
Primary Sclerosing Cholangitis-Associated Cholangiocarcinoma: From Pathogenesis to Diagnostic and Surveillance Strategies


Abstract
Simple Summary
Abstract
1. Introduction
2. Epidemiology
3. Risk Factors
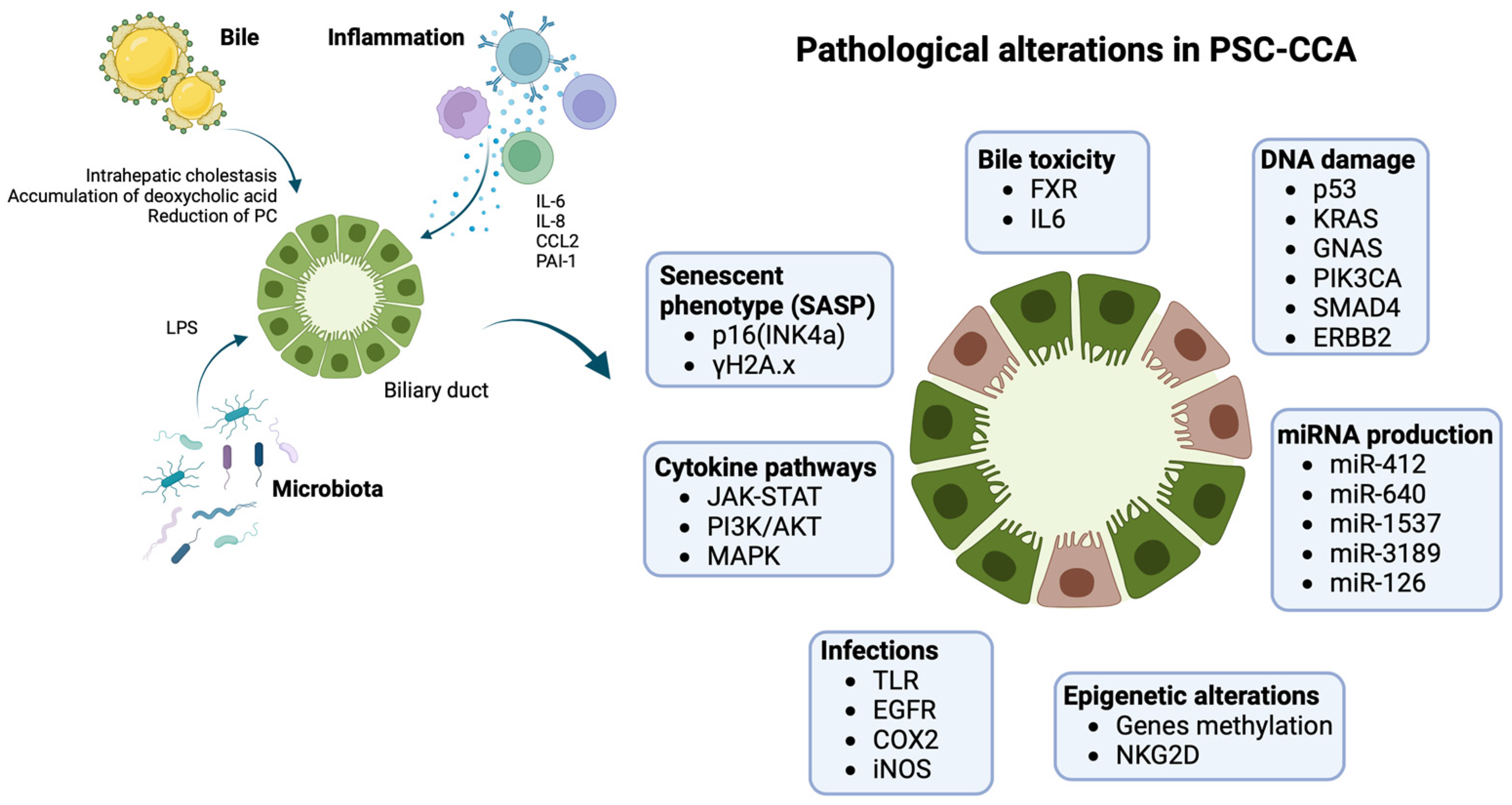
4. Pathogenesis
5. Clinical Presentation
6. Diagnosis
7. Surveillance of CCA in PSC
8. Future Perspective: Next-Generation Biomarkers for PSC-CCA Diagnosis and Surveillance

{kind=link}
| Marker | Sample | Patients Cohort | SE (%) | SP (%) | AUC | Ref. |
|---|---|---|---|---|---|---|
| Serum biomarkers panel | ||||||
| PKM2 | serum | CCA (n = 66) vs. PSC (n = 62) | 82% | 90% | 0.90 | [152] |
| CYFRA21.1 | ||||||
| MUC5AC | ||||||
| GGT | ||||||
| ELF score | serum | CCA (n = 36) vs. PSC-CCA (n = 32) vs. PSC (n = 119) | 81% | 60% | 0.74 | [151] |
| Volatile organic compounds | ||||||
| Acrylonitrile + 3-methyl hexane + benzene | bile | PSC-CCA (n = 11) vs. PSC (n = 21) | 91% | 73% | 0.89 | [154] |
| Ethane + 1-octene | bile | PSC-CCA (n = 11) vs. PSC (n = 21) | 80% | 100% | 0.90 | [154] |
| 2-propanol + Acetonitrile | urine | CCA (n = 6) vs. PSC (n = 10) | 83% | 85% | 0.86 | [156] |
| 2-propanol + carbon disulfide + trimethyl amine | urine | CCA (n = 6) vs. PSC (n = 10) vs. benign stenoses (n = 29) | 93% | 62% | 0.83 | [156] |
| DNA Methylation markers | ||||||
| CDO1 CNRIP1 SEPT9 VIM | biliary brushing | CCA (n = 34) PSC (n = 34) | 85% | 98% | 0.94 | [161] |
| CDO1 | bile | CCA-PSC (n = 38) vs. PSC (n = 205) | 79% | 90% | 0.88 | [162] |
| CNRIP1 | ||||||
| SEPT9 | CCA-PSC ≤ 12 months (n = 28) vs. PSC (n = 205) | 100% | 90% | 0.98 | [162] | |
| VIM | ||||||
| CCA-PSC ≤ 12 months (n = 28) vs. PSC > 36 months (n = 170) | 100% | 93% | 0.98 | [162] | ||
| miRNA | ||||||
| miRNA191 | bile | CCA (n = 46) vs. PSC (n = 13) vs. benign stenosis (n = 37) | 67% | 96% | - | [170] |
| U486-3p | ||||||
| U1274b | ||||||
| U16 | ||||||
| U484 | ||||||
| miR222 | serum | CCA (n = 40) vs. PSC (n = 40) | - | - | 0.77 | [171] |
| miR-483-5p | ||||||
| miR122 | serum | CCA (n = 31) vs. PSC (n = 40) | 32% | 90% | 0.65 | [93] |
| miR-26a | 52% | 93% | 0.78 | |||
| miR-1281 | 55% | 90% | 0.83 | |||
| miR-126 | 68% | 93% | 0.87 | |||
| miR30b | 52% | 88% | 0.78 | |||
| miR-640 | bile | CCA (n = 19) vs. PSC-CCA (n = 12) vs. PSC (n = 52) | 50% | 92% | 0.81 | [93] |
| miR-3189 | 67% | 89% | 0.80 | |||
| miR-1537 | 67% | 90% | 0.78 | |||
| miR-412 | 50% | 89% | 0.81 | |||
| Metabolomic analysis | ||||||
| histidine + PC(34:3) | serum | iCCA (n = 20) vs. PSC (n = 20) | 100% | 70% | 0.99 | [176] |
| Proteomic analysis | ||||||
| 22-peptides CC model | bile | CCA (n = 25) vs. PSC (n = 18) | 84% | 78% | 0.87 | [178] |
| 42-peptides panel | urine | CCA (n = 42) vs. PSC/benign stenosis (n = 81) | 83% | 79% | 0.87 | [177] |
| Combined BPA/UPA test | urine/bile | CCA (n = 16) vs. PSC/benign stenosis (n = 29) | 94% | 76% | 0.84 | [179] |
| Glycomic + proteomic analysis | ||||||
| Fucosylated fetuin A | serum | CCA (n = 20) vs. PSC (n = 39) | 62% | 90% | 0.82 | [180] |
| EVs mRNA | ||||||
| PON1 | serum | CCA (n = 12) vs. PSC (n = 6) | 100% | 100% | 1.00 | [184] |
| ATF4 | 100% | 100% | 1.00 | |||
| PHGDH | 100% | 100% | 1.00 | |||
| CLIP3 | urine | CCA (n = 23) vs. PSC (n = 5) | 87% | 100% | 0.97 | [184] |
| VCAM1 | 87% | 100% | 0.97 | |||
| TRIM33 | 87% | 100% | 0.97 | |||
| EVs non-coding RNA | ||||||
| MALAT1 | serum | CCA (n = 12) vs. PSC (n = 6) | 100% | 100% | 1.00 | [184] |
| LOC100190986 | 100% | 100% | 1.00 | |||
| SNORA11B | 100% | 100% | 1.00 | |||
| ATP5EP2 | urine | CCA (n = 23) vs. PSC (n = 5) | 87% | 100% | 0.94 | [184] |
| LOC100134713 | 83% | 100% | 0.93 | |||
| SNORA8 | 83% | 100% | 0.92 | |||
| EVs proteins | ||||||
| FIBG | serum | CCA (n = 43) vs. PSC (n = 30) | 88% | 63% | 0.80 | [183] |
| A1AG1 | 77% | 70% | 0.79 | |||
| S100A8 | 70% | 67% | 0.76 | |||
| FCN2 | serum | Early stage CCA (n = 13) vs. PSC (n = 30) | 100% | 81% | 0.96 | [183] |
| ITIH4 | 92% | 81% | 0.88 | |||
| FIBG | 92% | 81% | 0.88 | |||
| CRP | serum | PSC-CCA (n = 22) vs. PSC (n = 45) | 64% | 93% | 0.91 | [185] |
| FIBRINOGEN | ||||||
| FRIL | ||||||
| PIGR |
9. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Izquierdo-Sanchez, L.; Lamarca, A.; La Casta, A.; Buettner, S.; Utpatel, K.; Klümpen, H.-J.; Adeva, J.; Vogel, A.; Lleo, A.; Fabris, L.; et al. Cholangiocarcinoma Landscape in Europe: Diagnostic, Prognostic and Therapeutic Insights from the ENSCCA Registry. J. Hepatol. 2022, 76, 1109–1121. [Google Scholar] [CrossRef]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next Horizon in Mechanisms and Management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef]
- Bertuccio, P.; Malvezzi, M.; Carioli, G.; Hashim, D.; Boffetta, P.; El-Serag, H.B.; La Vecchia, C.; Negri, E. Global Trends in Mortality from Intrahepatic and Extrahepatic Cholangiocarcinoma. J. Hepatol. 2019, 71, 104–114. [Google Scholar] [CrossRef]
- Kaewpitoon, N. Opisthorchis Viverrini: The Carcinogenic Human Liver Fluke. WJG 2008, 14, 666. [Google Scholar] [CrossRef]
- Clements, O.; Eliahoo, J.; Kim, J.U.; Taylor-Robinson, S.D.; Khan, S.A. Risk Factors for Intrahepatic and Extrahepatic Cholangiocarcinoma: A Systematic Review and Meta-Analysis. J. Hepatol. 2020, 72, 95–103. [Google Scholar] [CrossRef]
- Wongjarupong, N.; Assavapongpaiboon, B.; Susantitaphong, P.; Cheungpasitporn, W.; Treeprasertsuk, S.; Rerknimitr, R.; Chaiteerakij, R. Non-Alcoholic Fatty Liver Disease as a Risk Factor for Cholangiocarcinoma: A Systematic Review and Meta-Analysis. BMC Gastroenterol. 2017, 17, 149. [Google Scholar] [CrossRef]
- Tyson, G.L.; El-Serag, H.B. Risk Factors for Cholangiocarcinoma. Hepatology 2011, 54, 173–184. [Google Scholar] [CrossRef]
- Karlsen, T.H.; Folseraas, T.; Thorburn, D.; Vesterhus, M. Primary Sclerosing Cholangitis—A Comprehensive Review. J. Hepatol. 2017, 67, 1298–1323. [Google Scholar] [CrossRef]
- Khan, S.A.; Tavolari, S.; Brandi, G. Cholangiocarcinoma: Epidemiology and Risk Factors. Liver Int. 2019, 39, 19–31. [Google Scholar] [CrossRef]
- Lazaridis, K.N.; LaRusso, N.F. Primary Sclerosing Cholangitis. N. Engl. J. Med. 2016, 375, 1161–1170. [Google Scholar] [CrossRef]
- Boonstra, K.; Weersma, R.K.; van Erpecum, K.J.; Rauws, E.A.; Spanier, B.W.M.; Poen, A.C.; van Nieuwkerk, K.M.; Drenth, J.P.; Witteman, B.J.; Tuynman, H.A.; et al. Population-Based Epidemiology, Malignancy Risk, and Outcome of Primary Sclerosing Cholangitis. Hepatology 2013, 58, 2045–2055. [Google Scholar] [CrossRef]
- Weismüller, T.J.; Trivedi, P.J.; Bergquist, A.; Imam, M.; Lenzen, H.; Ponsioen, C.Y.; Holm, K.; Gotthardt, D.; Färkkilä, M.A.; Marschall, H.-U.; et al. Patient Age, Sex, and Inflammatory Bowel Disease Phenotype Associate with Course of Primary Sclerosing Cholangitis. Gastroenterology 2017, 152, 1975–1984.e8. [Google Scholar] [CrossRef]
- Razumilava, N.; Gores, G.J.; Lindor, K.D. Cancer Surveillance in Patients with Primary Sclerosing Cholangitis. Hepatology 2011, 54, 1842–1852. [Google Scholar] [CrossRef]
- Song, J.; Li, Y.; Bowlus, C.L.; Yang, G.; Leung, P.S.C.; Gershwin, M.E. Cholangiocarcinoma in Patients with Primary Sclerosing Cholangitis (PSC): A Comprehensive Review. Clin. Rev. Allergy Immunol. 2020, 58, 134–149. [Google Scholar] [CrossRef]
- Tabibian, J.H.; Ali, A.H.; Lindor, K.D. Primary Sclerosing Cholangitis, Part 1: Epidemiology, Etiopathogenesis, Clinical Features, and Treatment. Gastroenterol. Hepatol. 2018, 14, 293–304. [Google Scholar]
- Horsley-Silva, J.L.; Rodriguez, E.A.; Franco, D.L.; Lindor, K.D. An Update on Cancer Risk and Surveillance in Primary Sclerosing Cholangitis. Liver Int. 2017, 37, 1103–1109. [Google Scholar] [CrossRef]
- Fevery, J.; Henckaerts, L.; Van Oirbeek, R.; Vermeire, S.; Rutgeerts, P.; Nevens, F.; Van Steenbergen, W. Malignancies and Mortality in 200 Patients with Primary Sclerosering Cholangitis: A Long-Term Single-Centre Study: Malignancies and Mortality in PSC. Liver Int. 2012, 32, 214–222. [Google Scholar] [CrossRef]
- Boberg, K.M.; Bergquist, A.; Mitchell, S.; Pares, A.; Rosina, F.; Broomé, U.; Chapman, R.; Fausa, O.; Egeland, T.; Rocca, G.; et al. Cholangiocarcinoma in Primary Sclerosing Cholangitis: Risk Factors and Clinical Presentation. Scand. J. Gastroenterol. 2002, 37, 1205–1211. [Google Scholar] [CrossRef]
- Zenouzi, R.; Weismüller, T.J.; Hübener, P.; Schulze, K.; Bubenheim, M.; Pannicke, N.; Weiler–Normann, C.; Lenzen, H.; Manns, M.P.; Lohse, A.W.; et al. Low Risk of Hepatocellular Carcinoma in Patients with Primary Sclerosing Cholangitis with Cirrhosis. Clin. Gastroenterol. Hepatol. 2014, 12, 1733–1738. [Google Scholar] [CrossRef]
- Burak, K.; Angulo, P.; Pasha, T.M.; Egan, K.; Petz, J.; Lindor, K.D. Incidence and Risk Factors for Cholangiocarcinoma in Primary Sclerosing Cholangitis. Am. J. Gastroenterol. 2004, 99, 523–526. [Google Scholar] [CrossRef]
- Trivedi, P.J.; Crothers, H.; Mytton, J.; Bosch, S.; Iqbal, T.; Ferguson, J.; Hirschfield, G.M. Effects of Primary Sclerosing Cholangitis on Risks of Cancer and Death in People with Inflammatory Bowel Disease, Based on Sex, Race, and Age. Gastroenterology 2020, 159, 915–928. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Martínez, S.; Rimola, J.; Londoño, M.C.; Cárdenas, A.; Forner, A. Cholangiocarcinoma: Early Detection and Screening in High-Risk Population. Hepatoma Res. 2022, 8, 30. [Google Scholar] [CrossRef]
- Carbone, M.; Kodra, Y.; Rocchetti, A.; Manno, V.; Minelli, G.; Gerussi, A.; Ronca, V.; Malinverno, F.; Cristoferi, L.; Floreani, A.; et al. Primary Sclerosing Cholangitis: Burden of Disease and Mortality Using Data from the National Rare Diseases Registry in Italy. Int. J. Environ. Res. Public Health 2020, 17, 3095. [Google Scholar] [CrossRef]
- Takakura, W.R.; Tabibian, J.H.; Bowlus, C.L. The Evolution of Natural History of Primary Sclerosing Cholangitis. Curr. Opin. Gastroenterol. 2017, 33, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Eaton, J.E.; Welle, C.L.; Bakhshi, Z.; Sheedy, S.P.; Idilman, I.S.; Gores, G.J.; Rosen, C.B.; Heimbach, J.K.; Taner, T.; Harnois, D.M.; et al. Early Cholangiocarcinoma Detection with Magnetic Resonance Imaging versus Ultrasound in Primary Sclerosing Cholangitis. Hepatology 2021, 73, 1868–1881. [Google Scholar] [CrossRef] [PubMed]
- Silveira, M.G.; Lindor, K.D. Clinical Features and Management of Primary Sclerosing Cholangitis. WJG 2008, 14, 3338. [Google Scholar] [CrossRef]
- LaRusso, N.F.; Shneider, B.L.; Black, D.; Gores, G.J.; James, S.P.; Doo, E.; Hoofnagle, J.H. Primary Sclerosing Cholangitis: Summary of a Workshop. Hepatology 2006, 44, 746–764. [Google Scholar] [CrossRef]
- Ahrendt, S. Diagnosis and Management of Cholangiocarcinoma in Primary Sclerosing Cholangitis. J. Gastrointest. Surg. 1999, 3, 357–368. [Google Scholar] [CrossRef]
- Takikawa, H.; Manabe, T. Primary Sclerosing Cholangitis in Japan? Analysis of 192 Cases. J. Gastroenterol. 1997, 32, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Okolicsanyi, L.; Fabris, L.; Viaggi, S.; Carulli, N.; Podda, M.; Ricci, G. Primary Sclerosing Cholangitis: Clinical Presentation, Natural History and Prognostic Variables: An Italian Multicentre Study. The Italian PSC Study Group. Eur. J. Gastroenterol. Hepatol. 1996, 8, 685–691. [Google Scholar]
- Escorsell, A.; Parés, A.; Rodés, J.; Solís-Herruzo, J.A.; Miras, M.; Morena, E.D.L. Epidemiology of Primary Sclerosing Cholangitis in Spain. J. Hepatol. 1994, 21, 787–791. [Google Scholar] [CrossRef]
- Villard, C.; Friis-Liby, I.; Rorsman, F.; Said, K.; Warnqvist, A.; Cornillet, M.; Kechagias, S.; Nyhlin, N.; Werner, M.; Janczewska, I.; et al. Prospective Surveillance for Cholangiocarcinoma in Unselected Individuals with Primary Sclerosing Cholangitis. J. Hepatol. 2023, 78, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Bergquist, A.; Weismüller, T.J.; Levy, C.; Rupp, C.; Joshi, D.; Nayagam, J.S.; Montano-Loza, A.J.; Lytvyak, E.; Wunsch, E.; Milkiewicz, P.; et al. Impact on Follow-up Strategies in Patients with Primary Sclerosing Cholangitis. Liver Int. 2023, 43, 127–138. [Google Scholar] [CrossRef]
- Choi, J.; Ghoz, H.M.; Peeraphatdit, T.; Baichoo, E.; Addissie, B.D.; Harmsen, W.S.; Therneau, T.M.; Olson, J.E.; Chaiteerakij, R.; Roberts, L.R. Aspirin Use and the Risk of Cholangiocarcinoma. Hepatology 2016, 64, 785–796. [Google Scholar] [CrossRef]
- Bowlus, C.L.; Lim, J.K.; Lindor, K.D. AGA Clinical Practice Update on Surveillance for Hepatobiliary Cancers in Patients with Primary Sclerosing Cholangitis: Expert Review. Clin. Gastroenterol. Hepatol. 2019, 17, 2416–2422. [Google Scholar] [CrossRef]
- Morris-Stiff, G.; Bhati, C.; Olliff, S.; Hübscher, S.; Gunson, B.; Mayer, D.; Mirza, D.; Buckels, J.; Bramhall, S.R. Cholangiocarcinoma Complicating Primary Sclerosing Cholangitis: A 24-Year Experience. Dig. Surg. 2008, 25, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Björnsson, E.; Angulo, P. Cholangiocarcinoma in Young Individuals with and without Primary Sclerosing Cholangitis. Am. J. Gastroenterol. 2007, 102, 1677–1682. [Google Scholar] [CrossRef]
- Chalasani, N.; Baluyut, A.; Ismail, A.; Zaman, A.; Sood, G.; Ghalib, R.; McCashland, T.M.; Reddy, K.R.; Zervos, X.; Anbari, M.A.; et al. Cholangiocarcinoma in Patients with Primary Sclerosing Cholangitis: A Multicenter Case-Control Study. Hepatology 2000, 31, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Bergquist, A.; Glaumann, H.; Persson, B.; Broomé, U. Risk Factors and Clinical Presentation of Hepatobiliary Carcinoma in Patients with Primary Sclerosing Cholangitis: A Case-Control Study: Risk Factors and Clinical Presentation of Hepatobiliary Carcinoma in Patients with Primary Sclerosing Cholangitis: A Case-Control Study. Hepatology 1998, 27, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Valle, M.B.; Björnsson, E.; Lindkvist, B. Mortality and Cancer Risk Related to Primary Sclerosing Cholangitis in a Swedish Population-Based Cohort. Liver Int. 2012, 32, 441–448. [Google Scholar] [CrossRef]
- Rupp, C.; Rössler, A.; Zhou, T.; Rauber, C.; Friedrich, K.; Wannhoff, A.; Weiss, K.; Sauer, P.; Schirmacher, P.; Süsal, C.; et al. Impact of Age at Diagnosis on Disease Progression in Patients with Primary Sclerosing Cholangitis. United Eur. Gastroenterol. J. 2018, 6, 255–262. [Google Scholar] [CrossRef]
- Deneau, M.R.; El-Matary, W.; Valentino, P.L.; Abdou, R.; Alqoaer, K.; Amin, M.; Amir, A.Z.; Auth, M.; Bazerbachi, F.; Broderick, A.; et al. The Natural History of Primary Sclerosing Cholangitis in 781 Children: A Multicenter, International Collaboration. Hepatology 2017, 66, 518–527. [Google Scholar] [CrossRef]
- Chung, B.K.; Karlsen, T.H.; Folseraas, T. Cholangiocytes in the Pathogenesis of Primary Sclerosing Cholangitis and Development of Cholangiocarcinoma. Biochim. Biophys. Acta (BBA)—Mol. Basis Dis. 2018, 1864, 1390–1400. [Google Scholar] [CrossRef]
- Björnsson, E.; Olsson, R.; Bergquist, A.; Lindgren, S.; Braden, B.; Chapman, R.W.; Boberg, K.M.; Angulo, P. The Natural History of Small-Duct Primary Sclerosing Cholangitis. Gastroenterology 2008, 134, 975–980. [Google Scholar] [CrossRef]
- Bjornsson, E. Patients with Small Duct Primary Sclerosing Cholangitis Have a Favourable Long Term Prognosis. Gut 2002, 51, 731–735. [Google Scholar] [CrossRef] [PubMed]
- Gulamhusein, A.F.; Eaton, J.E.; Tabibian, J.H.; Atkinson, E.J.; Juran, B.D.; Lazaridis, K.N. Duration of Inflammatory Bowel Disease Is Associated with Increased Risk of Cholangiocarcinoma in Patients with Primary Sclerosing Cholangitis and IBD. Am. J. Gastroenterol. 2016, 111, 705–711. [Google Scholar] [CrossRef]
- Chazouilleres, O.; Beuers, U.; Bergquist, A.; Karlsen, T.H.; Levy, C.; Samyn, M.; Schramm, C.; Trauner, M. EASL Clinical Practice Guidelines on Sclerosing Cholangitis. J. Hepatol. 2022, 77, 761–806. [Google Scholar] [CrossRef]
- Aabakken, L.; Karlsen, T.H.; Albert, J.; Arvanitakis, M.; Chazouilleres, O.; Dumonceau, J.-M.; Färkkilä, M.; Fickert, P.; Hirschfield, G.M.; Laghi, A.; et al. Role of Endoscopy in Primary Sclerosing Cholangitis: European Society of Gastrointestinal Endoscopy (ESGE) and European Association for the Study of the Liver (EASL) Clinical Guideline. J. Hepatol. 2017, 66, 1265–1281. [Google Scholar] [CrossRef]
- Chapman, M.H.; Webster, G.J.M.; Bannoo, S.; Johnson, G.J.; Wittmann, J.; Pereira, S.P. Cholangiocarcinoma and Dominant Strictures in Patients with Primary Sclerosing Cholangitis: A 25-Year Single-Centre Experience. Eur. J. Gastroenterol. Hepatol. 2012, 24, 1051–1058. [Google Scholar] [CrossRef] [PubMed]
- Janse, M.; Lamberts, L.E.; Verdonk, R.C.; Weersma, R.K. IBD Is Associated with an Increase in Carcinoma in PSC Irrespective of the Presence of Dominant Bile Duct Stenosis. J. Hepatol. 2012, 57, 473–474. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Rudolph, G.; Gotthardt, D.; Klöters-Plachky, P.; Kulaksiz, H.; Rost, D.; Stiehl, A. Influence of Dominant Bile Duct Stenoses and Biliary Infections on Outcome in Primary Sclerosing Cholangitis. J. Hepatol. 2009, 51, 149–155. [Google Scholar] [CrossRef]
- Hilscher, M.B.; Tabibian, J.H.; Carey, E.J.; Gostout, C.J.; Lindor, K.D. Dominant Strictures in Primary Sclerosing Cholangitis: A Multicenter Survey of Clinical Definitions and Practices. Hepatol. Commun. 2018, 2, 836–844. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.T.; Talwalkar, J.A.; Rosen, C.B.; Smyrk, T.C.; Abraham, S.C. Precancerous Bile Duct Pathology in End-Stage Primary Sclerosing Cholangitis, with and without Cholangiocarcinoma. Am. J. Surg. Pathol. 2010, 34, 27–34. [Google Scholar] [CrossRef]
- Fleming, K.A.; Boberg, K.M.; Glaumann, H.; Bergquist, A.; Smith, D.; Clausen, O.P.F. Biliary Dysplasia as a Marker of Cholangiocarcinoma in Primary Sclerosing Cholangitis. J. Hepatol. 2001, 34, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Bergquist, A.; Glaumann, H.; Stal, P.; Wang, G.-S.; Broome, U. Biliary Dysplasia, Cell Proliferation and Nuclear DNA-Fragmentation in Primary Sclerosing Cholangitis with and without Cholangiocarcinoma. J. Intern. Med. 2001, 249, 69–75. [Google Scholar] [CrossRef]
- de Vries, A.B. Distinctive Inflammatory Bowel Disease Phenotype in Primary Sclerosing Cholangitis. WJG 2015, 21, 1956. [Google Scholar] [CrossRef]
- Hirschfield, G.M.; Karlsen, T.H.; Lindor, K.D.; Adams, D.H. Primary Sclerosing Cholangitis. Lancet 2013, 382, 1587–1599. [Google Scholar] [CrossRef]
- Özdirik, B.; Müller, T.; Wree, A.; Tacke, F.; Sigal, M. The Role of Microbiota in Primary Sclerosing Cholangitis and Related Biliary Malignancies. Int. J. Mol. Sci. 2021, 22, 6975. [Google Scholar] [CrossRef]
- Saab, M.; Mestivier, D.; Sohrabi, M.; Rodriguez, C.; Khonsari, M.R.; Faraji, A.; Sobhani, I. Characterization of Biliary Microbiota Dysbiosis in Extrahepatic Cholangiocarcinoma. PLoS ONE 2021, 16, e0247798. [Google Scholar] [CrossRef]
- Jia, X.; Lu, S.; Zeng, Z.; Liu, Q.; Dong, Z.; Chen, Y.; Zhu, Z.; Hong, Z.; Zhang, T.; Du, G.; et al. Characterization of Gut Microbiota, Bile Acid Metabolism, and Cytokines in Intrahepatic Cholangiocarcinoma. Hepatology 2020, 71, 893–906. [Google Scholar] [CrossRef]
- Reich, M.; Spomer, L.; Klindt, C.; Fuchs, K.; Stindt, J.; Deutschmann, K.; Höhne, J.; Liaskou, E.; Hov, J.R.; Karlsen, T.H.; et al. Downregulation of TGR5 (GPBAR1) in Biliary Epithelial Cells Contributes to the Pathogenesis of Sclerosing Cholangitis. J. Hepatol. 2021, 75, 634–646. [Google Scholar] [CrossRef] [PubMed]
- Hohenester, S.; Maillette de Buy Wenniger, L.; Paulusma, C.C.; van Vliet, S.J.; Jefferson, D.M.; Oude Elferink, R.P.; Beuers, U. A Biliary HCO3− Umbrella Constitutes a Protective Mechanism against Bile Acid-Induced Injury in Human Cholangiocytes. Hepatology 2012, 55, 173–183. [Google Scholar] [CrossRef]
- Gauss, A. Biliary Phosphatidylcholine and Lysophosphatidylcholine Profiles in Sclerosing Cholangitis. WJG 2013, 19, 5454. [Google Scholar] [CrossRef]
- Henriksen, E.K.K.; Viken, M.K.; Wittig, M.; Holm, K.; Folseraas, T.; Mucha, S.; Melum, E.; Hov, J.R.; Lazaridis, K.N.; Juran, B.D.; et al. HLA Haplotypes in Primary Sclerosing Cholangitis Patients of Admixed and Non-European Ancestry. HLA 2017, 90, 228–233. [Google Scholar] [CrossRef]
- The International IBD Genetics Consortium (IIBDGC); International Genetics of Ankylosing Spondylitis Consortium (IGAS); International PSC Study Group (IPSCSG); Genetic Analysis of Psoriasis Consortium (GAPC); Psoriasis Association Genetics Extension (PAGE); Ellinghaus, D.; Jostins, L.; Spain, S.L.; Cortes, A.; Bethune, J.; et al. Analysis of Five Chronic Inflammatory Diseases Identifies 27 New Associations and Highlights Disease-Specific Patterns at Shared Loci. Nat. Genet. 2016, 48, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Folseraas, T.; Liaskou, E.; Anderson, C.A.; Karlsen, T.H. Genetics in PSC: What Do the “Risk Genes” Teach Us? Clin. Rev. Allergy Immunol. 2015, 48, 154–164. [Google Scholar] [CrossRef]
- The UK-PSCSC Consortium; The International IBD Genetics Consortium; The International PSC Study Group; Liu, J.Z.; Hov, J.R.; Folseraas, T.; Ellinghaus, E.; Rushbrook, S.M.; Doncheva, N.T.; Andreassen, O.A.; et al. Dense Genotyping of Immune-Related Disease Regions Identifies Nine New Risk Loci for Primary Sclerosing Cholangitis. Nat. Genet. 2013, 45, 670–675. [Google Scholar] [CrossRef]
- Alvaro, D.; Gigliozzi, A.; Attili, A.F. Regulation and Deregulation of Cholangiocyte Proliferation. J. Hepatol. 2000, 33, 333–340. [Google Scholar] [CrossRef]
- Raven, A.; Lu, W.-Y.; Man, T.Y.; Ferreira-Gonzalez, S.; O’Duibhir, E.; Dwyer, B.J.; Thomson, J.P.; Meehan, R.R.; Bogorad, R.; Koteliansky, V.; et al. Cholangiocytes Act as Facultative Liver Stem Cells during Impaired Hepatocyte Regeneration. Nature 2017, 547, 350–354. [Google Scholar] [CrossRef]
- Carpino, G.; Cardinale, V.; Renzi, A.; Hov, J.R.; Berloco, P.B.; Rossi, M.; Karlsen, T.H.; Alvaro, D.; Gaudio, E. Activation of Biliary Tree Stem Cells within Peribiliary Glands in Primary Sclerosing Cholangitis. J. Hepatol. 2015, 63, 1220–1228. [Google Scholar] [CrossRef] [PubMed]
- DiPaola, F.; Shivakumar, P.; Pfister, J.; Walters, S.; Sabla, G.; Bezerra, J.A. Identification of Intramural Epithelial Networks Linked to Peribiliary Glands That Express Progenitor Cell Markers and Proliferate after Injury in Mice. Hepatology 2013, 58, 1486–1496. [Google Scholar] [CrossRef] [PubMed]
- Guicciardi, M.E.; Trussoni, C.E.; LaRusso, N.F.; Gores, G.J. The Spectrum of Reactive Cholangiocytes in Primary Sclerosing Cholangitis. Hepatology 2020, 71, 741–748. [Google Scholar] [CrossRef]
- Carpino, G.; Nevi, L.; Overi, D.; Cardinale, V.; Lu, W.; Di Matteo, S.; Safarikia, S.; Berloco, P.B.; Venere, R.; Onori, P.; et al. Peribiliary Gland Niche Participates in Biliary Tree Regeneration in Mouse and in Human Primary Sclerosing Cholangitis. Hepatology 2020, 71, 972–989. [Google Scholar] [CrossRef]
- Clerbaux, L.-A.; Manco, R.; Van Hul, N.; Bouzin, C.; Sciarra, A.; Sempoux, C.; Theise, N.D.; Leclercq, I.A. Invasive Ductular Reaction Operates Hepatobiliary Junctions upon Hepatocellular Injury in Rodents and Humans. Am. J. Pathol. 2019, 189, 1569–1581. [Google Scholar] [CrossRef]
- Sato, K.; Marzioni, M.; Meng, F.; Francis, H.; Glaser, S.; Alpini, G. Ductular Reaction in Liver Diseases: Pathological Mechanisms and Translational Significances. Hepatology 2019, 69, 420–430. [Google Scholar] [CrossRef]
- Mederacke, I.; Hsu, C.C.; Troeger, J.S.; Huebener, P.; Mu, X.; Dapito, D.H.; Pradere, J.-P.; Schwabe, R.F. Fate Tracing Reveals Hepatic Stellate Cells as Dominant Contributors to Liver Fibrosis Independent of Its Aetiology. Nat. Commun. 2013, 4, 2823. [Google Scholar] [CrossRef]
- Volckaert, T.; De Langhe, S. Lung Epithelial Stem Cells and Their Niches: Fgf10 Takes Center Stage. Fibrogenes. Tissue Repair. 2014, 7, 8. [Google Scholar] [CrossRef]
- Tabibian, J.H.; O’Hara, S.P.; Splinter, P.L.; Trussoni, C.E.; LaRusso, N.F. Cholangiocyte Senescence by Way of N-Ras Activation Is a Characteristic of Primary Sclerosing Cholangitis: Hepatology. Hepatology 2014, 59, 2263–2275. [Google Scholar] [CrossRef] [PubMed]
- Coppé, J.-P.; Desprez, P.-Y.; Krtolica, A.; Campisi, J. The Senescence-Associated Secretory Phenotype: The Dark Side of Tumor Suppression. Annu. Rev. Pathol. Mech. Dis. 2010, 5, 99–118. [Google Scholar] [CrossRef]
- O’Hara, S.P.; Splinter, P.L.; Trussoni, C.E.; Guicciardi, M.E.; Splinter, N.P.; Al Suraih, M.S.; Nasser-Ghodsi, N.; Stollenwerk, D.; Gores, G.J.; LaRusso, N.F. The Transcription Factor ETS1 Promotes Apoptosis Resistance of Senescent Cholangiocytes by Epigenetically Up-Regulating the Apoptosis Suppressor BCL2L1. J. Biol. Chem. 2019, 294, 18698–18713. [Google Scholar] [CrossRef] [PubMed]
- Boberg, K.M.; Schrumpf, E.; Bergquist, A.; Broomé, U.; Pares, A.; Remotti, H.; Schjölberg, A.; Spurkland, A.; Clausen, O.P.F. Cholangiocarcinoma in Primary Sclerosing Cholangitis: K-Ras Mutations and Tp53 Dysfunction Are Implicated in the Neoplastic Development. J. Hepatol. 2000, 32, 374–380. [Google Scholar] [CrossRef]
- Kamp, E.J.; Dinjens, W.N.; Doukas, M.; Van Marion, R.; Verheij, J.; Ponsioen, C.Y.; Bruno, M.J.; Groot Koerkamp, B.; Trivedi, P.J.; Peppelenbosch, M.P.; et al. Genetic Alterations during the Neoplastic Cascade towards Cholangiocarcinoma in Primary Sclerosing Cholangitis. J. Pathol. 2022, 258, 227–235. [Google Scholar] [CrossRef]
- Goeppert, B.; Folseraas, T.; Roessler, S.; Kloor, M.; Volckmar, A.; Endris, V.; Buchhalter, I.; Stenzinger, A.; Grzyb, K.; Grimsrud, M.M.; et al. Genomic Characterization of Cholangiocarcinoma in Primary Sclerosing Cholangitis Reveals Therapeutic Opportunities. Hepatology 2020, 72, 1253–1266. [Google Scholar] [CrossRef]
- Yamada, D.; Rizvi, S.; Razumilava, N.; Bronk, S.F.; Davila, J.I.; Champion, M.D.; Borad, M.J.; Bezerra, J.A.; Chen, X.; Gores, G.J. IL-33 Facilitates Oncogene-induced Cholangiocarcinoma in Mice by an Interleukin-6-sensitive Mechanism. Hepatology 2015, 61, 1627–1642. [Google Scholar] [CrossRef] [PubMed]
- Meng, F.; Yamagiwa, Y.; Ueno, Y.; Patel, T. Over-Expression of Interleukin-6 Enhances Cell Survival and Transformed Cell Growth in Human Malignant Cholangiocytes. J. Hepatol. 2006, 44, 1055–1065. [Google Scholar] [CrossRef]
- Frampton, G.; Invernizzi, P.; Bernuzzi, F.; Pae, H.Y.; Quinn, M.; Horvat, D.; Galindo, C.; Huang, L.; McMillin, M.; Cooper, B.; et al. Interleukin-6-Driven Progranulin Expression Increases Cholangiocarcinoma Growth by an Akt-Dependent Mechanism. Gut 2012, 61, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Jaiswal, M.; LaRusso, N.F.; Burgart, L.J.; Gores, G.J. Inflammatory Cytokines Induce DNA Damage and Inhibit DNA Repair in Cholangiocarcinoma Cells by a Nitric Oxide-Dependent Mechanism. Cancer Res. 2000, 60, 184–190. [Google Scholar]
- Ehlken, H.; Schramm, C. Primary Sclerosing Cholangitis and Cholangiocarcinoma: Pathogenesis and Modes of Diagnostics. Dig. Dis. 2013, 31, 118–125. [Google Scholar] [CrossRef]
- Finzi, L.; Shao, M.X.G.; Paye, F.; Housset, C.; Nadel, J.A. Lipopolysaccharide Initiates a Positive Feedback of Epidermal Growth Factor Receptor Signaling by Prostaglandin E2 in Human Biliary Carcinoma Cells. J. Immunol. 2009, 182, 2269–2276. [Google Scholar] [CrossRef] [PubMed]
- Lozano, E.; Sanchez-Vicente, L.; Monte, M.J.; Herraez, E.; Briz, O.; Banales, J.M.; Marin, J.J.G.; Macias, R.I.R. Cocarcinogenic Effects of Intrahepatic Bile Acid Accumulation in Cholangiocarcinoma Development. Mol. Cancer Res. 2014, 12, 91–100. [Google Scholar] [CrossRef]
- Melum, E.; Karlsen, T.H.; Schrumpf, E.; Bergquist, A.; Thorsby, E.; Boberg, K.M.; Lie, B.A. Cholangiocarcinoma in Primary Sclerosing Cholangitis Is Associated with NKG2D Polymorphisms. Hepatology 2007, 47, 90–96. [Google Scholar] [CrossRef]
- Yang, H.; Li, T.W.H.; Peng, J.; Tang, X.; Ko, K.S.; Xia, M.; Aller, M. A Mouse Model of Cholestasis-Associated Cholangiocarcinoma and Transcription Factors Involved in Progression. Gastroenterology 2011, 141, 378–388.e4. [Google Scholar] [CrossRef]
- Voigtländer, T.; Gupta, S.K.; Thum, S.; Fendrich, J.; Manns, M.P.; Lankisch, T.O.; Thum, T. MicroRNAs in Serum and Bile of Patients with Primary Sclerosing Cholangitis and/or Cholangiocarcinoma. PLoS ONE 2015, 10, e0139305. [Google Scholar] [CrossRef]
- Banales, J.M.; Cardinale, V.; Carpino, G.; Marzioni, M.; Andersen, J.B.; Invernizzi, P.; Lind, G.E.; Folseraas, T.; Forbes, S.J.; Fouassier, L.; et al. Cholangiocarcinoma: Current Knowledge and Future Perspectives Consensus Statement from the European Network for the Study of Cholangiocarcinoma (ENS-CCA). Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 261–280. [Google Scholar] [CrossRef]
- Fevery, J.; Verslype, C.; Lai, G.; Aerts, R.; Van Steenbergen, W. Incidence, Diagnosis, and Therapy of Cholangiocarcinoma in Patients with Primary Sclerosing Cholangitis. Dig. Dis. Sci. 2007, 52, 3123–3135. [Google Scholar] [CrossRef]
- Lazaridis, K.N.; Gores, G.J. Primary Sclerosing Cholangitis and Cholangiocarcinoma. Semin. Liver Dis. 2006, 26, 042–051. [Google Scholar] [CrossRef]
- Sainani, N.I.; Catalano, O.A.; Holalkere, N.-S.; Zhu, A.X.; Hahn, P.F.; Sahani, D.V. Cholangiocarcinoma: Current and Novel Imaging Techniques. Radiographics 2008, 28, 1263–1287. [Google Scholar] [CrossRef]
- Bowlus, C.L.; Arrivé, L.; Bergquist, A.; Deneau, M.; Forman, L.; Ilyas, S.I.; Lunsford, K.E.; Martinez, M.; Sapisochin, G.; Shroff, R.; et al. AASLD Practice Guidance on Primary Sclerosing Cholangitis and Cholangiocarcinoma. Hepatology 2023, 77, 659–702. [Google Scholar] [CrossRef]
- Zhang, Y.; Uchida, M.; Abe, T.; Nishimura, H.; Hayabuchi, N.; Nakashima, Y. Intrahepatic Peripheral Cholangiocarcinoma: Comparison of Dynamic CT and Dynamic MRI. J. Comput. Assist. Tomogr. 1999, 23, 670–677. [Google Scholar] [CrossRef]
- Vilgrain, V.; Van Beers, B.E.; Flejou, J.-F.; Belghiti, J.; Delos, M.; Gautier, A.-L.; Zins, M.; Denys, A.; Menu, Y. Intrahepatic Cholangiocarcinoma: MRI and Pathologic Correlation in 14 Patients. J. Comput. Assist. Tomogr. 1997, 21, 59–65. [Google Scholar] [CrossRef]
- Charatcharoenwitthaya, P.; Enders, F.B.; Halling, K.C.; Lindor, K.D. Utility of Serum Tumor Markers, Imaging, and Biliary Cytology for Detecting Cholangiocarcinoma in Primary Sclerosing Cholangitis. Hepatology 2008, 48, 1106–1117. [Google Scholar] [CrossRef]
- Schramm, C.; Eaton, J.; Ringe, K.I.; Venkatesh, S.; Yamamura, J. Recommendations on the Use of Magnetic Resonance Imaging in PSC-A Position Statement from the International PSC Study Group. Hepatology 2017, 66, 1675–1688. [Google Scholar] [CrossRef]
- Venkatesh, S.K.; Welle, C.L.; Miller, F.H.; Jhaveri, K.; Ringe, K.I.; Eaton, J.E.; Bungay, H.; Arrivé, L.; Ba-Ssalamah, A.; Grigoriadis, A.; et al. Reporting Standards for Primary Sclerosing Cholangitis Using MRI and MR Cholangiopancreatography: Guidelines from MR Working Group of the International Primary Sclerosing Cholangitis Study Group. Eur. Radiol. 2022, 32, 923–937. [Google Scholar] [CrossRef] [PubMed]
- Chapman, R.; Fevery, J.; Kalloo, A.; Nagorney, D.M.; Boberg, K.M.; Shneider, B.; Gores, G.J. Diagnosis and Management of Primary Sclerosing Cholangitis. Hepatology 2010, 51, 660–678. [Google Scholar] [CrossRef]
- Anderson, C. Fluorodeoxyglucose PET Imaging in the Evaluation of Gallbladder Carcinoma and Cholangiocarcinoma. J. Gastrointest. Surg. 2004, 8, 90–97. [Google Scholar] [CrossRef]
- Fevery, J.; Buchel, O.; Nevens, F.; Verslype, C.; Stroobants, S.; Steenbergen, W.V. Positron Emission Tomography Is Not a Reliable Method for the Early Diagnosis of Cholangiocarcinoma in Patients with Primary Sclerosing Cholangitis. J. Hepatol. 2005, 43, 358–360. [Google Scholar] [CrossRef]
- Wannhoff, A.; Brune, M.; Knierim, J.; Weiss, K.H.; Rupp, C.; Gotthardt, D.N. Longitudinal Analysis of CA19-9 Reveals Individualised Normal Range and Early Changes before Development of Biliary Tract Cancer in Patients with Primary Sclerosing Cholangitis. Aliment. Pharmacol. Ther. 2019, 49, 769–778. [Google Scholar] [CrossRef]
- Levy, C.; Lymp, J.; Angulo, P.; Gores, G.J.; Larusso, N.; Lindor, K.D. The Value of Serum CA 19-9 in Predicting Cholangiocarcinomas in Patients with Primary Sclerosing Cholangitis. Dig. Dis. Sci. 2005, 50, 1734–1740. [Google Scholar] [CrossRef]
- Wannhoff, A.; Hov, J.R.; Folseraas, T.; Rupp, C.; Friedrich, K.; Anmarkrud, J.A.; Weiss, K.H.; Sauer, P.; Schirmacher, P.; Boberg, K.M.; et al. FUT2 and FUT3 Genotype Determines CA19-9 Cut-off Values for Detection of Cholangiocarcinoma in Patients with Primary Sclerosing Cholangitis. J. Hepatol. 2013, 59, 1278–1284. [Google Scholar] [CrossRef]
- Sinakos, E.; Saenger, A.K.; Keach, J.; Kim, W.R.; Lindor, K.D. Many Patients with Primary Sclerosing Cholangitis and Increased Serum Levels of Carbohydrate Antigen 19-9 Do Not Have Cholangiocarcinoma. Clin. Gastroenterol. Hepatol. 2011, 9, 434–439.e1. [Google Scholar] [CrossRef]
- Akdoğan, M.; Parlak, E.; Kayhan, B.; Balk, M.; Saydam, G.; Sahin, B. Are Serum and Biliary Carcinoembryonic Antigen and Carbohydrate Antigen19-9 Determinations Reliable for Differentiation between Benign and Malignant Biliary Disease? Turk. J. Gastroenterol. 2003, 14, 181–184. [Google Scholar]
- Claessen, M.M.H.; Vleggaar, F.P.; Tytgat, K.M.A.J.; Siersema, P.D.; van Buuren, H.R. High Lifetime Risk of Cancer in Primary Sclerosing Cholangitis. J. Hepatol. 2009, 50, 158–164. [Google Scholar] [CrossRef]
- Wannhoff, A.; Rupp, C.; Friedrich, K.; Brune, M.; Knierim, J.; Flechtenmacher, C.; Sauer, P.; Stremmel, W.; Hov, J.R.; Schirmacher, P.; et al. Inflammation But Not Biliary Obstruction Is Associated with Carbohydrate Antigen 19-9 Levels in Patients with Primary Sclerosing Cholangitis. Clin. Gastroenterol. Hepatol. 2015, 13, 2372–2379. [Google Scholar] [CrossRef]
- Venkatesh, P.G.K.; Navaneethan, U.; Shen, B.; McCullough, A.J. Increased Serum Levels of Carbohydrate Antigen 19-9 and Outcomes in Primary Sclerosing Cholangitis Patients without Cholangiocarcinoma. Dig. Dis. Sci. 2013, 58, 850–857. [Google Scholar] [CrossRef]
- Wannhoff, A.; Rupp, C.; Friedrich, K.; Knierim, J.; Flechtenmacher, C.; Weiss, K.H.; Stremmel, W.; Gotthardt, D.N. Carcinoembryonic Antigen Level in Primary Sclerosing Cholangitis Is Not Influenced by Dominant Strictures or Bacterial Cholangitis. Dig. Dis. Sci. 2017, 62, 510–516. [Google Scholar] [CrossRef]
- Qin, X.-L.; Wang, Z.-R.; Shi, J.-S.; Lu, M.; Wang, L.; He, Q.-R. Utility of Serum CA19-9 in Diagnosis of Cholangiocarcinoma: In Comparison with CEA. WJG 2004, 10, 427. [Google Scholar] [CrossRef]
- Taghavi, S.A.; Eshraghian, A.; Niknam, R.; Sivandzadeh, G.R.; Bagheri Lankarani, K. Diagnosis of Cholangiocarcinoma in Primary Sclerosing Cholangitis. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 575–584. [Google Scholar] [CrossRef]
- Ramage, J.K.; Donaghy, A.; Farrant, J.M.; Iorns, R.; Williams, R. Serum Tumor Markers for the Diagnosis of Cholangiocarcinoma in Primary Sclerosing Cholangitis. Gastroenterology 1995, 108, 865–869. [Google Scholar] [CrossRef]
- Razumilava, N.; Gores, G.J. Cholangiocarcinoma. Lancet 2014, 383, 2168–2179. [Google Scholar] [CrossRef]
- Khan, S.A.; Davidson, B.R.; Goldin, R.D.; Heaton, N.; Karani, J.; Pereira, S.P.; Rosenberg, W.M.C.; Tait, P.; Taylor-Robinson, S.D.; Thillainayagam, A.V.; et al. Guidelines for the Diagnosis and Treatment of Cholangiocarcinoma: An Update. Gut 2012, 61, 1657–1669. [Google Scholar] [CrossRef]
- Park, M.-S.; Kim, T.K.; Kim, K.W.; Park, S.W.; Lee, J.K.; Kim, J.-S.; Lee, J.H.; Kim, K.A.; Kim, A.Y.; Kim, P.N.; et al. Differentiation of Extrahepatic Bile Duct Cholangiocarcinoma from Benign Stricture: Findings at MRCP versus ERCP. Radiology 2004, 233, 234–240. [Google Scholar] [CrossRef]
- Meagher, S.; Yusoff, I.; Kennedy, W.; Martel, M.; Adam, V.; Barkun, A. The Roles of Magnetic Resonance and Endoscopic Retrograde Cholangiopancreatography (MRCP and ERCP) in the Diagnosis of Patients with Suspected Sclerosing Cholangitis: A Cost-Effectiveness Analysis. Endoscopy 2007, 39, 222–228. [Google Scholar] [CrossRef]
- Majeed, A.; Castedal, M.; Arnelo, U.; Söderdahl, G.; Bergquist, A.; Said, K. Optimizing the Detection of Biliary Dysplasia in Primary Sclerosing Cholangitis before Liver Transplantation. Scand. J. Gastroenterol. 2018, 53, 56–63. [Google Scholar] [CrossRef]
- Trikudanathan, G.; Navaneethan, U.; Njei, B.; Vargo, J.J.; Parsi, M.A. Diagnostic Yield of Bile Duct Brushings for Cholangiocarcinoma in Primary Sclerosing Cholangitis: A Systematic Review and Meta-Analysis. Gastrointest. Endosc. 2014, 79, 783–789. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Xia, M.; Jin, Y.; Zheng, H.; Shen, Z.; Dai, W.; Li, X.; Kang, M.; Wan, R.; Lu, L.; et al. More Endoscopy-Based Brushing Passes Improve the Detection of Malignant Biliary Strictures: A Multicenter Randomized Controlled Trial. Am. J. Gastroenterol. 2022, 117, 733–739. [Google Scholar] [CrossRef]
- von Seth, E.; Ouchterlony, H.; Dobra, K.; Hjerpe, A.; Arnelo, U.; Haas, S.; Bergquist, A. Diagnostic Performance of a Stepwise Cytological Algorithm for Biliary Malignancy in Primary Sclerosing Cholangitis. Liver Int. 2019, 39, 382–388. [Google Scholar] [CrossRef] [PubMed]
- Baron, T.H.; Harewood, G.C.; Rumalla, A.; Pochron, N.L.; Stadheim, L.M.; Gores, G.J.; Therneau, T.M.; De Groen, P.C.; Sebo, T.J.; Salomao, D.R.; et al. A Prospective Comparison of Digital Image Analysis and Routine Cytology for the Identification of Malignancy in Biliary Tract Strictures. Clin. Gastroenterol. Hepatol. 2004, 2, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Karlsen, T.H.; Vesterhus, M.; Boberg, K.M. Review Article: Controversies in the Management of Primary Biliary Cirrhosis and Primary Sclerosing Cholangitis. Aliment. Pharmacol. Ther. 2014, 39, 282–301. [Google Scholar] [CrossRef]
- Weber, A.; von Weyhern, C.; Fend, F.; Schneider, J.; Neu, B.; Meining, A.; Weidenbach, H.; Schmid, R.M.; Prinz, C. Endoscopic Transpapillary Brush Cytology and Forceps Biopsy in Patients with Hilar Cholangiocarcinoma. WJG 2008, 14, 1097. [Google Scholar] [CrossRef]
- Lee, S.J.; Lee, Y.S.; Lee, M.G.; Lee, S.H.; Shin, E.; Hwang, J.-H. Triple-Tissue Sampling during Endoscopic Retrograde Cholangiopancreatography Increases the Overall Diagnostic Sensitivity for Cholangiocarcinoma. Gut Liver 2014, 8, 669–673. [Google Scholar] [CrossRef]
- Fung, B.M.; Tabibian, J.H. Primary Sclerosing Cholangitis-Associated Cholangiocarcinoma: Special Considerations and Best Practices. Expert Rev. Gastroenterol. Hepatol. 2021, 15, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Njei, B.; McCarty, T.R.; Varadarajulu, S.; Navaneethan, U. Systematic Review with Meta-Analysis: Endoscopic Retrograde Cholangiopancreatography-Based Modalities for the Diagnosis of Cholangiocarcinoma in Primary Sclerosing Cholangitis. Aliment. Pharmacol. Ther. 2016, 44, 1139–1151. [Google Scholar] [CrossRef]
- de Vries, A.B.; van der Heide, F.; Ter Steege, R.W.F.; Koornstra, J.J.; Buddingh, K.T.; Gouw, A.S.H.; Weersma, R.K. Limited Diagnostic Accuracy and Clinical Impact of Single-Operator Peroral Cholangioscopy for Indeterminate Biliary Strictures. Endoscopy 2020, 52, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Kaura, K.; Sawas, T.; Bazerbachi, F.; Storm, A.C.; Martin, J.A.; Gores, G.J.; Abu Dayyeh, B.K.; Topazian, M.D.; Levy, M.J.; Petersen, B.T.; et al. Cholangioscopy Biopsies Improve Detection of Cholangiocarcinoma When Combined with Cytology and FISH, but Not in Patients with PSC. Dig. Dis. Sci. 2020, 65, 1471–1478. [Google Scholar] [CrossRef] [PubMed]
- Fung, B.M.; Tabibian, J.H. Biliary Endoscopy in the Management of Primary Sclerosing Cholangitis and Its Complications. Liver Res. 2019, 3, 106–117. [Google Scholar] [CrossRef]
- Wu, L.-M.; Jiang, X.-X.; Gu, H.-Y.; Xu, X.; Zhang, W.; Lin, L.-H.; Deng, X.; Yin, Y.; Xu, J.-R. Endoscopic Ultrasound-Guided Fine-Needle Aspiration Biopsy in the Evaluation of Bile Duct Strictures and Gallbladder Masses: A Systematic Review and Meta-Analysis. Eur. J. Gastroenterol. Hepatol. 2011, 23, 113–120. [Google Scholar] [CrossRef]
- Raine, T.; Thomas, J.P.; Brais, R.; Godfrey, E.; Carroll, N.R.; Metz, A.J. Test Performance and Predictors of Accuracy of Endoscopic Ultrasound-Guided Fine-Needle Aspiration for Diagnosing Biliary Strictures or Masses. Endosc. Int. Open 2020, 8, E1537–E1544. [Google Scholar] [CrossRef]
- Razumilava, N.; Gleeson, F.C.; Gores, G.J. Awareness of Tract Seeding with Endoscopic Ultrasound Tissue Acquisition in Perihilar Cholangiocarcinoma. Am. J. Gastroenterol. 2015, 110, 200. [Google Scholar] [CrossRef][Green Version]
- Navaneethan, U.; Njei, B.; Venkatesh, P.G.; Lourdusamy, V.; Sanaka, M.R. Endoscopic Ultrasound in the Diagnosis of Cholangiocarcinoma as the Etiology of Biliary Strictures: A Systematic Review and Meta-Analysis. Gastroenterol. Rep. 2015, 3, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Lu, Y.; Wu, J.; Bie, L.; Xia, L.; Gong, B. Diagnostic Utility of Endoscopic Retrograde Cholangiography/Intraductal Ultrasound (ERC/IDUS) in Distinguishing Malignant from Benign Bile Duct Obstruction. Dig. Dis. Sci. 2016, 61, 610–617. [Google Scholar] [CrossRef]
- Sun, B.; Hu, B. The Role of Intraductal Ultrasonography in Pancreatobiliary Diseases. Endosc. Ultrasound 2016, 5, 291. [Google Scholar] [CrossRef]
- Meister, T. Intraductal Ultrasound Substantiates Diagnostics of Bile Duct Strictures of Uncertain Etiology. WJG 2013, 19, 874. [Google Scholar] [CrossRef]
- Corral, J.E.; Mousa, O.Y.; Krishna, M.; Levink, I.J.M.; Pursell, K.R.; Afsh, M.; Kröner, P.T.; Harnois, D.M.; Wolfsen, H.C.; Wallace, M.B.; et al. Volumetric Laser Endomicroscopy in the Biliary and Pancreatic Ducts: A Feasibility Study with Histological Correlation. Endoscopy 2018, 50, 1089–1094. [Google Scholar] [CrossRef]
- Tyberg, A.; Xu, M.; Gaidhane, M.; Kahaleh, M. Second Generation Optical Coherence Tomography: Preliminary Experience in Pancreatic and Biliary Strictures. Dig. Liver Dis. 2018, 50, 1214–1217. [Google Scholar] [CrossRef] [PubMed]
- Slivka, A.; Gan, I.; Jamidar, P.; Costamagna, G.; Cesaro, P.; Giovannini, M.; Caillol, F.; Kahaleh, M. Validation of the Diagnostic Accuracy of Probe-Based Confocal Laser Endomicroscopy for the Characterization of Indeterminate Biliary Strictures: Results of a Prospective Multicenter International Study. Gastrointest. Endosc. 2015, 81, 282–290. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.H.; Tabibian, J.H.; Nasser-Ghodsi, N.; Lennon, R.J.; DeLeon, T.; Borad, M.J.; Hilscher, M.; Silveira, M.G.; Carey, E.J.; Lindor, K.D. Surveillance for Hepatobiliary Cancers in Patients with Primary Sclerosing Cholangitis. Hepatology 2018, 67, 2338–2351. [Google Scholar] [CrossRef]
- Nicoletti, A.; Maurice, J.B.; Thorburn, D. Guideline Review: British Society of Gastroenterology/UK-PSC Guidelines for the Diagnosis and Management of Primary Sclerosing Cholangitis. Frontline Gastroenterol. 2021, 12, 62–66. [Google Scholar] [CrossRef]
- von Seth, E.; Arnelo, U.; Enochsson, L.; Bergquist, A. Primary Sclerosing Cholangitis Increases the Risk for Pancreatitis after Endoscopic Retrograde Cholangiopancreatography. Liver Int. 2015, 35, 254–262. [Google Scholar] [CrossRef] [PubMed]
- Rupp, C.; Hippchen, T.; Bruckner, T.; Klöters-Plachky, P.; Schaible, A.; Koschny, R.; Stiehl, A.; Gotthardt, D.N.; Sauer, P. Effect of Scheduled Endoscopic Dilatation of Dominant Strictures on Outcome in Patients with Primary Sclerosing Cholangitis. Gut 2019, 68, 2170–2178. [Google Scholar] [CrossRef]
- Jendrek, S.T.; Gotthardt, D.; Nitzsche, T.; Widmann, L.; Korf, T.; Michaels, M.A.; Weiss, K.-H.; Liaskou, E.; Vesterhus, M.; Karlsen, T.H.; et al. Anti-GP2 IgA Autoantibodies Are Associated with Poor Survival and Cholangiocarcinoma in Primary Sclerosing Cholangitis. Gut 2017, 66, 137–144. [Google Scholar] [CrossRef]
- Saffioti, F.; Roccarina, D.; Vesterhus, M.; Hov, J.R.; Rosenberg, W.; Pinzani, M.; Pereira, S.P.; Boberg, K.M.; Thorburn, D. Cholangiocarcinoma Is Associated with a Raised Enhanced Liver Fibrosis Score Independent of Primary Sclerosing Cholangitis. Eur. J. Clin. Investig. 2019, 49, e13088. [Google Scholar] [CrossRef]
- Cuenco, J.; Wehnert, N.; Blyuss, O.; Kazarian, A.; Whitwell, H.J.; Menon, U.; Dawnay, A.; Manns, M.P.; Pereira, S.P.; Timms, J.F. Identification of a Serum Biomarker Panel for the Differential Diagnosis of Cholangiocarcinoma and Primary Sclerosing Cholangitis. Oncotarget 2018, 9, 17430–17442. [Google Scholar] [CrossRef]
- Loosen, S.H.; Roderburg, C.; Kauertz, K.L.; Pombeiro, I.; Leyh, C.; Benz, F.; Vucur, M.; Longerich, T.; Koch, A.; Braunschweig, T.; et al. Elevated Levels of Circulating Osteopontin Are Associated with a Poor Survival after Resection of Cholangiocarcinoma. J. Hepatol. 2017, 67, 749–757. [Google Scholar] [CrossRef]
- Navaneethan, U.; Parsi, M.A.; Lourdusamy, V.; Bhatt, A.; Gutierrez, N.G.; Grove, D.; Sanaka, M.R.; Hammel, J.P.; Stevens, T.; Vargo, J.J.; et al. Volatile Organic Compounds in Bile for Early Diagnosis of Cholangiocarcinoma in Patients with Primary Sclerosing Cholangitis: A Pilot Study. Gastrointest. Endosc. 2015, 81, 943–949.e1. [Google Scholar] [CrossRef]
- Navaneethan, U.; Parsi, M.A.; Gutierrez, N.G.; Bhatt, A.; Venkatesh, P.G.K.; Lourdusamy, D.; Grove, D.; Hammel, J.P.; Jang, S.; Sanaka, M.R.; et al. Volatile Organic Compounds in Bile Can Diagnose Malignant Biliary Strictures in the Setting of Pancreatic Cancer: A Preliminary Observation. Gastrointest. Endosc. 2014, 80, 1038–1045. [Google Scholar] [CrossRef]
- Navaneethan, U.; Parsi, M.A.; Lourdusamy, D.; Grove, D.; Sanaka, M.R.; Hammel, J.P.; Vargo, J.J.; Dweik, R.A. Volatile Organic Compounds in Urine for Noninvasive Diagnosis of Malignant Biliary Strictures: A Pilot Study. Dig. Dis. Sci. 2015, 60, 2150–2157. [Google Scholar] [CrossRef]
- Ishikawa, A.; Sasaki, M.; Sato, Y.; Ohira, S.; Chen, M.-F.; Huang, S.-F.; Oda, K.; Nimura, Y.; Nakanuma, Y. Frequent P16ink4a Inactivation Is an Early and Frequent Event of Intraductal Papillary Neoplasm of the Liver Arising in Hepatolithiasis. Human. Pathol. 2004, 35, 1505–1514. [Google Scholar] [CrossRef]
- Nakamoto, S.; Kumamoto, Y.; Igarashi, K.; Fujiyama, Y.; Nishizawa, N.; Ei, S.; Tajima, H.; Kaizu, T.; Watanabe, M.; Yamashita, K. Methylated Promoter DNA of CDO1 Gene and Preoperative Serum CA19-9 Are Prognostic Biomarkers in Primary Extrahepatic Cholangiocarcinoma. PLoS ONE 2018, 13, e0205864. [Google Scholar] [CrossRef]
- Amornpisutt, R.; Proungvitaya, S.; Jearanaikoon, P.; Limpaiboon, T. DNA Methylation Level of OPCML and SFRP1: A Potential Diagnostic Biomarker of Cholangiocarcinoma. Tumor Biol. 2015, 36, 4973–4978. [Google Scholar] [CrossRef]
- Kim, B.; Cho, N.-Y.; Shin, S.H.; Kwon, H.-J.; Jang, J.J.; Kang, G.H. CpG Island Hypermethylation and Repetitive DNA Hypomethylation in Premalignant Lesion of Extrahepatic Cholangiocarcinoma. Virchows Arch. 2009, 455, 343–351. [Google Scholar] [CrossRef]
- Andresen, K.; Boberg, K.M.; Vedeld, H.M.; Honne, H.; Jebsen, P.; Hektoen, M.; Wadsworth, C.A.; Clausen, O.P.; Lundin, K.E.A.; Paulsen, V.; et al. Four DNA Methylation Biomarkers in Biliary Brush Samples Accurately Identify the Presence of Cholangiocarcinoma. Hepatology 2015, 61, 1651–1659. [Google Scholar] [CrossRef]
- Vedeld, H.M.; Grimsrud, M.M.; Andresen, K.; Pharo, H.D.; von Seth, E.; Karlsen, T.H.; Honne, H.; Paulsen, V.; Färkkilä, M.A.; Bergquist, A.; et al. Early and Accurate Detection of Cholangiocarcinoma in Patients with Primary Sclerosing Cholangitis by Methylation Markers in Bile. Hepatology 2022, 75, 59–73. [Google Scholar] [CrossRef]
- Klump, B.; Hsieh, C.-J.; Dette, S.; Holzmann, K.; Kiebetalich, R.; Jung, M.; Sinn, U.; Ortner, M.; Porschen, R.; Gregor, M. Promoter Methylation of INK4a/ARF as Detected in Bile-Significance for the Differential Diagnosis in Biliary Disease. Clin. Cancer Res. 2003, 9, 1773–1778. [Google Scholar]
- Shin, S.-H.; Lee, K.; Kim, B.-H.; Cho, N.-Y.; Jang, J.-Y.; Kim, Y.-T.; Kim, D.; Jang, J.J.; Kang, G.H. Bile-Based Detection of Extrahepatic Cholangiocarcinoma with Quantitative DNA Methylation Markers and Its High Sensitivity. J. Mol. Diagn. 2012, 14, 256–263. [Google Scholar] [CrossRef]
- Sriraksa, R.; Zeller, C.; El-Bahrawy, M.A.; Dai, W.; Daduang, J.; Jearanaikoon, P.; Chau-in, S.; Brown, R.; Limpaiboon, T. CpG-Island Methylation Study of Liver Fluke-Related Cholangiocarcinoma. Br. J. Cancer 2011, 104, 1313–1318. [Google Scholar] [CrossRef][Green Version]
- Wasenang, W.; Chaiyarit, P.; Proungvitaya, S.; Limpaiboon, T. Serum Cell-Free DNA Methylation of OPCML and HOXD9 as a Biomarker That May Aid in Differential Diagnosis between Cholangiocarcinoma and Other Biliary Diseases. Clin. Epigenet. 2019, 11, 39. [Google Scholar] [CrossRef]
- Branchi, V.; Schaefer, P.; Semaan, A.; Kania, A.; Lingohr, P.; Kalff, J.C.; Schäfer, N.; Kristiansen, G.; Dietrich, D.; Matthaei, H. Promoter Hypermethylation of SHOX2 and SEPT9 Is a Potential Biomarker for Minimally Invasive Diagnosis in Adenocarcinomas of the Biliary Tract. Clin. Epigenet. 2016, 8, 133. [Google Scholar] [CrossRef]
- Letelier, P.; Riquelme, I.; Hernández, A.; Guzmán, N.; Farías, J.; Roa, J. Circulating MicroRNAs as Biomarkers in Biliary Tract Cancers. Int. J. Mol. Sci. 2016, 17, 791. [Google Scholar] [CrossRef]
- Marin, J.J.G.; Bujanda, L.; Banales, J.M. MicroRNAs and Cholestatic Liver Diseases. Curr. Opin. Gastroenterol. 2014, 30, 303–309. [Google Scholar] [CrossRef]
- Li, L.; Masica, D.; Ishida, M.; Tomuleasa, C.; Umegaki, S.; Kalloo, A.N.; Georgiades, C.; Singh, V.K.; Khashab, M.; Amateau, S.; et al. Human Bile Contains MicroRNA-Laden Extracellular Vesicles That Can Be Used for Cholangiocarcinoma Diagnosis. Hepatology 2014, 60, 896–907. [Google Scholar] [CrossRef]
- Bernuzzi, F.; Marabita, F.; Lleo, A.; Carbone, M.; Mirolo, M.; Marzioni, M.; Alpini, G.; Alvaro, D.; Boberg, K.M.; Locati, M.; et al. Serum microRNAs as Novel Biomarkers for Primary Sclerosing Cholangitis and Cholangiocarcinoma. Clin. Exp. Immunol. 2016, 185, 61–71. [Google Scholar] [CrossRef]
- Loosen, S.H.; Lurje, G.; Wiltberger, G.; Vucur, M.; Koch, A.; Kather, J.N.; Paffenholz, P.; Tacke, F.; Ulmer, F.T.; Trautwein, C.; et al. Serum Levels of miR-29, miR-122, miR-155 and miR-192 Are Elevated in Patients with Cholangiocarcinoma. PLoS ONE 2019, 14, e0210944. [Google Scholar] [CrossRef]
- Correa-Gallego, C.; Maddalo, D.; Doussot, A.; Kemeny, N.; Kingham, T.P.; Allen, P.J.; D’Angelica, M.I.; DeMatteo, R.P.; Betel, D.; Klimstra, D.; et al. Circulating Plasma Levels of MicroRNA-21 and MicroRNA-221 Are Potential Diagnostic Markers for Primary Intrahepatic Cholangiocarcinoma. PLoS ONE 2016, 11, e0163699. [Google Scholar] [CrossRef]
- Miolo, G.; Muraro, E.; Caruso, D.; Crivellari, D.; Ash, A.; Scalone, S.; Lombardi, D.; Rizzolio, F.; Giordano, A.; Corona, G. Pharmacometabolomics Study Identifies Circulating Spermidine and Tryptophan as Potential Biomarkers Associated with the Complete Pathological Response to Trastuzumab-Paclitaxel Neoadjuvant Therapy in HER-2 Positive Breast Cancer. Oncotarget 2016, 7, 39809–39822. [Google Scholar] [CrossRef]
- Hensley, C.T.; Faubert, B.; Yuan, Q.; Lev-Cohain, N.; Jin, E.; Kim, J.; Jiang, L.; Ko, B.; Skelton, R.; Loudat, L.; et al. Metabolic Heterogeneity in Human Lung Tumors. Cell 2016, 164, 681–694. [Google Scholar] [CrossRef]
- Banales, J.M.; Iñarrairaegui, M.; Arbelaiz, A.; Milkiewicz, P.; Muntané, J.; Muñoz-Bellvis, L.; La Casta, A.; Gonzalez, L.M.; Arretxe, E.; Alonso, C.; et al. Serum Metabolites as Diagnostic Biomarkers for Cholangiocarcinoma, Hepatocellular Carcinoma, and Primary Sclerosing Cholangitis. Hepatology 2019, 70, 547–562. [Google Scholar] [CrossRef]
- Metzger, J.; Negm, A.A.; Plentz, R.R.; Weismüller, T.J.; Wedemeyer, J.; Karlsen, T.H.; Dakna, M.; Mullen, W.; Mischak, H.; Manns, M.P.; et al. Urine Proteomic Analysis Differentiates Cholangiocarcinoma from Primary Sclerosing Cholangitis and Other Benign Biliary Disorders. Gut 2013, 62, 122–130. [Google Scholar] [CrossRef]
- Lankisch, T.O.; Metzger, J.; Negm, A.A.; Voβkuhl, K.; Siwy, J.; Weismüller, T.J.; Schneider, A.S.; Thedieck, K.; Baumeister, R.; Zürbig, P.; et al. Bile Proteomic Profiles Differentiate Cholangiocarcinoma from Primary Sclerosing Cholangitis and Choledocholithiasis. Hepatology 2011, 53, 875–884. [Google Scholar] [CrossRef]
- Voigtländer, T.; Metzger, J.; Schönemeier, B.; Jäger, M.; Mischak, H.; Manns, M.P.; Lankisch, T.O. A Combined Bile and Urine Proteomic Test for Cholangiocarcinoma Diagnosis in Patients with Biliary Strictures of Unknown Origin. United Eur. Gastroenterol. J. 2017, 5, 668–676. [Google Scholar] [CrossRef]
- Betesh, L.; Comunale, M.A.; Wang, M.; Liang, H.; Hafner, J.; Karabudak, A.; Giama, N.H.; Moser, C.D.; Miyoshi, E.; Roberts, L.R.; et al. Identification of Fucosylated Fetuin-A as a Potential Biomarker for Cholangiocarcinoma. Prot. Clin. Appl. 2017, 11, 1600141. [Google Scholar] [CrossRef]
- Lapitz, A.; Arbelaiz, A.; Olaizola, P.; Aranburu, A.; Bujanda, L.; Perugorria, M.J.; Banales, J.M. Extracellular Vesicles in Hepatobiliary Malignancies. Front. Immunol. 2018, 9, 2270. [Google Scholar] [CrossRef]
- Hirsova, P.; Ibrahim, S.H.; Verma, V.K.; Morton, L.A.; Shah, V.H.; LaRusso, N.F.; Gores, G.J.; Malhi, H. Extracellular Vesicles in Liver Pathobiology: Small Particles with Big Impact. Hepatology 2016, 64, 2219–2233. [Google Scholar] [CrossRef] [PubMed]
- Arbelaiz, A.; Azkargorta, M.; Krawczyk, M.; Santos-Laso, A.; Lapitz, A.; Perugorria, M.J.; Erice, O.; Gonzalez, E.; Jimenez-Agüero, R.; Lacasta, A.; et al. Serum Extracellular Vesicles Contain Protein Biomarkers for Primary Sclerosing Cholangitis and Cholangiocarcinoma. Hepatology 2017, 66, 1125–1143. [Google Scholar] [CrossRef] [PubMed]
- Lapitz, A.; Arbelaiz, A.; O’Rourke, C.J.; Lavin, J.L.; Casta, A.L.; Ibarra, C.; Jimeno, J.P.; Santos-Laso, A.; Izquierdo-Sanchez, L.; Krawczyk, M.; et al. Patients with Cholangiocarcinoma Present Specific RNA Profiles in Serum and Urine Extracellular Vesicles Mirroring the Tumor Expression: Novel Liquid Biopsy Biomarkers for Disease Diagnosis. Cells 2020, 9, 721. [Google Scholar] [CrossRef]
- Lapitz, A.; Azkargorta, M.; Milkiewicz, P.; Olaizola, P.; Zhuravleva, E.; Grimsrud, M.M.; Schramm, C.; Arbelaiz, A.; O’Rourke, C.J.; La Casta, A.; et al. Liquid Biopsy-Based Protein Biomarkers for Risk Prediction, Early Diagnosis, and Prognostication of Cholangiocarcinoma. J. Hepatol. 2023, 79, 93–108. [Google Scholar] [CrossRef]
- Valle, J.W.; Kelley, R.K.; Nervi, B.; Oh, D.-Y.; Zhu, A.X. Biliary Tract Cancer. Lancet 2021, 397, 428–444. [Google Scholar] [CrossRef] [PubMed]
- Singhi, A.D.; Nikiforova, M.N.; Chennat, J.; Papachristou, G.I.; Khalid, A.; Rabinovitz, M.; Das, R.; Sarkaria, S.; Ayasso, M.S.; Wald, A.I.; et al. Integrating Next-Generation Sequencing to Endoscopic Retrograde Cholangiopancreatography (ERCP)-Obtained Biliary Specimens Improves the Detection and Management of Patients with Malignant Bile Duct Strictures. Gut 2020, 69, 52–61. [Google Scholar] [CrossRef]
- Arechederra, M.; Rullán, M.; Amat, I.; Oyon, D.; Zabalza, L.; Elizalde, M.; Latasa, M.U.; Mercado, M.R.; Ruiz-Clavijo, D.; Saldaña, C.; et al. Next-Generation Sequencing of Bile Cell-Free DNA for the Early Detection of Patients with Malignant Biliary Strictures. Gut 2022, 71, 1141–1151. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Catanzaro, E.; Gringeri, E.; Burra, P.; Gambato, M. Primary Sclerosing Cholangitis-Associated Cholangiocarcinoma: From Pathogenesis to Diagnostic and Surveillance Strategies. Cancers 2023, 15, 4947. https://doi.org/10.3390/cancers15204947
Catanzaro E, Gringeri E, Burra P, Gambato M. Primary Sclerosing Cholangitis-Associated Cholangiocarcinoma: From Pathogenesis to Diagnostic and Surveillance Strategies. Cancers. 2023; 15(20):4947. https://doi.org/10.3390/cancers15204947
Chicago/Turabian StyleCatanzaro, Elisa, Enrico Gringeri, Patrizia Burra, and Martina Gambato. 2023. "Primary Sclerosing Cholangitis-Associated Cholangiocarcinoma: From Pathogenesis to Diagnostic and Surveillance Strategies" Cancers 15, no. 20: 4947. https://doi.org/10.3390/cancers15204947
APA StyleCatanzaro, E., Gringeri, E., Burra, P., & Gambato, M. (2023). Primary Sclerosing Cholangitis-Associated Cholangiocarcinoma: From Pathogenesis to Diagnostic and Surveillance Strategies. Cancers, 15(20), 4947. https://doi.org/10.3390/cancers15204947