics in China and United States, 2022: Profiles, trends, and determinants. Chin. Med. J. 2022, 135, 584–590. [Google Scholar] [CrossRef]
- De, B.; Fu, S.; Chen, Y.; Das, P.; Ku, K.; Maroongroge, S.; Woodhouse, K.D.; Hoffman, K.E.; Nguyen, Q.; Reed, V.K.; et al. Patient, physician, and policy factors underlying variation in use of telemedicine for radiation oncology cancer care. Cancer Med. 2022, 11, 2096–2105. [Google Scholar] [CrossRef]
- Lee, E.C.; Grigorescu, V.; Enogieru, I.; Smith, S.R.; Samson, L.W.; Conmy, A.; De Lew, N. Updated National Survey Trends in Telehealth Utilization and Modality: 2021–2022 (Issue Brief No. HP-2023-09); Office of the Assistant Secretary for Planning and Evaluation, Ed.; US Department of Health and Human Services: Washington, DC, USA, 2023.
- Donner, C.F.; ZuWallack, R.; Nici, L. The Role of Telemedicine in Extending and Enhancing Medical Management of the Patient with Chronic Obstructive Pulmonary Disease. Medicina 2021, 57, 726. [Google Scholar] [CrossRef]
- Chan, R.; Crichton, M.; Crawford-Williams, F.; Agbejule, O.; Yu, K.; Hart, N.; Alves, F.d.A.; Ashbury, F.; Eng, L.; Fitch, M.; et al. The efficacy, challenges, and facilitators of telemedicine in post-treatment cancer survivorship care: An overview of systematic reviews. Ann. Oncol. 2021, 32, 1552–1570. [Google Scholar] [CrossRef]
- Doarn, C.R. Telemedicine and psychiatry-a natural match. Mhealth 2018, 4, 60. [Google Scholar] [CrossRef] [PubMed]
- Riemer-Reiss, M.L. Utilizing Distance Technology for Mental Health Counseling. J. Ment. Health Couns. 2000, 22, 189. [Google Scholar]
- ConnDrake, C.; Lian, T.; Cameron, B.; Medynskaya, K.; Bosworth, H.B.; Shah, K. Understanding Telemedicine’s “New Normal”: Variations in Telemedicine Use by Specialty Line and Patient Demographics. Telemed. e-Health 2022, 28, 51–59. [Google Scholar]
- Sheets, L.R.; Wallach, E.; Khairat, S.; Mutrux, R.; Edison, K.; Becevic, M. Similarities and Differences Between Rural and Urban Telemedicine Utilization. Perspect. Health Inf. Manag. 2021, 18, 1e. [Google Scholar]
- Donelan, K.; Barreto, E.A.; Sossong, S.; Michael, C.; Estrada, J.J.; Cohen, A.B.; Wozniak, J.; Schwamm, L.H. Patient and clinician experiences with telehealth for patient follow-up care. Am. J. Manag. Care 2019, 25, 40–44. [Google Scholar]
- Hennemann-Krause, L.; Lopes, A.J.; Araújo, J.A.; Petersen, E.M.; Nunes, R.A. The assessment of telemedicine to support outpatient palliative care in advanced cancer. Palliat. Support. Care 2015, 13, 1025–1030. [Google Scholar] [CrossRef] [PubMed]
- Spelten, E.; Hardman, R.; Pike, K.; Yuen, E.; Wilson, C. Best practice in the implementation of telehealth-based supportive cancer care: Using research evidence and discipline-based guidance. Patient Educ. Couns. 2021, 104, 2682–2699. [Google Scholar] [CrossRef]
- Worster, B.; Swartz, K. Telemedicine and Palliative Care: An Increasing Role in Supportive Oncology. Curr. Oncol. Rep. 2017, 19, 37. [Google Scholar] [CrossRef] [PubMed]
- Uppal, A.; Kothari, A.N.; Scally, C.P.; Roland, C.L.; Bednarski, B.K.; Katz, M.H.; Vauthey, J.-N.; Chang, G.J.; in collaboration with the D3CODE Team. Adoption of Telemedicine for Postoperative Follow-Up After Inpatient Cancer-Related Surgery. JCO Oncol. Pract. 2022, 18, e1091–e1099. [Google Scholar] [CrossRef]
- Sitter, K.E.; Wong, D.H.; Bolton, R.E.; Vimalananda, V.G. Clinical Appropriateness of Telehealth: A Qualitative Study of Endocrinologists’ Perspectives. J. Endocr. Soc. 2022, 6, bvac089. [Google Scholar] [CrossRef]
- Uscher-Pines, L.; Parks, A.M.; Sousa, J.; Raja, P.; Mehrotra, A.; Huskamp, H.A.; Busch, A.B. Appropriateness of Telemedicine Versus In-Person Care: A Qualitative Exploration of Psychiatrists’ Decision Making. Psychiatr. Serv. 2022, 73, 849–855. [Google Scholar] [CrossRef] [PubMed]
- Hasson, S.P.; Waissengrin, B.; Shachar, E.; Hodruj, M.; Fayngor, R.; Brezis, M.; Nikolaevski-Berlin, A.; Pelles, S.; Safra, T.; Geva, R.; et al. Rapid implementation of telemedicine during the COVID-19 pandemic: Perspectives and preferences of patients with cancer. Oncologist 2021, 26, e679–e685. [Google Scholar] [CrossRef]
- Tripepi, M.; Pizzocaro, E.; Giardino, A.; Frigerio, I.; Guglielmi, A.; Butturini, G. Telemedicine and pancreatic cancer: A systematic review. Telemed. e-Health 2023, 29, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Cha, E.E.; Lynch, K.; Cahlon, O.; Gomez, D.R.; Shaverdian, N.; Gillespie, E.F. Radiation Oncologist Perceptions of Telemedicine from Consultation to Treatment Planning: A Mixed-Methods Study; Elsevier: Amsterdam, The Netherlands, 2020; pp. 421–429. [Google Scholar]
- Tevaarwerk, A.J.; Chandereng, T.; Osterman, T.; Arafat, W.; Smerage, J.; Polubriaginof, F.C.G.; Heinrichs, T.; Sugalski, J.; Martin, D.B. Oncologist perspectives on telemedicine for patients with cancer: A National Comprehensive Cancer Network survey. JCO Oncol. Pract. 2021, 17, e1318–e1326. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Pre-COVID-19 3/2019–2/2020 N = 50,585 | Peak COVID-19 3/2020–2/2021 N = 48,522 | Post-Peak 3/2021–2/2022 N = 55,612 | |||
|---|---|---|---|---|---|---|
| Age (yrs) | No. | % | No. | % | No. | % |
| Age (yrs) | ||||||
| 0–18 | 12 | 0% | 11 | 0% | 15 | 0% |
| 19–29 | 179 | 0% | 171 | 0% | 169 | 0% |
| 30–39 | 1565 | 3% | 1496 | 3% | 1691 | 3% |
| 40–49 | 6175 | 12% | 5817 | 12% | 6352 | 11% |
| 50–59 | 12,572 | 25% | 11,926 | 25% | 13,298 | 24% |
| 60–69 | 16,126 | 32% | 15,630 | 32% | 17,849 | 32% |
| 70–79 | 12,259 | 24% | 11,992 | 25% | 14,315 | 26% |
| 80–89 | 3358 | 7% | 3227 | 7% | 3959 | 7% |
| 90+ | 333 | 1% | 307 | 1% | 353 | 1% |
| Sex | ||||||
| Female | 34,058 | 67% | 32,747 | 67% | 37,061 | 67% |
| Male | 16,527 | 33% | 15,775 | 33% | 18,551 | 33% |
| Cancer Type | ||||||
| Breast | 34,270 | 68% | 32,908 | 68% | 37,250 | 67% |
| Prostate | 16,315 | 32% | 15,614 | 32% | 18,362 | 33% |
| Ethnicity | ||||||
| Not Hispanic or Latino | 44,522 | 88% | 42,739 | 88% | 48,602 | 87% |
| Hispanic or Latino | 3164 | 6% | 3143 | 6% | 3707 | 7% |
| Missing | 2899 | 6% | 2640 | 5% | 3303 | 6% |
| Race | ||||||
| White | 38,921 | 77% | 37,195 | 77% | 42,168 | 76% |
| Black or African American | 4349 | 9% | 4372 | 9% | 5042 | 9% |
| Asian or Indian | 3395 | 7% | 3289 | 7% | 3986 | 7% |
| Other | 1434 | 3% | 1420 | 3% | 1725 | 3% |
| Missing | 2486 | 5% | 3275 | 7% | 2691 | 5% |
| Primary Language | ||||||
| English | 47,186 | 93% | 45,784 | 94% | 52,575 | 95% |
| Spanish | 757 | 1% | 710 | 1% | 809 | 1% |
| Russian | 477 | 1% | 426 | 1% | 471 | 1% |
| Other | 2165 | 4% | 2395 | 5% | 1757 | 3% |
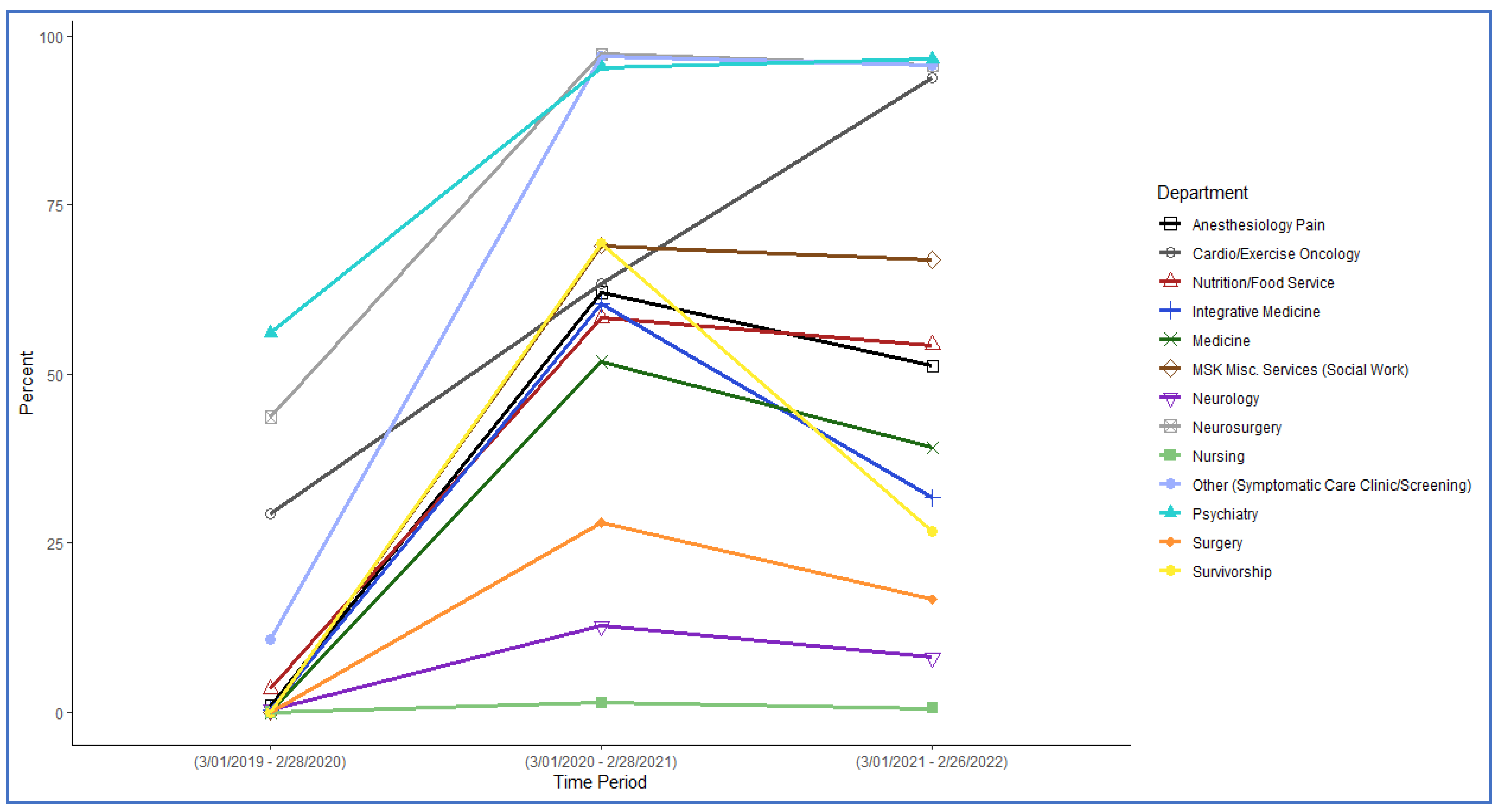
| Department/Specialty | Pre-COVID-19 3/2019–2/2020 N = 202,296 | Peak COVID-19 3/2020–2/2021 N = 180,649 | Post-Peak 3/2021–2/2022 N = 219,288 | ||||
|---|---|---|---|---|---|---|---|
| No. | % | No. | % | No. | % | p-Value * | |
| Anesthesiology/Pain Mgmt. | |||||||
| Telemedicine | 11 | 1% | 1066 | 62% | 1186 | 51% | <0.001 |
| In person | 1282 | 99% | 653 | 38% | 1132 | 49% | |
| Cardio-Oncology/Exercise | |||||||
| Telemedicine | 29 | 29% | 104 | 63% | 527 | 94% | <0.001 |
| In person | 70 | 71% | 60 | 37% | 34 | 6% | |
| Integrative Medicine | |||||||
| Telemedicine | 139 | 3% | 1588 | 58% | 2043 | 54% | 0.001 |
| In person | 3965 | 97% | 1136 | 42% | 1722 | 46% | |
| Medicine | |||||||
| Telemedicine | 383 | 0% | 51,959 | 60% | 31,912 | 32% | <0.001 |
| In person | 89,425 | 100% | 34,205 | 40% | 68,655 | 68% | |
| Neurology | |||||||
| Telemedicine | 0 | 0% | 2221 | 52% | 2267 | 39% | <0.001 |
| In person | 4498 | 100% | 2069 | 48% | 3531 | 61% | |
| Neurosurgery | |||||||
| Telemedicine | 0 | 0% | 265 | 69% | 347 | 67% | 0.517 |
| In person | 409 | 100% | 119 | 31% | 172 | 33% | |
| Nursing | |||||||
| Telemedicine | 73 | 0% | 1397 | 13% | 1164 | 8% | <0.001 |
| In person | 17,059 | 100% | 9589 | 87% | 13,190 | 92% | |
| Nutrition/Food Service | |||||||
| Telemedicine | 824 | 44% | 2287 | 97% | 2742 | 96% | 0.001 |
| In person | 1067 | 56% | 63 | 3% | 126 | 4% | |
| Psychiatry | |||||||
| Telemedicine | 566 | 11% | 6965 | 97% | 7665 | 96% | <0.001 |
| In person | 4708 | 89% | 219 | 3% | 352 | 4% | |
| Social Work | |||||||
| Telemedicine | 1316 | 56% | 1906 | 95% | 2372 | 97% | 0.045 |
| In person | 1033 | 44% | 92 | 5% | 84 | 3% | |
| Surgery | |||||||
| Telemedicine | 0 | 0% | 15,028 | 28% | 11,159 | 17% | <0.001 |
| In person | 66,882 | 100% | 38,679 | 72% | 56,130 | 83% | |
| Survivorship | |||||||
| Telemedicine | 3 | 0% | 5107 | 69% | 2331 | 27% | <0.001 |
| In person | 7433 | 100% | 2268 | 31% | 6378 | 73% | |
| Other | |||||||
| Telemedicine | 0 | 0% | 22 | 1% | 12 | 1% | 0.015 |
| In person | 1121 | 100% | 1582 | 99% | 2055 | 99% | |
| All | |||||||
| Telemedicine | 3344 | 2% | 89,915 | 50% | 65,727 | 30% | <0.001 |
| In person | 198,952 | 98% | 90,734 | 50% | 153,561 | 70% | |
| Department/Specialty | Peak COVID-19 3/2021–2/2022 N = 180,649 | Post-Peak 3/2021–2/2022 N = 219,288 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| New | Follow-Up | Other | New | Follow-Up | Other | |||||||
| No. | % | No. | % | No. | % | No. | % | No. | % | No. | % | |
| Anesthesiology/Pain Mgmt. | ||||||||||||
| Telemedicine | 46 | 14% | 1020 | 74% | 0 | 0% | 6 | 1% | 1180 | 63% | 0 | 0% |
| In person | 294 | 86% | 359 | 26% | 0 | 0% | 444 | 99% | 688 | 37% | 0 | 0% |
| Cardio/Exercise | ||||||||||||
| Telemedicine | 14 | 100% | 13 | 100% | 77 | 56% | 99 | 100% | 220 | 100% | 208 | 86% |
| In person | 0 | 0% | 0 | 0% | 60 | 44% | 0 | 0% | 0 | 0% | 34 | 14% |
| Integrative Med. | ||||||||||||
| Telemedicine | 552 | 92% | 882 | 56% | 154 | 28% | 834 | 79% | 976 | 46% | 233 | 41% |
| In person | 49 | 8% | 698 | 44% | 389 | 72% | 225 | 21% | 1163 | 54% | 334 | 59% |
| Medicine | ||||||||||||
| Telemedicine | 6077 | 69% | 44,540 | 59% | 1342 | 100% | 4145 | 38% | 26,176 | 30% | 1591 | 100% |
| In person | 2733 | 31% | 31,466 | 41% | 6 | 0% | 6696 | 62% | 61,959 | 70% | 0 | 0% |
| Neurology | ||||||||||||
| Telemedicine | 257 | 29% | 1964 | 58% | 0 | 0% | 133 | 12% | 2134 | 46% | 0 | 0% |
| In person | 633 | 71% | 1436 | 42% | 0 | 0% | 983 | 88% | 2548 | 54% | 0 | 0% |
| Neurosurgery | ||||||||||||
| Telemedicine | 94 | 75% | 171 | 66% | 0 | 0% | 137 | 71% | 208 | 64% | 2 | 100% |
| In person | 31 | 25% | 88 | 34% | 0 | 0% | 55 | 29% | 117 | 36% | 0 | 0% |
| Nursing | ||||||||||||
| Telemedicine | 72 | 100% | 1184 | 11% | 141 | 60% | 73 | 99% | 775 | 6% | 316 | 80% |
| In person | 0 | 0% | 9495 | 89% | 94 | 40% | 1 | 1% | 13,112 | 94% | 77 | 20% |
| Nutrition/Food | ||||||||||||
| Telemedicine | 51 | 61% | 47 | 60% | 2189 | 100% | 377 | 82% | 150 | 79% | 2215 | 100% |
| In person | 32 | 39% | 31 | 40% | 0 | 0% | 85 | 18% | 41 | 21% | 0 | 0% |
| Psychiatry | ||||||||||||
| Telemedicine | 655 | 95% | 5604 | 97% | 706 | 99% | 721 | 87% | 6312 | 96% | 632 | 99% |
| In person | 38 | 5% | 173 | 3% | 8 | 1% | 111 | 13% | 234 | 4% | 7 | 1% |
| Social Work | ||||||||||||
| Telemedicine | 24 | 43% | 26 | 30% | 1856 | 100% | 32 | 52% | 31 | 36% | 2309 | 100% |
| In person | 32 | 57% | 60 | 70% | 0 | 0% | 30 | 48% | 54 | 64% | 0 | 0% |
| Surgery | ||||||||||||
| Telemedicine | 2567 | 27% | 12,442 | 28% | 19 | 100% | 1611 | 13% | 9501 | 17% | 47 | 100% |
| In person | 6976 | 73% | 31,703 | 72% | 0 | 0% | 10,912 | 87% | 45,218 | 83% | 0 | 0% |
| Survivorship | ||||||||||||
| Telemedicine | 911 | 74% | 4196 | 68% | 0 | 0% | 478 | 30% | 1853 | 26% | 0 | 0% |
| In person | 323 | 26% | 1945 | 32% | 0 | 0% | 1110 | 70% | 5268 | 74% | 0 | 0% |
| Other | ||||||||||||
| Telemedicine | 2 | 29% | 20 | 1% | 0 | 0% | 1 | 9% | 11 | 1% | 0 | 0% |
| In person | 5 | 71% | 1577 | 99% | 0 | 0% | 10 | 91% | 2045 | 99% | 0 | 0% |
| All | ||||||||||||
| Telemedicine | 11,322 | 50% | 72,109 | 48% | 6484 | 92% | 8647 | 30% | 49,527 | 27% | 7553 | 94% |
| In person | 11,146 | 50% | 79,031 | 52% | 557 | 8% | 20,662 | 70% | 132,447 | 73% | 452 | 6% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chimonas, S.; Lipitz-Snyderman, A.; Spiegelhoff, Z.; Chakraborty, N.; Seier, K.; White, C.; Kuperman, G. Persistence of Telemedicine Usage for Breast and Prostate Cancer after the Peak of the COVID-19 Pandemic. Cancers 2023, 15, 4961. https://doi.org/10.3390/cancers15204961
Chimonas S, Lipitz-Snyderman A, Spiegelhoff Z, Chakraborty N, Seier K, White C, Kuperman G. Persistence of Telemedicine Usage for Breast and Prostate Cancer after the Peak of the COVID-19 Pandemic. Cancers. 2023; 15(20):4961. https://doi.org/10.3390/cancers15204961
Chicago/Turabian StyleChimonas, Susan, Allison Lipitz-Snyderman, Zoe Spiegelhoff, Nirjhar Chakraborty, Kenneth Seier, Charlie White, and Gilad Kuperman. 2023. "Persistence of Telemedicine Usage for Breast and Prostate Cancer after the Peak of the COVID-19 Pandemic" Cancers 15, no. 20: 4961. https://doi.org/10.3390/cancers15204961
APA StyleChimonas, S., Lipitz-Snyderman, A., Spiegelhoff, Z., Chakraborty, N., Seier, K., White, C., & Kuperman, G. (2023). Persistence of Telemedicine Usage for Breast and Prostate Cancer after the Peak of the COVID-19 Pandemic. Cancers, 15(20), 4961. https://doi.org/10.3390/cancers15204961