
Divergent Patterns in Care Utilization and Financial Distress between Patients with Blood Cancers and Solid Tumors: A National Health Interview Survey Study, 2014–2020


Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
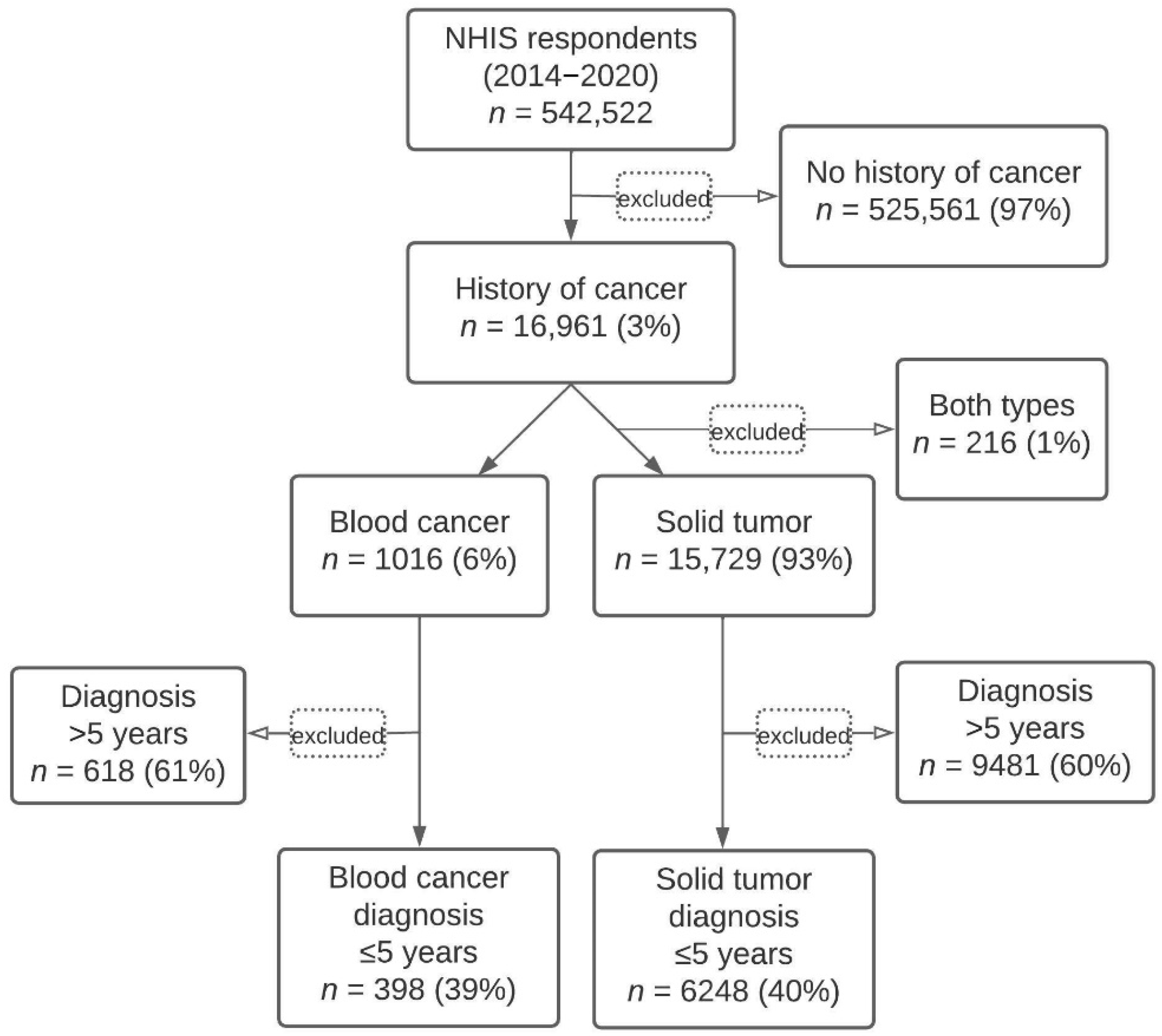
2.1. Cohort Identification
2.2. Study Measures
2.2.1. Medical Care Utilization in the Last 12 Months
2.2.2. Financial Barriers to Care in the Last 12 Months
2.2.3. Financial Distress of Affording Care
2.3. Statistical Analysis
3. Results
3.1. Cohort Identification
3.2. Respondent Characteristics
3.3. Factor Analysis
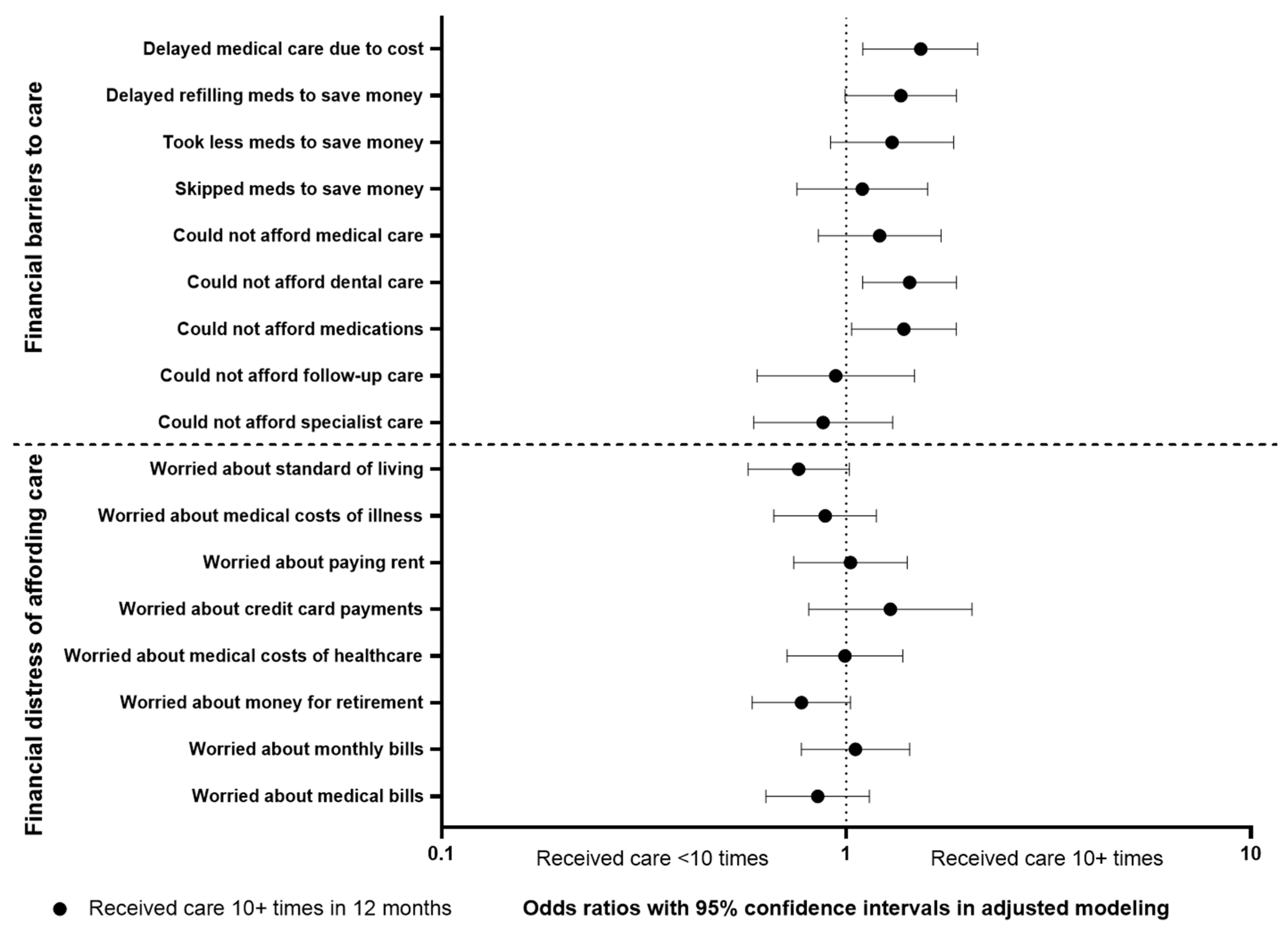
3.4. Association of Medical Care Utilization with Financial Barriers and Financial Distress
3.5. Associations of Cancer Type with Study Outcomes
3.5.1. Extracted Domain Factors
3.5.2. Multivariable Analyses of Study Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Carrera, P.M.; Kantarjian, H.M.; Blinder, V.S. The financial burden and distress of patients with cancer: Understanding and stepping-up action on the financial toxicity of cancer treatment. CA Cancer J. Clin. 2018, 68, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Narang, A.K.; Nicholas, L.H. Out-of-Pocket Spending and Financial Burden Among Medicare Beneficiaries With Cancer. JAMA Oncol. 2017, 3, 757–765. [Google Scholar] [CrossRef]
- Smith, G.L.; Lopez-Olivo, M.A.; Advani, P.G.; Ning, M.S.; Geng, Y.; Giordano, S.H.; Volk, R.J. Financial Burdens of Cancer Treatment: A Systematic Review of Risk Factors and Outcomes. J. Natl. Compr. Cancer Netw. 2019, 17, 1184–1192. [Google Scholar] [CrossRef] [PubMed]
- De Souza, J.A.; Yap, B.J.; Wroblewski, K.; Blinder, V.; Araújo, F.S.; Hlubocky, F.J.; Nicholas, L.H.; O’Connor, J.M.; Brockstein, B.; Ratain, M.J.; et al. Measuring financial toxicity as a clinically relevant patient-reported outcome: The validation of the COmprehensive Score for financial Toxicity (COST). Cancer 2017, 123, 476–484. [Google Scholar] [CrossRef]
- Zafar, S.Y.; Peppercorn, J.M.; Schrag, D.; Taylor, D.H.; Goetzinger, A.M.; Zhong, X.; Abernethy, A.P. The financial toxicity of cancer treatment: A pilot study assessing out-of-pocket expenses and the insured cancer patient’s experience. Oncologist 2013, 18, 381–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shankaran, V.; Leahy, T.; Steelquist, J.; Watabayashi, K.; Linden, H.; Ramsey, S.; Schwartz, N.; Kreizenbeck, K.; Nelson, J.; Balch, A.; et al. Pilot Feasibility Study of an Oncology Financial Navigation Program. J. Oncol. Pract. 2018, 14, e122–e129. [Google Scholar] [CrossRef] [PubMed]
- Lathan, C.S.; Cronin, A.; Tucker-Seeley, R.; Zafar, S.Y.; Ayanian, J.Z.; Schrag, D. Association of Financial Strain With Symptom Burden and Quality of Life for Patients With Lung or Colorectal Cancer. J. Clin. Oncol. 2016, 34, 1732–1740. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mols, F.; Tomalin, B.; Pearce, A.; Kaambwa, B.; Koczwara, B. Financial toxicity and employment status in cancer survivors. A systematic literature review. Support. Care Cancer 2020, 28, 5693–5708. [Google Scholar] [CrossRef] [PubMed]
- Pearce, A.; Tomalin, B.; Kaambwa, B.; Horevoorts, N.; Duijts, S.; Mols, F.; van de Poll-Franse, L.; Koczwara, B. Financial toxicity is more than costs of care: The relationship between employment and financial toxicity in long-term cancer survivors. J. Cancer Surviv. 2019, 13, 10–20. [Google Scholar] [CrossRef] [PubMed]
- Zafar, S.Y.; Newcomer, L.N.; McCarthy, J.; Fuld Nasso, S.; Saltz, L.B. How Should We Intervene on the Financial Toxicity of Cancer Care? One Shot, Four Perspectives. Am. Soc. Clin. Oncol. Educ. Book 2017, 37, 35–39. [Google Scholar] [CrossRef]
- Witte, J.; Mehlis, K.; Surmann, B.; Lingnau, R.; Damm, O.; Greiner, W.; Winkler, E.C. Methods for measuring financial toxicity after cancer diagnosis and treatment: A systematic review and its implications. Ann. Oncol. 2019, 30, 1061–1070. [Google Scholar] [CrossRef] [Green Version]
- Arastu, A.; Patel, A.; Mohile, S.G.; Ciminelli, J.; Kaushik, R.; Wells, M.; Culakova, E.; Lei, L.; Xu, H.; Dougherty, D.W.; et al. Assessment of Financial Toxicity Among Older Adults With Advanced Cancer. JAMA Netw. Open 2020, 3, e2025810. [Google Scholar] [CrossRef] [PubMed]
- Rotenstein, L.S.; Dusetzina, S.B.; Keating, N.L. Out-of-Pocket Spending Not Associated with Oral Oncolytic Survival Benefit. J. Manag. Care Spec. Pharm. 2018, 24, 494–502. [Google Scholar] [CrossRef]
- Phuar, H.L.; Begley, C.E.; Chan, W.; Krause, T.M. Tyrosine Kinase Inhibitors Initiation, Cost Sharing, and Health Care Utilization in Patients with Newly Diagnosed Chronic Myeloid Leukemia: A Retrospective Claims-Based Study. J. Manag. Care Spec. Pharm. 2019, 25, 1140–1150. [Google Scholar] [CrossRef] [PubMed]
- Dusetzina, S.B.; Winn, A.N.; Abel, G.A.; Huskamp, H.A.; Keating, N.L. Cost sharing and adherence to tyrosine kinase inhibitors for patients with chronic myeloid leukemia. J. Clin. Oncol. 2014, 32, 306–311. [Google Scholar] [CrossRef] [Green Version]
- Huntington, S.F.; Weiss, B.M.; Vogl, D.T.; Cohen, A.D.; Garfall, A.L.; Mangan, P.A.; Doshi, J.A.; Stadtmauer, E.A. Financial toxicity in insured patients with multiple myeloma: A cross-sectional pilot study. Lancet Haematol. 2015, 2, e408–e416. [Google Scholar] [CrossRef]
- Goodwin, J.A.; Coleman, E.A.; Sullivan, E.; Easley, R.; McNatt, P.K.; Chowdhury, N.; Stewart, C.B. Personal financial effects of multiple myeloma and its treatment. Cancer Nurs. 2013, 36, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Jones, W.C.; Parry, C.; Devine, S.; Main, D.S.; Okuyama, S.; Tran, Z.V. Prevalence and predictors of distress in posttreatment adult leukemia and lymphoma survivors. J. Psychosoc. Oncol. 2015, 33, 124–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nipp, R.D.; Shui, A.M.; Perez, G.K.; Kirchhoff, A.C.; Peppercorn, J.M.; Moy, B.; Kuhlthau, K.; Park, E.R. Patterns in Health Care Access and Affordability Among Cancer Survivors During Implementation of the Affordable Care Act. JAMA Oncol. 2018, 4, 791–797. [Google Scholar] [CrossRef]
- Zheng, Z.; Jemal, A.; Han, X.; Guy, G.P.; Li, C.; Davidoff, A.J.; Banegas, M.P.; Ekwueme, D.U.; Yabroff, K.R. Medical financial hardship among cancer survivors in the United States. Cancer 2019, 125, 1737–1747. [Google Scholar] [CrossRef]
- Fenn, K.M.; Evans, S.B.; McCorkle, R.; DiGiovanna, M.P.; Pusztai, L.; Sanft, T.; Hofstatter, E.W.; Killelea, B.K.; Knobf, M.T.; Lannin, D.R.; et al. Impact of financial burden of cancer on survivors’ quality of life. J. Oncol. Pract. 2014, 10, 332–338. [Google Scholar] [CrossRef] [PubMed]
- Su, C.T.; Okullo, D.; Hingtgen, S.; Levine, D.A.; Goold, S.D. Affordable Care Act and Cancer Survivors’ Financial Barriers to Care: Analysis of the National Health Interview Survey, 2009–2018. JCO Oncol. Pract. 2021, 17, e1603–e1613. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, R.; Abouzaid, S.; Bonafede, M.; Cai, Q.; Parikh, K.; Cosler, L.; Richardson, P. Trends in overall survival and costs of multiple myeloma, 2000–2014. Leukemia 2017, 31, 1915–1921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, Z.; Jemal, A.; Banegas, M.P.; Han, X.; Yabroff, K.R. High-Deductible Health Plans and Cancer Survivorship: What Is the Association With Access to Care and Hospital Emergency Department Use? J. Oncol. Pract. 2019, 15, e957–e968. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- De Oliveira, C.; Cheng, J.; Chan, K.; Earle, C.C.; Krahn, M.; Mittmann, N. High-Cost Patients and Preventable Spending: A Population-Based Study. J. Natl. Compr. Cancer Netw. 2020, 18, 23–31. [Google Scholar] [CrossRef]
- Öhlén, J.; Cohen, J.; Håkanson, C. Determinants in the place of death for people with different cancer types: A national population-based study. Acta Oncol. 2017, 56, 455–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joynt, K.E.; Gawande, A.A.; Orav, E.J.; Jha, A.K. Contribution of preventable acute care spending to total spending for high-cost Medicare patients. JAMA 2013, 309, 2572–2578. [Google Scholar] [CrossRef] [Green Version]
- Bruera, E.; Sweeney, C.; Russell, N.; Willey, J.S.; Palmer, J.L. Place of death of Houston area residents with cancer over a two-year period. J. Pain Symptom Manag. 2003, 26, 637–643. [Google Scholar] [CrossRef]
- LeBlanc, T.W.; Abernethy, A.P.; Casarett, D.J. What is different about patients with hematologic malignancies? A retrospective cohort study of cancer patients referred to a hospice research network. J. Pain Symptom Manag. 2015, 49, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; Didwaniya, N.; Vidal, M.; Shin, S.H.; Chisholm, G.; Roquemore, J.; Bruera, E. Quality of end-of-life care in patients with hematologic malignancies: A retrospective cohort study. Cancer 2014, 120, 1572–1578. [Google Scholar] [CrossRef]
- Damlaj, M.; El Fakih, R.; Hashmi, S.K. Evolution of survivorship in lymphoma, myeloma and leukemia: Metamorphosis of the field into long term follow-up care. Blood Rev. 2019, 33, 63–73. [Google Scholar] [CrossRef]
- Joseph, N.S.; Kaufman, J.L.; Dhodapkar, M.V.; Hofmeister, C.C.; Almaula, D.K.; Heffner, L.T.; Gupta, V.A.; Boise, L.H.; Lonial, S.; Nooka, A.K. Long-Term Follow-Up Results of Lenalidomide, Bortezomib, and Dexamethasone Induction Therapy and Risk-Adapted Maintenance Approach in Newly Diagnosed Multiple Myeloma. J. Clin. Oncol. 2020, 38, 1928–1937. [Google Scholar] [CrossRef]
- National Center for Health Statistics. What to Expect If You Have Been Selected to Participate in NHIS. Available online: https://www.cdc.gov/nchs/nhis/participants/whattoexpect.htm (accessed on 11 March 2022).
- Blewett, L.; Rivera Drew, J.A.; King, M.L.; Williams, K.C. IPUMS Health Surveys: National Health Interview Survey, 6.4th ed.; IPUMS: Minneapolis, MN, USA, 2019. [Google Scholar] [CrossRef]
- Zhao, J.; Mao, Z.; Fedewa, S.A.; Nogueira, L.; Yabroff, K.R.; Jemal, A.; Han, X. The Affordable Care Act and access to care across the cancer control continuum: A review at 10 years. CA Cancer J. Clin. 2020, 70, 165–181. [Google Scholar] [CrossRef]
- Minnesota Population Center, University of Manchester User Note—Sampling Weights. Available online: https://nhis.ipums.org/nhis/userNotes_weights.shtml (accessed on 13 September 2021).
- Dashputre, A.A.; Gatwood, K.S.; Gatwood, J. Medication Adherence, Health Care Utilization, and Costs Among Patients Initiating Oral Oncolytics for Multiple Myeloma or Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma. J. Manag. Care Spec. Pharm. 2020, 26, 186–196. [Google Scholar] [CrossRef]
- Kenzik, K.M.; Bhatia, R.; Bhatia, S. Expenditures for First- and Second-Generation Tyrosine Kinase Inhibitors Before and After Transition of Imatinib to Generic Status. JAMA Oncol. 2020, 6, 542–546. [Google Scholar] [CrossRef]
- Klein, I.A.; Rosenberg, S.M.; Reynolds, K.L.; Zubiri, L.; Rosovsky, R.; Piper-Vallillo, A.J.; Gao, X.; Boland, G.; Bardia, A.; Gaither, R.; et al. Impact of Cancer History on Outcomes Among Hospitalized Patients with COVID-19. Oncologist 2021. [Google Scholar] [CrossRef] [PubMed]
- Fillmore, N.R.; La, J.; Szalat, R.E.; Tuck, D.P.; Nguyen, V.; Yildirim, C.; Do, N.V.; Brophy, M.T.; Munshi, N.C. Prevalence and Outcome of COVID-19 Infection in Cancer Patients: A National Veterans Affairs Study. J. Natl. Cancer Inst. 2021, 113, 691–698. [Google Scholar] [CrossRef]
- Howell, D.A.; Roman, E.; Cox, H.; Smith, A.G.; Patmore, R.; Garry, A.C.; Howard, M.R. Destined to die in hospital? Systematic review and meta-analysis of place of death in haematological malignancy. BMC Palliat. Care 2010, 9, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pisu, M.; Henrikson, N.B.; Banegas, M.P.; Yabroff, K.R. Costs of cancer along the care continuum: What we can expect based on recent literature. Cancer 2018, 124, 4181–4191. [Google Scholar] [CrossRef] [Green Version]
- Watabayashi, K.; Steelquist, J.; Overstreet, K.A.; Leahy, A.; Bradshaw, E.; Gallagher, K.D.; Balch, A.J.; Lobb, R.; Lavell, L.; Linden, H.; et al. A Pilot Study of a Comprehensive Financial Navigation Program in Patients with Cancer and Caregivers. J. Natl. Compr. Cancer Netw. 2020, 18, 1366–1373. [Google Scholar] [CrossRef]
- Coughlin, S.S.; Dean, L.T.; Cortes, J.E. Financial assistance programs for cancer patients. Curr. Cancer Rep. 2021, 3, 119–123. [Google Scholar] [CrossRef]
- Mian, H.S.; Fiala, M.A.; Wildes, T.M. Burden of Treatment Among Older Adults With Newly Diagnosed Multiple Myeloma. Clin. Lymphoma Myeloma Leuk. 2021, 21, e152–e159. [Google Scholar] [CrossRef]
- Garcia-Manero, G.; Griffiths, E.A.; Steensma, D.P.; Roboz, G.J.; Wells, R.; McCloskey, J.; Odenike, O.; DeZern, A.E.; Yee, K.; Busque, L.; et al. Oral cedazuridine/decitabine for MDS and CMML: A phase 2 pharmacokinetic/pharmacodynamic randomized crossover study. Blood 2020, 136, 674–683. [Google Scholar] [CrossRef]
- Dee, E.C.; Nipp, R.D.; Muralidhar, V.; Yu, Z.; Butler, S.S.; Mahal, B.A.; Nguyen, P.L.; Sanford, N.N. Financial worry and psychological distress among cancer survivors in the United States, 2013–2018. Support. Care Cancer 2021, 29, 5523–5535. [Google Scholar] [CrossRef]
- Ethun, C.G.; Bilen, M.A.; Jani, A.B.; Maithel, S.K.; Ogan, K.; Master, V.A. Frailty and cancer: Implications for oncology surgery, medical oncology, and radiation oncology. CA Cancer J. Clin. 2017, 67, 362–377. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Baseline Demographic Variables | Respondents with Cancer | ||
|---|---|---|---|
| Blood Cancer Respondents (95% Confidence Interval) | Solid Tumor Respondents (95% Confidence Interval) | p Value | |
| N | 398 | 6248 | |
| Mean age, years | 61.5 (59.2–63.7) | 63.5 (63.0–64.0) | 0.08 |
| Mean time after diagnosis, years | 1.5 (0.8–2.2) | 2.2 (1.9–2.4) | 0.08 |
| Sex, male (%) | 52.8 (46.5–59.1) | 44.7 (43.1–46.2) | 0.01 |
| Race, white (%) | 93.4 (90.5–96.3) | 90.2 (89.2–91.2) | 0.08 |
| Ethnicity, Hispanic (%) | 6.3 (3.4–9.2) | 8.9 (7.7–10.1) | 0.15 |
| Marital status, married (%) | 59.7 (53.6–65.7) | 58.5 (57.0–60.1) | 0.72 |
| Persons in the family, number | 2.4 (2.3–2.6) | 2.3 (2.2–2.3) | 0.06 |
| Educational status, college and above (%) | 64.8 (57.5–72.0) | 61.0 (59.1–62.9) | 0.33 |
| Total combined family income (%) | 0.03 | ||
| Less than USD 50,000 | 37.7 (31.8–43.6) | 46.6 (44.9–48.4) | |
| USD 50,000–USD 99,999 | 33.0 (27.0–39.0) | 28.7 (27.1–30.2) | |
| USD 100,000 or more | 29.3 (22.9–35.7) | 24.7 (23.2–26.2) | |
| Above the poverty threshold (%) | 92.8 (90.0–95.6) | 89.6 (88.5–90.7) | 0.07 |
| Currently lacks health insurance coverage (%) | 2.4 (0.1–4.8) | 3.2 (2.6–3.8) | 0.56 |
| Currently covered by Medicaid or other public assistance/state-sponsored plan (%) | 14.3 (9.2–19.4) | 15.2 (13.8–16.6) | 0.75 |
| Currently covered by private health insurance (%) | 64.0 (58.4–69.6) | 59.1 (57.4–60.7) | 0.10 |
| Currently covered by Medicaid (%) | 10.7 (7.3–14.1) | 12.3 (11.2–13.4) | 0.40 |
| Currently covered by Medicare (%) | 52.8 (46.4–59.3) | 55.6 (53.9–57.2) | 0.42 |
| Baseline health status, fair to poor (%) | 40.6 (34.3–46.9) | 32.3 (30.8–33.7) | 0.008 |
| Activity limitation (%) | 62.3 (54.6–70.0) | 61.7 (59.8–63.6) | 0.89 |
| Geographic region (%) | 0.13 | ||
| Northeast | 21.5 (16.3–26.8) | 19.5 (17.9–21.0) | |
| Northcentral/Midwest | 24.1 (18.8–29.3) | 22.5 (21.1–23.9) | |
| South | 29.4 (23.8–35.0) | 36.9 (35.1–38.6) | |
| West | 25.0 (19.0–31.1) | 21.1 (19.5–22.7) | |
| Study Measure | Factor Loadings | Communality Estimates |
|---|---|---|
| Medical care utilization (in the last 12 months) | Factor eigenvalue: 1.30 | |
| Received care 10+ times | 0.59 | 0.35 |
| >4 days hospitalized, if hospitalized ≥ 1× | 0.56 | 0.31 |
| >1 times hospitalized, if hospitalized ≥ 1× | 0.55 | 0.30 |
| >1 emergency room visit | 0.29 | 0.09 |
| >7 visits to a doctor or health professional | 0.47 | 0.22 |
| Saw or spoke to medical specialist | 0.19 | 0.04 |
| Financial barriers to care (in the last 12 months) | Factor eigenvalue: 4.16 | |
| Delayed medical care due to cost | 0.61 | 0.37 |
| Delayed refilling medications to save money | 0.80 | 0.63 |
| Took less medication to save money | 0.80 | 0.64 |
| Skipped medications to save money | 0.77 | 0.59 |
| Could not afford medical care | 0.68 | 0.46 |
| Could not afford dental care | 0.52 | 0.27 |
| Could not afford medications | 0.71 | 0.50 |
| Could not afford follow-up care | 0.57 | 0.33 |
| Could not afford specialist care | 0.60 | 0.36 |
| Financial distress of affording care | Factor eigenvalue: 4.41 | |
| Worried about standard of living | 0.76 | 0.58 |
| Worried about medical costs of illness/accident | 0.77 | 0.59 |
| Worried about paying rent | 0.82 | 0.67 |
| Worried about credit card payments | 0.73 | 0.54 |
| Worried about medical costs of healthcare | 0.72 | 0.52 |
| Worried about money for retirement | 0.76 | 0.58 |
| Worried about monthly bills | 0.84 | 0.71 |
| Worried about medical bills | 0.48 | 0.23 |
| (A) Association of Extracted Domain Factors and Blood Cancer Diagnosis | |||
|---|---|---|---|
| Extracted Factor for Each Domain | Regression Coefficient (β) Estimate | t Value | p Value |
| Medical care utilization (in the last 12 months) | 0.36 | 2.35 | 0.02 |
| Financial barriers to care (in the last 12 months) | −0.19 | −4.84 | <0.0001 |
| Financial distress of affording care | 0.64 | 2.28 | 0.03 |
| (B) Association of Individual Study Outcomes and Blood Cancer Diagnosis | |||
| Odds ratio (95% CI), compared to solid tumor respondents | Wald’s p value | ||
| Medical care utilization (in the last 12 months) | |||
| Received care 10+ times | 1.19 (0.84–1.69) | 0.34 | |
| >4 days hospitalized, if hospitalized ≥ 1× | 1.37 (0.90–2.08) | 0.15 | |
| >1 times hospitalized, if hospitalized ≥ 1× | 1.67 (0.97–2.89) | 0.07 | |
| >1 emergency room visit | 0.93 (0.70–1.24) | 0.61 | |
| >7 visits to a doctor or health professional | 1.01 (0.77–1.34) | 0.93 | |
| Saw or spoke to medical specialist | 1.73 (1.17–2.57) | 0.01 | |
| Financial barriers to care (in the last 12 months) | |||
| Delayed medical care due to cost | 0.47 (0.22–1.03) | 0.06 | |
| Delayed refilling medications to save money | 0.37 (0.18–0.76) | 0.01 | |
| Took less medication to save money | 0.42 (0.20–0.86) | 0.02 | |
| Skipped medications to save money | 0.49 (0.25–0.99) | 0.05 | |
| Could not afford medical care | 0.52 (0.18–1.53) | 0.24 | |
| Could not afford dental care | 0.87 (0.51–1.49) | 0.61 | |
| Could not afford medications | 0.51 (0.27–0.96) | 0.04 | |
| Could not afford follow-up care | 0.29 (0.10–0.89) | 0.03 | |
| Could not afford specialist care | 0.22 (0.07–0.73) | 0.01 | |
| Financial distress of affording care | |||
| Worried about standard of living | 1.25 (0.64–2.44) | 0.52 | |
| Worried about medical costs of illness/accident | 0.86 (0.43–1.71) | 0.66 | |
| Worried about paying rent | 1.58 (0.83–2.99) | 0.16 | |
| Worried about credit card payments | 2.09 (0.62–7.00) | 0.23 | |
| Worried about medical costs of healthcare | 3.36 (1.50–7.51) | <0.01 | |
| Worried about money for retirement | 1.64 (0.87–3.10) | 0.12 | |
| Worried about monthly bills | 1.23 (0.62–2.45) | 0.55 | |
| Worried about medical bills | 1.30 (0.78–2.17) | 0.32 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, C.T.; Veenstra, C.M.; Patel, M.R. Divergent Patterns in Care Utilization and Financial Distress between Patients with Blood Cancers and Solid Tumors: A National Health Interview Survey Study, 2014–2020. Cancers 2022, 14, 1605. https://doi.org/10.3390/cancers14071605
Su CT, Veenstra CM, Patel MR. Divergent Patterns in Care Utilization and Financial Distress between Patients with Blood Cancers and Solid Tumors: A National Health Interview Survey Study, 2014–2020. Cancers. 2022; 14(7):1605. https://doi.org/10.3390/cancers14071605
Chicago/Turabian StyleSu, Christopher T., Christine M. Veenstra, and Minal R. Patel. 2022. "Divergent Patterns in Care Utilization and Financial Distress between Patients with Blood Cancers and Solid Tumors: A National Health Interview Survey Study, 2014–2020" Cancers 14, no. 7: 1605. https://doi.org/10.3390/cancers14071605
APA StyleSu, C. T., Veenstra, C. M., & Patel, M. R. (2022). Divergent Patterns in Care Utilization and Financial Distress between Patients with Blood Cancers and Solid Tumors: A National Health Interview Survey Study, 2014–2020. Cancers, 14(7), 1605. https://doi.org/10.3390/cancers14071605