Figure 1.
Categories and progress overview of neuroendocrine tumor biomarkers.
Figure 1.
Categories and progress overview of neuroendocrine tumor biomarkers.
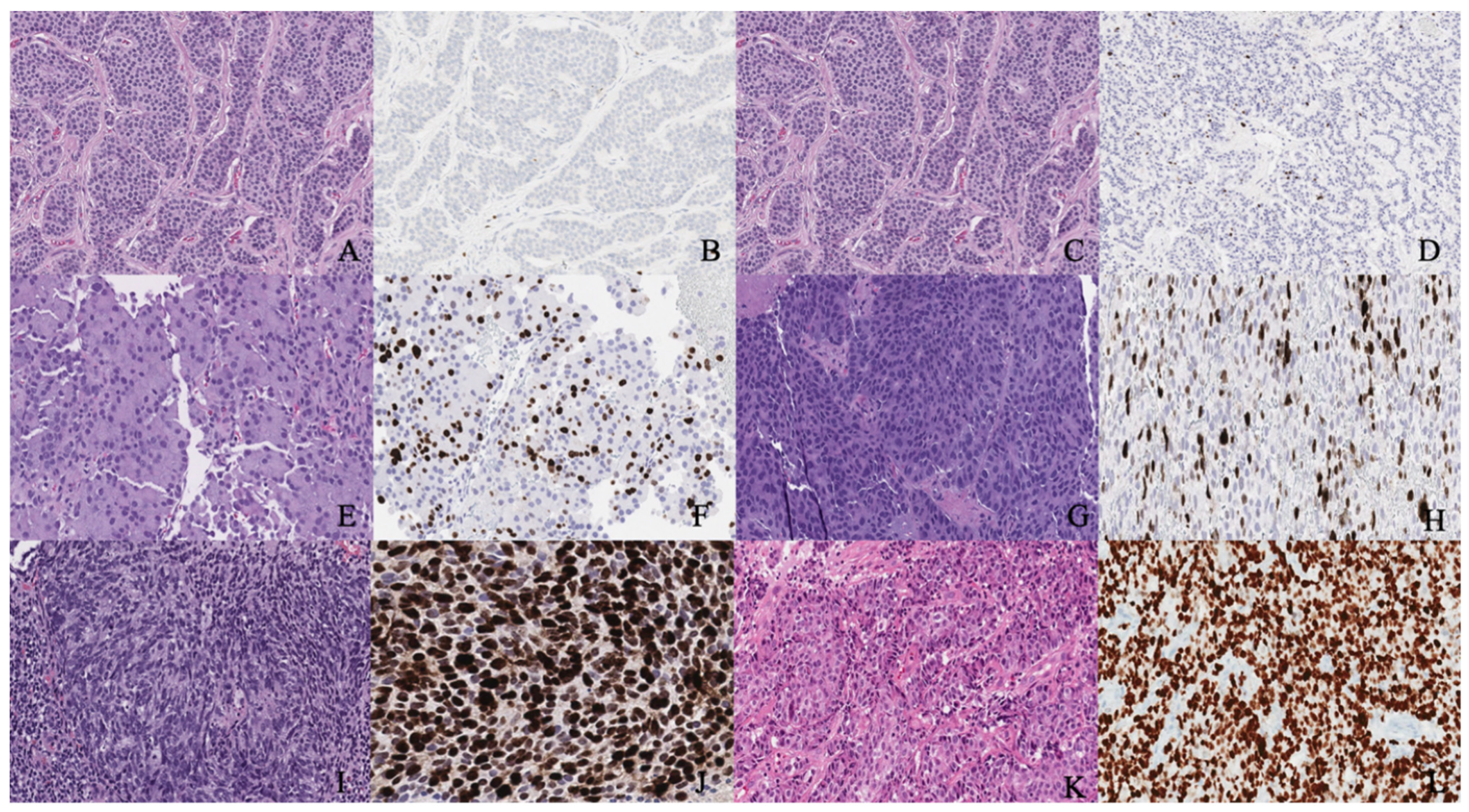
Figure 2.
(A,B) Well-differentiated NET grade 1. (A) Well-differentiated neuroendocrine tumor grade 1 (low grade) with an organoid pattern, with a meshwork of thin fibrovascular septa surrounding nests of tumor cells. Tumor cells are uniform with a polygonal shape, round to oval nuclei with salt and pepper chromatin, inconspicuous nucleoli, and moderate to abundant eosinophilic cytoplasm. (B) The Ki67 immunohistochemical stain shows a proliferation rate of 2%. (C,D) Well-differentiated NET grade 2. (C) Neuroendocrine cells in a well-differentiated neuroendocrine tumor, grade 2. Tumor cells are relatively uniform and round. The nuclear chromatin is finely granular. (D) The Ki67 immunohistochemical stain shows a proliferation rate of 10%. (E,F) Well-differentiated NET grade 3. (E) Neuroendocrine cells in a well-differentiated neuroendocrine tumor, grade 3. Tumor cells are relatively uniform and round with eosinophilic cytoplasm. The nuclear chromatin is granular. (F) The Ki67 immunohistochemical stain shows a proliferation rate of 30–40%. (G,H) Poorly differentiated neuroendocrine carcinoma. (G) The tumor shows solid nests of poorly differentiated epithelioid cells with dense chromatin. (H) Ki67 immunohistochemical stain shows a proliferation rate of 80%. (I,J) Small cell carcinoma. (I) Sheets of oval blue cells with minimal cytoplasm. The chromatin is dense. Nuclei demonstrate molding and smudging. (J) Ki67 shows a proliferation index of 80%. (K,L) Large cell neuroendocrine carcinoma. (K) Tumor cells with sheets of large, epithelioid cells. Cytologic features show abundant cytoplasm, coarse chromatin, nuclear pleomorphism, and prominent nucleoli. (L) Ki67 is greater than 90%.
Figure 2.
(A,B) Well-differentiated NET grade 1. (A) Well-differentiated neuroendocrine tumor grade 1 (low grade) with an organoid pattern, with a meshwork of thin fibrovascular septa surrounding nests of tumor cells. Tumor cells are uniform with a polygonal shape, round to oval nuclei with salt and pepper chromatin, inconspicuous nucleoli, and moderate to abundant eosinophilic cytoplasm. (B) The Ki67 immunohistochemical stain shows a proliferation rate of 2%. (C,D) Well-differentiated NET grade 2. (C) Neuroendocrine cells in a well-differentiated neuroendocrine tumor, grade 2. Tumor cells are relatively uniform and round. The nuclear chromatin is finely granular. (D) The Ki67 immunohistochemical stain shows a proliferation rate of 10%. (E,F) Well-differentiated NET grade 3. (E) Neuroendocrine cells in a well-differentiated neuroendocrine tumor, grade 3. Tumor cells are relatively uniform and round with eosinophilic cytoplasm. The nuclear chromatin is granular. (F) The Ki67 immunohistochemical stain shows a proliferation rate of 30–40%. (G,H) Poorly differentiated neuroendocrine carcinoma. (G) The tumor shows solid nests of poorly differentiated epithelioid cells with dense chromatin. (H) Ki67 immunohistochemical stain shows a proliferation rate of 80%. (I,J) Small cell carcinoma. (I) Sheets of oval blue cells with minimal cytoplasm. The chromatin is dense. Nuclei demonstrate molding and smudging. (J) Ki67 shows a proliferation index of 80%. (K,L) Large cell neuroendocrine carcinoma. (K) Tumor cells with sheets of large, epithelioid cells. Cytologic features show abundant cytoplasm, coarse chromatin, nuclear pleomorphism, and prominent nucleoli. (L) Ki67 is greater than 90%.
![Cancers 14 01835 g002]()
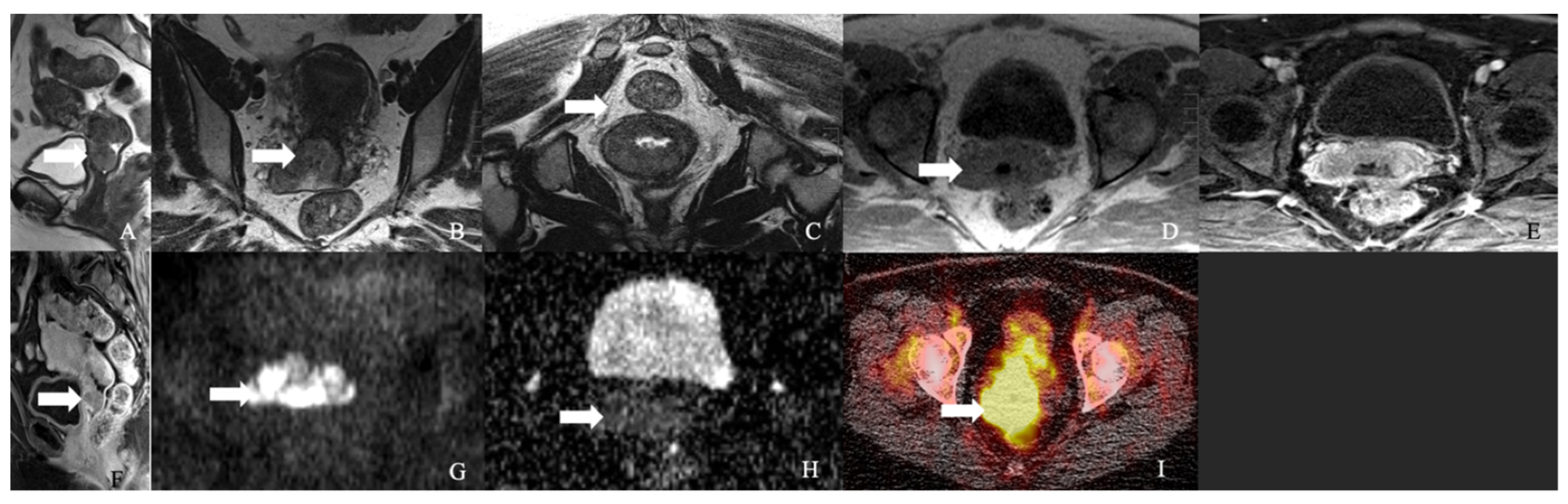
Figure 3.
A 62-year-old female with neuroendocrine carcinoma of the cervix. (A) Sagittal T2 weighted image, (B) axial T2 weighted image, (C) oblique T2 weighted image, (D) axial pre-contrast T1 weighted image, (E) axial fat-saturated post-contrast T1 weighted image, (F) sagittal fat-saturated post-contrast T1 weighted image, (G) axial diffusion-weighted images (B-100), (H) axial apparent diffusion coefficient MRI images, and (I) Axial Ga-68 dotatate PET/CT image demonstrate a FDG avid enhancing mass in the cervix (arrow) with restricted diffusion and no parametrium involvement. The mass biopsy reported a small cell neuroendocrine carcinoma.
Figure 3.
A 62-year-old female with neuroendocrine carcinoma of the cervix. (A) Sagittal T2 weighted image, (B) axial T2 weighted image, (C) oblique T2 weighted image, (D) axial pre-contrast T1 weighted image, (E) axial fat-saturated post-contrast T1 weighted image, (F) sagittal fat-saturated post-contrast T1 weighted image, (G) axial diffusion-weighted images (B-100), (H) axial apparent diffusion coefficient MRI images, and (I) Axial Ga-68 dotatate PET/CT image demonstrate a FDG avid enhancing mass in the cervix (arrow) with restricted diffusion and no parametrium involvement. The mass biopsy reported a small cell neuroendocrine carcinoma.
Figure 4.
A 52-year-old female with a neuroendocrine tumor of the cervix uteri. (A) Transverse and (B) sagittal ultrasound image of the cervix demonstrates a heterogenous cervical mass (arrow) measuring about 14 cm. (C) Sagittal T2 weighted image, (D) sagittal apparent diffusion coefficient map, and (E) sagittal fat-saturated post-contrast T1 weighted MRI images demonstrate a mass in the cervix uteri (arrow) with restricted diffusion. The mass biopsy reported a small cell neuroendocrine tumor of grade G3.
Figure 4.
A 52-year-old female with a neuroendocrine tumor of the cervix uteri. (A) Transverse and (B) sagittal ultrasound image of the cervix demonstrates a heterogenous cervical mass (arrow) measuring about 14 cm. (C) Sagittal T2 weighted image, (D) sagittal apparent diffusion coefficient map, and (E) sagittal fat-saturated post-contrast T1 weighted MRI images demonstrate a mass in the cervix uteri (arrow) with restricted diffusion. The mass biopsy reported a small cell neuroendocrine tumor of grade G3.
Figure 5.
2018 FIGO staging system for cervical cancer. Stage I, confined to the cervix. Stage IA, ≤5 mm depth. Stage IA1, ≤3 mm depth. Stage IA2, 3 mm and ≤5 mm depth. Stage IB, >5 mm depth. Stage IB1, ≤2 cm maximum diameter. Stage IB2, >2 cm and ≤4 cm maximum diameter. Stage IB3, >4 cm maximum diameter. Stage II, beyond the uterus but not involving the lower one-third of the vagina or pelvic sidewall. Stage IIA, upper two-thirds of the vagina. Stage IIA1, upper two-thirds of the vagina and ≤4 cm. Stage IIA2, Upper two-thirds of the vagina and >4 cm. Stage IIB, parametrial invasion. Stage III, lower vagina, pelvic sidewall, ureters, and lymph nodes. Stage IIIA, lower one-third of the vagina. Stage IIIB, pelvic sidewall. Stage IIIC, pelvic, and para-aortic lymph node involvement. Stage IIIC1, pelvic lymph node involvement. Stage IIIC2, para-aortic lymph node involvement. Stage IV, adjacent and distant organs. Stage IVA, rectal or bladder involvement. Stage IVB, distant organs outside the pelvis.
Figure 5.
2018 FIGO staging system for cervical cancer. Stage I, confined to the cervix. Stage IA, ≤5 mm depth. Stage IA1, ≤3 mm depth. Stage IA2, 3 mm and ≤5 mm depth. Stage IB, >5 mm depth. Stage IB1, ≤2 cm maximum diameter. Stage IB2, >2 cm and ≤4 cm maximum diameter. Stage IB3, >4 cm maximum diameter. Stage II, beyond the uterus but not involving the lower one-third of the vagina or pelvic sidewall. Stage IIA, upper two-thirds of the vagina. Stage IIA1, upper two-thirds of the vagina and ≤4 cm. Stage IIA2, Upper two-thirds of the vagina and >4 cm. Stage IIB, parametrial invasion. Stage III, lower vagina, pelvic sidewall, ureters, and lymph nodes. Stage IIIA, lower one-third of the vagina. Stage IIIB, pelvic sidewall. Stage IIIC, pelvic, and para-aortic lymph node involvement. Stage IIIC1, pelvic lymph node involvement. Stage IIIC2, para-aortic lymph node involvement. Stage IV, adjacent and distant organs. Stage IVA, rectal or bladder involvement. Stage IVB, distant organs outside the pelvis.
![Cancers 14 01835 g005]()
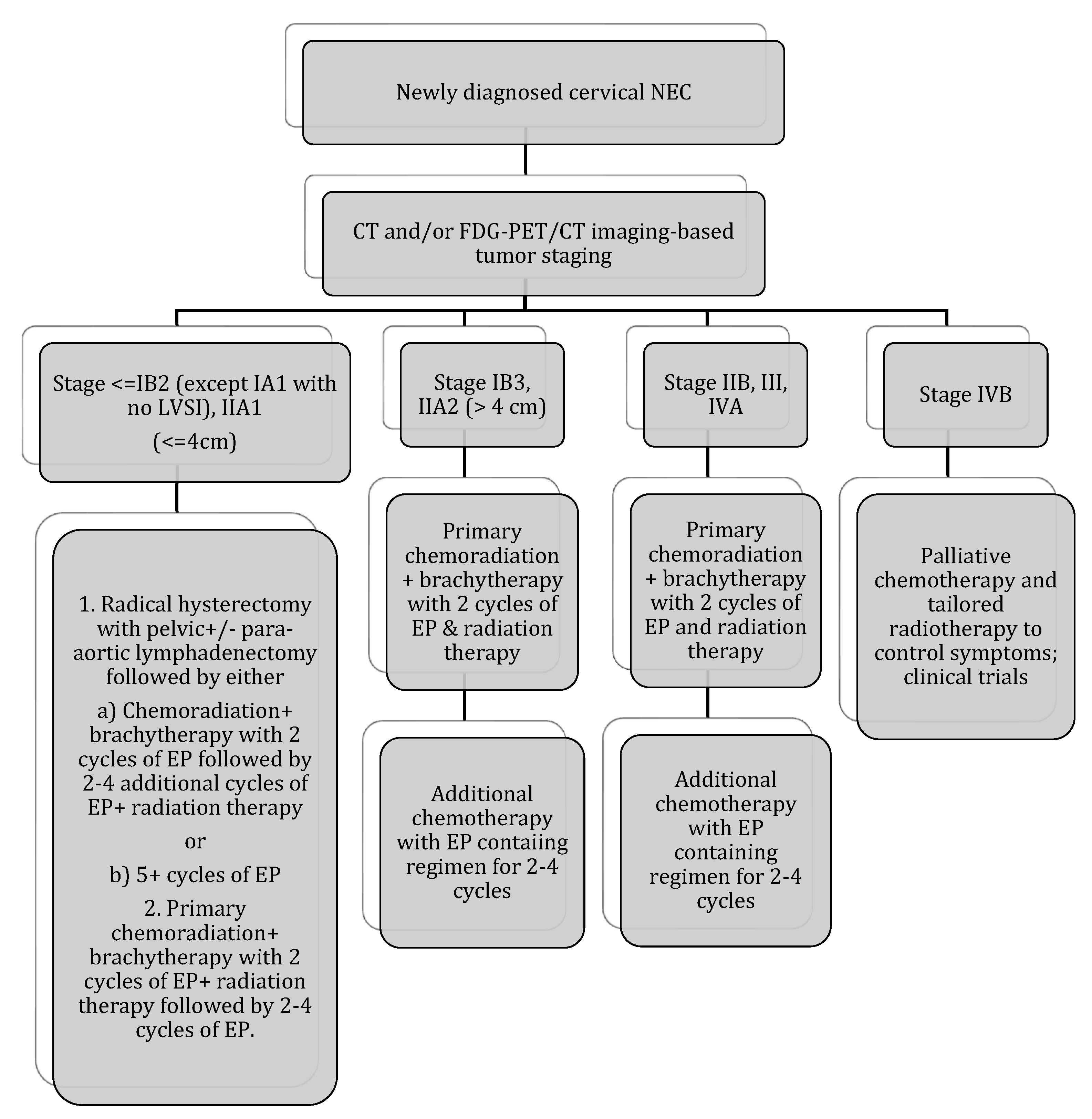
Figure 6.
Stage-based treatment algorithm for cervical neuroendocrine carcinoma [
2]. NEC: neuroendocrine carcinoma; LVSI: lymphovascular space invasion; EP: etoposide and cisplatin; chemotherapy with EP alone: cisplatin 60–80 mg/m
2 on day 1 every 3 weeks and etoposide 80–120 mg/m
2 on days 1–3 every 3 weeks (with growth factor support); chemotherapy with EP + radiation therapy: 2 cycles of EP q3 weeks (cisplatin 60 mg/m
2 and etoposide 100 mg/m
2 given on day 1 of 21 day cycle) during radiation therapy followed by an additional 2–4 cycles of EP alone (recommended regimen). Radiotherapy: 40–45 Gy external beam radiotherapy ±40–45 Gy brachytherapy (modified from Winer et al.).
Figure 6.
Stage-based treatment algorithm for cervical neuroendocrine carcinoma [
2]. NEC: neuroendocrine carcinoma; LVSI: lymphovascular space invasion; EP: etoposide and cisplatin; chemotherapy with EP alone: cisplatin 60–80 mg/m
2 on day 1 every 3 weeks and etoposide 80–120 mg/m
2 on days 1–3 every 3 weeks (with growth factor support); chemotherapy with EP + radiation therapy: 2 cycles of EP q3 weeks (cisplatin 60 mg/m
2 and etoposide 100 mg/m
2 given on day 1 of 21 day cycle) during radiation therapy followed by an additional 2–4 cycles of EP alone (recommended regimen). Radiotherapy: 40–45 Gy external beam radiotherapy ±40–45 Gy brachytherapy (modified from Winer et al.).
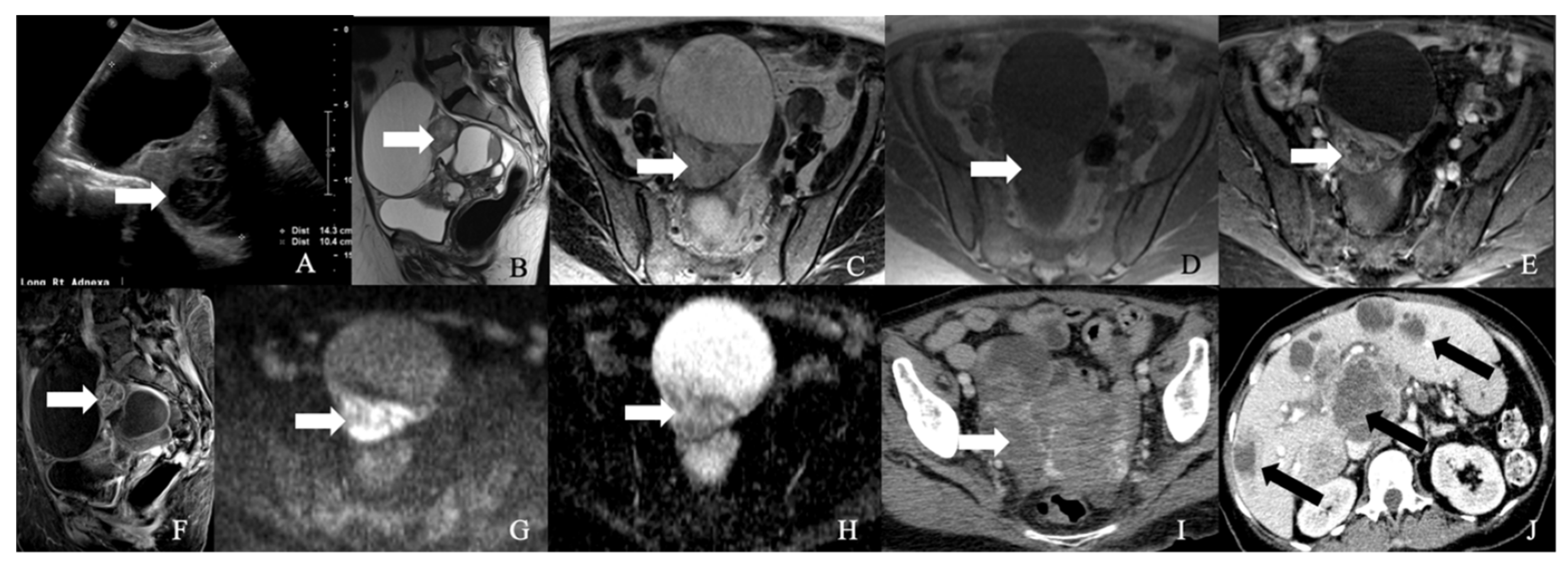
Figure 7.
52-year-old female with a neuroendocrine tumor of the ovary. (A) Transverse ultrasound image of the pelvis demonstrates a heterogeneous mass in the pelvis (arrow) measuring about 14 cm. (B) Sagittal T2 weighted image, (C) axial T2 weighted image, (D) axial pre-contrast T1 weighted image, (E) axial fat-saturated post-contrast T1 weighted image, (F) sagittal fat-saturated post-contrast T1 weighted image, (G) axial diffusion-weighted images (B-100), (H) axial apparent diffusion coefficient images demonstrate a multiloculated mass with enhancing nodule (arrow) and restricted diffusion, (I) axial post-contrast CT image of the pelvis shows the heterogenous mass (arrow), and (J) axial post-contrast CT image of the abdomen demonstrates the multiple hepatic metastases (arrow). The mass was resected, and a biopsy reported neuroendocrine tumor of the ovary with synaptophysin, CD56, CK7, and CDX-2 were positive, and chromogranin was focally positive, with a Ki67 index of less than 5%.
Figure 7.
52-year-old female with a neuroendocrine tumor of the ovary. (A) Transverse ultrasound image of the pelvis demonstrates a heterogeneous mass in the pelvis (arrow) measuring about 14 cm. (B) Sagittal T2 weighted image, (C) axial T2 weighted image, (D) axial pre-contrast T1 weighted image, (E) axial fat-saturated post-contrast T1 weighted image, (F) sagittal fat-saturated post-contrast T1 weighted image, (G) axial diffusion-weighted images (B-100), (H) axial apparent diffusion coefficient images demonstrate a multiloculated mass with enhancing nodule (arrow) and restricted diffusion, (I) axial post-contrast CT image of the pelvis shows the heterogenous mass (arrow), and (J) axial post-contrast CT image of the abdomen demonstrates the multiple hepatic metastases (arrow). The mass was resected, and a biopsy reported neuroendocrine tumor of the ovary with synaptophysin, CD56, CK7, and CDX-2 were positive, and chromogranin was focally positive, with a Ki67 index of less than 5%.
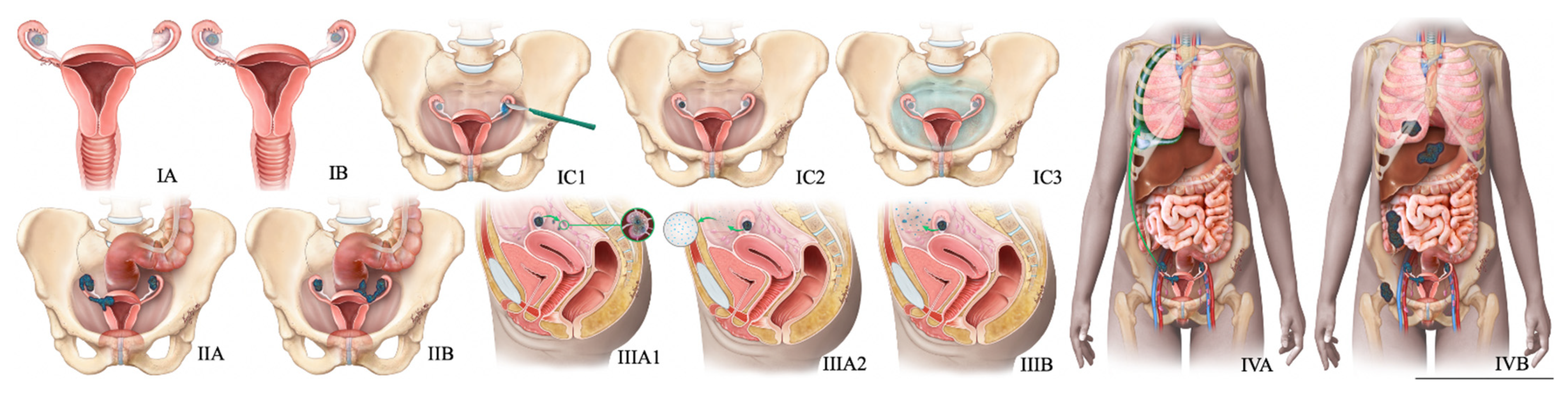
Figure 8.
FIGO staging system for ovarian cancer. In stage IA cancer, the tumor is limited to one ovary or fallopian tube. The tumor is limited to both ovaries or fallopian tubes in stage IB cancer. Stage IC1 cancer results from the intraoperative spill. In stage IC3 cancer, malignant cells are found in ascites or peritoneal washings. In stage IIA, the tumor extends to or is implanted on (or both) uterus or fallopian tubes (or both). Stage IIIA1 cancer shows positive retroperitoneal lymph nodes. Stage IIIA2 cancer, microscopic, extrapelvic (above pelvic brim) peritoneal involvement is seen with or without positive retroperitoneal lymph nodes. Stage IIIB or stage IIIC cancer, macroscopic, extrapelvic (above pelvic brim) peritoneal involvement is seen with or without positive retroperitoneal lymph nodes (≤2 cm for stage IIIB and >2 cm for stage IIIC). Stage IVA cancer indicates pleural effusion with positive cytology. Stage IVB cancer, hepatic or splenic parenchymal metastasis is seen (or both) and metastasis to extra-abdominal organs.
Figure 8.
FIGO staging system for ovarian cancer. In stage IA cancer, the tumor is limited to one ovary or fallopian tube. The tumor is limited to both ovaries or fallopian tubes in stage IB cancer. Stage IC1 cancer results from the intraoperative spill. In stage IC3 cancer, malignant cells are found in ascites or peritoneal washings. In stage IIA, the tumor extends to or is implanted on (or both) uterus or fallopian tubes (or both). Stage IIIA1 cancer shows positive retroperitoneal lymph nodes. Stage IIIA2 cancer, microscopic, extrapelvic (above pelvic brim) peritoneal involvement is seen with or without positive retroperitoneal lymph nodes. Stage IIIB or stage IIIC cancer, macroscopic, extrapelvic (above pelvic brim) peritoneal involvement is seen with or without positive retroperitoneal lymph nodes (≤2 cm for stage IIIB and >2 cm for stage IIIC). Stage IVA cancer indicates pleural effusion with positive cytology. Stage IVB cancer, hepatic or splenic parenchymal metastasis is seen (or both) and metastasis to extra-abdominal organs.
![Cancers 14 01835 g008]()
Figure 9.
Diagnostic algorithm for ovarian NENs.
Figure 9.
Diagnostic algorithm for ovarian NENs.
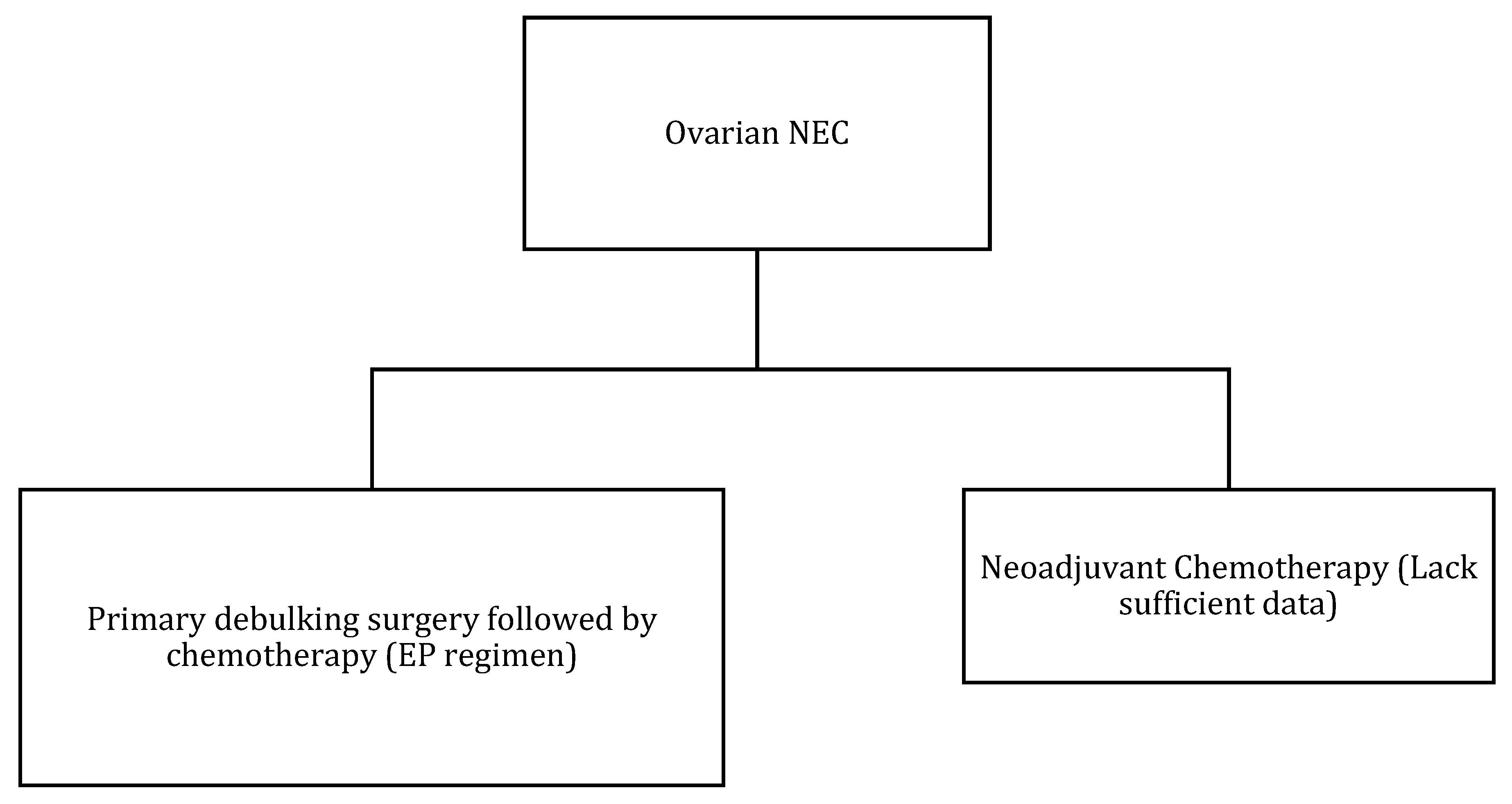
Figure 10.
Treatment algorithm of ovarian NEC. If non-surgical or metastatic disease: palliative chemotherapy (EP regimen) or enrollment into clinical trials.
Figure 10.
Treatment algorithm of ovarian NEC. If non-surgical or metastatic disease: palliative chemotherapy (EP regimen) or enrollment into clinical trials.
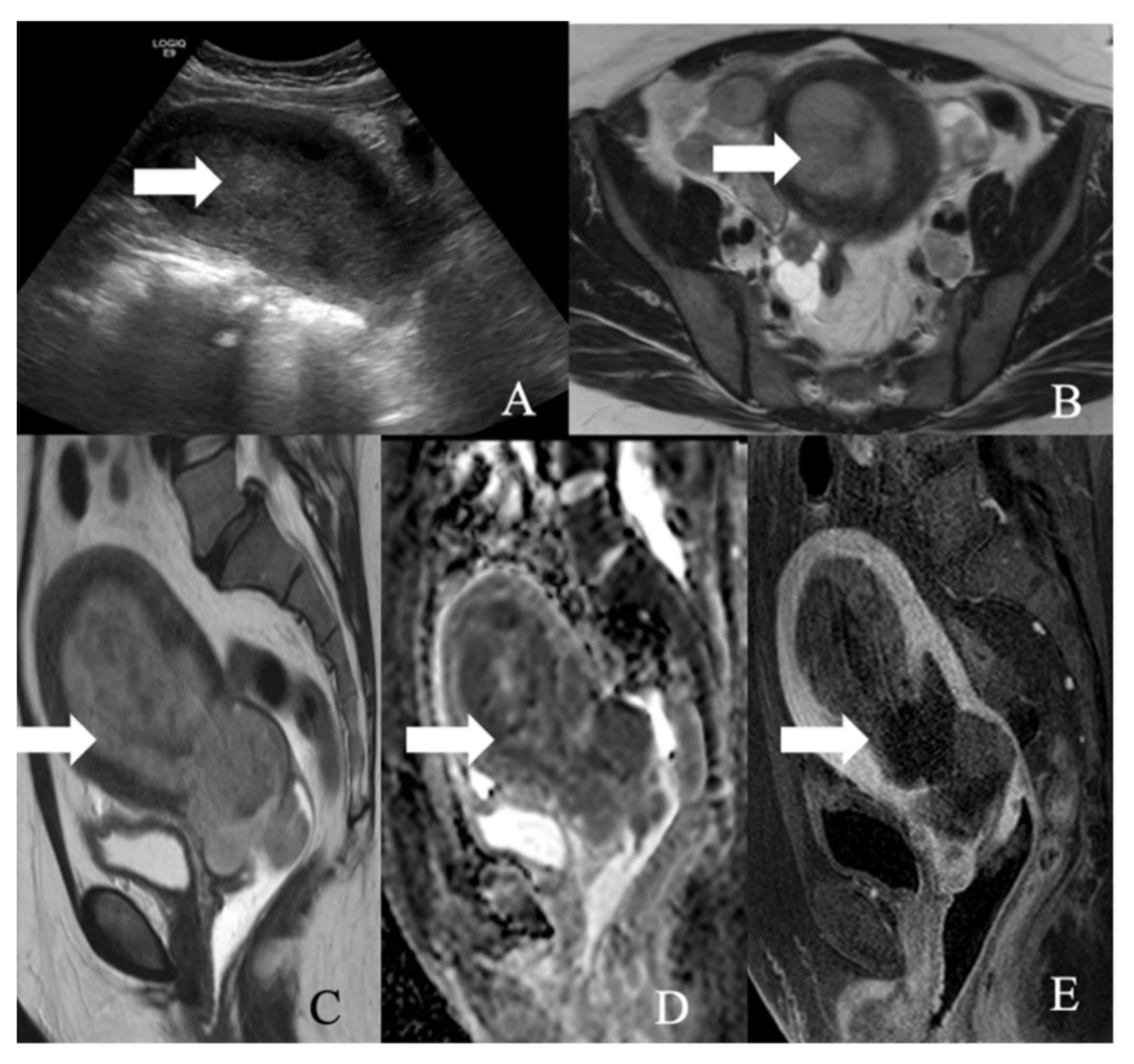
Figure 11.
A 52-year-old female with a large cell neuroendocrine tumor of the endometrium. (A) Transverse ultrasound image of the uterus demonstrates thickened endometrium (arrow), (B) axial T2 weighted image, (C) sagittal T2 weighted image, (D) sagittal apparent diffusion coefficient map, and (E) sagittal fat-saturated post-contrast T1 weighted MRI images demonstrate a hypoenhancing tumor in the endometrium (arrow) with restricted diffusion.
Figure 11.
A 52-year-old female with a large cell neuroendocrine tumor of the endometrium. (A) Transverse ultrasound image of the uterus demonstrates thickened endometrium (arrow), (B) axial T2 weighted image, (C) sagittal T2 weighted image, (D) sagittal apparent diffusion coefficient map, and (E) sagittal fat-saturated post-contrast T1 weighted MRI images demonstrate a hypoenhancing tumor in the endometrium (arrow) with restricted diffusion.
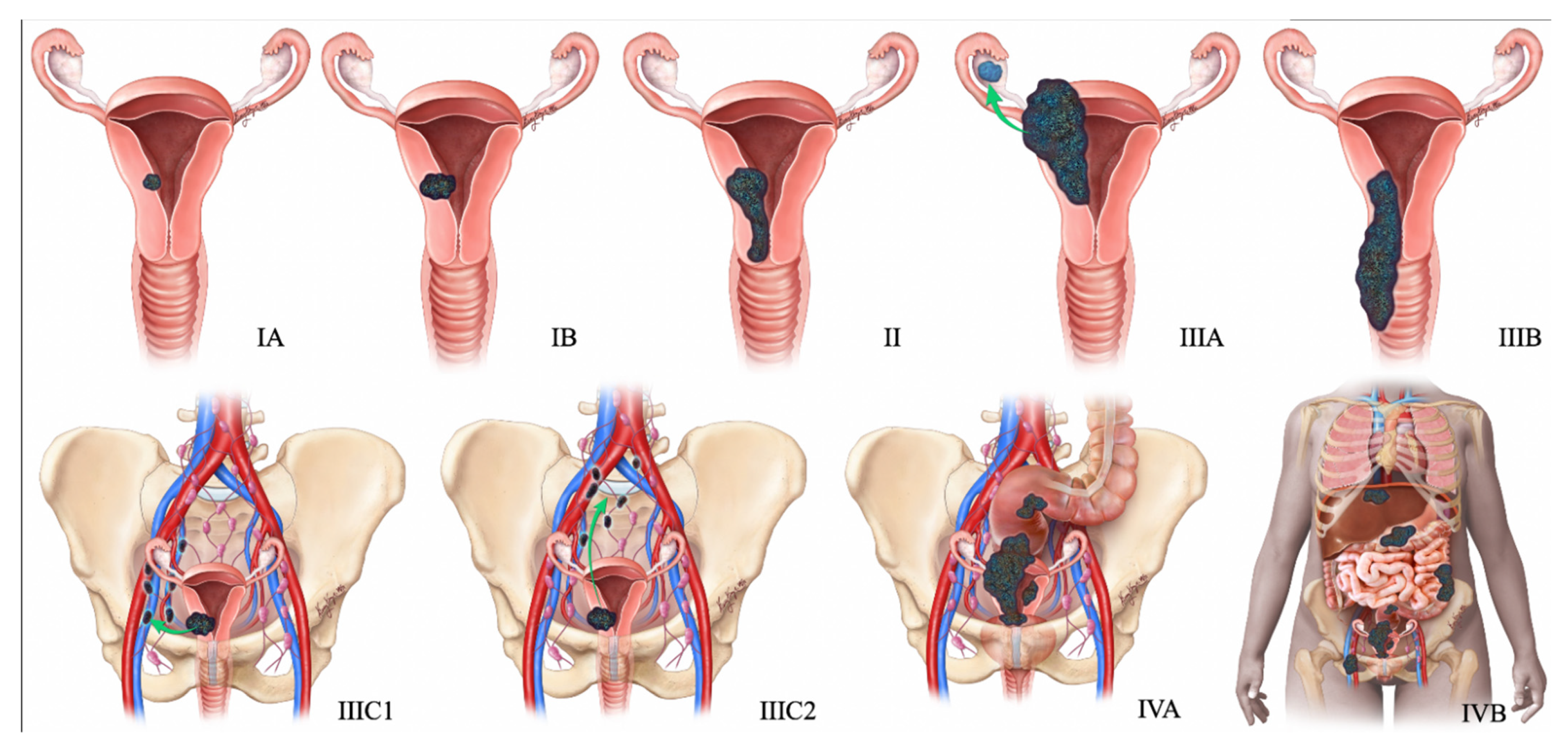
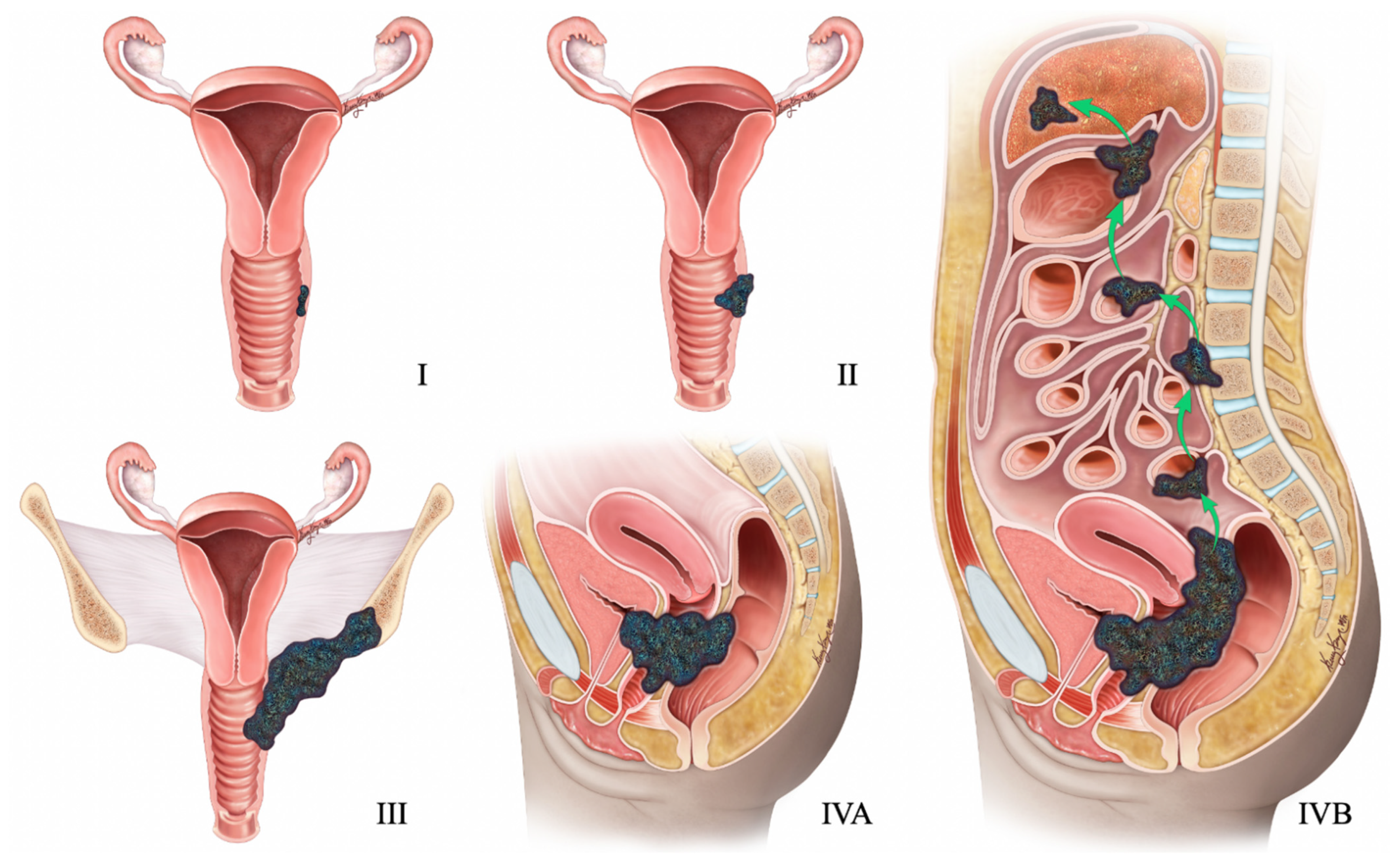
Figure 12.
2009 FIGO staging system for endometrial cancer. Stage I tumor confined to the uterus. Stage IA < 50% myometrial invasion. Stage IB ≥ 50% myometrial invasion. Stage II Cervical stromal invasion. Stage IIIA tumor invasion into serosa or adnexa. Stage IIIB vaginal or parametrial involvement. Stage IIIC1 pelvic node involvement. Stage IIIC2 paraaortic node involvement. Stage IVA tumor invasion into bladder or bowel mucosa. Stage IVB distant metastases (including abdominal metastases) or inguinal lymph node involvement.
Figure 12.
2009 FIGO staging system for endometrial cancer. Stage I tumor confined to the uterus. Stage IA < 50% myometrial invasion. Stage IB ≥ 50% myometrial invasion. Stage II Cervical stromal invasion. Stage IIIA tumor invasion into serosa or adnexa. Stage IIIB vaginal or parametrial involvement. Stage IIIC1 pelvic node involvement. Stage IIIC2 paraaortic node involvement. Stage IVA tumor invasion into bladder or bowel mucosa. Stage IVB distant metastases (including abdominal metastases) or inguinal lymph node involvement.
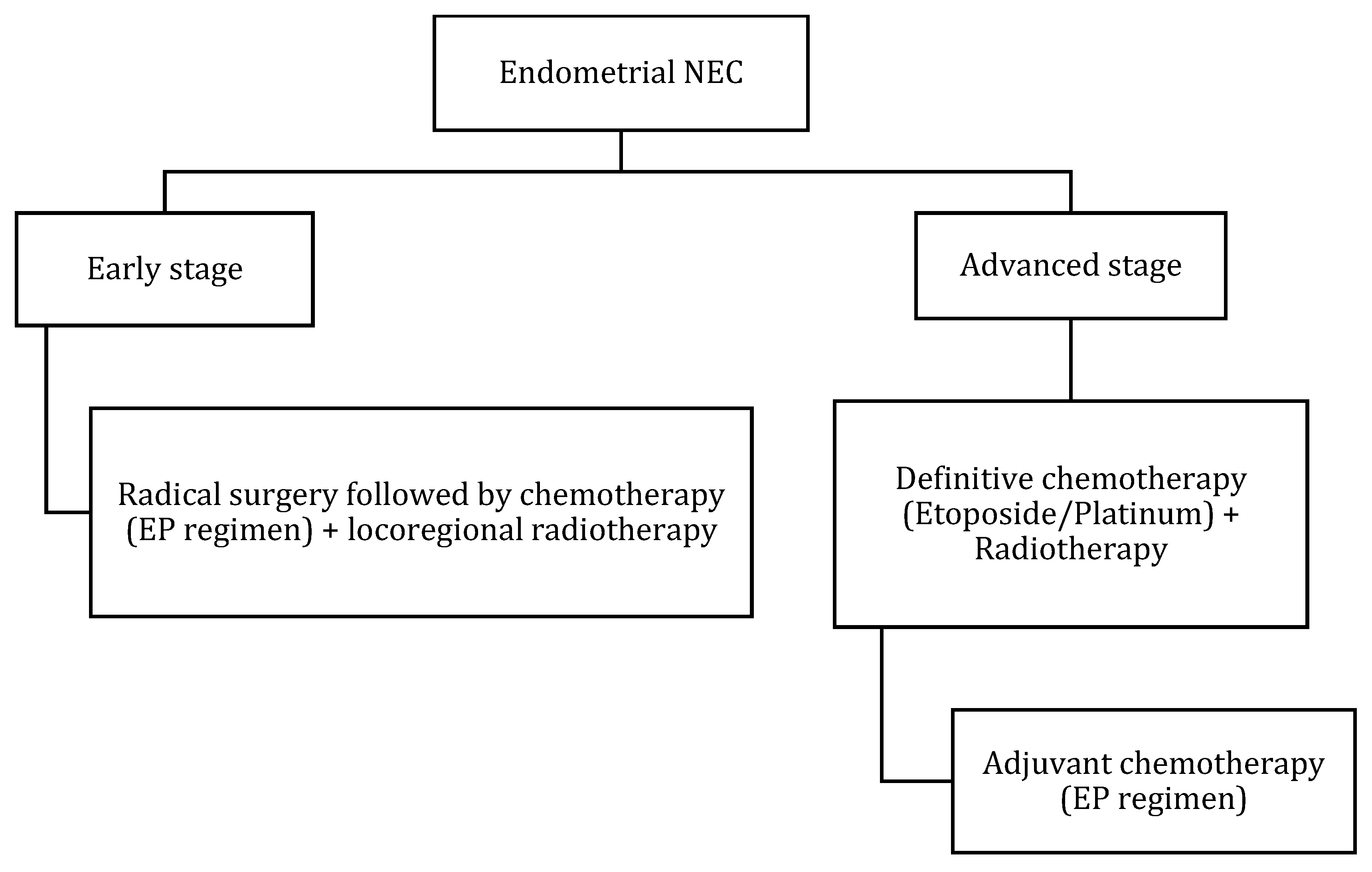
Figure 13.
Treatment algorithm of endometrial NEC. If non-surgical or metastatic disease: palliative chemotherapy with EP regimen or enrollment into clinical trials.
Figure 13.
Treatment algorithm of endometrial NEC. If non-surgical or metastatic disease: palliative chemotherapy with EP regimen or enrollment into clinical trials.
Figure 14.
FIGO Staging of vaginal tumors. Stage I is limited to the vaginal wall. Stage II is beyond the vaginal wall without pelvic sidewall involvement. Stage III extends to the pelvic sidewall. Stage IVA infiltrates bladder or rectum or the tumor extending beyond the pelvis, with any nodal metastasis. Stage IVB has distant metastasis.
Figure 14.
FIGO Staging of vaginal tumors. Stage I is limited to the vaginal wall. Stage II is beyond the vaginal wall without pelvic sidewall involvement. Stage III extends to the pelvic sidewall. Stage IVA infiltrates bladder or rectum or the tumor extending beyond the pelvis, with any nodal metastasis. Stage IVB has distant metastasis.
Figure 15.
Treatment algorithm of vaginal/vulvar NEC. If non-surgical or metastatic disease: palliative chemotherapy with EP regimen or enrollment in clinical trials.
Figure 15.
Treatment algorithm of vaginal/vulvar NEC. If non-surgical or metastatic disease: palliative chemotherapy with EP regimen or enrollment in clinical trials.
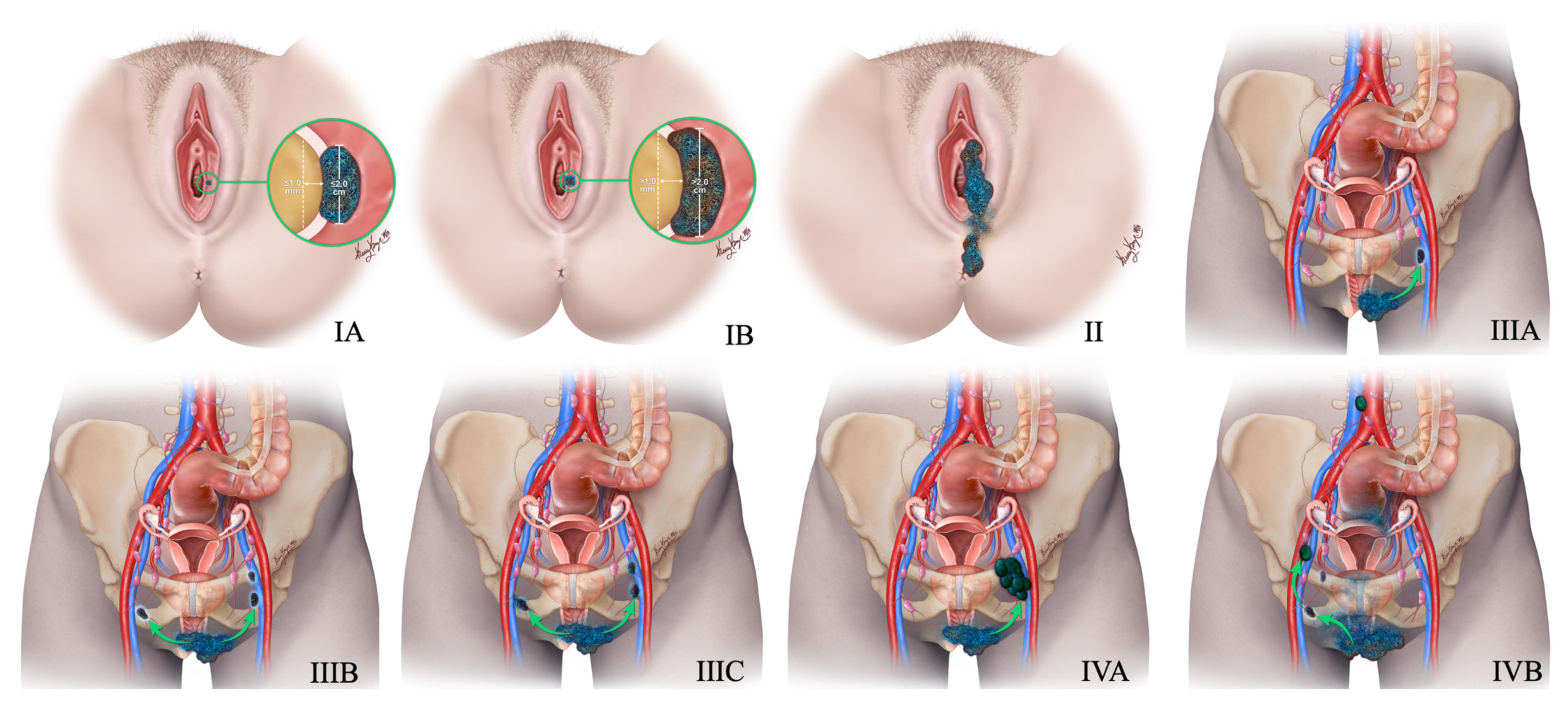
Figure 16.
New 2021 FIGO Staging of vulvar tumors. Stage-I tumor confined to the vulva. Stage IA tumor size less than equal to 2 cm and stromal invasion less than equal to 1 mm. Stage IB tumor size more than 2 cm and stromal invasion more than 1 mm. Stage II tumor of any size with extension to lower one-third of the urethra, lower one-third of the vagina, lower one-third of the anus with negative nodes. Stage III tumor of any size with extension to the upper part of adjacent perineal structures or with any number of nonfixed, nonulcerated lymph nodes. Stage IIIA tumor of any size with disease extension to the upper two-thirds of the urethra, upper two-thirds of the vagina, bladder mucosa, rectal mucosa, or regional lymph node metastases less than equal to 5 mm. Stage IIIB regional lymph node metastases more than 5 mm. Stage IIIC regional lymph node metastases with extracapsular spread. Stage IV tumor of any size fixed to bone or fixed, ulcerated lymph node metastases, or distant metastases. Stage IVA disease fixed to the pelvic bone or fixed or ulcerated regional lymph node metastases. Stage IVB distant metastases.
Figure 16.
New 2021 FIGO Staging of vulvar tumors. Stage-I tumor confined to the vulva. Stage IA tumor size less than equal to 2 cm and stromal invasion less than equal to 1 mm. Stage IB tumor size more than 2 cm and stromal invasion more than 1 mm. Stage II tumor of any size with extension to lower one-third of the urethra, lower one-third of the vagina, lower one-third of the anus with negative nodes. Stage III tumor of any size with extension to the upper part of adjacent perineal structures or with any number of nonfixed, nonulcerated lymph nodes. Stage IIIA tumor of any size with disease extension to the upper two-thirds of the urethra, upper two-thirds of the vagina, bladder mucosa, rectal mucosa, or regional lymph node metastases less than equal to 5 mm. Stage IIIB regional lymph node metastases more than 5 mm. Stage IIIC regional lymph node metastases with extracapsular spread. Stage IV tumor of any size fixed to bone or fixed, ulcerated lymph node metastases, or distant metastases. Stage IVA disease fixed to the pelvic bone or fixed or ulcerated regional lymph node metastases. Stage IVB distant metastases.
![Cancers 14 01835 g016]()
Table 1.
WHO terminology for NEN of gynecologic tract, fifth edition.
Table 1.
WHO terminology for NEN of gynecologic tract, fifth edition.
| Category | Grade | Site |
|---|
| NET | 1,2 | Uterus, cervix, vulva, vagina |
| NEC: | 3 | Ovary, uterus, cervix, vulva, vagina |
| Small cell | | |
| Large cell | | |
| combined small cell NEC | | |
| combined large cell NEC | | |
| Carcinoid | 1 | Ovary only |
Table 2.
In general, Grading criteria for neuroendocrine neoplasms.
Table 2.
In general, Grading criteria for neuroendocrine neoplasms.
| Terminology | Differentiation | Grade | Mitotic Rate | Ki-67 Index |
|---|
| NET G1 | Well-differentiated | Low | <2 | <3% |
| NET G2 | Well-differentiated | Intermediate | 2–20 | 3–20% |
| NET G3 | Well-differentiated | High | >20 | >20% |
| SCNEC | Poorly differentiated | High | >20 | >20% |
| LCNEC | Poorly differentiated | High | >20 | >20% |
| MiNEN | Well or poorly differentiated | Variable | Variable | Variable |
Table 3.
Overview of biomarkers in NEN.
Table 3.
Overview of biomarkers in NEN.
| Circulating and Imaging Biomarkers | Considerations | Level of Evidence |
|---|
| 68Ga-SRS | It is a PET imaging with a positron-emitting radionuclide. It has been extensively studied with excellent metrics. It is considered a gold standard imaging modality in NEN. False positive rates may be observed in inflammation, renal cancer, lymphoma, and meningioma. | High |
| Chromogranin A | It is a component of dense core granules in neuroendocrine cells. Extensive studies are performed with varied testing subjects and results. Moderate metrics with high false-positive rates due to interaction with proton-pump inhibitors, and renal and liver failure. | Moderate |
| NETest | It is an multianalyte with mRNA transcripts. Prospective studies were conducted with excellent statistics. It is limited by its lower availability and higher costs. | Moderate |
| CT | It is an imaging modality. It has excellent availability and is less expensive. However, limited by the radiation dose and the application of nephrotoxic contrast agents. | Moderate |
| MRI | It is an imaging modality. It is easily available and has intermediate costs. However, limited by the duration of the scan and patient contraindications, such as claustrophobia and metal implants in the body. | Moderate |
| 111In-SRS | It is a SPECT imaging with γ-emitting radionuclide. Inferior compared to excellent metric of 68Ga-SRS. | Moderate |
| 18F-FDG | It is a PET imaging with positron-emitting radionuclide. It has low sensitivity in identifying well-differentiated NEN. Limited by its high cost. | Moderate |
| Chromogranin B | It is a part of family of chromogranin A. Limited studies are available with poor metrics. May be considered sensitive to rectal and ovarian NEN. | Low |
| Neuron-specific enolase | It is a glycolytic enzyme. Limited studies are available with poor metrics in well-differentiated NEN. It is expressed in poorly differentiated tumors. | Low |
| Amine uptake | It is a SPECT or PET imaging with amine transporters. It is limited by its availability (18F-DOPA and 11C-5-HTP) and sensitivity (123I-MIBG). | Low |
Table 4.
MRI of the pelvis protocol.
Table 4.
MRI of the pelvis protocol.
| Description | Field-of-View (FOV) | Slice Thickness | Spacing | Frequency Encoding | Frequency × Phase |
|---|
| Coronal T2 (include kidneys) | 420 | 5 | 0 | S/I | 288 × 192 |
| Sagittal T2 | 240 | 5 | 0 | A/P | 320 × 224 |
| Field of View Sagittal b = 50, 600 | 240 | 5 | 0 | S/I | 96 × 80 |
| Axial T2 | 240 | 5 | 0 | L/R | 320 × 224 |
| Axial T1 | 240 | 5 | 0 | L/R | 320 × 224 |
| Axial DWI b = 50, 400, 800 | 380+ | 5 | 0 | L/R | 96 × 160 |
| Axial 3D Precontrast contrast | 240 | 5 | −2.5 | L/R | 320 × 224 |
| Dynamic | 240 | 5 | −2.5 | S/I | 256 × 224 |
| Post contrast Axial 3D immediate delay | 240 | 5 | −2.5 | L/R | 320 × 224 |
Table 5.
FIGO 2018 staging of cervical cancer.
Table 5.
FIGO 2018 staging of cervical cancer.
| Stage | Extent of Disease |
|---|
| I | Tumor confined to cervix |
| IA | ≤5 mm depth |
| IA1 | ≤3 mm depth |
| IA2 | 3 mm and ≤5 mm depth |
| IB | >5 mm depth |
| IB1 | ≤2 cm maximum diameter |
| IB2 | >2 cm and ≤4 cm maximum diameter |
| IB3 | >4 cm maximum diameter |
| Stage II | Beyond the uterus but not involving the lower one-third of the vagina or pelvic sidewall |
| IIA | Upper two-thirds of the vagina |
| IIA1 | Upper two-thirds of the vagina and ≤4 cm |
| IIA2 | Upper two-thirds of the vagina and >4 cm |
| IIB | Parametrial invasion |
| Stage III | Lower vagina, pelvic sidewall, ureters, and lymph nodes |
| IIIA | Lower one-third of the vagina |
| IIIB | Pelvic sidewall |
| IIIC | Pelvic and para-aortic lymph node involvement |
| IIIC1 | Pelvic lymph node involvement |
| IIIC2 | Para-aortic lymph node involvement |
| Stage IV | Adjacent and distant organs |
| IVA | Rectal or bladder involvement |
| IVB | Distant organs outside the pelvis |
Table 6.
Differences between WHO’s 2014 and 2020 classification of ovarian neuroendocrine tumors.
Table 6.
Differences between WHO’s 2014 and 2020 classification of ovarian neuroendocrine tumors.
| WHO Classification | Category | Tumor |
|---|
| WHO 2014 | Monodermal teratoma and somatic-type tumors from a dermoid cyst | Carcinoid |
| | Miscellaneous tumors | Small-cell ovarian NEC pulmonary type |
| | Miscellaneous tumors | paraganglioma |
| | No category | Small-cell ovarian NEC hypercalcemia type |
| WHO 2020 | Neuroendocrine neoplasms | Grade-1: Carcinoid; Grade-3: ovarian NEC |
Table 7.
Variants of ovarian carcinoid tumors and their pathological and immunohistochemical features.
Table 7.
Variants of ovarian carcinoid tumors and their pathological and immunohistochemical features.
| Variant | Pathological Feature | Immunohistochemistry |
|---|
| Insular (most common: around 50%) | Polygonal tumor cells arranged in nests with an abundant cytoplasm accommodating eosinophilic granules, a round/oval nuclei containing salt and pepper chromatin; Hyaline appearing conspicuous stroma with sporadical psammomatous calcification. | Positive for chromogranin, synaptophysin, CD56, and CK7. Negative for CK20. |
| Trabecular | Parallel trabecular/wavy ribboned arrangements of regular cells with similar nuclear features to insular variant. | Positive for synaptophysin, CD56, and CK7. Negative for CK20. Negative for chromogranin similar to Sertoli cell tumor (SCT) with trabecular architecture. SCT is usually positive for inhibin and calretinin and negative for synaptophysin compared to trabecular carcinoid, which exhibits a converse immune profile. |
| Strumal (40% of ovarian carcinoids) | Admixture of insular/trabecular carcinoid elements and thyroid tissue; Intestinal type mucinous glands can be seen in 40% of cases. | Positive staining for carcinoid component (neuroendocrine markers) and thyroid component (thyroid transcription factor-1). |
| Mucinous, also known as goblet cell carcinoids (rarest) | Glands or acini lined by cuboidal/columnar epithelium with mucin-filled-cytoplasm. | CDX2 and CK20 positive; CK7 negative. |
Table 8.
Differentiating features between ovarian small cell carcinoma of pulmonary and hypercalcemic type.
Table 8.
Differentiating features between ovarian small cell carcinoma of pulmonary and hypercalcemic type.
| Features | SCCOPT | SCCOHT |
|---|
| Mean age at diagnosis | 51 years | 24 years |
| Histopathological features | Spindle-shaped cells; scanty cytoplasm; inconspicuous nucleoli in sheets, dispersed chromatin, and nuclear molding | Prominent nucleoli, clumped chromatin; larger cells in 50% of cases |
| Laterality | Bilateral in 50% of cases | Almost always unilateral |
| Hypercalcemia | None | >65% of cases |
| Immunohistochemistry | Positive for chromogranin A in 53% of cases | Positive for chromogranin A in 9.5% of cases and vimentin in 94% of cases |
| Molecular features | Retained expression of SMARCA4 | Loss of expression of SMARCA4 |
Table 9.
The International Federation of Gynecology and Obstetrics (FIGO) staging of ovarian cancer (2014).
Table 9.
The International Federation of Gynecology and Obstetrics (FIGO) staging of ovarian cancer (2014).
| Stage | Extent of Disease |
|---|
| I | Tumor confined to ovaries |
| IA | Tumor limited to 1 ovary, capsule intact, no tumor on surface, negative washing |
| IB | Tumor involves both ovaries otherwise like IA |
| IC | Tumor limited to 1 or both ovaries |
| IC1 | Surgical spill |
| IC2 | Capsule rupture before surgery or tumor on ovarian surface |
| IC3 | Malignant cells in the ascites or peritoneal washings |
| II | Tumor involves 1 or both ovaries with pelvic extension (below the pelvic brim or primary peritoneal cancer |
| IIA | Extension and/or implant on uterus and/or fallopian tubes |
| IIB | Extension to other pelvic intraperitoneal tissues |
| III | Tumor involves 1 or both ovaries with cytologically or histologically confirmed spread to the peritoneum outside the pelvis and / or metastatic to the retroperitoneal lymph nodes |
| IIIA1 | Positive retroperitoneal lymph nodes only |
| IIIA1(i) | Metastasis ≤ 10 mm |
| IIIA1(ii) | Metastasis > 10 mm |
| IIIA2 | Microscopic, extrapelvic (above the brim) peritoneal involvement ± positive retroperitoneal lymph nodes |
| IIIB | Macroscopic, extrapelvic, peritoneal metastasis ≤ 2 cm ± positive retroperitoneal lymph nodes. Includes extension to the capsule of liver/spleen |
| IIIC | Macroscopic, extrapelvic, peritoneal metastasis > 2 cm ± positive retroperitoneal lymph nodes. Includes extension to the capsule of liver/spleen |
| IV | Distant metastasis excluding peritoneal metastasis |
| IVA | Pleural effusion with positive cytology |
| IVB | Hepatic and/or splenic parenchymal metastasis, metastasis to extra-abdominal organs (including inguinal lymph nodes and lymph nodes outside the abdominal cavity) |
Table 10.
2009 FIGO staging for endometrial cancer.
Table 10.
2009 FIGO staging for endometrial cancer.
| Stage | Extent of Disease |
|---|
| I | Tumor confined to uterus |
| IA | <50% myometrial invasion |
| IB | ≥50% myometrial invasion |
| II | Cervical stromal invasion |
| IIIA | Tumor invasion into serosa or adnexa |
| IIIB | Vaginal or parametrial involvement |
| IIIC1 | Pelvic node involvement |
| IIIC2 | Paraaortic node involvement |
| IVA | Tumor invasion into bladder or bowel mucosa |
| IVB | Distant metastases (including abdominal metastases) or inguinal lymph node involvement |
Table 11.
2009 FIGO staging of vaginal cancer.
Table 11.
2009 FIGO staging of vaginal cancer.
| Stage | Extent of Disease |
|---|
| I | Tumor confined to vaginal wall |
| II | Involvement of paravaginal tissue but not the pelvic wall |
| III | Either spread to pelvic lymph nodes and/or pelvic wall and/or lower vagina and/or causing hydronephrosis |
| IVA | Involvement of bladder, rectum or beyond pelvis with/without positive lymph node |
| IVB | Spread to distant organs |
Table 12.
American Joint Committee on Cancer (AJCC) staging of vaginal cancer.
Table 12.
American Joint Committee on Cancer (AJCC) staging of vaginal cancer.
| AJCC Stage | Corresponding FIGO Stage | Description |
|---|
| IA | I | Tumor size < 2 cm and confined to the vagina |
| IB | I | Tumor > 2 cm and confined to the vagina |
| IIA | II | Tumor < 2 cm and is beyond the vaginal wall without the involvement of pelvic side wall |
| IIB | II | Tumor > 2 cm and is beyond the vaginal wall without pelvic sidewall involvement |
| III | III | Tumor extends to the pelvic side wall, lower third of the vagina, and/or causes hydronephrosis; Pelvic/inguinal lymph node metastasis |
| IVA | IVA | Infiltration of bladder or rectum or the tumor extending beyond the pelvis; any nodal metastasis |
| IVB | IVB | Distant metastasis |
Table 13.
New (2021) FIGO staging for carcinoma of the vulva.
Table 13.
New (2021) FIGO staging for carcinoma of the vulva.
| Stage | Extent of Disease |
|---|
| I | Tumor confined to vulva |
| IA | Tumor size less than equal to 2 cm and stromal invasion less than equal to 1 mm |
| IB | Tumor size more than 2 cm and stromal invasion more than 1 mm |
| II | Tumor of any size with extension to lower one-third of the urethra, lower one-third of the vagina, lower one third of the anus with negative nodes |
| III | Tumor of any size with extension to upper part of adjacent perineal structures, or with any number of nonfixed, nonulcerated lymph node |
| IIIA | Tumor of any size with disease extension to upper two-thirds of the urethra, upper two-thirds of the vagina, bladder mucosa, rectal mucosa, or regional lymph node metastases less than equal to 5 mm3 |
| IIIB | Regional lymph node metastases more than 5 mm |
| IIIC | Regional lymph node metastases with extracapsular spread |
| IV | Tumor of any size fixed to bone, or fixed, ulcerated lymph node metastases, or distant metastases |
| IVA | Disease fixed to pelvic bone, or fixed or ulcerated regional lymph node metastases |
| IVB | Distant metastases |


 ,
, 





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}