

Menopausal Status Contributes to Overall Survival in Endometrial Cancer Patients



Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients’ Characteristics
2.2. Laboratory Tests
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
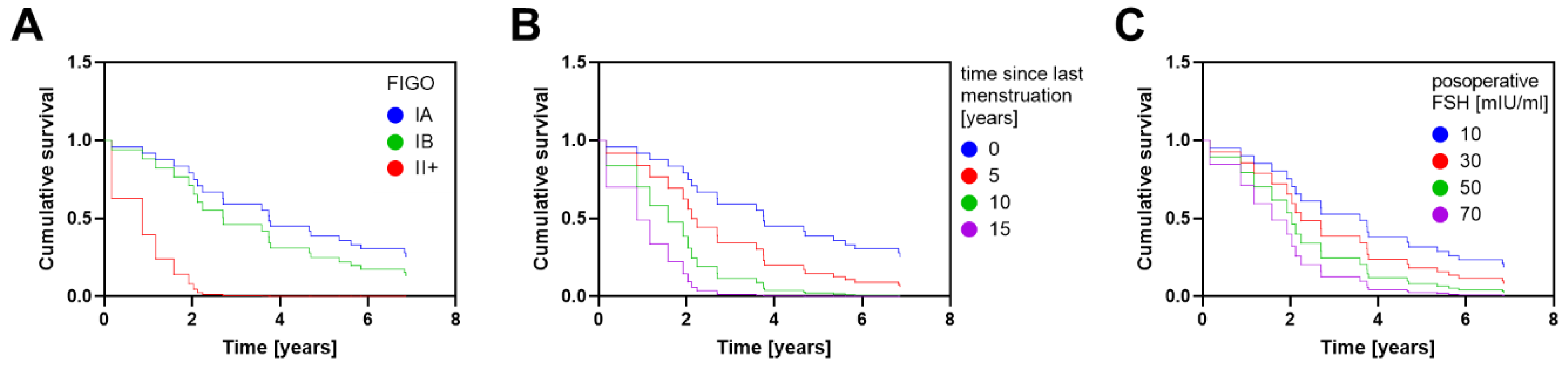
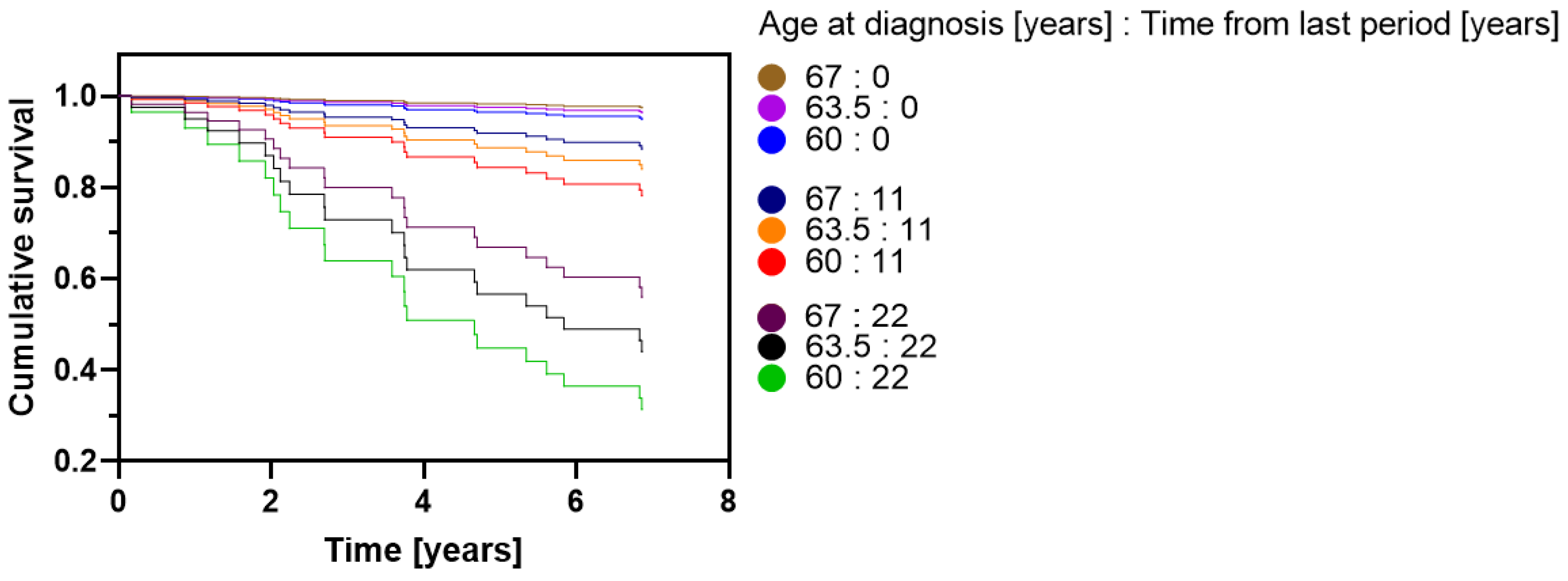
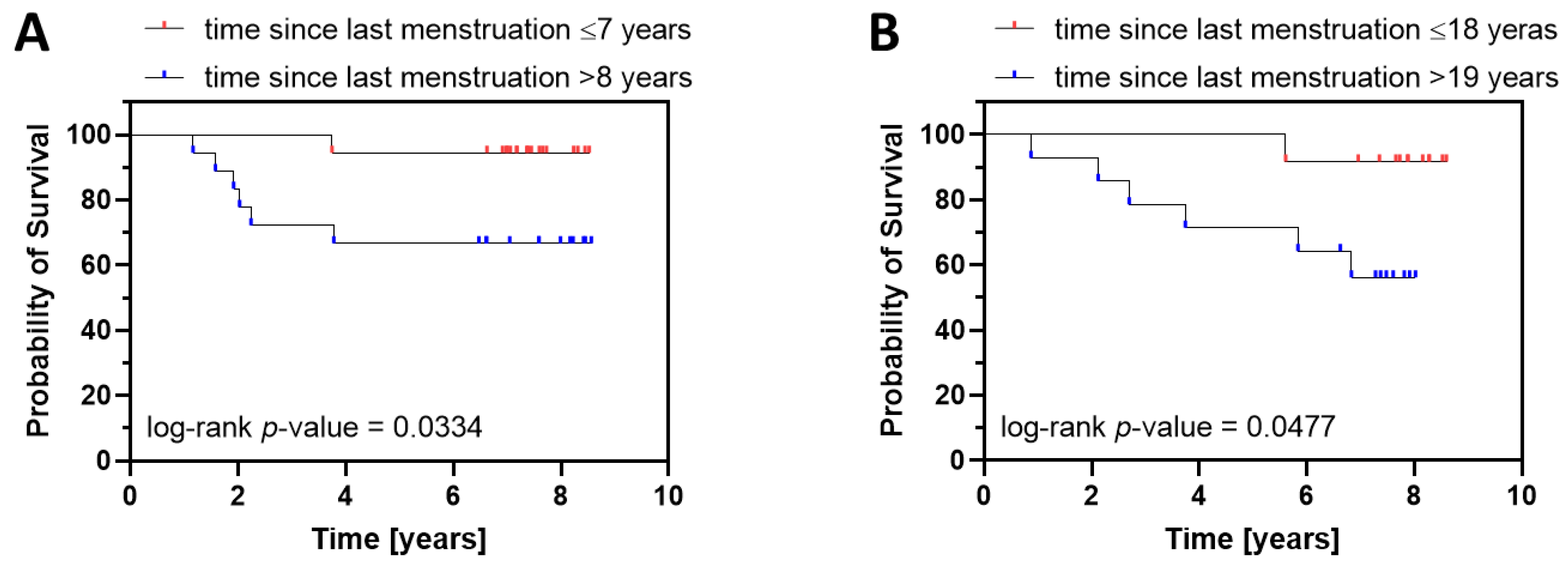
3.2. Effects of Prognostic Factors on Overall Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Amant, F.; Moerman, P.; Neven, P.; Timmerman, D.; Van Limbergen, E.; Vergote, I. Endometrial cancer. Lancet 2005, 366, 491–505. [Google Scholar] [CrossRef] [PubMed]
- Benedetti Panici, P.; Basile, S.; Salerno, M.G.; Di Donato, V.; Marchetti, C.; Perniola, G.; Palagiano, A.; Perutelli, A.; Maneschi, F.; Lissoni, A.A.; et al. Secondary analyses from a randomized clinical trial: Age as the key prognostic factor in endometrial carcinoma. Am. J. Obstet. Gynecol. 2014, 210, 363.e1–363.e10. [Google Scholar] [CrossRef]
- Ouldamer, L.; Bendifallah, S.; Body, G.; Touboul, C.; Graesslin, O.; Raimond, E.; Collinet, P.; Coutant, C.; Lavoué, V.; Lévêque, J.; et al. Predicting poor prognosis recurrence in women with endometrial cancer: A nomogram developed by the FRANCOGYN study group. Br. J. Cancer 2016, 115, 1296–1303. [Google Scholar] [CrossRef] [PubMed]
- Cancer Genome Atlas Research Network; Kandoth, C.; Schultz, N.; Cherniack, A.D.; Akbani, R.; Liu, Y.; Shen, H.; Robertson, A.G.; Pashtan, I.; Shen, R.; et al. Integrated genomic characterization of endometrial carcinoma. Nature 2013, 497, 67–73. [Google Scholar] [CrossRef]
- Talhouk, A.; McConechy, M.K.; Leung, S.; Yang, W.; Lum, A.; Senz, J.; Boyd, N.; Pike, J.; Anglesio, M.; Kwon, J.S.; et al. Confirmation of ProMisE: A simple, genomics-based clinical classifier for endometrial cancer. Cancer 2017, 123, 802–813. [Google Scholar] [CrossRef]
- McAlpine, J.; Leon-Castillo, A.; Bosse, T. The rise of a novel classification system for endometrial carcinoma; integration of molecular subclasses. J. Pathol. 2018, 244, 538–549. [Google Scholar] [CrossRef] [PubMed]
- Torrente, M.; Sousa, P.A.; Hernández, R.; Blanco, M.; Calvo, V.; Collazo, A.; Guerreiro, G.R.; Núñez, B.; Pimentao, J.; Sánchez, J.C.; et al. An Artificial Intelligence-Based Tool for Data Analysis and Prognosis in Cancer Patients: Results from the Clarify Study. Cancers 2022, 14, 4041. [Google Scholar] [CrossRef]
- Abdol Manap, N.; Ng, B.K.; Phon, S.E.; Abdul Karim, A.K.; Lim, P.S.; Fadhil, M. Endometrial Cancer in Pre-Menopausal Women and Younger: Risk Factors and Outcome. Int. J. Environ. Res. Public Health 2022, 19, 9059. [Google Scholar] [CrossRef]
- Schach, E.; Kothari, J.; Perkiss, E.; Hutchinson-Colas, J.; Turock, H.; McGreevey, J.; Bachmann, G.; NJ Commission on Women’s Reentry Health Committee. Symptomatic menopause: Additional challenges for incarcerated women. Maturitas 2021, 150, 37–41. [Google Scholar] [CrossRef]
- Morabia, A.; Costanza, M.C. International variability in ages at menarche, first livebirth, and menopause. World Health Organization Collaborative Study of Neoplasia and Steroid Contraceptives. Am. J. Epidemiol. 1998, 148, 1195–1205. [Google Scholar] [CrossRef]
- Hillard, T. Diagnosis of perimenopause and menopause (Section 5). NICE guideline—Menopause: Diagnosis and management. Post Reprod. Health 2016, 22, 56–58. [Google Scholar] [CrossRef] [PubMed]
- Soares, C.N.; Almeida, O.P.; Joffe, H.; Cohen, L.S. Efficacy of estradiol for the treatment of depressive disorders in perimenopausal women: A double-blind, randomized, placebo-controlled trial. Arch. Gen. Psychiatry 2001, 58, 529–534. [Google Scholar] [CrossRef] [PubMed]
- Bompoula, M.S.; Valsamakis, G.; Neofytou, S.; Messaropoulos, P.; Salakos, N.; Mastorakos, G.; Kalantaridou, S.N. Demographic, clinical and hormonal characteristics of patients with premature ovarian insufficiency and those of early menopause: Data from two tertiary premature ovarian insufficiency centers in Greece. Gynecol. Endocrinol. 2020, 36, 693–697. [Google Scholar] [CrossRef] [PubMed]
- Abildgaard, J.; Tingstedt, J.; Zhao, Y.; Hartling, H.J.; Pedersen, A.T.; Lindegaard, B.; Dam Nielsen, S. Increased systemic inflammation and altered distribution of T-cell subsets in postmenopausal women. PLoS ONE 2020, 15, e0235174. [Google Scholar] [CrossRef]
- Sasada, S.; Yunokawa, M.; Takehara, Y.; Ishikawa, M.; Ikeda, S.; Kato, T.; Tamura, K. Baseline risk of recurrence in stage I-II endometrial carcinoma. J. Gynecol. Oncol. 2018, 29, e9. [Google Scholar] [CrossRef] [PubMed]
- Dou, Y.; Song, K.; Fu, Y.; Shen, Y.; Zhang, C.; Yao, S.; Xu, C.; Xia, M.; Lou, G.; Liu, J.; et al. Risk Factors and Prognosis of Early Recurrence in Stage I-II Endometrial Cancer: A Large-Scale, Multi-Center, and Retrospective Study. Front. Med. 2022, 9, 808037. [Google Scholar] [CrossRef]
- Creutzberg, C.L.; van Putten, W.L.; Koper, P.C.; Lybeert, M.L.; Jobsen, J.J.; Wárlám-Rodenhuis, C.C.; De Winter, K.A.; Lutgens, L.C.; van den Bergh, A.C.; van de Steen-Banasik, E.; et al. Surgery and postoperative radiotherapy versus surgery alone for patients with stage-1 endometrial carcinoma: Multicentre randomised trial. PORTEC Study Group. Post Operative Radiation Therapy in Endometrial Carcinoma. Lancet 2000, 355, 1404–1411. [Google Scholar] [CrossRef]
- Singh, N.; Hirschowitz, L.; Zaino, R.; Alvarado-Cabrero, I.; Duggan, M.A.; Ali-Fehmi, R.; Euscher, E.; Hecht, J.L.; Horn, L.C.; Ioffe, O.; et al. Pathologic Prognostic Factors in Endometrial Carcinoma (Other Than Tumor Type and Grade). Int. J. Gynecol. Pathol. 2019, 38 (Suppl. 1), S93–S113. [Google Scholar] [CrossRef]
- Kolehmainen, A.; Pasanen, A.; Tuomi, T.; Koivisto-Korander, R.; Bützow, R.; Loukovaara, M. Clinical factors as prognostic variables among molecular subgroups of endometrial cancer. PLoS ONE 2020, 15, e0242733. [Google Scholar] [CrossRef]
- Celik, E.; Kizildag Yirgin, I.; Goksever Celik, H.; Engin, G.; Sozen, H.; Ak, N.; Saip, P.; Onder, S.; Topuz, S.; Salihoglu, M.Y. Does visceral adiposity have an effect on the survival outcomes of the patients with endometrial cancer? J. Obstet. Gynaecol. Res. 2021, 47, 560–569. [Google Scholar] [CrossRef]
- Yu, Z.; Wei, S.; Zhang, J.; Shi, R.; An, L.; Feng, D.; Wang, H. Development and Validation of a Novel Prognostic Model for Endometrial Cancer Based on Clinical Characteristics. Cancer Manag. Res. 2021, 13, 8879–8886. [Google Scholar] [CrossRef]
- Gemer, O.; Segev, Y.; Helpman, L.; Hag-Yahia, N.; Eitan, R.; Raban, O.; Vaknin, Z.; Leytes, S.; Ben Arie, A.; Amit, A.; et al. Is there a survival advantage in diagnosing endometrial cancer in asymptomatic postmenopausal patients? An Israeli Gynecology Oncology Group study. Am. J. Obstet. Gynecol. 2018, 219, 181.e1–181.e6. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Cong, R.; Kong, F.; Ma, J.; Wu, Q.; Ma, X. Fibrinogen Is a Coagulation Marker Associated with the Prognosis of Endometrial Cancer. OncoTargets Ther. 2019, 12, 9947–9956. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.; Chen, Y.; Zhu, Y.; Wu, Q.; Yao, C.; Xia, H.; Li, C. Postoperative Systemic Immune-Inflammation Index (SII): A Superior Prognostic Factor of Endometrial Cancer. Front. Surg. 2021, 8, 704235. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Zhang, J.; Fan, X.; Ma, J.; He, J.; Kang, S.; Cheng, J.; Ma, J. Identification of risk factors for the prognosis of Chinese patients with endometrial carcinoma. Medicine 2021, 100, e27305. [Google Scholar] [CrossRef]
- Nakanishi, T.; Ishikawa, H.; Suzuki, Y.; Inoue, T.; Nakamura, S.; Kuzuya, K. Association between menopausal state and prognosis of endometrial cancer. Int. J. Gynecol. Cancer 2001, 11, 483–487. [Google Scholar] [CrossRef]
- Gottwald, L.; Chałubińska, J.; Moszyńska-Zielińska, M.; Piekarski, J.; Tyliński, W.; Szwalski, J.; Kubiak, R.; Pasz-Walczak, G.; Hendzel, K.; Ciałkowska-Rysz, A. Endometrioid endometrial cancer—The prognostic value of selected clinical and pathological parameters. Ginekol. Pol. 2011, 82, 743–748. [Google Scholar]
- Laban, M.; El-Swaify, S.T.; Ali, S.H.; Refaat, M.A.; Sabbour, M.; Farrag, N. Preoperative detection of occult endometrial malignancies in endometrial hyperplasia to improve primary surgical therapy: A scoping review of the literature. Int. J. Gynaecol. Obstet. 2022, 159, 21–42. [Google Scholar] [CrossRef]
- Rajadurai, V.A.; Chivers, P.; Ayres, C.; Mohan, G.R.; Stewart, C.; Leung, Y.C.; Wan, K.M.; Cohen, P.A. Predictors of endometrial carcinoma in patients with atypical endometrial hyperplasia at a tertiary gynaecological cancer centre in Western Australia. Aust. N. Z. J. Obstet. Gynaecol. 2021, 61, 275–283. [Google Scholar] [CrossRef]
- Karakas, L.A.; Atilgan, A.O.; Akilli, H.; Kuscu, U.E.; Haberal, A.; Ayhan, A. Nulliparity and postmenopausal status are independent factors of malignancy potential of endometrial intraepithelial neoplasia in polyps. Int. J. Gynaecol. Obstet. 2021, 152, 433–438. [Google Scholar] [CrossRef]
- Allen, N.E.; Key, T.J.; Dossus, L.; Rinaldi, S.; Cust, A.; Lukanova, A.; Peeters, P.H.; Onland-Moret, N.C.; Lahmann, P.H.; Berrino, F.; et al. Endogenous sex hormones and endometrial cancer risk in women in the European Prospective Investigation into Cancer and Nutrition (EPIC). Endocr. Relat. Cancer 2008, 15, 485–497. [Google Scholar] [CrossRef] [PubMed]
- Kanat-Pektas, M.; Yenicesu, O.; Gungor, T.; Bilge, U. Predictive power of sexual hormones and tumor markers in endometrial cancer. Arch. Gynecol. Obstet. 2010, 281, 709–715. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Value |
|---|---|
| Median (range) Age, years | 63.5 (37–86) |
| Median age of menarche (range) Age, years | 14 (10–19) |
| Median age of menopause (range) Age, years | 52 (37–61) |
| Median time from menopause to cancer diagnosis (range) years | 11 (0–38) |
| Median (range) BMI kg/m2 | 32.0 (19.6–46.6) |
| BMI category, n (%) | |
| Normal | 10 (10.9%) |
| Overweight | 25 (27.2%) |
| Obese | 57 (62.0%) |
| Tumor differentiation grade, n (%) | |
| G1 | 19 (20.7%) |
| G2 | 66 (71.7%) |
| G3 | 7 (7.6%) |
| FIGO stage, n (%) | |
| IA | 52 (56.5%) |
| IB | 22 (23.9%) |
| II–IV | 18 (19.6%) |
| Endometrioid histology, n (%) | 92 (100%) |
| Surgical treatment, n (%) | |
| TAH/TLH + BSO | 40 (43.5%) |
| TAH/TLH + BSO + LND | 52 (56.5%) |
| Type of adjuvant treatment, n (%) | |
| None | 34 (37.0%) |
| Brachy ± external beam radiotherapy | 58 (63.0%) |
| No of patients who recurred, n (%) | 15 (16.3%) |
| Overall survival rate, n (%) | |
| FIGO IA | 46 (88.5%) |
| FIGO IB | 18 (81.8%) |
| FIGO II–IV | 7 (38.9%) |
| Parameter | Value |
|---|---|
| Mean CA125 serum concentration (range) [U/mL] | 232.1 (4.7–11336.0) |
| Mean HE4 serum concentration (range) [pmol/l] | 190.3 (34.3–3137.0) |
| Mean preoperative LH serum concentration (range) [IU/mL] | 20.3 (2.6–48.7) |
| Mean preoperative FSH serum concentration (range) [mIU/mL] | 46.9 (1.1–97.5) |
| Mean postoperative LH serum concentration (range) [IU/mL] | 22.4 (0.1–53.7) |
| Mean postoperative FSH serum concentration (range) [mIU/mL] | 50.1 (1.0–116.0) |
| Variable | Hazard Ratio | 95% CI (Profile Likelihood) | p-Value |
|---|---|---|---|
| Age [years] | 0.9060 | 0.7943 to 1.039 | 0.1460 |
| FIGO [IB vs IA] | 1.468 | 0.3410 to 5.856 | 0.5866 |
| FIGO [II–IV vs IA] | 10.77 | 3.514 to 37.95 | <0.0001 (*) |
| BMI [kg/m2] | 1.041 | 0.9559 to 1.137 | 0.3582 |
| adjuvant treatment [brachytherapy vs. no adjuvant treatment] | 0.9537 | 0.3633 to 2.581 | 0.9235 |
| parity [number of offspring] | 0.8941 | 0.6172 to 1.254 | 0.5326 |
| time since last menstruation [years] | 1.151 | 1.003 to 1.329 | 0.0478 (*) |
| postoperative FSH serum concentration [mIU/mL] | 1.020 | 0.9997 to 1.040 | 0.0493 (*) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barczyński, B.; Frąszczak, K.; Wnorowski, A.; Kotarski, J. Menopausal Status Contributes to Overall Survival in Endometrial Cancer Patients. Cancers 2023, 15, 451. https://doi.org/10.3390/cancers15020451
Barczyński B, Frąszczak K, Wnorowski A, Kotarski J. Menopausal Status Contributes to Overall Survival in Endometrial Cancer Patients. Cancers. 2023; 15(2):451. https://doi.org/10.3390/cancers15020451
Chicago/Turabian StyleBarczyński, Bartłomiej, Karolina Frąszczak, Artur Wnorowski, and Jan Kotarski. 2023. "Menopausal Status Contributes to Overall Survival in Endometrial Cancer Patients" Cancers 15, no. 2: 451. https://doi.org/10.3390/cancers15020451
APA StyleBarczyński, B., Frąszczak, K., Wnorowski, A., & Kotarski, J. (2023). Menopausal Status Contributes to Overall Survival in Endometrial Cancer Patients. Cancers, 15(2), 451. https://doi.org/10.3390/cancers15020451